Embed Size (px)
Citation preview
Gianfranco Cervellin
Pronto Soccorso e Medicina d’UrgenzaAzienda Ospedaliero-Universitaria di Parma
Vertigine in ED: inquadramento diagnostico.

vertigo/dizziness vertigine/capogiro= ?
Problemino semantico:

LipotimiaPrelipotimia
Svenimento
Mancamento
Deliquio

Ann Intern Med. 2001;134:823-832
Dizziness is one of the most challenging symptoms in medicine. It is difficult to define, impossible to measure, a challenge to diagnose, and troublesome to treat. The word dizziness is used to mean various sensations of body orientation and position that are frequently difficult for patients to describe

Problemino culturale:
Ricerca su PubMed 22 aprile 2015
• Vertigo ���� 14259 articoli, di cui >650 2014/15
• Dizziness ���� 26849 articoli, di cui >950 2014/15

VERTIGINE
Definizione
Vertere = girare
Sintomatologia caratterizzata da una rotazione dell’ambiente rispetto all’individuo o dell’individuo rispetto all’ambiente

20-30 % della popolazione generale
Epidemiologia
La prevalenza varia con l’età e il sesso
<<<<16% 35%
18-35 aa > 80 aa

Fisiopatologia
sistema visivo
sistema labirinticosistema propriocettivo
componente psichica
SNC
Nuclei vestibolari
centrali

Diagnosi differenziale dei disturbi dell’equilibrio (1)
Cause cardiovascolari
• Aritmie iper- e ipocinetiche
• Ipotensione ortostatica
• Ipovolemia o anemia
• Ischemia miocardica
• Patologia valvolare o cardiaca strutturale
• Ipossia
• Crisi vaso-vagale
Cause otologiche o neurologiche
• VPPB
• Nevrite vestibolare
• Malattia di Ménière
• Evento cerebrovascolare
• Insuff. vertebrobasilare
• Neurinoma dell’acustico
• Sclerosi multipla

Diagnosi differenziale dei disturbi dell’equilibrio (1)
Cause cardiovascolari
• Aritmie iper- e ipocinetiche
• Ipotensione ortostatica
• Ipovolemia o anemia
• Ischemia miocardica
• Patologia valvolare o cardiaca strutturale
• Ipossia
• Crisi vaso-vagale
Cause otologiche o neurologiche
• VPPB
• Nevrite vestibolare
• Malattia di Ménière
• Evento cerebrovascolare
• Insuff. vertebrobasilare
• Neurinoma dell’acustico
• Sclerosi multipla

Dottore, mentre lavoravo nell’orto ho avvertito un gran capogiro, e dopo
pochi secondi una tremendascossa al petto!
Parma, 4 maggio 2015
Maschio, 64 anni, nel nov. 2014 duplice BPAC e impianto di ICD.Interrogato ICD: TV 220 bpm ���� shock

