Embed Size (px)
DESCRIPTION
A thesis presented on the vaccine market and how the market is insufficient for meeting the needs ofconsumers. Evidence will be produced demonstrating several inadequacies within the firm, government’s role in creating incentives, and retarding competition, and why we as consumers should be alarmed.
Citation preview
THE VACCINE MARKET: A CAUSE FOR ALARM
By
Donald William Hansel
A thesis submitted in partial fulfillment of the requirements for the degree of
B.S. Economics
The George Washington University
2010

THE GEORGE WASHINGTON UNIVERSITY
ABSTRACT
Failures of the Vaccine Market: A Cause for Alarm
By Donald William Hansel
Pro-seminar/Thesis Advisor: Professor Robert Trost Department of Economics
A thesis presented on the vaccine market and how the market is insufficient for meeting the needs of
consumers. Evidence will be produced demonstrating several inadequacies within the firm,
government’s role in creating incentives, and retarding competition, and why we as consumers should
be alarmed.

i
TABLE OF CONTENTS
Preface.......................................................................................................................................................................... ii
Introduction ................................................................................................................................................................ 1
Chapter I: Vaccine Production ................................................................................................................................ 5
Chapter II: Market Incentives ................................................................................................................................. 9
Are You In or Are You Out .......................................................................................................................... 10
Creating Incentives .......................................................................................................................................... 16
Chapter III: Superbug ............................................................................................................................................ 20
The Black Death .............................................................................................................................................. 20
Pandemics ......................................................................................................................................................... 21
Bioterrorism ...................................................................................................................................................... 23
Chapter IV: Conclusions ....................................................................................................................................... 25
Bibliography ............................................................................................................................................................. 29
Notes ......................................................................................................................................................................... 32
ii
ACKNOWLEDGMENTS
The author wishes to express sincere appreciation to Professor Trost for his assistance in the
preparation of this thesis as well as his dedication to the class. In addition, I want to dedicate this thesis
to all those who have suffered due to vaccines or the lack there-of; we may never have all the answers
but let us build a world where we do right by each other.
“My idea of a better-ordered world is one in which medical discoveries would be free of patents and there will be no profiteering from life and death.”
- The late Prime Minister Indira Gandhi
1
I n t r o d u c t i o n
THE VACCINE MARKET
Vaccines are an integral part of a functioning, productive, and healthy society. Every year
millions of people are vaccinated against various diseases which force manufacturers to face hard
economical and ethical decisions regarding investment and supply. The decision to enter the vaccine
market can be daunting; Investments in research and development (R&D) can pay out big or can
result in nothing at all.
Our vaccine system operates in an atmosphere of constant uncertainty, and fragility. The
vaccine market is entirely dependent upon chicken eggs, a supply that is affected not only by other
markets but a supply that is receptive to disease and death. This nearly century old procedure has been
effective and reliable thus far, however, with diseases such as avian flu, how safe is this supply, and
how far are we willing to extend our faith in this archaic, time-consuming, inefficient method. Within
the market exists the technology and techniques that stem away from such a risky supply. This
technological and modern process is not only more efficient, and more reliable, but ensures us of an
adequate supply of vaccine in times of need; however, vaccine manufactures articulate that this
technology would cost an extreme amount of money – not because the process is more expensive, but
because adopting such technology would incur restructuring plants, or creating entirely new ones to
accommodate the new methodology.
2
In October 2004 Klaus Stoehr, the chief influenza expert at the World Health Organization
(WHO) stated that “There is currently too little momentum in the development of pandemic . . .
vaccines. . .We had three pandemics in the last century and there is no reason to believe there won’t be
one in this century.”H1N1 was that realization, and the market showed us that is was unprepared for
the task at hand – with H1N1 we were lucky, but the next pandemic may be right around the corner.
The trouble we face is a moral one: should we allow our market to fail us simply to make a
profit?
Currently vaccine companies create 300 million flu shots a year, but in a pandemic we could
need billions of doses . . . Vaccines are simply not a lucrative prospect for drug companies,
which can make much higher profits on “blockbuster” drugs. Vaccines are risky: anything
injected in a healthy person can end up doing harm, leading to costly lawsuits and bad press.
Also a pandemic may never hit, so business leaders are reluctant to spend money on new
factories that might never be used. (Erika Check)
From the business perspective, firms are looking out for their own self interest; they must be willing to
invest in products to which there is a healthy return in their investment. The market is highly risky too,
firms face choices that could lead them to success or lead them to failure, making the wrong choice
could set development and production back by months or even years. Within the United States there
exist only four major vaccine manufacturers, similar conditions exist around the developed world.
These vaccine manufacturers primarily operate within their home country, failing to make use of
economies of scale by competing and marketing abroad. Instead of a competitive atmosphere between
firms we witness one that is more like an oligopoly, stifling out competition and smothering
3
possibilities for new entrants into the market. This leaves the world with a “potential market [that] has
been to small and uncertain to encourage the vaccine industry to make large investment in research,
development, and manufacturing of new products.”(National Academy of Sciences). By creating
incentives and reformatting the market we can create a market that is competitive, robust, and just, and
silence the siren of alarm.
In Chapter I the production of vaccines will be explored. I will be discussing how the limited
production capacity of the market is directly correlated with decreasing investments in Research and
Development and how patents limit overall production capacity.
Sellers may be able to identify persons who may benefit from treatment, thus allowing firms to
extract consumer surplus; however, for vaccines info is less available and firms are unwilling to
produce a product with such low returns compared to the therapeutic drug market. This chapter will
therefore too discuss the process of developing influenza vaccine and how and why firms continue to
use inefficient techniques. Ultimately this chapter will assist on shedding light on the production
inadequacies and failure of suppliers within the vaccine market.
Chapter II will pick-up where Chapter I leaves off. I will be introducing a game theoretical
model that explores the rationale behind why firms should not enter the market for vaccines under
patentable conditions as well as free market conditions. Chapter II is appropriately named Incentives,
in that I will be discussing incentives to address the issues presented within the models.
Klaus Stoehr, the chief influenza expert at the WHO stated back in 2004 that “There is
currently too little momentum in the development of pandemic [vaccines] . . . We had three pandemics
in the last century and there is no reason to believe there won’t be one in this century.” Chapter III will
explore such an academic question: What if we experienced a pandemic on a global scale not seen

4
since the years of ore, a pandemic with the infectiousness of H1N1 and the kill rate of the Black
Death. Could the market handle such a demand and once the market finally reacted would it be too
late without governmental interference? I will also briefly touch base on the threat of bioterrorism and
why there is a cause of alarm.
Chapter IV will touch base with overall conclusions of my analysis of the vaccine market, and
address any unanswered questions that may be left beyond this paper. Lastly I will conclude with an
ethical synopsis of the vaccine market and why ignoring our internal ethical and moral understandings
are the ultimate cause for alarm.
