Embed Size (px)
Citation preview

2/25/2017
1
Vascular & Interventional RadiologyOral Board Review
Aaron T. Rucks, D.O., M.S.
Interventional Radiologist
1
2
2/25/2017
2
3
4
2/25/2017
3
5
5

2/25/2017
4
6
7
2/25/2017
5
8
2/25/2017
6
9
10
2/25/2017
7
11
12
2/25/2017
8
13
14 Right flank pain, sepsis, hypotension
2/25/2017
9
15
16
R R

2/25/2017
10
17
18
2/25/2017
11
19
20
2/25/2017
12
21

2/25/2017
13
22
23
2/25/2017
14
24
Review
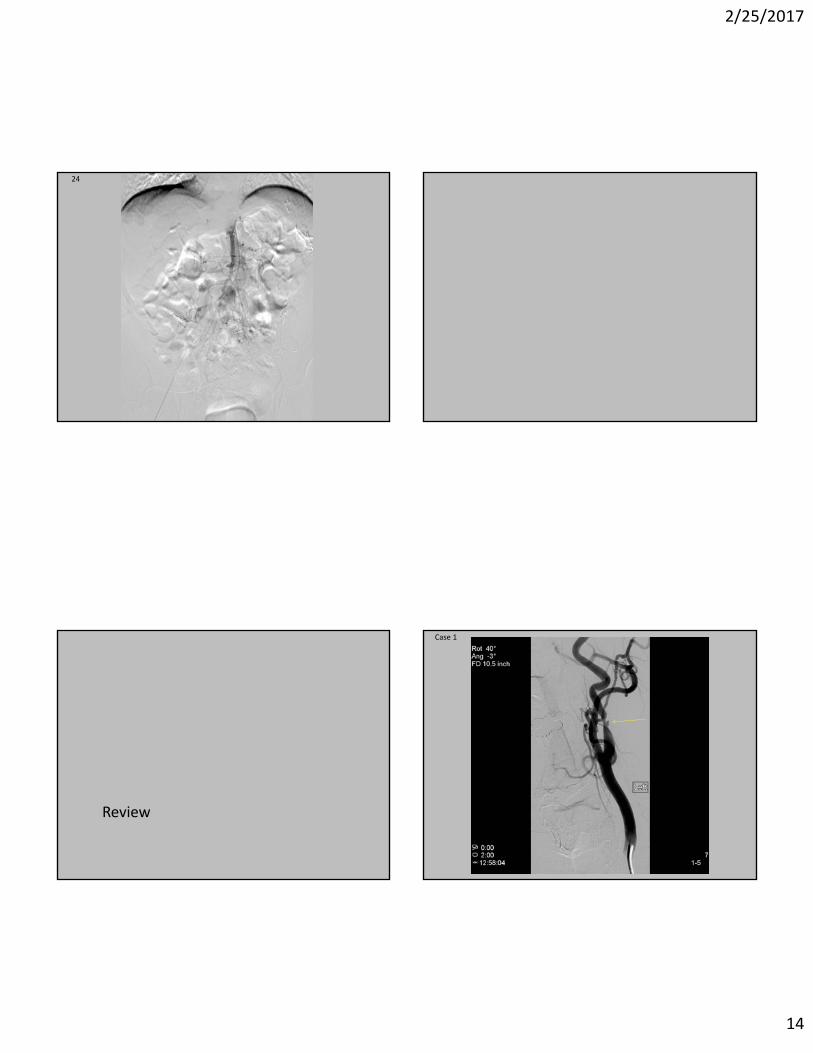
Case 1
2/25/2017
15
Carotid Artery Stenosis• Findings: Ulcerative plaque with significant stenosis proximal internal carotid
artery.• Differential Diagnosis:
– Atherosclerosis– Dissection– Fibromuscular dysplasia– Trauma– Vasculitis
• Treatment Options:– Carotid endarterectomy (CEA)
• NASCET treat symptomatic >50%– 2yr stroke risk stenoses 70‐99% : medical management 26%, surgical CEA 9%
• ACAS treat asymptomatic >60%– 5yr stroke risk stenoses >60%: medical management 11%, surgical CEA 5.1%
– Carotid stenting• Symptomatic >70%
North American Symptomatic Carotid Endarterectomy Trial (NASCET)Endarterectomy for Asymptomatic Carotid Atherosclerosis Study (ACAS)
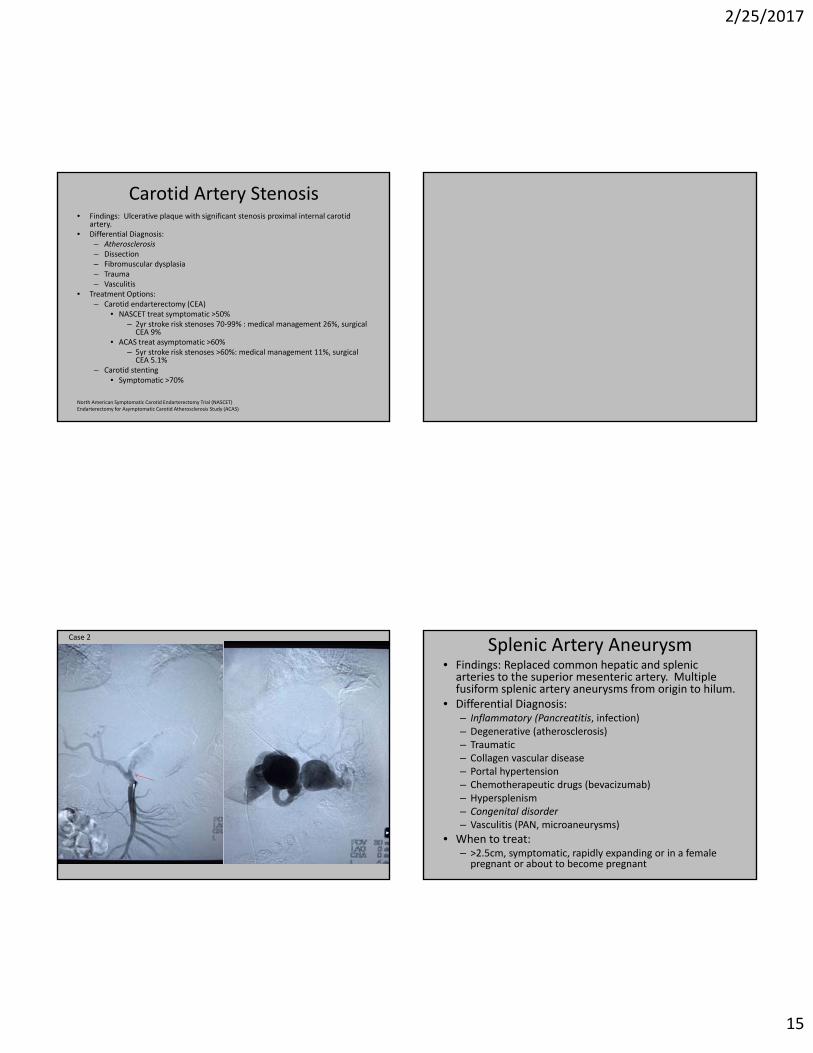
Case 2
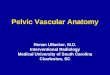
Splenic Artery Aneurysm• Findings: Replaced common hepatic and splenic arteries to the superior mesenteric artery. Multiple fusiform splenic artery aneurysms from origin to hilum.
• Differential Diagnosis:– Inflammatory (Pancreatitis, infection)– Degenerative (atherosclerosis)– Traumatic– Collagen vascular disease– Portal hypertension– Chemotherapeutic drugs (bevacizumab)– Hypersplenism– Congenital disorder– Vasculitis (PAN, microaneurysms)
• When to treat:– >2.5cm, symptomatic, rapidly expanding or in a female pregnant or about to become pregnant

2/25/2017
16
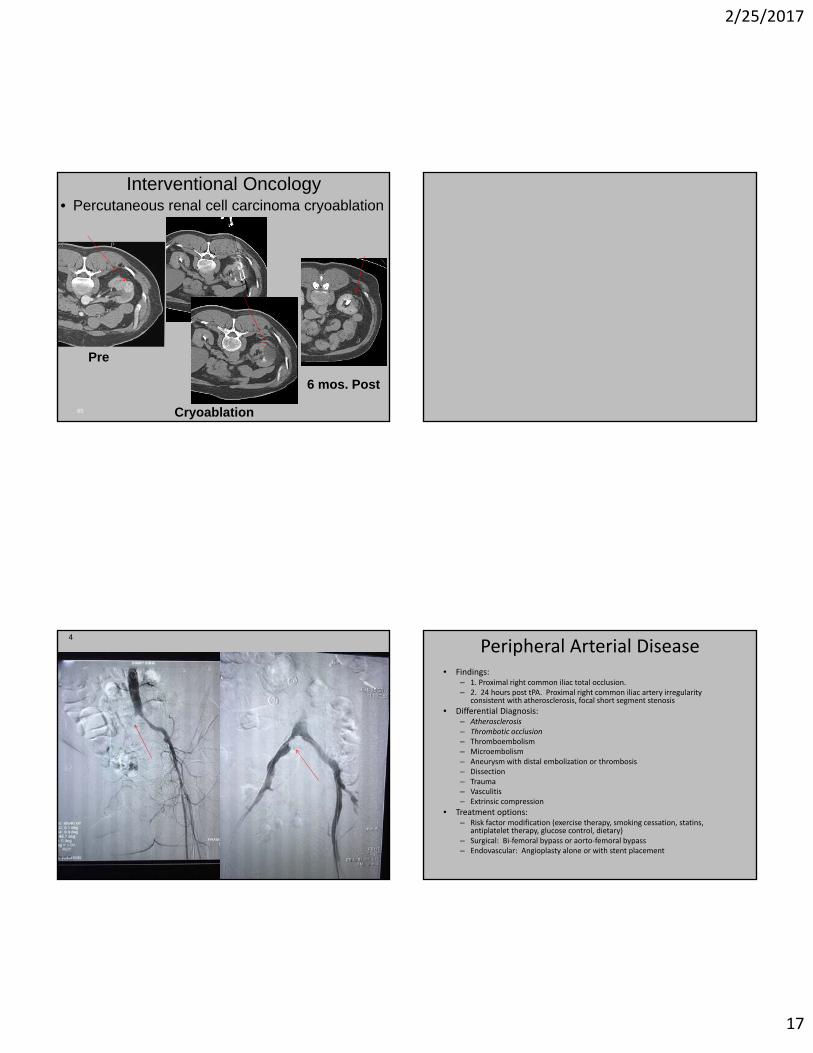
3 Renal Mass• Findings: < 3 cm renal mass not meeting criteria for a simple cyst.
• Differential Diagnosis:– Renal Cell Carcinoma– Oncocytoma– Lymphoma– Angiomyolipoma (doubtful no macroscopic fat)
• Treatment Options:– Active surveillance (CT/MR 6‐12 month intervals)– Partial nephrectomy– Laparoscopic cryoablation or radiofrequency ablation– Percutaneous image guided cryoablation (Stage 1a <4cm) – 5yr retrospective data similar to surgery
• cryoablation, radiofrequency ablation, microwave ablation
2/25/2017
17
• Percutaneous renal cell carcinoma cryoablationInterventional Oncology
65
Pre
Cryoablation
6 mos. Post
4
Peripheral Arterial Disease• Findings:
– 1. Proximal right common iliac total occlusion.– 2. 24 hours post tPA. Proximal right common iliac artery irregularity
consistent with atherosclerosis, focal short segment stenosis
• Differential Diagnosis:– Atherosclerosis– Thrombotic occlusion– Thromboembolism– Microembolism– Aneurysm with distal embolization or thrombosis– Dissection– Trauma– Vasculitis– Extrinsic compression
• Treatment options:– Risk factor modification (exercise therapy, smoking cessation, statins,
antiplatelet therapy, glucose control, dietary)– Surgical: Bi‐femoral bypass or aorto‐femoral bypass– Endovascular: Angioplasty alone or with stent placement

