Embed Size (px)
Citation preview

© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–1
Gerald W. Staton, Jr., m.d.Roland H. Ingram, Jr., m.d.
Chronic diffuse infiltrative lung disease encompasses a wide va-riety of disorders that primarily affect the alveoli and lung inter-stitium; involvement of the airways and the pulmonary vascula-ture is secondary to the interstitial process.
Chronic diffuse infiltrative lung disease affects a surprisinglylarge proportion of the population. A study from New Mexicosuggests a prevalence of 81 cases per 100,000 in males and 67 casesper 100,000 in females. Pulmonary fibrosis and idiopathic pulmo-nary fibrosis (IPF) are the most common diagnoses.1 In the UnitedStates, some of these disorders are more common in ethnic mi-norities, though data are incomplete.2
Pathogenesis
Certain pathogenetic mechanisms of lung injury may affect thedevelopment of diffuse infiltrative lung disease. In animal studies,several causative agents (e.g., bleomycin, paraquat, radiation, andcyclophosphamide) have been shown to produce a pattern of in-jury that resembles common idiopathic varieties of the disorder.3
In these models, there is initial damage to type I epithelial andcapillary endothelial cells. After a phase of edema and mild hem-orrhage, sometimes with extravascular fibrin accumulation, thereis an influx of neutrophils. Newly recruited lymphocytes and mac-rophages appear a few days later. Under the influence of variousgrowth factors, the type II cells replicate and spread out, replacingthe damaged type I epithelial cells. Within 2 weeks, collagen, elas-tin, and other extracellular matrix components are present, andeventually, extensive lung fibrosis becomes evident. A combina-tion of environmental exposures and genetic susceptibility mayplay a significant role in the pathogenesis of the disease.4 Varia-tions in this common pathway lead to the specific diseases dis-cussed in this subsection.
Approach to the Patient with Suspected Chronic DiffuseInfiltrative Lung Disease
Although more than 100 causes of diffuse infiltrative lung dis-ease have been described, a smaller group of causes accounts forthe vast majority of cases. Given the nonspecificity of the clinical,radiographic, and sometimes even pathologic features, the differ-ential diagnosis should be approached carefully.5 In all cases, ahistory and physical examination should be performed, a chestradiograph should be taken, and pulmonary function should beevaluated. Although such measures often do not lead to a defini-tive diagnosis, they help determine the likeliest causes in a givencase and thus serve to markedly limit the diagnostic possibilities,thereby reducing costs and effort of further studies.
presenting symptoms and patient history
The most common presenting complaints in diffuse infiltrativelung disease are dyspnea of gradual onset—initially with extremeexertion—and nonproductive cough. Chest pain and hemoptysisare uncommon except in specific disorders.
The history should include careful questioning as to the dura-tion of symptoms—usually cough or dyspnea. Often, symptomshave been present for many months or even years, which wouldrender an infectious cause very unlikely. In contrast, a more rap-idly evolving course, over days to weeks, increases concern aboutinfection. Exclusion of infection as the cause of diffuse infiltrativelung disease is of paramount importance because of the need forspecific antimicrobial therapy and because many noninfectiouscauses of this disorder are treated with glucocorticoids. Fevermay be observed in several noninfectious types of diffuse infiltra-tive lung disease (e.g., sarcoidosis, hypersensitivity pneumonitis,collagen vascular disease, and drug-induced disease), but its pres-ence should always alert the clinician to the possibility of infec-tion. Infectious diffuse infiltrative lung disease that evolves suba-cutely over weeks to months is rarely caused by common viral orbacterial organisms. On the other hand, mycobacterial and path-ogenic fungal infections (e.g., histoplasmosis, coccidioidomyco-sis, and blastomycosis) can present subacutely and are usually as-sociated with fever. Perhaps the most common infectious cause isPneumocystis carinii pneumonia (PCP) in a patient with AIDS.AIDS-related PCP may present as dyspnea that evolves slowlyover many weeks, occasionally without fever or other evidence ofsystemic toxicity; this pattern may resemble that of common non-infectious causes of diffuse infiltrative lung disease. A careful his-tory regarding risk factors for HIV infection is a critical part of theevaluation of all patients with recent-onset diffuse infiltrativelung disease.
In addition to establishing the duration of illness and the pres-ence or absence of fever and other systemic complaints, the histo-ry should focus on the patient’s occupation and medications.Many different occupational exposures can lead to diffuse infiltra-tive lung disease, but most are rarely encountered in clinical prac-tice. Occupation-related varieties are caused by exposure to the in-organic dusts, such as asbestos and silica, or to organic dusts thatcause hypersensitivity pneumonitis. Asbestosis typically becomesevident many years after exposure, so in taking the history, it isimportant to note the patient’s prior occupations. The most com-mon cause of occupation-related hypersensitivity pneumonitis isfarmer’s lung, which primarily affects dairy farmers. A farmershould be questioned carefully about any relation between respi-ratory or systemic symptoms and exposure to organic material(moldy hay or grain) that may contain thermophilic actino-mycetes. The history should also include questions about possi-ble exposure to pigeons or pet birds and to humidifiers, becausesuch exposure can result in hypersensitivity pneumonitis [seeTable 1].
Many drugs have been reported to cause diffuse infiltrativelung disease. A history should focus on both prescribed and over-the-counter medications and should include questions aboutmedications taken during the preceding weeks or months [seeTable 2].
Finally, the history should seek to determine whether therehave been symptoms that indicate the presence of an underlyingcollagen vascular disease or vasculitis. A history that reveals theprior occurrence of Raynaud phenomenon, photosensitivity, skinrashes, or arthritis carries great diagnostic relevance.
V C H R O N I C D I F F U S E I N F I LT R AT I V E L U N GD I S E A S E

physical examination
The physical examination has less diagnostic utility than thehistory but is important nonetheless. Collagen vascular disordersmay be suggested by detection of synovitis, telangiectasia, sclero-dactyly, or a malar rash. Sarcoidosis also involves extrapulmo-nary organs and should be suspected if uveitis, erythema nodosum,or plaquelike skin lesions consistent with cutaneous sarcoidosisare detected. Malignant diffuse infiltrative lung disease (i.e., lym-phangitic spread) may be associated with findings relevant to theprimary tumor, such as an abdominal or breast mass, hepato-megaly, or guaiac-positive stools. Finally, cardiovascular exami-nation is very important because on occasion, chronic pulmonaryvenous congestion resulting from occult mitral stenosis or leftventricular failure may present as diffuse infiltrative lung disease.
laboratory examination
The laboratory examination comprises studies that are more orless routine (e.g., complete blood count, biochemical screening)and those that are more specialized. Sarcoidosis may be suggest-ed by cytopenias if the bone marrow is involved or by the pres-ence of hypercalcemia or elevated serum liver enzyme levels.Collagen vascular disease and malignancy may also result in cy-topenias. Peripheral eosinophilia would suggest chronic eosino-philic pneumonia. Uncommonly, eosinophilic granuloma pre-
sents as a diffuse pulmonary disorder together with laboratoryevidence of diabetes insipidus.
Additional laboratory tests, such as autoimmune serology anddetermination of angiotensin-converting enzyme (ACE) level,may prove useful, depending on the clinical and radiographicfeatures in a given case. Antinuclear antibodies or rheumatoidfactor is usually present in the serum of patients with collagenvascular disorders, but it is also found in low titer in up to 50% ofpatients with IPF. Increased serum levels of ACE are suggestiveof sarcoidosis, but ACE can also be elevated in miliary tuberculo-sis, berylliosis, asbestosis, and silicosis. Hypersensitivity pneumo-nitis is nearly always associated with the presence of serum anti-body against the offending antigen. However, the presence ofantibody against one of the causative agents of hypersensitivitypneumonitis in serum does not prove that hypersensitivity pneu-monitis is the cause of diffuse infiltrative lung disease but onlythat there has been sufficient exposure to the antigen to elicit animmunologic response. Resolution of pneumonitis with disap-pearance of antibody after stopping the exposure provides a moreconclusive association.
chest radiography
Radiographic features are for the most part nonspecific. Dif-fuse infiltrative lung disease may be characterized by bilaterally
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–2
Probable Antigen(s)
Thermophilic actinomycetes, Micropolyspora faeni, Thermoactino-myces vulgaris
Thermophilic actinomycetes, T. sacchari, T. vulgaris
Bird proteins
Rat urine proteins
Altered proteins
Thermophilic actinomycetes, T. candidus, T. vulgaris, Penicilliumspecies, Amoeba species, Klebsiella species, and Candida species
Antigen Source
Moldy hay
Moldy pressed sugarcane (Bagasse)
Bird droppings, products, and feathers
Rat fur
Chemical exposures
Contaminated humidifiers, dehumidifiers,air conditioners, and heating systems
Disease
Farmer’s lung
Bagassosis
Multiple bird handler’s diseases
Laboratory worker’s lung
Diisocyanates and trimellitic anhydrides
Ventilator lung
Table 1 Common Causes of Hypersensitivity Pneumonitis
Notes
Dose related, worse with O2Induces pulmonary fibrosis, with high mortality and occasionally alveolar proteinosisVariable onset and courseSynergistic with mitomycin-CDose related, delayed onset
Long half-life, induces ARDS after proceduresInduce SLE
Produces granulomas, as found on biopsyInduces Goodpasture-like syndrome, SLE, bronchiolitis obliteransInjectable only; induces BAL lymphocytosis
Induces acute and chronic parenchymal lung diseaseBOOP, PIE, or pulmonary fibrosis
I.V. injection produces talc granulomasInduces BOOP, alveolar hemorrhage
Drugs
BleomycinBusulfanCyclophosphamideVinblastineNitrosoureas
AmiodaroneHydralazine, others
MethotrexatePenicillamineGold
NitrofurantoinSulfasalazine
MethylphenidateCocaine
Category
Chemotherapeutic agents
Cardiovascular drugs
Anti-inflammatory drugs
Antibiotics
Illicit drugs
Table 2 Drugs That Commonly Induce Chronic Parenchymal Lung Disease
ARDS—acute respiratory distress syndrome BAL—bronchoalveolar lavage BOOP—bronchiolitis obliterans organizing pneumonia PIE—peripheral eosinophilia

symmetrical interstitial, alveolar, or mixed alveolar-interstitial ra-diographic patterns. In some cases, the lung fields appear com-pletely normal on the chest radiograph despite the presence ofsignificant clinical and physiologic abnormalities. There are cer-tain ancillary radiographic clues that, if present, may help in mak-ing the differential diagnosis and in narrowing the list of possiblecauses [see Table 3].
high-resolution computed tomography
The use of high-resolution computed tomography (HRCT)represents a significant advance in the evaluation of diffuse pa-renchymal lung disease. With the use of HRCT, the extent, loca-tion, and pattern of lung involvement can be determined withgreat accuracy [see Figure 1]. HRCT can often detect abnormalitiesin patients who have symptoms of interstitial lung disease butwhose chest radiographs are normal. When combined with clini-cal data and chest radiography, HRCT of the chest can lead to aspecific diagnosis in 60% to 80% of cases.6 When HRCT indicatesa specific diagnosis (e.g., eosinophilic granuloma), the need for alung biopsy is eliminated.5
pulmonary function testing
Pulmonary function testing provides diagnostic clues to thepresence of diffuse infiltrative lung disease and is useful duringthe course of the disease. The hallmarks of the disorder include arestrictive ventilatory pattern (reduced lung volume), a normal orincreased ratio of forced expiratory volume in 1 second to forcedvital capacity (FEV1/FVC), a reduction in the diffusing capacityof the lung for carbon monoxide (Dlco), and a reduction in arter-ial oxygen tension (Pao2 ) associated with normal or reduced ar-terial carbon dioxide tension (Paco2 ). In addition, there is usuallysignificant exercise limitation resulting from a fall in Pao2 , abnor-malities in respiratory mechanics, associated pulmonary vasculardisease, or a combination of these factors.
bronchoalveolar lavage
In most cases, the cause of lung disease remains uncertain de-spite careful clinical, radiographic, laboratory, and physiologicevaluation. The next step is usually to perform bronchoscopy withbronchoalveolar lavage (BAL) and transbronchial lung biopsy.Certain causes can be diagnosed solely by BAL, others only by bi-opsy, and some by either technique. BAL is most useful for diag-nosing infectious causes, especially PCP. The diagnostic sensitiv-ity of this procedure for AIDS-related PCP is approximately 90%to 95%. Thus, it is the procedure of choice for diagnosing the 20%to 50% of cases of AIDS-related PCP that cannot be diagnosed
by induced sputum examination. Other opportunistic infections,such as cytomegalovirus pneumonia and disseminated fungal ortuberculous infection, can also be diagnosed by BAL. Noninfec-tious causes that can be diagnosed by this technique include alve-olar proteinosis, lymphangitic carcinomatosis, and alveolar cellcarcinoma. In addition, BAL may provide helpful information byrevealing one of the following changes: (1) increased numbers ofeosinophils in chronic eosinophilic pneumonia, (2) asbestos bod-ies in asbestosis, (3) so-called foamy cells with lamellar inclusionsin amiodarone-induced disease, (4) hyperplastic and atypical typeII pneumocytes in cytotoxic drug-induced lung injury, (5) Langer-hans cells in eosinophilic granuloma, and (6) a bloody effluentwith abundant hemosiderin in alveolar macrophages in diffusealveolar hemorrhage. Quantitating the number and distributionof inflammatory cells (e.g., macrophages, lymphocytes, and neu-trophils) may suggest a specific diagnosis.7 The alveolar lavage
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–3
b
a
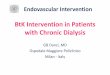
Figure 1 High-resolution computed tomography (HRCT) inpatients with chronic diffuse interstitial lung disease can occa-sionally suggest a specific diagnosis. (a) Posteroanterior radiog-raphy demonstrates a diffuse interstitial process, but differen-tial diagnosis is lengthy. (b) HRCT shows a combinedinterstitial and cystic process that is virtually diagnostic of eosinophilic granuloma of the lung.
Primary Diagnostic Considerations
Sarcoidosis, lymphoma, carcinoma, granulo-matous infection
Collagen vascular disease, asbestosis, lymphan-giomyomatosis (chylous), tuberculosis
Eosinophilic granuloma, Pneumocystis cariniipneumonia, lymphangiomyomatosis
Silicosis, eosinophilic granuloma, sarcoidosis
Eosinophilic pneumonia, bronchiolitis obliteransorganizing pneumonia, drug-induced injury
Associated Radiographic Finding
Hilar adenopathy
Pleural effusion
Pneumothorax
Upper lung zone predominance
Peripheral predominance
Table 3 Radiographic Clues to Diagnosis of Diffuse Infiltrative Lung Disease

