Embed Size (px)
Citation preview
Ventilation and health in non-industrial indoor environments:
report from a European Multidisciplinary Scientific Consensus
Meeting (EUROVEN)
Introduction
Ventilation is the process of exchanging indoor (pol-luted) air with outdoor (presumably fresh and clean)air. Its main purpose is to create optimal conditions for
humans in indoor environments, taking into accounttheir health, comfort, and productivity by providing airfor breathing, for removing and diluting indoorpollutants, for adding or removing moisture, and forheating or cooling.
Abstract Scientific literature on the effects of ventilation on health, comfort, andproductivity in non-industrial indoor environments (offices, schools, homes, etc.)has been reviewed by a multidisciplinary group of European scientists, calledEUROVEN, with expertise in medicine, epidemiology, toxicology, and engin-eering. The group reviewed 105 papers published in peer-reviewed scientificjournals and judged 30 as conclusive, providing sufficient information on ven-tilation, health effects, data processing, and reporting, 14 as providing relevantbackground information on the issue, 43 as relevant but non-informative orinconclusive, and 18 as irrelevant for the issue discussed. Based on the data inpapers judged conclusive, the group agreed that ventilation is strongly associatedwith comfort (perceived air quality) and health [Sick Building Syndrome (SBS)symptoms, inflammation, infections, asthma, allergy, short-term sick leave], andthat an association between ventilation and productivity (performance of officework) is indicated. The group also concluded that increasing outdoor air supplyrates in non-industrial environments improves perceived air quality; that out-door air supply rates below 25 l/s per person increase the risk of SBS symptoms,increase short-term sick leave, and decrease productivity among occupants ofoffice buildings; and that ventilation rates above 0.5 air changes per hour (h)1) inhomes reduce infestation of house dust mites in Nordic countries. The groupconcluded additionally that the literature indicates that in buildings with air-conditioning systems there may be an increased risk of SBS symptoms comparedwith naturally or mechanically ventilated buildings, and that improper main-tenance, design, and functioning of air-conditioning systems contributes toincreased prevalence of SBS symptoms.
P. Wargocki1*, J. Sundell1**,W. Bischof2, G. Brundrett3,P. O. Fanger1, F. Gyntelberg4,S. O. Hanssen5, P. Harrison6,A. Pickering7, O. Sepp)nen8,P. Wouters91Technical University of Denmark, Kongens Lyngby,Denmark, 2Friedrich-Schiller-Universit�t Jena, Erfurt,Germany, 3 Royal Society of Health, London, UnitedKingdom, 4Bispebjerg Hospital, Copenhagen, Denmark,5Norwegian University of Science and Technology,Trondheim, Norway, 6MRC Institute for Environmentand Health, Leicester, United Kingdom, 7WythenshaweHospital, Manchester, United Kingdom, 8HelsinkiUniversity of Technology, Espoo, Finland, 9BelgianBuilding Research Institute, Brussels, Belgium
Key words: Ventilation; Outdoor air supply rate;Ventilation system; Non-industrial indoor environments;Offices; Schools; Homes; Health; EUROVEN.
P. WargockiInternational Center for Indoor Environment and Energy,Technical University of Denmark, Building 402DK-2800 Kongens Lyngby, DenmarkTel.: +45 45 25 40 11Fax: +45 45 93 21 66e-mail: [email protected]*Scientific Secretary.**Chairman and project leader.
Received for review 27 June 2001. Accepted forpublication 20 July 2001.� Indoor Air (2002)
Practical ImplicationsVentilation requirements in many existing guidelines and standards may be too low to protect occupants of offices,schools, and homes from health and comfort problems and may not be optimal for human productivity. Higherventilation rates can increase energy costs in relation to building operation, but these can be reduced by loweringpollution loads on the air indoors, e.g., by prudent and systematic maintenance of heating/ventilation/air-conditioning(HVAC) systems and by reducing superfluous pollution sources indoors. Energy costs can also be reduced by usingefficient heat recovery systems. Source control and new ways of conditioning air are required.
Indoor Air 2002; 12: 113–128http://www.blackwellmunksgaard.comPrinted in Denmark. All rights reserved
Copyright � Blackwell Munksgaard 2002
INDOOR AIRISSN 0905-6947
113
Several literature reviews have been published on theeffects of ventilation on health. Their main andcommon conclusion was that the ventilation rates ator below 10 l/s per person can significantly aggravatehealth outcomes, mainly Sick Building Syndrome(SBS) symptoms (Godish and Spengler, 1996; Mendell,1993; Menzies and Bourbeau, 1997; Seppanen et al.,1999) and that there is an indication that increasing theventilation rate from 10 l/s per person up to 20 l/s perperson may further reduce SBS symptoms (Seppanenet al., 1999). The reviews have shown, additionally,that an increased prevalence of SBS symptoms isassociated with the use of air-conditioning in buildings(Mendell and Smith, 1990; Menzies and Bourbeau,1997). These literature reviews included studies pub-lished in peer-reviewed journals and in conferenceproceedings without scrutinizing their scientific merit ina multidisciplinary fashion as in, e.g. Nordic interdis-ciplinary reviews (Sundell and Bornehag, 1999). Con-sequently, the European Multidisciplinary ScientificNetwork on Indoor Environment and Health con-cerning associations between ventilation and health(EUROVEN) was established in order to create amultidisciplinary forum for adequate communicationof scientific results between different disciplines. Thepurpose of EUROVEN is to define the link betweenventilation and health in non-industrial indoor envi-ronments. To reach this goal, scientists with anexpertise in medicine, epidemiology, toxicology, andengineering reviewed the peer-reviewed scientific stud-ies coming with the scope of EUROVEN. The presentpaper describes their work and the final consensusstatement reached by the EUROVEN group.
Methods
The scientific peer-reviewed literature on the effects ofventilation on health in non-industrial indoor environ-ments was reviewed by a multidisciplinary group ofEuropean scientists with expertise in medicine, epi-demiology, toxicology, and engineering. In the presentwork, the term �ventilation� describes both the ventila-tion rate, i.e. the amount of outdoor air supplied toindoor spaces unless otherwise indicated, and theventilation system, i.e. the way the air is supplied toindoor spaces – naturally or mechanically, with orwithout air-conditioning. Natural ventilation is definedas an airflow caused by pressure from wind and/orindoor–outdoor temperature differences. Mechanicalventilation is defined as an airflow caused by a fanthrough intake and/or exhaust vents specificallyinstalled for ventilation (ASHRAE, 1993). Mechanicalventilation without air-conditioning is defined as amechanical ventilation system in which the supply air isfiltered and heated, or in which the air is exhausted bya fan. Mechanical ventilation with air-conditioning isdefined as a mechanical ventilation system in which the
supply air is filtered and heated, and is additionallycooled and/or humidified and/or dehumidified. Healthis understood very broadly reflecting the basic defini-tion of the World Health Organization (WHO, 1948),which states that health is a state of complete physical,mental, and social well-being and not merely theabsence of disease or infirmity. Consequently, studieson the effects of ventilation on human comfort andproductivity were also taken into account. Non-indus-trial indoor environments are represented by all kindsof indoor environments not related to industrialexposures.The scientific literature was gathered by searching
through the following databases: MEDLINE byNational Library of Medicine; Cambridge ScientificAbstracts (including Mechanical EngineeringAbstracts, Environmental Sciences, and PollutionManagement Search subfiles, Biological SciencesSearch subfiles, TOXLINE, ERIC, Computer andInformation System Abstracts) and AIRBASE by theAir Infiltration and Ventilation Center (AIVC). Theselected databases cover papers published in scientificjournals from 1966 (two earlier papers from 1936 and1955 were also included in the review). Four categoriesof search profiles were established: ventilation, envi-ronment, health, and publication, each with severalsearching records. As a source of search records,keyword indexes of the international conferencesIndoor Air 1990, 1993 and 1999, and Healthy Build-ings 1997 and 2000, were used. Only papers with title,keywords or abstract including records in each of thefour search categories were selected. The category�ventilation� included 25 different records pertaining toventilation rates, e.g. air change rate, air supply rate,etc., as well as ventilation systems, e.g. natural venti-lation, mechanical ventilation, etc. The category �envi-ronment� included 49 different records pertaining tonon-industrial indoor environments, e.g. dwellings,schools, offices, etc. The category �health� included 91different records pertaining to health, comfort, andproductivity, e.g. symptoms, diseases, odor, perceivedair quality, absenteeism, productivity, asthma, etc. Thecategory �publication� included three records pertainingto peer-reviewed publications: journal article, journalpaper, ASHRAE Transactions.More than 200 papers were gathered by searching
databases. They were then screened through theirabstracts to exclude articles that did not pertain to theEUROVEN scope, reviews, as well as the papersconcerning Legionnaires disease, humidifier fever, andradon. After this initial screening, 105 papers wereselected and thoroughly reviewed by nine scientists.Each paper was reviewed by two scientists, oneassigned to be a prime reviewer and the other oneassigned to be secondary reviewer. Each scientistreviewed 23 or 24 papers, half of them as primereviewer. The articles were assigned to scientists for
Wargocki et al.
114

review completely at random; however, no paper wasassigned to a scientist if he was one of the authors.When reviewing the paper, information on differentaspects of the study was collected including design,methods, data analysis, measurements of airflow ratesand effects on health, possible bias, etc., its results andmain conclusions. Reviewed papers were then classifiedas: relevant and conclusive – providing sufficientinformation on ventilation, health effects, data pro-cessing, and reporting; relevant but non-informative –lacking essential information concerning ventilation orhealth effects; relevant but inconclusive – with incom-plete data processing or reporting; background articles– providing additional background information deal-ing with the EUROVEN scope; irrelevant – not dealingwith the EUROVEN scope or describing case studies.Classification of each paper was first made independ-ently by each reviewer. Then, during the plenarymeeting, the whole group decided on a final classifica-tion. The data in the papers judged during plenarydiscussions of the whole EUROVEN group as conclu-sive were used to formulate the final consensusstatement and conclusions.