5
C h a p t e r I
VACCINE PRODUCTION/SUPPLIERS
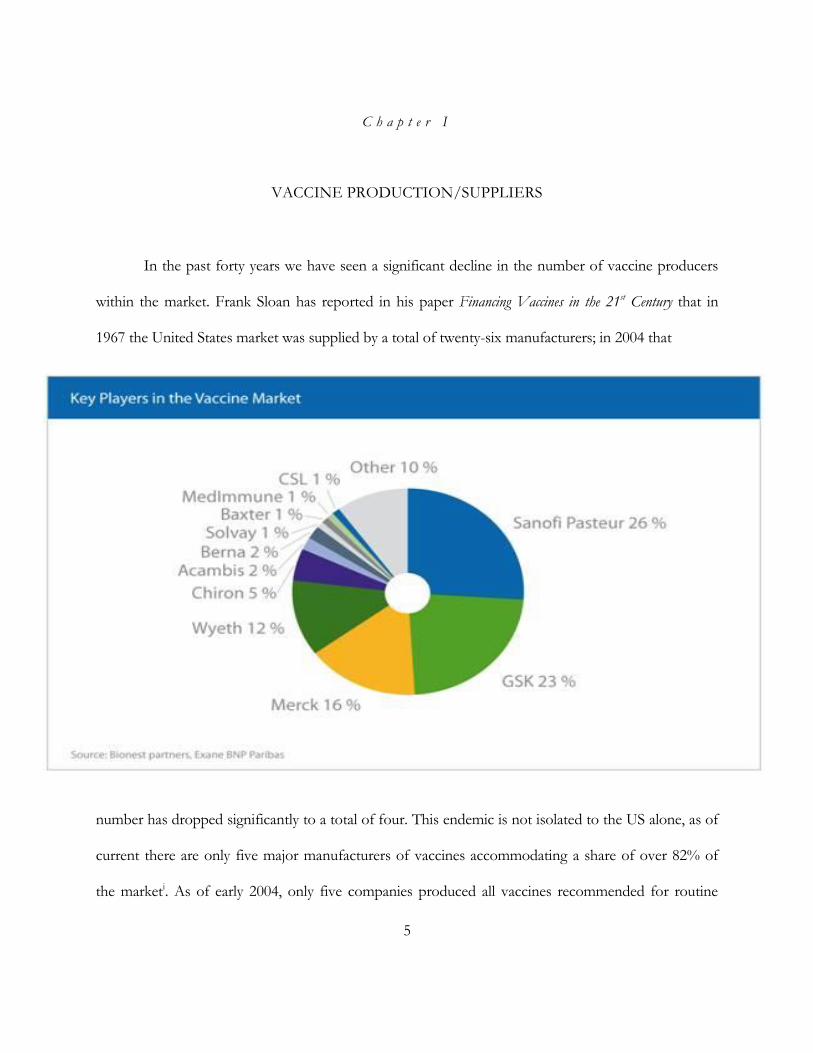
In the past forty years we have seen a significant decline in the number of vaccine producers
within the market. Frank Sloan has reported in his paper Financing Vaccines in the 21st Century that in
1967 the United States market was supplied by a total of twenty-six manufacturers; in 2004 that
number has dropped significantly to a total of four. This endemic is not isolated to the US alone, as of
current there are only five major manufacturers of vaccines accommodating a share of over 82% of
the marketi. As of early 2004, only five companies produced all vaccines recommended for routine
6
vaccination for both children and adults and out of those five companies only three were U.S.-based
firms. Recently the market has experienced unprecedented shortages in eight of the eleven of those
routine vaccines, along with eight major vaccine products produced and manufactured by only one
supplier (Institute of Medicine, 2004). Limited production capacity and the ever obvious trend in
declining suppliers is the cause. In the past decade the U.S. has suffered tremendous shortages of
influenza vaccineii; in the past ten years the U.S. has suffered a shortage nearly fifty-percent of the time.
One of the many variables resulting in firms’ failures to bring an adequate supply to market are the
complications in creating a viable vaccine.
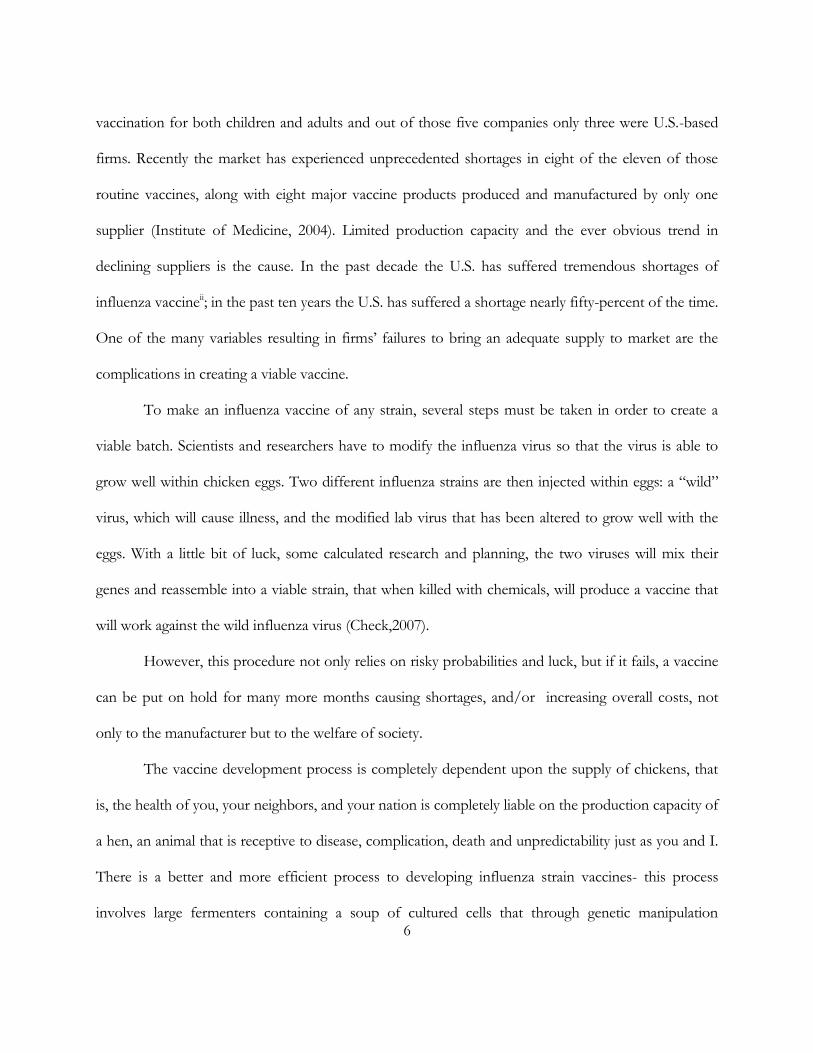
To make an influenza vaccine of any strain, several steps must be taken in order to create a
viable batch. Scientists and researchers have to modify the influenza virus so that the virus is able to
grow well within chicken eggs. Two different influenza strains are then injected within eggs: a “wild”
virus, which will cause illness, and the modified lab virus that has been altered to grow well with the
eggs. With a little bit of luck, some calculated research and planning, the two viruses will mix their
genes and reassemble into a viable strain, that when killed with chemicals, will produce a vaccine that
will work against the wild influenza virus (Check,2007).