2/25/2017
18
Initial Arteriogram Post Angioplasty and Stenting
55
2/25/2017
19
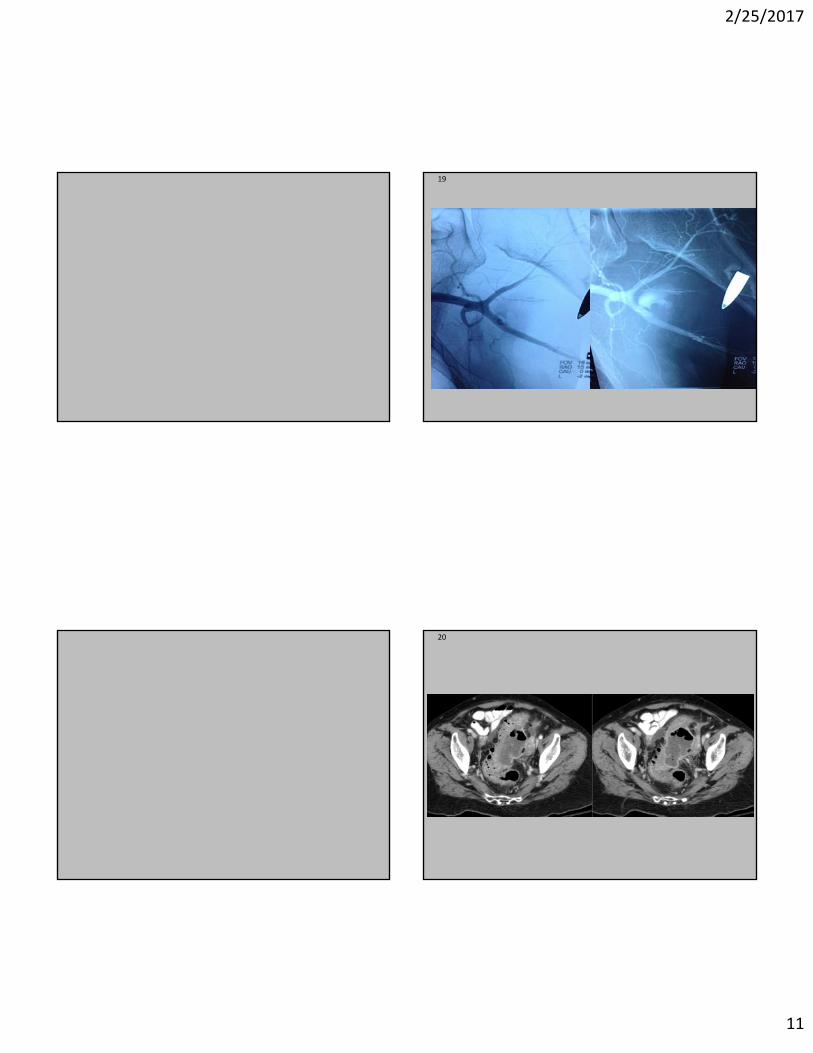
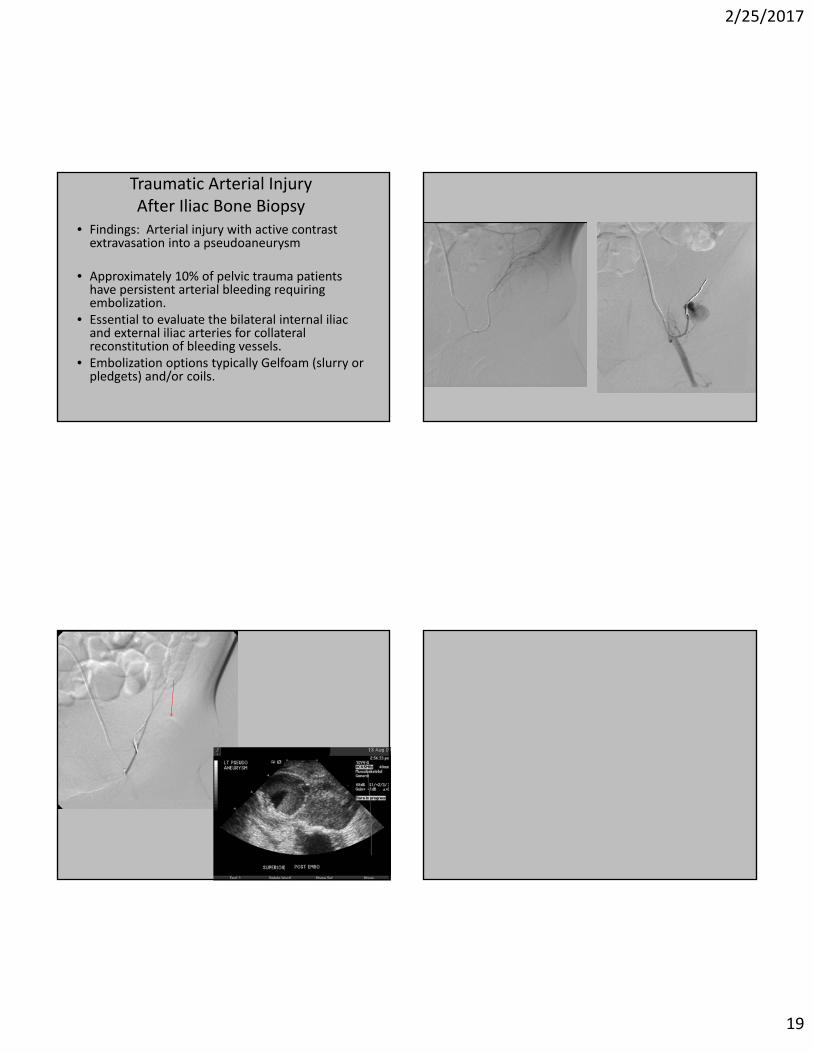
Traumatic Arterial InjuryAfter Iliac Bone Biopsy
• Findings: Arterial injury with active contrast extravasation into a pseudoaneurysm
• Approximately 10% of pelvic trauma patients have persistent arterial bleeding requiring embolization.
• Essential to evaluate the bilateral internal iliac and external iliac arteries for collateral reconstitution of bleeding vessels.
• Embolization options typically Gelfoam (slurry or pledgets) and/or coils.

2/25/2017
20
6
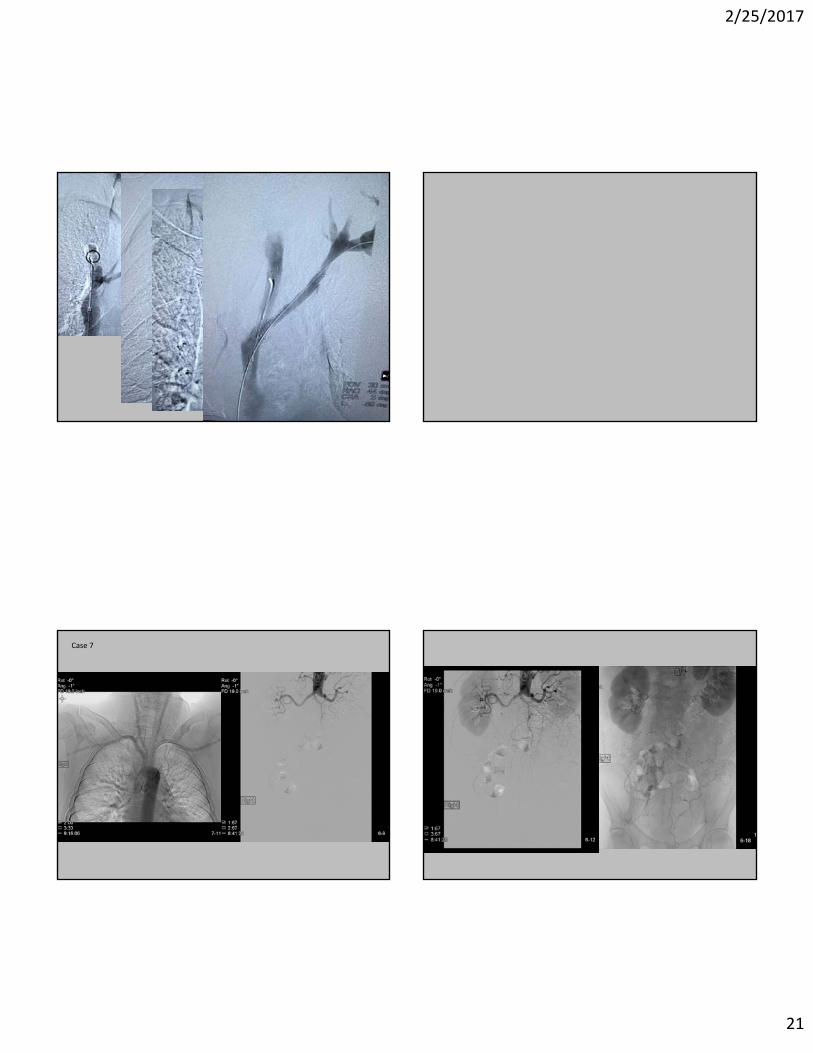
• Findings: Occlusion of the left brachiocephalic vein with acute thrombus. Multiple collateral veins. Focal short segment stenosis SVC.
• Differential diagnosis:– Malignancy (lung ca, mediastinal tumor, 1° leiomyosarcoma)– Radiation therapy– Intimal injury (vascular catheters or devices)– Chemotherapeutic agents– Trauma– Fibrosing mediastinitis– Aortic or brachiocephalic aneurysm– Infection
• Treatment– Endovascular vs. radiation vs. chemotherapy vs. surgical (rare)– Combination
SVC Syndrome
2/25/2017
21
Case 7

