Embed Size (px)
Citation preview

923
Plasma cortisol levels during dexamethasone adrenal suppression.
Hydrocortisone was administered as 125 mg in rectal foam (n 6, solidline) or 20 mg orally (n = 2, broken line). Horizontal broken lines normalrange. Mean and SD shown.
was administered rectally. The patients then lay on a bed or sat in acomfortable chair until the end of the study. The foam was retainedfor at least 6 h by all patients. Blood samples for cortisol estimationwere withdrawn from the cannula for up to 6 h. In 2 of the patients,dexamethasone suppression was continued for a further 2 days andblood samples were taken at the same times as on the first day. Onthe second day, no other form of steroid was given because theobject was to confirm adrenal suppression throughout the 6 h. Onthe third day, these 2 patients received an oral dose of 20 mghydrocortisone acetate at 0900.The mean values for hydrocortisone absorption are shown in the
figure. Plasma cortisol levels increased in all 6 volunteers after rectalfoam and exceeded the lower limit of normal in all of the 2, 4, and6 h samples. In every case, the peak was in the 4 h sample and rangedfrom 225 to 1020 nmol/1. The absorption profile was similar for allpatients. The two subjects who also had samples taken duringdexamethasone suppression alone maintained endogenous cortisollevels below 60 nmol/1 throughout the 6 h period of study.
Systemic absorption from 125 mg of hydrocortisone in rectalfoam was less than that from a 20 mg oral dose (figure).Nevertheless, use of rectal foam does result in a range of
physiological cortisol levels not dissimilar to those obtained after theoral dose that is typically used in maintenance therapy for adrenalfailure.
Clinicians should be aware of the potential for adrenal
suppression and steroid adverse effects after hydrocortisone rectalfoam, particularly if patients are using the foam chronically. Themanufacturers have taken immediate steps to amend the
promotional material and data sheet.
Gastroenterology Unit,Royal Hallamshire Hospital,Sheffield S10 2JF
P. A. CANNC. D. HOLDSWORTH
1. Ruddell WSJ, Dickinson RJ, Dixon MF, Axon ATR. Treatment of distal ulcerativecolitis in relapse: Comparison of hydrocortisone enemas and rectal hydrocortisonefoam. Gut 1980; 21: 885-89.
2. Somerville KW, Langman MJS, Kane SP, et al. Effect of treatment on symptoms andquality of life in patients with ulcerative colitis: Comparative tnal of hydrocortisoneacetate foam and prednisolone 21-phosphate enemas. Br Med J 1985; 291: 866.
3. Farmer RG, Schumacher OP. Treatment of ulcerative colitis with hydrocortisoneenemas: Relationship of hydrocortisone absorption, adrenal suppression andclinical response. Dis Colon Rectum 1970; 13: 355-61.
DURAL SINUS THROMBOSIS
SIR,-Your Jan 24 editorial states that: "Anticoagulation is notrecommended for other forms [other than cavernous sinus
thrombosis] of dural sinus thrombosis and should be used only aftercareful consideration and exclusion of cortical venous infarction....The mortality of superior sagittal sinus thrombosis (78 %) must stillbe considered high".
These statements do not correspond to our experience ofcerebral venous thrombosis (CVT). Before the introduction ofangiography, CVT was diagnosed at necropsy and was thereforethought to be usually fatal. In early angiographic seriesl2 the casefatality rate was 30-50 %, but in later series3,4 it was between 25%and 30%, and in a series of 38 consecutive cases it was only 10%.5Several reasons may explain this decrease, the main one probablybeing that it is now possible to diagnose "benign" forms of CVTwith few symptoms and spontaneous recovery. Another reason isthat septic thrombosis has, since the use of antibiotics, become bothfar less frequent (4/38 in our series’) and severe.The use of anticoagulants in CVT remains controversial. They
are usually considered dangerous because the promotehaemorrhage into an already haemorrhagic infarct. However, insome reports, a considerable improvement was observed just afterthe initiation of heparin,5,6 and in our series of 23 heparin-treatedpatients there were no deaths, and 19 patients recovered
completely.5 It therefore seems that, in the vast majority of patients,anticoagulants are not harmful, and that, in some, they may belife-saving. Although in CVT anticoagulants do carry a risk ofincreasing intracranial haemorrhage, this risk is probably very lowand the benefits outweigh the dangers.