liquid of healthy nonsmokers typically contains 84% to 99% mac-rophages, 1% to 14% lymphocytes, and 0% to 1% neutrophils.The common causes of nongranulomatous diffuse infiltrativelung disease (e.g., IPF, some of the collagen vascular disorders,and asbestosis) are often characterized by a neutrophilic alveoli-tis, whereas sarcoidosis and hypersensitivity pneumonitis are as-sociated with increases in lymphocytes. However, overlap exists(e.g., IPF with an increased number of lymphocytes or sarcoido-sis with a normal number of lymphocytes).
lung biopsy
In many cases, the diagnosis remains unknown until a lung biopsy is obtained. Pathologically, these disorders may be charac-terized by variable degrees of involvement of alveolar septa oralveoli by inflammatory cells, mesenchymal cells, fibrosis, granu-loma, or neoplastic cells. In rare instances, the abnormal substancethat accumulates in the lung parenchyma is blood, proteinaceousmaterial (alveolar proteinosis), amyloid, smooth muscle (lym-phangiomyomatosis or tuberous sclerosis), or an abnormal mate-rial that is deposited as a result of an inherited storage disorder(Gaucher disease, Niemann-Pick disease, or Hermansky-Pudlaksyndrome).
Lung tissue may be obtained either by transbronchial lung bi-opsy during bronchoscopy [see Table 4] or by one of two open bi-opsy techniques: traditional open lung biopsy or video-assistedthoracoscopy. Transbronchial lung biopsy is most useful in diag-nosing infectious diffuse infiltrative lung disease and sarcoidosis.Noncaseating granulomas can be demonstrated on transbronchi-al lung biopsy specimens in 70% to 90% of patients with sarcoido-sis. The diagnostic yield is highest (approximately 90%) in patientswith radiographically apparent lung disease (stages II and III )and lowest (approximately 70%) in patients with hilar adenop-athy alone (stage I). Whether one proceeds to open lung biopsyafter obtaining a nonspecific transbronchial lung biopsy dependson the specific clinical and radiographic features in an individual
case, the impact that a more precise diagnosis would have on ther-apy, and an assessment of the risk of open lung biopsy in a givencase5 [see Figure 2]. The frequency with which open lung biopsy isperformed to better define the histopathologic features of nonin-fectious forms of the disease varies greatly among different cen-ters. Use of video-assisted thoracoscopy rather than open lung bi-opsy has not resulted in the anticipated decrease in morbidityand cost.8
treatment
The treatment recommendations in this subsection are basedon small, nonrandomized series (often without control groups),case reports, and clinical experience. There are very few random-ized controlled trials of treatment for these diseases.
Even before a specific diagnosis is known, preventive mea-sures can be initiated. Immunization against pneumococcal anti-gens (every 5 years) and yearly immunizations against influenzaare indicated. Patients who have a reversible obstructive defectmay benefit from bronchodilators. Supplemental oxygen given atrest and with exercise will often improve patients’ tolerance of ac-tivities of daily living.9 Pulmonary hypertension and cor pul-monale occurring in patients with far advanced disease can beimproved with appropriate treatment [see 14:XI Pulmonary Hyper-tension, Cor Pulmonale, and Primary Pulmonary Vascular Diseases].
Chronic Diffuse Infiltrative Lung Disease of Known Etiology
drug-induced disease
Many different drugs have been reported to cause diffuse infil-trative lung disease [see Table 2].10 Estimates are that drug-inducedlung disease affects several hundred thousand patients each year.To minimize the morbidity and mortality of drug-induced dis-ease, early recognition is critical. Discontinuance of the offendingagent is often followed by spontaneous improvement, whereasfailure to appreciate the causal relation between the drug and thepulmonary disease can lead to irreversible lung injury. Unfortu-nately, certain aspects of drug-induced disease can hinder therecognition of this cause-and-effect relation. First, the drugs thatcause diffuse infiltrative lung disease are numerous, and drug-in-duced lung disease usually occurs in only a small fraction of pa-tients who receive such drugs. Second, the onset of the pulmo-nary disease may occur weeks to months after the drug is begun.In the case of cytotoxic drug-induced disease, the onset of respira-tory symptoms can occur many weeks after the last exposure tothe offending agent. Finally, the drugs that cause diffuse infiltra-tive lung disease are often prescribed for conditions that arethemselves associated with an increased risk of the disease. Forexample, a patient who receives an anticancer chemotherapeuticagent is at risk for infection and tumor infiltration of the lung.Similarly, the anti-inflammatory drugs that cause parenchymallung disease are often prescribed for one of the collagen vasculardisorders that can have diffuse infiltrative lung disease as one ofits features. For all these reasons, the physician must have aheightened awareness of the possibility of a drug-induced etiolo-gy in patients with diffuse infiltrative lung disease.
Disease Induced by Cytotoxic Drugs
Diffuse infiltrative lung disease is a major cause of morbidityand mortality in patients undergoing treatment for an underlyingmalignancy.10 In some cases, the drug used to treat the malignan-cy is the direct cause of the pulmonary lesions. Some patients die
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–4
Table 4 Diagnostic Efficacy of Transbronchial Lung Biopsy
Diseases Frequently Diagnosed by TLB FindingsInfectious diffuse infiltrative lung diseaseSarcoidosisLymphangitic carcinomaAlveolar cell carcinomaTalc-induced diffuse infiltrative lung disease
Diseases Suggested by TLB FindingsCytotoxic-induced diseaseBronchiolitis obliterans organizing pneumonia (occasionally)Eosinophilic pneumoniaHypersensitivity pneumonitis
Not Diagnosable by TLB FindingsIdiopathic pulmonary fibrosis
Diseases commonly misdiagnosed as idiopathic pulmonary fibrosisEosinophilic granulomaLymphangiomyomatosisBronchiolitis obliterans organizing pneumoniaHypersensitivity pneumonitisSarcoidosis (occasional cases)Lymphangitic carcinoma (occasional cases)
TLB—transbronchial lung biopsy

of cytotoxic drug-induced pulmonary toxicity, and others experi-ence permanent impairment of lung function irrespective of beingcured of their malignancy. Most of the drugs used in the treatmentof malignancy have the potential to cause diffuse infiltrative lungdisease. The major offending agents are bleomycin, cyclophos-phamide, methotrexate, and the nitrosoureas. Cyclophosphamideand methotrexate are also being used increasingly in the manage-ment of nonmalignant conditions, though they are administeredat much lower doses in the treatment of these disorders than in thetreatment of malignancy. Drug-induced pulmonary disease oc-curs less frequently at these lower doses, but it can occur.
Clinical manifestations The clinical features of cytotoxicdrug-induced disease are nonspecific. Cough and dyspnea are of-ten prominent, and fever is not uncommon. The chest radiographusually reveals bilateral and symmetrical interstitial infiltrates,though asymmetry may be seen early in the course of disease.The pace of the disease, both clinically and radiologically, is vari-able. Most often the onset is subacute, with cough and dyspneaoccurring over several weeks. A more explosive onset, with fea-tures of acute respiratory distress syndrome (ARDS) and an ur-gent need for mechanical ventilatory support, can also be seen.Lung fibrosis resulting from therapy with bleomycin and otheragents can occur insidiously over many months.
Pathologic features The pathologic features of cytotoxicdrug-induced disease are distinctive but not pathognomonic. In-
terstitial inflammatory cell infiltration and fibrosis may be ob-served. However, the most characteristic finding of cytotoxicdrug-induced disease is an increase in type II pneumocytes thatshow marked atypia. This pathologic feature is highly suggestiveof cytotoxic drug-induced disease, but similar changes in type IIcells can be seen with severe viral infections and during thereparative phase of ARDS.
A somewhat different pathologic picture is seen with diseaseinduced by cytarabine or methotrexate. Cytarabine has been as-sociated with an often fatal form of noncardiac pulmonary edema.Methotrexate-induced disease has been associated with granulo-mas, lymphocytic alveolitis, and a significant increase in helper T cells.
Diagnosis Diagnosis of cytotoxic drug-induced lung diseaseis established by defining a previous exposure to the offendingagent, excluding infection as the cause of the lung damage, anddemonstrating pathologic features that are consistent with drug-induced injury. The temporal relation between drug exposure andthe onset of lung disease is variable. An interval of a few weeks be-tween the last exposure to the drug and the onset of symptoms isnot unusual; in rare cases, this interval can be as long as severalmonths. The clinical and radiographic features of lung disease in-duced by a cytotoxic drug are indistinguishable from those causedby opportunistic infection. Thus, an aggressive approach to diag-nosis is required. Failure to detect an infectious etiology by bron-choscopy increases the likelihood of drug-induced disease, espe-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–5
History (including occupations and hobbies), physical examination,
review of old radiographs
Bronchosocopy, BAL,lung biopsy (histology and particle
analysis), VATS
Occupation and environment(inhalation of organic antigen
or particle; drug reaction) General Categories
More Certainty Further investigation ofcauses in workplace or home
Aspect of systemic illness(multiorgan involvement,
chronic infection, aspiration, malignancy)
Assess function of other organs; blood serologies;
mammography; endoscopy
Cause not obvious, difficult tojudge; often limited to lungs
(IPF, sarcoidosis, LAM, LCG, pulmonary–renal syndromes)
High-resolution lung CT scan,pulmonary function test, assessment of DLco, blood
serologies
Confirmation Assess response to therapy;rule out infection or tumor
Tissue diagnosis
Rarely Rarely Often
Trial of avoidance
Figure 2 Algorithm for the evaluation of diffuse interstitial lung disease.5 (BAL—bronchoalveolar lavage; IPF—idiopathic pulmonary fibrosis; LAM—lymphangioleiomyomatosis; LCG—Langerhans cell granulomatosis; DLco—diffusing capacity of the lung for carbonmonoxide; VATS—video-assisted thoracoscopic surgery).

cially if the characteristic type II cell changes are observed in atransbronchial lung biopsy specimen. However, open lung biopsymay be required to confidently exclude infection and to better de-fine the histopathologic features of cytotoxic drug-induced injury.Even with open lung biopsy, the diagnosis of cytotoxic drug-in-duced disease remains inferential because there are no pathogno-monic criteria on which to base a diagnosis.
Treatment Elimination of further drug exposure is essentialin managing cytotoxic drug-induced lung disease. Anecdotal re-ports indicate that glucocorticoid therapy has been associatedwith rapid improvement in gas exchange and reversal of chestradiograph abnormalities. If the cytotoxic drug-induced diseaseis very severe or appears to progress despite elimination of furtherdrug exposure, an empirical course of glucocorticoids is advisable.
Prevention Cytotoxic drug-induced lung disease is not eas-ily prevented, because these drugs are often necessary for opti-mal treatment of an underlying potentially fatal malignancy.For patients with testicular carcinoma who receive bleomycin,the risk of pulmonary lesions appears to be dose related. Moni-toring of the Dlco and spirometry during therapy may in somecases permit detection of lung injury early enough to allow dis-continuance of further drug exposure and lessen the likelihoodof permanent and severe lung impairment. However, therapyfor non-Hodgkin lymphoma with bleomycin in combinationwith doxorubicin, cyclophosphamide, vincristine, and pred-nisone causes diffuse infiltrative lung disease in a non–dose-de-pendent fashion, thereby impeding efforts to prevent it. Per-haps the most effective strategy to reduce morbidity andmortality from cytotoxic drug-induced disease is not to preventit altogether but rather to diagnose it as early as possible; furtherdrug exposure can then be avoided by switching to alternativechemotherapy regimens whenever feasible.
Noncytotoxic Drugs That May Cause Disease
Diffuse infiltrative lung disease may result from exposure to avariety of noncytotoxic agents, including antibiotics, anti-inflam-matory agents, antiarrhythmics, and illicit drugs.10 In addition,this disorder may be one of the manifestations of drug-inducedsystemic lupus erythematosus (SLE).
Nitrofurantoin Nitrofurantoin, an antibacterial agent usedprimarily for the treatment of urinary tract infection, is one of themost common causes of drug-induced lung disease.10
Both acute and chronic pulmonary toxicity can occur, but theacute syndrome is much more common. The acute pleuropulmo-nary reaction begins 2 to 10 days after initial drug exposure and ismanifested by dyspnea, cough, and often fever. Pleurisy occursin one third of patients. The chest radiograph shows a pattern ofalveolar or interstitial infiltrates, sometimes accompanied by apleural effusion. Peripheral blood eosinophilia may be observed.The disorder is diagnosed on the basis of a history of recent expo-sure to nitrofurantoin and spontaneous resolution of the clinicaland radiographic changes 1 to 4 days after discontinuance of thedrug. This rate of resolution is much faster than would occurwith infection and serves to establish the diagnosis with a highdegree of certainty. Chronic toxicity is not associated with sys-temic symptoms and has a clinical and radiographic picture thatis indistinguishable from that of IPF. If there is no improvementwithin 2 to 3 months after withdrawal of the drug, corticosteroidtherapy is indicated.
Amiodarone Amiodarone is an antiarrhythmic agent that isused most often in the treatment of refractory ventricular tachy-arrhythmia. This drug is associated with a variety of dose-depen-dent toxic effects on different organs, but the major limitation to itsuse is pulmonary toxicity, which occurs in 5% to 7% of cases.Amiodarone-induced pulmonary toxicity is usually heralded bythe onset of cough and dyspnea that may initially be attributed tocongestive heart failure. Systemic symptoms, including low-gradefever, are not uncommon. The chest radiograph may show a bilat-eral, symmetrical interstitial process similar to that observed inother types of diffuse infiltrative lung disease. However, more un-usual radiographic patterns are not uncommon and include uni-lateral disease and isolated upper lobe disease; the latter findingmay suggest tuberculosis. Pleural effusion occurs occasionally.
A diagnosis of amiodarone-induced lung disease is establishedprimarily by excluding other likely causes of the pulmonary dis-order, especially infection and heart failure. Bronchoscopy withBAL and biopsy helps exclude infection and reveals the presenceof so-called foamy macrophages with lamellar inclusions (visual-ized by electron microscopy). These changes within macrophagesare indicative of exposure to amiodarone but do not prove that thedrug is the cause of the pulmonary process, because similar chang-es are seen in asymptomatic persons who are receiving the drug.
Withdrawal of the drug is the cornerstone of management, butglucocorticoids seem to be useful in more severe or persistent cas-es. Interestingly, there have been several reports of acute amio-darone-induced lung disease in patients who have undergonerelatively minor surgical procedures, such as placement of an au-tomatic defibrillator, or in those who have undergone pulmonaryangiography, possibly as a consequence of oxygen supplementa-tion during the procedure. Often, the disease follows a fulminantcourse, and sometimes the outcome is fatal. Because the half-lifeof the drug is several weeks, patients who undergo these proce-dures are still at risk for acute lung injury if the drug was discon-tinued 1 to 2 months before the procedure.
Gold and penicillamine Gold and penicillamine, used pri-marily for the management of rheumatoid arthritis and other colla-gen vascular disorders, can lead to diffuse infiltrative lung disease.It may be difficult to determine whether the pulmonary damage iscaused by the therapeutic agent or by the underlying disorder,even with an open lung biopsy. Discontinuance of the drug, alongwith empirical corticosteroid therapy if symptoms are severe, isadvisable. Penicillamine has also been implicated in cases of dif-fuse alveolar hemorrhage with glomerulonephritis, drug-inducedSLE, and panbronchiolitis with severe airflow obstruction.
Illicit drugs Illicit drugs can also cause diffuse infiltrativelung disease. Talc-induced granulomatosis and pulmonary fi-brosis can result from injection of crushed and dissolved am-phetamines or narcotic pills that have talc as the filler. The dis-ease can progress years after the last exposure, because the talcpersists in the lungs and continues to elicit an inflammatory re-sponse. Open lung or transbronchial lung biopsy reveals agranulomatous inflammation with abundant talc particles,which can be visualized with polarizing microscopy. Failure toevaluate granulomas with the polarizing microscope may leadto an erroneous diagnosis of sarcoidosis. The diagnosis canalso be made by detecting talc in the retina. Heroin use can leadto acute pulmonary edema but does not in itself cause a chron-ic diffuse infiltrative lung disease. Cocaine has been associatedwith acute pulmonary edema and has been reported to cause
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–6

diffuse alveolar hemorrhage and a syndrome of pulmonary in-filtrates with eosinophilia. Cocaine-related pulmonary reac-tions do not lead to chronic lung lesions.
pneumoconioses
Environmental or occupational exposure to particulate mattercan cause several pneumoconioses that manifest as asthma, chron-ic bronchitis, or diffuse parenchymal (mostly interstitial) disease.Representative pneumoconioses include asbestosis, silicosis, coalworker’s pneumoconiosis (CWP), and berylliosis.
Asbestosis
Exposure to asbestos, a silicate used in insulation, in friction-bearing surfaces, and to strengthen materials, is associated withthe development of pleural changes (plaques and effusions), anincreased incidence of malignancy (bronchogenic carcinoma andmesothelioma), and diffuse interstitial fibrosis. Only diffuse inter-stitial fibrosis is called asbestosis.11
Asbestosis is characterized by the gradual onset of dyspnea 20to 30 years after exposure to asbestos. Cough is usually presentbut is nonproductive unless the patient has been a smoker andhas complicating chronic bronchitis. Fine end-inspiratory ralescan be heard before the chest radiograph becomes abnormal, anddigital clubbing is common. In the late stages of asbestosis, signsof cor pulmonale may develop.
Early in the course of disease, the chest radiograph may benormal, but small, irregular linear shadows gradually develop inthe lower lung zones. Pulmonary function tests may show re-striction, decreased Dlco, and exercise-induced hypoxemia. Di-agnosis of asbestosis is made when a patient has a history of ex-posure to asbestos, pleural plaques (an objective indicator ofexposure), and, in uncertain cases, excess asbestos in specimensobtained from the lung (by BAL, transbronchial lung biopsy, oropen lung biopsy).
There is no specific treatment for patients with asbestosis.11
Silicosis
Silicosis is a chronic fibrotic lung disease caused by exposureto crystalline free silica.11 The occupational settings in which sig-nificant free-silica exposure may occur include certain types ofmining; the cutting, polishing, and carving of stone; foundry work;and abrasive cleaning (sandblasting). Exposure of approximately5 years’ duration is usually required for the development of sili-cosis unless the exposure is very heavy. There are two forms ofsilicosis: simple nodular silicosis, in which many patients areasymptomatic or suffer only from chronic bronchitis secondaryto tobacco use, and progressive massive fibrosis (PMF), in whichpatients may develop disabling dyspnea.
Physical findings are often absent. Radiographically, simplenodular silicosis is characterized by diffuse, small, rounded opac-ities that tend to be more prominent in the upper lobes. Hilarnode enlargement may be seen, sometimes with concentric (egg-shell) calcifications. In patients with PMF, the opacities coalesceinto large, irregularly shaped masses. In patients with simplenodular silicosis, pulmonary function may be normal or may ex-hibit a mixed pattern of obstruction and restriction. Severe restric-tion and hypoxemia, as well as pulmonary hypertension, devel-op in patients who have PMF.
Diagnosis of silicosis can usually be made if a patient has a his-tory of exposure and if the chest radiograph is consistent with sil-icosis (see above). In atypical cases, the presence of silica in BALliquid or in lung biopsy specimens (often guided by CT scan of
the chest) can establish the diagnosis and exclude tuberculosisand carcinoma.
Tuberculosis and infection with atypical mycobacteria occurwith increased frequency in patients with silicosis and may beconfused with the progression of the silicosis, making conclusivediagnosis difficult. Because cell-mediated immunity appears tobe normal in patients with silicosis, the tuberculin skin test can behelpful in identifying patients in whom diagnosis of tuberculosisshould be explored.
Silicosis has been thought to be an untreatable disease,11 thoughone report suggests that oral glucocorticoids reduce lung inflam-mation and improve lung function.12 Prevention of further expo-sure to silica and prevention and treatment of active tuberculosisare important aspects of care.
Coal Worker’s Pneumoconiosis
CWP is an uncommon cause of pulmonary fibrosis in workerswho are exposed to coal dust and graphite. Most of these patientsare miners.
Many patients with CWP have a chronic cough that is some-times productive of gray or black sputum, which may be causedby chronic bronchitis that is related to tobacco use or exposure tocoal dust. Much like silicosis, CWP comprises simple CWP andPMF. PMF is characterized by severe dyspnea, whereas simpleCWP is not associated with an increased incidence of dyspnea.The radiographic changes characteristic of simple CWP are small,rounded opacities; opacities that are larger than 1 cm are arbitrar-ily classified as PMF. Simple CWP does not progress if dust expo-sure is eliminated, whereas PMF can progress after exposure hasstopped.
There is no specific treatment for either form of disease.
Berylliosis
Beryllium is a metal that is used in modern high-technology in-dustries. High-intensity exposure to beryllium can cause an acutechemical bronchitis and pneumonitis, which is very rare today be-cause of strict environmental controls. However, chronic beryllio-sis is still frequently seen. Chronic berylliosis is characterized bymultisystemic granulomatous disease that has many similaritiesto sarcoidosis and that occurs months to years after exposure. Thenumber of chronic cases appears to be decreasing, probably be-cause of increased awareness of the disease and environmentalcontrols. Beryllium is thought to bind to host proteins that arecarried throughout the body. These beryllium-protein complexesstimulate a delayed hypersensitivity response, which producesgranulomatous inflammation at the sites of disease activity.
The symptoms of berylliosis are dyspnea, cough, chest pain,fatigue, weight loss, and arthralgia. Rales are not an early feature.The radiographic findings, which may precede clinical symp-toms, include ill-defined nodular and irregular opacities that aresometimes associated with hilar adenopathy. As the disease pro-gresses, the lungs become smaller and areas of honeycombingdevelop. Pulmonary function tests may be normal; more often,however, they are characterized by a low Dlco with or withoutrestriction, or they demonstrate mild obstruction. Other abnor-malities include hyperuricemia, hypercalcemia, hypercalciuria,and elevated serum levels of ACE.
The criteria for diagnosis include a well-documented historyof exposure or a demonstration of excess beryllium in patientspecimens; objective evidence on radiography and pulmonaryfunction testing for the presence of lower respiratory tract diseasethat is consistent with berylliosis; and demonstration of granulo-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–7

