Embed Size (px)
Citation preview

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 1/7
From Figures to Values: The Implicit Ethical
Judgements in our Measures of Health
Paolo VineisÃ, School of Public Health, Imperial College London
Roberto Satolli, Zadig, Milano Italy
ÃCorresponding author: Paolo Vineis, School of Public Health, Imperial College London, St Mary’s Campus, Norfolk Place W2 1PG London.
Tel: +44 (0)20 75943372; Fax: +44 (0)20 75943196; Email: [email protected]
The objective of the article is to examine the extensions of a clinical measure of efficacy, the Number Needed to
Treat (NNT), in different settings including screening, scanning, genetic testing and primary prevention, and the
associated ethical implications. We examine several situations in which the use of the NNT or NNS (Number
Needed to Screen) has been suggested, such as Prostate-Specific Antigen for prostate cancer, Magnetic
Resonance Imaging scans, genetic testing and banning of smoking. For each application, we explore the ethical
implications of the relevant measure. We have found that the different measures have different ethical impli-
cations. For example, the Number Needed to Prevent is the only measure that can be lower than one, indicating
with a numerical example that prevention is better than cure. Conversely, we raise questions about the accept-
ability of genetic screening. In a realistic example, we show that primary prevention of the effects of arsenic in
drinking water, targeted to the most susceptible, would require to genetically screen a large number of subjects,
whereas giving rise to ethical concerns. We warn against the abuse of testing, in particular genetic testing, we
show that different measures are associated with different ethical issues and that prevention tends to be better
than cure.
Introduction
How the impact of medical and preventive activities is
measured is one of the important issues that epidemi-
ologists face, and it has moral implications. The purpose
of this article is to show how different measures of treat-
ment and prevention are associated with very different
impacts for the populations involved, and entail differ-
ent moral implications. For the aim of this analysis, any
clinical or public health intervention can be considered
worthy on the basis of two ethical principles: (i) benefits
should exceed harm (beneficence) and (ii) the priority in
the use of public resources should be for interventions
that produce more benefits for more people (utility).
Number Needed to Treat
The Number Needed to Treat (NNT) is probably the
most useful single figure that one needs to know in order
to judge the efficacy of a therapy, and in fact of any
medical intervention. Its properties have been
described—see (Schulzer and Mancini, 1996) and
(Walter, 2001) for reviews and a discussion of statistical
aspects—and its use has thrived in the last decades—see
(Zulman et al., 2008) for an application to Public
Health strategies. It is a summary measure that allows
the physician to estimate how many patients need toreceive a treatment to have a benefit, it can be compared
with the expected burden of side-effects, with alternative
courses of action, and can lead to a cost–benefit analysis.
However, its extensions to testing, screening, scanning
(including incidental findings) and primary prevention
have not been fully explored and will be analysed here
from a public health perspective.
By examining different scenarios, we will address the
moral implications involved in the use of the NNT and
derived measures.
Scenario 1: Therapy and Tertiary Prevention
The NNT is the number of patients that is necessary to
treat with a drug or any other medical intervention to
save one life, to avoid the loss of 1 year of life (or of one
Quality Adjusted Life Years (QALY)), or to reduce other
specified adverse health outcomes. The NNT (Box 1) is a
function of the efficacy of the therapy and of the fre-
quency of the outcome we want to avoid or prevent.
PUBLIC HEALTH ETHICS VOLUME 5 NUMBER 1 2012 22–28 22
doi:10.1093/phe/phs003
! The Author 2012. Published by Oxford University Press. Available online at www.phe.oxfordjournals.org

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 2/7
When the therapy is very effective, like surgery for
appendicitis, and the outcome is frequent in the absence
of intervention, then the NNT is very close to 1, i.e. we
save almost all patients who are treated. This is a very
uncommon occurrence in medicine, and most NNTs
fluctuate around 50–500. Notice that the NNT may be
high, even for a common adverse outcome, not only if
the therapy is ineffective, but also if spontaneous recov-
ery occurs, since the measure of efficacy is based on acomparison between treated and untreated patients
(Box 1). Therefore, we may have a very high NNT in
the case of pancreatic cancer (frequency of death 100%,
highly ineffective therapies), but also for the therapy of
the common influenza, depending on the day of obser-
vation (with very high rate of spontaneous recoveries a
few days after treatment initiation).