However, this procedure not only relies on risky probabilities and luck, but if it fails, a vaccine
can be put on hold for many more months causing shortages, and/or increasing overall costs, not
only to the manufacturer but to the welfare of society.
The vaccine development process is completely dependent upon the supply of chickens, that
is, the health of you, your neighbors, and your nation is completely liable on the production capacity of
a hen, an animal that is receptive to disease, complication, death and unpredictability just as you and I.
There is a better and more efficient process to developing influenza strain vaccines- this process
involves large fermenters containing a soup of cultured cells that through genetic manipulation
7
produce a viable vaccines- however, the manufacturing methods incorporated would force companies
to erect new facilities, invest in new and costly technological expenditures that current manufactures
see as unnecessary for a stream-lined process that has been thus far effective for nearly one-hundred
years. I on the other hand refute manufacturer claims - the efficiency, and more importantly, the gain
in vaccine reliability by investing within these new technologies far outweighs the costs subjected upon
manufacturers, and that in the long run manufacturers would recoup their cost in investments by
ensuring a supply of vaccine that is less prone to production risk, and is more effective in addressing
supply shortages.
When it comes to making vaccines other than influenza some institutes may be more equipped
than others, the problem that many producers face is the patent system. For example, reverse genetics
a procedure for creating vaccines via stitching virus genes into loops of DNA called plasmids, is
patented; therefore, companies that may be better off and more efficient to make a vaccine would
have to pay royalties to the patent holders. Companies are naturally reluctant to do this, thus stalling
the process (103-104).
The main assumption many undertake is that if people value a product more than it costs to
produce, suppliers will serve the need. However, this is not likely to happen with new pharmaceuticals
especially vaccines. Eggs, or shoes differ from pharmaceuticals in two important ways. First, people
who buy shoes gain all the benefits from their use, whereas the benefits of vaccination spill over to
others because vaccines typically interfere with the spread of the disease. Second, whereas the main
expenses involved in producing shoes are raw materials . . . the main cost of producing new [vaccines]
is R&D (Kremer & Glennerster, 31). In his book The Economics of Research and Development in
the Pharmaceutical Industry William Comanor submits validating evidence regarding the inefficiencies
of the production of pharmaceutical drugs: In year 2000 dollars it takes approximately $802 Million in
8
R&D expenditures to create a new vaccine, compared to 1987 where total expenditures per new
vaccine were $237 Million; the difference is fundamental evidence in the direct correlation between the
ever increasing costs of research for new drugs and the declining productivity of pharmaceutical
research.
If the current low participation of producers within the market continues there will be dire
repercussions not only for production but for society in the form of market failures such as
asymmetric information between producers and consumers and supply shocks which can send ripples
through the economic foundations of a country; however developing countries have much more to
lose by the exiting of companies from the market; Developed countries have the luxury of efficient
“non-corrupt” governments, with monopsony power that will ensure a rebound from certain and
inevitable market failures, whereas developing countries have few such luxuries. With such a large
decrease in supply, prices will naturally inflate forcing consumers to exit in said nations. Developing
countries too face another wicked reality: as the total number of producers and research dollars
decrease across the market so too will the R&D dollars towards neglected diseases such as
HIV/AIDS, Malaria, Tuberculosis, etc will be significantly reduced. The National Academy of
Sciences has recently reported that there is insufficient production capacity amongst market
participants; the implications of the continuing trend of firms exiting the market can only end in one
conclusion: If firms find producing vaccines to be unprofitable currently, they are also unlikely to
invest in R&D to develop new vaccines (Sloan & Eesley).
9
C h a p t e r I I
MARKET INCENTIVES
Vaccine production is not the most lucrative or profitable market. Pharmaceutical companies
are unwilling to make the initial investment within the market due to its risky undertaking and an
unsupportive market atmosphere. Therapeutic drugs that aim to prolong/sustain the life of the
inflicted while decreasing comfort and increasing dependence are more profitable than simply curing
the disease. Over the years drug sales pertaining to relieving ailments have increased steadily, whereas
vaccine sales too have been growing but at an insignificant pace when compared to the overall health
care/ Pharmaceutical industry.
In 2008 the top 50 Pharmaceutical companies brought in sales of over $558 billioniii for
prescription drugs alone, whereas the vaccineiv market worldwide took in sales of roughly $18.7 billionv
or less than 2% of the entire market.
As addressed in the previous chapter, we have seen unprecedented decreases of market
participation, productivity, and massive vaccine shortages. The questions we must ask and answer is
why. Why are firms leaving the market, what are the disincentives/ causes behind the exit of firms
from the market, and more importantly what is being done to incentivize firms to invest in R&D,
research into neglected diseases, etc, and lure firms to enter the market for vaccine research,
development and production.
10
Are You In or Are You Out?
Within the market for vaccines lays the dilemma of whether to invest within a vaccine product
or not to invest. That is, when two firms engage/enter the market for a vaccine of which none yet
exist, they are faced with certain questions: Is there a demand for the product? Will the firm make a
profit off the product? Is anyone currently within the market, or planning on entering the market?