Diagnosi differenziale dei disturbi dell’equilibrio (2)
Effetti farmacologici:
• Aminoglicosidi
• Anticonvulsivanti
• Anti-ipertensivi
• Ipoglicemizzanti
• Antipsicotici
• Ipnotici/sedativi
• Alcool
• …..
Altre:
• Psichiatriche (iperventilazione, disturbi d’ansia)
• Patologie della tiroide
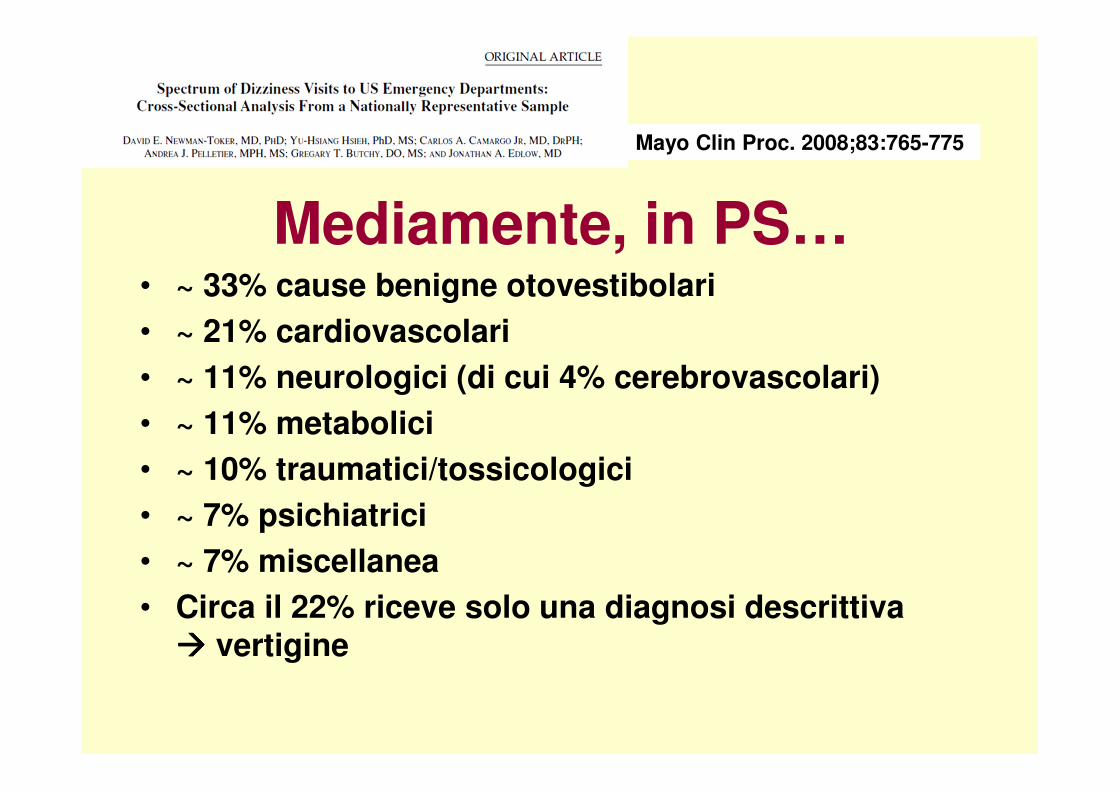
Mediamente, in PS…• ~ 33% cause benigne otovestibolari
• ~ 21% cardiovascolari
• ~ 11% neurologici (di cui 4% cerebrovascolari)
• ~ 11% metabolici
• ~ 10% traumatici/tossicologici
• ~ 7% psichiatrici
• ~ 7% miscellanea
• Circa il 22% riceve solo una diagnosi descrittiva ���� vertigine
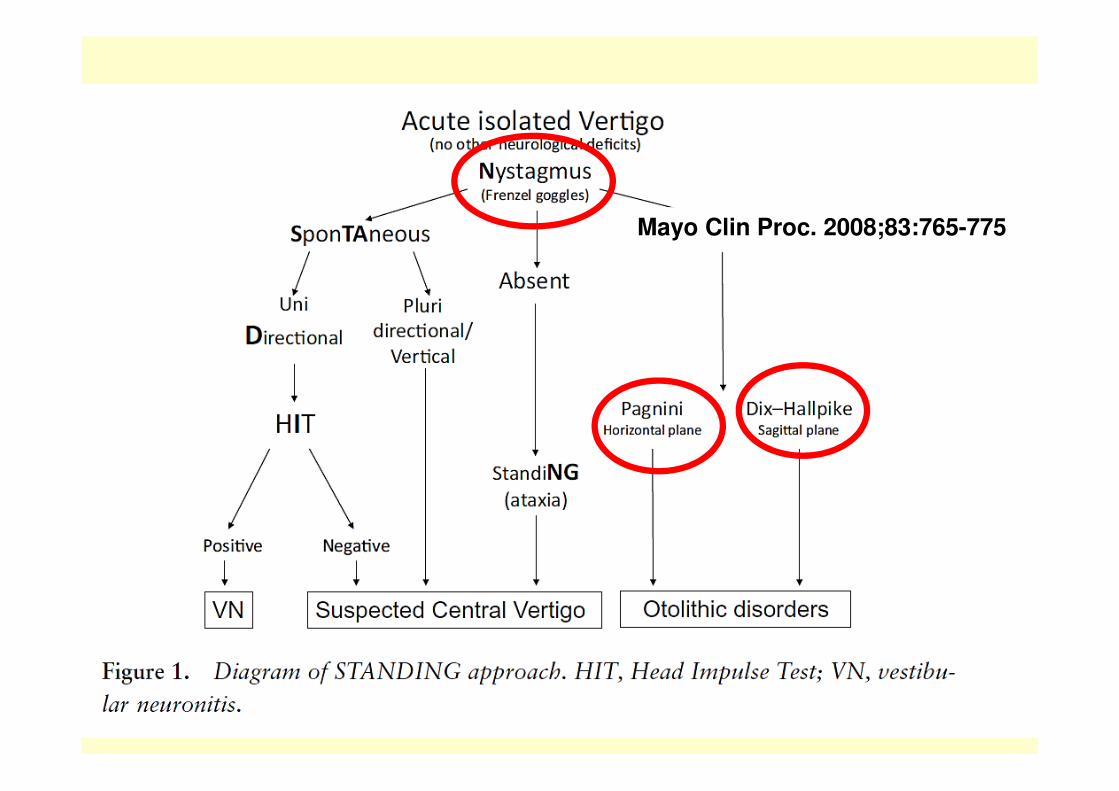
Mayo Clin Proc. 2008;83:765-775
Mayo Clin Proc. 2008;83:765-775
A total of 9472 dizziness cases (3.3% of visits) were sampled over 13 years (weighted 33.6 million). Predefined dangerous disorders were diagnosed in 15%, especiallyamong those older than 50 years (20.9% vs 9.3%; P<.001). Dizziness cases were evaluated longer (mean 4.0 vs 3.4 hours), imageddisproportionately (18.0% vs 6.9% undergoing computed tomographyor magnetic resonance imaging), and admitted more often(18.8% vs 14.8%) (all p<0.001).