2/25/2017
22
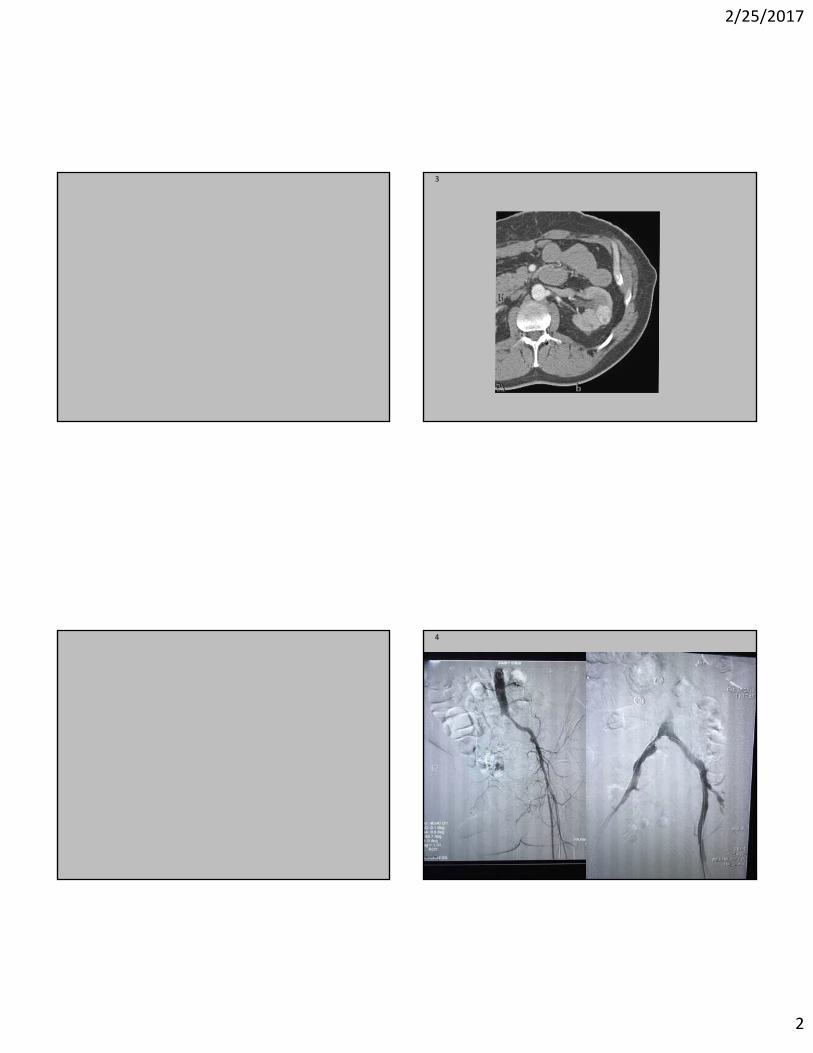
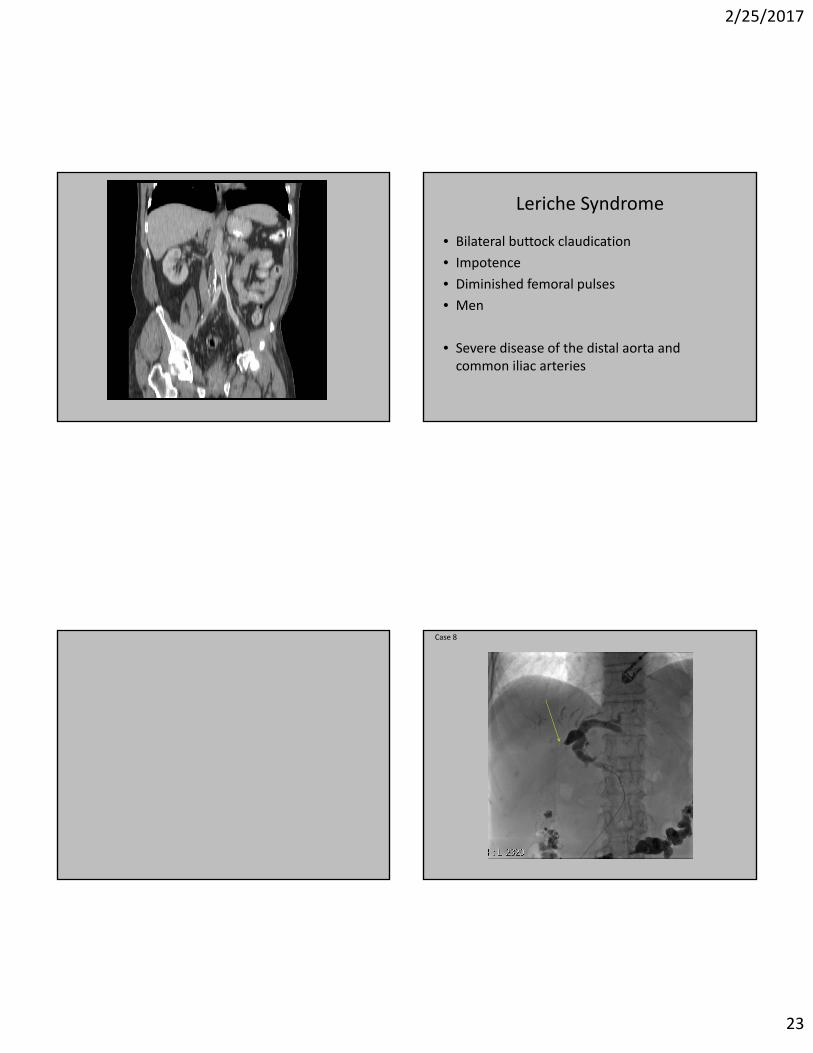
Aortoiliac occlusive disease• Findings:
– Arteriogram: Complete occlusion of the infrarenal abdominal aorta, delayed imaging demonstrated faint collateral flow to the lower extremities.
– CT: Similar to arteriogram. Complete occlusion of the infrarenal abdominal aorta and left renal artery and superior mesenteric stenoses.
• Differential Diagnosis:– Atherosclerosis– Embolic occlusion– Hypoplastic aorta syndrome (Abdominal aortic coarctation)– Neurofibromatosis– Takayasu’s arteritis
• Treatment options:– Surgical: Aortobifemoral graft or axillobifemoral graft– Smoking cessation– Risk factor modification (exercise therapy, smoking cessation, statins,
antiplatelet therapy, glucose control, dietary)
Case 7
2/25/2017
23
Leriche Syndrome
• Bilateral buttock claudication
• Impotence
• Diminished femoral pulses
• Men
• Severe disease of the distal aorta and common iliac arteries
Case 8
2/25/2017
24
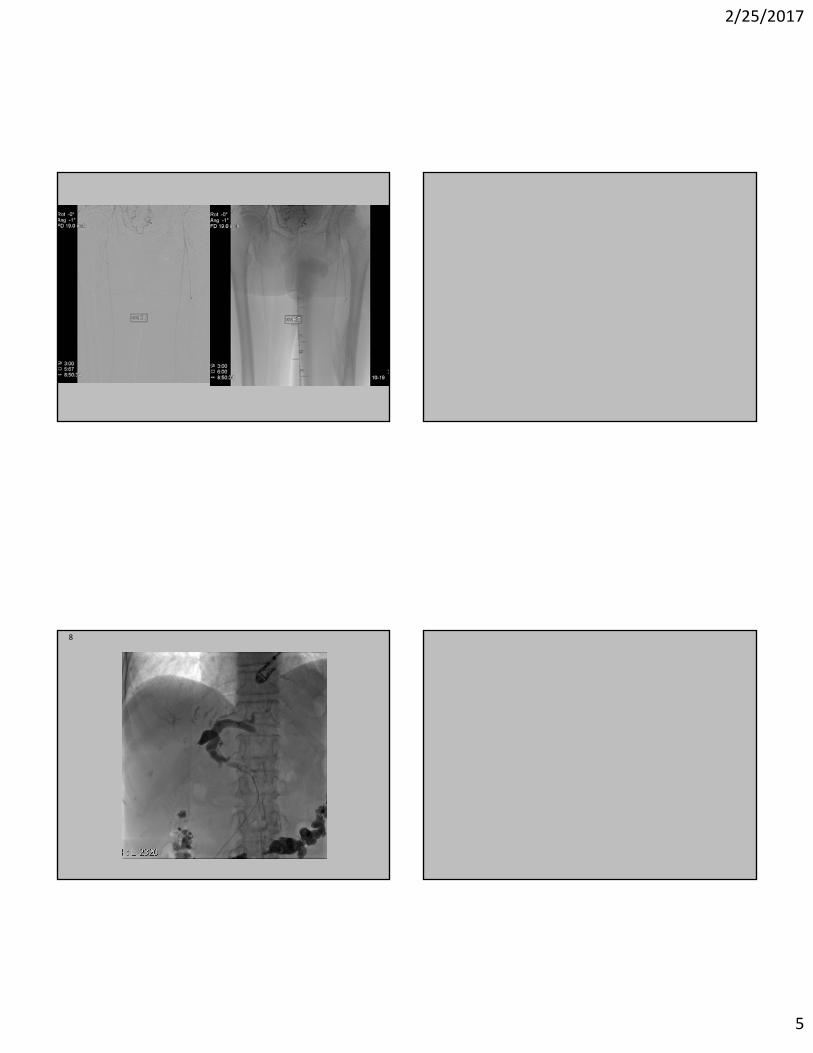
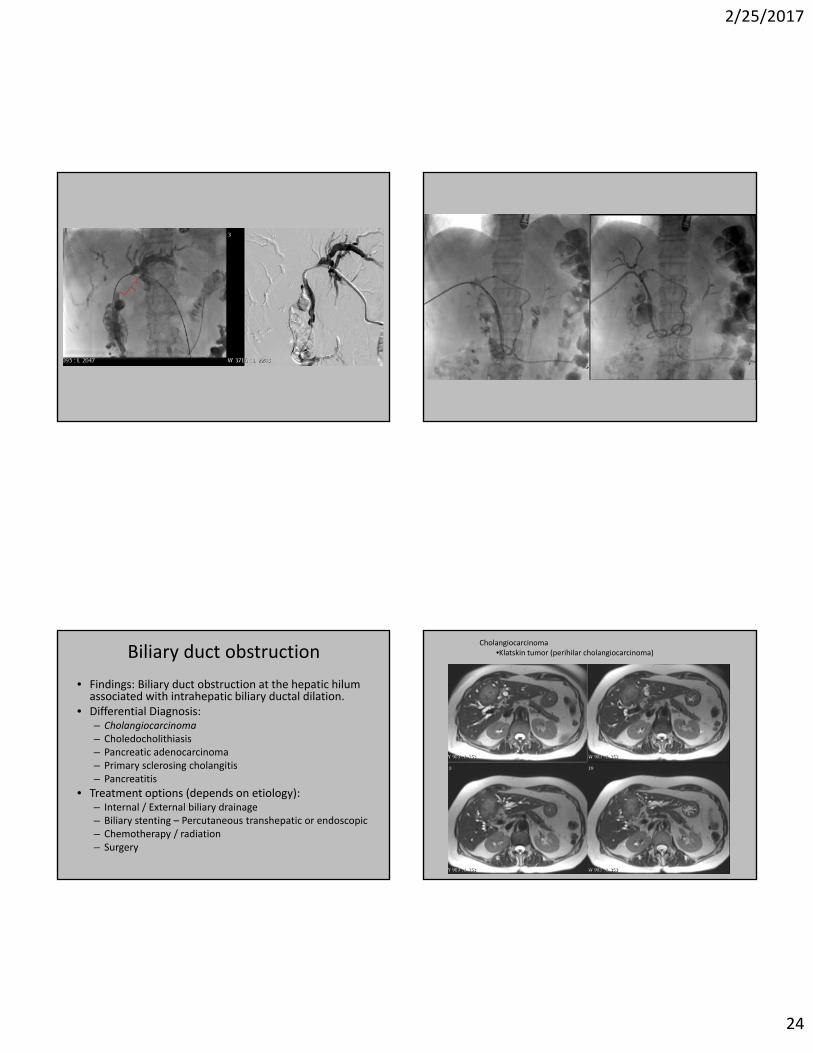
Biliary duct obstruction
• Findings: Biliary duct obstruction at the hepatic hilum associated with intrahepatic biliary ductal dilation.
• Differential Diagnosis:– Cholangiocarcinoma– Choledocholithiasis– Pancreatic adenocarcinoma– Primary sclerosing cholangitis– Pancreatitis
• Treatment options (depends on etiology):– Internal / External biliary drainage– Biliary stenting – Percutaneous transhepatic or endoscopic– Chemotherapy / radiation– Surgery
Cholangiocarcinoma•Klatskin tumor (perihilar cholangiocarcinoma)
2/25/2017
25
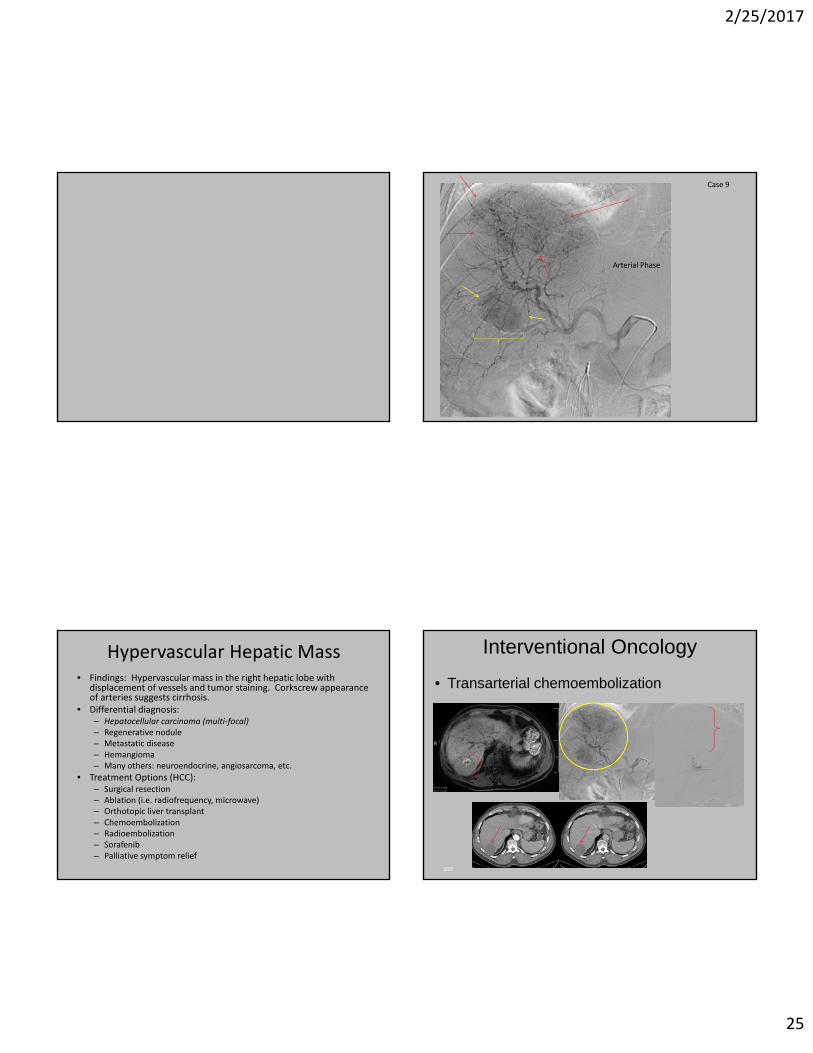
Case 9
Arterial Phase
Hypervascular Hepatic Mass• Findings: Hypervascular mass in the right hepatic lobe with
displacement of vessels and tumor staining. Corkscrew appearance of arteries suggests cirrhosis.
• Differential diagnosis:– Hepatocellular carcinoma (multi‐focal)– Regenerative nodule– Metastatic disease– Hemangioma– Many others: neuroendocrine, angiosarcoma, etc.
• Treatment Options (HCC):– Surgical resection– Ablation (i.e. radiofrequency, microwave)– Orthotopic liver transplant– Chemoembolization– Radioembolization– Sorafenib– Palliative symptom relief
• Transarterial chemoembolization
Interventional Oncology
100

