Embed Size (px)
Citation preview

British Journal of Plastic Surgery (2002), 55, 55-58 �9 2002 The British Association of Plastic Surgeons doi: 10.1054/bjps.2001.3741
I . R , T , S . OU.NAL OF P L A S T , C S U . G . . Y
Vascular endothelial growth factor gene therapy in ischaemic rat skin flaps
G. O'Toole*t, D. MacKenzie*t, R. Lindemant, M. E Buckley'~, D. Marucci*, N. McCarthy,- and M. Poole*
*Department of Plastic and Reconstructive Surgery, St George Hospital; and tDepartment of Haematology, Prince of Wales Hospital, Sydney, Australia
SUMMARY. Gene therapy with the complementary DNA (cDNA) of the angiogenic cytokine vascular endothelial growth factor (VEGF) has emerged as a promising strategy in the treatment of myocardial and lower-limb ischaemia. The objective of this study was to determine whether these principles could be applied to a recognised model of skin- flap ischaemia. Plasmid vectors including the cDNA of green fluorescent protein (GFP) and one of three VEGF iso- forms (A165, B167 or B186) were constructed, and their base sequences confirmed. GFP expression was used as a marker of successful in vitro transfection of human endothelial cells with each plasmid. The plasmids were then admin- istered subcutaneously to rat abdominal skin flaps surgically rendered ischaemic, and the percentage of viable tissue was assessed at 1 week. Angiograms of the flaps and histological preparations of flap tissue were assessed for evidence of angiogenesis. The survival of flaps treated with VEGF A165 or B167 cDNA was significantly greater than that of controls (P < 0.05). The survival of flaps treated with VEGF B 186 cDNA was greater than that of controls, but statisti- cal significance was not reached. Angiograms and microvessel density counts failed to produce evidence of angiogene- sis. With improved delivery strategies, VEGF may have a role in the management of surgical ischaemia. �9 2002 The British Association of Plastic Surgeons
Keywords: gene therapy, vascular endothelial growth factor, reconstructive surgery.
Gene therapy with the complementary DNA (cDNA) of the angiogenic cytokine vascular endothelial growth factor (VEGF) has emerged as a promising strategy in the treat- ment of myocardial and lower-limb ischaemia. The VEGF family of polypeptides, the most potent of the various fam- ilies of angiogenic cytokines, includes VEGF A, VEGF B, VEGF C, VEGF D, VEGF E and placental growth factor. There are four isoforms of VEGF A and two of VEGF B. Most in vivo studies have been performed with VEGF A isoforms. Early human trials report VEGF A gene-therapy induced angiogenesis in the muscles of the ischaemic lower limb 1,2 and in ischaemic cardiac muscle)
Although therapeutic angiogenesis with recombinant human cytokines has been explored in a variety of animal models of direct relevance to reconstructive surgery, the only publication to date describing gene therapy using VEGF cDNA administered to a skin flap is that of Taub et al. 4 In the study, significant (P < 0.05) improvement in the viability of ischaemic rat skin flaps that had received intra-arterial VEGF A121 cDNA was reported, and increased VEGF protein deposition was confirmed by immunohistochemistry.
The objective of this study was to test the efficacy of VEGF gene therapy using cDNA of other VEGF iso- forms (A165, B 167, B 186) in a similar animal model.
Methods
Preparation of the plasmid vector
The cDNA of VEGF A 165, VEGF B 167 and VEGF B 186 (Amrad Biotech R+D, Burnley, Victoria, Australia) were
cloned separately into an expression vector encoding green fluorescent protein (GFP) and a CMV promoter (pEGFP N1; Clontech Laboratories Inc., Palo Alto, CA, USA). Each VEGF isoform's cDNA was cloned between the EcoR1 and BamHI restriction sites of the multiple cloning site, upstream of the GFP cDNA, which acted as a marker of gene expression in subsequent in vitro exper- iments. DNA sequencing confirmed that the VEGF-GFP fusion gene had been cloned in frame.