Within this hypothetical game we are assuming two pharmaceutical companies with equal
resources, who are deciding whether to enter into the market for a new vaccine. The game will also be
one played with perfect information – each firm will possess knowledge of the others’ intention to
enter or not to enter based on publications, announcements, grants applications, etc. The question we
must answer is, is there a solution to this enter/invest or not enter/not invest game between the two
firms.vi
There can only be one winner within this game, as we know according to patent laws whoever
develops the vaccine first will receive monopoly rights and profits of the product. Developing vaccines
is also not an exact science but a system of trial and error with large cost in R&D and cost also
incurred during clinical trials; therefore I have assigned the success of a vaccine with a probability of
(1-q) where q is the probability of failure. To maintain simplicity, payoffs are straight forward as
follows: If you are the winner of the game you are paid monopoly profits minus costs, if you are the
loser you incur a profit of 0 if you decide not to invest, if you decide to invest however, you will incur
the cost of your R&D and clinical trials, etc. If both firms decide not to invest both will incur a payout
of 0. When both firms invest, they are entering into competition with each other; whoever succeeds in
creating the vaccine first will take the market. Since we have assumed that both firms are equipped
11
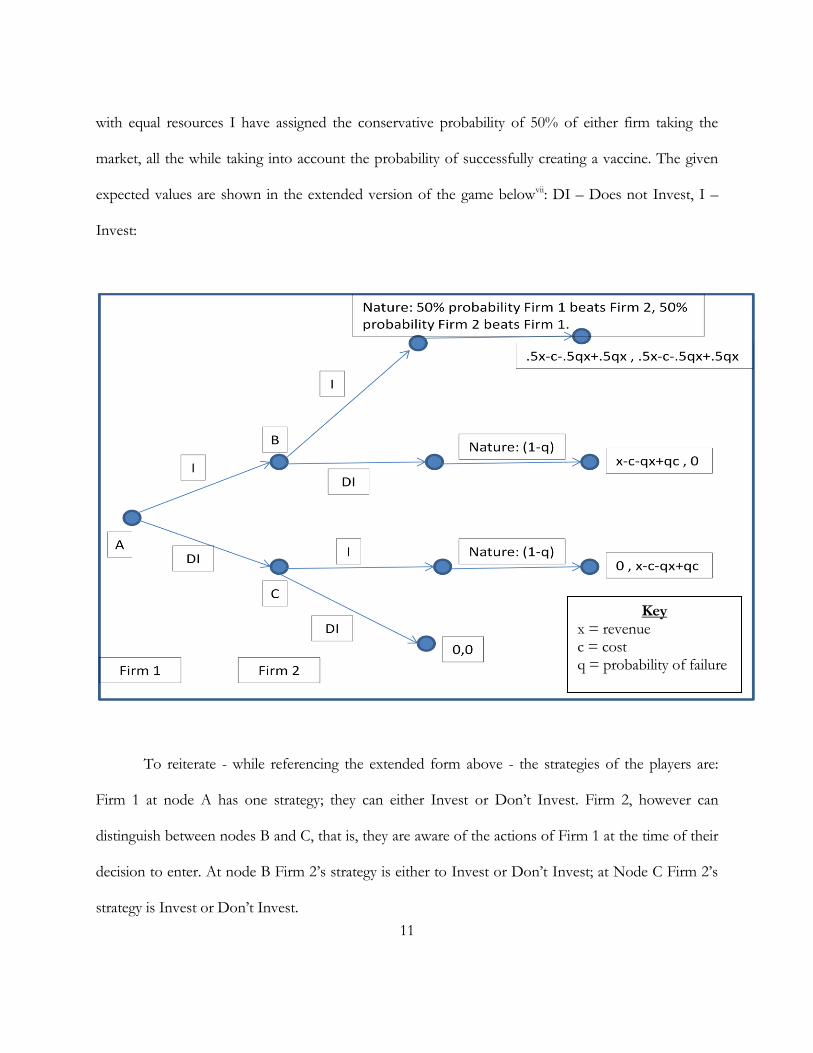
with equal resources I have assigned the conservative probability of 50% of either firm taking the
market, all the while taking into account the probability of successfully creating a vaccine. The given
expected values are shown in the extended version of the game belowvii: DI – Does not Invest, I –
Invest:
To reiterate - while referencing the extended form above - the strategies of the players are:
Firm 1 at node A has one strategy; they can either Invest or Don’t Invest. Firm 2, however can
distinguish between nodes B and C, that is, they are aware of the actions of Firm 1 at the time of their
decision to enter. At node B Firm 2’s strategy is either to Invest or Don’t Invest; at Node C Firm 2’s
strategy is Invest or Don’t Invest.
Key x = revenue c = cost q = probability of failure
12
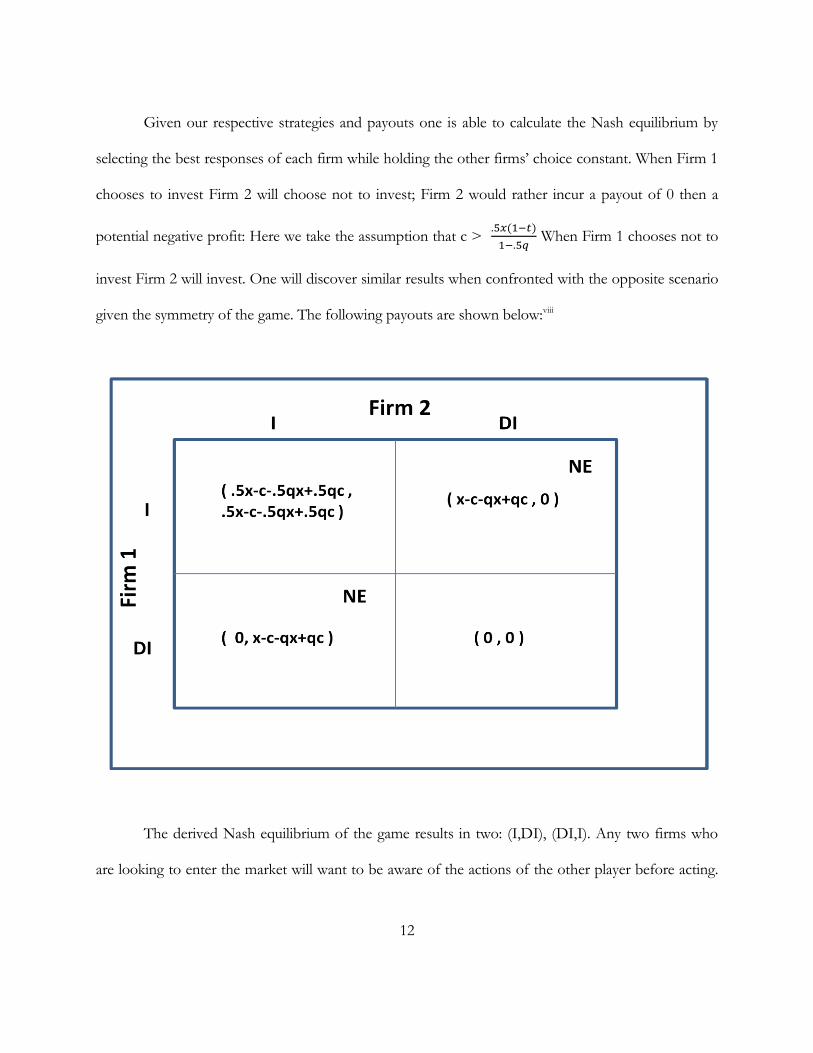
Given our respective strategies and payouts one is able to calculate the Nash equilibrium by
selecting the best responses of each firm while holding the other firms’ choice constant. When Firm 1
chooses to invest Firm 2 will choose not to invest; Firm 2 would rather incur a payout of 0 then a
potential negative profit: Here we take the assumption that c >
When Firm 1 chooses not to
invest Firm 2 will invest. One will discover similar results when confronted with the opposite scenario
given the symmetry of the game. The following payouts are shown below:viii
The derived Nash equilibrium of the game results in two: (I,DI), (DI,I). Any two firms who
are looking to enter the market will want to be aware of the actions of the other player before acting.
13
Firm 2 is at a disadvantage as Firm 1 can steal the market simply by entering the game (First mover
advantage) and deterring Firm 2 from entering, as long as the conditions previously mentioned hold.
Given our two equilibriums, we may be led to believe that either of these equilibriums is
efficient, however this is not the case. In each scenario a firm is essentially pushed out of the market
and deterred from entering. Because of this deterrence, research in various vaccines may be hindered.
It is logical to presume that the more firms working on a vaccine the higher the probability of success
in bringing an effective vaccine to market, when this probability is decreased and success solely relies
on the efforts of one firm society may suffer from negative externalities, including prolonged disease,
decrease in productivity due to illness, etc. These negative externalities translate our equilibriums into
inefficient outcomes.