matous inflammation in the lung, lymph nodes, or other sites ofdisease activity.
Differentiating berylliosis from sarcoidosis may be difficult. Adiagnosis of sarcoidosis is suggested by the presence of uveitisand erythema nodosum, the presence of hilar adenopathy with-out parenchymal infiltrates, or improvement after short-term ad-ministration of steroids. A diagnosis of berylliosis is suggested bylymphocyte transformation in response to beryllium compoundsperformed on lymphocytes obtained from blood or BAL.
The most important step in the management of berylliosis isprevention of further exposure. Glucocorticoids may improve thecourse of the disease, but these agents may have to be given forthe rest of the patient’s life.13
hypersensitivity pneumonitis
The term hypersensitivity pneumonitis (allergic alveolitis) re-fers to interstitial lung disease that results from inhalation of or-ganic antigens.14 Several organic antigens cause this syndrome[see Table 1], but the most common form of hypersensitivity pneu-monitis, called farmer’s lung, is caused by inhalation of proteinsfrom thermophilic Actinomyces organisms present in moldy hayand grain. Other relatively common causes of hypersensitivitypneumonitis include pigeon breeder’s disease and bird fancier’sdisease, in which inhaled proteins from pigeons or pet birds in-
duce the syndrome. Humidifier lung disease is a type of hyper-sensitivity pneumonitis that results from exposure to contaminat-ed forced-air systems. The responsible antigens in such cases areActinomyces organisms, as in farmer’s lung, but also can includeAureobasidium organisms and various amebae. Forms of hyper-sensitivity pneumonitis other than farmer’s lung, pigeon breed-er’s disease, bird fancier’s disease, and humidifier lung diseaseare rare and generally result from exposure to antigens in ratherarcane occupations (e.g., paprika slicing and mummy wrapping).
Pathogenesis and Pathology
The pathogenesis of hypersensitivity pneumonitis is not fullyunderstood. The current hypothesis is that inhaled material caus-es direct activation of the alternative complement pathway, lead-ing to the formation of chemotactic factors for neutrophils and inturn to acute neutrophilic alveolitis. The products of complementactivation also stimulate the alveolar macrophages to producemonokines, causing a sequence of events that results in granulo-ma formation.
The pathologic changes in hypersensitivity pneumonitis havebeen well defined by examination of open lung biopsy specimensof a large number of patients with farmer’s lung disease. All pa-tients have an interstitial pneumonitis, and two thirds have scat-tered granulomas. Fibrosis may occur in more chronic forms ofthe disease, and as many as 50% of patients may have bronchioli-tis obliterans. The pathologic picture of lymphocytic interstitialpneumonitis with granuloma formation and bronchiolitis obliter-ans is characteristic of hypersensitivity pneumonitis [see Figure 3].BAL studies have examined the nature of the lymphocyte popu-lation in the lung and have demonstrated that the lymphocytesare predominantly of the suppressor-cytotoxic T cell subclass.This inversion of the ratio of helper T cells to suppressor-cytotox-ic T cells in hypersensitivity pneumonitis contrasts with the pre-dominance of helper T cells in patients with sarcoidosis. The find-ing of an intense lymphocytic alveolitis with inversion of the ratioof helper T cells to suppressor-cytotoxic T cells suggests hyper-sensitivity pneumonitis, but this pattern cannot be consideredspecific, because a similar lavage profile may be seen in other dis-orders (e.g., IPF associated with a lymphocytic alveolitis).
Clinical Manifestations
Hypersensitivity pneumonitis exists in two basic clinical forms:acute and chronic.
Acute hypersensitivity pneumonitis Acute hypersensitivitypneumonitis is characterized by fever, chills, cough, dyspnea,and malaise that typically occur 4 to 8 hours after antigenic expo-sure. Most patients with acute hypersensitivity pneumonitis im-prove spontaneously after exposure to the antigen ceases. Occa-sionally, patients experience a more severe episode characterizedby hypoxemia and by considerable respiratory distress and re-quire hospitalization. Because of the prominence of systemicsymptoms during the acute episode, the patient may be errone-ously diagnosed as having a respiratory infection. With continu-ing exposure to the inhaled antigen—as may occur in people liv-ing on a farm, for example—the patient may have daily episodesof acute hypersensitivity pneumonitis that blend into each other.If this pattern occurs, the patient may complain of having a flulikeillness for many weeks. Respiratory symptoms, such as coughand wheezing, that occur immediately after exposure to an or-ganic material should not be attributed to hypersensitivity pneu-monitis but rather to an irritant response within the airways.
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–8
b
a
Figure 3 Open-lung biopsy specimen from a patient with hypersensi-tivity pneumonitis (farmer’s lung disease) shows characteristic featuresof (a) scattered granulomas and (b) bronchiolitis obliterans.

Chronic hypersensitivity pneumonitis In chronic hyper-sensitivity pneumonitis, there are usually no systemic symptoms;rather, the symptom complex is marked by chronic dyspnea andcough on exertion. The clinical presentation is that of interstitiallung disease of uncertain etiology.
Diagnosis
There is no single diagnostic test that can be used to establish anunequivocal diagnosis of hypersensitivity pneumonitis. Therefore,one must rely on a combination of history, radiography, serologicstudy, and exclusion of other possible causes. A history of previ-ous episodes of acute hypersensitivity pneumonitis is of great diagnostic value. In taking the history, the clinician should focuson establishing whether a relevant antigenic exposure has oc-curred and, if so, try to determine whether this exposure causedtypical acute symptoms to occur several hours later. Such a histo-ry is more likely to be obtained in cases of heavy exposure (e.g., tomoldy hay or a pigeon coop) than in cases of low-level exposure(e.g., to a humidifier or a single bird). In the latter circumstance,the exposure is more or less continuous, and it is much more dif-ficult to establish a causal relation between antigenic exposureand symptoms. Patients should be questioned carefully as to theiroccupations and hobbies and whether symptoms resolve whenthey are on vacation or at other times when they are away fromthe putative source of illness. At least 50% of patients who pre-sent with the chronic form of the disease deny having a history ofan acute episode. Such acute episodes may well have occurred,but the patient may have attributed the symptoms to respiratorytract infections. The patient may spontaneously improve on hos-pitalization for evaluation of a respiratory illness, only to experi-ence a recurrence of symptoms soon after returning home. Such ahistory should always raise suspicion about hypersensitivitypneumonitis as a cause of the respiratory illness.
Chest radiography The chest radiographs of patients withacute hypersensitivity pneumonitis may vary from demonstratingno changes to demonstrating alveolar, nonlobar infiltrates. As chron-ic disease develops, a reticular, nodular, or combined infiltrateevolves, and fibrosis may become evident during continued anti-genic exposure. HRCT can be very useful in suggesting the diag-nosis and differentiating hypersensitivity pneumonitis from IPF.15
Serologic study Serologic study is useful primarily in estab-lishing that there has been exposure to a specific antigen. Nearlyall patients with farmer’s lung and pigeon breeder’s disease haveantibodies to thermophilic Actinomyces organisms and pigeon se-rum, respectively. However, these antibodies may also be presentin the serum of a significant percentage of asymptomatic persons.Hence, the presence of antibody in serum does not establish a di-agnosis of hypersensitivity pneumonitis but demonstrates thatthere has been significant exposure to the antigen.
Bronchoscopy Patients who present with subacute to chron-ic hypersensitivity pneumonitis should undergo diagnostic bron-choscopy with BAL and transbronchial biopsy. The lavage fluid inhypersensitivity pneumonitis typically shows an intense lympho-cytosis, often with more than 50% lymphocytes. As noted earlier,these are primarily suppressor-cytotoxic T cells. As time elapsessince the last exposure to antigen, BAL tends to normalize.16
Lung biopsy Transbronchial lung biopsy would be expect-ed to show a nonspecific interstitial pneumonitis in most patients
and may show evidence of granuloma or bronchiolitis obliterans.Even in the two thirds of cases in which granulomas are present,these lesions are more scattered than sarcoid granulomas and aretherefore not as likely to be demonstrated by transbronchial biop-sy. Open lung biopsy is usually reserved for especially difficultand confusing cases in which a diagnosis cannot be establishedby a combination of history, radiography, serologic study, andbronchoscopy. Few patients who have hypersensitivity pneumo-nitis require open lung biopsy for diagnosis.
Treatment
Treatment of hypersensitivity pneumonitis primarily involvesstopping the exposure to the causative antigen. This step may beaccomplished rather early in the case of humidifier lung diseaseor bird fancier’s disease but is somewhat more difficult to accom-plish in patients with farmer’s lung. Sometimes, the dairy farmeris able to have another person do the work that involves expo-sure to the moldy hay. High-efficiency masks may help reducethe number of spores the patient inhales. Improvement in farm-ing practices, including better ventilation and other steps to re-duce the moisture content of hay, may significantly lessen theantigenic load. Referral of the patient to a center that deals withagricultural lung disease is appropriate.
Glucocorticoids are used primarily for acute hypersensitivitypneumonitis characterized by severe systemic symptoms and gasexchange abnormalities. Patients with subacute to chronic hyper-sensitivity pneumonitis may also improve more rapidly if theyare given a course of glucocorticoids for several weeks. Elimina-tion of further antigen exposure is essential when glucocorticoidsare administered. Otherwise, the symptoms may be masked byuse of the glucocorticoids, and continued exposure to the antigencould result in further lung damage. When antigenic exposureceases, most patients undergo spontaneous improvement. Pa-tients who have entered a fibrotic phase of the disease may notshow substantial improvement, and there is a small subset of pa-tients who seem to deteriorate even though antigenic exposurehas apparently been eliminated. In the latter group, it may bebeneficial to follow the serum antibody level; with lack of furtherexposure, the titer will gradually fall. An unchanging or rising ti-ter would suggest continuing antigenic exposure.
malignant diffuse infiltrative lung disease
Diffuse involvement of the lung by malignancy occurs withlymphangitic carcinomatosis, alveolar cell carcinoma, lympho-ma, and leukemia.
Disease Caused by Pulmonary Lymphangitic Carcinomatosis
Pulmonary lymphangitic carcinomatosis most often resultsfrom adenocarcinomas. The adenocarcinomas usually originatein the breast, gastrointestinal tract, or lung. The symptoms refer-able to lymphangitic tumor—that is, cough and dyspnea—arethe same as those of nonmalignant diffuse infiltrative lung dis-ease. However, lymphangitic carcinomatosis generally progressesmuch faster than other interstitial lung diseases; survival beyond 3to 6 months is unusual. The chest radiograph shows bilateral retic-ular or reticulonodular infiltrates and, often, Kerley B lines. Thelatter finding should, in the absence of heart failure, raise suspi-cion that malignancy is responsible for the pulmonary disorder.Pleural effusions and hilar adenopathy may also be observed.Less often, lymphangitic carcinomatosis presents as unilateral in-volvement, or the patient has an entirely normal chest radiograph
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–9

© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–10
Radiographic Clues
BHA; upper lung field infil-trates; bronchovascular bun-dle nodularity on HRCT
Sometimes normal initially;bibasilar reticular infiltrates;peripheral fibrotic changeswith subpleural honeycomb-ing on HRCT
Bibasilar hazy opacities;ground-glass changes withsome linear and reticulo-nodular infiltrates on HRCT
Diffuse bilateral airspace opac-ities; areas of ground-glasschanges and consolidationon HRCT
Reticulonodular infiltrates
Bilateral hazy opacities; bilat-eral patchy ground-glasschanges on HRCT
Some have solitary focal infil-trates; bilateral patchy alveo-lar or ground-glass infiltrates;bilateral areas of consolida-tion on HRCT
Usually have bilateral diffuseor patchy infiltrates; onHRCT, may be ground-glass,fibrotic, or combination
Pneumothorax common,sometimes at presentation;nodules and cysts seen onchest radiograph and HRCT
Bilateral alveolar filling thatlooks like pulmonary edemawithout signs of congestion
Bilateral peripheral; often upper lung field infiltratesvery suggestive
Fluffy perihilar acinar shadows; alveolar filling on HRCT
Diffuse, thin-walled cysts on HRCT
Pulmonary Function
Restriction with de-creased Dlco; some have obstruction
Diffusion decreased morethan lung volumes
Restrictive defects less severe than in IPF
Rapidly progressive restrictive defect withhypoxemia
Restrictive defect with decreased Dlco
Restrictive defect with decreased Dlco
Mixed restriction and obstruction
Restrictive defect with decreased Dlco
Mixed restriction and obstruction with de-creased Dlco
Restrictive defect with de-creased Dlco; increasedshunt fraction
Restrictive and obstruc-tive defects
Restrictive pattern thatimproves with clinicalresolution; Dlco in-creased with bleeding
Obstruction with increased lung volumes;Dlco decreased
Associated Diseases, Exposures, Risk Factors
Familial incidence sometimes
Familial IPF, cigarette smoking, chronic aspiration,? viral infections
Highly associated with cigarette smoking
Viral prodrome
Autoimmune disorders (Sjögren syndrome), dys-proteinemias, viral infec-tions (HIV), bone marrowtransplantation
Collagen vascular disorders,exposures to agents knownto cause hypersensitivitypneumonitis, other environ-mental exposures, drugs
Many idiopathic but some associated with infections,collagen vascular disorders,aspiration, transplantation,inhaled toxins
Rheumatoid arthritis, SLE,PSS, Sjögren syndrome,MCTD, PM/DM
Cigarette smoking
Most cases idiopathic; associ-ated with acute silica expo-sure, several hematologicmalignancies, busulfan
None
Cigarette smoking, hydro-carbon exposure
Tuberous sclerosis producesidentical radiographic picture
Clinical and Laboratory Clues
Young African-American, fe-males; minimal symptoms;skin lesions; increasedSACE activity
Older men; slowly progres-sive dyspnea; dry end-in-spiratory rales; clubbing of digits
Middle-aged men; slowlyprogressive dyspnea; clubbing of digits
Rapid onset of dyspnea,cough, fever evolving torespiratory failure
Older women more thanmen; associated disordermay dominate clinical picture
Middle-aged; women slightlygreater than men; dyspneaand cough; often with fever
Idiopathic BOOP seen in old-er patients; abrupt onset ofcough, dyspnea, fever; ralesand wheezes
Often asymptomatic; pro-gressive dyspnea, cough,sometimes with chest pain,hemoptysis; positiveserologies
Age 20–50 years; sometimesasymptomatic; cough anddyspnea
Abnormal radiograph, acutecomplicating infection, orprogressive cough and dys-pnea; increased LDH
Middle-aged women; pro-ductive cough, dyspnea, fe-ver, wheezing; eosinophilia
Young male cigarette smok-ers; most have hemoptysis;drop in hemoglobin, hema-turia, iron deficiency; posi-tive anti-GBM antibody
Women in childbearingyears; dyspnea, hemop-tysis, pneumothorax, chylothorax
Entity
Sarcoidosis
Idiopathic pulmonaryfibrosis (IPF)
Desquamative intersti-tial pneumonia/res-piratory bronchiolitisinterstitial lung dis-ease (DIP/RBILD)
Acute interstitial pneumonia (AIP)
Lymphocytic interstitial pneumonia (LIP)
Nonspecific interstitialpneumonia and fibrosis (NSIP/F)
Bronchiolitis obliter-ans organizingpneumonia (BOOP)
Collagen vascular disease
Eosinophilic granuloma
Alveolar proteinosis
Chronic eosinophilicpneumonia (CEP)
Anti–glomerular base-ment membrane (anti-GBM)
Lymphangio-myomatosis
Table 5 Chronic Diffuse Parenchymal Lung Diseases of Unknown Cause*
*After ruling out infections, drugs, and inhalants (organic and inorganic).ARDS—acute respiratory distress syndrome BHA—bilateral hilar adenopathy DAD—diffuse alveolar damage Dlco—diffusing capacity of the lung for carbon monoxideHRCT—high-resolution computed tomography LDH—lactate dehydrogenase LIP—lymphocytic infiltrative pneumonia MCTD—mixed connective tissue disease PM/DM—polymyositis/dermatomyositis PSS—progressive systemic sclerosis SACE—serum angiotensin-converting enzyme SLE—systemic lupus erythematosusUIP—usual interstitial pneumonia