In vitro testing of the plasmid vector
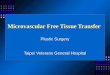
The three plasmid vectors encoding VEGF A165-GFP, VEGF B 167-GFP and VEGF B 186-GFP were used sep- arately to transfect human umbilical-vein endothelial cells (HUVECs). The appearance of the HUVECs 2 days after transfection is shown in Figure 1. The brilliant green fluorescence confirmed that each of the plasmids was capable of transfecting mammalian cells, and that the transfected cells expressed the respective fusion genes.
In vivo study
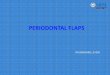
Ethics approval for the use of male Sprague-Dawley rats (weighing 400-550g) was granted by the University of New South Wales Animal Care and Ethics Committee. The surgical model (Fig. 2) was based on that originally described by Finseth and Cutting to investigate the 'delay phenomenon'. 5 General anaesthesia was induced and maintained using 2% halothane in oxygen. The rats were placed supine and their abdominal skin was shaved.
55

56 British Journal of Plastic Surgery
Figure 1--Green fluorescent protein expression in human umbilical- vein endothelial cells (HUVECs).
A square flap was designed to be 8 cm in length in the midline, from the pubis to the approximate level of the xiphoid depending on the size of the rat, and 8 cm in width, with the rat's midline as its midpoint (Fig. 2A,B). The flap was raised from the fascia of the abdominal wall, on the superficial inferior epigastric neurovascular pedi- cles arising in the groin (Fig. 2C). At this point, the flap was viable in its entirety. However, in this model, in order to render the flap ischaemic, one inferior epigastric neu- rovascular bundle was divided (Fig. 2C,D). The flap on the side of the divided vessels was, thus, dependent on the blood supply to the opposite half of the flap for its sur- vival. In this way 'conceptually... a random pattern flap is now attached to an axial pattern flap'. 5 Without any intervention, over subsequent days an area of necrosis develops on the random-pattern half of the flap (Fig. 3).
A solution of either plasmid DNA or saline was injected at 10 equally spaced subcutaneous sites along the length of the midline of the flap (Fig. 2D). A total of 60 rats were divided into five groups (Table 1). Rats in group 1 received 50 Ixg plasmid DNA encoding VEGF A165 and GFP in 1 ml saline. In group 2 the plasmid vec- tor encoding VEGF B167 and GFP was administered, and in group 3 the plasmid vector encoded VEGF B186 and GFP. Group 4 was a control group, in which the same plasmid vector encoding GFP, but without a VEGF gene, was administered. In group 5 the rats received 1 ml of subcutaneous saline.
The skin was then replaced (Fig. 2E) and sutured in its original anatomical location (Fig. 2F). While the rat was still anaesthetised, a rigid collar was made from X-ray
Figure 2--The surgical model.
film, and placed comfortably around the neck of the rat to prevent it from tampering with the skin flap. Any rat that managed to remove its collar and tamper with its flap was excluded from the study.
The extent of flap survival was determined on day 7. A template of the remaining viable segment of each flap was traced, and an image was captured and analysed using a software package (UTHSCA Image Tools). Immediately prior to euthanasia, the inferior epigastric artery was cannulated under microscopic control, and saline was injected gently to flush blood from the flap. The saline could be seen to emerge from the flap in the inferior epigastric vein. A radio-opaque mixture of iron oxide and gelatin suspended in water at 37 ~ was then injected intra-arterially. 6 Angiograms were acquired, and the vascularity of the skin flaps was assessed.
Following angiography, tissue from the midpoint of each skin flap was preserved for histological assessment of microvessel density. Slides were stained with haema- toxylin and eosin, and a count of dermal and subcuta- neous blood vessels at five points was performed at high magnification after blinding of the slide identity. The number of blood vessels was counted from the fibrous tis- sue layer deep to the panniculus carnosus to the epidermis

Vascular endothelial growth factor gene therapy in ischaemic rat skin flaps 57
, ' i"
100
95
90
~186t:iJl~ ~ e l 2 1 ~ Saline
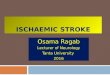
Figure 4---Results of rat flap survival on day 7. Values shown are mean percentages and standard deviations.