Now lets explore an example free from all intervention, a pure free market model where a
given firm is producing a vaccine for an infectious disease. Now, suppose the social value for creating
“yoodles” is $1, that is, consumers are willing to spend at most $1 each for a “yoodle”; the
manufacturer for “yoodles” would more than graciously be happy to produce “yoodles” as long as his
cost were less than $1. per “yoodle”. This however is not the case for vaccines. Let us suppose that
one billion people were each willing to pay $50 to be free from “X”- disease. The social value would
then be $50 billion. Now keeping in mind our assumption regarding the absence of any governmental
role in the vaccine industry, incentives for R&D would be insufficient due to the difficulties inherent
in capturing knowledge that comes from commercialization. Suppose, a pharmaceutical company
thought that if it spent $500 million it would have a 10% chance of developing a vaccine for X-disease.
From a societal point of view an investment of $500 million for a 10% chance of generating a return
of 49.5 billion would be a negligible risk compared to the benefits. Nonetheless, the R&D might not
be privately profitable. Suppose the vaccine could be copied and produced for 45 cents a dose.
14
If the original developer tried to sell the vaccine even at marginal cost, 50 cents per dose, the price that
would allow it to recoup its R&D cost, another company would sell less than the 50 cents and capture
the market (Kremer and Glennerster, 32). Given such circumstances even under free market
conditions we can conclude that not even potential entrants to market would make the initial
investment in the first place.
One such failure that the vaccine market faces is what I call the asymmetric-reduction
problem: When a vaccine is introduced to society asymmetric information exist between producers
and consumers. Producers of the vaccine know demand exists for a vaccine, however in normal
conditions not everyone will require a said vaccine, healthy, a less at risk citizens have no need to ask
for a vaccine, although it may be in their self interest to consume, firms have no idea who is at risk or
who it not, or even who has the disease. Consumers on the others hand know if they have the disease
and require vaccination or if they are high at risk and should seek vaccination. Therefore those who
will consume vaccines will either be those infected or those who have a high probability of becoming
infected, either case a small percentage of the total potential market. However, if we take the
summation of the entire actual market (those who will purchase and consume the vaccine) we will see
that that total is less than the summation of those who should be vaccinatedix. The logic behind this
conclusion is rather simplistic: assume the infectious disease is spread via others who are already
infected, those who are infected have the most incentive to become vaccinated followed by those
individuals who are high at risk. Initially some of the infected are vaccinated as their demand to be
cured is higher than those seeking simply to avoid infection, however as more people become
vaccinated the probability of contracting the infectious disease becomes lower, therefore some
individuals who may have classified themselves as high risk individuals drop out of the market. As
more of the infected become vaccinated the probability of infection again decreases and once more
15
those who once considered themselves high at risk reevaluate themselves as not at risk and therefore
drop out. This pattern continues for some time but one ultimate conclusion can be drawn: On a
theoretical level only those infected with an infection shall seek treatment and therefore comprise the
entire market, in reality however we can expect of mix of infected and high risk individuals consuming
the vaccine; none-the-less the entire in the end will be less than that from the beginning.
This dilemma provides disincentives for firms to enter into the vaccine market. With initial
costs in the hundreds of millions to develop and bring to market an effective vaccine it can take over a
decade for companies to recover their R&D costs (Committee on HIV Prevention Strategies in the
United States, CHPSUS). With vaccine development primarily oriented towards diseases and strains
inflicted upon developed countries (CHPSUS) the developing world is hit the hardest by the lack of
incentives and lack of producers within today’s market. Between 1975 and 1997, 1,233 drugs were
licensed worldwide, however only four of those vaccines were developed by private firms for
tropical/neglected diseases of humans (Stigltiz, Edlin, Delong, 54); further, because firms are often
forced to provide their product just slightly above marginal costs it can takes years or decades before
children and adults are treated for preventable diseases within the developed world, for example,
millions of children are left dead due to Haemophilus influenza, it wasn’t however until fourteen years
after the introduction of the vaccine in developed countries that developing countries began receiving
regular doses of the vaccines, yet still fewer than 10% of infants in the world’s poorest seventy-five
countries were routinely receiving vaccination (Berndt, Ernst, Rachel Glennerster, Michael Kremer,
Jean Le, Ruth Levine, Georg Weisaecker, and Heidi Williams, 2007).

16
Creating Incentives
A house without support cannot stand, so too the market without the proper incentives
cannot function and is doomed to fail. Things left unto themselves eventually will fail, this is clearly
evident within the vaccine market: A loss of 20 vaccine producers supplying the U.S. in the past 40
years, many mandatory/recommended vaccines produced by only one manufacturer, the ever
increasing cost of R&D and the ever decreasing productivity of Pharmaceutical firms, not to mention
lack of incentive for entering into research for neglected diseases. Pharmaceutical firms have an
obligation to their investors to produce a product that will generate returns and dividends and
therefore are unlikely to invest time and effort into producing vaccines without some promise of a
reasonable return. Pharmaceutical companies however are often left with daunting risks and ultimately
will be unwilling to make an initial investment, that is where governmental agencies, international
organizations and philanthropic organizations will have to partner with pharmaceutical companies to
produce and support vaccine research (Sherman, 326) for diseases that may not fall in the category as
profit bearing.
Governments have stepped in to correct the market failures that occur within the vaccine
market, for example, to encourage and ensure a steady supply of influenza vaccine for Canada,
Cananda has partnered with firms and has made promises to buy enough vaccine for the country’s
entire population. The U.S. government has made similar deals with firms, however governments are
interested in purchasing products at the lowest possible price in order to maximize tax-payer dollars –
Governments and large international organizations like UNICEF purchase over 50% of all
17
manufactured vaccines, they are therefore able to broker deals to prices just above marginal cost. The
government’s attempt to incentivize in this manner unintentionally provides disincentive for firms, all
the while increasing consumer welfare. Patents are also used to provide incentives for firms to enter
the market and conduct original research, however, a major disadvantage for patents is the large
deadweight losses incurred due to, the nature of patents, authorizing monopoly power (Frank Sloan
and Charles Eesley, 119).
In 1993 the Institute of Medicine Council published the following statement regarding private
sector involvement within the Vaccine Market: “ the private sector alone cannot sustain the costs and
risks associated with the development of most Children’s Vaccine Initiative vaccines, and because the
successful development of vaccines requires an integrated process, the committee recommends that an
entity, tentatively called the National Vaccine Authority, be organized to advance the development,
production, and procurement of new and improved vaccines of limited commercial potential but of
global public health need” (Mitchell, Philopose, and Sanford 1993). This proposal ultimately suggests
that government enter into the research, development, and manufacturing of vaccines that the private
market would otherwise ignore. What is concerning though, is that despite a call for such an institution
Congress has yet to consider such a proposal seriously.
