Embed Size (px)
Citation preview

1
VALIDATION AND QUALIFICATION
Lizette Caballero, B.S., M.T. (ASCP)Laboratory Manager
Cellular Therapy LaboratoryFlorida Hospital Cancer Institute
Orlando, FL
2
Learning Objectives• Validation of Equipment
– Provide an overview of equipment validation– Outline the components of a validation plan– Provide a specific example of an equipment
validation
• Validation of Process– Provide overview for process validation– Outline the components of a process validation– Provide a specific example of a process validation

3
When do we do it?
• Applies to new or significantly changed equipment or processes that affect donor or patient safety, or the safety, purity or potency of products.
• Examples include:– Equipment used during product processing– Transport procedures, including transport
carrier– New or revised processing procedures

4
Equipment Validation or Qualification
• Phase I– Equipment Installation Qualification (IQ)
• Identify the equipment• Installation/Maintenance/Calibration
requirements verified with Biomed• SOP written to include maintenance /calibration
requirements• Equipment added to Preventive maintenance
list• Supply vendor qualification check completed• Supplies added to order list• Individual(s) responsible for completing this
phase

5
Equipment Validation or Qualification
Validation Checklist Instrument: _____________________ SN: _________________
Directions: Initial each item as it is completed. Initials/Date Checklist Item
Equipment Installation Qualification (IQ) Identify Equipment
Installation / Maintenance / Calibration requirements verified with Biomed
SOP Written SOP includes maintenance / calibration requirements Equipment added to PM list Supply vendor qualification check completed Supplies added to order list
IQ validation plan completed Operation Qualification (OQ)
Operational variables / critical control points identified SOP(s) written SOP specifies expected outcomes Training and competency records completed
OQ validation plan completed Performance Qualification (PQ)
Product performance (specifications / outcome) identified Monitoring process in place SOP written SOP includes tolerance limits and action for non-conformities PQ validation plan completed

6
Equipment Validation or Qualification
• Phase II– Operation Qualification (OQ)
• Operational Variable/Critical control points identified
• Does the instrument function as described by manufacturer?
• SOP written• SOP specifies expected outcomes• Training and competency records completed• Individual(s) responsible for completing this
phase