Figure 3--The appearance of control flaps 7 days postoperatively.
Table 1 Details of the three experimental groups and the two control groups
group 1 n = 14
group 2 n = 13
group 3 n = 11
group 4 (control) n = 11
group 5 (con~ol) n = 11
50 p,g plasmid DNA encoding VEGF A165 and GFP in 1 ml saline
50 ixg plasmid DNA encoding VEGF B167 and GFP in I ml saline
50 ixg plasmid DNA encoding VEGF B186 and GFP in 1 ml saline
50 ixg plasmid DNA encoding GFP in 1 ml saline
I ml saline
Results
The mean flap survival rates and standard deviations are shown in Figure 4.
A statistically significant difference in flap survival was seen between the rats that received the VEGF A165 cDNA (group 1; 90.3% mean survival) and those that received saline (group 5; 81.2% mean survival) (P = 0.03). While a trend towards increased flap survival was observed in group 1 compared with the GFP control (group 4; 83.2% mean survival), statistical significance was not reached (P=0.06). Significantly improved flap survival was seen in rats that had received VEGF B167 cDNA (group 2; 92.1% mean survival) compared with each of the control groups (groups 4 and 5 ) (P = 0.02 and P=0.01 , respectively). Although the rats that had received the VEGF B186 cDNA (group 3; 86.2% mean survival) had a higher mean flap survival than the rats in control groups 4 and 5, statistical analysis of the results revealed P values of 0.39 and 0.25, respectively. The con- trol groups did not differ significantly from each other.
There were no clear differences in the number or cali- bre of the vessels in treated and control flaps, as assessed by angiography. A typical angiogram is shown in Figure 5. Histological examination revealed considerable variation in the number of blood vessels per slide from individual flaps, resulting in mean values with large standard devia- tions; a statistically significant difference was not demon- strated between treated and control groups.
in five adjacent areas, and all vessels were included, regardless of size.
Statistical analysis of the data
Flap survival and microvessel-count data were assessed using a one-way analysis of variance (ANOVA) followed by a post-hoc Duncan's multiple range test (Statistica Statsoft, Tulsa, OK, USA).
Discussion
This study was designed to determine whether the adminis- tration of the cDNA of VEGF A165 is effective in protect- ing ischaemic skin flaps from necrosis, as has been previously shown in ischaemic muscle. There is little pub- lished research regarding the cDNA of the VEGF B 167 and B186 isoforms; therefore, this study also investigated their use as agents of gene therapy in ischaemic skin flaps.

58 British Journal of Plastic Surgery
ischaemia cannot be otherwise reversed is not certain. Research evidence of the beneficial effect of VEGF gene therapy in critically ischaemic human myocardium 3 and lower limb 1'2 might suggest that in flap surgery the ther- apy should be reserved for critically ischaemic tissue. However, research into the applications of VEGF gene therapy in reconstructive surgery is at an early stage, and the ideal recipient tissue remains uncertain. Other issues, such as improving the efficiency and safety of the deliv- ery of genetic material to human tissue, are yet to be fully investigated. Nevertheless, our results suggest, in principle, that VEGF gene transfer may be of use as an adjunct to standard reconstructive surgical techniques.
Figure 5--Angiogram of flap at day 7.
Our results suggest that the VEGF A165 cDNA is effective in this model. The demonstration of improved flap survival in group 1 is consistent with published evi- dence of the potential of VEGF A165 cDNA as a thera- peutic agent in ischaemic tissue. VEGF B 167 cDNA was also shown to be effective in this setting. Neither VEGF A165 nor VEGF B167 gene therapy has previously been attempted in skin flaps. The group of rats treated with the cDNA of VEGF B 186 showed a higher mean percentage flap survival than both control groups, but the differences did not reach statistical significance.