despite severe dyspnea and hypoxemia. In patients with lym-phangitic carcinomatosis and a normal chest radiograph, tumorcells are often found in abundance in small pulmonary vessels, oc-casionally resulting in severe pulmonary hypertension (tumor em-
bolism syndrome). Diagnosis is generally made by bronchoscopy,either by BAL alone or by transbronchial biopsy. An alternativemeans of establishing the diagnosis is by microvascular cytologicexamination of blood aspirated through a wedged pulmonary
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–11
Therapy
For many—none; when indicated,steroids, antimalarials, methotrexate
A minority respond to steroids; cyto-toxic therapy with cyclophosphamide,azathioprine; in unresponsive patients,colchicine
Good response to discontinuance of smoking; good response to steroids
Supportive care with oxygen, mechanicalventilation; not clear whether steroidsof any benefit
Treatment of underlying disorder; some respond to steroids, others require immunosuppressive agents
Good response to steroids
Focal infiltrates do not require therapy; for others, steroids are successful withhigh incidence of relapse
In some, steroids useful (PM/DM, Sjögren syndrome); in others, cyto-toxic therapy indicated
Smoking cessation; steroids not clearly of benefit
Some patients require no therapy; wholelung lavage is treatment of choice
Steroids are effective, producing rapidresponse; relapse common
Immunosuppressive agents, glucocorti-coids, plasmapheresis
Oophorectomy, progesterone treatment,or a combination of the two; lungtransplantation for end-stage disease
Prognosis
Excellent
Complete recovery not possible; mortality 68%; median survival 2–3 yr
Complete recovery possible;mortality 27%; mean sur-vival 12 yr
Mortality 78%; survival oftenless than 6 mo
Depends on underlying disor-der; can be progressive
Complete recovery possible;median survival 13.5 yr; sur-vival worse with increasedfibrosis
Patients with focal BOOP haveno increased mortality; thosewith diffuse disease have agood prognosis with steroids
Depends on the associatedprocess, response to therapy
Median survival 6 yr; olderage, airflow obstruction, hyperinflation—poor prognosis
Some patients will undergospontaneous remission; excellent response to wholelung lavage
Spontaneous remissions in10%; many require long-term steroids; with steroids,death uncommon from CEP
50% mortality; dialysis neededafter 2 yr
25% mortality at 8 yr
Histopathology
Noncaseous granulomas; must excludegranulomatous infection, berylliosis
UIP; fibrosis with widening of the alveolarsepta; fibroblastic foci of varying age;minimal inflammation
Homogeneous filling of air spaces, especially in the peribronchiolar areas
Diffuse alveolar damage; cannot be differ-entiated from ARDS pathologically
Lymphocytic infiltrate of alveolar wallsand alveoli that must be distinguishedfrom lymphoma
Often confused with UIP; temporally uni-form mixture of alveolar wall inflamma-tion (mostly lymphocytes and plasmacells and fibrosis)
Intraluminal plugs of connective tissue in the bronchioles, alveolar ducts, andalveolar spaces
Some have UIP pattern, but NSIP/F, LIP,BOOP, DAD also seen
Nodular lesions containing Langerhanscells with Birbeck granules
Granular, eosinophilic material withinalveolar spaces that stains positively with the periodic acid–Schiff staining
Massive, mixed interstitial and alveolar inflammatory infiltrates that have a higheosinophil content
Alveolar hemorrhage, sometimes with linear immunofluorescent staining; kid-ney biopsy shows crescentic glomerulo-nephritis and linear immunofluorescentstaining
Diffuse proliferation of smooth musclecells in the lung and visceral pleura, with cyst formation
Extrathoracic Manifestations
Neurologic, eye, skin, heart,liver, hypercalcemia, joints
Arthralgias; cor pulmonalelate in disease
None
None
Depends on associated disorder
None
Depends on associated disorder
Arthritis, skin rash or thick-ening, dysphagia, serositis,dry eyes/mouth, myositis,pulmonary hypertension
Bone lesions, diabetes insipidus
None
None
Glomerulonephritis
Renal angiomyolipomas
Table 5 Chronic Diffuse Parenchymal Lung Diseases of Unknown Cause (continued)

arterial catheter. This technique may be considered in the verybreathless patient in whom right heart catheterization may bebetter tolerated than bronchoscopy. Open lung biopsy is only oc-casionally required to diagnose lymphangitic carcinomatosis.
Disease Caused by Alveolar Cell Carcinoma
Alveolar cell carcinoma may present as a simple nodule ormass, as multiple nodules, or with air-space disease that can befocal, multifocal, or quite diffuse.17 When the tumor presents asdiffuse disease, the differential diagnosis includes nonmalignantcauses of diffuse alveolar filling, such as pulmonary edema, alve-olar proteinosis, alveolar sarcoidosis, and alveolar hemorrhage.Diagnosis of alveolar cell carcinoma is usually established fairlyeasily by bronchoscopy with BAL and transbronchial biopsy.
Disease Caused by Lymphoma or Leukemia
Lymphoma and leukemia may cause diffuse infiltrative lungdisease. Lymphomatous involvement of the lung parenchyma isusually seen in association with mediastinal lymphadenopathyand evidence of extrathoracic lymphoma.18 On occasion, isolatedpulmonary disease is the presenting manifestation of lymphoma.When the underlying leukemia is poorly controlled, leukemic in-filtration of the lung is usually seen and may contribute to deathby causing respiratory failure. Diagnosis of leukemic or lym-phomatous infiltration of the lung may require open lung biopsyto adequately characterize the nature of the infiltrating processand to completely exclude infection. However, in some cases,bronchoscopy may suffice for making the diagnosis.
Chronic Diffuse Infiltrative Lung Disease of Unknown Etiology
An overview of diagnosis and treatment for chronic diffuseinfiltrative lung disease of unknown etiology is presented [seeTable 5].
sarcoidosis
Sarcoidosis is a multisystem disease of unknown etiology thatis characterized pathologically by the presence of noncaseatinggranulomas in various tissues.19 Any organ system may be affect-ed. Most patients are asymptomatic and seek medical attentionbecause of unrelated respiratory symptoms; most of those pa-tients who are asymptomatic are first recognized through a chestradiograph abnormality. Fewer than 5% of patients with sarcoi-dosis have a normal chest radiograph. Further, the morbidity andmortality that are associated with sarcoidosis result most oftenfrom pulmonary involvement. Thus, it is appropriate to think ofsarcoidosis as primarily a respiratory tract disorder that may alsohave features of extrapulmonary disease.
Many infectious and noninfectious conditions are associatedwith granuloma formation and a histopathologic picture indistin-guishable from that of sarcoidosis. Thus, diagnosis of sarcoidosisrequires the exclusion of other causes of granuloma formation.Berylliosis and histoplasmosis, for example, can have clinicopath-ologic features identical to those of sarcoidosis [see Approach tothe Patient with Suspected Chronic Diffuse Infiltrative Lung Dis-ease, above].
Epidemiology
Sarcoidosis occurs worldwide, in all ethnic groups, but thereare striking regional and ethnic differences in its incidence andprevalence. For example, in the United States, sarcoidosis is 10
times more common in blacks than in whites and tends to be moresevere in black patients. However, this increased prevalence is notobserved in blacks in Europe. It has been estimated that theprevalence of sarcoidosis in the United States is between one in10,000 and one in 2,500. Persons 20 to 40 years of age are most of-ten affected, but the disease can present in children and the elder-ly. Males and females are affected almost equally, with the preva-lence of sarcoidosis being only slightly higher in females. Familialsarcoidosis has been reported in a number of kindreds; less com-monly, sarcoidosis has been diagnosed in both a husband and awife, which would suggest a common environmental factor.
Pathogenesis
A specific sequence of events leads to granuloma formation in sarcoidosis20 [see Figure 4]. Expansion of the helper T cell pop-ulation in the lungs likely occurs through the activation of T cellsby macrophages via interleuken-1 (IL-1) and the subsequent re-lease of IL-2 (also termed T cell growth factor) by the helper Tcell. IL-2 causes self-replication of the existing T cell population.This population of helper T cells (dominantly of the Th1-type),which are greatly increased in number and in degree of activi-ty, recruits monocytes from peripheral blood into the lung by re-leasing monocyte chemotactic factor and colony-stimulating fac-tors and thereby participates in the formation of granulomas. Themonocytes become tissue macrophages and, ultimately, the epi-thelioid cells and multinucleated giant cells that form the core of the granuloma. Monocyte- and macrophage-derived fibroblastgrowth factors may, in some patients, lead to the development offibrosis. Another effect of the expanded and activated helper Tcell population at sites of disease activity is local stimulation of Bcells to produce immunoglobulin, which accounts for the hyper-gammaglobulinemia that is often seen in this disorder.
Clinical Manifestations of Intrathoracic Sarcoidosis
The most common manifestations of intrathoracic sarcoidosisare bilateral hilar lymphadenopathy and diffuse infiltrative lungdisease. A staging system has been created on the basis of thepresence or absence of these two manifestations on radiography:stage I, bilateral hilar lymphadenopathy alone; stage II, bilateralhilar lymphadenopathy and diffuse infiltrative lung disease; andstage III, diffuse infiltrative lung disease alone [see Figure 5].
Symptoms resulting from parenchymal lung involvement in-clude dyspnea and cough. Pulmonary function abnormalities arefound in nearly all symptomatic patients and in some patientswho are asymptomatic. Physiologic abnormalities in patients withsymptomatic sarcoidosis typically consist of a reduction in Dlcoand vital capacity without airflow obstruction. The Dlco typical-ly becomes abnormal before the vital capacity, but both are usual-ly affected in persons with moderate to severe symptoms. Air-flow obstruction is relatively uncommon except in patients withadvanced disease or with endobronchial involvement of largerairways. In rare instances, diffuse endobronchial granulomas insmall airways lead to a predominantly obstructive abnormalityin patients who present with stage I disease.
Most patients with stage I sarcoidosis are asymptomatic, andthe abnormality is detected on a routine chest radiograph. Whenstage I disease is symptomatic, the symptoms are nonpulmonaryin nature and consist of systemic complaints of fever, malaise,arthralgia, or erythema nodosum. The presence of fever, bilateralhilar lymphadenopathy, arthralgia or arthritis, and erythema no-dosum is known as Löfgren syndrome.21 Approximately 10% ofpatients who have stage I disease display evidence of extrapul-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–12

monary organ involvement (e.g., involvement of the eyes, ner-vous system, or lacrimal glands). Approximately 75% of patientswho have stage I sarcoidosis will undergo spontaneous remis-sion within 2 years after presentation. Erythema nodosum at ini-tial presentation increases the likelihood of spontaneous remis-sion. Those patients in whom bilateral hilar lymphadenopathyfails to remit within 2 years may remain stable, may undergospontaneous remission at a later time, or may develop progres-sive pulmonary disease. No more than 10% to 15% of patients de-velop progressive pulmonary disease.
The frequency of symptoms is higher in patients with stage IIsarcoidosis, but asymptomatic cases are not unusual. Symptomsmay be primarily systemic, as in stage I disease, or may arise frompulmonary involvement. A presentation of extensive radiograph-ic abnormalities associated with only minimal respiratory symp-toms is not uncommon. Roughly 50% of patients with stage IIsarcoidosis will be in remission 2 years after presentation. Stage IIdisease is more likely to be progressive and to follow a chronicsymptomatic course than stage I disease.
Stage III disease is found at presentation in 5% to 15% of pa-tients. Respiratory symptoms are common, but as in stage II dis-ease, the chest radiograph may make the patient appear muchworse than is actually the case. Only one third of patients withstage III sarcoidosis will be in remission 2 years after presentation.The disease commonly takes a chronic course that eventuallyleads to lung fibrosis. Certain extrapulmonary manifestations ofchronic sarcoidosis, such as infiltrative skin disease, occur much
more often in patients with stage III disease than in patients withstage I or stage II disease. This chronic course of stage III disease isnot surprising, because patients who are diagnosed at this point inthe disease process may represent those persons who earlier hadbilateral hilar lymphadenopathy (stages I and II) and failed to un-dergo spontaneous remission.
Unusual manifestations of intrathoracic sarcoidosis includepleural effusion, alveolar infiltrates, large nodular opacities, cavi-tation, atelectasis, and calcification. Pleural involvement occurs in1% to 4% of patients and consists of pleural effusion or thickeningof the visceral and parietal pleurae. Effusions are rarely large, andthey typically contain a high percentage of lymphocytes. Pleuralbiopsy reveals granulomas, and the major differential diagnosis toconsider in patients with pleural sarcoidosis is tuberculosis. Alve-olar sarcoidosis has variable presentations, ranging from patchyinfiltrates in asymptomatic patients to rather extensive air-spaceconsolidation in patients with respiratory failure. Nodules of 2 to10 cm in diameter occur and rarely cavitate. The differential diag-nosis of nodular sarcoidosis includes fungal infection, tubercu-lous infection, and, especially, metastatic tumor. Atelectasis can becaused by endobronchial sarcoidosis. Calcification in lymph nodes isa late manifestation of disease and is seen in 5% of patients.
Necrotizing sarcoid granulomatosis, characterized by massesof confluent granulomas with some degree of vasculitis, is proba-bly a variant of sarcoidosis. The two disorders have many fea-tures in common, including hilar lymphadenopathy and extra-pulmonary granulomatous inflammation.
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–13
AntigenMacrophage
Antigen T CellActivation
IL-1
Fibroblast Growth Factors(IGF-1, PDGF, TGF-β, IL-3,IFN-γ, TNF-α)
Fibrin,Fibronectin
Fibrosis
T Cell ProliferationRecruitment of
Monocytes
MonocyteChemotactic Factor and
Colony-Stimulating Factors
B Cell Helper Factors (IL-6, IL-4)
PolyclonalB Cell ActivationFibroblast
ImmunoglobulinSecretion
IL-2
T Cell
GranulomaFormation
TNF-α IL-1
Figure 4 A current theory of the pathogenesis of sarcoidosisholds that the disease is caused by a lack of modulation of the im-mune response after antigen recognition occurs. [For description,see Chronic Diffuse Infiltrative Lung Disease of Unknown Etiolo-gy, Pathogenesis, in text.] (IFN-γ—interferon gamma; IGF-1—insulinlike growth factor–1; IL—interleukin; PDGF—platelet-derived growth factor; TGF-β—transforming growth factor–β;TNF-α—tumor necrosis factor–α).