7
Equipment Validation or QualificationValidation Checklist
Instrument: _____________________ SN: _________________
Directions: Initial each item as it is completed. Initials/Date Checklist Item
Equipment Installation Qualification (IQ) Identify Equipment
Installation / Maintenance / Calibration requirements verified with Biomed
SOP Written SOP includes maintenance / calibration requirements Equipment added to PM list Supply vendor qualification check completed Supplies added to order list
IQ validation plan completed Operation Qualification (OQ)
Operational variables / critical control points identified SOP(s) written SOP specifies expected outcomes Training and competency records completed
OQ validation plan completed Performance Qualification (PQ)
Product performance (specifications / outcome) identified Monitoring process in place SOP written SOP includes tolerance limits and action for non-conformities PQ validation plan completed
8
Equipment Validation or Qualification
• Phase III– Performance Qualification
• Does the equipment function correctly and consistently for the intended application (Mock products)
• Monitoring process in place• SOP written
9
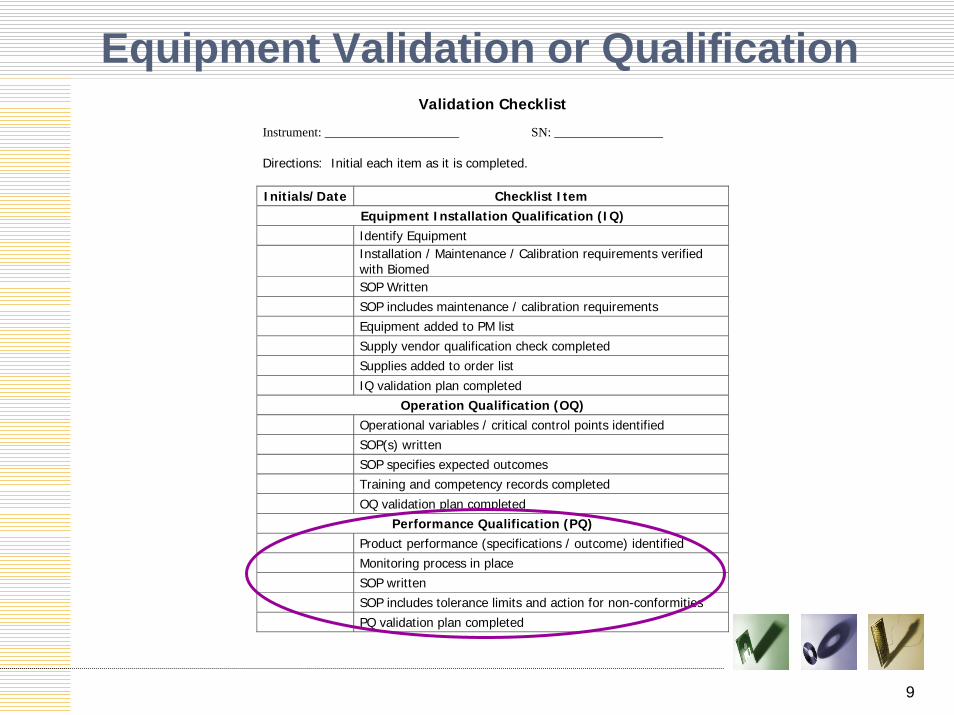
Equipment Validation or QualificationValidation Checklist
Instrument: _____________________ SN: _________________
Directions: Initial each item as it is completed. Initials/Date Checklist Item
Equipment Installation Qualification (IQ) Identify Equipment
Installation / Maintenance / Calibration requirements verified with Biomed
SOP Written SOP includes maintenance / calibration requirements Equipment added to PM list Supply vendor qualification check completed Supplies added to order list
IQ validation plan completed Operation Qualification (OQ)
Operational variables / critical control points identified SOP(s) written SOP specifies expected outcomes Training and competency records completed
OQ validation plan completed Performance Qualification (PQ)
Product performance (specifications / outcome) identified Monitoring process in place SOP written SOP includes tolerance limits and action for non-conformities PQ validation plan completed

10
Equipment Validation or Qualification
• Example of Equipment Validation-Steps to follow:– Identify equipment used to be implemented
or improved.
– Select equipment and determine which elements require validation or qualification.
– Write an SOP according to procedure
11
Writing The Validation Plan• Validation Title
• Assign Validation Number
• Type of Validation (IQ, OQ or PQ)
• Purpose of the Validation
• System Description- Define the scope or beginning and ending steps of the validation. Include identification of equipment.
12
Example of Control Rate Freezer Validation
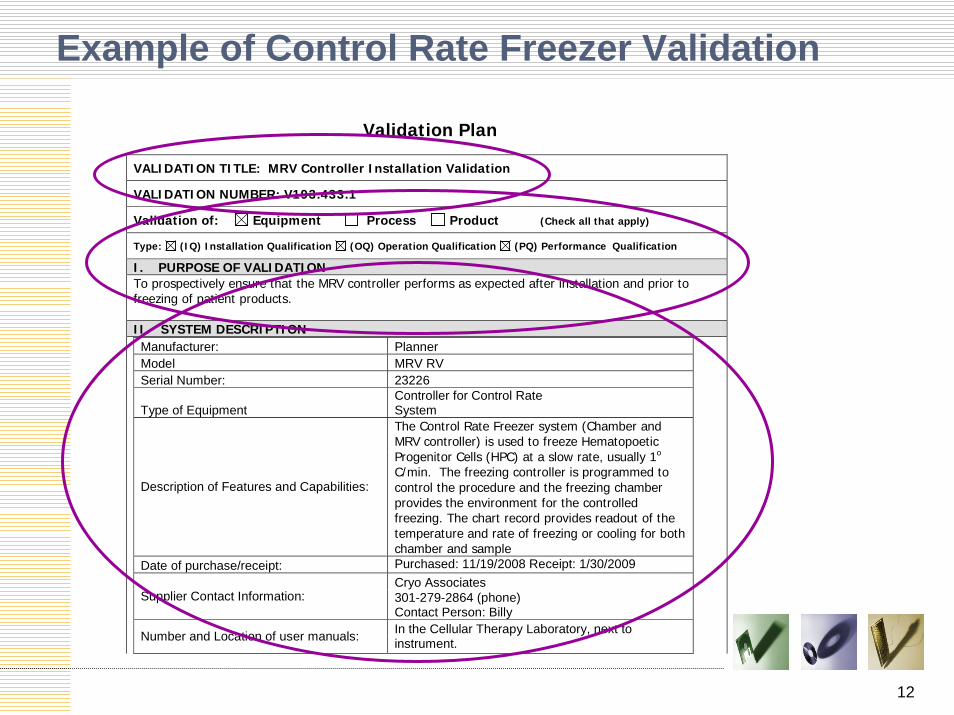
Validation Plan
VALIDATION TITLE: MRV Controller Installation Validation
VALIDATION NUMBER: V193.433.1
Validation of: Equipment Process Product (Check all that apply)
Type: (IQ) Installation Qualification (OQ) Operation Qualification (PQ) Performance Qualification
I. PURPOSE OF VALIDATION To prospectively ensure that the MRV controller performs as expected after installation and prior to freezing of patient products. II. SYSTEM DESCRIPTION
Manufacturer: Planner Model MRV RV Serial Number: 23226
Type of Equipment Controller for Control Rate System
Description of Features and Capabilities:
The Control Rate Freezer system (Chamber and MRV controller) is used to freeze Hematopoetic Progenitor Cells (HPC) at a slow rate, usually 1o C/min. The freezing controller is programmed to control the procedure and the freezing chamber provides the environment for the controlled freezing. The chart record provides readout of the temperature and rate of freezing or cooling for both chamber and sample
Date of purchase/receipt: Purchased: 11/19/2008 Receipt: 1/30/2009 Cryo Associates
Supplier Contact Information: 301-279-2864 (phone) Contact Person: Billy
Number and Location of user manuals: In the Cellular Therapy Laboratory, next to instrument.