Results
Of the 105 papers reviewed by the group (see thesubsection in the References for the complete list), 61papers were excluded: 18 were judged to provideinformation that was irrelevant to the scope of thepresent work or were classified as case studies(marked by an asterix, *, in the reference list), and43 were judged to be either non-informative orinconclusive. Of the remaining 44 papers, 14 werejudged to provide background information relevantto the EUROVEN scope and 30 were judgedconclusive and thus used to formulate the consensusstatement. Thirty papers judged as conclusive werepublished in 17 different peer-reviewed scientificjournals (Table 1) with specialties ranging fromengineering to medical sciences, epidemiology, occu-pational hygiene, and allergy, and described ninestudies carried out in the USA and 21 in Europe, ofwhich 17 were conducted in European Nordic coun-tries (Denmark, Finland, Norway, Sweden). Thestudies were carried out in more than 1000 buildingscomprising offices, assembly halls, schools, homes,jails, and nursery homes with more than 65,000occupants comprising children, adults, and seniorcitizens. Most studies were carried out during thewinter, spring or autumn season.Table 2 lists the papers judged by the group to be
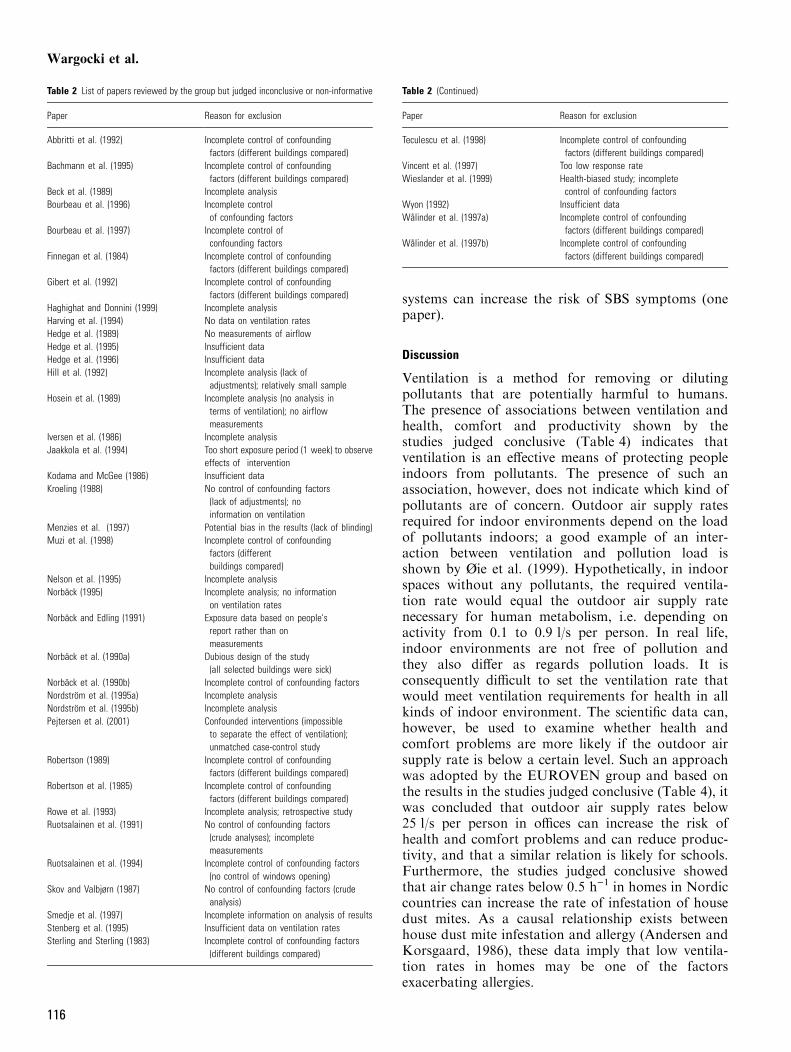
non-informative or inconclusive and provides thereason for such classification, which was mainly thelack of proper statistical analysis and control ofconfounding factors. Many of the papers listed inTable 2 assumed that outdoor air was clean, that
heating/ventilation/air-conditioning (HVAC) systemswere cleaned, and that pollution loads in differentbuildings were similar; many of them did not mentionwhether the air was recirculated or whether themeasured airflow rate was the total or the outdoorair supply rate.Table 3 shows data from 14 papers providing back-
ground information for the EUROVEN work. Theydescribe experimental studies on ventilation require-ments to control perceived air quality in spacespolluted by bioeffluents emitted by humans, in spacespolluted by tobacco smoke, and in spaces polluted byemissions from building materials, and experimentsshowing that HVAC system components can aggravatethe perceived air quality in spaces. They also presentstudies investigating the association between mortalityin hot weather and the presence of air-conditioning,thus indicating a positive thermal impact of air-conditioning on human health, as well as studiesindicating that increasing the ventilation rate candecrease the risk of infections.The data from 22 papers judged by the group to be
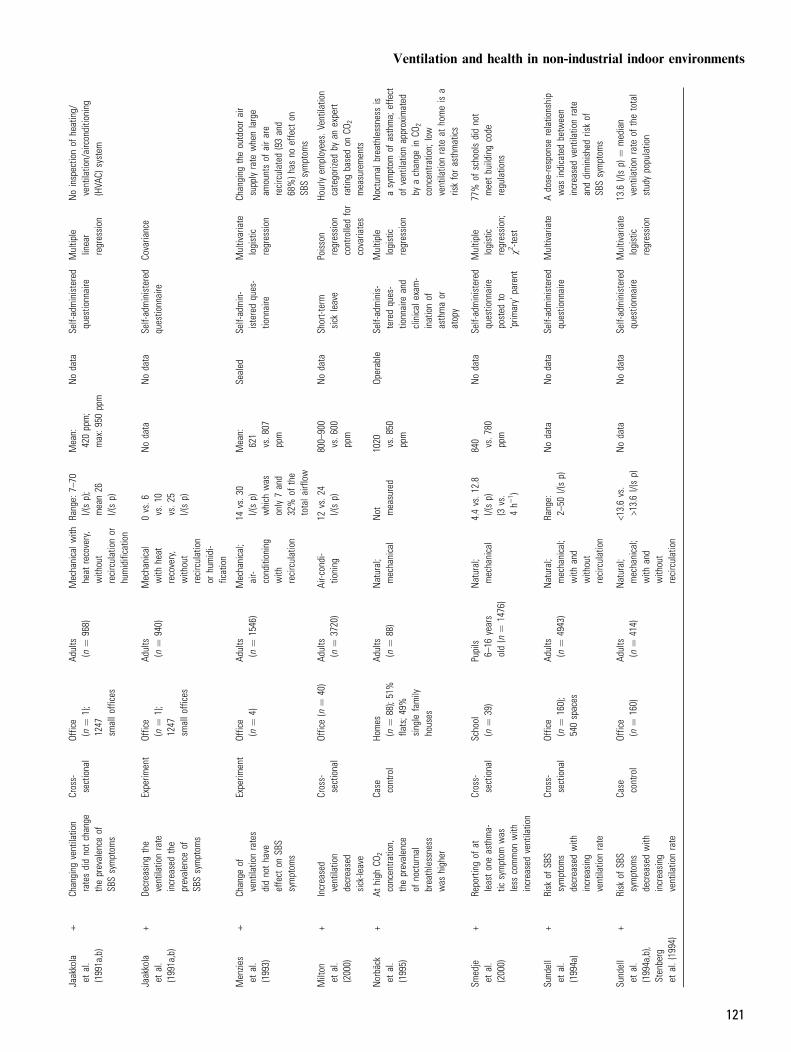
conclusive, presented in Table 4, show that increasingthe ventilation rate improves perceived air quality,decreases the prevalence of SBS symptoms and theintensity of clinical symptoms, reduces absenteeism, andimproves the performance of office work; only in twostudies was no effect of a changed ventilation rateobserved (Jaakkola et al., 1991a,b; Menzies et al.,1993). The outdoor air supply rates in the studiespresented in Table 4 ranged from 0 to 50 l/s per person.The data from nine papers judged by the group to
be conclusive, presented in Table 5, suggest that therisk of SBS symptoms is higher in air-conditionedbuildings compared with naturally or mechanicallyventilated buildings (six of seven papers), that therisk of infections increases with the presence ofrecirculation (one paper), and that dirty HVAC
Table 1 List of scientific journals in which the papers judged relevant were published
Journal name No. of papers
Allergy 2American Journal of Epidemiology 1Annals of Occupational Hygiene 1Applied Occupational and Environmental Hygiene 1Archives of Environmental Health 1Energy and Buildings 2Environment International 2Epidemiology 2Indoor Air 8International Archives of Occupational and Environmental Health 1International Journal of Epidemiology 1JAMA ) Journal of the American Medical Association 1Journal of Allergy and Clinical Immunology 1Journal of the American Geriatrics Society 1New England Journal of Medicine 2Occupational and Environmental Medicine 2Scandinavian Journal of Work, Environment & Health 1
Ventilation and health in non-industrial indoor environments
115
systems can increase the risk of SBS symptoms (onepaper).
Discussion
Ventilation is a method for removing or dilutingpollutants that are potentially harmful to humans.The presence of associations between ventilation andhealth, comfort and productivity shown by thestudies judged conclusive (Table 4) indicates thatventilation is an effective means of protecting peopleindoors from pollutants. The presence of such anassociation, however, does not indicate which kind ofpollutants are of concern. Outdoor air supply ratesrequired for indoor environments depend on the loadof pollutants indoors; a good example of an inter-action between ventilation and pollution load isshown by Øie et al. (1999). Hypothetically, in indoorspaces without any pollutants, the required ventila-tion rate would equal the outdoor air supply ratenecessary for human metabolism, i.e. depending onactivity from 0.1 to 0.9 l/s per person. In real life,indoor environments are not free of pollution andthey also differ as regards pollution loads. It isconsequently difficult to set the ventilation rate thatwould meet ventilation requirements for health in allkinds of indoor environment. The scientific data can,however, be used to examine whether health andcomfort problems are more likely if the outdoor airsupply rate is below a certain level. Such an approachwas adopted by the EUROVEN group and based onthe results in the studies judged conclusive (Table 4), itwas concluded that outdoor air supply rates below25 l/s per person in offices can increase the risk ofhealth and comfort problems and can reduce produc-tivity, and that a similar relation is likely for schools.Furthermore, the studies judged conclusive showedthat air change rates below 0.5 h)1 in homes in Nordiccountries can increase the rate of infestation of housedust mites. As a causal relationship exists betweenhouse dust mite infestation and allergy (Andersen andKorsgaard, 1986), these data imply that low ventila-tion rates in homes may be one of the factorsexacerbating allergies.
Table 2 List of papers reviewed by the group but judged inconclusive or non-informative
Paper Reason for exclusion
Abbritti et al. (1992) Incomplete control of confoundingfactors (different buildings compared)
Incomplete control of confoundingfactors (different buildings compared)
Bachmann et al. (1995)
Beck et al. (1989) Incomplete analysisBourbeau et al. (1996) Incomplete control
of confounding factorsBourbeau et al. (1997) Incomplete control of
confounding factorsFinnegan et al. (1984) Incomplete control of confounding
factors (different buildings compared)Incomplete control of confoundingfactors (different buildings compared)
Gibert et al. (1992)
Haghighat and Donnini (1999) Incomplete analysisHarving et al. (1994) No data on ventilation ratesHedge et al. (1989) No measurements of airflowHedge et al. (1995) Insufficient dataHedge et al. (1996) Insufficient dataHill et al. (1992) Incomplete analysis (lack of
adjustments); relatively small sampleHosein et al. (1989) Incomplete analysis (no analysis in
terms of ventilation); no airflowmeasurements
Iversen et al. (1986) Incomplete analysisJaakkola et al. (1994) Too short exposure period (1 week) to observe
effects of interventionKodama and McGee (1986) Insufficient dataKroeling (1988) No control of confounding factors
(lack of adjustments); noinformation on ventilation
Menzies et al. (1997) Potential bias in the results (lack of blinding)Muzi et al. (1998) Incomplete control of confounding
factors (differentbuildings compared)
Nelson et al. (1995) Incomplete analysisNorb�ck (1995) Incomplete analysis; no information
on ventilation ratesNorb�ck and Edling (1991) Exposure data based on people's
report rather than onmeasurements
Norb�ck et al. (1990a) Dubious design of the study(all selected buildings were sick)
Norb�ck et al. (1990b) Incomplete control of confounding factorsNordstrGm et al. (1995a) Incomplete analysisNordstrGm et al. (1995b) Incomplete analysisPejtersen et al. (2001) Confounded interventions (impossible
to separate the effect of ventilation);unmatched case-control study
Robertson (1989) Incomplete control of confoundingfactors (different buildings compared)
Robertson et al. (1985) Incomplete control of confoundingfactors (different buildings compared)
Rowe et al. (1993) Incomplete analysis; retrospective studyRuotsalainen et al. (1991) No control of confounding factors
(crude analyses); incompletemeasurements
Ruotsalainen et al. (1994) Incomplete control of confounding factors(no control of windows opening)
Skov and Valbjørn (1987) No control of confounding factors (crudeanalysis)
Smedje et al. (1997) Incomplete information on analysis of resultsStenberg et al. (1995) Insufficient data on ventilation ratesSterling and Sterling (1983) Incomplete control of confounding factors
(different buildings compared)
Table 2 (Continued)
Paper Reason for exclusion
Teculescu et al. (1998) Incomplete control of confoundingfactors (different buildings compared)
Vincent et al. (1997) Too low response rateWieslander et al. (1999) Health-biased study; incomplete
control of confounding factorsWyon (1992) Insufficient dataWIlinder et al. (1997a) Incomplete control of confounding
factors (different buildings compared)WIlinder et al. (1997b) Incomplete control of confounding
factors (different buildings compared)
Wargocki et al.
116
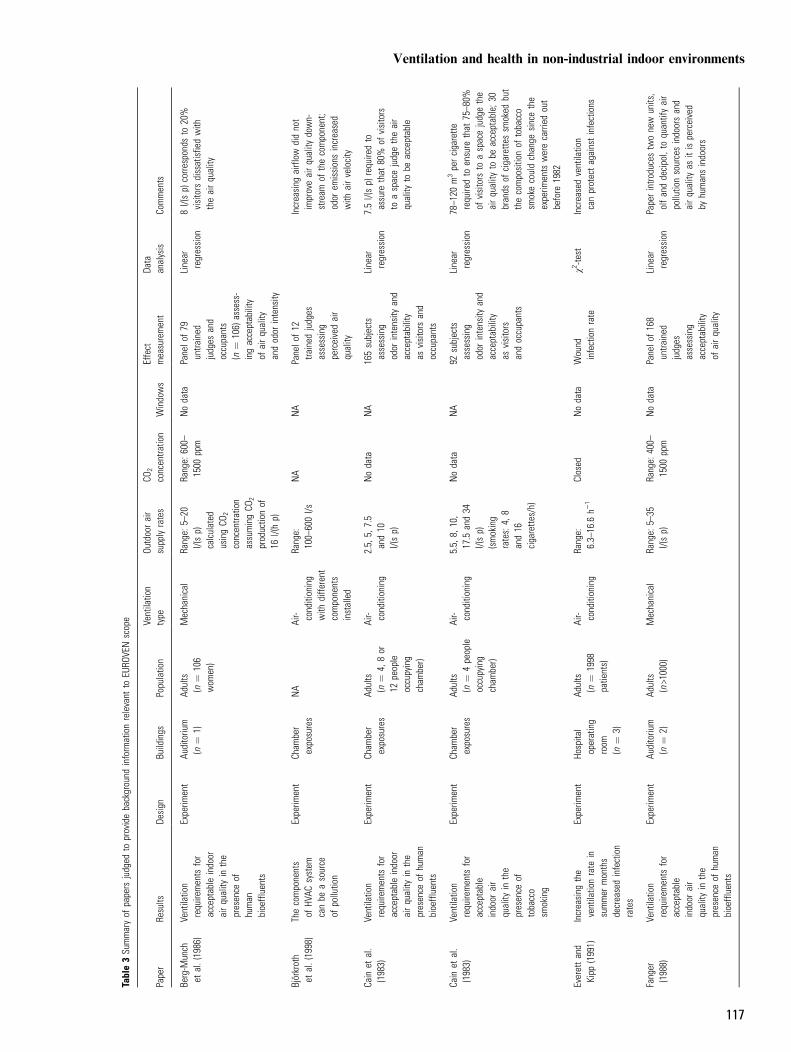
Table3Su
mmaryof
papers
judged
toprovidebackground
inform
ationrelevant
toEU
ROVE
Nscope
Paper
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2
concentra
tion
Windows
Effect
measurement
Data
analysis
Comments
Berg-M
unch
etal.(1986)
Ventilatio
nrequire
ments
for
acceptable
indoor
airquality
inthe
presence
ofhuman
bioeffluents
Experim
ent
Auditoriu
m(n
¼1)
Adults
(n¼
106
wom
en)
Mechanical
Range:
5–20
l/(sp)
calculated
usingCO
2
concentra
tion
assumingCO
2
productio
nof
16l/(hp)
Range:
600–
1500
ppm
Nodata
Panelo
f79
untra
ined
judges
and
occupants
(n¼
106)
assess-
ingacceptability
ofairquality
andodor
intensity
Linear
regression
8l/(sp)
corre
sponds
to20%
visitors
dissatisfie
dwith
theairquality
Bjorkroth
etal.(1998)
Thecomponents
ofHV
ACsystem
canbe
asource
ofpollutio
n
Experim
ent
Cham
ber
exposures
NA
Air- conditioning
with
diffe
rent
components
installed
Range:
100–
600l/s
NA
NA
Pane
lof12
trained
judges
assessing
perceivedair
quality
Increasing
airflow
didnot
improveairquality
down-
stream
ofthecomponent;
odor
emissionsincreased
with
airvelocity
Cain
etal.