Frank Lichtenberg author of Ensuring the Future Supply of Vaccines offers his solution to the
incentive debate; he argues that a way for policy makers to satisfy the market is to allow vaccines prices
to adjust to market-clearing levels. He further critiques that this approach would reduce government
disincentives for R&D, and perhaps establish incentives for greater private vaccine development and
production. I argue in favor of this implementation, however on a global socialistic scale. This scale
would be equivalent to a ladder per se, where developed countries, that would be at the top, which
tend to be more wealthy are charged prices closer to the market bearing level, therefore allowing
18
manufacturers to recoup their costs more quickly and efficiently. The benefits of this scale is that as
manufacturers recoup their costs and begin making profits they have incentive to expand and lower
costs to reach the widest consumer base as possible in order to maximize profits, this effect would
trickle down to the developing and poorest countries of the world and thus bring prices down closer
and closer to marginal cost.
However, this model is not perfect as it provides no incentives for developing vaccines for
neglected diseases, as vaccines will still be produced for those diseases which are prevalent in the
developed world. Researchers, academics, and economists have other suggestions that will benefit and
incentivize the R&D, and production for neglected diseases: They have offered push programs which
offer R&D tax credits and other monetary awards regardless of whether a viable product is
established; Sloan and Eesley debate the use of a public subsidy disguised in the package of a prize
system, where the developer is rewarded for innovation, as it would be under patents, but the new
product is placed within the public domain where prices are set near marginal cost, avoiding the
deadweight loss that ultimately goes hand in hand with the patent system. Sponsorship programs,
similar to what the Bill and Melinda Gates Foundation provides, may be our best bet. Under a
sponsorship program, sponsors agree to provide monetary support for research and development of
vaccines however two conditions apply, the patent system is null and void, and no monetary dollars
are given to the firm until a viable product is produced. Sponsors can range from individuals, to
international organizations, to philanthropic foundations; sponsorship is similar to an X-prize however
on a large scale. In a successful model sponsorship would incentivize firms by ensuring a market for
their product, sponsors would agree to pay a relatively high price for X amount of vaccine in exchange
for a commitment by the manufacturer to supply additional doses to developing countries in
need(Kremer and Glennerster, 75), essentially upon delivery of a product sponsors would cover the
19
R&D costs’ of the firm, and the firm would be obligated to share its fruits of knowledge with the
market. For a short time however the “sponsored” firm will be able to enjoy monopoly pricing and
profits as competing firms create generic vaccine products, as competitors enter the market the overall
price falls eventually to marginal costs. In this scenario, the sponsors win, the initial producing firms
wins, the market wins and most importantly the people win.
It is wise to note, before concluding this chapter, that no one single way is a solution, but an
effective measure for ensuring the stability of the market will require a cocktail of ingenuity and policy.
And that perhaps is our best option to optimally resolve this magnificent problem.
20
C h a p t e r I I I
SUPERBUGx
We cannot let history be forgotten. Our technology may be more advanced, our understanding
more sophisticated but the threat of pandemic is real. Currently vaccines companies can create over
300 million flu shots a year, but in a pandemic we could need billions of doses (Check). This cause of
alarm can no longer remain an academic debate but be brought to the front as a real element that
jeopardizes our public health and safety.
Black Death
The black death was perhaps the world’s worst pandemic in human history. The plague
dominated and peaked in Europe between 1348 and 1350 however continued to ravage the continent
with frequent recurrences until the late 17th century; it is estimated that anywhere between one third to
two thirds of Europe’s entire population was wiped out due to the onset of the infection. Journals of
residents during these eras report entire towns becoming decimated by the onslaught of this invisible
terror with many towns losing 10%-40% of residents.
Borders were closed off, towns quarantined, entire nations practically coming to economic
stand stills. Jean-Baptiste Colbert a French politician who served as the controller-General of Finances
of France during the 1600’s had the daunting task of choosing between economic activity (a great
concern of his) and the protection of the health of the capital and the surrounding region. . . He chose
21
the latter and succeeded in confining the plague to the northernmost regions of France (Bourdelais,
27).
Today we know a lot more in regards to medicine and spread of infection and disease
compared to our ancestors of Europe, and there is no doubt that their ignorance in the beginning
helped spread and propagate the disease, however there is no question that we too would face a similar
chose as Colbert did during a time of pandemic proportion – economic welfare and pressures of
policy, or health and the lives of billions - as we awaited a cure, a vaccine, a solution. With our mass
transit systems allowing people to travel to every part of the globe every day, and with our ill-equipped
facilities the world would face such proportions as Europe did, however on a much larger and global
scale.
Pandemics
Although the probability of a “killer” Pandemic here and now may be low, it is statistically
inevitable that one will occur in the future. The amount of antibiotics now on the market is staggering.
Our curse is that bacteria and viruses are constantly mutating, and changing with every so many
generations. Antibiotics do not help the situation. These medicines enter a new variable into the
mutation process, and there use can cause adverse results, creating a strain that is resistant to drugs;
thereby increasing the probability of a pandemic.
H1N1 was such a virus that many believed was the Superbug that finally arrived unannounced
to our homes. Its kill rate proved to be less than the annual influenza strain but the rate of infection
was exponential. Erika Check explains that once a pandemic strain is born, such as H1N1, researchers
22
will find themselves in a frantic panic to create a vaccine that is effective against it; and Acting Director
General Michael D. Boyd of the International Federation of Pharmaceutical Manufacturers and
Associations addressed the public by announcing "Our members are better prepared than ever to face
a pandemic influenza threat. Vaccine makers are ready to start producing
novel H1N1vaccines,”xi however, the kind gentleman forgot to mention that they were not prepared,
fore if they were then he could have kindly explained why the market was plagued with research and
development and production problems, that it wasn’t until government stepped in and suspended the
patent and liability laws applicable to Pharmaceutical industries that we began to witness a steady
supply of vaccine. Evidently we witnessed the market fail right before us.
If indeed H1N1 proved to be a pandemic of epic proportions similar to what the black death
was to Europe the world would not have been prepared. Demand would overwhelm the production
capacities of current manufacturers, and millions would be left dead, a global pandemic could reach
over 2 billion people (30% of the world population) and would take 8 months to produce only 900
million doses, assuming research and development is complete. The economic loss too would be
tantalizing, under a pandemic the global economy would suffer a loss of $800 billion a year, or a 2%
loss of global GDPxii.
Under these conditions governments would have no choice but to step-in and act. Such is a
concern of certain policy makers as reflected in the House Bill H.R. 4100, the National Vaccine
Authority Act: this bill if enacted would be established by the U.S. Department of Health and Human
Services and would engage in research, development, and production of vaccines to protect the civilian
population against bioterrorist attacks. The National Vaccine Authority would oversee a government
owned laboratory that would be operated by private contractors to produce vaccines the private sector
23
does not supply(Litchenberg, 129). In a case of a Pandemic whether natural or terroristic this facility
could be quickly converted to research, develop, produce, and distribute vaccines required by the
population.
Bioterrorism
In this modern day bioterrorism is less of an academic roundtable discussion and now of
serious concern.