The NNT increases with a decreasing frequency of the
outcome, whereas in contrast adverse side-effects of
therapies have the same occurrence rate, irrespectively
of the frequency of the outcome that we want to prevent.
For example, there is a fixed proportion of subjects who
will undergo aplastic anaemia after treatment with ibu-
profen, whether or not the drug is properly used in ser-
iously sick patients who really need it or inappropriately
used in subjects with a mild and self-containing disease.
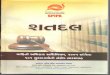
This relationship is represented in Figure 1, which shows
that treatment should be initiated only when the advan-
tages overcome the side-effects. This well-known Figure
is usually applied to therapies, but common sense would
suggest to apply it to any medical act. Walter and
Sinclair (2009) have recently analysed the issue of
the ‘minimum target event risk for treatment’, i.e. the
threshold to undertake a treatment, and they noticed the
frequent lack of information that may allow an
informed decision.
The ‘first ethical implication’ is that any benefit
should be compared with side-effects, and the two are
asymmetric, because only benefits of treatment are
influenced by the frequency of the outcome, so thatdamage without benefit can easily occur for rare out-
comes. Benefit and harm are asymmetric also because
they do not necessarily refer to the same persons, so that
an intervention can slightly harm a large number of
people in order to benefit only one person. These two
asymmetries are in contrast with both the principles of
beneficence and of utility.
Number Needed to Test
Suppose that a doctor wants to prescribe a
Computerized Tomography (CT) for joint pain. If it is
highly likely that the CT will help her/him—to decide
whether to treat the patient or not, then the NNT for
therapy can be simply estimated for the treated subjects.
But if any treatment is unlikely to be undertaken, why is
the test performed? Has the doctor considered the po-
tential side-effects of the CT for the patient? In this cir-
cumstance, it seems reasonable to estimate not actually
the NNT, but the Number Needed to Test. In the case of
Box 1. Example of a measure of treatment efficacy
Let us consider a drug that is supposed to prevent heart disease (e.g. a statin). To express its efficacy, one can
calculate the frequency of deaths or of illnesses, after a sufficiently long time, in the treated group compared with
the control group. In a large study in healthy subjects with normal cholesterol, but with an altered level of an
inflammation marker (CRP) (the Jupiter study), the deaths were 12.5 per year every 1000 people in the control
group, and 10 in those treated with the drug. The two frequencies can be compared by calculating the difference(i.e. the deaths decreased by 2.5 per 1000 per year). However, this measure is rarely used to communicate benefits.
The authors of clinical trials prefer to calculate the percent of risk reduction in the treated arm compared with
controls, in this case 20 per cent (i.e. 2.5 divided by 12.5). In this way, the apparently modest absolute result is
transformed into a more attractive relative reduction. In other words, when the basal risk is low, even a modest
absolute benefit translates into an apparently large relative benefit. However, one of the most useful measures is the
NNT in order to avoid one adverse event such as death. In our example, the drug benefits 12.5 patients out of 1000
treated for 5 years (2.5 multiplied by 5 years). This means that (1000 divided by 12.5) subjects need to be treated to
obtain one benefit, i.e. to avoid one death. The NNT is thus 80 subjects. Is it large or small? To give an idea,
70 elderly patients with hypertension need to be treated for 5 years with anti-hypertensives, in order to avoid one
death; or, 100 male adults with no sign of heart disease need to take aspirin for 5 years in order to avoid an
infarction. Not only is the NNT an easily interpretable measure, but also allows comparative analyses including
costs. For example, if a year of therapy against cholesterol costs E1000 per patient; then approximately E400,000are needed to prevent one death by treating 80 people for 5 years.
FROM FIGURES TO VALUES 23

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 3/7
appendicitis, diagnosis is very simple, and in most cases
all patients undergoing the relevant tests will have thecorrect diagnosis and will be saved by surgery. But this is
clearly an exception. The doctor may decide to perform
a CT scan in 1000 patients with joint pain to identify the
10 who can theoretically benefit from a specific therapy.
The NNT for those 10 patients may be, say, 10 (to be
optimistic), i.e. out of the 10 patients with that condi-
tion who are treated, only 1 will recover, thanks to the
treatment. The other nine will get the drug (with its
side-effects) with no benefit. But we also have to include
in the equation the 990 patients who underwent a CT
scan with no gain. Therefore, the Number Needed to
Test is in fact 999, and among the side-effects, we have to
count also those of the diagnostic test. Again, the fre-
quency of the side-effects is independent of the efficacy
(or lack of) of the treatment and of the frequency of the
outcome.