13
Equipment Validation or Qualification
• Responsibility assignment
• List of SOPs, personnel, equipment and supplies required:– Include SOPs for operation, maintenance,
quality control and supplies if required– Review current SOPs and list SOPs
requiring revision– List all equipment used in validation– List supplies- including labels and training
forms
14
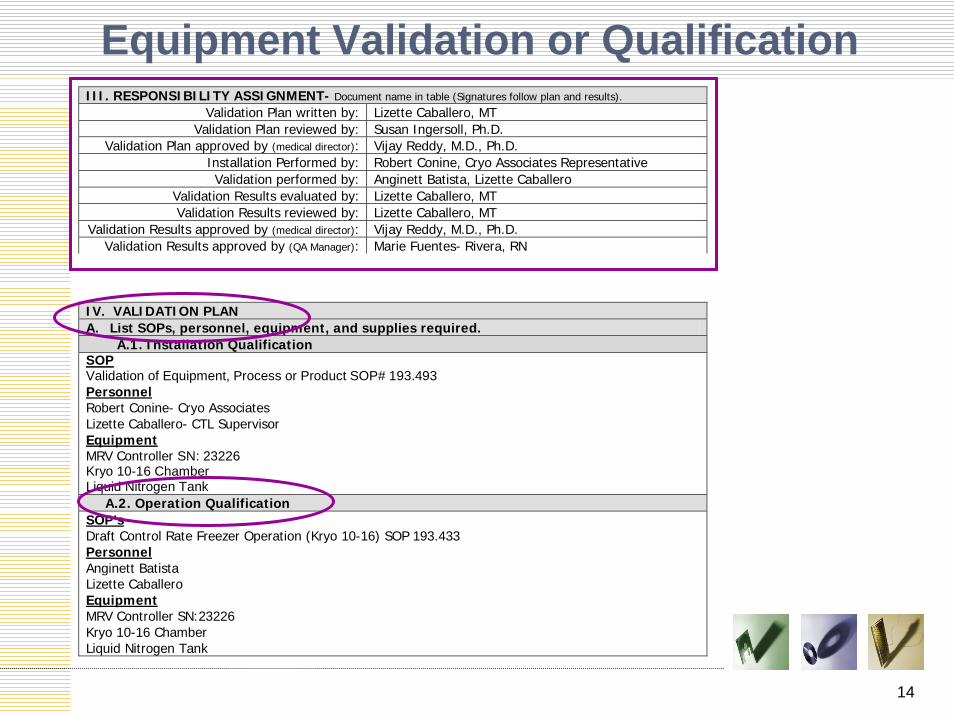
Equipment Validation or QualificationIII. RESPONSIBILITY ASSIGNMENT- Document name in table (Signatures follow plan and results).
Validation Plan written by: Lizette Caballero, MT Validation Plan reviewed by: Susan Ingersoll, Ph.D.
Validation Plan approved by (medical director): Vijay Reddy, M.D., Ph.D. Installation Performed by: Robert Conine, Cryo Associates Representative Validation performed by: Anginett Batista, Lizette Caballero
Validation Results evaluated by: Lizette Caballero, MT Validation Results reviewed by: Lizette Caballero, MT
Validation Results approved by (medical director): Vijay Reddy, M.D., Ph.D. Validation Results approved by (QA Manager): Marie Fuentes- Rivera, RN
IV. VALIDATION PLAN A. List SOPs, personnel, equipment, and supplies required. A.1. Installation Qualification SOP Validation of Equipment, Process or Product SOP# 193.493 Personnel Robert Conine- Cryo Associates Lizette Caballero- CTL Supervisor Equipment MRV Controller SN: 23226 Kryo 10-16 Chamber Liquid Nitrogen Tank A.2. Operation Qualification SOP’s Draft Control Rate Freezer Operation (Kryo 10-16) SOP 193.433 Personnel Anginett Batista Lizette Caballero Equipment MRV Controller SN:23226 Kryo 10-16 Chamber Liquid Nitrogen Tank