Neurology Clinic,Hôpital de la Salpétrière,75651 Paris, France MARIE-GERMAINE BOUSSER
1. Krayenbuhl HA. Cerebral venous and sinus thrombosis. Clin Neurosurg 1967; 14:1-24.
2. Weber G. Zerebrale venen und sinus thrombosen. Schweiz Arch Neurol Psychiat 1958;82: 320-44.
3. Bansal BC, Gupta RR, Prakash C. Stroke during pregnancy and puerperium in youngfemales below the age of 40 years as a result of cerebral venous/venous sinusthrombosis. Jpn Heart J 1980; 21: 171-83
4. Rousseaux P, Bernard MH, Scharpereel B, Guyot JF. Thrombose des sinus vemeuxintra craniens (à propos de 22 cas). Neurochirurgie 1978; 24: 2-6.
5. Bousser M-G, Chiras J, Sauron B, Bories J, Castaigne P. Cerebral venous thrombosis:a review of 38 cases. Stroke 1985; 16: 199-213.
6. Fairbum B. Intracranial venous thrombosis complicating oral contraception:Treatment by anticoagulant drugs. Br Med J 1973; ii: 647
VALPROATE INHIBITION OF UREA SYNTHESIS
SiR,—Dr Kamoun and Dr Rabier (Jan 3, p 48) suggest that thehyperammonaemia and inhibited urea synthesis observed after theadministration of valproatel may be attributed to reduced synthesisof argininosuccinate.
Studies using similar in-vitro preparations or bolus adminis-tration of valproate have identified widespread metabolic effects onthe liver and kidney.2-5 These techniques are powerful and valuablein the detection of such effects but the importance of the findingsmust eventually be tested in experiments with replicate clinicaltherapeutic regimens. Factors which may cause discrepancybetween the results of the different approaches include the
biochemical effects of the many metabolites of valproate, which willnot be present in vitro, and the availability of acetyl-CoA, whichmay be limiting in vitro but not in the intact organism.
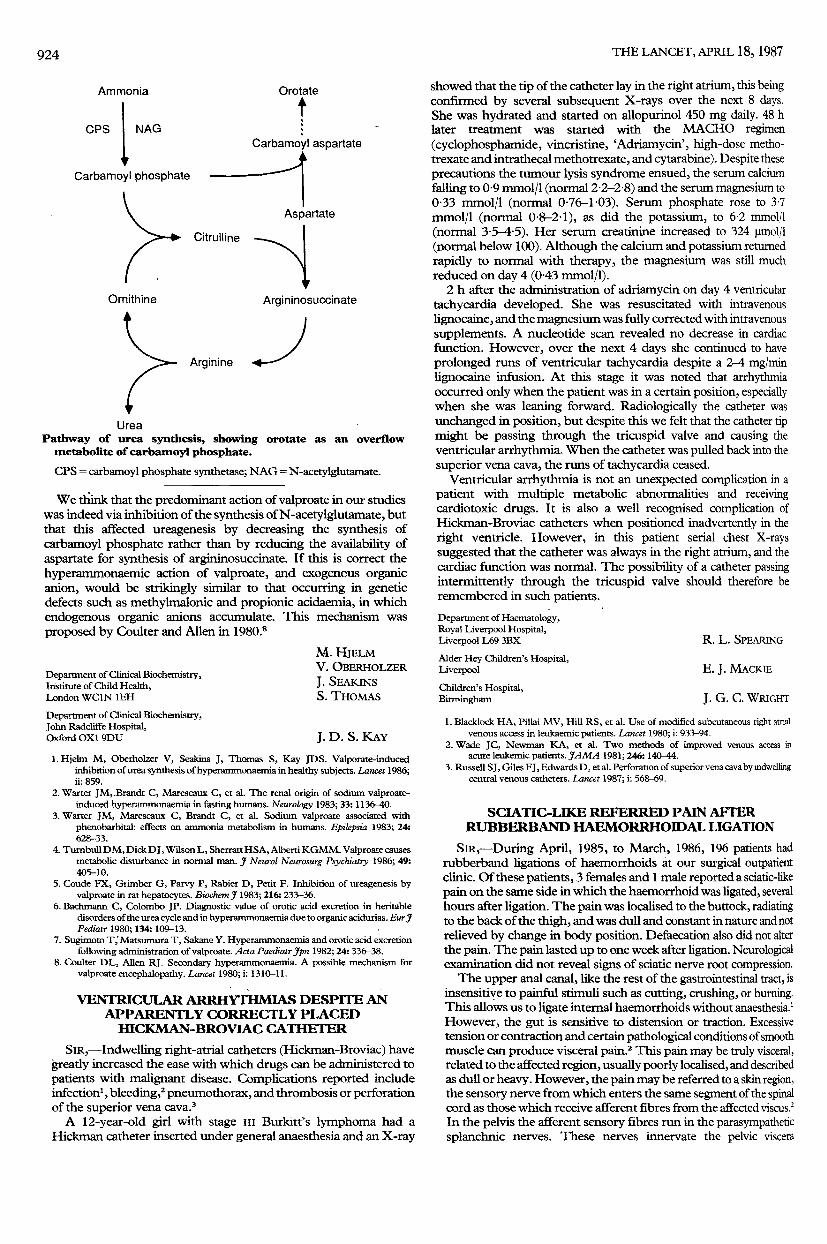
Orotate excretion may be used as a marker of carbamoylphosphate accumulation (see figure), and inhibition at any stagedownstream of carbamoyl phosphate synthesis would be expectedto increase orotate excretion. This reasoning is supported by studiesof genetic defects in this pathway. The administration of valproatedecreased orotate excretion, both in our experiments and in aprevious clinical study,’ which suggests that the site of inhibition ofureagenesis is not at the synthesis of argininosuccinate. If, however,the supply of aspartate is limited, as suggested by Kamoun andRabier, the link between accumulation of carbamoyl phosphate andexcretion of orotate may be broken, since aspartate is needed for thesynthesis of orotate (figure). Citrulline would then be expected toaccumulate: this was not detectable in our experiments.