2/25/2017
26
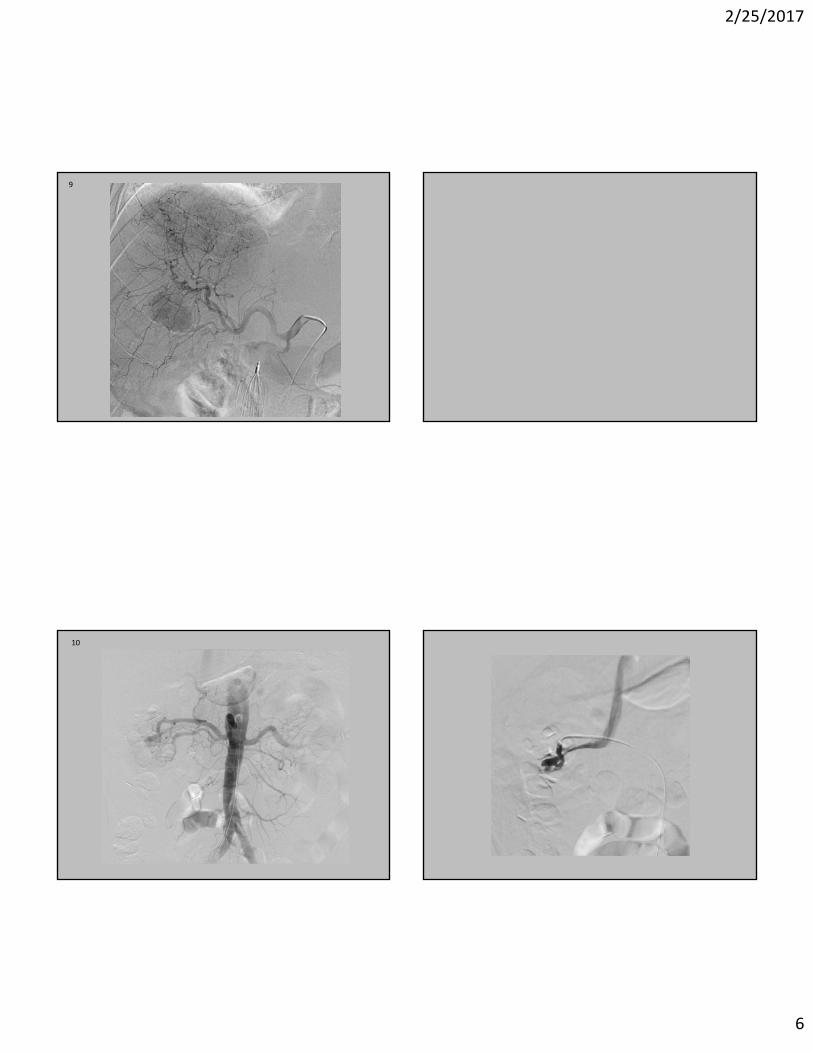
Case 10
Hematuria, S/P superior pole partial nephrectomy
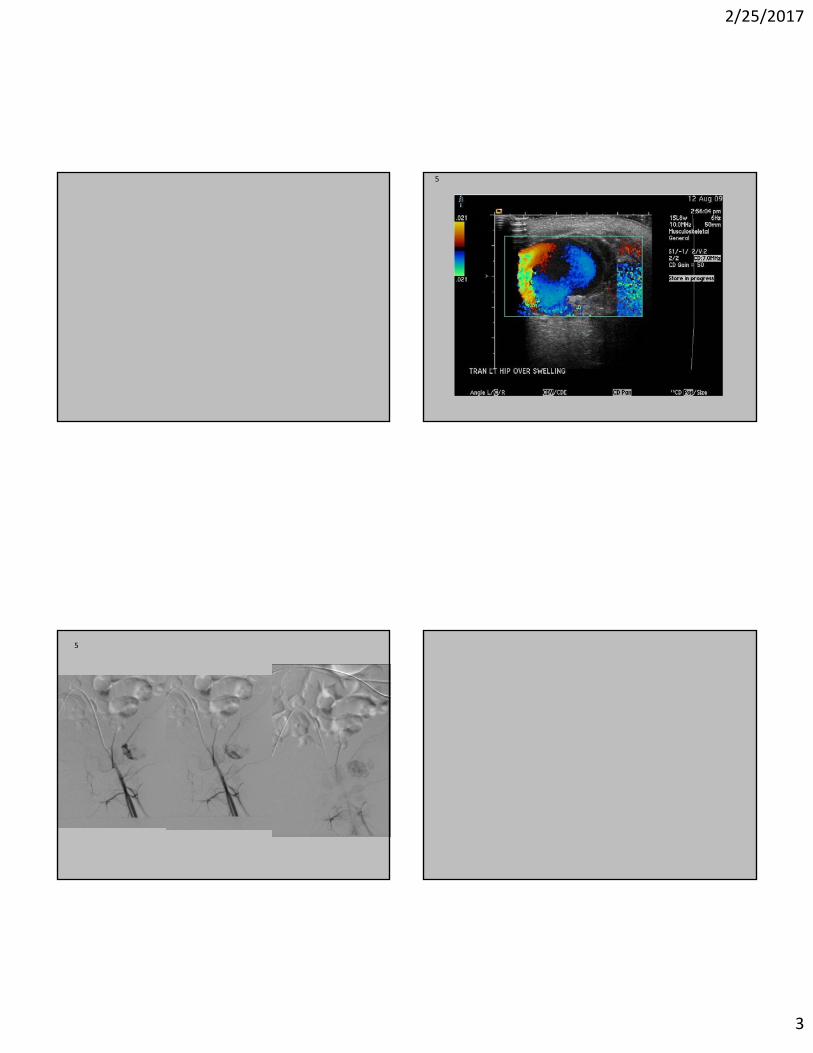
Pseudoaneurysm with AV Fistula
Right Renal Aneurysm & AV Fistula• Findings: Pseudoaneurysm and AV fistula right kidney. No vascularity seen in the superior pole of the right kidney. Surgical clip.
• Differential Diagnosis (Intra‐renal aneurysm)– Arteritis (Polyarteritis nodosa)– Drug use (speed kidney, cocaine)– Extrinsic compression (secondary)– Pseudoaneurysm (trauma, iatrogenic)
• Differential Diagnosis (AV Fistula / AVM)– Traumatic or iatrogenic– Congenital renal AVMs are rare
• Treatment:– Transcatheter embolization (detachable coils)– AVMs cyanoacrylate (glue)

2/25/2017
27
Case 11
2/25/2017
28
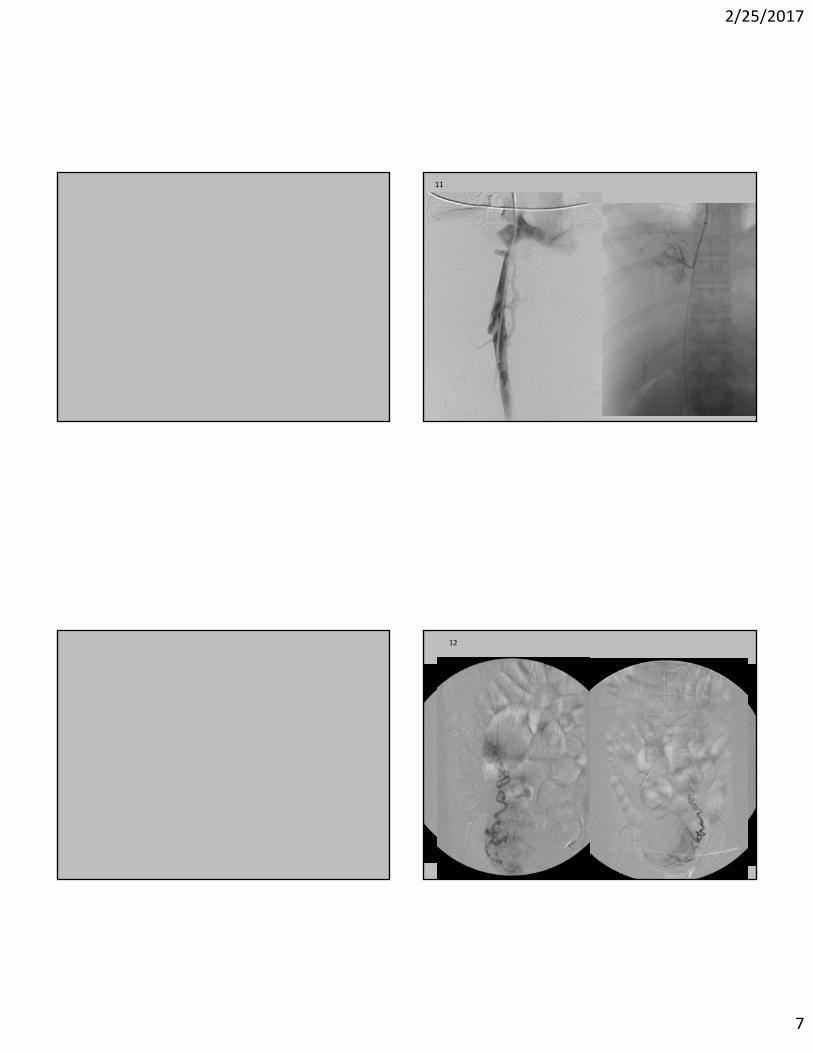
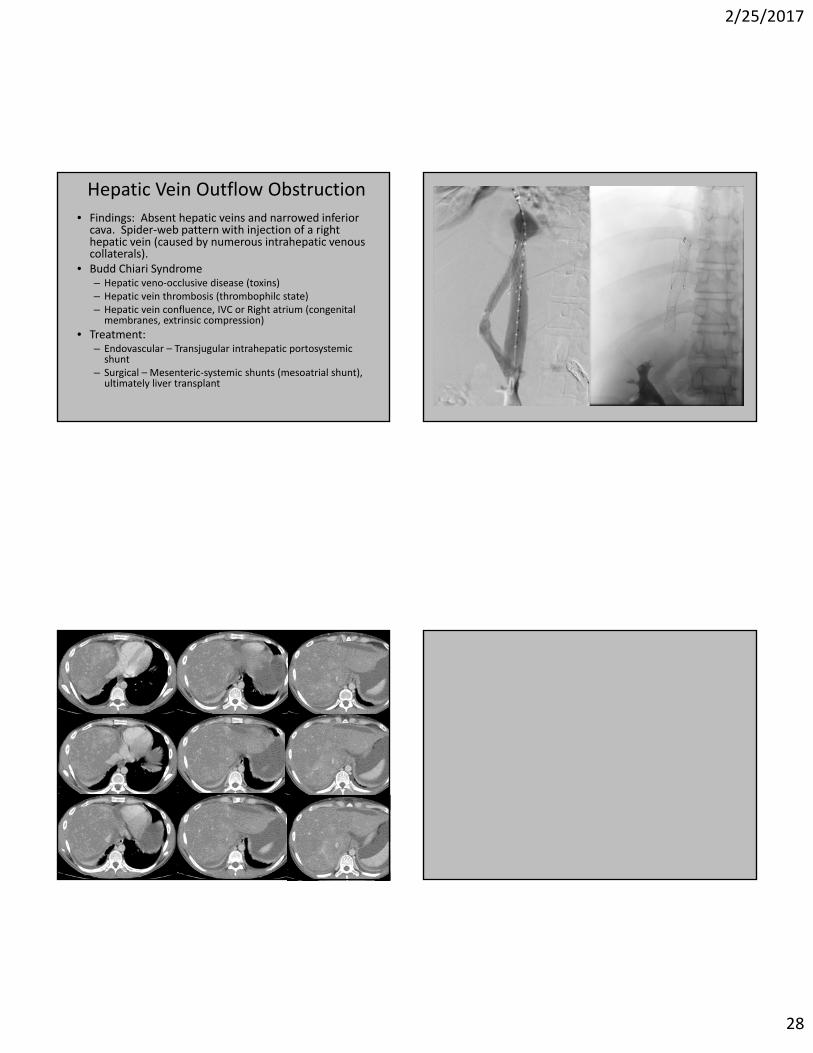
Hepatic Vein Outflow Obstruction
• Findings: Absent hepatic veins and narrowed inferior cava. Spider‐web pattern with injection of a right hepatic vein (caused by numerous intrahepatic venous collaterals).
• Budd Chiari Syndrome– Hepatic veno‐occlusive disease (toxins)– Hepatic vein thrombosis (thrombophilc state)– Hepatic vein confluence, IVC or Right atrium (congenital membranes, extrinsic compression)
• Treatment:– Endovascular – Transjugular intrahepatic portosystemic shunt
– Surgical – Mesenteric‐systemic shunts (mesoatrial shunt), ultimately liver transplant
2/25/2017
29
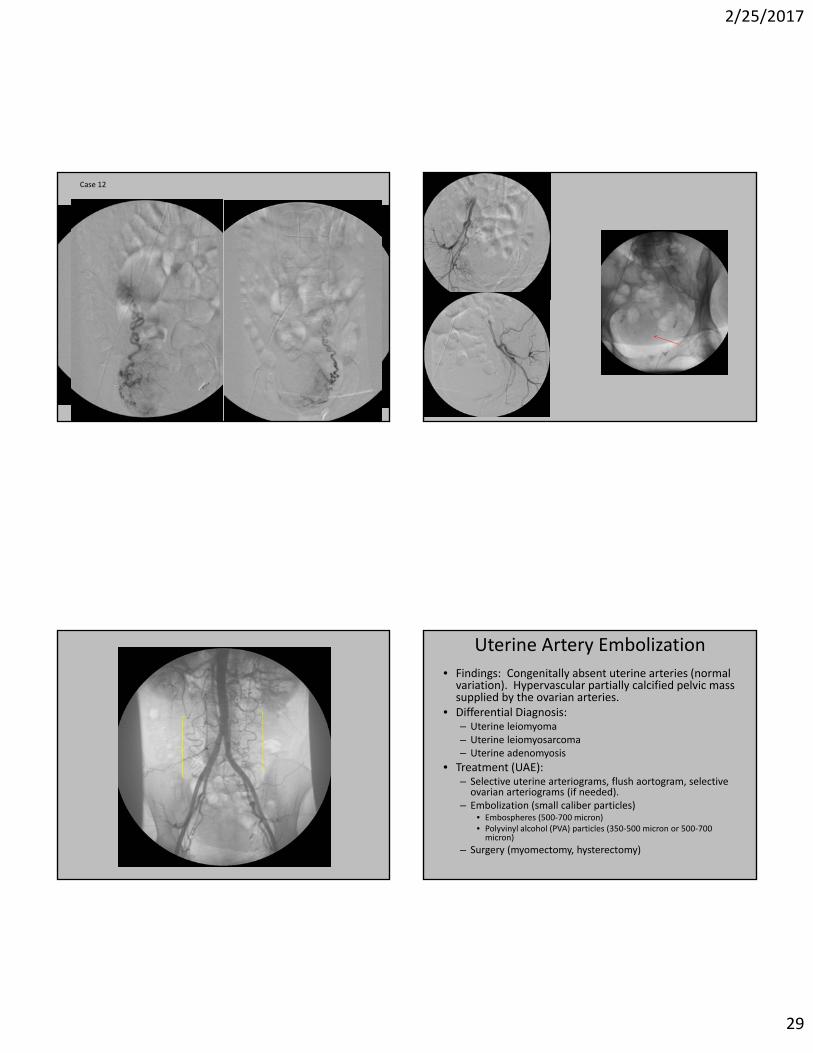
Case 12
Uterine Artery Embolization
• Findings: Congenitally absent uterine arteries (normal variation). Hypervascular partially calcified pelvic mass supplied by the ovarian arteries.
• Differential Diagnosis:– Uterine leiomyoma– Uterine leiomyosarcoma– Uterine adenomyosis
• Treatment (UAE):– Selective uterine arteriograms, flush aortogram, selective ovarian arteriograms (if needed).
– Embolization (small caliber particles)• Embospheres (500‐700 micron)• Polyvinyl alcohol (PVA) particles (350‐500 micron or 500‐700 micron)
– Surgery (myomectomy, hysterectomy)