15
Equipment Validation or Qualification
A.3. Performance Qualification SOP’s Draft Control Rate Freezer Operation (Kryo 10-16) SOP 193.433 HPC Cryopreservation With or Without Volume Depletion SOP 193.432 Viability Test Procedure SOP 193.406 Personnel Anginett Batista Lizette Caballero Equipment MRV Controller SN:23226 Kryo 10-16 Chamber Kryo 10-16 Probe Liquid Nitrogen Tank Cell-Dyn 1700 Beckman Centrifuge Supplies and Reagents Cryovials Plasma-Lyte A DMSO EDTA Tubes Peripheral Blood from donor Pipet 12X75 Tubes Tips Trypan Blue Hemacytometer

16
Equipment Validation or Qualification
• Establish the number of test samples required for validation– This may be determined by the manufacturer or
regulations, but in any case must be adequate to assure a high degree of confidence in the validation results (for most cases no less than 3 samples)
• Establish testing conditions– Step by step directions to perform validation– Consult with department director/designee or
regulatory specialist

17
Equipment Validation or Qualification
A. Establish the number of test samples required. B.1. Installation Qualification Not applicable B.2. Operation Qualification One test run will be performed with the freezer empty to ensure that the freezer runs properly. B.3. Performance Qualification Three test runs will be performed using conditions similar to a stem cell product prior to using the freezer to cryopreserve any patient products and 20 patient products will be prospectively analyzed to ensure that the freezer is working properly after installation.
C. Establish testing conditions (Step-by-step directions for validation.) C.1. Installation Qualification
1. Identify Equipment 2. Check SN and add to Bio Med Surveillance program 3. Check SOP for changes if applicable 4. Get completed IQ paperwork from Cryo Associate Representative
C.2. Operation Qualification
1. Program new controller using program described on Draft SOP 193.433 Control Rate Freezer Operation.
2. One test run will be performed with the freezer empty to ensure that the freezer runs properly. The printed graph will be reviewed for accuracy and reproducibility of cryopreservation program.
3. Perform personnel training