924
Pathway of urea synthesis, showing orotate as an overflowmetabolite of carbamoyl phosphate.
CPS = carbamoyl phosphate synthetase; NAG = N-acetylglutamate.
We think that the predominant action of valproate in our studieswas indeed via inhibition of the synthesis of N-acetylglutamate, butthat this affected ureagenesis by decreasing the synthesis ofcarbamoyl phosphate rather than by reducing the availability ofaspartate for synthesis of argininosuccinate. If this is correct thehyperammonaemic action of valproate, and exogenous organicanion, would be strikingly similar to that occurring in geneticdefects such as methylmalonic and propionic acidaemia, in whichendogenous organic anions accumulate. This mechanism wasproposed by Coulter and Allen in 1980.8
Department of Clinical Biochemistry,Institute of Child Health,London WC1N 1EH
M. HJELMV. OBERHOLZER
J. SEAKINSS. THOMAS
Department of Clinical Biochemistry,John Radcliffe Hospital,Oxford OX1 9DU J. D. S. KAY
1. Hjelm M, Oberholzer V, Seakins J, Thomas S, Kay JDS. Valporate-inducedinhibition of urea synthesis of hyperammonaemia in healthy subjects. Lancet 1986;ii: 859.
2. Warter JM, Brandt C, Marescaux C, et al. The renal origin of sodium valproate-induced hyperammonaemia in fasting humans. Neurology 1983; 33: 1136-40.
3. Warter JM, Marescaux C, Brandt C, et al. Sodium valproate associated withphenobarbital: effects on ammonia metabolism in humans. Epilepsia 1983; 24:628-33.
4. Turnbull DM, Dick DJ, Wilson L, Sherratt HSA, Alberti KGMM. Valproate causesmetabolic disturbance in normal man. J Neurol Neurosurg Psychiatry 1986; 49:405-10.
5. Coude FX, Grimber G, Parvy P, Rabier D, Petit F. Inhibition of ureagenesis byvalproate in rat hepatocytes. Biochem J 1983; 216: 233-36.
6. Bachmann C, Colombo JP. Diagnostic value of orotic add excretion in heritabledisorders of the urea cycle and in hyperammonaemia due to organic acidurias. Eur JPediatr 1980; 134: 109-13.
7. Sugimoto T, Matsumura T, Sakane Y. Hyperammonaemia and orotic add excretionfollowing administration of valproate. Acta Paediatr Jpn 1982; 24: 336-38.
8. Coulter DL, Allen RJ. Secondary hyperammonaemia. A possible mechanism forvalproate encephalopathy. Lancet 1980; i: 1310-11.