Quali accertamenti?

ACAD EMERG MED 2008;15:744–750
From 1995 to 2004, the rate of visits for vertigo-dizziness increased by 37%and demonstrated a significant linear trend (p < 0.001).The utilization of computerized tomography and magnetic resonance imaging (CT ⁄ MRI) increased 169% from 1995 to 2004, which was more than any other test.The rate of central nervous system diagnoses (e.g., cerebrovascular disease or brain tumor) did not increase over time.

ACAD EMERG MED 2013;20:689–696
The estimated number of 2011 US ED visits for dizziness or vertigo was3.9 million (95% confidence interval [CI] = 3.6 to 4.2 million)
The proportion undergoing diagnostic imaging by computedtomography (CT), magnetic resonance imaging (MRI), or both in 2011 was estimated to be 39.9% (39.4% CT, 2.3% MRI).The mean per-ED-dizziness-visit cost was $1,004. The total extrapolated 2011 national costs were $3.9 billion.Rising costs over time appear to reflect the rising prevalence of ED visits for dizziness and increased rates of imaging use.

Stroke 2015;46:108-113
All Eds in Ontario, years 2006-2011.Among 41794 qualifying patients, 8596 (20.6%) received ED head CT imaging, and 99.8% of these patients were able to be matched to a control.One fifth of patients diagnosed with peripheral vertigo in Ontario received imaging that is not recommended in guidelines.

20 EDs in California, year 2008.Of 378 992 patients seen in 2008, 20 795 (5.5%) had at least one ED visit for dizziness.Overall, 5585 patients (26.9%) had a head CT and 652 (3.1%) had a brain MRI.Higher neuroimaging rates did not translate into higher stroke diagnoses rates.The use of neuroimaging for ED patients with dizziness varies substantially without an associated improvement in stroke diagnosis.

Laryngoscope, 2013;123:2250–2253
Of 1681 patients identified, 810 (48%) received CT brain/head scan.Of these, only 0.74% yielded clinically significant pathology requiring intervention.However, 12.2% of MRI studies yielded discovery of significant abnormalities.These data reveal a great opportunity for cost savings by developing stricter guidelines for ordering CT scans for this set of ED patients.However, appropriately directed MRI of the brain is recommended in patients with dizziness and other neurological signs or symptoms.

Mayo Clin Proc. 2012;87:1080-1088
Academic ED, years 2007-2009.Of 907 patients experiencing dizziness (mean age, 59 years), 49 (5%) had a serious neurologic diagnosis, including 37 cerebrovascular events. Dizziness was often caused by benign conditions, such as peripheral vertigo (294 patients [32%]) or orthostatic hypotension (121 patients [13%]).Age 60 years or older (OR, 5.7), a chief complaint of imbalance (OR, 5.9), and any focal examination abnormality (OR, 5.9) were independently associated with serious neurologic diagnoses, whereas isolated dizziness symptoms were inversely associated (OR, 0.2).

Ann Emerg Med. 2011;57:34-41
California EDs, year 2005. 31,159 patients.The 180-day cumulative incidence of vascular event, cerebrovascular event, or cardiovascular event was 0.93%, 0.63%, and 0.32% respectively.Few patients experience a major vascular event after discharge home with a diagnosis of dizziness or vertigo, with a stroke occurring in less than 1 in 500 patients within the first month.