The ‘second moral implication’ is that testing itself
(not only treatment) can lead to a large number of use-
less interventions, and the related discomfort. In fact,
the ratio between useful and useless interventions can be
much higher than for the NNT. Therefore, the calcula-
tion of the Number Needed to Test is more useful than
the NNT in evaluating the beneficence and utility of any medical intervention.
Scenario 2: Secondary Prevention—the
Example of PSA Testing
The 1000 hypothetical patients above were all affected
by joint pain. What about a screening scenario, such as
Prostate-Specific Antigen (PSA) for prostate cancer?
This situation is similar to the estimation of Number
Needed to Test, but the computation needs to incorp-
orate the prevalence of the condition in asymptomatic
subjects. It is like the Number Needed to Test but in the
absence of signs and symptoms, and therefore with a
usually much lower disease prevalence. In fact, the
Number Needed to Screen (NNS) for breast cancer
screening, e.g. is around 2500–20,000, depending on
the age bands. This means that at least 2500 women
will undergo the screening test to identify a fraction
who have a potentially malignant lesion, among whom
there is one who will be saved by the screening activity.
This leads to a ‘third moral implication’, i.e. the over-
all effect of a screening test in asymptomatic subjects
depends on the prevalence of the asymptomatic condi-
tion, so that a test has completely different effectiveness,
e.g. in different age groups, and in accord to the prin-
ciples of beneficence and utility should not be offered to
a population with a low prevalence of the condition,
when the expected benefits are likely to be exceeded by the harm.
According to one study, 3 million American men
aged 40–74 years would show abnormal PSA levels if
screened (>4.0 nanograms per millilitre; with a pro-
posed threshold of 2.5 nanograms per millilitre, an add-
itional 3 million men would be abnormal). However,
only 0.4 per cent of men in the age range 40–74 years
are expected to die every year from prostate cancer. Let
us suppose that screening reduces the risk of dying by 20
per cent, probably an optimistic estimate [this is the
estimate found in the European ERSPC trial, not in
the American PLCO (Andriole et al., 2009; Schroder
et al., 2009)]. With the figures given in the recent
ERSPC report (Schroder et al., 2009), the absolute risk
reduction is 0.7 per 1000 in 10 years, which gives a NNS
to save a life of 1400 (1/0.0007), a rather high value.
Another way to estimate the impact is to say that 48
additional tumours need to be treated to prevent one
death (Schroder et al., 2009). This means that approxi-
mately 1399 subjects will undergo screening with no
benefit, and 47/48 will suffer from all the complications
related to prostatectomy with no real gain in survival.
If we consider the different life expectations, the NNS toavoid the loss of 1 year (or a QALY) would probably be
higher for older people (70 years), in spite of the
higher prevalence of the cancer.
Scenario 3: Disease Prediction—the Example
of Genetic Testing
One can argue that breast cancer screening is useful
indeed, at least over the age of 50 years; and perhaps,
Figure 1. The Figure shows that with an increasing
frequency of health effects (outcomes) the NNT is lower,
i.e. the benefits of treatment are higher, whereas harm is
independent of the frequency of outcomes (see also Box 1).
24 VINEIS AND SATOLLI

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 4/7
less convincingly, that also PSA screening may be useful.
But there are instances in which no benefit can be
demonstrated. One such instance is screening for
low-penetrant genetic variants. Let us consider what
the website of Decode, an Icelandic firm specialized in
genetic research, offers. They suggest that by sending
them a blood sample they can identify the gene variants
that predispose to cancer and other chronic diseases.
What happens if one has a ‘bad gene’? There are in
fact only two possibilities: one is early diagnosis by a
screening test such as mammography, a strategy used
in women with Breast Cancer 1 (BRCA1) mutations; the
other is a primary preventive strategy, e.g. quitting
smoking for a smoking-related cancer.
Here, we are interested in the methodological proper-
ties of the NNT and the ensuing moral implications.
According to Decode’s website to predict the onset of
bladder cancer, a smoking-related cancer, they will look
at two gene variants, one in the region 8q24 (chromo-some 8) and the other in 5p15 (chromosome 5). Is it
useful? Will one be benefited? It is very hard to say, since
Decode does not explain what one is supposed to do
with the genetic information they offer. The only ways
to make use of such information are either to prevent
exposures to carcinogens or to screen the carriers of the
variant(s) with greater intensity than non-carriers.