Clinical Manifestations of Extrathoracic Sarcoidosis
Although extrathoracic sarcoidosis is a much less commoncause of morbidity than intrathoracic disease, it can dominate theclinical picture in some patients.
Erythema nodosum, a nongranulomatous panniculitis, is themost common cutaneous manifestation of sarcoidosis. More than90% of patients with sarcoidosis who develop erythema nodosumhave a stage I radiograph; the other 10% have stage II radio-graphs. Granulomatous skin lesions occur in 10% to 30% of pa-tients and are especially common in African Americans. Lupuspernio is a bluish-purple swollen lesion on the nose, cheeks, ear-lobes, fingers and toes, lips, or knees that may become disfiguring.Skin plaques tend to be violaceous, angular, and flat with a raisededge. Psoriasislike plaques may also be seen. Nodules may be ele-vated or may arise in the subcutaneous tissue. As a rule, thesegranulomatous skin manifestations of sarcoidosis are seen withchronic and persistent stage III pulmonary disease.
Ocular involvement occurs in about 25% of patients with sar-coidosis. The uveal tract is most often affected; sarcoidosis is re-sponsible for 2% to 4% of all cases of uveitis. Anterior uveal tractdisease with iridocyclitis usually presents as tearing and photo-phobia with little or no pain. Heerfordt syndrome, or uveoparotidfever, is an uncommon manifestation of sarcoidosis that consistsof uveitis, parotid enlargement, cranial nerve palsies, subacutemeningitis, and systemic symptoms. Posterior uveitis (chorioret-initis) causes blurring of vision, or patients may be asymptomat-ic. Chorioretinitis may be difficult to detect when anterior uveitisis present.
The nervous system is affected in fewer than 5% of patientswith sarcoidosis. Central nervous system manifestations includechronic meningitis, encephalopathy, hypothalamic lesions, cranialnerve involvement, and seizures. Peripheral sensory and motorneuropathy may be seen. Chronic meningitis in sarcoidosis maybe difficult to distinguish from tuberculous or fungal meningitisand is typically associated with cerebrospinal fluid lymphocytosis,increased CSF protein levels, and, sometimes, low CSF glucoselevels. Sarcoidosis can give rise to space-occupying lesions in vari-ous locations, resulting in diverse neurologic abnormalities.
Evidence of cardiac sarcoidosis is seen much more often at au-topsy than would be suspected on the basis of clinical manifesta-tions. Rhythm disturbances are the most common manifestations
of cardiac sarcoidosis. Both ventricular tachyarrhythmias andcomplete heart block can occur and can lead to sudden death.Other, less common features of cardiac sarcoidosis include heartfailure, pericardial disease, papillary muscle dysfunction, and ven-tricular aneurysm in the absence of coronary artery disease. Echo-cardiography, Holter monitoring, and thallium-201 scanning mayshow abnormalities but do not necessarily indicate that granulo-mas are in the myocardium. Age, comorbidities, and the types ofabnormalities must be taken into account to assess the probabili-ty of myocardial sarcoidosis.
Bone or joint involvement is observed in 1% to 10% of patients.Bone disease is characterized by cystic lesions and tends to be re-stricted to the fingers and toes. Swollen digits may be seen. Syn-ovial sarcoidosis can present as monoarticular or polyarticularchronic arthritis.
Patients with sarcoidosis often have liver and spleen granulo-mas, but liver dysfunction or massive splenomegaly is unusual. Inrare cases, sarcoidosis leads to cirrhosis and portal hypertension.Upper respiratory tract involvement is usually manifested by na-sal or laryngeal symptoms. Epistaxis and nasal congestion, whichmay be mistaken for allergic or vasomotor rhinitis, are commonsymptoms. Sarcoidosis should be considered when nasal obstruc-tion is refractory to conventional therapy. Laryngeal sarcoidosisinvolves the supraglottic structures and, on occasion, the vocalcords. Hoarseness is the most common symptom, but upper air-way obstruction can occur.
Endocrine abnormalities in sarcoidosis include hypercalcemiaand pituitary dysfunction, which may present as diabetes insip-idus. Hypercalcemia is seen much less often than hypercalciuria.Hypercalcemia and hypercalciuria in sarcoidosis are caused bythe unregulated, increased synthesis of 1,25-dihydroxyvitamin Dby activated macrophages in the granulomas, resulting in an in-crease in calcium absorption in the gut.
Diagnosis
The diagnosis of sarcoidosis is established by demonstration ofnoncaseating granulomas in tissue [see Figure 6] and exclusion ofother causes of granulomas. Intrathoracic sarcoidosis is diagnosedmost easily by bronchoscopy with transbronchial lung biopsy.The yield of transbronchial lung biopsy depends on the radio-graphic stage. In patients with pulmonary infiltrates (stages II and
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–14
a b c
Figure 5 (a) In stage I sarcoidosis, the chest radiograph reveals bilateral hilar and right paratracheal adenopathy with normal lung paren-chyma. (b) In stage II sarcoidosis, adenopathy and parenchymal infiltration are apparent on the radiograph. (c) Stage III sarcoidosis is char-acterized by parenchymal infiltration, without definite adenopathy.

III), transbronchial lung biopsy demonstrates noncaseating gran-ulomas in approximately 90% of cases. In stage I disease, the yieldis 60% to 70%. If a diagnosis is not established by transbronchiallung biopsy, mediastinoscopy is indicated and will provide a di-agnosis in over 95% of cases. Biopsy of extrapulmonary tissuescan be used for diagnosis when clinically indicated (e.g., in pa-tients with peripheral lymph node enlargement or skin lesions).
When noncaseating granulomas are found in tissue, possiblecauses of granuloma formation other than sarcoidosis must al-ways be excluded. Occasionally, lymphoma or carcinoma is asso-ciated with granulomatous inflammation in local lymph nodes. In-fectious causes of granulomas in the lungs and mediastinal lymphnodes, particularly tuberculosis and histoplasmosis, should beruled out. A tuberculin skin test, fungal serologic studies, and theuse of special stains on tissue biopsy specimens are necessary. Forexample, such findings as hilar lymphadenopathy, pulmonaryinfiltrates, and noncaseating granulomas in tissue may promptthe physician to make a presumptive diagnosis of sarcoidosiswhile these special studies are pending. If a high complement fix-ation titer for histoplasmosis were detected, the diagnosis wouldbe changed to histoplasmosis.
At the time of bronchoscopy, BAL is usually performed in ad-dition to biopsy. In active sarcoidosis, the lavage fluid usuallyshows increased numbers of lymphocytes, and the ratio of helperT cells to suppressor-cytotoxic T cells is elevated. Because otherpulmonary disorders, both infectious and noninfectious, may beassociated with lymphocytosis, this finding lacks diagnostic speci-ficity. Hypersensitivity pneumonitis may be confused with sar-coidosis because both disorders are associated with lavage fluidlymphocytosis and noncaseating granulomas in tissue. However,an inverted ratio of helper T cells to suppressor-cytotoxic T cells istypically seen in hypersensitivity pneumonitis. Levels of ACE areusually elevated in active sarcoidosis. Therefore, the measurementof ACE levels may aid in the diagnosis of sarcoidosis. However, itis not clear whether this test has much diagnostic value beyondsatisfying essential pathologic criteria. Diagnosis of sarcoidosis onthe basis of an elevated ACE level alone, without confirmation ofthe diagnosis by demonstration of noncaseating granulomas intissue, is not recommended. Elevated ACE levels have also beendetected in miliary tuberculosis, leprosy, biliary cirrhosis, silicosis,and asbestosis. With the exception of miliary tuberculosis, it is not
likely that these diseases would be clinically confused with sarcoi-dosis. When the ACE level is elevated, repeated ACE measure-ments during treatment of sarcoidosis may be helpful because theACE level often correlates with disease activity.
Differential Diagnosis
The differential diagnosis of stage I sarcoidosis primarily in-cludes lymphoma and granulomatous infections such as tuber-culosis and histoplasmosis. More infrequent causes of bilateral hi-lar lymphadenopathy include metastatic carcinoma (especiallyrenal cell carcinoma) and amyloidosis. Most patients who havelymphoma that manifests as bilateral hilar lymphadenopathyhave peripheral lymphadenopathy, splenomegaly, or systemicsymptoms such as fever, weight loss, and night sweats. Youngadults who present with asymptomatic bilateral hilar adenopa-thy but neither peripheral lymphadenopathy nor splenomegalyare very unlikely to have lymphoma. It is therefore reasonable tomake a presumptive diagnosis of stage I sarcoidosis in such pa-tients without confirming the diagnosis by examination of a tis-sue specimen. However, a tuberculin skin test and fungal sero-logic studies should be performed, and clinical and radiographicfollow-up is required to ensure that there is no evidence of pro-gression of the disease. If disease progression is observed, it is im-perative to perform a tissue biopsy to establish the diagnosis.
Treatment
Glucocorticoids are standard therapy for symptomatic sarcoi-dosis, though there is no definitive proof that they influence long-term outcome. Most patients respond very well to therapy, andoften, low dosages of prednisone (e.g., 15 mg every other day)may be effective in suppressing disease activity. A higher dosage(e.g., 40 to 60 mg/day) is usually given for a few weeks to induceregression of disease activity. The primary indication for gluco-corticoids is symptomatic pulmonary involvement. Other indica-tions include significant systemic symptoms (e.g., fever or weightloss), hypercalcemia, and involvement of extrapulmonary tissuesthat leads to established functional impairment or a risk of organdysfunction. The required duration of therapy is uncertain. It iscommon practice to treat pulmonary sarcoidosis with prednisonefor 1 year, then to withdraw the drug to see whether the disease isin remission. Relapses of the disease are treated in a similar fash-ion, with higher initial dosages of prednisone that are tapered to alow dosage for maintenance. Some patients relapse repeatedly asprednisone is withdrawn and require low-dose suppressive ther-apy indefinitely.
If the use of steroids is strictly contraindicated or if the patientdoes not respond to steroid therapy, methotrexate22 or chloram-bucil may be tried. Chloroquine is often useful in patients withskin disease.
Lung transplantation in sarcoidosis has been associated withhistologic evidence of recurrence in the transplanted lung, but thesurvival of these patients has been comparable to the survival ofpatients undergoing lung transplantation for other indications.23
idiopathic pulmonary fibrosis
IPF, also known as fibrosing alveolitis, is one of the mostcommon causes of chronic diffuse infiltrative lung disease.24 Al-though this disorder has characteristic clinical, radiographic,physiologic, and histopathologic features, none of these featuresis pathognomonic. Therefore, a diagnosis of IPF requires notonly a compatible clinicopathologic picture but also the exclu-sion of all other causes of diffuse disease. For example, the pul-
© 2001 WebMD Inc. All rights reserved.June2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–15
Figure 6 Noncaseating granulomas can be seen in this tissue biopsyspecimen from a patient with sarcoidosis.

monary manifestations of IPF may be indistinguishable fromdiffuse disease associated with collagen vascular disorders; as-bestosis; chemotherapy-induced lung fibrosis and several close-ly associated disorders; bronchiolitis obliterans organizingpneumonia (BOOP); lymphocytic interstitial pneumonia (LIP);desquamative interstitial pneumonia/respiratory bronchiolitisinterstitial lung disease (DIP/RBILD); acute interstitial pneumo-nia (AIP); and nonspecific interstitial pneumonia/ fibrosis(NSIP/F).24
Pathogenesis
The pathogenesis of IPF is not well understood. A viral trig-ger has been suspected of playing a role in certain instances be-cause a substantial minority of patients date the onset of theirrespiratory symptoms to a flulike illness. Cigarette smoking,chronic aspiration, exposure to various environmental factors,and use of antidepressant drugs have been suggested as riskfactors.24 A genetic susceptibility may also be important. It maybe that IPF results when a genetically susceptible person is ex-posed to a viral or environmental agent that triggers a set ofevents leading to a cascade of inflammatory, immune, and fi-brotic processes in the lung.
The alveolitis of early IPF is characterized by an increase in thenumber of activated neutrophils and the presence of activatedmacrophages in the BAL specimen. Neutrophils may be attractedto the lung by an imbalance between macrophage-derived chemo-attractant substances (e.g., tumor necrosis factor–α [TNF-α] andIL-8) and anti-inflammatory substances (e.g., interferon gammaand IL-10).25 In some cases, the chemoattractants will be releasedin response to local immune complexes. Immune complexeshave been detected in lung tissue, lavage liquid, and blood of pa-tients with high-intensity neutrophilic alveolitis. Once in the lung,the neutrophils may cause local tissue injury by releasing variouspotentially toxic substances, such as oxygen radicals and proteo-lytic enzymes. Lung inflammation may eventually be followedby extensive fibrosis. It is possible that the chronic neutrophilic in-flammation of IPF plays a role in the development of lung fibro-sis. However, the fibrogenic process probably results in large partfrom the activity of lung macrophages. Macrophages from pa-tients with IPF spontaneously release growth factors for fibro-blasts, such as transforming growth factor–β, causing an increasein fibroblasts in the lung.3 The macrophages in this disease alsorelease fibronectin, a substance that promotes binding and migra-tion of fibroblasts. These macrophages spontaneously release fi-broblast stimulatory factors, such as IL-1β and TNF-α, that causefibroblasts to secrete increased amounts of the constituents of theextracellular matrix. Thus, alveolar macrophages appear to play acritical role in the development of IPF.
Clinical Manifestations
As with other types of diffuse infiltrative lung disease, dyspneaon exertion and cough are the most prominent symptoms. Physi-cal examination typically reveals fine dry inspiratory rales. Cyano-sis may be noted when hypoxemia is severe, and features of corpulmonale (e.g., elevated jugular venous pressure, edema, and aprominent pulmonic second heart sound) indicate advanced dis-ease. Clubbing of the digits is noted in 25% to 50% of cases but isoften absent early in the course of the disease. There are no otherextrathoracic manifestations of disease. Clinical evidence of extra-pulmonary disease (e.g., arthritis, skin disease, or serositis) sug-gests a systemic disorder, such as sarcoidosis or one of the colla-gen vascular diseases, rather than IPF.
Diagnosis
A diagnosis of IPF is established by correlating histopatho-logic and clinical findings. Clinically, IPF is suspected when adiffuse infiltrative lung disease occurs with no involvement ofother organ systems and there is no apparent relation to infec-tion, environmental exposure, or drugs. The chest radiographshows no evidence of hilar adenopathy or pleural effusion. Lab-oratory tests in IPF are generally unrevealing, except for thepresence of a positive antinuclear antibody or positive rheuma-toid factor in up to 50% of cases. Thus, serum antinuclear anti-body and rheumatoid factor cannot be relied on to differentiateIPF from diffuse infiltrative lung disease associated with colla-gen vascular disorders.
The initial approach to diagnosing IPF is to exclude as manycauses of diffuse infiltrative lung disease as possible by a combi-nation of history and clinical examination. However, a number ofcauses remain that cannot be reliably identified without a lung bi-opsy. Such causes include stage III sarcoidosis, lymphangitic car-cinomatosis, lymphangioleiomyomatosis, eosinophilic granulo-ma, DIP/RBILD, NSIP/F, LIP, AIP, and the more diffuse forms of BOOP.
Imaging studies The radiographic features are nonspecificand most often consist of a bilateral reticular or reticulonodularpattern that typically appears in the lower lung fields; if cor pul-monale develops, enlargement of the pulmonary arteries andheart occurs. In as many as 10% of patients with symptomaticIPF, the chest radiograph may be entirely normal. Radiographicfindings in patients with IPF are limited to the lung fields. Hilarlymphadenopathy or pleural effusion suggests a different causeof diffuse infiltrative lung disease.
HRCT may be helpful at this stage of the evaluation becausethe pattern of abnormalities seen in IPF is specific, and many ofthese other causes have characteristic and very different patterns.26
Also, it is likely that HRCT would reveal abnormalities in cases inwhich the chest radiograph is normal.
The HRCT pattern in IPF includes patchy, peripheral, sub-pleural, bibasal reticular abnormalities with minimal ground-glass opacity. With advanced disease, honeycomb lung and trac-tion bronchiectasis/bronchiolectasis, indicating end-stage lungfibrosis, are seen. Extensive areas of ground-glass haziness, indi-cating an acinar filling process, are not characteristic of IPF andmay be seen in AIP, LIP, DIP/RBILD, and NSIP/F.
Pulmonary function testing The physiologic abnormalitiesof IPF are basically the same as those described for diffuse infil-trative lung disease. The classic composite physiologic picture ofIPF is reduced Dlco, restriction of lung volume, exercise-inducedoxygen desaturation, and absence of airflow obstruction. Some ofthe alterations correlate with the pathologic findings.27
Histopathologic features The histopathologic features ofIPF are nonspecific. Similar histopathologic findings are observedin diffuse infiltrative lung disease associated with collagen vascu-lar disease, various types of drug-induced diffuse disease, andother disorders. Chronic fibrosis and a scant inflammatory cell in-filtrate, the essential pathologic features of IPF, are common reac-tions to a variety of agents.
The histopathologic picture in IPF is termed usual interstitialpneumonitis (UIP) and is characterized by minimal interstitial in-flammatory round cell infiltrate, widening of alveolar septa, andfibrosis with fibroblastic foci28 [see Figure 7]. The distribution of the
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–16