(1983)
Ventilatio
nrequire
ments
for
acceptable
indoor
airquality
inthe
presence
ofhuman
bioeffluents
Experim
ent
Cham
ber
exposures
Adults
(n¼
4,8or
12people
occupying
cham
ber)
Air- conditioning
2.5,
5,7.5
and10
l/(sp)
Nodata
NA
165subjects
assessing
odor
intensity
and
acceptability
asvisitors
and
occupants
Linear
regression
7.5l/(sp)
require
dto
assure
that
80%
ofvisitors
toaspacejudgetheair
quality
tobe
acceptable
Cain
etal.
(1983)
Ventilatio
nrequire
ments
for
acceptable
indoor
air
quality
inthe
presence
oftobacco
smoking
Experim
ent
Cham
ber
exposures
Adults
(n¼
4people
occupying
cham
ber)
Air- conditioning
5.5,
8,10,
17.5
and34
l/(sp)
(smoking
rates:
4,8
and16
cigarette
s/h)
Nodata
NA
92subjects
assessing
odor
intensity
and
acceptability
asvisitors
andoccupants
Linear
regression
78–1
20m3percigarette
require
dto
ensure
that
75–8
0%of
visitors
toaspacejudgethe
airquality
tobe
acceptable;3
0brands
ofcigarette
ssm
oked
but
thecompositio
nof
tobacco
smokecouldchange
sincethe
experim
ents
werecarried
out
before
1982
Everettand
Kipp
(1991)
Increasing
the
ventilatio
nrate
insummer
months
decreasedinfection
rates
Experim
ent
Hospita
loperating
room
(n¼
3)
Adults
(n¼
1998
patie
nts)
Air- conditioning
Range:
6.3–
16.6
h)1
Closed
Nodata
Wound
infectionrate
v2-te
stIncreasedventilatio
ncanprotectagainstinfections
Fanger
(1988)
Ventilatio
nrequire
ments
for
acceptable
indoor
air
quality
inthe
presence
ofhuman
bioeffluents
Experim
ent
Auditoriu
m(n
¼2)
Adults
(n>1000)
Mechanical
Range:
5–35
l/(sp)
Range:
400–
1500
ppm
Nodata
Panelo
f168
untra
ined
judges
assessing
acceptability
ofairquality
Linear
regression
Paperintro
ducestw
onew
units,
olfanddecipol,to
quantifyair
pollutio
nsourcesindoorsand
airquality
asitis
perceived
byhumansindoors
Ventilation and health in non-industrial indoor environments
117
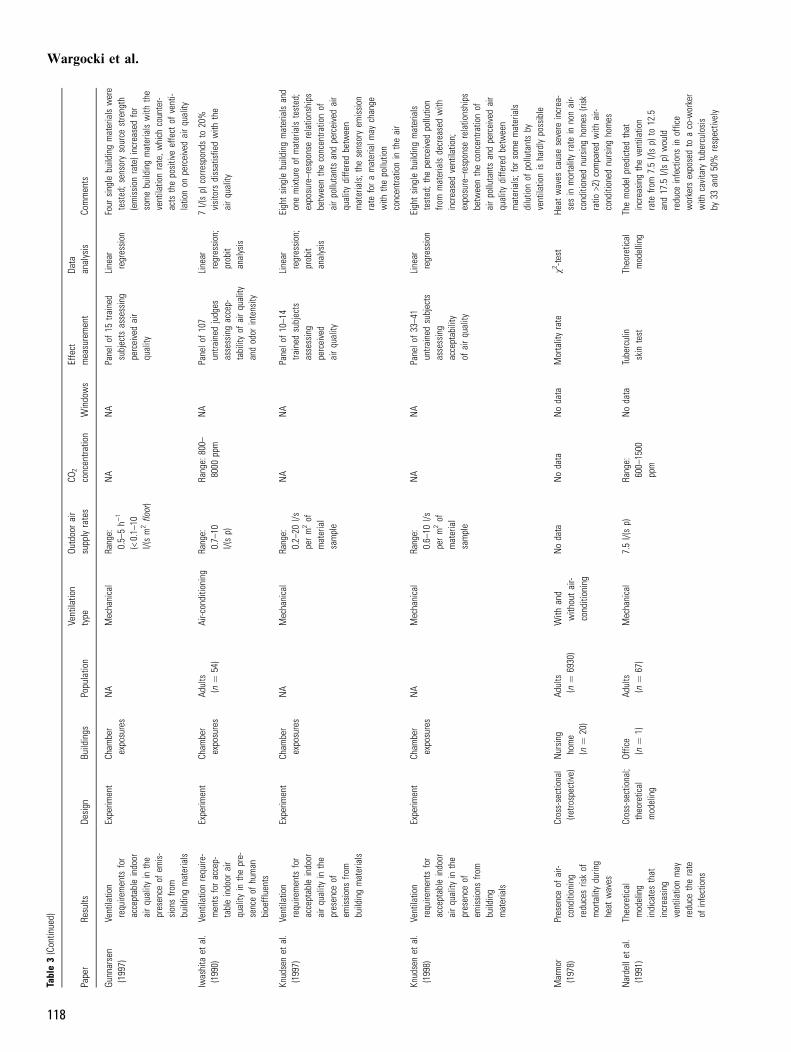
Table3(Contin
ued)
Paper
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2
concentra
tion
Windows
Effect
measurement
Data
analysis
Comments
Gunnarsen
(1997)
Ventilatio
nrequ
iremen
tsfor
acceptab
leindo
orairqu
ality
inthe
presen
ceof
emis-
sion
sfro
mbu
ildingmaterials
Expe
rimen
tCh
ambe
rexpo
sures
NA
Mecha
nical
Rang
e:0.5–
5h)
1
(<0.1–
10l/(sm
2floor)
NA
NA
Pane
lof15
trained
subjects
assessing
perceivedair
quality
Line
arregression
Four
sing
lebu
ildingmaterials
were
tested
;sen
sory
source
streng
th(emission
rate)increased
for
somebu
ildingmaterials
with
the
ventilatio
nrate,w
hich
coun
ter-
acts
thepo
sitiveeffect
ofventi-
latio
non
perceivedairqu
ality
Iwashita
etal.
(199
0)Ve
ntilatio
nrequ
ire-
men
tsforaccep-
tableindo
orair
quality
inthepre-
senceof
human
bioe
fflue
nts
Expe
rimen
tCh
ambe
rexpo
sures
Adults
(n¼
54)
Air-c
onditio
ning
Rang
e:0.7–
10l/(sp)
Rang
e:80
0–80
00pp
mNA
Pane
lof10
7un
trained
judg
esassessingaccep-
tabilityof
airqu
ality
andod
orintensity
Line
arregression
;prob
itan
alysis
7l/(sp)
corre
spon
dsto
20%
visitors
dissatisfie
dwith
the
airqu
ality
Knud
senet
al.
(199
7)Ve
ntilatio
nrequ
iremen
tsfor
acceptab
leindo
orairqu
ality
inthe
presen
ceof
emission
sfro
mbu
ildingmaterials
Expe
rimen
tCh
ambe
rexpo
sures
NA
Mecha
nical
Rang
e:0.2–
20l/s
perm2of
material
sample
NA
NA
Pane
lof10
–14
trained
subjects
assessing
perceived
airqu
ality
Line
arregression
;prob
itan
alysis
Eigh
tsing
lebu
ildingmaterials
and
onemixture
ofmaterials
tested
;expo
sure–respo
nserelatio
nships
betw
eentheconcen
tratio
nof
airpo
llutantsan
dpe
rceivedair
quality
diffe
redbe
twee
nmaterials;the
sensoryem
ission
rate
foramaterialm
aychan
gewith
thepo
llutio
nconcen
tratio
nin
theair
Knud
senet
al.
(199
8)Ve
ntilatio
nrequ
iremen
tsfor
acceptab
leindo
orairqu
ality
inthe
presen
ceof
emission
sfro
mbu
ilding
materials
Expe
rimen
tCh
ambe
rexpo
sures
NA
Mecha
nical
Rang
e:0.6–
10l/s
perm2of
material
sample
NA
NA
Pane
lof33
–41
untra
ined
subjects
assessing
acceptab
ility
ofairqu
ality
Line
arregression
Eigh
tsing
lebu
ildingmaterials
tested
;the
perceivedpo
llutio
nfro
mmaterials
decrea
sedwith
increa
sedventilatio
n;expo
sure–respo
nserelatio
nships
betw
eentheconcen
tratio
nof
airpo
llutantsan
dpe
rceivedair
quality
diffe
redbe
twee
nmaterials;for
somematerials
dilutio
nof
pollutantsby
ventilatio
nis
hardly
possible
Marmor
(197
8)Presen
ceof
air-
cond
ition
ing
redu
cesriskof
mortalitydu
ring
heat
waves
Cross-sectiona
l(re
trospective)
Nursing
home
(n¼
20)
Adults
(n¼
6930
)With
and
with
outair-
conditioning
Noda
taNoda
taNoda
taMortalityrate
v2-te
stHe
atwaves
causesevere
increa
-sesin
mortalityrate
inno
nair-
cond
ition
ednu
rsingho
mes
(risk
ratio
>2)c
ompa
redwith
air-
cond
ition
ednu
rsingho
mes
Narde
llet
al.
(199
1)Th
eoretical
mod
eling
indicatesthat
increa
sing
ventilatio
nmay
redu
cetherate
ofinfections
Cross-sectiona
l;theo
retical
mod
eling
Office
(n¼
1)Ad
ults
(n¼
67)
Mecha
nical
7.5l/(sp)
Rang
e:60
0–15
00pp
m
Noda
taTube
rculin
skin
test
Theo
retical
mod
elling
Themod
elpred
ictedthat
increa
sing
theventilatio
nrate
from
7.5l/(sp)
to12
.5an
d17
.5l/(sp)
wou
ldredu
ceinfections
inoffice
workers
expo
sedto
aco-w
orker
with
cavitary
tube
rculosis
by33
and50
%respectively
Wargocki et al.