Unfortunately, the second possibility does not apply in
this situation since there is no effective early detection
test for bladder cancer.
The ‘fourth moral implication’ is that, for beneficence
and utility, no testing should be done when an effectiveintervention is not available.
Let us then imagine that we screen people in order to
suggest them to avoid exposure to a bladder carcinogen,
such as arsenic. The example is purely theoretical and
has been fully developed elsewhere (Vineis et al., 2005).
We hypothesize that the relative risk associated with the
gene variant is 1.5 (low penetrance), that the cumulative
risk for bladder cancer is 1 per cent in the normal popu-
lation (1.5 per cent among the carriers of the gene vari-
ant), and that reduction or elimination of exposure to
arsenic leads to a 50 per cent reduction in the risk of
bladder cancer (all realistic assumptions). This means
that the cumulative risk after intervention is 0.75 per
cent in carriers of the gene variant, and the risk reduc-
tion becomes 0.015–0.0075, i.e. 0.75 pre cent, leading to
a NNT of 133 (1/0.75). Under this scenario, if the
exposure to arsenic is reduced only in the carriers of
the variant, we will need to ‘treat’ (i.e. to reduce expos-
ure for) 133 exposed subjects to prevent one case. If
exposure to arsenic is instead reduced for the ‘wild-type’
(again with an efficacy of 50 per cent), then the NNT is
200. The difference between 133 and 200 is clearly not
striking, i.e. selecting those with the gene variant is not
particularly advantageous. But there is a further com-
plication, because we need to screen the population to
identify the variant carriers; the wild-type occurs in 80
per cent of the people, the variant only in 20 per cent.
This means it would be necessary to screen 666 subjects
to identify the 133 to ‘treat ’ with preventive policies to
avoid one case of cancer (if we want to treat only the
variant carriers). So the costs and side-effects of screen-
ing may not be worthwhile, even without considering
ethical issues related to utility, etc.
Thus, the ‘fifth moral implication’ is that testing may
divert attention from a more equitable and effective
(on a population basis) intervention, in this case pri-
mary prevention.
Scenario 4: Incidental Findings—the Exampleof Brain Imaging
A clear example of a recent application of the NNTest is
a meta-analysis of studies on brain magnetic resonance
imaging (MRI), in which a rather high prevalence
(0.7%) of incidental findings occurs (Morris et al.,
2009). We could discuss whether this is screening or
not: usually, MRI is done because of symptoms, but
often it is done for research, and in any case incidental
findings arise that are unrelated to the symptoms.
Screening is usually not the purpose, or at least
the requirements of a screening test are not met.Clinicians do not know yet how to deal with incidental
findings, such as aneurysms, and guidelines are not
available. The authors of the meta-analysis use (appar-
ently for the first time) what they call the Number
Needed to Scan , which is only 50 for ‘any non-neoplastic
incidental finding’, clearly a very low figure: every 50
scans, one will be considered suspect or pathological.
It is worth noting that this Number Needed to Scan
has little to do with the NNT (or to screen), which is
the number of patients we need to treat/screen to avoid
one adverse outcome like death. In the case of scanning,
the index just tells us the number we need to scan to find
one positive result of any kind, irrespective of treatment
efficacy or usefulness of the finding.
It seems that the risk of haemorrhage from unrup-
tured aneurysms is low, but MRI is too recent to allow
for a sufficiently long follow-up. In contrast, the risk of
stroke or death from surgical interventions is sizable. In
practice, we do not know where we are positioned in the
graph of risks versus benefits shown in Figure 1.
Consider also that 94 per cent of meningiomas remain
FROM FIGURES TO VALUES 25

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 5/7
asymptomatic and 63 per cent do not grow. On the
other side, the occasional discovery of a brain lesion
for the patient means the loss of the driving licence,
insurance and (in some countries and for some jobs)
of employment. These are all side-effects of the MRI that
do not depend on the efficacy of treatments and the
frequency of the outcomes.
This example is an extension of the fifth moral impli-
cation. In this case, not only there is no known beneficial
intervention, but also even the natural history of the
disease is little understood.