There was no angiographic or histological evidence of increased microvessel density in any experimental group. This may be due to technical shortcomings. Using mono- chromatic synchrotron radiation microangiography, Takeshita et al reported that angiogenesis after VEGF gene transfer results in small networks of arteries with diameters of less than 100~m. 7 Others have suggested that standard methods of contrast angiography cannot provide images of arteries of less than 200 tzm in diame- ter. s However, it is by no means certain that the improved survival of the rat skin flaps treated with VEGF cDNA resulted from undetected angiogenesis. VEGF isoforms have functions other than neovascularisation, to which the effect of this gene therapy may be attributed. These include a protective reparative effect on microvessels. The prevention of microvessel regression in an ischaemic environment may be enough to improve skin-flap sur- vival in treated rats.
In conclusion, despite the lack of evidence of angio- genesis, the cDNA of VEGF A165 and VEGF B 167 have been shown to be effective in protecting ischaemic rat skin flaps from necrosis. The cDNA of VEGF B186 did not result in a statistically significant improvement in flap survival.
Whether it would be appropriate to administer VEGF gene therapy to all flaps or only to those in which critical
References
1. Isner JM, Pieczek A, Schainfeld R, et al. Clinical evidence of anglo- genesis after arterial gene transfer of phVEGF165 in patient with ischaemic limb. Lancet 1996; 348: 370-4.
2. Baumgartner I, Pieczek A, Manor O, et al. Constitutive expression of phVEGFj65 after intramuscular gene transfer promotes collateral vessel development in patients with critical limb ischemia. Circulation 1998; 97:1114-23.
3. Rosengart TK, Lee LY, Patel SR, et al. Angiogenesis gene therapy: phase I assessment of direct intramyocardial administration of an adenovirus vector expressing VEGF 121 cDNA to individuals with clinically significant severe coronary artery disease. Circulation 1999; 100: 468-74.
4. Taub PJ, Marmur JD, Zhang WX, et al. Locally administered vascu- lar endothelial growth factor cDNA increases survival of ischemic experimental skin flaps. Plast Reconstr Surg 1998; 102: 2033-9.
5. Finseth F, Cutting C. An experimental neurovascular island skin flap for the study of the delay phenomenon. Plast Reconstr Surg 1978; 61: 412-20.
6. Rees MJW, Taylor GI. A simplified lead oxide cadaver injection technique. Plast Reconstr Surg 1986; 77: 141-5.
7. Takeshita S, Isshiki T, Mori H, et al. Microangiographic assessment of collateral vessel formation following direct gene transfer of vascular endothelial growth factor in rats. Cardiovasc Res 1997; 35: 547-52.
8. Isner JM, Losordo DW. Therapeutic angiogenesis for heart failure. Nature Med 1999; 5: 491-2.
The Authors
Greg O'Toole MB, ChB, FRCS, Plastic Surgery Research Fellow Duncan MacKenzie MBBS, FRCS, Plastic Surgery Research Fellow Damian Marucci MBBS, BA, Surgical Research Fellow Michael Poole MBBS, MD, FRACS, FRCS, Professor of Plastic Surgery
Department of Plastic and Reconstructive Surgery, St George Hospital, Kogarah, Sydney, New South Wales 2217, Australia.
Rob Lindeman MBBS, PhD, FRACP, FRCPA, Consultant Haematologist Michael F. Buekley MB, ChB, PhD, FRCPA, Head of Molecular Genetics and Cytogenetics Nigel McCarthy BSc, MSe, Research Assistant
Department of Haematology, Prince of Wales Hospital, Randwick, Sydney, New South Wales 2031, Australia.
Correspondence to Mr G. O'Toole, c/o 1 Eastcote View, Pinner, Middlesex HA5 1AT, UK.
Paper received 27 June 2001. Accepted 25 October 2001, after revision.