118
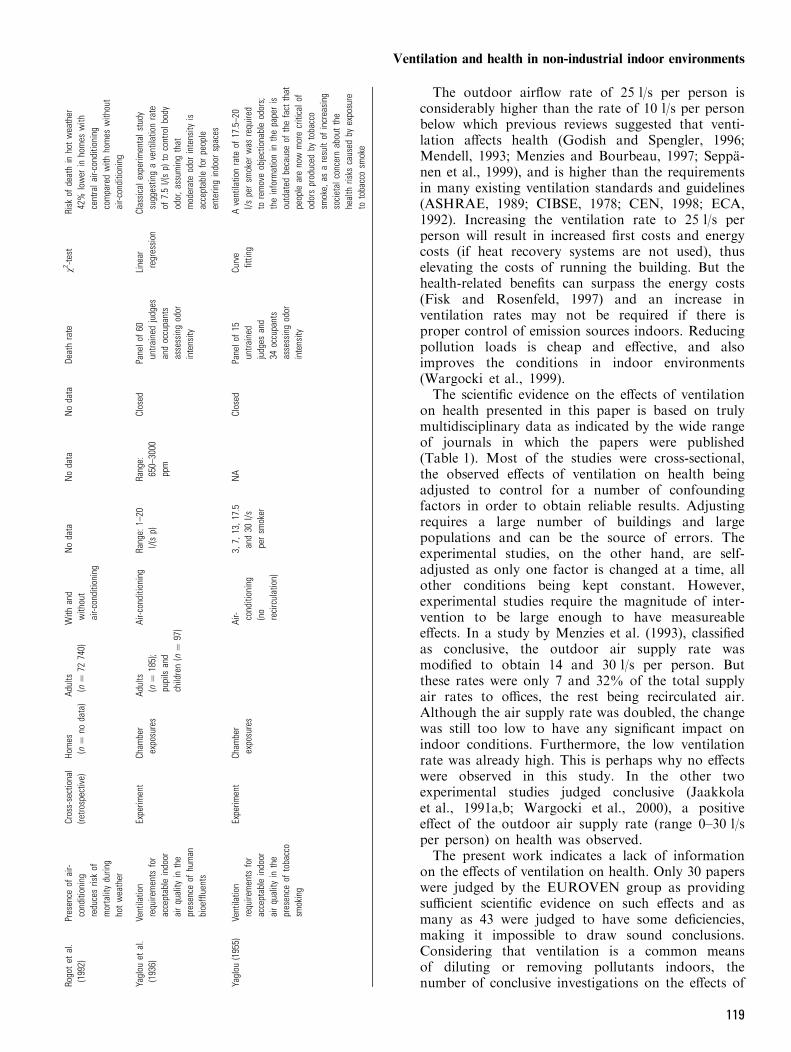
The outdoor airflow rate of 25 l/s per person isconsiderably higher than the rate of 10 l/s per personbelow which previous reviews suggested that venti-lation affects health (Godish and Spengler, 1996;Mendell, 1993; Menzies and Bourbeau, 1997; Seppa-nen et al., 1999), and is higher than the requirementsin many existing ventilation standards and guidelines(ASHRAE, 1989; CIBSE, 1978; CEN, 1998; ECA,1992). Increasing the ventilation rate to 25 l/s perperson will result in increased first costs and energycosts (if heat recovery systems are not used), thuselevating the costs of running the building. But thehealth-related benefits can surpass the energy costs(Fisk and Rosenfeld, 1997) and an increase inventilation rates may not be required if there isproper control of emission sources indoors. Reducingpollution loads is cheap and effective, and alsoimproves the conditions in indoor environments(Wargocki et al., 1999).The scientific evidence on the effects of ventilation
on health presented in this paper is based on trulymultidisciplinary data as indicated by the wide rangeof journals in which the papers were published(Table 1). Most of the studies were cross-sectional,the observed effects of ventilation on health beingadjusted to control for a number of confoundingfactors in order to obtain reliable results. Adjustingrequires a large number of buildings and largepopulations and can be the source of errors. Theexperimental studies, on the other hand, are self-adjusted as only one factor is changed at a time, allother conditions being kept constant. However,experimental studies require the magnitude of inter-vention to be large enough to have measureableeffects. In a study by Menzies et al. (1993), classifiedas conclusive, the outdoor air supply rate wasmodified to obtain 14 and 30 l/s per person. Butthese rates were only 7 and 32% of the total supplyair rates to offices, the rest being recirculated air.Although the air supply rate was doubled, the changewas still too low to have any significant impact onindoor conditions. Furthermore, the low ventilationrate was already high. This is perhaps why no effectswere observed in this study. In the other twoexperimental studies judged conclusive (Jaakkolaet al., 1991a,b; Wargocki et al., 2000), a positiveeffect of the outdoor air supply rate (range 0–30 l/sper person) on health was observed.The present work indicates a lack of information
on the effects of ventilation on health. Only 30 paperswere judged by the EUROVEN group as providingsufficient scientific evidence on such effects and asmany as 43 were judged to have some deficiencies,making it impossible to draw sound conclusions.Considering that ventilation is a common meansof diluting or removing pollutants indoors, thenumber of conclusive investigations on the effects ofRo
gotet
al.
(199
2)Presen
ceof
air-
cond
ition
ing
redu
cesriskof
mortalitydu
ring
hotwea
ther
Cross-sectiona
l(re
trospective)
Homes
(n¼
noda
ta)
Adults
(n¼
7274
0)With
and
with
out
air-c
onditio
ning
Noda
taNoda
taNoda
taDe
athrate
v2-te
stRisk
ofde
athin
hotwea
ther
42%
lower
inho
mes
with
centrala
ir-cond
ition
ing
compa
redwith
homes
with
out
air-c
onditio
ning
Yaglou
etal.
(193
6)Ve
ntilatio
nrequ
iremen
tsfor
acceptab
leindo
orairqu
ality
inthe
presen
ceof
human
bioe
fflue
nts
Expe
rimen
tCh
ambe
rexpo
sures
Adults
(n¼
185);
pupils
and
children(n
¼97
)
Air-c
onditio
ning
Rang
e:1–
20l/(sp)
Rang
e:65
0–30
00pp
m
Closed
Pane
lof60
untra
ined
judg
esan
doccupa
nts
assessingod
orintensity
Line
arregression
Classicale
xperimen
tals
tudy
sugg
estin
gaventilatio
nrate
of7.5l/(sp)
tocontrolb
ody
odor,a
ssum
ingthat
mod
erateod
orintensity
isacceptab
leforpe
ople
enterin
gindo
orspaces
Yaglou
(195
5)Ve
ntilatio
nrequ
iremen
tsfor
acceptab
leindo
orairqu
ality
inthe
presen
ceof
toba
cco
smoking
Expe
rimen
tCh
ambe
rexpo
sures
Air- cond
ition
ing
(no
recirculation)
3,7,
13,1
7.5
and30
l/spe
rsm
oker
NA
Closed
Pane
lof15
untra
ined
judg
esan
d34
occupa
nts
assessingod
orintensity
Curve
fittin
gAventilatio
nrate
of17
.5–2
0l/s
persm
oker
was
requ
ired
toremoveob
jectiona
bleod
ors;
theinform
ationin
thepa
peris
outdated
becauseof
thefact
that
peop
leareno
wmorecriticalo
fod
orsprod
uced
bytoba
cco
smoke,
asaresultof
increa
sing
societal
concernab
outthe
health
risks
caused
byexpo
sure
totoba
ccosm
oke
Ventilation and health in non-industrial indoor environments
119
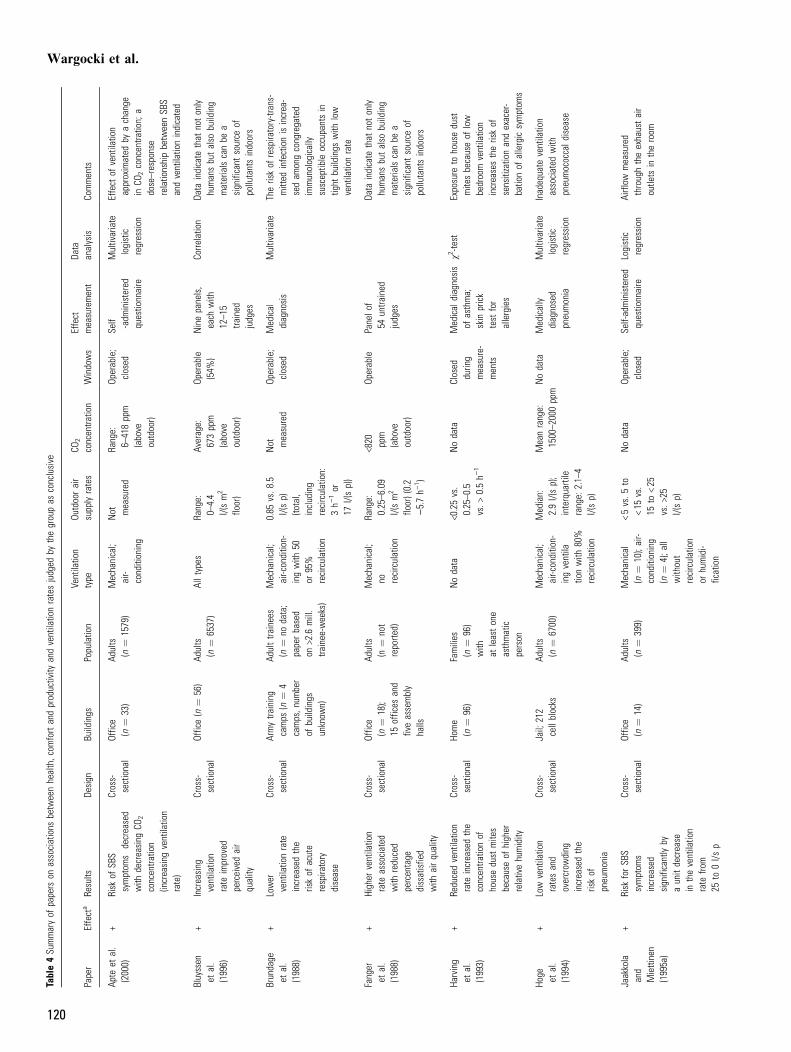
Table4Su
mmaryof
papers
onassociations
betw
eenhealth,c
omfort
andproductivity
andventilatio
nratesjudged
bythegroupas
conclusive
Paper
Effecta
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2
concentra
tion
Windows
Effect
measurement
Data
analysis
Comments
Apte
etal.
(2000)
+Risk
ofSB
Ssymptom
sdecreased
with
decreasing
CO2
concentra
tion
(increasing
ventilatio
nrate)
Cross-
sectional
Office
(n¼
33)
Adults
(n¼
1579)
Mechanical;
air-
conditioning
Not measured
Range:
6–418ppm
(above
outdoor)
Operable;
closed
Self -adm
inistered
questio
nnaire
Multivariate
logistic
regression
Effect
ofventilatio
napproximated
byachange
inCO
2concentra
tion;
adose–response
relatio
nshipbetw
eenSB
Sandventilatio
nindicated
Bluyssen
etal.
(1996)
+Increasing
ventilatio
nrate
improved
perceivedair
quality
Cross-
sectional
Office(n
¼56)
Adults
(n¼
6537)
Alltypes
Range:
0–4.4
l/(sm2
floor)
Average:
673ppm
(above
outdoor)
Operable
(54%
)Ninepanels,
each
with
12–1
5tra
ined
judges
Corre
latio
nDa
taindicate
that
notonly
humansbutalso
building
materials
canbe
asignificant
source
ofpollutantsindoors
Brundage
etal.
(1988)
+Lower
ventilatio
nrate
increasedthe
riskof
acute
respira
tory
disease
Cross-
sectional
Armytra
ining
camps
(n¼
4camps,n
umber
ofbuildings
unknow
n)
Adulttra
inees
(n¼
nodata;
paperbased
on>2.6
mill.
trainee-w
eeks)
Mechanical;
air-c
onditio
n-ingwith
50or
95%
recirculation
0.85
vs.8
.5l/(sp)
(total,
including
recirculation:
3h)
1or
17l/(sp))
Not measured
Operable;
closed
Medical
diagnosis
Multivariate
Theriskof
respira
tory-trans-
mitted
infectionis
increa-
sedam
ongcongregated
immunologically
susceptib
leoccupantsin
tight
buildings
with
low
ventilatio
nrate
Fanger
etal.
(1988)
+Higher
ventilatio
nrate
associated
with
reduced
percentage
dissatisfie
dwith
airquality
Cross-
sectional
Office
(n¼
18);
15offices
and
fiveassembly
halls
Adults
(n¼
not
reporte
d)
Mechanical;
no recirculation
Range:
0.25–6
.09
l/(sm2
floor)(0.2
)5.7h)
1 )
<820 ppm
(above
outdoor)
Operable
Panelo
f54
untra
ined
judges
Data
indicate
that
notonly
humansbutalso
building
materials
canbe
asignificant
source
ofpollutantsindoors
Harving
etal.
(1993)
+Re
ducedventilatio
nrate
increasedthe
concentra
tionof
housedust
mite
sbecauseof
higher
relativehumidity
Cross-
sectional
Home
(n¼
96)
Families
(n¼
96)
with
atleastone
asthmatic
person
Nodata
<0.25vs.
0.25–0
.5vs.>
0.5h)
1
Nodata
Closed
durin
gmeasure-
ments
Medical
diagnosis
ofasthma;
skin
prick
test
for
allergies
v2-te
stExposure
tohousedust
mite
sbecauseof
low
bedroom
ventilatio
nincreasestheriskof
sensitizatio
nandexacer-
batio
nof
allergic
symptom
s
Hoge etal.
(1994)
+Low
ventilatio
nratesand
overcrow
ding
increasedthe
riskof
pneumonia
Cross-
sectional
Jail;
212
cellblocks
Adults
(n¼
6700)
Mechanical;
air-c
onditio
n-ingventila
tionwith
80%
recirculation
Median:
2.9l/(sp);
interquartile
range:
2.1–
4l/(sp)
Meanrange:
1500–2
000ppm
Nodata
Medically
diagnosed
pneumonia
Multivariate
logistic
regression
Inadequate
ventilatio
nassociated
with
pneumococcald
isease
Jaakkola
and
Miettinen
(1995a)
+Risk
forSB
Ssymptom
sincreased
significantly
byaunitdecrease
intheventilatio
nrate
from
25to
0l/s
p
Cross-
sectional
Office
(n¼
14)
Adults
(n¼
399)
Mechanical
(n¼
10);air-
conditioning
(n¼
4);a
llwith
out
recirculation
orhumidi-
fication
<5vs.5
to<15
vs.
15to
<25
vs.>
25l/(sp)
Nodata
Operable;
closed
Self-administered
questio
nnaire
Logistic
regression
Airflow
measured
throughtheexhaustair
outle
tsin
theroom
Wargocki et al.
120
Jaakkola
etal.
(1991a,b)
‚Ch
anging
ventilatio
nratesdidnotchange
theprevalence
ofSB
Ssymptom
s
Cross-
sectional
Office
(n¼
1);
1247
smallo
ffices
Adults
(n¼
968)
Mechanicalw
ithheat
recovery,
with
out
recirculationor
humidificatio
n
Range:
7–70
l/(sp);
mean26
l/(sp)
Mean:
420ppm;
max:9
50ppm
Nodata
Self-administered
questio
nnaire
Multip
lelinear
regression
Noinspectio
nof
heating/
ventilatio
n/airconditio
ning
(HVA
C)system
Jaakkola
etal.