lesion is irregular: areas of intense fibrosis can coexist with areasof near-normal lung in the same open lung biopsy specimen.
UIP must be differentiated from DIP/RBILD, AIP, LIP, NSIP/F,and BOOP, because of different prognoses29 and treatment ap-proaches (see below).
Lung biopsy Transbronchial lung biopsy is a sensitive toolfor diagnosing sarcoidosis and lymphangitic cancer and may re-veal pathologic features suggestive of IPF (i.e., fibrosis and wid-ened alveolar septa with scant inflammatory cell infiltrate). Openlung biopsy is needed to exclude other causes of diffuse disease.It is up to the clinician to decide whether to proceed to open lungbiopsy when clinical evaluation and transbronchial lung biopsyare highly suggestive of IPF. Open lung biopsy is advisable whenthere is any doubt about whether there is an infectious cause.Open lung biopsy should usually be performed in younger pa-tients to establish the diagnosis of the underlying disorder with areasonable degree of certainty.5 Older patients with typical clini-cal features and a compatible transbronchial lung biopsy resultmay be reasonably spared the morbidity associated with openlung biopsy. In certain cases, it may be reasonable to diagnose IPFwithout any tissue biopsy. For example, a tissue biopsy may notbe needed to diagnose IPF in an elderly patient who has had pro-gressive dyspnea on exertion for many months to years and whohas fine, end-inspiratory crackles and clubbing of the digits on ex-amination, bilateral coarse interstitial infiltrates, low-titer serumantinuclear antibody, and no evidence of an environmental or adrug-related disorder.
Prognosis and Treatment
The median survival for patients with newly diagnosed IPF is 2 to 3 years.30 Most deaths result from progressive pulmonaryimpairment.
Prednisone is used to treat progressive disease, and about 20%to 30% of patients receiving prednisone show symptomatic, radio-graphic, and functional improvement.24 However, even those whorespond usually do not show dramatic improvement, unlike pa-tients with symptomatic sarcoidosis who are treated with gluco-corticoids. The response to prednisone is better if fibrosis is lessprominent than inflammation on open lung biopsy; response istypically poorer if fibrosis predominates.31 However, because lunginvolvement is heterogeneous, the histopathologic features mayvary in different regions of the lungs. Thus, open lung biopsy isnot indicated for the purpose of deciding whether to treat symp-tomatic patients with glucocorticoids. Studies of the relation be-tween HRCT results and improvement in pulmonary functionsuggest that the extent of the ground-glass pattern of attenuationcorrelates with responsiveness to glucocorticoids.31 One of the bestpredictors of long-term outcome is a short-term (6 to 12 weeks) re-sponse to prednisone, with responders having a better prognosis.31
Cyclophosphamide or azathioprine has also been used in con-junction with prednisone, usually when prednisone alone hasproved to be unsuccessful.24 Predictors of a beneficial response tocytotoxic therapy include short duration of symptoms and agood transient response to glucocorticoid therapy.32 Occasionally,patients who fail to respond to prednisone therapy show improve-ment with combined immunosuppressive therapy or with col-chicine.33 Single-lung transplantation has also been used success-fully for end-stage lung fibrosis.34
Several new, innovative therapies for IPF are being assessed.35
In a recently published randomized controlled trial, a combina-tion of interferon gamma-1b and low-dose prednisolone given to
IPF patients unresponsive to steroids or other immunosuppres-sive agents led to greater improvement in lung function over 12months than was seen with prednisolone alone.36
desquamative interstitial pneumonia/respiratorybronchiolitis interstitial lung disease
Patients with DIP/RBILD present with cough and dyspnea ofinsidious onset.28 Clubbing of digits is present in about 50% ofcases. The average age at onset of symptoms is the early to mid-dle 40s, which is significantly younger than the age at onset of IPFsymptoms. Men are affected twice as often as women. Almost allof these patients are cigarette smokers, and many investigatorsfeel that the disease is caused by tobacco use.
The chest radiograph typically shows vague, bibasilar opaci-ties that correlate with ground-glass densities on HRCT. Somestudies have found more reticulonodular and linear changes.28
The lung biopsy specimen in DIP/RBILD is characterized by afairly homogeneous pattern in which alveolar spaces are filledwith pigmented alveolar macrophages. These accumulations ofmacrophages are often accentuated in peribronchiolar air spaces,sparing the more distal air spaces28 [see Figure 8].
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–17
Figure 7 Usual interstitial pneumonia is characterized by alveolar sep-tal thickening, caused by fibrosis; minimal inflammatory cell infiltrate;honeycombing; and irregular involvement from one region to the next.
Figure 8 Desquamative interstitial pneumonia/respiratory bronchioli-tis interstitial lung disease. The alveoli and septal walls are filled withmacrophages, and no fibrosis is apparent.

Discontinuance of smoking has been associated with improve-ment of symptoms. In some series, many patients improve with-out therapy, and steroids have been associated with a beneficialresponse in about 60%. The mortality is 20% to 30%, and themean survival is 12 years.
acute interstitial pneumonia
Acute interstitial pneumonia is a distinct idiopathic conditionthat produces respiratory failure of rapid onset.37 AIP is alsoknown as Hamman-Rich syndrome.
The clinical presentation of patients with AIP is similar to thatof patients with ARDS except that, in AIP patients, no predispos-ing factor can be identified. Patients often have had a viral pro-drome before onset. Over a period of less than 30 days, symp-toms of dyspnea, cough with mucoid sputum, and fever evolveinto respiratory failure. Imaging studies by routine chest radio-graph or HRCT show diffuse pulmonary infiltrates with ground-glass changes and consolidation.
The diagnosis is made by the recognition of a clinical illnesscompatible with ARDS in the absence of a predisposing factor af-ter the exclusion of other alveolar-filling diseases such as infec-tious pneumonia (especially PCP), alveolar hemorrhage, and eo-sinophilic pneumonia. The diagnosis is usually made throughbronchoscopy with bronchoalveolar lavage.
AIP is characterized pathologically by the findings of diffusealveolar damage. It cannot be differentiated from ARDS causedby sepsis, toxins, or shock [see Figure 9]. AIP evolves through thesame sequence of pathologic patterns as ARDS [see 14:X Pulmo-nary Edema].
Treatment is largely supportive through use of oxygen with ei-ther noninvasive or invasive mechanical ventilation. Steroids areadvocated, but their use is not supported by controlled trials.
The mean 6-month mortality is 78%.
lymphocytic interstitial pneumonia
LIP is an interstitial lung disease characterized by diffuse or lo-calized lymphocytic infiltration of the alveolar and interstitial ar-eas of the lung. This disorder can occur in association with anumber of autoimmune processes (especially Sjögren syndrome),dysproteinemias, viral infections (HIV), bone marrow transplan-tation, or as an idiopathic process.
LIP occurs more often in women than men. The mean age ofonset is 56 years. Patients present with dyspnea and cough, but
the associated disorder may dominate the clinical picture. Ralesand lymphadenopathy are common physical findings.
Imaging studies typically show reticulonodular infiltrates. Thepresence of hilar or mediastinal adenopathy or pleural effusionsuggests lymphoma. HRCT will usually show a mixture of inter-stitial and alveolar (ground-glass) changes.
Bronchoscopic specimens can be useful, showing a strikinglymphocytosis on BAL and revealing lymphocytic infiltration ontransbronchial lung biopsy [see Figure 10]. The pathologist will of-ten need to use special studies to differentiate LIP from neoplasticforms of lymphocytic infiltration of the lung.
Patients with LIP should be treated for their underlying disor-der, if present. Some patients respond to steroids, though manyrequire immunosuppressive agents.
nonspecific interstitial pneumonia/fibrosis
NSIP/F has often been confused with IPF. In one retrospectiveanalysis of patients that had been diagnosed with IPF, 14% werefound to have NSIP/F and were noted to have a better prognosisthan patients with IPF.29
NSIP/F occurs in middle-aged adults, with a mean age ofonset of 49 years, but it can also affect children and olderadults. There is a slight female predominance. Although somecases are idiopathic, many of the patients have collagen vascu-lar diseases, and some have a history of environmental or ther-apeutic drug exposures. A few of the patients have a history ofan acute lung injury, such as that caused by pneumonia, ARDS,or surgery.
Dyspnea, cough, and sometimes fever are the dominant clini-cal features, with imaging studies showing bilateral interstitial in-filtrates. HRCT scanning demonstrates bilateral, patchy areas ofground-glass abnormality.
NSIP/F can only be diagnosed by lung biopsy. As with IPF,transbronchial lung biopsy is not likely to produce an adequatespecimen, and therefore open biopsy is required. Pathologically,NSIP/F is characterized by a temporally uniform mixture of alve-olar wall inflammation (mostly lymphocytes and plasma cells)and fibrosis [see Figure 11].
Steroids provide improvement in more than half of the pa-tients with NSIP/F, and the prognosis for patients with NSIP/F issignificantly better than that for patients with IPF.38
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–18
Figure 9 Acute interstitial pneumonia. The biopsy specimen showsdiffuse alveolar damage.
Figure 10 Lymphocytic interstitial pneumonia. The biopsy specimen shows infiltration of the alveolar walls and alveoli with mature lymphocytes.

bronchiolitis obliterans organizing pneumonia
BOOP [see 14:IV Focal and Multifocal Lung Disease], also calledcryptogenic organizing pneumonitis,39 occurs partly in the inter-stitium, partly within the alveoli, and partly in the small airways.BOOP is another disorder sometimes incorrectly diagnosed asIPF. The disease may result from any number of secondary caus-es, including inhalation of toxic fumes (e.g., oxides of nitrogen),viral infections, aspiration, lung transplantation, collagen vascu-lar disorders, and other lung diseases, such as IPF and hypersen-sitivity pneumonitis.
Clinical Manifestations
BOOP occurs in three clinical patterns: symptomatic idiopath-ic, secondary, and focal asymptomatic.40 Although a thoroughhistory sometimes identifies one of the secondary causes men-tioned above, in some patients with idiopathic BOOP, an openlung biopsy is required to distinguish the disease from other dif-fuse parenchymal processes.
Patients with BOOP are usually 50 to 60 years of age. The ill-ness frequently begins abruptly and is characterized by drycough and dyspnea; fever, malaise, and fatigue are more com-mon in patients with BOOP than in those with IPF. Physical ex-amination sometimes discloses rales that are often associatedwith wheezes. Clubbing of the digits, which is common in IPF,is absent.
Diagnosis
The diagnosis of BOOP is made by the correlation of the clinicalfindings with the results of imaging studies, particularly HRCT.Lung biopsy is often required in those patients with idiopathicBOOP.
The chest radiograph typically shows bilateral patchy alveo-lar or ground-glass infiltrates, in contrast to the interstitial infil-trates that occur in IPF. HRCT often shows bilateral areas ofconsolidation involving mainly the subpleural region or peri-bronchovascular region, or both, that are quite suggestive of thediagnosis.41 Pulmonary function tests demonstrate obstruction,restriction, or a mixed pattern with decreased diffusing capacityand hypoxemia.
The lung biopsy in BOOP is characterized by the presence ofintraluminal plugs of connective tissue in the bronchioles, alveo-lar ducts, and alveolar spaces [see Figure 12].
Treatment
Treatment with glucocorticoids has been quite successful, andmany patients respond dramatically within days of starting ther-apy. When glucocorticoids are withdrawn, however, many pa-tients relapse and experience recurrent systemic symptoms, infil-trates, and hypoxemia. Patients with focal asymptomatic BOOPdo not require therapy.
collagen vascular diseases with associated pulmonary involvement
Collagen vascular diseases commonly affect the lung. As manyas two thirds of patients have clinical evidence of pleuropulmo-nary involvement, and nearly all have abnormal findings at au-topsy. The immune mechanism is thought to be immune complexdeposition, but the evidence that this mechanism is at work ismore convincing in some collagen vascular disorders than in oth-ers. Pulmonary function tests in patients with interstitial infiltratesand fibrosis show restriction, small airway obstruction, and re-duced Dlco with hypoxemia at rest, which worsens with exercise.HRCT of the chest often detects subtle interstitial disease that can-not be seen by routine chest radiography. Although the chronicinterstitial disease seen in some of these disorders is pathological-ly indistinguishable from IPF, patients with a collagen vasculardisease seem to have a better prognosis than those with IPF 42; thisis true even for those patients in whom collagen vascular diseasedevelops after IPF.43 Other patients with collagen vascular diseasewill have a pathologic pattern consistent with one of the otherIPF-like disorders such as NSIP/F or BOOP.
Systemic Lupus Erythematosus
SLE is one of the most prevalent of the collagen vascular dis-eases, especially in African-American women of childbearing age;however, as many as 18% of cases occur after the fifth decade oflife. Drug-induced SLE is a common clinical problem, especially inelderly patients with heart disease. Drugs that commonly causeSLE include hydralazine, procainamide, isoniazid, phenytoin,quinidine, methyldopa, and several of the beta-blocking agents.A few other drugs have been implicated, but the evidence is lessstrong.
Pleuropulmonary complications of SLE occur frequently (in38% to 89% of cases) and often must be differentiated from infec-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–19
Figure 11 Nonspecific interstitial pneumonia/fibrosis. The biopsyspecimen shows a temporally uniform mixture of alveolar wall inflam-mation (mostly lymphocytes and plasma cells and fibrosis).
Figure 12 Bronchiolitis obliterans organizing pneumonia. The biop-sy specimen shows intraluminal plugs of connective tissue in the bron-chioles, alveolar ducts, and alveolar spaces.

tions.44 Pleural disease, atelectasis, acute lupus pneumonitis, andchronic intersititial pneumonitis are the most common clinicalproblems. Less commonly, alveolar hemorrhage or pulmonaryvascular disease (acute reversible hypoxemia syndrome, vasculi-tis, or thromboembolism) may occur. Pleuropulmonary disease isfrequently the presentation of patients with drug-induced SLE.
Acute lupus pneumonitis initially presents as sudden onset ofcough and dyspnea. Radiographically, it appears as patchy basilaropacities. Occasionally, radiography shows only horizontal linearshadows that have been attributed to small areas of atelectasis; pa-tients in whom this occurs usually respond well to glucocorticoids.
Chronic interstitial pneumonitis occurs as a complication inabout 10% of patients with SLE. Many of the patients withchronic interstitial pneumonitis have mild, often asymptomat-ic disease detectable only by lung function testing and HRCT.Some cases are the result of prior episodes of acute lupus pneu-monitis. Pathologically, most of these cases are similar to casesof NSIP/F. Rarely, chronic interstitial pneumonitis evolves intosevere pulmonary fibrosis. Steroids and other immunosup-pressive agents may be beneficial, but no trials have been per-formed to investigate this.
Patients with SLE may present with overwhelming alveolar he-morrhage or have occult hemorrhage during the course of theirdisease. Severe alveolar hemorrhage in SLE is associated with a70% mortality. The symptoms are cough and dyspnea with orwithout hemoptysis; chest radiographs show fluffy alveolar infil-trates that may be patchy or confluent. Treatment is similar to thatof Goodpasture syndrome and includes plasmapheresis and im-munosuppressive therapy [see 10:V Glomerular Diseases].
Rheumatoid Arthritis
Although the incidence of rheumatoid arthritis is higher inwomen than in men, pleuropulmonary complications occur morefrequently in men.45 Pleuropulmonary complications are clinical-ly apparent in up to 14% of patients within 2 years of presenta-tion46 and in approximately 50% of patients over the course of theillness; a much higher percentage have pathologic involvement.In occasional cases, thoracic involvement becomes apparent be-fore the articular disease, making diagnosis difficult.
The most frequent pleuropulmonary problems are interstitiallung disease, bronchiolitis, pleural disease, and parenchymal rheu-matoid nodules. Less common problems include chronic airflowobstruction, bronchiectasis, BOOP, bronchiolitis obliterans, andpulmonary vasculopathy. These problems are usually associatedwith active arthritis, high titers of rheumatoid factor, circulatingimmune complexes, and cryoglobulinemia.
Diffuse interstitial pneumonitis with fibrosis is the most com-mon and serious pulmonary problem in patients with rheuma-toid arthritis. Dyspnea, sometimes with cough, is the symptomthat occurs most frequently. Clubbing of the fingers may be pres-ent. The chest radiograph evolves from fine nodularity to coarsereticulation and finally to a honeycomb pattern. Results of BALmay be abnormal, demonstrating increased numbers of lympho-cytes, neutrophils, eosinophils, or all three; this variability has notbeen shown to have a bearing on management. In patients withinterstitial disease that is characterized by increased cellularity inlung biopsy specimens or the presence of progressive symptoms,glucocorticoids should be administered.
Rheumatoid (necrobiotic) nodules may be found in many tis-sues, including the lung parenchyma, endobronchial mucosa,and pleurae; in any of these locations, the nodules may cavitate.These lesions have a characteristic histopathologic appearance on
microscopic examination; unless percutaneous transthoracic nee-dle biopsy or open lung biopsy is performed, such lesions can bedifficult to differentiate from those of malignancy or tuberculosis.Most rheumatoid nodules do not cause symptoms, and treatmentis rarely necessary once a diagnosis is established.
Progressive Systemic Sclerosis
Progressive systemic sclerosis (PSS), also called scleroderma, isa disorder that predominantly affects women in the fourth tosixth decades of life. The prognosis is unfavorable, especially inAfrican Americans, men, and patients with pulmonary disease.
Pulmonary complications, particularly interstitial lung disease,frequently develop, occurring in as many as 90% of confirmedcases of PSS.47 Interstitial lung disease in PSS is characterized bybasilar reticular or reticulonodular fine infiltrates that becomecoarser as the disease progresses. In addition, radiography mayshow a loss of volume over time, and pneumothorax may occur.Evidence of pulmonary hypertension may be greater than wouldbe expected from the degree of radiographic abnormality or pul-monary function disturbance, especially when Raynaud phenom-enon is part of the clinical syndrome.
Glucocorticoids are not useful as therapy for interstitial lungdisease associated with PSS; cyclophosphamide may be effectivein patients who are shown by BAL to have active alveolitis.47 As aresult of esophageal motility disturbance, aspiration of gastricand esophageal contents often occurs; aspiration occurs more fre-quently when patients are in the recumbent position. Aspirationcan be prevented by elevating the upper body to the near-uprightposition.
CREST syndrome (calcinosis, Raynaud phenomenon, esopha-geal dysmotility, sclerodactyly, telangiectasia) is a variant of PSS.Patients with CREST syndrome have prominent pulmonary vas-cular disease. This pulmonary hypertension may be associatedwith interstitial fibrosis, as is seen in PSS, or it may occur as anisolated finding [see 15:V Scleroderma and Related Diseases].
Polymyositis and Dermatomyositis
Polymyositis and dermatomyositis are autoimmune disordersthat are characterized by weakness and occasionally by pain inproximal limb and neck muscles, skin rash (dermatomyositis),and neoplasm. The most frequent pulmonary complications ofpolymyositis and dermatomyositis are respiratory failure causedby respiratory muscle weakness, aspiration secondary to posteri-or pharyngeal and proximal esophageal weakness, and intersti-tial lung disease.48
Interstitial lung disease is seen in a minority of patients andmay be associated with anti–Jo-1 antibody, an autoantibody thatis specific to the cellular enzyme histidyl-tRNA synthetase. Thesepatients may have BOOP, pulmonary fibrosis, or diffuse alveolardamage. In contrast to the interstitial disease associated with manyof the other connective tissue disorders, that associated with poly-myositis and dermatomyositis responds well to glucocorticoidtherapy.
Sjögren Syndrome
Sjögren syndrome comprises the triad of keratoconjunctivitissicca, xerostomia, and recurrent swelling of the parotid glands andis often (in 60% of cases) associated with other collagen vasculardiseases. Sjögren syndrome frequently includes pleuropulmonaryproblems, but in many cases, these problems are secondary to theunderlying connective tissue disease. Thoracic complications thatmay be directly related to Sjögren syndrome include interstitial
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–20