1°versione 2011
PS/MURGORLNeurologiaNeuroradiologiaGoverno Clinico

Criteri d’inclusione: Tutti i pazienti che si sono presentati al PS di Parma nel 1°semestre 2009 riferendo, come sintomo principale, vertigine, capogiri o disequilibrio.
Criteri d’esclusione:
Pazienti che risultavano affetti, già dalla valutazione
iniziale, da pseudo-vertigine, ipotensione severa, panic-
attack
Analisi della situazione locale.

Accessi al Pronto Soccorso - I Semestre 2009Totale pazienti con accesso al P.S.: 42.940
Totale pazienti con accesso al P.S. per vertigine: 516 (circa 1,3% degli accessi)Sesso : maschi 203 (40%); femmine 313 (60%)
Indagini di 1°livello (ECG, esami ematochimici): 377 (73%)
Utilizzo di indagini neuroradiologiche TAC encefalo:
140 (27%), di cui il 33% chieste dal Medico di P.S. e il 67% dal Neurologo
Percentuale di ricovero :Su 516 pazienti 65 (12%) sono stati ricoverati di cui: 18 in MU, 15 in Neurologia,
7 in ORL, 25 in reparti di Medicina.
I pazienti dimessi sono stati 451 (88%): fra questi 27 (5% del totale) dopo un
periodo di osservazione breve intensiva (OBI).

Età pazienti ricoverati

Consulenze richieste da P.S.:
Su 516 pazienti 319 (62%) hanno ricevuto una consulenza specialistica;
di questi 62 (12%) hanno ricevuto entrambe le consulenze (neurologica e ORL)
Farmaci utilizzati nei pazienti trattati in acuto in Pronto Soccorso:
Su 516 pazienti 137 (26%) hanno ricevuto terapia direttamente in P.S.;
i farmaci utilizzati sono stati i seguenti:
FANS (4,5%)
Antidopaminergici e Antiemetici (Levosulpiride, metoclopramide, ondansetron)
(24,5%)
Benzodiazepine (3%)


Risultati?
Neurologo
ORL

HINTS

Stroke. 2009;40:3504-3510
• Head-Impulse
• Nystagmus
• Test-of-Skew

ACAD EMERG MED 2013;20:987–996
HINTS stroke sensitivity was 96.5%, specificity was 84.4%, LR+ was 6.19, and LR– was 0.04 and did not vary by age. For any central lesion, sensitivity was 96.8%, specificity was 98.5%,LR+ was 63.9, and LR– was 0.03 for HINTS Sensitivity was 99.2%, specificity was 97.0%, LR+ was 32.7, and LR– was 0.01 for HINTS “plus” (any new hearing loss added to HINTS). Initial MRIs were falsely negative in 15 of 105 (14.3%) infarctions; all but one was obtained before 48 hours after onset, and all were confirmed by delayed MRI.

ACAD EMERG MED 2013;20:987–996

ACTA Otorhinolaryngologica Italica 2014;34:419-26
Emergency Medicine Australasia 2015;27:126-31
Mayo Clin Proc. 2008;83:765-775

Giusto per complicare un po’ le cose…

Acta Otolaryngol. 2014;134:1140-5
Taura A, Funabiki K, Ohgita H, Ogino E, Torii H, Matsunaga M, Ito J.
One-third of vertiginous episodes during the follow-up period are caused by benign paroxysmal positional vertigo in patients with Meniere's disease.
296 patients with Meniere's disease, followed for 12 months187 vertiginous episodes (37.9%) were caused by BPPVThe lateral semicircular canal was the most frequently involved canal

Any space for biomarkers?

ACAD EMER MED 2014;21:736–741












![LA VERTIGINE PAROSSISTICA POSIZIONALE: I TEST …cenavest.altervista.org/pdfrelazioni/Vietri 2015/Califano_-Test... · THE ROLLING STONES SATISFACTION [OFFICIAL VIDEO].mpg . Title:](https://img.pdfslide.net/doc/110x75/5ee2d980ad6a402d666d1519/la-vertigine-parossistica-posizionale-i-test-2015califano-test-the-rolling.jpg)













![[Una vertigine ma non solo una vertigine!!!!!] Dr. ssa Lidia Catarzi Dr. Gianni Taccetti Ictus tra territorio ed ospedale](https://img.pdfslide.net/doc/110x75/5542eb59497959361e8c4bfc/una-vertigine-ma-non-solo-una-vertigine-dr-ssa-lidia-catarzi-dr-gianni-taccetti-ictus-tra-territorio-ed-ospedale.jpg)