VENTRICULAR ARRHYTHMIAS DESPITE ANAPPARENTLY CORRECTLY PLACEDHICKMAN-BROVIAC CATHETER
SIR,-Indwelling right-atrial catheters (Hickman-Broviac) havegreatly increased the ease with which drugs can be administered topatients with malignant disease. Complications reported includeinfection1, bleeding,2 pneumothorax, and thrombosis or perforationof the superior vena cava. 3A 12-year-old girl with stage til Burkitt’s lymphoma had a
Hickman catheter inserted under general anaesthesia and an X-ray
showed that the tip of the catheter lay in the right atrium, this beingconfirmed by several subsequent X-rays over the next 8 days.She was hydrated and started on allopurinol 450 mg daily. 48 hlater treatment was started with the MACHO regimen(cyclophosphamide, vincristine, ’Adriamycin’, high-dose metho-trexate and intrathecal methotrexate, and cytarabine). Despite theseprecautions the tumour lysis syndrome ensued, the serum calciumfalling to 0-9 mmol/1 (normal 2-2-2-8) and the serum magnesium to0-33 mmol/1 (normal 0-76-1-03). Serum phosphate rose to 37mmol/1 (normal 0-8-2-1), as did the potassium, to 62 mmolfl(normal 3-5-15). Her serum creatinine increased to 324 umol/1(normal below 100). Although the calcium and potassium returnedrapidly to normal with therapy, the magnesium was still muchreduced on day 4 (0 43 mmol/1).
2 h after the administration of adriamycin on day 4 ventriculartachycardia developed. She was resuscitated with intravenouslignocaine, and the magnesium was fully corrected with intravenoussupplements. A nucleotide scan revealed no decrease in cardiacfunction. However, over the next 4 days she continued to haveprolonged runs of ventricular tachycardia despite a 2-4 mg/minlignocaine infusion. At this stage it was noted that arrhythmiaoccurred only when the patient was in a certain position, especiallywhen she was leaning forward. Radiologically the catheter wasunchanged in position, but despite this we felt that the catheter tipmight be passing through the tricuspid valve and causing theventricular arrhythmia. When the catheter was pulled back into thesuperior vena cava, the runs of tachycardia ceased.
Ventricular arrhythmia is not an unexpected complication in apatient with multiple metabolic abnormalities and receivingcardiotoxic drugs. It is also a well recognised complication ofHickman-Broviac catheters when positioned inadvertently in theright ventricle. However, in this patient serial chest X-rayssuggested that the catheter was always in the right atrium, and thecardiac function was normal. The possibility of a catheter passingintermittently through the tricuspid valve should therefore beremembered in such patients.
Department of Haematology,Royal Liverpool Hospital,Liverpool L69 3BX R. L. SPEARING
Alder Hey Children’s Hospital,Liverpool E. J. MACKIEChildren’s Hospital,Birmingham J. G. C. WRIGHT
1. Blacklock HA, Pillai MV, Hill RS, et al. Use of modified subcutaneous right atnalvenous access in leukaemic patients. Lancet 1980; i: 933-94.
2. Wade JC, Newman KA, et al. Two methods of improved venous access inacute leukemic patients. JAMA 1981; 246: 140-44.
3. Russell SJ, Giles FJ, Edwards D, et al. Perforation of superior vena cava by indwellingcentral venous catheters. Lancet 1987; i: 568-69.
SCIATIC-LIKE REFERRED PAIN AFTERRUBBERBAND HAEMORRHOIDAL LIGATION
SIR,-During April, 1985, to March, 1986, 196 patients hadrubberband ligations of haemorrhoids at our surgical outpatientclinic. Of these patients, 3 females and 1 male reported a sciatic-likepain on the same side in which the haemorrhoid was ligated, severalhours after ligation. The pain was localised to the buttock, radiatingto the back of the thigh, and was dull and constant in nature and notrelieved by change in body position. Defaecation also did not alterthe pain. The pain lasted up to one week after ligation. Neurologicalexamination did not reveal signs of sciatic nerve root compression.The upper anal canal, like the rest of the gastrointestinal tract, is
insensitive to painful stimuli such as cutting, crushing, or burning.This allows us to ligate internal haemorrhoids without anaesthesia.’However, the gut is sensitive to distension or traction. Excessivetension or contraction and certain pathological conditions of smoothmuscle can produce visceral pain.2 This pain may be truly visceral,related to the affected region, usually poorly localised, and describedas dull or heavy. However, the pain may be referred to a skin region,the sensory nerve from which enters the same segment of the spinalcord as those which receive afferent fibres from the affected viscus.)In the pelvis the afferent sensory fibres run in the parasympatheticsplanchnic nerves. These nerves innervate the pelvic viscera