2/25/2017
30
13
Abdominal Aortic Aneurysm
• Findings: AAA S/P Endograft. Enhancement in the aneurysm sac with a communication to the left common iliac artery.
• Differential Diagnosis:
– Endoleak (Which type?)
– Type Ib
• Treatment Options:
– Depends on endoleak type
Endoleaks Post AAA Repair
• Type I: Attachment: lack of seal between endograft and wall of artery
• Type II: Branch to branch: retrograde flow in IMA, lumbar, gonadal, or median sacral artery
• Type III: Device integrity: hole in graft material, separation of modular elements
• Type IV: Porous graft material: "bleed‐through" due to interstices in fabric of graft material
• Type V: Endo‐tension: No visible contrast or flow in aneurysm sac, but continued expansion
• Early: within 30 days of procedure• Late: after 30 days

2/25/2017
31
AAA Endoleak Treatment Options• Type I: Must be treated immediately.
– Place an extension at affected end– Place a balloon expandable or bare metal stent at the compromised
seal zone– Open repair
• Type II: May spontaneously thrombose– Embolization with either a transarterial or percutaneous approach– Open repair
• Type III: Must be treated immediately.– Stent‐graft extension to cover the separated modular component or
hole within the original graft– Realign endograft
• Type IV: Rare, Self limited and no treatment– Reverse anticoagulation
• Type V: Endo‐tension: No visible contrast or flow in aneurysm sac, but continued expansion. Consider additional imaging.– Open surgical repair is the only treatment
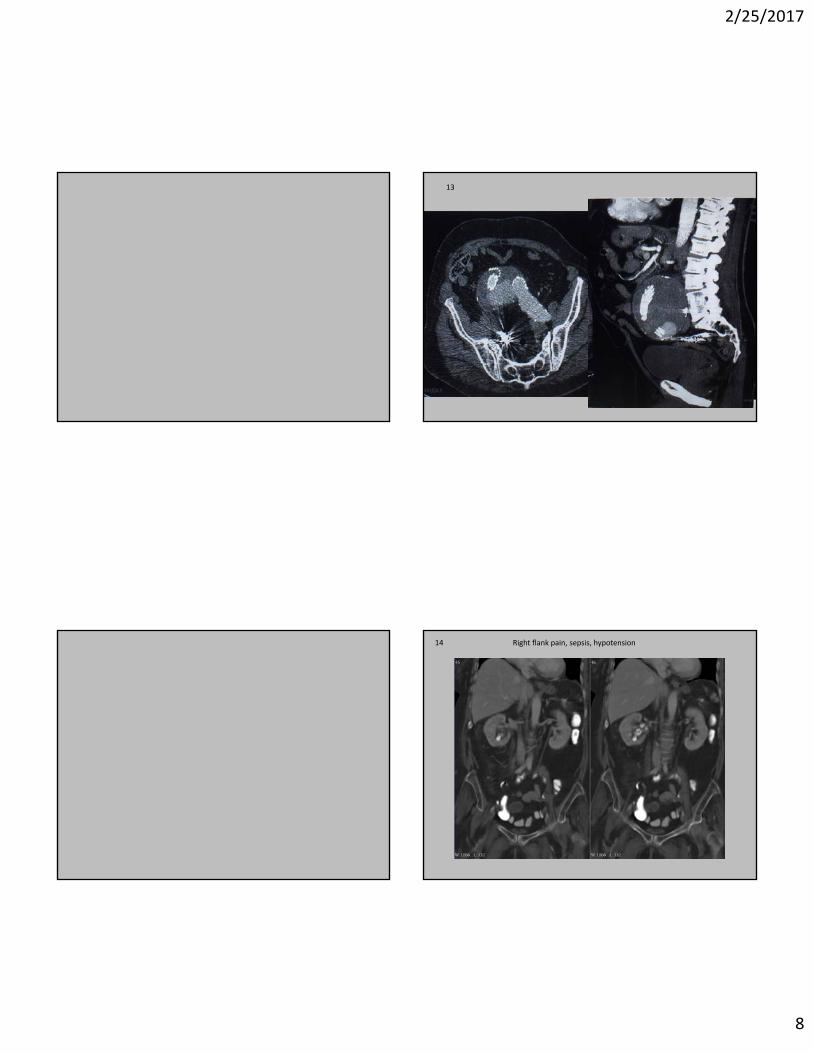
14 Right flank pain, sepsis, hypotension Urinary Obstruction• Findings: Staghorn calculus and hydroureter. Mild hydronephrosis better seen on additional images.
• Differential Diagnosis:– Nephrolithiasis
– Obstructing mass