infiltrates, often lymphocytic in nature (LIP); pleurisy with orwithout effusion; follicular bronchiolitis; and desiccation of thetracheobronchial tree, producing bronchiectasis and recurrentbronchitis or pneumonitis.49
Dyspnea is the primary symptom of the interstitial disease as-sociated with Sjögren syndrome, whereas hoarseness and coughthat is productive of thick, tenacious sputum are symptoms of la-ryngeal and tracheobronchial involvement. Chest radiographymay show interstitial infiltrates with a prominent nodular com-ponent. These infiltrates have a lymphoplasmacytic histologythat can be difficult to differentiate from that seen in patients withlymphoma. Results of pulmonary function tests demonstrate restrictive, obstructive, or mixed patterns. The lymphocytic inter-stitial pneumonitis and bronchiolitis associated with Sjögren syn-drome respond to glucocorticoid treatment or immunosuppres-sive therapy.
Mixed Connective Tissue Disease
Several reports have described patients who have features ofSLE, PSS, and polymyositis, often with associated pulmonary dis-ease.50 A hallmark of such mixed connective tissue disease is thepresence of high titers of antibodies to extractable nuclear ribonu-cleoprotein (anti-nRNP). This syndrome is usually a relatively be-nign disease that responds well to glucocorticoids, although somecases display a less benign course that is associated with fatal dif-fuse interstitial lung disease or pulmonary hypertension.
eosinophilic granuloma of the lung
Eosinophilic granuloma of the lung, or pulmonary histiocytosisX, is an uncommon cause of diffuse infiltrative lung disease thatprimarily affects persons who are 20 to 50 years of age.51 The dis-ease is uncommon in African Americans and extraordinarily rarein Asians. The etiology of eosinophilic granuloma is unknown, butthere is a strong association with cigarette smoking. In childrenand young adults, eosinophilic granuloma is a systemic diseasewith a similar histologic appearance, and either diabetes insipidusresulting from pituitary involvement or eosinophilic granulomaof bone may be seen in 15% to 20% of patients.
Clinical Manifestations
Most patients with pulmonary eosinophilic granuloma havecough or dyspnea, but as many as 25% of affected persons haveonly radiographic abnormalities and no symptoms. Between 10%and 20% of patients develop pneumothoraces, and a spontaneouspneumothorax may be the initial manifestation of the disease. Theassociation of spontaneous pneumothorax with radiographic evi-dence of diffuse interstitial infiltrates suggests a diagnosis of eo-sinophilic granuloma or AIDS-related PCP.
The patterns seen on chest radiographs and HRCT in eosino-philic granuloma are variable. Nodular and ground-glass opacitieswith thick-walled cysts are typically present early in the course ofthe disease. Later, thin-walled cysts, linear opacities, and emphy-sematous lesions are seen.
Eosinophilic granuloma often causes a reduction in Dlco andvital capacity. However, unlike most other types of diffuse infil-trative lung disease, airflow obstruction is a characteristic feature,particularly in the later stages of the disease. The high incidenceof airflow obstruction in eosinophilic granuloma may result frombronchiolar involvement in earlier stages of the disease and frombullae in late-stage disease. Smoking may also be a contributingfactor in the high frequency of airflow obstruction in this disor-der. Significant impairment of exercise performance is frequent
and is greater than might be expected from the degree of volumerestriction. Increasing wasted ventilation ratio (Vd/Vt) and fall-ing Pao2 with exercise result in poor exercise performance in pa-tients with pulmonary vascular abnormalities.52
Histopathologic Features
The histopathologic features of eosinophilic granuloma areunique and include the presence of cells that resemble Langerhanscells in the skin. These cells stain positively with anti-CD1a mono-clonal antibody and are shown by electron microscopy to containcharacteristic inclusions termed X bodies, or Birbeck granules.51
These cells can be seen in other types of diffuse infiltrative lungdisease, but their numbers are much greater in eosinophilic granu-loma. In patients with eosinophilic granuloma, CD4+ T cells are inapposition to Langerhans cells, and there are increased numbers ofneuroendocrine cells.53 Granulocyte-macrophage colony-stimulat-ing factor and TGF-β are found in the lesions, suggesting thatthese factors are potential mediators of the stimulation of Langer-hans cells and fibroblasts, respectively. These findings suggest thatthe pathogenesis of eosinophilic granuloma involves interactionsamong these cells that result in fibroblast stimulation and fibrosis.
Diagnosis
The diagnosis of eosinophilic granuloma can be made mostconfidently by open lung biopsy. However, it has been suggestedthat the finding of more than 5% CD1a+ cells in BAL fluid, alongwith an appropriate clinical and radiographic picture, may suf-fice for diagnosis.51 HRCT may prove to be a useful noninvasivetechnique for diagnosing eosinophilic granuloma.
Prognosis and Treatment
Patients with eosinophilic granuloma have a median survivalof 6 years after diagnosis. Increased age, airflow obstruction, andhyperinflation are predictors of a poor prognosis.
Patients with eosinophilic granuloma have shown improve-ment after smoking cessation, and treatment with glucocorticoidshas been reported to be effective, though no therapy has been suf-ficiently studied or has produced sufficiently convincing evidenceof clinical benefit to justify a definitive recommendation.
alveolar proteinosis
Alveolar proteinosis is a rare disease of unknown etiology char-acterized by the intra-alveolar accumulation of a cellular lipopro-teinaceous material that resembles surfactant.54 The accumulationof surfactant-like material may result from increased productionor decreased degradation of surfactant by macrophages. It hasbeen proposed that underutilization of surfactant, with decreasedreturn from alveoli to type II cells, may overwhelm the normalmacrophage’s ability to clear this substance. In addition, the lipo-proteinaceous material may inhibit the macrophage’s defenseagainst infection, thereby producing the increased incidence ofinfection with intracellular pathogens that has been observed inpatients with alveolar proteinosis. A disorder that is clinicallysimilar to idiopathic alveolar proteinosis occurs in persons withacute silica exposure (usually sandblasters) and in patients withany of several hematologic disorders.
Clinical Manifestations
Patients with alveolar proteinosis present in one of three ways:(1) without symptoms but with an abnormal chest radiograph; (2)with abrupt onset of cough, fever, and chest pain caused by thedisease and complicated by opportunistic infection (with Nocar-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–21

dia species, fungi, or Mycobacterium species); and (3) with dyspneaand cough (sometimes productive) of gradual onset. Physicalfindings are often minimal. The chest radiograph or HRCT usual-ly shows a bilateral alveolar filling process mimicking pulmonaryedema but without Kerley B lines, pleural effusions, or enlarge-ment of the central vasculature. In later stages of the disease,coarse interstitial markings resulting from superimposed fibrosiscan be seen. An elevated serum lactate dehydrogenase level with-out elevation of other serum enzyme levels may help the physi-cian make the diagnosis.
Histopathologic Features
The histopathologic changes in alveolar proteinosis includethe presence of a granular, eosinophilic material within alveolarspaces that stains positively with the periodic acid-Schiff (PAS)reagent [see Figure 13]. Inflammation and fibrosis have been de-tected in some cases but are usually not prominent features. Elec-tron microscopy reveals that the intra-alveolar substance containsnumerous lamellar bodies, similar to those found in type II epi-thelial cells.
Diagnosis
Diagnosis of pulmonary alveolar proteinosis is made mostconveniently by BAL. The effluent appears grossly turbid, andstaining reveals large amounts of the PAS-positive material [seeFigure 13]. PCP causes accumulation of a similar intra-alveolarsubstance, and this infection must be excluded by special stains.The lavage liquid should be cultured for Nocardia species, fungi,and Mycobacterium species.
Treatment
Treatment of alveolar proteinosis is indicated if significantdyspnea is present at the time of diagnosis or if lesser symptomsfail to remit spontaneously after an observation period of severalmonths. Because some patients undergo spontaneous remission,it is preferable to wait several months whenever possible beforeinstituting treatment. Therapy for pulmonary alveolar proteino-sis consists of whole lung lavage with sterile saline. The non-lavaged lung is protected by a double-lumen endotracheal tube.Most patients improve substantially after removal of the alveolar
material by lavage, and the contralateral lung can be lavaged at alater date.
eosinophilic pneumonia
Pulmonary infiltrates with peripheral eosinophilia (PIE), occa-sionally with bronchospasm, are most often the result of acute hy-persensitivity.55 PIE comprises five syndromes: (1) simple pulmo-nary eosinophilia (Löffler syndrome); (2) prolonged pulmonaryeosinophilia without asthma; (3) pulmonary eosinophilia withasthma [see 14:II Asthma]; (4) tropical pulmonary eosinophilia; and(5) pulmonary vasculitis (allergic granulomatosis and angiitis) [see14:IV Focal and Multifocal Lung Disease]. In many of these disor-ders, substances secreted by eosinophils may help cause injury tothe lung parenchyma, airways, or both. Although hypereosino-philic syndrome is not included in this classification, it too is occa-sionally associated with pulmonary infiltrates [see 14:VII Disordersof the Chest Wall]. A new disorder, acute eosinophilic pneumonia,has been described. Miscellaneous disorders that may also causepulmonary infiltrates with blood eosinophilia include infections(e.g., tuberculosis, brucellosis, and fungal diseases), neoplastic dis-eases (e.g., bronchogenic carcinoma, Hodgkin disease, and immu-noblastic lymphadenopathy), and immune processes (e.g., rheu-matoid lung disease and sarcoidosis).
Simple Pulmonary Eosinophilia (Löffler Syndrome)
Löffler syndrome is characterized by transient and sometimesmigratory infiltrates and by mild symptoms lasting less than 1month. The infiltrates are usually homogeneous in density; eithera single infiltrate or multiple infiltrates may occur. Symptoms maybe absent, or dyspnea and dry cough may develop. Pathologic ex-amination reveals interstitial and intra-alveolar accumulation ofeosinophils, macrophages, and fluid. Löffler syndrome may beidiopathic or may be caused by parasitic infestation (e.g., with As-caris or Strongyloides) or a drug (e.g., nitrofurantoin or penicillin).Therapy consists of removing the offending drug or treating theparasitic infestation; in most cases, no other therapy is required.Occasionally, patients with very symptomatic idiopathic diseaserequire glucocorticoid therapy.
Prolonged Pulmonary Eosinophilia without Asthma
Prolonged pulmonary eosinophilia (chronic eosinophilicpneumonia) is an idiopathic disease that predominantly affectsmiddle-aged women. It is characterized by productive cough,dyspnea, malaise, weight loss, night sweats, and fever associatedwith progressive peripheral pulmonary infiltrates. Hemoptysisand wheezing may be present, which may lead to confusionwith other causes of PIE. Pulmonary function test results may benormal or may show either restriction or obstruction.56 Openlung biopsy specimens show massive, mixed inflammatory infil-trates that have a high eosinophil content. Some pulmonary ves-sels may contain a few inflammatory cells, but true vasculitis isnot present.
Diagnosis is based on the clinical syndrome, chest radiogra-phy, and whether or not blood eosinophilia is present. If resultsof chest radiography show typical dense peripheral infiltrateswith central sparing, the diagnosis can be made without tissueexamination. Usually, confirmatory information can be easily ob-tained by BAL and transbronchial lung biopsy.
Spontaneous remissions occur in as many as 10% of cases, butrespiratory failure can also occur. Treatment with glucocorticoidsis rapidly effective. Because relapses are frequent, the need tocontinue therapy for as long as 5 years is common.
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–22
Figure 13 Bronchoalveolar lavage effluent reveals distinctive periodicacid–Schiff–positive material that is diagnostic of alveolar proteinosis.

Pulmonary Eosinophilia with Asthma
Allergic bronchopulmonary aspergillosis can cause pulmo-nary infiltrates in a patient with asthma [see 14:II Asthma].
Tropical Pulmonary Eosinophilia
The diagnosis of tropical pulmonary eosinophilia is suggestedby the onset of asthma, fever, and marked blood eosinophilia andthe presence of basilar mixed reticulonodular and alveolar infil-trates in a person who has recently traveled to the Far East.57 Thisdisease probably represents a form of filariasis (caused by Wuch-ereria bancrofti or other organisms). Despite therapy with diethyl-carbamazine, many patients with this disorder have persistent in-flammation and develop chronic interstitial disease.
Pulmonary Vasculitis (Allergic Granulomatosis and Angiitis)
Allergic granulomatosis and angiitis is a multisystem disordercharacterized by vasculitis and necrotizing granulomatous in-flammation that involve the lungs, nervous system, and skin.58
Although the kidneys, heart, spleen, and GI tract are much lesscommonly affected, any organ or tissue may be involved. Theprominence of eosinophilia and elevated IgE levels suggest thatimmediate hypersensitivity mechanisms may play an importantrole in pathogenesis [see 14:IV Focal and Multifocal Lung Disease].
Hypereosinophilic Syndrome
Hypereosinophilic syndrome is characterized by a wide rangeof clinical manifestations that occur when mature eosinophils in-filtrate organs [see 5:VII Nonmalignant Disorders of Leukocytes].
Acute Eosinophilic Pneumonia
Acute eosinophilic pneumonia is characterized by the acuteonset of cough, dyspnea, fever, tachypnea, and rales; patientsfrequently require mechanical ventilation.59 There is no clear as-sociation with cigarette smoking, environmental exposures, ordrug intake, and patients tend to be young. Blood eosinophiliais not seen in most cases and is therefore not useful in diagnos-ing this disorder. Chest radiography and CT scanning shownonspecific combinations of alveolar (ground-glass) infiltratesand mixed alveolar-interstitial infiltrates that are sometimes as-sociated with pleural effusions. The diagnosis can be made bybronchoalveolar lavage, which shows dramatic increases in thepercentage of eosinophils, often to greater than 20% (the nor-mal count is less than 1%). The administration of corticoste-roids leads to rapid improvement, and relapses after steroidwithdrawal are rare.
diffuse alveolar hemorrhage
Alveolar hemorrhage syndromes are characterized by diffuseparenchymal bleeding in the absence of blood aspiration, coagu-lopathy, elevation of pulmonary venous pressure, or an identifi-able local cause (e.g., pulmonary emboli, cancer, or bronchitis).Frequently, diffuse alveolar hemorrhage is immunologically me-diated and is often associated with glomerulonephritis.
The diseases that cause this syndrome are anti–glomerularbasement membrane (anti-GBM) antibody disease (Goodpasturesyndrome), idiopathic and rapidly progressive glomerulonephri-tis with or without immune complexes, vasculitis (e.g., Wegenergranulomatosis), SLE, and idiopathic pulmonary hemosiderosis.60
Although each of these disorders has suggestive clinical charac-teristics, in many cases the diagnosis cannot be made on clinicalgrounds. In addition, many patients with diffuse alveolar hemor-
rhage are acutely ill, making a rapid and specific evaluation neces-sary. A suggested diagnostic approach to such a patient consists ofthe following steps:
1. Obtain serum to test for anti-GBM antibody, antinuclear andanti-DNA antibody, antineutrophil cytoplasmic antibody, com-plement levels, and immune complexes.
2. Perform bronchoalveolar lavage with an iron stain of the ob-tained specimen. If hemosiderin-laden macrophages are pres-ent in large numbers, the diagnosis of alveolar hemorrhage isconfirmed.
3. If step 1 fails to confirm a diagnosis or the results are notrapidly available, a biopsy of the kidney, lung, or another in-volved site should be performed. Immunofluorescence andelectron microscopy with routine tissue examination shouldbe included.
Almost all cases of alveolar hemorrhage can be rapidly diag-nosed if the physician follows this approach. Treatment withhigh doses of intravenous glucocorticoids should be startedwhile the evaluation is in progress, because alveolar hemorrhagecan rapidly become life threatening.
Anti-GBM Antibody Disease
Anti-GBM antibody disease occurs in young men who smokecigarettes. It is characterized by glomerulonephritis and diffusealveolar hemorrhage61 and is caused by cytotoxic antibody againstthe α3 chain of type IV collagen in glomerular and alveolar base-ment membranes.
Many patients present with hemoptysis, which can be mas-sive; however, some episodes of hemorrhage occur without he-moptysis. Most patients complain of dyspnea, and gross hema-turia is common. Iron deficiency anemia is present in nearly allpatients, and renal failure is present initially in 50% of cases.
Chest radiography initially shows fluffy perihilar acinar shad-ows; later, interstitial changes are seen. Pulmonary function testsdemonstrate a restrictive pattern that improves with clinical reso-lution. Dlco may be increased because of carbon monoxide up-take by extravascular hemoglobin. As the disease becomes chron-ic, interstitial radiographic changes and restrictive pulmonaryfunction abnormalities may persist.
The diagnosis is confirmed when circulating anti-GBM anti-body is detected (95% of patients have anti-GBM antibody) or lin-ear deposits of IgG (occasionally IgA) are demonstrated on theglomerular or alveolar basement membrane. Anti-GBM antibodycan also be eluted from the involved tissue.
Current recommendations for treatment include immunosup-pressive agents, glucocorticoids, and plasmapheresis. Despite thisaggressive therapy, 50% of patients die or require long-term dial-ysis after 2 years. Death is often caused by massive alveolar hem-orrhage that is frequently precipitated by infection.
Idiopathic Pulmonary Hemosiderosis
Idiopathic pulmonary hemosiderosis, a disorder characterizedby recurrent alveolar hemorrhage, occurs primarily in children(usually younger than 10 years of age) and young adults. When itoccurs in adults, men are more often affected than women. Pre-sentation of the disease is similar to that of Goodpasture syn-drome except for the absence of renal involvement. Recurrentepisodes of clinical and subclinical hemorrhage occur over time,resulting in lung damage that may be obstructive or restrictive innature. Lung tissue shows changes of acute and chronic hemor-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–23