18
Equipment Validation or Qualification C.3. Performance Qualification Three test runs will be performed prior to using the freezer to cryopreserve any patient products and 20 patient products will be prospectively analyzed to ensure that the freezer is working properly after installation. Part I. Perform three test runs following this procedure:
A. Collect peripheral blood using 5 EDTA tubes from a donor. B. Prepare a buffy coat with the EDTA blood sample by centrifuging for 5 minutes at 1000
RPM’s. C. Save red cells and plasma. D. Label two cryovials with: Donor’s name, Date of testing, test sample number. E. Make a hole in one of the cryovial’s lid to allow chamber probe placement. F. Using a 12 X 75 plastic tube mix:
1. buffy coat cells from step B. 2. 0.4ml plasma from step C. 3. 0.4mlPlasma-Lyte A 4. 0.2ml DMSO
G. Run WBC (using SOP# 193.455 “Cell-Dyn Analyzer Operation” and viability using SOP# 193.406 “Viability Test procedure”)
H. Transfer mix from step F to 2 cryovials from step D (1.0ml each). I. Insert Chamber probe trough hole in lid of cryiovial containing cells and freezing media. J. Place both cryovials inside chamber K. Start cryopreservation procedure following SOP 193.433 “Control Rate Freezer Operation”. L. Move sample without probe to Liquid Nitrogen Tank. Discard 2nd cryovial (the one with the hole
on the lid). M. Save print out of cryopreservation graph. N. Repeat steps 1-10 using two more donors. O. Keep cryovial for at least 24 hours before testing. P. After 24 hrs thaw cryovial using waterbath and perform:
1. Viability test 2. WBC counts
Part II. Collect the following data from 20 consecutive products:
A. WBC counts pre and post. B. Viability post thaw. C. ANC and PLT engraftment.

19
Equipment Validation or Qualification
• List of data/records to be collected Examples include:– New or revised SOPs, labels and forms
– Training and competency records
– Checklists
– Quality Control and outcome measurements

20
Equipment Validation or Qualification
C. Determine data/records to be collected. D.1. Installation Qualification
1. When and where received. 2. Condition upon receipt. 3. Installation paperwork by Cryo Associates representative to include: start up, self checks,
calibration, etc. 4. Sticker provided by Bio Med with assigned ESN number.
D.2. Operation Qualification 1. After mock run the print out of graph will be reviewed and saved.
D.3. Performance Qualification 1. The following will be checked for acceptable performance for Part I and II :
a. Viability post thaw b. WBC counts pre and post thawed c. ANC and PLT Engraftment for products from 20 patients.
2. Prepare table with Pre and Post values. 3. Prepare graphs to show results.

21
Equipment Validation or Qualification
• Establish Acceptance criteria for each data/record collected– Must be defined and measurable
• List of references
• Validation Plan Signatures
22
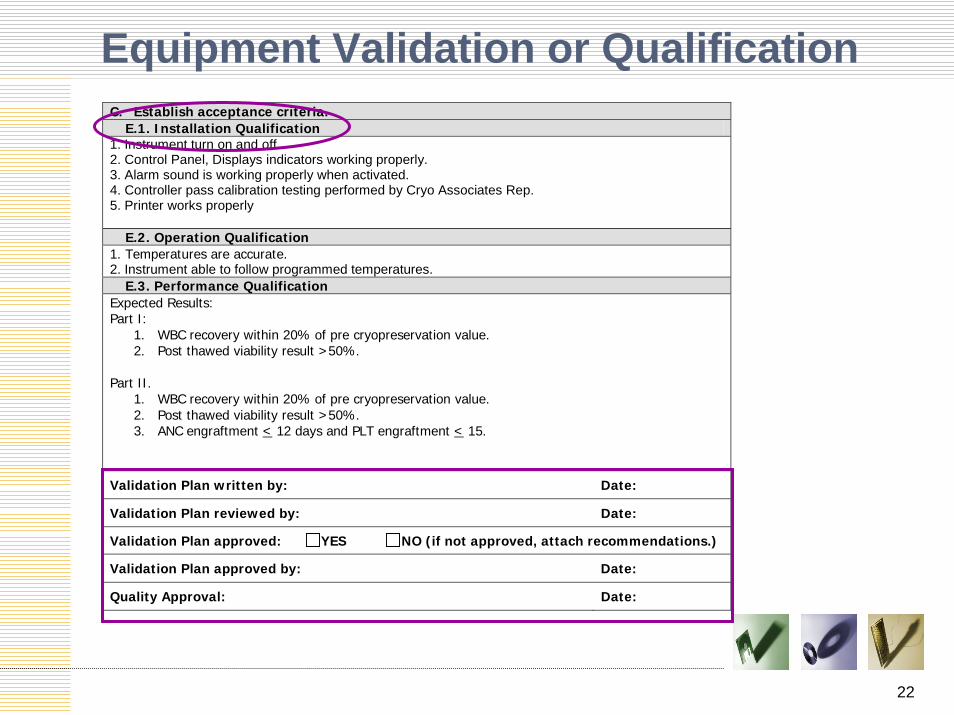
Equipment Validation or QualificationC. Establish acceptance criteria. E.1. Installation Qualification 1. Instrument turn on and off. 2. Control Panel, Displays indicators working properly. 3. Alarm sound is working properly when activated. 4. Controller pass calibration testing performed by Cryo Associates Rep. 5. Printer works properly E.2. Operation Qualification 1. Temperatures are accurate. 2. Instrument able to follow programmed temperatures. E.3. Performance Qualification Expected Results: Part I:
1. WBC recovery within 20% of pre cryopreservation value. 2. Post thawed viability result >50%.
Part II.
1. WBC recovery within 20% of pre cryopreservation value. 2. Post thawed viability result >50%. 3. ANC engraftment < 12 days and PLT engraftment < 15.
Validation Plan written by: Date:
Validation Plan reviewed by: Date:
Validation Plan approved: YES NO (if not approved, attach recommendations.)
Validation Plan approved by: Date:
Quality Approval: Date:

23
Validation Results
DATE(S) OF VALIDATION:
VI. VALIDATION RESULTS A. List SOPs, personnel, equipment, supplies, or procedure steps that deviated from or
were added to original validation plan. State reason for change and document approval of change.
B. Record the number of test samples used. C. Record data/records collected. (Attach separate sheet or data-collection forms if
necessary.) VII. CONCLUSION A. Validation data evaluation and determination of acceptance. Data must meet pre-determined acceptance criteria. B. Comments/Actions. VIII. VALIDATION RESULTS SIGNATURES
Validation performed by: Date:
Validation results evaluated by: Date:
Validation reviewed by: Date:
Validation Results approved: YES NO (if not approved, attach revised plan.)
Medical Director Approval: Date:
Quality Approval: Date:
24
FDA Guidance for Industry Process Validation: General Principles and Practices
• Process validation is defined as the collection and evaluation of data, from the process design stage throughout production, which establishes scientific evidence that a process is capable of consistently delivering quality products
• Process validation activities:– Process Design: The commercial process is defined during
this stage based on knowledge gained through development and scale-up activities
– Process Qualification: During this stage, the process design is confirmed as being capable of reproducible commercial manufacturing
– Continued Process Verification: Ongoing assurance is gained during routine production that the process remains in a state of control

25
Example of Process Validation
• Validation of change in sampling for bacterial and fungal culturesCurrent process is to draw 0.2ml of final product (post processing) and 2.8 ml of concurrent plasma. Then Bacterial and Fungal culture bottles are inoculated with 1.5ml of mixture in each bottle.
We want to change this process to be able to test a representative specimen of the cryopreserved product by collecting 3.5 ml of freezing media (Plasma-Lyte A, concurrent plasma and DMSO) and mix with final product prior to inoculation of culture bottles.

26
Process Validation
• Validation Title: Validation of Sample to be Used for Microbial and Fungal Cultures
• Purpose of Validation: To determine if the addition of DMSO to the Microbial and Fungal Culture inhibits the growth of contaminants
• System Description: HPC, aphereis products are tested for microbial and fungal contamination. This process is used to determine if the HPC, apheresis product is contaminated during the cryopreservation process or apheresis processThe cultures will grow under the proper conditions in the presence of 20% or 10% DMSO

27
Process Validation
• Validation Plan: List of SOPs, personnel, equipment and supplies to be used during validation
• Establish the number of test samples required: – Three independent test runs are required to assure that the
addition of DMSO to the Microbial and Fungal Cultures do not inhibit the growth. If the results of the three independent tests are identical then the results will be considered acceptable; if not then 2 more independent experiments will be performed