– Blood clots in collecting system
– Papillary necrosis with sloughing
• Treatment (Proteus mirabilis):– Emergent decompression and antibiotics
– Percutaneous nephroureteral stent, bridge to lithotripsy.
2/25/2017
32
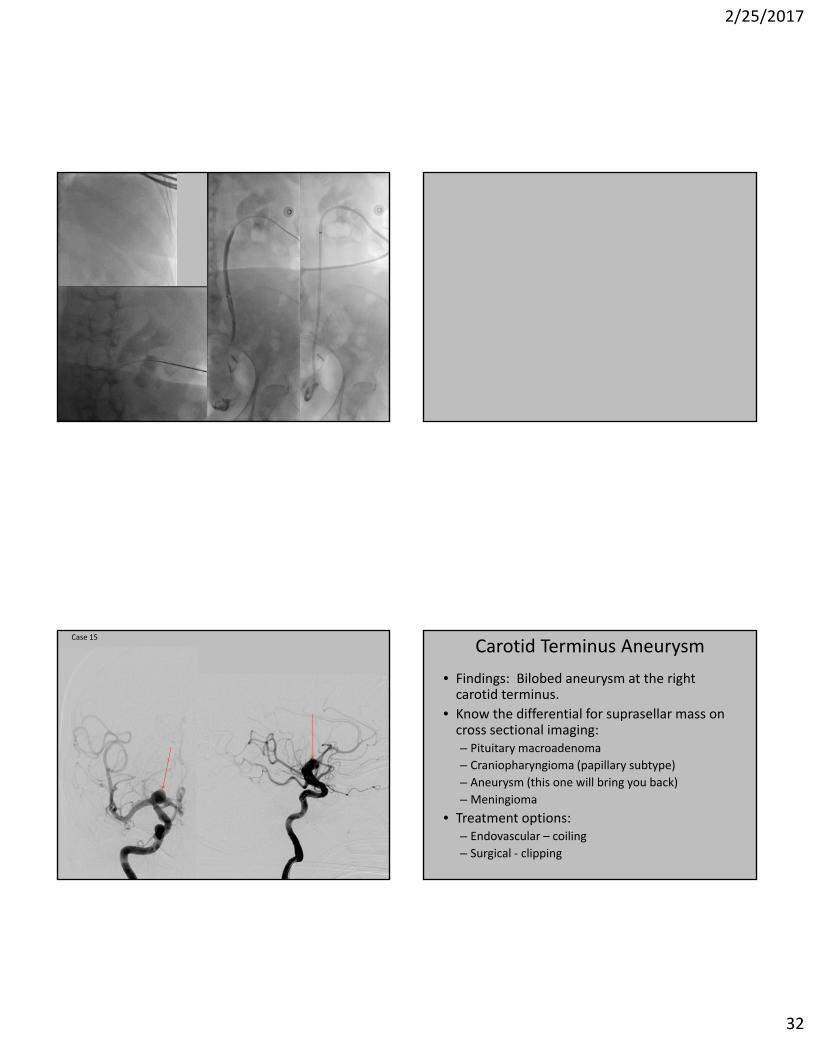
Case 15
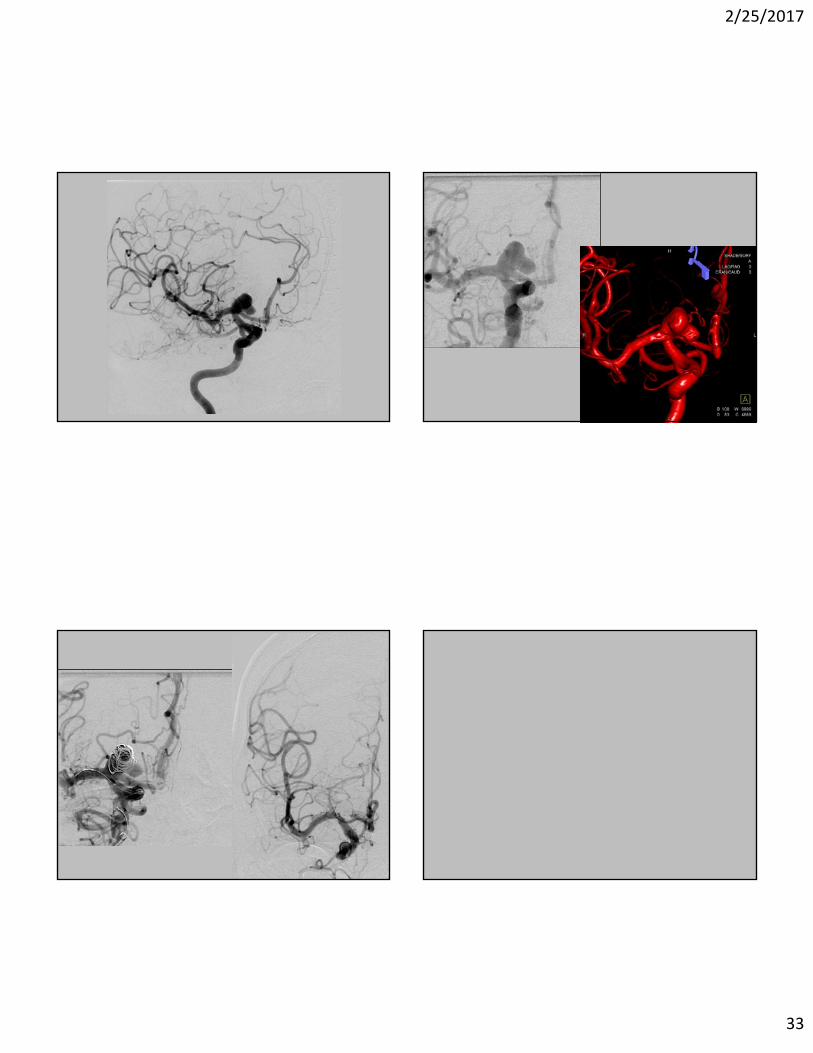
Carotid Terminus Aneurysm
• Findings: Bilobed aneurysm at the right carotid terminus.
• Know the differential for suprasellar mass on cross sectional imaging:– Pituitary macroadenoma
– Craniopharyngioma (papillary subtype)
– Aneurysm (this one will bring you back)
– Meningioma
• Treatment options:– Endovascular – coiling
– Surgical ‐ clipping
2/25/2017
33
2/25/2017
34
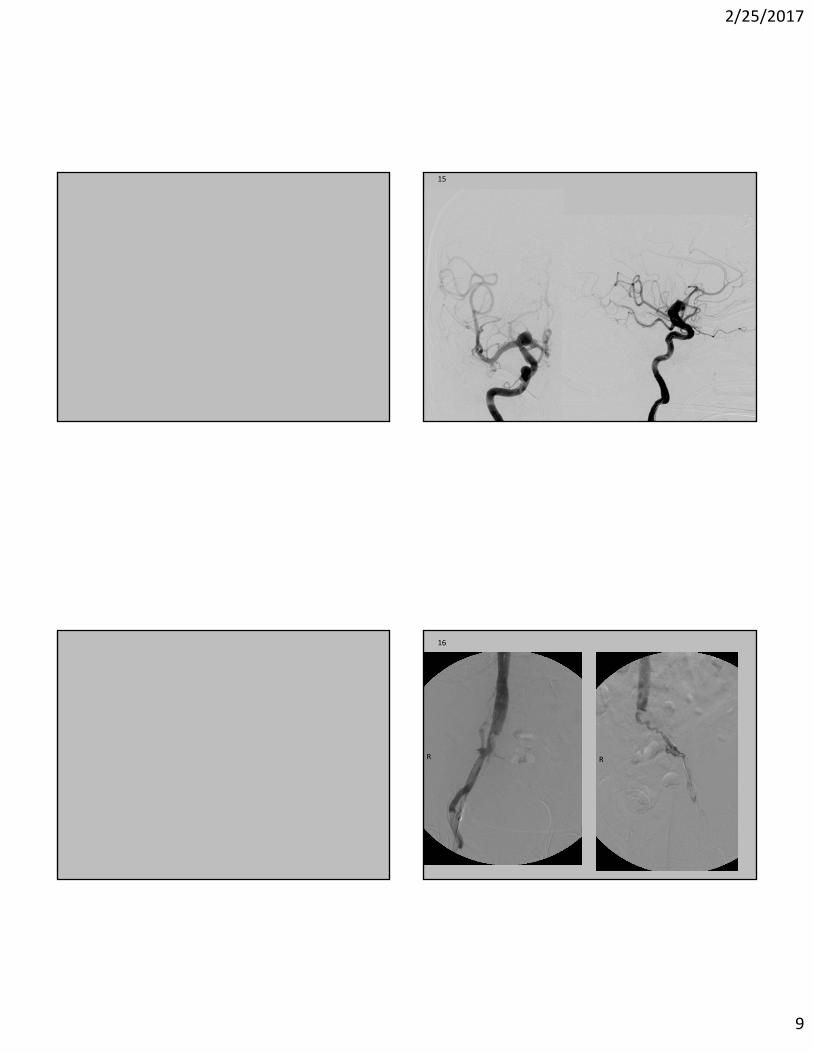
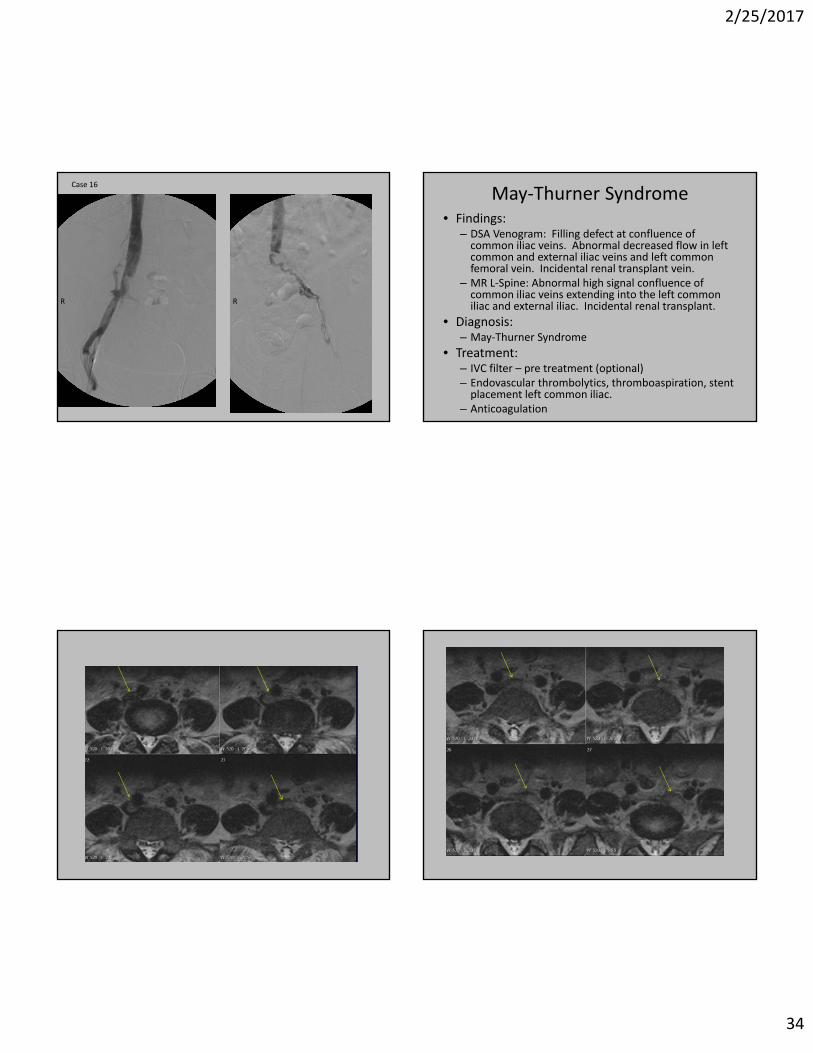
Case 16
R R
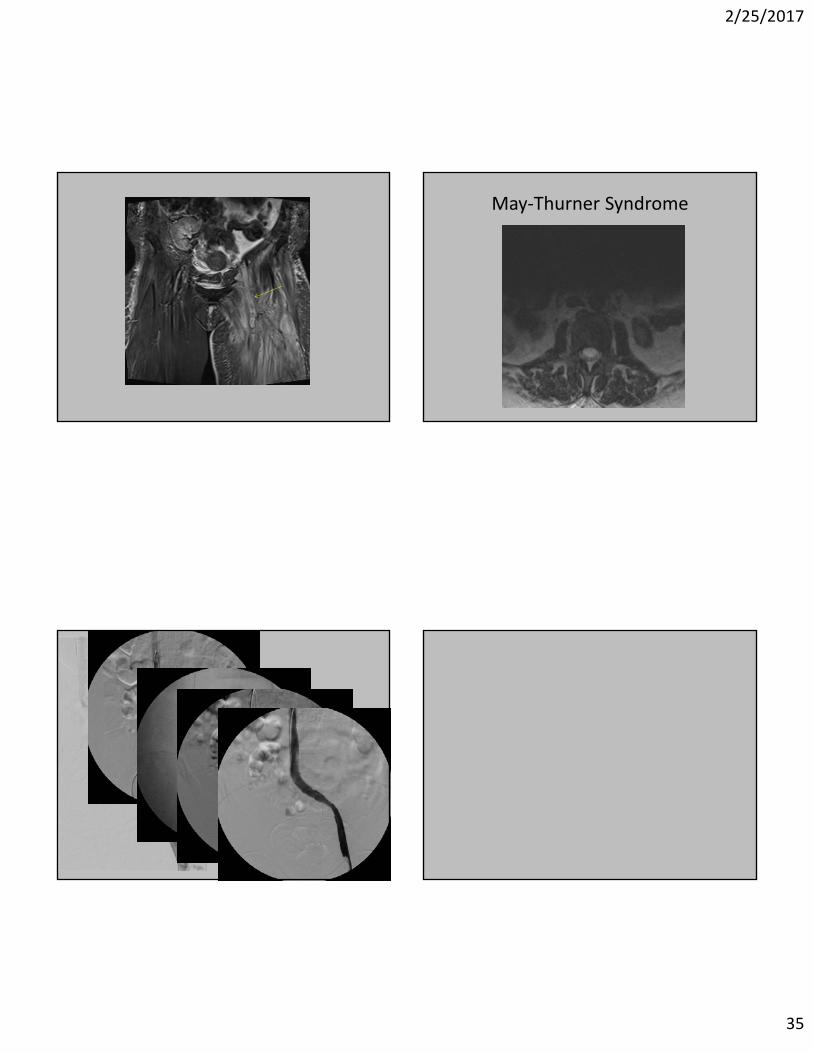
May‐Thurner Syndrome• Findings:
– DSA Venogram: Filling defect at confluence of common iliac veins. Abnormal decreased flow in left common and external iliac veins and left common femoral vein. Incidental renal transplant vein.
– MR L‐Spine: Abnormal high signal confluence of common iliac veins extending into the left common iliac and external iliac. Incidental renal transplant.
• Diagnosis:– May‐Thurner Syndrome
• Treatment:– IVC filter – pre treatment (optional)– Endovascular thrombolytics, thromboaspiration, stent placement left common iliac.
– Anticoagulation
2/25/2017
35
May‐Thurner Syndrome
2/25/2017
36
Case 17
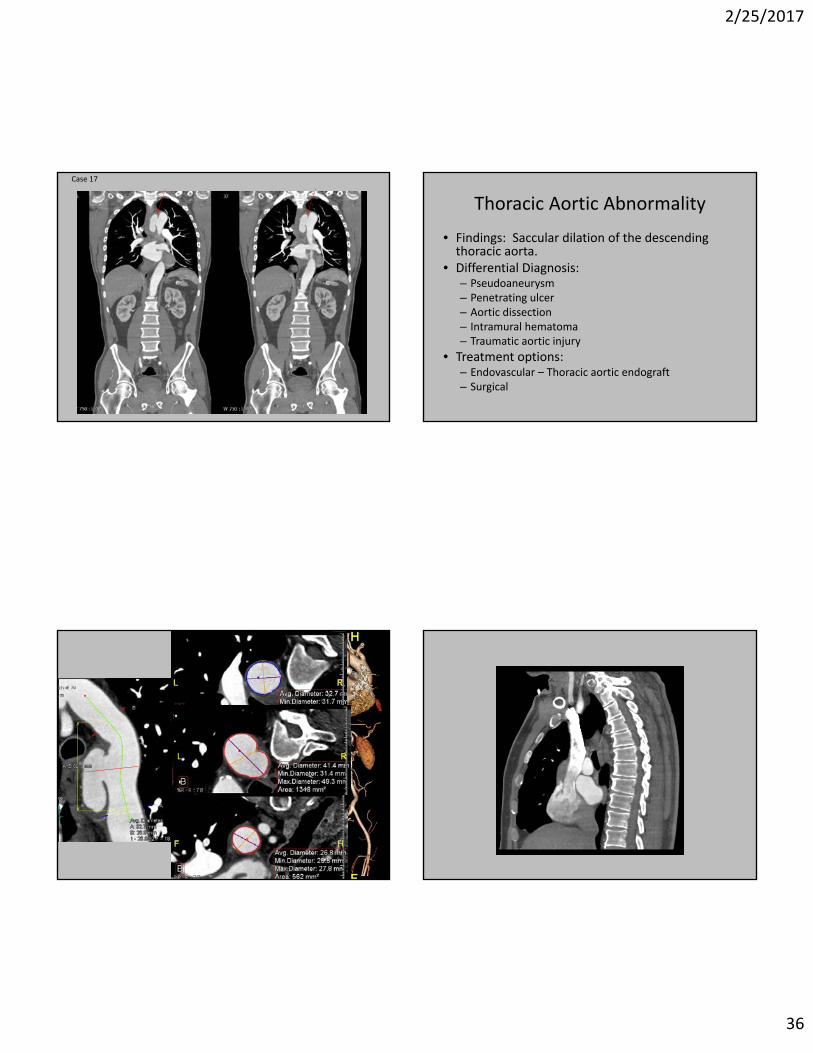
Thoracic Aortic Abnormality
• Findings: Saccular dilation of the descending thoracic aorta.
• Differential Diagnosis:– Pseudoaneurysm– Penetrating ulcer– Aortic dissection– Intramural hematoma– Traumatic aortic injury
• Treatment options:– Endovascular – Thoracic aortic endograft– Surgical
2/25/2017