(1991a,b)
+De
creasing
the
ventilatio
nrate
increasedthe
prevalence
ofSB
Ssymptom
s
Experim
ent
Office
(n¼
1);
1247
smallo
ffices
Adults
(n¼
940)
Mechanical
with
heat
recovery,
with
out
recirculation
orhumidi-
fication
0vs.6
vs.1
0vs.2
5l/(sp)
Nodata
Nodata
Self-administered
questio
nnaire
Covaria
nce
Menzie
set
al.
(1993)
‚Ch
ange
ofventilatio
nrates
didnothave
effect
onSB
Ssymptom
s
Experim
ent
Office
(n¼
4)Ad
ults
(n¼
1546)
Mechanical;
air-
conditioning
with
recirculation
14vs.3
0l/(sp)
which
was
only
7and
32%
ofthe
totala
irflow
Mean:
621
vs.8
07ppm
Sealed
Self-admin-
isteredques-
tionnaire
Multivariate
logistic
regression
Changing
theoutdoorair
supply
rate
whenlarge
amountsof
airare
recirculated
(93and
68%)h
asno
effect
onSB
Ssymptom
s
Milton
etal.
(2000)
+Increased
ventilatio
ndecreased
sick-le
ave
Cross-
sectional
Office(n
¼40)
Adults
(n¼
3720)
Air-c
ondi-
tioning
12vs.2
4l/(sp)
800–
900
vs.6
00ppm
Nodata
Short-term
sick
leave
Poisson
regression
controlledfor
covaria
tes
Hourly
employees.
Ventilatio
ncategorized
byan
expert
ratin
gbasedon
CO2
measurements
Norba
cket
al.
(1995)
+At
high
CO2
concentra
tion,
theprevalence
ofnocturnal
breathlessness
was
higher
Case control
Homes
(n¼
88);51%
flats;4
9%single
family
houses
Adults
(n¼
88)
Natural;
mechanical
Not measured
1020 vs.8
50ppm
Operable
Self-adminis-
teredques-
tionnaire
and
clinical
exam
-inationof
asthmaor
atopy
Multip
lelogistic
regression
Nocturnal
breathlessness
isasymptom
ofasthma;
effect
ofventilatio
napproximated
byachange
inCO
2
concentra
tion;
low
ventilatio
nrate
athomeis
ariskforasthmatics
Smedje
etal.
(2000)
+Re
porting
ofat
leastoneasthma-
ticsymptom
was
less
common
with
increasedventilatio
n
Cross-
sectional
School
(n¼
39)
Pupils
6–16
years
old(n
¼1476)
Natural;
mechanical
4.4vs.1
2.8
l/(sp)
(3vs.
4h)
1 )
840 vs.7
80ppm
Nodata
Self-administered
questio
nnaire
posted
to'prim
ary'
parent
Multip
lelogistic
regression;
v2-te
st
77%
ofschoolsdidnot
meetbuildingcode
regulatio
ns
Sundell
etal.
(1994a)
+Risk
ofSB
Ssymptom
sdecreasedwith
increasing
ventilatio
nrate
Cross-
sectional
Office
(n¼
160);
540spaces
Adults
(n¼
4943)
Natural;
mechanical;
with
and
with
out
recirculation
Range:
2–50
l/(sp)
Nodata
Nodata
Self-administered
questio
nnaire
Multivariate
Adose-re
sponse
relatio
nship
was
indicatedbetw
een
increasedventilatio
nrate
anddiminishedriskof
SBSsymptom
s
Sundell
etal.
(1994a,b),
Stenberg
etal.(1994)
+Risk
ofSB
Ssymptom
sdecreasedwith
increasing
ventilatio
nrate
Case control
Office
(n¼
160)
Adults
(n¼
414)
Natural;
mechanical;
with
and
with
out
recirculation
<13.6vs.
>13.6l/(sp)
Nodata
Nodata
Self-administered
questio
nnaire
Multivariate
logistic
regression
13.6
l/(sp)
¼median
ventilatio
nrate
ofthetotal
studypopulatio
n
Ventilation and health in non-industrial indoor environments
121
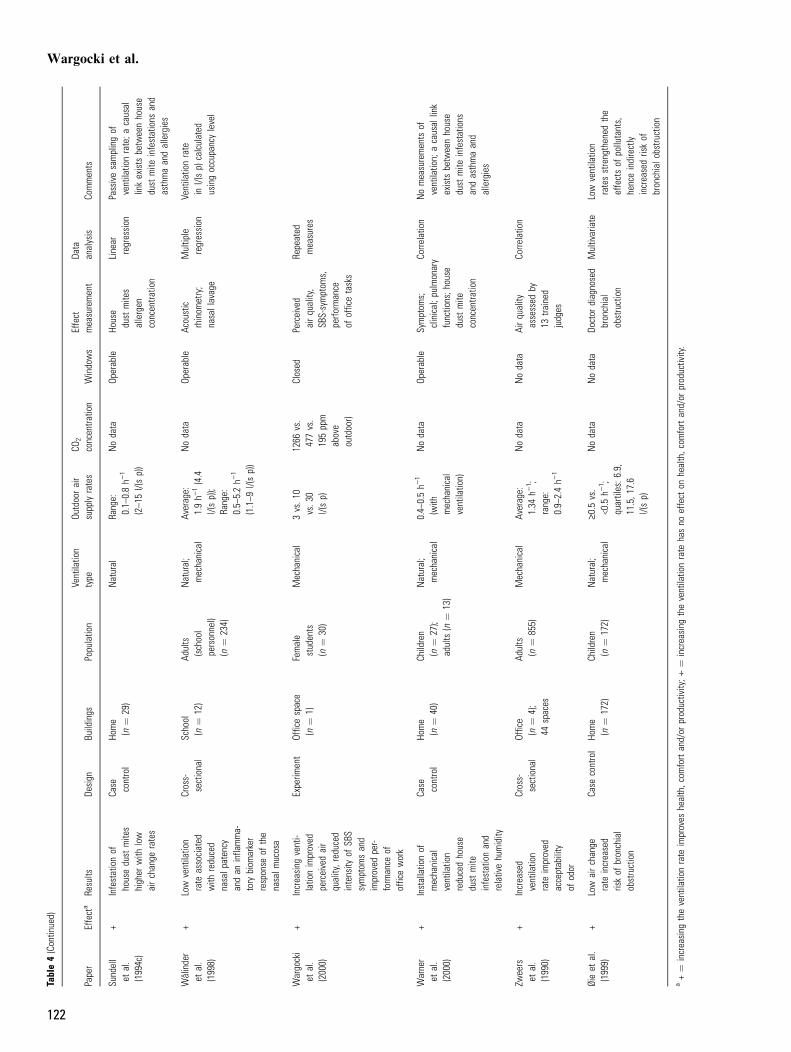
Table4(Contin
ued)
Paper
Effecta
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2
concentra
tion
Windows
Effect
measurement
Data
analysis
Comments
Sundell
etal.
(1994c)
+Infestationof
housedust
mite
shigher
with
low
airchange
rates
Case control
Home
(n¼
29)
Natural
Range:
0.1–
0.8h)
1
(2–1
5l/(sp))
Nodata
Operable
House
dust
mite
sallergen
concentra
tion
Linear
regression
Passivesamplingof
ventilatio
nrate;a
causal
linkexists
betw
eenhouse
dust
mite
infestations
and
asthmaandallergies
WIlinder
etal.
(1998)
+Low
ventilatio
nrate
associated
with
reduced
nasalp
atency
andan
infla
mma-
tory
biom
arker
response
ofthe
nasalm
ucosa
Cross-
sectional
School
(n¼
12)
Adults
(school
personnel)
(n¼
234)
Natural;
mechanical
Average:
1.9h)
1(4.4
l/(sp));
Range:
0.5–
5.2h)
1
(1.1–9
l/(sp))
Nodata
Operable
Acoustic
rhinom
etry;
nasallavage
Multip
leregression
Ventilatio
nrate
inl/(sp)
calculated
usingoccupancylevel
Wargocki
etal.
(2000)
+Increasing
venti-
latio
nimproved
perceivedair
quality,reduced
intensity
ofSB
Ssymptom
sand
improved
per-
form
ance
ofofficework
Experim
ent
Officespace
(n¼
1)Female
students
(n¼
30)
Mechanical
3vs.1
0vs.3
0l/(sp)
1266
vs.
477vs.
195ppm
above
outdoor)
Closed
Perceived
airquality,
SBS-symptom
s,perfo
rmance
ofofficetasks
Repeated
measures
Warner
etal.
(2000)
+Installatio
nof
mechanical
ventilatio
nreducedhouse
dust
mite
infestationand
relativehumidity
Case control
Home
(n¼
40)
Children
(n¼
27);
adults
(n¼
13)
Natural;
mechanical
0.4–
0.5h)
1
(with
mechanical
ventilatio
n)
Nodata
Operable
Symptom
s;clinical;p
ulmonary
functio
ns;h
ouse
dust
mite
concentra
tion
Corre
latio
nNomeasurements
ofventilatio
n;acausal
link
exists
betw
eenhouse
dust
mite
infestations
andasthmaand
allergies
Zweers
etal.
(1990)
+Increased
ventilatio
nrate
improved
acceptability
ofodor
Cross-
sectional
Office
(n¼
4);
44spaces
Adults
(n¼
855)
Mechanical
Average:
1.34
h)1 ;
range:
0.9–
2.4h)
1
Nodata
Nodata
Airquality
assessed
by13
trained
judges
Corre
latio
n
Øieet
al.
(1999)
+Low
airchange
rate
increased
riskof
bronchial
obstruction
Case
control
Home
(n¼
172)
Children
(n¼
172)
Natural;
mechanical
‡0.5
vs.
<0.5
h)1 ;
quartiles:6
.9,
11.5,1
7.6
l/(sp)
Nodata
Nodata
Doctor
diagnosed
bronchial
obstruction
Multivariate
Low
ventilatio
nratesstrengthened
the
effectsof
pollutants,
henceindirectly
increasedriskof
bronchialo
bstru
ction
a+¼
increasing
theventilatio
nrate
improves
health,c
omfort
and/or
productivity;‚
¼increasing
theventilatio
nrate
hasno
effect
onhealth,c
omfort
and/or
productivity.
Wargocki et al.
122
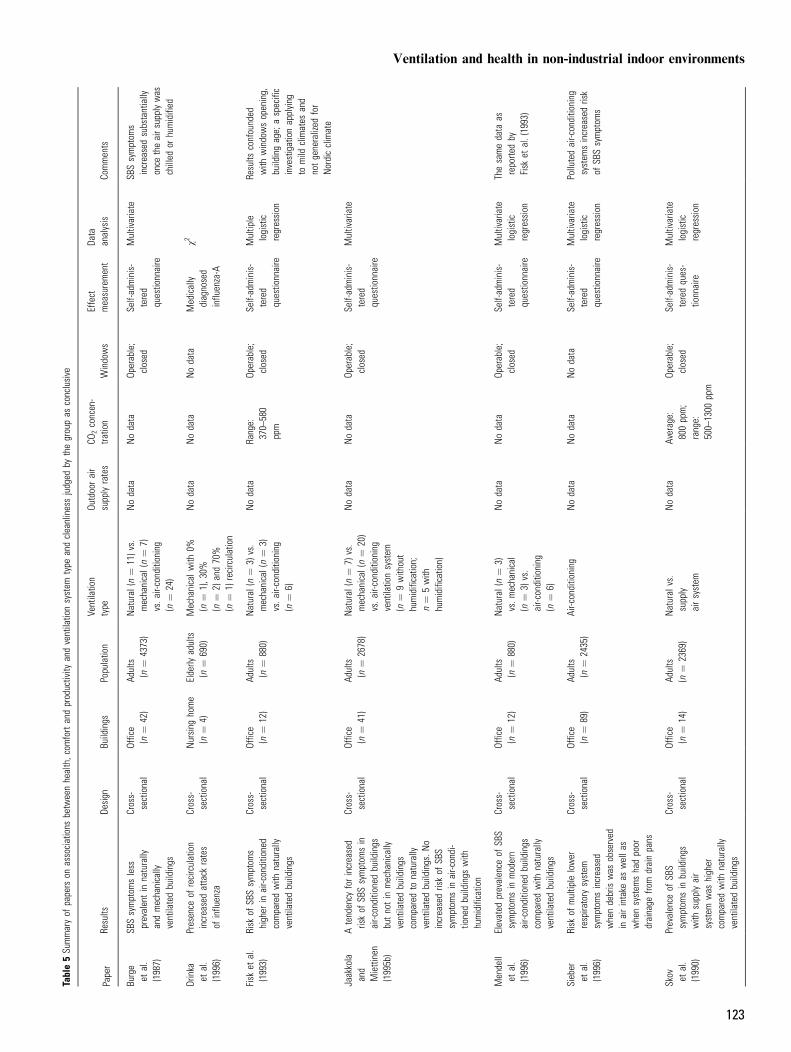
Table5Su
mmaryof
papers
onassociations
betw
eenhealth,c
omfort
andproductivity
andventilatio
nsystem
type
andcleanlinessjudged
bythegroupas
conclusive
Paper
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2concen-
tratio
nWindows
Effect
measurement
Data
analysis
Comments
Burge
etal.