28
Process Validation• Establish Testing Conditions:
– Preparation of the Inoculums (Staphylococcus epidermidis and Candida albicans)
• Dilute each culture to 0.5 O.D. Dilute the bacteria with sterilesaline and the fungus with sterile water. This 0.5 dilution represents approximately 108 CFU/ml
• Dilute 1:100 to give 106 CFU/ml• Dilute to 3 X 103 CFU/ml by adding 3ul of the 108 dilution to 1
ml of diluent
– Label 4 BACT Myco/F-Lytic and PEDS PLUS/F bottles with date, Experiment # and: 20%, 10%, No DMSO, Negative Control
– Collect 4 tubes of blood in ACD
– Spin 3 tubes at 3000RPM for 10 minutes

29
Process Validation• Draw up 3ml of the remaining blood in 3cc syringe
and inoculate the negative control bottles with 1.5ml of blood
• Take off 3ml of the remaining blood and place 1.5ml each into two sterile tubes– Spike one tube with 75 CFU of Staphylococcus epidermidis
(25ul of the 3 X 103 CFU/ml dilution of each organism)– Spike the other tube with Candida albicans
• This result in a bottle being inoculated with 10 CFU of the appropriate organism
30
Process Validation• Make up freezing media using supernatant
plasma, plasma Lyte A and DMSO
• Prepare test samples for Bacteria and Fungal organism– 20% DMSO Bacteria Test sample– 10% DMSO Bacteria test Sample– No DMSO Bacteria Test Sample
• Inoculate bottles with each sample (bacterial and fungal)