37
Case 18
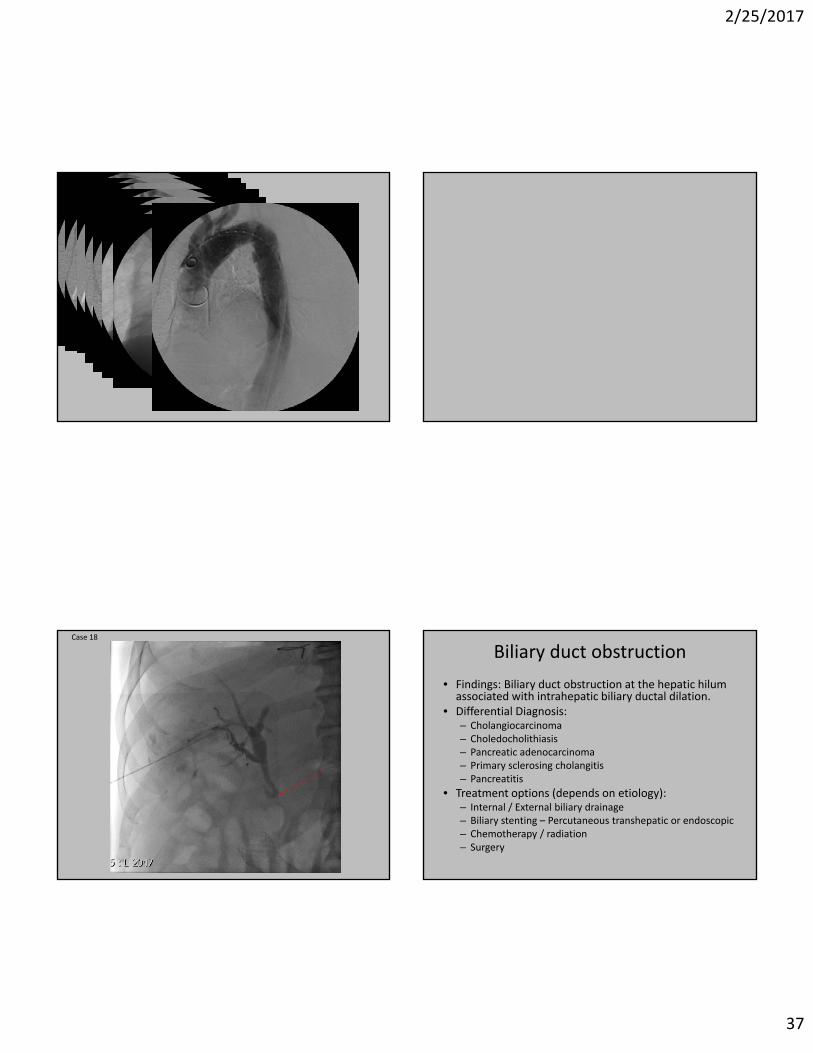
Biliary duct obstruction
• Findings: Biliary duct obstruction at the hepatic hilum associated with intrahepatic biliary ductal dilation.
• Differential Diagnosis:– Cholangiocarcinoma– Choledocholithiasis– Pancreatic adenocarcinoma– Primary sclerosing cholangitis– Pancreatitis
• Treatment options (depends on etiology):– Internal / External biliary drainage– Biliary stenting – Percutaneous transhepatic or endoscopic– Chemotherapy / radiation– Surgery
2/25/2017
38
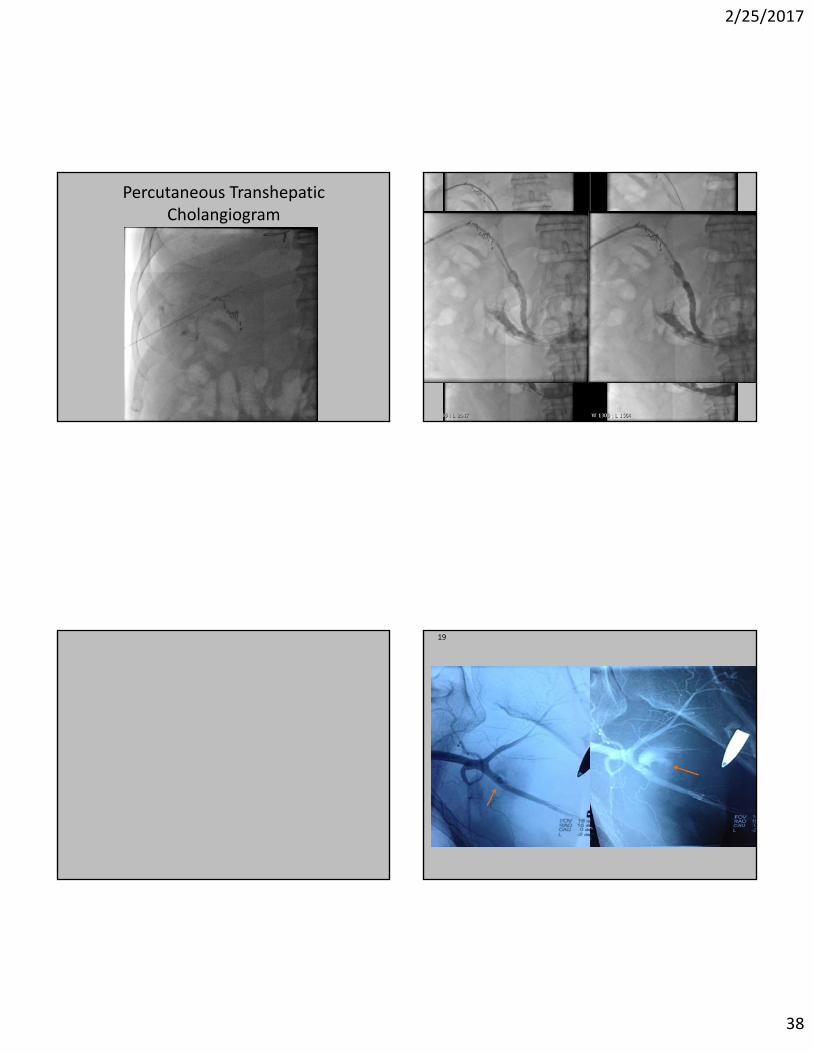
Percutaneous Transhepatic Cholangiogram
19
2/25/2017
39
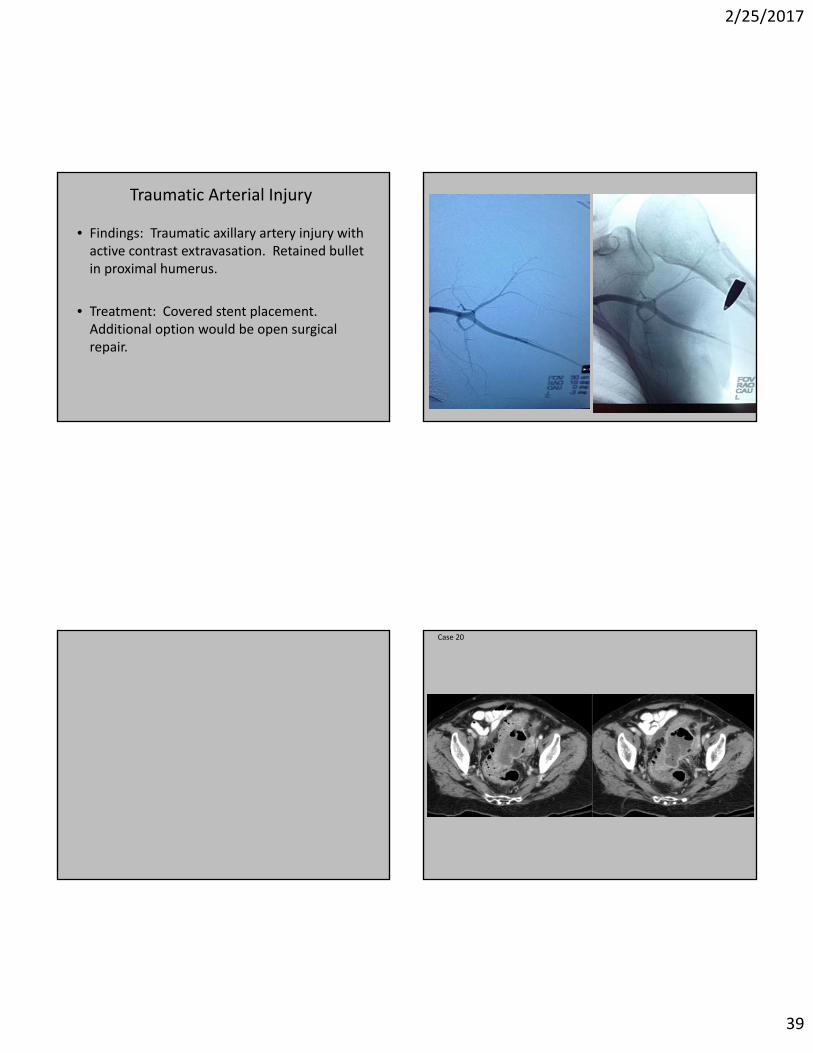
Traumatic Arterial Injury
• Findings: Traumatic axillary artery injury with active contrast extravasation. Retained bullet in proximal humerus.
• Treatment: Covered stent placement. Additional option would be open surgical repair.
Case 20
2/25/2017
40
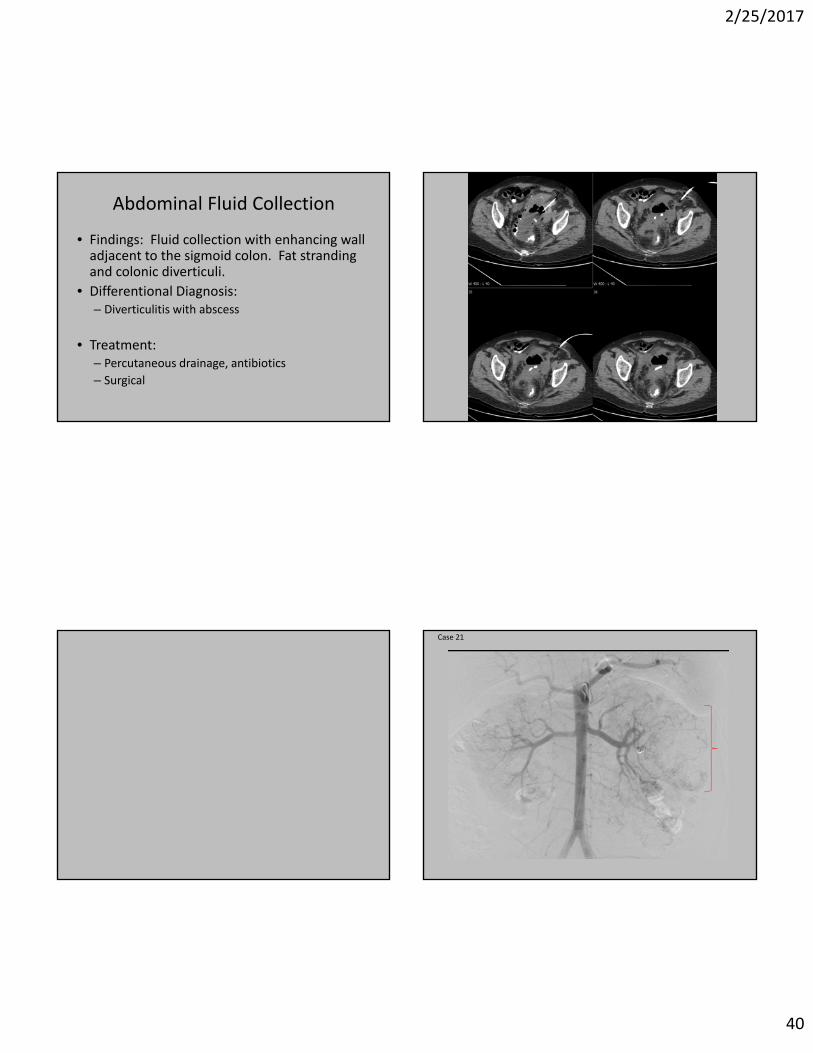
Abdominal Fluid Collection
• Findings: Fluid collection with enhancing wall adjacent to the sigmoid colon. Fat stranding and colonic diverticuli.
• Differentional Diagnosis:– Diverticulitis with abscess
• Treatment:– Percutaneous drainage, antibiotics
– Surgical
Case 21
2/25/2017
41
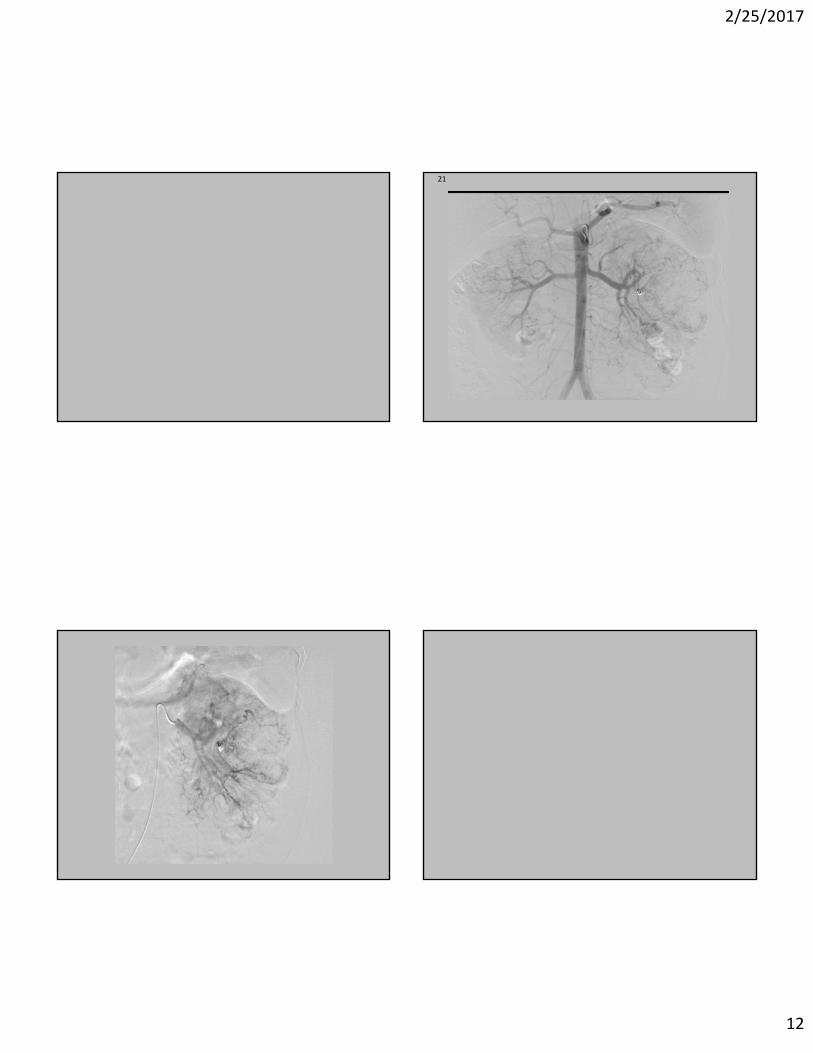
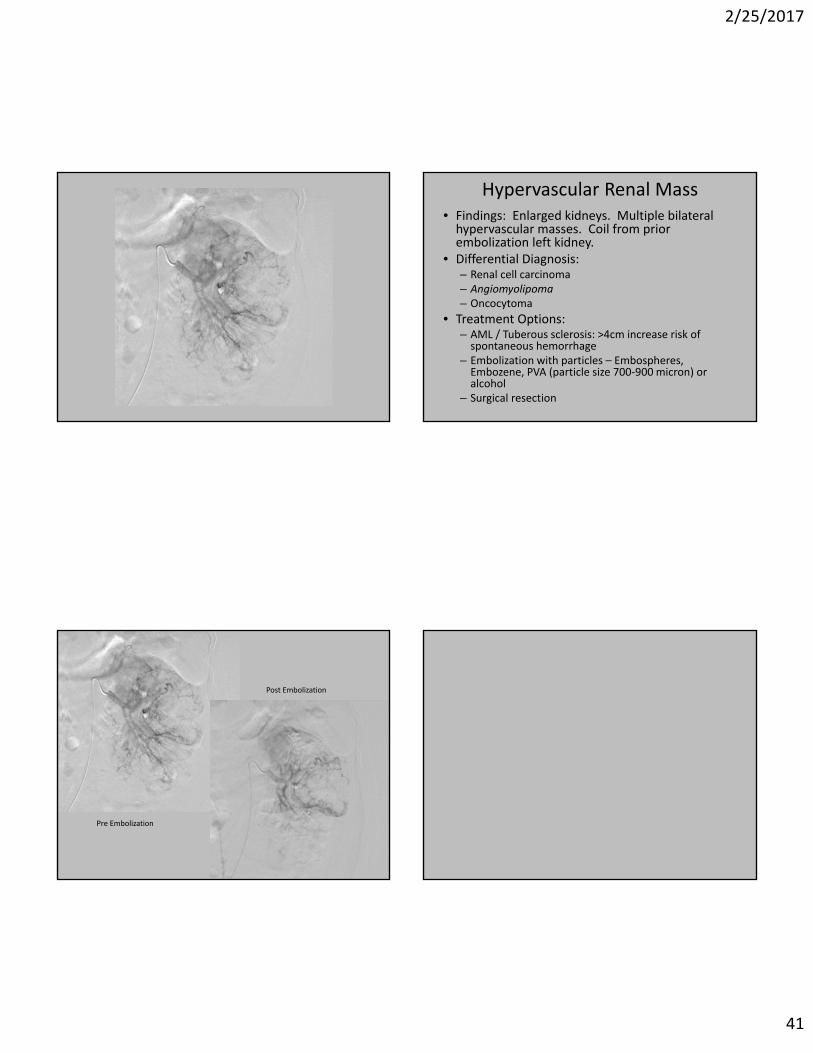
Hypervascular Renal Mass• Findings: Enlarged kidneys. Multiple bilateral hypervascular masses. Coil from prior embolization left kidney.
• Differential Diagnosis:– Renal cell carcinoma– Angiomyolipoma– Oncocytoma
• Treatment Options:– AML / Tuberous sclerosis: >4cm increase risk of spontaneous hemorrhage
– Embolization with particles – Embospheres, Embozene, PVA (particle size 700‐900 micron) or alcohol
– Surgical resection
Pre Embolization
Post Embolization