(1987)
SBSsymptom
sless
prevalentin
naturally
andmechanically
ventilatedbuildings
Cross-
sectional
Office
(n¼
42)
Adults
(n¼
4373)
Natural
(n¼
11)v
s.mechanical(n¼
7)vs.a
ir-conditioning
(n¼
24)
Nodata
Nodata
Operable;
closed
Self-adminis-
tered
questio
nnaire
Multivariate
SBSsymptom
sincreasedsubstantially
once
theairs
upplywas
chilled
orhumidified
Drinka
etal.
(1996)
Presence
ofrecirculation
increasedattack
rates
ofinflu
enza
Cross-
sectional
Nursing
home
(n¼
4)Elderly
adults
(n¼
690)
Mechanicalw
ith0%
(n¼
1),3
0%(n
¼2)
and70%
(n¼
1)recirculation
Nodata
Nodata
Nodata
Medically
diagnosed
influ
enza-A
v2
Fisk
etal.
(1993)
Risk
ofSB
Ssymptom
shigher
inair-c
onditio
ned
comparedwith
naturally
ventilatedbuildings
Cross-
sectional
Office
(n¼
12)
Adults
(n¼
880)
Natural
(n¼
3)vs.
mechanical(n¼
3)vs.a
ir-conditioning
(n¼
6)
Nodata
Range:
370–
580
ppm
Operable;
closed
Self-adminis-
tered
questio
nnaire
Multip
lelogistic
regression
Results
confounded
with
windowsopening,
buildingage;
aspecific
investigationapplying
tomild
climates
and
notgeneralized
for
Nordicclimate
Jaakkola
and
Miettinen
(1995b)
Atendency
forincreased
riskof
SBSsymptom
sin
air-c
onditio
nedbuildings
butnotin
mechanically
ventilatedbuildings
comparedto
naturally
ventilatedbuildings.N
oincreasedriskof
SBS
symptom
sin
air-c
ondi-
tionedbuildings
with
humidificatio
n
Cross-
sectional
Office
(n¼
41)
Adults
(n¼
2678)
Natural
(n¼
7)vs.
mechanical(n¼
20)
vs.a
ir-conditioning
ventilatio
nsystem
(n¼
9with
out
humidificatio
n;n¼
5with
humidificatio
n)
Nodata
Nodata
Operable;
closed
Self-adminis-
tered
questio
nnaire
Multivariate
Mendell
etal.
(1996)
Elevated
prevalence
ofSB
Ssymptom
sin
modern
air-c
onditio
nedbuildings
comparedwith
naturally
ventilatedbuildings
Cross-
sectional
Office
(n¼
12)
Adults
(n¼
880)
Natural
(n¼
3)vs.m
echanical
(n¼
3)vs.
air-c
onditio
ning
(n¼
6)
Nodata
Nodata
Operable;
closed
Self-adminis-
tered
questio
nnaire
Multivariate
logistic
regression
Thesamedata
asreporte
dby
Fisk
etal.(1993)
Sieber
etal.
(1996)
Risk
ofmultip
lelower
respira
tory
system
symptom
sincreased
whendebris
was
observed
inairintake
aswella
swhensystem
shadpoor
drainage
from
drainpans
Cross-
sectional
Office
(n¼
89)
Adults
(n¼
2435)
Air-c
onditio
ning
Nodata
Nodata
Nodata
Self-adminis-
tered
questio
nnaire
Multivariate
logistic
regression
Pollutedair-c
onditio
ning
system
sincreasedrisk
ofSB
Ssymptom
s
Skov etal.
(1990)
Prevalence
ofSB
Ssymptom
sin
buildings
with
supply
air
system
was
higher
comparedwith
naturally
ventilatedbuildings
Cross-
sectional
Office
(n¼
14)
Adults
(n¼
2369)
Natural
vs.
supply
airsystem
Nodata
Average:
800ppm;
range:
500–
1300
ppm
Operable;
closed
Self-adminis-
teredques-
tionnaire
Multivariate
logistic
regression
Ventilation and health in non-industrial indoor environments
123
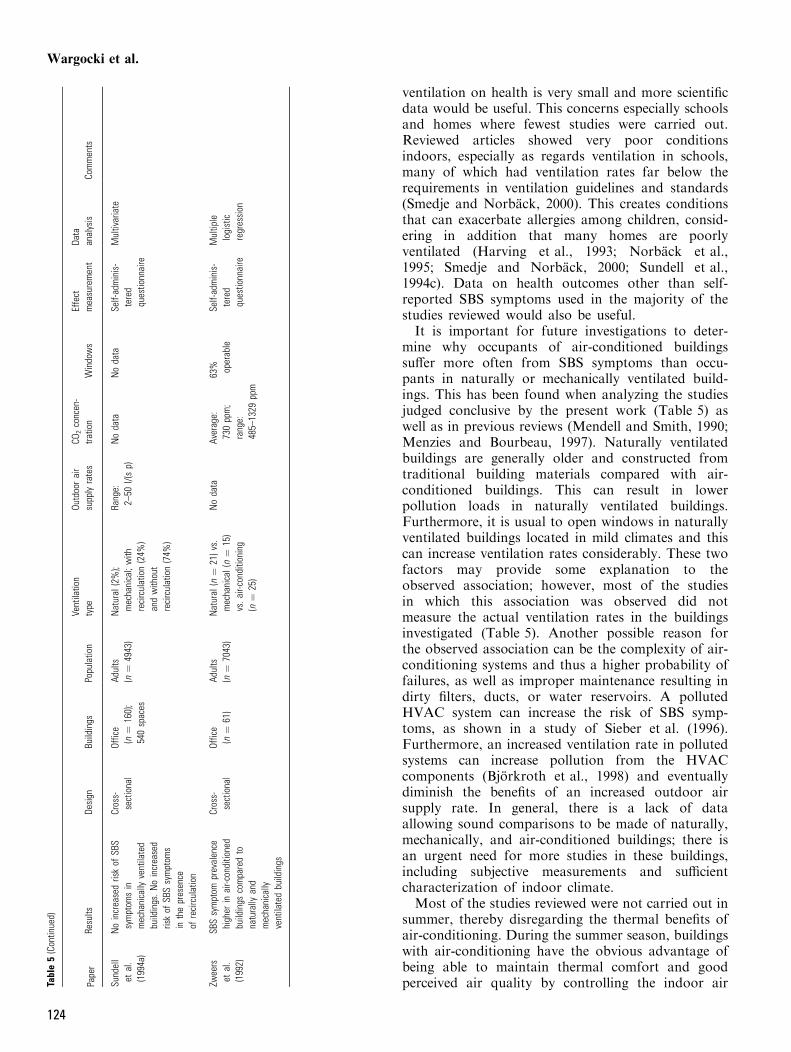
ventilation on health is very small and more scientificdata would be useful. This concerns especially schoolsand homes where fewest studies were carried out.Reviewed articles showed very poor conditionsindoors, especially as regards ventilation in schools,many of which had ventilation rates far below therequirements in ventilation guidelines and standards(Smedje and Norback, 2000). This creates conditionsthat can exacerbate allergies among children, consid-ering in addition that many homes are poorlyventilated (Harving et al., 1993; Norback et al.,1995; Smedje and Norback, 2000; Sundell et al.,1994c). Data on health outcomes other than self-reported SBS symptoms used in the majority of thestudies reviewed would also be useful.It is important for future investigations to deter-
mine why occupants of air-conditioned buildingssuffer more often from SBS symptoms than occu-pants in naturally or mechanically ventilated build-ings. This has been found when analyzing the studiesjudged conclusive by the present work (Table 5) aswell as in previous reviews (Mendell and Smith, 1990;Menzies and Bourbeau, 1997). Naturally ventilatedbuildings are generally older and constructed fromtraditional building materials compared with air-conditioned buildings. This can result in lowerpollution loads in naturally ventilated buildings.Furthermore, it is usual to open windows in naturallyventilated buildings located in mild climates and thiscan increase ventilation rates considerably. These twofactors may provide some explanation to theobserved association; however, most of the studiesin which this association was observed did notmeasure the actual ventilation rates in the buildingsinvestigated (Table 5). Another possible reason forthe observed association can be the complexity of air-conditioning systems and thus a higher probability offailures, as well as improper maintenance resulting indirty filters, ducts, or water reservoirs. A pollutedHVAC system can increase the risk of SBS symp-toms, as shown in a study of Sieber et al. (1996).Furthermore, an increased ventilation rate in pollutedsystems can increase pollution from the HVACcomponents (Bjorkroth et al., 1998) and eventuallydiminish the benefits of an increased outdoor airsupply rate. In general, there is a lack of dataallowing sound comparisons to be made of naturally,mechanically, and air-conditioned buildings; there isan urgent need for more studies in these buildings,including subjective measurements and sufficientcharacterization of indoor climate.Most of the studies reviewed were not carried out in
summer, thereby disregarding the thermal benefits ofair-conditioning. During the summer season, buildingswith air-conditioning have the obvious advantage ofbeing able to maintain thermal comfort and goodperceived air quality by controlling the indoor airTa
ble5(Contin
ued)
Paper
Results
Design
Buildings
Populatio
nVe
ntilatio
ntype
Outdoorair
supply
rates
CO2concen-
tratio
nWindows
Effect
measurement
Data
analysis
Comments
Sundell
etal.
(1994a)
Noincreasedriskof
SBS
symptom
sin
mechanically
ventilated
buildings.N
oincreased
riskof
SBSsymptom
sin
thepresence
ofrecirculation
Cross-
sectional
Office
(n¼
160);
540spaces
Adults
(n¼
4943)
Natural
(2%);
mechanical;with
recirculation(24%
)andwith
out
recirculation(74%
)
Range:
2–50
l/(sp)
Nodata
Nodata
Self-adminis-
tered
questio
nnaire
Multivariate
Zweers
etal.
(1992)
SBSsymptom
prevalence
higher
inair-c
onditio
ned
buildings
comparedto
naturally
and
mechanically
ventilatedbuildings
Cross-
sectional
Office
(n¼
61)
Adults
(n¼
7043)
Natural
(n¼
21)v
s.mechanical(n¼
15)
vs.a
ir-conditioning
(n¼
25)
Nodata
Average:
730ppm;
range:
485–
1329
ppm
63% operable
Self-adminis-
tered
questio
nnaire
Multip
lelogistic
regression
Wargocki et al.
124

temperature and humidity. The benefits of air-condi-tioning in extremely hot conditions have been indicatedin studies in nursing homes (Marmor, 1978) and inordinary households (Rogot et al., 1992) where thepresence of air-conditioning significantly reduced therisk of mortality compared with buildings without air-conditioning.Another possible artifact in many studies reviewed
was the assumption that clean outdoor air was used forventilation and that HVAC systems were clean. Infuture experiments some way of assessing cleanliness ofoutdoor and supplied air and cleanliness of HVACsystems would be useful.
Conclusions (consensus statement)
The following consensus was reached by the EUROV-EN group:
• The literature shows a strong association betweenventilation and comfort (as indicated by perceivedair quality) and health (as indicated by SBS symp-toms, inflammation, infections, asthma, allergy,short-term sick leave). It also indicates that there isan association between ventilation rate and produc-tivity (as indicated by performance of office work).
• The literature indicates that outdoor air rates below25 l/s per person in offices increase the risk ofSBS symptoms, increase short-term sick leave, anddecrease productivity. They also suggest that thesame may apply for schools but little information onthis aspect is available at present.
• The literature indicates that air change rates above0.5 h)1 in homes reduce the degree of infestation ofhouse dust mites in Nordic countries. Taking intoaccount the causal link between house dust mitesinfestation and asthma and allergies, these datasuggest that decreased ventilation may exacerbateallergies.
• The literature indicates that occupants of manybuildings with air-conditioning systems may havean increased risk of SBS symptoms compared withoccupants in naturally or mechanically ventilatedbuildings, implying thus that new ways of condi-tioning the air may be required. These results could
be confounded by a number of factors such asimproper maintenance of HVAC systems (the morecomplex the system the more liable it is to fail),building age (new types of building material arelikely to be found in air-conditioned buildingserected in the past 30 years), and unknown factorssuch as window opening. The studies were fur-thermore carried out mainly in transient and coldseasons, without taking into account the thermalbenefits of air-conditioning in hot seasons.
• The literature shows that improper maintenance,design, and functioning of HVAC systems contri-butes to an increased prevalence of SBS symptoms.This indicates a need for safety factors and propermaintenance of ventilation systems, including suchaspects as appropriate distance separating the inletand exhaust, replacing dirty filters, cleaning ducts,and the prevention of water reservoirs and water inthe systems.
• The literature shows that pollution sources otherthan the pollutants emitted by humans (bioefflu-ents) are important indoors. Consequently, propersource control is required in the first place, andsecondly the design of ventilation rates based on allpollution loads present indoors.
• The present work indicates the gaps where know-ledge is lacking as regards the effects of ventilationon human health, comfort, and productivity. Moreinformation is required on links between ventilationrates and health in schools and homes, and on theassociation between type of ventilation system andhealth effects.
Acknowledgments
The present work has been supported by EuropeanCommission in the framework of programmes andactions in the health and consumer protection sectorsSANCO through Grant Agreement No. SI2.142318(99CVF2-608) to the National Institute of PublicHealth in Sweden. Many thanks are due to MonaLakso who acted as an administrative secretary for thework and a contact person to EU, and whose assist-ance has been crucial for the project.