31
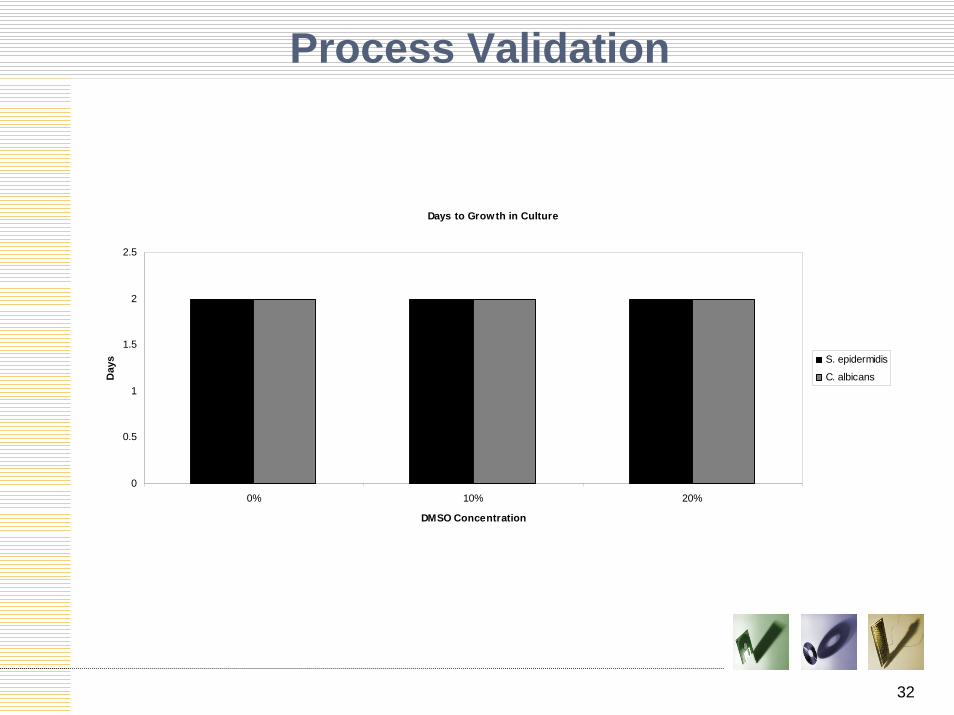
Process Validation• Data to be Collected: reports of growth from
both bacterial and fungal cultures
• Expected Results: – The negative control will no grow any microbial or
fungal culture– The No DMSO control will grow both bacteria and
fungus– The 10% and 20% DMSO test samples will grow
the bacteria and fungus the blood was inoculated with.
32
Process Validation
Days to Growth in Culture
0
0.5
1
1.5
2
2.5
0% 10% 20%
DMSO Concentration
Day
s S. epidermidis
C. albicans
33
Process Validation
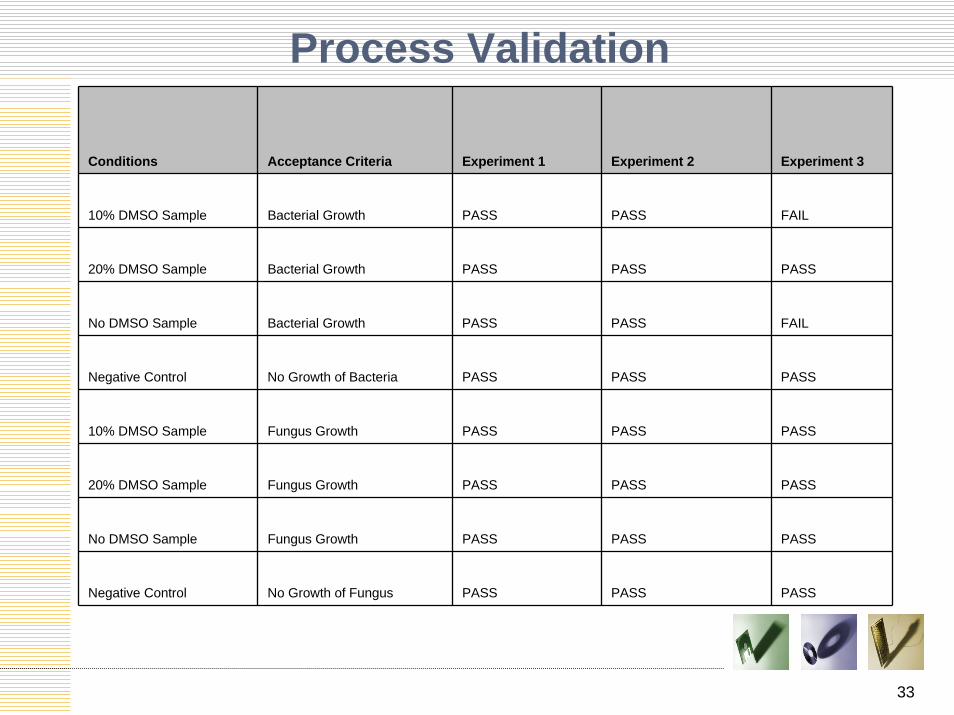
Conditions Acceptance Criteria Experiment 1 Experiment 2 Experiment 3
10% DMSO Sample Bacterial Growth PASS PASS FAIL
20% DMSO Sample Bacterial Growth PASS PASS PASS
No DMSO Sample Bacterial Growth PASS PASS FAIL
Negative Control No Growth of Bacteria PASS PASS PASS
10% DMSO Sample Fungus Growth PASS PASS PASS
20% DMSO Sample Fungus Growth PASS PASS PASS
No DMSO Sample Fungus Growth PASS PASS PASS
Negative Control No Growth of Fungus PASS PASS PASS
34
Process Validation
• Acceptance Criteria: If the 20% DMSO is deemed acceptable then 20% DMSO will be added to the micro cultures mix with the product during future HPC processing
• Validation Data Evaluation and Determination of Acceptance: We have shown that the addition of 20% DMSO to the sample that is used for the inoculation of the microbiology culture bottles does not inhibit growth. Therefore is acceptable to add freeze media, containing DMSO, to the culture inocolum
35
Summary• Perform validation according to
Validation Plan• Data/records evaluation and
determination of acceptance must meet pre-determined test criteria
• Ensure new or revised SOPs, forms or labels are in place for use
• Ensure completion of training and competency records
• Ensure ongoing monitoring is in place

36
Contact InformationLizette CaballeroMT(ASCP)2501 North Orange Ave Ste 786Orlando, FL [email protected]

37





