2/25/2017
42
Case 22
Hypervascular Intracranial Abnormality
• Findings: Hypervascular intracranial structure posteriorly with arterial supply from the right vertebral artery, demonstrating early venous drainage.
• Differential Diagnosis:– Arteriovenous malformation– Hypervascular mass– Moyamoya disease– Aneurysm
• Treatment Options:– Surgical ‐ Gamma Knife– Endovascular ‐ Onyx

2/25/2017
43
Case 23
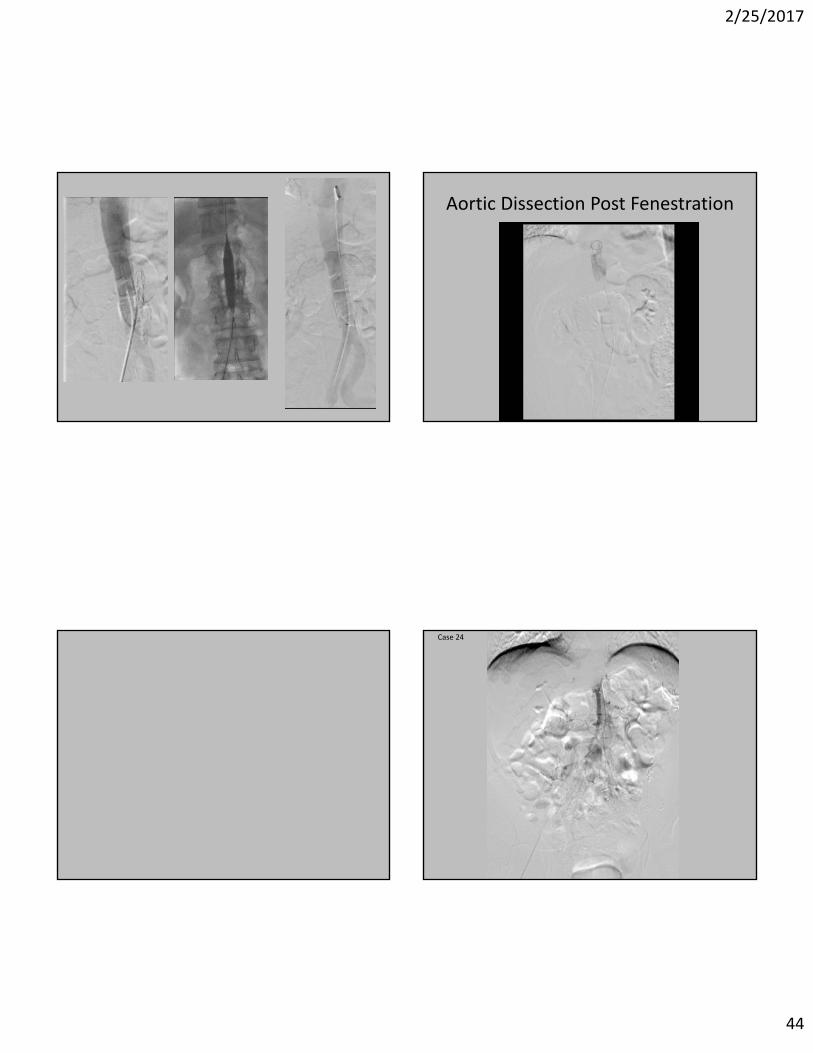
Aortic Dissection
• Findings: Intimal flap descending thoracic aorta and abdominal aorta. Infrarenal aorta not visualized. Dissection flap continuing into superior mesenteric artery with minimal arterial flow.
• Differential Diagnosis:– Hypertension– Trauma– Connective tissue disorder– Marfan syndrome– Bicuspid aortic valve– Coarctation of the aorta
• Treatment Options:– Stanford A: Surgical– Stanford B: Medical management, endovascular fenestration, surgical
if extends or end organ compromise
Type A
DeBakey I DeBakey II
Type B
DeBakey III
2/25/2017
44
Aortic Dissection Post Fenestration
Case 24

2/25/2017
45
Multiple Visceral Aneurysms
• Findings: Multiple aneurysms of the superior mesenteric artery branches.
• Differential Diagnosis:– Atherosclerosis
– Vasculitis (polyarteritis nodosa)
– Mycotic / septic emboli
– Trauma
• Treatment:– Depends on underlying etiology.
– Surgery
– ?stent graft
THANK YOU….
2/25/2017
46
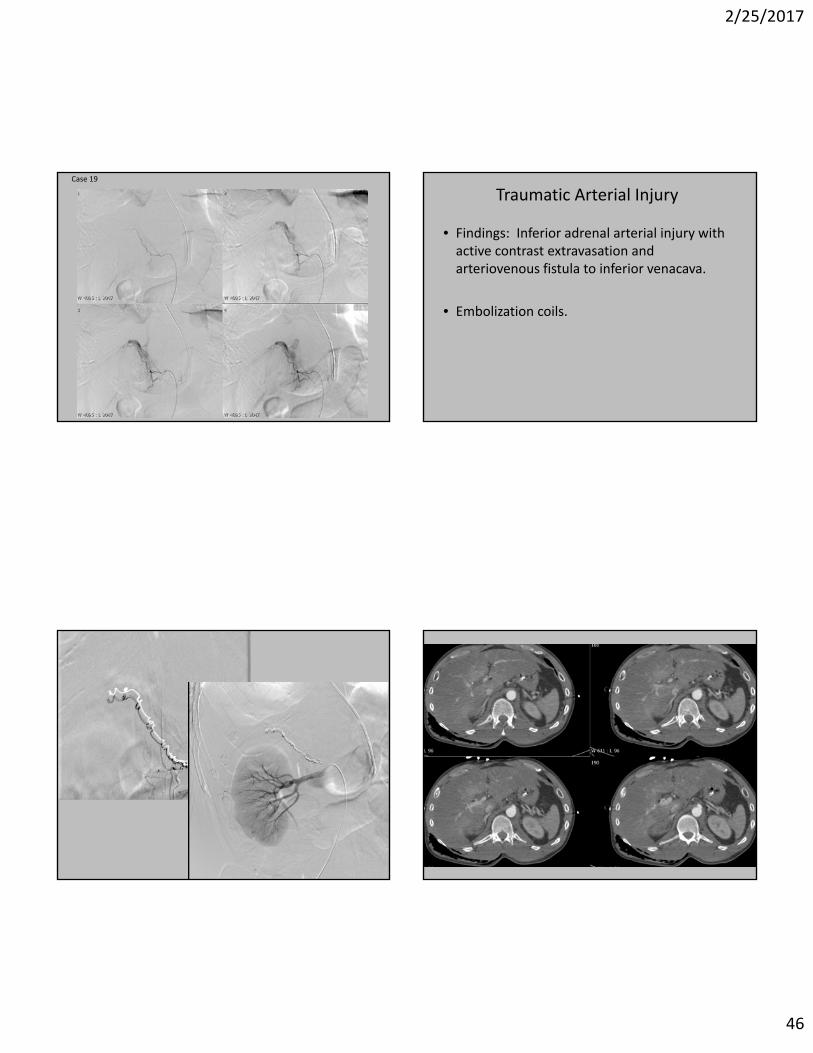
Case 19
Traumatic Arterial Injury
• Findings: Inferior adrenal arterial injury with active contrast extravasation and arteriovenous fistula to inferior venacava.
• Embolization coils.

2/25/2017
47
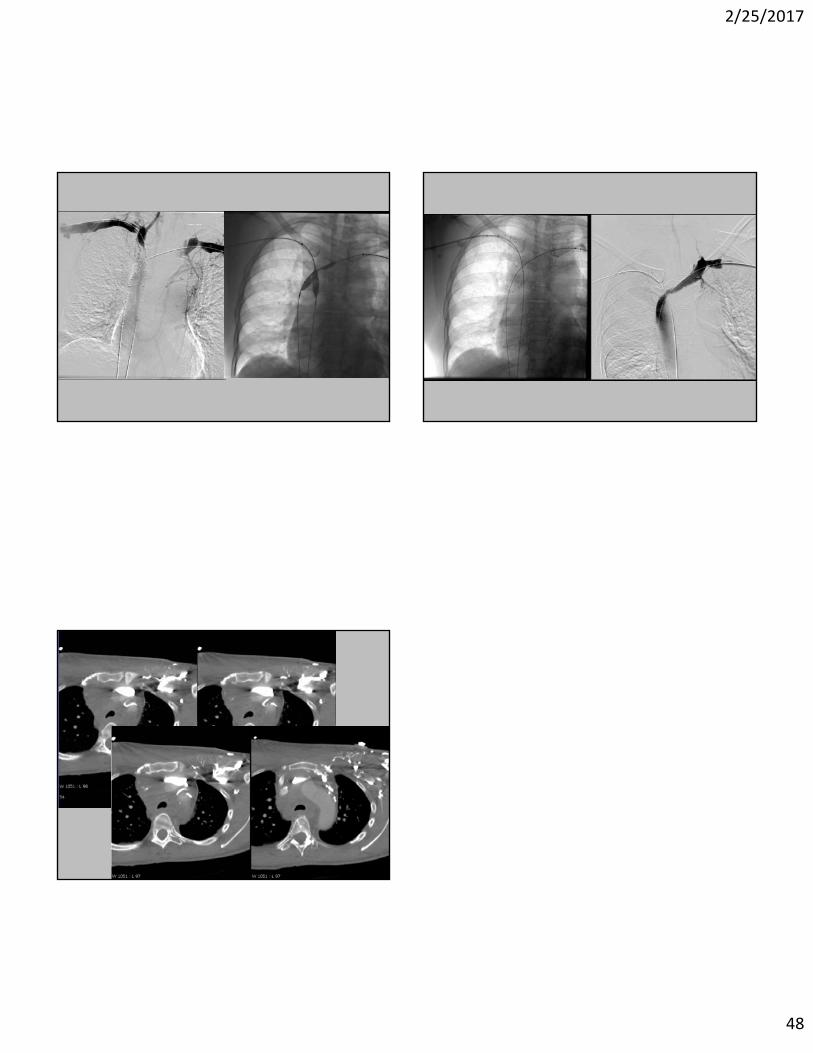
Case 6
• Findings: Occlusion of the bilateral brachiocephalic veins and superior venacava. Multiple collateral veins.
• Differential diagnosis:– Malignancy (lung ca, mediastinal tumor, 1° leiomyosarcoma)– Radiation therapy– Intimal injury (vascular catheters or devices)– Chemotherapeutic agents– Trauma– Fibrosing mediastinitis– Aortic or brachiocephalic aneurysm– Infection
• Treatment– Endovascular vs. radiation vs. chemotherapy vs. surgical (rare)– Combination
SVC Syndrome
2/25/2017
48