rhage, but no vasculitis, immune complexes, or linear-stainingdeposits are found.
Patients with idiopathic pulmonary hemosiderosis are treatedwith glucocorticoids. Anecdotal evidence supports the use of im-munosuppressive agents and plasmapheresis. Mean survival is 3 to 5 years, but spontaneous remissions and long-term survivaldo occur.
lymphangioleiomyomatosis
The onset of lymphangioleiomyomatosis, which affects wom-en of childbearing age almost exclusively, is often heralded bysome combination of hemoptysis, pneumothorax, and chylotho-rax.62 At the onset of symptoms, there may be no diffuse radio-graphic abnormality, though a fine reticulonodular process, pre-dominating at the lung bases, may be seen. Occasionally, there isa diffuse interstitial pattern in association with hyperinflation. Incontrast to most diffuse infiltrative lung diseases, this disorder isoften characterized by obstructive physiology with increasedlung volumes, which has been attributed to peribronchial smoothmuscle hypertrophy. In addition, Dlco is usually decreased.
The diagnosis may be strongly suspected in a young non-smoking woman with chylothorax, fixed airway obstruction, anda diffuse interstitial radiographic pattern.63 HRCT that shows dif-fuse, thin-walled cysts is diagnostic. These findings are identicalto those of tuberous sclerosis. Open lung biopsy reveals diffuseproliferation of smooth muscle cells in the lung and visceral pleu-ra, with cyst formation possibly secondary to bronchiolar obstruc-tion. Approximately 50% of patients also have renal angiomy-olipomas as an associated finding, often first identified on CTscanning. More than 75% of patients survive longer than 8 years.64
There is some evidence that disease progression is hormone de-pendent, and some slowing of progression has been reportedwith oophorectomy, progesterone treatment, or a combination ofthe two. Lung transplantation may be considered for end-stagedisease. Although transplantation may be lifesaving, there havebeen cases of recurrence in the transplanted lung, emphasizingthe systemic nature of the disorder.
microlithiasis
Microlithiasis is an exceedingly rare, sometimes familial disor-der that is most often diagnosed in an asymptomatic patient by aroutine chest radiograph. The chest radiograph reveals a striking-ly distinct and diffuse scattering of small calcified nodules that, onhistopathologic examination, are seen to be calcified spheres thatoccupy the alveolar space.65 This condition may progress to respi-ratory failure. A possible response to treatment with disodium eti-dronate, a diphosphonate, has been reported in a single patient.66
Gerald W. Staton, Jr., M.D., participates in the speakers’ bureaus of Glaxo-SmithKline and Intermune Pharmaceuticals, Inc.; Roland H. Ingram, Jr., M.D.,has no commercial relationships with manufacturers of products or providersof services discussed in this subsection.
References1. Coultas DB, Zumwalt RE, Black WC, et al: The epidemiology of interstitial lung dis-eases. Am J Respir Crit Care Med 150:967, 19942. Respiratory diseases disproportionately affecting minorities. The NHLBI WorkingGroup. Chest 108:1380, 19953. Cooper JA Jr: Pulmonary fibrosis: pathways are slowly coming into light. Am J RespirCell Mol Biol 22: 520, 20004. Lympany PA, du Bois RM: Diffuse lung disease: product of genetic susceptibility andenvironmental encounters. Thorax 52:92, 1997
5. Reynolds HY: Diagnostic and management strategies for diffuse interstitial lung dis-ease. Chest 113:192, 19986. Raghu G, Mageto YN, Lockhart D, et al: The accuracy of the clinical diagnosis of new-onset idiopathic pulmonary fibrosis and other interstitial lung disease: a prospectivestudy. Chest 116:1168, 19997. Drent M, van Nierop MA, Gerritsen FA, et al: A computer program using BALF-analy-sis results as a diagnostic tool in interstitial lung diseases. Am J Respir Crit Care Med153:736, 19968. Molin LJ, Steinberg JB, Lanza LA: VATS increases costs in patients undergoing lung bi-opsy for interstitial lung disease. Ann Thorac Surg 58:1595, 19949. Harris-Eze AO, Sridhar G, Clemens RE, et al: Oxygen improves maximal exercise per-formance in interstitial lung disease. Am J Respir Crit Care Med 150:1616, 199410. Rosenow E: Drug-induced pulmonary disease. Dis Mon 40:253, 199411. Mossman BT, Churg A: Mechanisms in the pathogenesis of asbestosis and silicosis.Am J Respir Crit Care Med 157:1666, 199812. Sharma SK, Pande JN, Verma K: Effect of prednisolone treatment in chronic silicosis.Am Rev Respir Dis 143:814, 199113. Rossman MD: Chronic beryllium disease: diagnosis and management. EnvironHealth Perspect 104(suppl 5):945, 199614. Matar LD, McAdams HP, Sporn TA: Hypersensitivity pneumonitis. AJR Am JRoentgenol 174:1061, 200015. Lynch DA, Newell JD, Logan PM, et al: Can CT distinguish hypersensitivity pneu-monitis from idiopathic pulmonary fibrosis? AJR Am J Roentgenol 165:807, 199516. Drent M, van Velzen-Blad H, Diamant M, et al: Bronchoalveolar lavage in extrinsic al-lergic alveolitis: effect of time elapsed since antigen exposure. Eur Respir J 6:1276, 199317. Akira M, Atagi S, Kawahara M, et al: High-resolution CT findings of diffuse bronchi-oloalveolar carcinoma in 38 patients. AJR Am J Roentgenol 173:1623, 199918. Bragg DG, Chor PJ, Murray KA, et al: Lymphoproliferative disorders of the lung:histopathology, clinical manifestations, and imaging features. AJR Am J Roentgenol 163:273, 199419. Statement on sarcoidosis. Joint statement of the American Thoracic Society (ATS), theEuropean Respiratory Society (ERS) and the World Association of Sarcoidosis and OtherGranulomatous Disorders (WASOG). Am J Respir Crit Care Med 160: 736, 199920. Newman LS, Rose CS, Maier LA: Sarcoidosis. N Engl J Med 336:1224, 199721. Mañá J, Gómez-Vaquero C, Montero A, et al: Löfgren’s syndrome revisited: a studyof 186 patients. Am J Med 107:1999, 199922. Baughman RP, Lower EE: A clinical approach to the use of methotrexate for sarcoido-sis. Thorax 54:742, 199923. Walker S, Mikhail G, Banner N, et al: Medium term results of lung transplantation forend stage pulmonary sarcoidosis. Thorax 53:281, 199824. Idiopathic pulmonary fibrosis: diagnosis and treatment: international consensus state-ment. Joint statement of the American Thoracic Society (ATS) and the European Respira-tory Society (ERS). Am J Respir Crit Care Med 161:646, 200025. Coker RK, Laurent GJ: Anticytokine approaches in pulmonary fibrosis: bringing fac-tors into focus. Thorax 52:294, 199726. Hansell DM: High-resolution computed tomography in the evaluation of fibrosingalveolitis. Clin Chest Med 20:739, 199927. Cherniack RM, Colby TV, Flint A, et al: Correlation of structure and function in idio-pathic pulmonary fibrosis. Am J Respir Crit Care Med 151:1180, 199528. Katzenstein AL, Myers JL: Idiopathic pulmonary fibrosis: clinical relevance of patho-logic classification. Am J Respir Crit Care Med 157:1301, 199829. Bjoraker JA, Ryu JH, Edwin MK, et al: Prognostic significance of histopathologic sub-sets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 157:199, 199830. Hubbard R, Johnston I, Britton J: Survival in patients with cryptogenic fibrosing alve-olitis: a population-based cohort study. Chest 113:396, 199831. Gay SE, Kazerooni EA, Towes GB, et al: Idiopathic pulmonary fibrosis: predicting re-sponse to therapy and survival. Am J Respir Crit Care Med 157:1063, 199832. Van Oortegem K, Wallaert B, Marquette CH, et al: Determinants of response to im-munosuppressive therapy in idiopathic pulmonary fibrosis. Eur Respir J 7:1950, 199433. Douglas WW, Ryu JH, Bjoraker JA, et al: Colchicine versus prednisone as treatment ofusual interstitial pneumonia. Mayo Clin Proc 72:201, 199734. Meyers BF, Lynch JP, Trulock EP, et al: Single versus bilateral lung transplantation foridiopathic pulmonary fibrosis: a ten-year institutional experience. J Thorac CardiovascSurg 120:99, 200035. Mason RJ, Schwarz MI, Hunninghake GW, et al: Pharmacological therapy for idio-pathic pulmonary fibrosis: past, present, and future. Am J Respir Crit Care Med 160:1771,199936. Ziesche R, Hofbauer E, Wittmann K, et al: A preliminary study of long-term treat-ment with interferon gamma-1b and low-dose prednisolone in patients with idiopathicpulmonary fibrosis. N Engl J Med 341:1264, 199937. Bouros D, Nicholson AC, Polychronopoulos V, et al: Acute interstitial pneumonia.Eur Respir J 15:412, 200038. Nagai S, Kitaichi M, Itoh H, et al: Idiopathic nonspecific interstitial pneumonia/fibro-sis: comparison with idiopathic pulmonary fibrosis and BOOP. Eur Respir J 12:1010, 199839. Alasaly K, Muller N, Ostrow DN, et al: Cryptogenic organizing pneumonia: a reportof 25 cases and a review of the literature. Medicine (Baltimore) 74:201, 199540. Lohr RH, Boland BJ, Douglas WW, et al: Organizing pneumonia: features and prog-nosis of cryptogenic, secondary, and focal variants. Arch Intern Med 157:1323, 199741. Lee KS, Kullnig P, Hartman TE, et al: Cryptogenic organizing pneumonia: CT find-
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–24

ings in 43 patients. AJR Am J Roentgenol 162:543, 199442. Agustí C, Xaubet A, Roca J, et al: Interstitial pulmonary fibrosis with and without as-sociated collagen vascular disease: results of a two year follow up. Thorax 47:1035, 199243. Homma Y, Ohtsuka Y, Tanimura K, et al: Can interstitial pneumonia as the sole pre-sentation of collagen vascular diseases be differentiated from idiopathic interstitial pneu-monia? Respiration 62:248, 199544. Keane MP, Lynch JP III: Pleuropulmonary manifestations of systemic lupus erythe-matosus. Thorax 55:159, 200045. Tanoue L: Pulmonary manifestations of rheumatoid arthritis. Clin Chest Med 19:667,199846. Gabbay E, Tarala R, Will R, et al: Interstitial lung disease in recent onset rheumatoidarthritis. Am J Respir Crit Care Med 156:528, 199747. Minai OA, Dweik RA, Arroliga AC: Manifestations of scleroderma pulmonary dis-ease. Clin Chest Med 19:713, 199848. Schwarz MI: The lung in polymyositis. Clin Chest Med 19:701, 199849. Cain HC, Noble PW, Matthay RA: Pulmonary manifestations of Sjögren’s syndrome.Clin Chest Med 19:687, 199850. Prakash UB: Respiratory complications in mixed connective tissue disease. Clin ChestMed 19:733, 199851. Vassallo R, Ryu JH, Colby TV, et al: Pulmonary Langerhans’-cell histiocytosis. N EnglJ Med 342:1969, 200052. Crausman RS, Jennings CA, Tuder RM, et al: Pulmonary histiocytosis X: pulmonaryfunction and exercise pathophysiology. Am J Respir Crit Care Med 153:426, 199653. Aguayo SM, King TE Jr, Waldron JA Jr, et al: Increased pulmonary neuroendocrinecells with bombesin-like immunoreactivity in adult patients with eosinophilic granuloma.J Clin Invest 86:838, 199054. Shah PL, Hansell D, Lawson PR, et al: Pulmonary alveolar proteinosis: clinical aspectsand current concepts on pathogenesis. Thorax 55:67, 200055. Allen JN, Davis WB: Eosinophilic lung diseases. Am J Respir Crit Care Med 150:1423,199456. Marchand E, Reynaud-Gaubert M, Lauque D, et al: Idiopathic chronic eosinophilic
pneumonia: a clinical and follow-up study of 62 cases. Groupe d’Etudes et de Recherchesur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Medicine (Baltimore) 77:299,199857. Ong RK, Doyle RL: Tropical pulmonary eosinophilia. Chest 113:1673, 199858. Choi YH, Im JG, Han BK, et al: Thoracic manifestation of Churg-Strauss syndrome:radiologic and clinical findings. Chest 117:117, 200059. Pope-Harman A, Davis W, Allen E, et al: Acute eosinophilic pneumonia: a summaryof 15 cases and review of the literature. Medicine (Baltimore) 75:334, 199660. Schwarz MI, Brown KK: Small vessel vasculitis of the lung. Thorax 55:502, 200061. Ball JA, Young KR Jr: Pulmonary manifestations of Goodpasture’s syndrome: anti-glomerular basement membrane disease and related disorders. Clin Chest Med 19:777,199862. Report of workshop on lymphangioleiomyomatosis. National Heart, Lung, and BloodInstitute. Am J Respir Crit Care Med 159:679, 199963. Chu SC, Horiba K, Usuki J, et al: Comprehensive evaluation of 35 patients with lym-phangioleiomyomatosis. Chest 115:1041, 199964. Kitaichi M, Nishimura K, Itoh H, et al: Pulmonary lymphangioleiomyomatosis: a re-port of 46 patients including a clinicopathologic study of prognostic factors. Am J RespirCrit Care Med 151:527, 199565. Prakash UB, Barham SS, Rosenow EC 3rd, et al: Pulmonary alveolar microlithiasis: areview including ultrastructural and pulmonary function studies. Mayo Clin Proc 58:290,198366. Göcmen A, Toppare MF, Kiper N, et al: Treatment of pulmonary alveolar microlithi-asis with a diphosphonate—preliminary results of a case. Respiration 59:250, 1992
AcknowledgmentsFigure 1 Courtesy of Dr. Sam Aguayo, Veterans Affairs Medical Center, Decatur, Georgia.Figure 4 Andy Christie.Figures 7 through 12 Courtesy of Dr. Anthony Gal, Emory University Hospital, De-catur, Georgia.
© 2001 WebMD Inc. All rights reserved.June 2001 Update
WebMD Scientific American® MedicineRESPIRATORY MEDICINE:V Chronic Diffuse Infiltrative Lung Disease–25