In the current market, to create a viable vaccine it can take between 10-12 years to develop a
new product and bring it to marketxiii. It can take, however, between 2-3 years to bring a new bio-terror
weapon onto the black-market (National Academy of Sciences,85). This inadequate gap between
vaccine development and bio-weaponry means that our National Security is directly related to our
ability to produce viable vaccines, quickly and efficiently.
The national Academy of Sciences has reported that amongst the four major vaccine
manufacturers, there is insufficient production capacity to keep the citizens of the United States safe in
the event of a bioterrorist attack. They also report that the potential market has been too small, to
encourage the vaccine industry to make large investments needed in research, development and
manufacturing facilities.
In a recent report by the CDC there are over 23 diseases out there that could be used by
terrorist as weapons. Out of those 23 only a small percentage are currently being worked on or exist.
Anthrax is just one of those vaccines that is currently being manufactured, although researchers are
calling for a second generation vaccine that would be more effective in combating the bacteria;
24
however ,there only exist currently one licensed manufacturer for anthrax vaccine, with limited
production capacity due to regulatory restraintsxiv. That is why the DoD underwent an independent
review of their vaccine acquisition program and recommended an integrated approach between DoD
and the vaccine industry, along with a national vaccine production facility that would allow maximal
flexibility and expandable manufacturing capability for the production of various types of vaccines.
This proposal has yet to gain footing in the houses of Congress.
25
C h a p t e r I V
CONCLUSIONS
The non-lucrative nature of vaccines is its largest downfall. From the business point of view it
does not make good-sense to enter into a business with such low returns and high probabilities of
failure. With life-prolonging drugs Pharmaceutical companies ensure a market, they ensure consumer
demand while producing an effective supply. Unlike drugs that create an atmosphere of dependence
between consumer and drug in order to suppress infection or fight infection, vaccines aim at
immunizing a population in hopes of eradicating a disease. Once the disease is eradicated the market
for such a vaccine dries up. Essentially the firms’ product is the markets’ undoing. For example: think
of all the drugs that Pharmaceutical firms produce to combat HIV and the profits that these
companies make off said products, now suppose GSK tomorrow developed a vaccine for HIV/AIDS.
World, public and governmental pressure would force GSK to sell such a product close to marginal
cost, further, a vaccine would make GSK drugs for HIV all but obsolete. Because revenue per drugs
far exceeds revenue per vaccine there is incentive for Pharmaceutical companies not to create vaccines
or discover cures but to discover and create drugs that would essentially let an individual live a fairly
normal, long and dependent life.
There exists the dilemma within today’s society that is symptom focused. We believe if the
symptoms are gone/ suppressed, then we are essentially cured, however this is not the case. As a
society we must reorient ourselves to finding the cure. We must also fundamentally inquire within
ourselves as to whether profiteering from life and death is wrong.
26
The Center for Global Development Advance Market Commitment Working Group reported
that “Scientific breakthroughs are by no means the answer to all the problems. . . But they can play and
have played in the past, a major role in improving the health of those who have the least. Building on
the achievements of the past, this generation of scientist could find ways to prevent malaria and
tuberculosis, stop the spread of HIV/AIDS,” and more, “But such accomplishments are unlikely to
happen without incentives that take such work out of the exclusive realm of altruism and charity, and
place it squarely in the domain of functioning, sustainable markets, creating incentives for the private
sector to bring the full weight of its experience and assets to bear.”
However, the current atmosphere is not viable for producing an effective self-sustaining market,
whether it be for developed countries or developing ones.
Currently the distribution of R&D expenditures across disease groups is uneven, indicating a
possible market failure in the allocation of R&D resources from a global viewpoint (Sloan and Hsieh),
further evidenced by the estimate that nearly 10% of the world’s R&D investment is in finding
solutions for diseases that affect over 90% of the world’s populationxv. If the free market is unwilling
to accommodate the world who are we to rely on: Government, altruistic philanthropic individuals?
Indeed governments of the developed world could implement and nationalize vaccine development
and research but developing countries lack the market, the finances and the ability to sustain such an
operation. In the short-run individuals may be able to incentivize research, however, a market based
on altruism cannot not stand without a solid market foundation. And that is why I argue in favor of
sponsorship programs along with other incentivizing programs such as push and pull funding, our
ultimate goal should not to create a prize system but to develop a “market”.
Externalities arise when people who become infectious do not take account of the costs they
impose on others (Gersovtiz, 469), this negative externality inflicted onto the innocent is a particular
27
market failure facing society, therefore, perhaps a world institution is in order, under the direction of
the U.N., an institution whose primary goal is to remain unbiased and to research and develop the
vaccines that plague our world today; A global initiative to downplay the negative externalities imposed
on society both economic and social and to ensure the health and prosperity of the inhabitants of this
planet.
Indeed a cause of alarm is warranted when addressing the vaccine market. The market is too
small and too ill-prepared to handle an epidemic of mass proportions and the production capacity of
current manufacturers is insufficient. As evidenced back in 2004 the U.S. suffered a massive shortage
of influenza vaccine, this was due to a Chiron plant in the UK that shut down abruptly. In that one
plant shutting down the nation’s annual supply of vaccine was cut by more than 50%. I have
attempted to demonstrate that the vaccine market is on a downward trend, and that trend is not in the
best interest of U.S. citizens, nor the people of the globe. Competition amongst firms is not
theoretically sound and when firms compete they incur higher probabilities of failure and loss, nor may
competing firms for the same product be socially and economically optimal due to duplication,
however history has shown us that competition is feasible: During the cold war competition between
the United States and Russia was at a peak, not only for military dominance but also for vaccines, a
young Russian, Albert Sabine created a vaccine for Polio, a vaccine that was created by the help of
competition (Seytre and Shaffer). Now polio is practically eradicated from the world. The ability to
provide viable incentives is there, the only thing that stands in the way is politics and policy. Yet
politics and policy cannot stand on the side-lines forever, with the increasing threat of bioterrorism
more of a reality than ever the moment to begin research in these diseases is now. There is no doubt
that the world will face a global killer pandemic, the only question is when. Whether we can effectively
28
combat such a disease efficiently and effectively directly depends on the sustainability of our market
today, and what our governments are doing to prepare for such a scenario.
Lastly the ethical question we must answer is, do some people deserve vaccination more than
others and at what costs to the rest of society, are profits enough justification to let millions die due to
preventable disease? If we are truly going to attempt to let the market work if we for a moment accept
that the market is working we may first wish to ponder about these questions, think of our future, and
think of whether it is fundamentally right to profit off the suffering of another.
29
BIBLIOGRAPHY
2013, By. "Global Market for Vaccines Worth $36.3 Billion by 2013 | Reuters." Business &
Financial News, Breaking US & International News | Reuters.com. 24 Jan. 2008. Web. 22
Nov. 2010. <http://www.reuters.com/article/idUS172183 24-Jan-2008 BW20080124>.
Barder, Owen, Michael Kremer, and Heidi Williams. "Advance Market Commitments: How to
Stimulate Investment in Vaccines for Neglected Diseases." The Economists' Voice: Top
Economists Take on Today's Problems. Ed. Joseph E. Stiglitz, Aaron S. Edlin, and Long J.