References
Andersen, I. and Korsgaard, J. (1986) Asth-ma and the indoor environment. Assess-ment of the health implications of highindoor humidity, Environ. Int., 12, 121–127.
ASHRAE (1989) Standard 62-89: Ventilationfor Acceptable Indoor Air Quality, Atlan-ta, GA, American Society of HeatingRefrigerating and, Air-ConditioningEngineers, Inc.
ASHRAE (1993) ASHRAE Handbook –Fundamentals, Atlanta, GA,American Society of Heating, Refriger-ating and, Air-Conditioning Engineers,Inc.
CEN (1998) Technical Report CR 1752:Ventilation for Buildings: Design Criteriafor the Indoor Environment, Brussels,European Committee for Standardiza-tion.
CIBSE (1978) CIBSE Guide Section A1,Environmental Criteria for Design,London, The Chartered Institution ofBuilding Services Engineers.
European Collaborative Action Indoor AirQuality and its Impact on Man (ECA)(1992) Guidelines for Ventilation Require-ments in Buildings, Luxembourg, Office forPublications of the European Communi-ties, Report No. 11 (EUR 14449 EN).
Ventilation and health in non-industrial indoor environments
125
Fisk, W.J. and Rosenfeld, A.H. (1997) Esti-mates of improved productivity andhealth from better indoor environments,Indoor Air, 7, 158–172 (Errata, IndoorAir, 8 (1998), 301).
Godish, T. and Spengler, J.D. (1996) Rela-tionships between ventilation and indoorair quality: a review, Indoor Air, 6, 135–145.
Mendell, M.J. (1993) Non-specific symptomsin office workers: a review and summaryof the epidemiologic literature, IndoorAir, 3, 227–236.
Mendell, M.J. and Smith, A.H. (1990) Con-sistent pattern of elevated symptoms inair-conditioned office buildings:a reanalysis of epidemiologic studies, Am.J. Pub. Health, 80, 1193–1199.
Menzies, D. and Bourbeau, J. (1997) Build-ing-related illnesses, New Engl. J. Med.,337, 1524–1531.
Seppanen, O.A., Fisk, W.J. and Mendell,M.J. (1999) Association of ventilationrates and CO2-concentrations with healthand other responses in commercial andinstitutional buildings, Indoor Air, 9, 226–252.
Sundell, J. and Bornehag, C.-G. (1999)Nordic interdisciplinary reviews of thescientific literature concerning the rela-tionship between indoor environmentalfactors and health, Nordworks. In: Raw,G., Aizlewood, C. and Warren, P. (eds)Proceedings of Indoor Air ¢99, Edinburgh,the 8th International Conference onIndoor Air Quality and Climate, Vol. 1,pp. 177–182.
Wargocki, P., Wyon, D.P., Baik, Y.K.,Clausen, G. and Fanger, P.O. (1999)Perceived air quality, Sick BuildingSyndrome (SBS) symptoms and pro-ductivity in an office with two differentpollution loads, Indoor Air, 9, 165–179.
World Health Organization (WHO) (1948)The Constitution of World Health Organ-ization, Geneva, WHO.
Papers reviewed by the EUROVEN groupAbbritti, G., Muzi, G., Accattoli, M.P.,Fiordi, T., dell’Omo, M., Colangeli, C.,Gabrielli, A.R., Fabbri, T. and d’Aless-andro, A. (1992) High prevalence of sickbuilding syndrome in a new air-condi-tioned building in Italy, Arch. Environ.Health, 47, 16–22.
Apte, M.G., Fisk, W.J. and Daisey, J.M.(2000) Associations between indoor CO2concentrations and sick building syn-drome symptoms in US office buildings:an analysis of the 1994–1996 BASE studydata, Indoor Air, 10, 246–257.
Bachmann, M., Turck, W. and Myers, J.(1995) Sick building symptoms in officeworkers: a follow-up study before andone year after changing buildings, Occup.Med., 45, 11–15.
Beck, H.I., Bjerring, P. and Harving, H.(1989) Atopic dermatitis and the indoorclimate. The effect from preventivemeasures, Acta Derm. Venereol., 69, 162–165.
*Berardi, B.M., Leoni, E., Marchesini, B.,Cascella, D. and Raffi, G.B. (1991)Indoor climate and air quality in newoffices: effects of a reduced air-exchangerate, Int. Arch. Occup. Environ. Health,63, 233–239.
Berg-Munch, B., Clausen, B.G. and Fanger,P.O. (1986) Ventilation requirements forthe control of body odor in spaces occu-pied by women, Environ. Int., 12, 195–199.
Bjorkroth, M., Seppanen, O. and Torkki, A.(1998) Chemical and sensory emissionsfrom HVAC components and ducts. In:Moschandreas, D. (ed.) Design, Con-struction and Operation of Healthy Build-ings – Solutions to Global and RegionalConcerns, ASHRAE, 47–55.
Bluyssen, P.M., de Oliveira Fernandes, E.,Groes, L., Clausen, G., Fanger, P.O.,Valbjørn, O., Bernhard, C.A. and Roulet,C.A. (1996) European indoor air qualityaudit project in 56 office buildings, IndoorAir, 6, 221–238.
Bourbeau, J., Brisson, C. and Allaire, S.(1996) Prevalence of the sick buildingsyndrome symptoms in office workersbefore and after being exposed to abuilding with an improved ventilationsystem, Occup. Environ. Med., 53, 204–210.
Bourbeau, J., Brisson, C. and Allaire, S.(1997) Prevalence of the sick buildingsyndrome symptoms in office workersbefore and six months and three yearsafter being exposed to a building with animproved ventilation system, Occup.Environ. Med., 54, 49–53.
Brundage, J.F., Scott, R.M., Lednar,W.M., Smith, D.W. and Miller, R.N.(1988) Building-associated risk of feb-rile acute respiratory diseases in Armytrainees, J. Am. Med. Assoc., 259, 2108–2112.
Burge, S., Hedge, A., Wilson, E., Bass, J.H.and Robertson, A. (1987) Sick Buildingsyndrome: a study of 4,373 office work-ers, Ann. Occup. Hyg., 31, 493–504.
Cain, W., Leaderer, R., Isseroff, L., Bergl-und, R., Huey, E., Lipsitt, E. and Perl-mann, D. (1983) Ventilation requirementsin buildings – I. Control of occupancyodor and tobacco smoke, Atmos. Envi-ron., 17, 1183–1197.
*Dale, H.C.A. and Smith, P. (1985) Bed-room ventilation: attitudes and policies,Energy Res., 9, 431–439.
Drinka, P.J., Krause, P., Schilling, M., Mil-ler, B.A., Shult, P. and Gravenstein, S.(1996) Report of an outbreak: nursinghome architecture and influenza-Aattack rates, J. Am. Geriatr. Soc., 44, 910–913.
Everett, W.D. and Kipp, H. (1991) Epi-demiologic observations of operatingroom infections resulting from variationsin ventilation and temperature, Am.J. Infect. Control, 19, 277–282.
Fanger, P.O. (1988) Introduction to the olfand the decipol units to quantify air pol-lution perceived indoors and outdoors,Energy and Buildings, 12, 1–6.
Fanger, P.O., Lauridsen, J., Bluyssen, P. andClausen, G. (1988) Air pollution sourcesin offices and assembly halls, quantifiedby the olf unit, Energy and Buildings, 12,7–19.
Finnegan, M.J., Pickering, C.A. and Burge,P.S. (1984) The sick building syndrome:prevalence studies, Br. Med. J., 289,1573–1575.
Fisk, W.J., Mendell, M.J., Daisey, J.M.,Faulkner, D., Hodgson, A.T., Nematol-lahi, M. and Macher, J.M. (1993) Phase 1of the California healthy building study,Indoor Air, 4, 246–254.
Gibert, I., Chevalier, A. and Lambrozo, J.(1992) No difference in rates of absen-teeism between workers in air-condi-tioned offices and naturally ventilatedones: a data base study, Indoor Environ-ment, 1, 279–284.
Gunnarsen, L. (1997) The influence of area-specific ventilation rate on emission fromconstruction products, Indoor Air, 7, 116–120.
*Gustafsson, D., Andersson, K., Fagerlund,I. and Kjellman, N.I. (1996) Significanceof indoor environment for the develop-ment of allergic symptoms in childrenfollowed up to 18 months of age, Allergy,51, 789–795.
Haghighat, F. and Donnini, G. (1999)Impact of psycho-social factors on per-ception of the indoor air environmentstudies in 12 office buildings, Building andEnvironment, 34, 479–503.
*Harrison, J., Pickering, C.A., Faragher,E.B., Austwick, P.K., Little, S.A. andLawton, L. (1992) An investigation of therelationship between microbial and par-ticulate indoor air pollution and the sickbuilding syndrome, Resp. Med., 86, 225–235.
Harving, H., Korsgaard, J. and Dahl, R.(1993) House-dust mites and associatedenvironmental conditions in Danishhomes, Allergy, 48, 106–109.
Harving, H., Korsgaard, J. and Dahl, R.(1994) Clinical efficacy of reduction inhouse-dust mite exposure in specially de-signed, mechanically ventilated ‘‘healthy’’homes, Allergy, 49, 866–870.
*Hedge, A. (1984) Evidence of a relationshipbetween office design and self-reports ofill health among office workers in theUnited Kingdom, J. Arch. Plann. Res., 1,163–174.
Hedge, A., Burge, P.S., Robertson, A.S.,Wilson, S. and Harris-Bass, J. (1989)Work-related illness in offices: a proposed
Wargocki et al.
126
model of the �Sick Building Syndrome�,Environ. Int., 15, 143–158.
Hedge, A., Erickson, W.A. and Rubin, G.(1995) Individual and occupational cor-relates of sick building syndrome, IndoorAir, 5, 10–21.
Hedge, A., Erickson, W.A. and Rubin, G.(1996) Predicting sick building syndromeat the individual and aggregate levels,Environ. Int., 22, 3–19.
Hill, B.A., Craft, B.F. and Burkart, J.A.(1992) Carbon dioxide, particulates, andsubjective human responses in officebuildings without histories of indoor airquality problems, Appl. Occup. Environ.Hyg., 7, 101–111.
*Hoffman, R.E., Wood, R.C. and Kreiss, K.(1993) Building-related asthma in Denveroffice workers, Am. J. Public Health, 83,89–93.
Hoge, C.W., Reichler, M.R., Dominguez,E.A., Bremer, J.C., Mastro, T.D., Hend-ricks, K.A., Musher, D.M., Elliott, J.A.,Facklam, R.R. and Breiman, R.F.(1994) An epidemic of pneumococcaldisease in an overcrowded, inadequatelyventilated jail, New Engl. J. Med., 331,643–648.
Hosein, H.R., Corey, P. and Robertson, J.M.(1989) The effect of domestic factors onrespiratory symptoms and FEV1, Int. J.Epidemiol., 18, 390–396.
*Ihenacho, H.N. (1990) Air-conditioningand health: effect on pulse and bloodpressure of young healthy, Nigerians,Central African J. Med., 36, 147–150.
Iversen, M., Bach, E. and Lundqvist, G.R.(1986) Health and comfort changesamong tenants after retrofitting oftheir housing, Environ. Int., 12, 161–166.
Iwashita, G., Kimura, K., Tanabe, S., Yos-hizawa, S. and Ikeda, K. (1990) Indoorair quality assessment based on humanolfactory sensation, J. Arch. Plann. Envi-ron. Eng., 410, 9–19.
Jaakkola, J.J. and Miettinen, P. (1995a)Ventilation rate in office buildings andsick building syndrome, Occup. Environ.Med., 52, 709–714.
Jaakkola, J.J. and Miettinen, P. (1995b)Type of ventilation system in officebuildings and sick building syndrome,Am. J. Epidemiol., 141, 755–765.
Jaakkola, J.J.K., Reinikainen, L.M., Hei-nonen, O.P., Majanen, A. and Seppanen,O. (1991a) Indoor air requirements forhealthy office buildings: recommenda-tions based on epidemiologic study,Environ. Int., 17, 371–378.
Jaakkola, J.J.K., Heinonen, O.P. andSeppanen, O. (1991b) Mechanical venti-lation in office buildings and the sickbuilding syndrome: an experimental andepidemiological study, Indoor Air, 1, 111–121.
Jaakkola, J.J.K., Tuomaala, P. and Seppa-nen, O. (1994) Air recirculation and sick
building syndrome: blinded cross-overtrial, Am. J. Pub. Health, 84, 422–428.
*Kelland, P. (1992) Sick building syndrome,working environments and hospital staff,Indoor Environ, 1, 335–340.
Knudsen, H.N., Clausen, G. and Fanger,P.O. (1997) Sensory characterization ofemissions from materials, Indoor Air, 7,107–115.
Knudsen, H.N., Valbjørn, O. and Nielsen,P.A. (1998) Determination of exposure–response relationships for emissions frombuilding products, Indoor Air, 8, 264–275.
Kodama, A.M. and McGee, R.I. (1986)Airborne microbial contaminants in in-door environments, Naturally ventilatedand air-conditioned homes, Arch. Envi-ron. Health, 41, 306–311.
Kroeling, P. (1988) Health and well-beingdisorders in air-conditioned buildings;comparative investigations of the �build-ing illness� syndrome, Energy and Build-ings, 11, 277–282.