Bradford. De. New York: Columbia UP, 2008. 54-57. Print.
Bourdelais, Patrice. Epidemics Laid Low: a History of What Happened in Rich Countries.
Baltimore: Johns Hopkins UP, 2006. 11+. Print.
Check, Erika. "The Rush to Develop an Avian Flu Vaccine." Vaccines. Ed. Ken R. Wells. Detroit:
Greenhaven, 2007. Print.
Comanor, William S. "The Economics of Research and Development in the Pharmaceutical
Industry." Pharmaceutical Innovation: Incentives, Competition, and Cost-benefit Analysis
in International Perspective. Ed. Frank A. Sloan and Chee-Ruey Hsieh. Cambridge:
Cambridge UP, 2007. 66+. Print.
Committee on HIV Prevention Strategies in the United States. "The Development of an AIDS
Vaccine Is Not a "Magic Bullet" Solution." AIDS in Developing Countries. Ed. Nancy
Harris. San Diego: Greenhaven, 2003. 56-58. Print.
30
Gersovitz, Mark. "Birth, Recoveries, Vaccinations, and Externalities." Economics for an Imperfect
World: Essays in Honor of Joseph E. Stiglitz. Ed. Bruce Greenwald, Richard Arnott, Ravi
Kanbur, and Barry Nalebuff. Cambridge, MA: MIT, 2003. 469. Print.
Herrick, Devon. "What’s Behind the Flu Vaccine Shortage | Publications | National Center for
Policy Analysis | NCPA." Free-Market Public Policy | National Center for Policy Analysis
| NCPA. 4 Oct. 2004. Web. 22 Oct. 2010. <http://www.ncpa.org/pub/ba493>.
Kremer, Michael, and Rachel Glennerster. Strong Medicine. Princeton, NJ: Princeton UP, 2004.
Print.
Levine, Ruth, Michael Kremer, Alice Albright, and Owen Barder. Making Markets for Vaccines:
Ideas to Action : the Report of the Center for Global Development Advance Market
Commitment Working Group. [Washington, D.C.]: Center for Global Development, 2005.
Print.
Lichtenberg, Frank R. "Ensuring the Future Supply of Vaccines, Is a National Vaccine Authority
the Answer?" Ed. Chee-Ruey Hsieh. Pharmaceutical Innovation: Incentives, Competition,
and Cost-benefit Analysis in International Perspective. Ed. Frank A. Sloan. Cambridge:
Cambridge UP, 2007. Print.
"Market - BUSINESS - AmVac Research - AmVac Research GmbH - Innovative &
Multifunctional Vaccines." HOME - AmVac Research - AmVac Research GmbH -
Innovative & Multifunctional Vaccines. Web. 08 Dec. 2010. <http://www.amvac-
research.de/158.0.html?&L=1>.
The National Academy of Sciences. "The Challenge of Creating Vaccines Against Bioterrorism
Agents." Vaccines. Ed. Ken R. Wells. Detroit: Greenhaven, 2007. Print.
31
Pandemics. Digital image. Http://www.weforum.org/pdf/CSI/Pandemics.pdf. World Economic
Forum. Web. 07 Dec. 2010. <http://www.weforum.org>.
"The Pharma Top 50 - Pharmaceutical Technology." Pharmaceutical Technology -
Pharmaceutical Manufacturing & Development News & Research for Scientists.
PHARMACEUTICAL TECHNOLOGY EUROPE, 1 July 2009. Web. 08 Dec. 2010.
<http://pharmtech.findpharma.com/pharmtech/Business/The-Pharma-Top-
50/ArticleStandard/Article/detail/605705>.
Seytre, Bernard, and Mary Shaffer. "The Competition to Develop an Oral Polio Vaccine."
Vaccines. Ed. Ken R. Wells. Detroit: Greenhaven, 2007. Print.
Sherman, Irwin W. The Elusive Malaria Vaccine: Miracle or Mirage? Washington, DC: ASM,
2009. 326. Print.
Sloan, Frank A., and Charles E. Eesley. "Implementing a Public Subsidy for Vaccines."
Pharmaceutical Innovation: Incentives, Competition, and Cost-benefit Analysis in
International Perspective. Ed. Frank A. Sloan and Chee-Ruey Hsieh. Cambridge:
Cambridge UP, 2007. Print.
Sloan, Frank A., and Chee-Ruey Hsieh. "Introduction." Pharmaceutical Innovation: Incentives,
Competition, and Cost-benefit Analysis in International Perspective. Cambridge:
Cambridge UP, 2007. 7-8. Print.
Web.
Year, By. "Pharmaceutical Companies Are Ready For The H1N1 Influenza Pandemic." Medical
News Today: Health News. Web. 22 Nov. 2010.
<http://www.medicalnewstoday.com/articles/154476.php>.
32
i AmVac Research GmbH, http://www.amvac-research.de/158.0.html?&L=1 ,Accessed 10/22/10
ii The United States suffered shortages of flu vaccine in 2000-2002, 2004, and most recently in 2009.
iiihttp://pharmtech.findpharma.com/pharmtech/Business/The-Pharma-Top-
50/ArticleStandard/Article/detail/605705 accessed 12/06/10
iv We are only considering vaccines for humans.
v http://www.reuters.com/article/idUS172183+24-Jan-2008+BW20080124 , BCC research accessed 10/22/10
vi The assumption of zero governmental interference is also taken into account. The game simply seeks to see
how two firms in the vaccine market would act given perfect competition.
vii Expected values for given payouts: E(DI,DI) = 0
(DI,I) = (0, x- c) with probability of success denoted by Nature (1-q); E(DI,I) = (0) + (1-q)(x-c) = x-c-qx+qc
(I,DI) = because of the symmetry of the game E(I,DI) = x-c-qx+qc
(I,I) = (x-c-qx+qc, -c) or (-c,x-c-qx+qc) with probability of success denoted by Nature (.5); E(I,I) = .5(x-c-
qx+qc) + (.5)(-c) = .5x-c-.5qx+.5qc
viii Note: The strategic form of this game has been compressed in order to show those payouts and strategies
most relevant to the game: If we uncompress we would see Firm 2, the column player with strategies (I,I),
(I,DI), (DI,I), (DI,DI) and Firm 1, row player with strategies (I), (DI). The compressed form that is
represented does not take away from the given actions that Firm 1 and Firm 2 would take given their best
responses.
ix Those infected plus those considered high at risk individuals.
x A microorganism that carries resistance genes and is able to survive exposure to antibiotics. I am also including
within this context a more broad definition that includes viruses that are highly infectious/contagious and are
attributable to a high probability of death.
xi http://www.medicalnewstoday.com/articles/154476.php accessed 10/22/10 xii http://www.weforum.org/pdf/CSI/Pandemics.pdf accessed 12/07/10
xiii Committee on HIV Prevention Strategies in the United States
xiv National Academy of Sciences
xv The report of the Center for Global Development Advance Market Commitment Working Group