Marmor, M. (1978) Heat wave mortality innursing homes, Environ. Res., 17, 102–115.
*McDonald, J.C., Armstrong, B., Benard, J.,Cherry, N.M. and Farant, J.P. (1993)Sick building syndrome in a Canadianoffice complex, Arch. Environ. Health, 48,298–304.
Mendell, M.J., Fisk, W.J., Deddens, J.A.,Seavey, W.G., Smith, A.H., Smith, D.F.,Hodgson, A.T., Daisey, J.M. and Gold-man, L.R. (1996) Elevated symptom pre-valence associated with ventilation type inoffice buildings, Epidemiology, 7, 583–589.
*Menzies, D., Tamblyn, R.M., Nunes, F.,Hanley, J. and Tamblyn, R.T. (1996)Exposure to varying levels of contami-nants and symptoms among workers intwo office buildings, Am. J. Pub. Health,86, 1629–1633.
Menzies, D., Pasztor, J., Nunes, F., Leduc, J.and Chan, C.H. (1997) Effect of a newventilation system on health and well-being of office workers, Arch. Environ.Health, 52, 360–367.
Menzies, R., Tamblyn, R., Farant, J.P.,Hanley, J., Nunes, F. and Tamblyn, R.(1993) The effect of varying levels ofoutdoor-air supply on the symptoms ofsick building syndrome, New Engl. J.Med., 328, 821–827.
*Merrill, J.L. and TenWolde, A. (1989)Overview of moisture-related damage inone group of Wisconsin manufacturedhouses, ASHRAE Trans., 95, Part, 1,405–414.
Milton, D., Glencross, P. and Walters, M.(2000) Risk of sick-leave associated withoutdoor air supply rate, humidificationand occupants complaints, Indoor Air, 10,212–221.
Muzi, G., Abbritti, G., Accattoli, M.P.and dell’Omo, M. (1998) Prevalence ofirritative symptoms in a nonproblem
air-conditioned office building, Int. Arch.Occup. Environ. Health, 71, 372–378.
Nardell, E.A., Keegan, J., Cheney, S.A. andEtkind, S.C. (1991) Airborne infection.Theoretical limits of protection achiev-able by building ventilation, Am. Rev.Resp. Dis., 144, 302–306.
Nelson, N.A., Kaufman, J.D., Burt, J. andKarr, C. (1995) Health symptoms and thework environment in four non-problemUnites States office buildings, Scand.J. Work Environ. Health, 21, 51–59.
Norback, D. (1995) Subjective indoor airquality in schools – the influence of highroom temperature, carpeting, fleecy wallmaterials, and volatile organic com-pounds (VOC), Indoor Air, 5, 237–246.
Norback, D. and Edling, C. (1991) Envi-ronmental, occupational, and personalfactors related to the sick building syn-drome in the general population, Br.J. Industr. Medicine, 48, 451–462.
Norback, D., Bjornsson, E., Janson, C.,Widstrom, J. and Boman, G. (1995)Asthmatic symptoms and volatile organiccompounds, formaldehyde, and carbondioxide in dwellings, Occup. Environ.Med., 52, 388–395.
Norback, D., Michel, I. and Widstrom, J.(1990a) Indoor air quality and personalfactors related to the sick building syn-drome, Scand. J. Work Environ. Health,16, 121–128.
Norback, D., Torgen, M. and Edling, C.(1990b) Volatile organic compounds,respirable dust, and personal factorsrelated to prevalence and incidence of sickbuilding syndrome in primary schools, Br.J. Industr. Med., 47, 733–741.
Nordstrom, K., Norback, D. and Akselsson,R. (1995a) Subjective indoor air quality inhospitals – The influence of building age,ventilation flow, and personal factors,Indoor Environ., 4, 37–44.
Nordstrom, K., Norback, D. and Akselsson,R. (1995b) Influence of indoor air qualityand personal factors on the sick buildingsyndrome (SBS) in Swedish geriatrichospitals, Occup.Environ. Med., 52, 170–176.
Øie, L., Nafstad, P., Botten, G., Magnus, P.and Jaakkola, J.K. (1999) Ventilation inhomes and bronchial obstruction inyoung children, Epidemiology, 10, 294–299.
*Paul, W.S., Moore, P.S., Karabatsos, N.,Flood, S.P., Yamada, S., Jackson, T. andTsai, T.F. (1993) Outbreak of Japaneseencephalitis on the island of Saipan, 1990,J. Infect. Dis., 167, 1053–1058.
Pejtersen, J., Brohus, H., Hyldgaard, C.E.,Nielsen, J.B., Valbjørn, O., Hauschildt,P., Kjærgaard, S.K. and Wolkoff, P.(2001) Effect of renovating an officebuilding on occupants’ comfort andhealth, Indoor Air, 11, 10–25.
*Richards, A.L., Hyams, K.C., Watts, D.W.,Rozmajzl, P.J., Woody, J.N. and Merrel,
Ventilation and health in non-industrial indoor environments
127
B.R. (1993) Respiratory disease amongmilitary personnel in Saudi Arabia duringOperation Desert Shield, Am. J. Pub.Health, 83, 1326–1329.
Robertson, A.S. (1989) Building sickness –are symptoms related to office lightning?,Ann. Occup. Hyg., 33, 47–59.
Robertson, A.S., Burge, P.S., Hedge, A.,Sims, J., Gill, F.S., Finnegan, M., Pic-kering, C.A. and Dalton, G. (1985)Comparison of health problems relatedto work and environmental measurementsin two office buildings with differentventilation systems, Br. Med. J., 10,373–376.
Rogot, E., Sorlie, P.D. and Backlund, E.(1992) Air-conditioning and mortality inhot weather, Am. J. Epidemiol., 136, 106–116.
Rowe, D., Wilke, S. and Guan, L. (1993)Examination of sick leave absencesfrom work in buildings with various ratesof ventilation, Indoor Environ., 2, 276–284.
Ruotsalainen, R., Jaakkola, J.J.K., Ronn-berg, R., Majanen, A. and Seppanen, O.(1991) Symptoms and perceived indoorair quality among occupants of housesand apartments with different ventilationsystems, Indoor Air, 1, 428–438.
Ruotsalainen, R., Jaakkola, N. and Jaakko-la, J.J.K. (1994) Ventilation rate as a de-terminant of symptoms and perceivedodors among workers in daycare centers,Environ. Int., 20, 731–737.
*Salisbury, S.A. (1984) A typically frustra-ting building investigation, Ann. Am.Conf. Governmental Industrial Hygienists,10, 129–130.
*Shigematsu, I. and Minowa, M. (1985)Indoor infection in a modern building,Tokai J. Exp. Clin. Med., 10, 407–413.
Sieber, W.K., Stayner, L.T., Malkin, R.,Petersen, M.R., Mendell, M.J., Walling-ford, K.M., Crandall, M.S., Wilcox, T.G.and Reed, L. (1996) The National Insti-tute for Occupational Safety and Healthindoor environmental evaluation experi-ence, Part three: Associations betweenenvironmental factors and self-reportedhealth conditions, Appl. Occup. Environ.Hyg., 11, 1387–1392.
Skov, P. and Valbjørn, O. (1987) The sickbuilding syndrome in the office environ-ment: The Danish Town Hall study,Environ. Int., 13, 339–349.
Skov, P., Valbjørn, O. and Pedersen, B.V.(1990) Influence of indoor climate on thesick building syndrome in an office envi-ronment, Scand. J. Work Environ. Health,16, 363–371.
Smedje, G. and Norback, D. (2000) Newventilation systems at select schools inSweden – effects on asthma and exposure,Arch. Environ. Health, 55, 18–25.
Smedje, G., Norback, D. and Edling, C.(1997) Subjective indoor air quality inschools in relation to exposure, IndoorAir, 7, 143–150.
Stenberg, B., Eriksson, N., Hoog, J.,Sundell, J. and Wall, S. (1994) The SickBuilding Syndrome (SBS) in office work-ers. A case-referent study of personal,psychosocial and building-related riskindicators, Int. J. Epidemiol., 23, 1190–1197.
Stenberg, B., Eriksson, N., Mild, K.H.,Hoog, J., Sandstrom, M., Sundell, J.and Wall, S. (1995) Facial skin symp-toms in visual display terminal workers(VDT). A case-referent study of personal,psychosocial, building- and VDT-relatedrisk indicators, Int. J. Epidemiol., 24, 796–803.
Sterling, E. and Sterling, T. (1983) The im-pact of different ventilation levels andfluorescent lighting types on building ill-ness: an experimental study, Can. J. Pub.Health, 74, 385–392.
*Sullivan-Bolyai, J.Z., Lumish, R.M., Smith,E.W., Howell, J.T., Bregman, D.J., Lund,M., Page, R.C. and Page, R.C. (1979)Hyperpyrexia due to air-conditioningfailure in a nursing home, Public HealthRep., 94, 466–470.
Sundell, J., Lindvall, T. and Stenberg, B.(1994a) Associations between type ofventilation and air flow rates in officebuildings and the risk of SBS-symptomsamong occupants, Environ. Int., 20, 239–251.
Sundell, J., Lindvall, T., Stenberg, B. andWall, S. (1994b) Sick Building Syndrome(SBS) in office workers and facial skinsymptoms among VDT-workers in rela-tion to building and room characteristics:two case-referent studies, Indoor Air, 4,83–94.
Sundell, J., Wickman, M., Pershagen, G. andNordvall, S.L. (1994c) Ventilation inhomes infested by house-dust mites,Allergy, 50, 106–112.
*Tamblyn, R.M., Menzies, R.I., Tamblyn,R.T., Farant, J.P. and Hanley, J. (1992)The feasibility of using a double blindexperimental cross-over design to studyinterventions for sick building syndrome,J. Clin. Epidemiol., 45, 603–612.
Teculescu, D.B., Sauleau, E.A., Massin, N.,Bohadana, A.B., Buhler, O., Benamghar,L. and Mur, J.M. (1998) Sick-buildingsymptoms in office workers in north-eastern France: a pilot study, Int.Arch. Occup. Environ. Health, 71, 353–356.
*Turiel, I., Hollowell, C.D., Miksch, R.R.,Rudy, J.V., Young, R.A. and Coye, M.J.(1983) Effects of reduced ventilation onindoor air quality in an office building,Atmos. Environ., 17, 51–64.
Vincent, D., Annesi, I., Festy, B. andLambrozo, J. (1997) Ventilation system,indoor air quality, and health outcomes inParisian modern office workers, Environ.Res., 75, 100–112.
Walinder, R., Norback, D., Wieslander, G.,Smedje, G. and Erwall, C. (1997a) Nasalcongestion in relation to low air exchangerate in schools. Evaluation by acousticrhinometry, Acta Otolaryngol., 117, 724–727.
Walinder, R., Norback, D., Wieslander, G.,Smedje, G. and Erwall, C. (1997b) Nasalmucosal swelling in relation to low airexchange rate in schools, Indoor Air, 7,198–205.
Walinder, R., Norback, D., Wieslander, G.,Smedje, G., Erwall, C. and Venge, P.(1998) Nasal patency and biomarkers innasal lavage – the significance of air ex-change rate and type of ventilation inschools, Int. Arch. Occup. Environ.Health, 71, 479–486.
Wargocki, P., Wyon, D.P., Sundell, J.,Clausen, G. and Fanger, P.O. (2000)The effects of outdoor air supply ratein an office on perceived air quality,Sick Building Syndrome (SBS) symp-toms and productivity, Indoor Air, 10,222–236.
Warner, J.A., Frederick, J.M., Bryant, T.N.,Wiech, C., Raw, G.J., Hunter, C., Ste-phen, F.R., McIntyre, D.A. and Warner,J.O. (2000) Mechanical ventilation andhigh-efficiency vacuum cleaning: a com-bined strategy of mite and mite allergenreduction in the control of mite-sensitiveasthma, J. Allergy Clin. Immunol., Part 1,105, 75–82.
Wieslander, G., Norback, D., Walinder, R.,Erwall, C. and Venge, P. (1999) Inflam-mation markers in nasal lavage, and nasalsymptoms in relation to relocation to anewly painted building: a longitudinalstudy, Int. Arch. Occup. Environ. Health,72, 507–515.
Wyon, D.P. (1992) Sick buildings and theexperimental approach, Environ. Tech-nol., 13, 313–322.
Yaglou, C.P. (1955) Ventilation require-ments for cigarette smoke, ASHAETransactions, 61, 25–32.
Yaglou, C.P., Riley, E.C. and Coggins, D.I.(1936) Ventilation requirements, ASH-RAE Trans., 42, 133–162.
Zweers, T., Skov, P., Valbjørn, O. andMølhave, L. (1990) The effect of ventila-tion and air pollution on perceived indoorair quality in five town halls, Energy andBuildings, 14, 175–181.
Zweers, T., Preller, L., Brunekreef, B. andBoleij, J.S.M. (1992) Health and indoorcomplaints of 7043 office workers in 61buildings in the Netherlands, Indoor Air,2, 127–136.
Wargocki et al.
128








![The American-European Consensus Conference on ARDS, Part 2nitric oxide inhalation [35], tracheal gas insuflation [36,37] and perfluorcarbon associated (partial liquid) ventilation](https://img.pdfslide.net/doc/110x75/60596b5850961912b931593c/the-american-european-consensus-conference-on-ards-part-2-nitric-oxide-inhalation.jpg)