Scenario 5: the Number Needed to Prevent
As an article in the New York Times stated in January
2007, for most Americans, the biggest health threat is
not avian flu, West Nile or mad cow disease. Its their
health-care system: ‘advanced technology allows doctors
to look really hard for things to be wrong. We can detecttrace molecules in the blood. We can direct fiber-optic
devices into every orifice. And CT scans, ultrasounds,
MRI and PET scans let doctors define subtle struc-
tural defects deep inside the body. These technologies
make it possible to give a diagnosis to just about
everybody . . . Second, the rules are changing. Expert
panels constantly expand what constitutes disease:
thresholds for diagnosing diabetes, hypertension,
osteoporosis and obesity have all fallen in the last few
years. The criterion for normal cholesterol has dropped
multiple times. With these changes, disease can now be
diagnosed in more than half the population’.
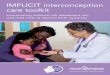
In more technical terms, this escalation is represented
in Figure 2 that shows how the NNT or NNS is increas-
ing when we move to the left from death or frank symp-
tomatic disease to early diagnosis and to ‘pre-clinical
conditions’. In fact, this encompasses a series of meas-
ures that include the NNT on the right, then the
Number Needed to Test, then the NNS on the left.
The latter shift has repeatedly occurred in recent years
with almost all the thresholds used for diagnostic pur-
poses: cholesterol from 160 to 130 or 100 milligrams per
decilitre, fasting glycaemia from 140 milligrams per
decilitre to 126 milligrams per decilitre, systolic blood
pressure from 160 to 140 mmHg and then 120 mmHg. If
we add genetic testing for inherited susceptibility to dis-
ease, the NNT/NNS shifts further to the left in Figure 2.One important property of prevention is that the
NNP (Number Needed to Prevent one case of disease)
can be<1. This apparently paradoxical situation occurs
when a relatively limited preventive action has an
impact that goes beyond those who are directly affected
by it, e.g. for an indirect fallout. The typical example is
herd immunity : vaccinating a relatively limited number
of subjects prevents the disease in many more, e.g.
Figure 2. The vertical axis shows the NNT, the number of subjects who need to be examined and treated to avoid one adverse
effect such as death. The dark grey area represents those who are beyond the clinical threshold, i.e. those who already suffer
from symptoms or have signs of disease. The light grey area includes those who are considered ill only because they are above
a certain threshold such as glycaemia, though they still feel well. With a decreasing threshold in asymptomatic persons, the
NNT increases (to the left).
26 VINEIS AND SATOLLI

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 6/7
treating 10, we save 100. Similarly, banning smoking in
public places has a positive effect not only in those po-
tentially exposed to second-hand smoke (the target
population), but also in smokers, who will smoke less.
Zulman et al. (2008) have considered how the NNT
helps disentangling the efficacies of different public
health strategies, including focused strategies aimed athigh-risk groups, versus unfocused strategies aimed at
the general population. They notice that a population-
based intervention is a good option (in terms of NNT,
though it should be more adequately called NNP) if
there are no adverse effects, whereas a targeted approach
may prevent more deaths while treating fewer people if
adverse effects are present.
The ‘sixth moral implication’ seems to be that pre-
vention is better than cure also for a very technical
reason, related to utility and beneficence, i.e. at least in
certain cases the ratio between the ‘treated’ individuals
and the benefited individuals is <1.
Conclusions
By reviewing the different measures related to the ori-
ginal NNT (as summarized in Table 1), we have identi-
fied some interesting features of each of them. In
exceptional cases, the NNT is 1, when all patients
would die and all are saved; but usually the NNT is
>1, and it is even greater if we consider the Number
Needed to Test rather than the NNT, i.e. we include in
the denominator all the subjects who undergo a diag-
nostic test rather than only those who are offered the
treatment. By definition, the NNS is greater than the
NNT, because it involves asymptomatic persons whose
disease prevalence is lower than for the symptomatic
ones. If we want to screen for genetic susceptibility, as
several commercial laboratories now propose, we
have to compare the benefits gained by screening and
treating only the susceptibles, with the benefits
obtained by treating the whole population. At least for
low-penetrant genes, we may conclude that the overall
effort is far from being justified, as our example of
arsenic shows. Clearly, if there is no benefit (or benefits
are unknown, like in the case of the Number Needed to
Scan with MRI), the NNS tends to infinity.
Finally, if we extend the reasoning to primary preven-
tion, we discover an interesting property of the NNP,i.e. it is the only measure that can be <1, when the
benefit of prevention goes beyond the target of the pre-
ventive effort. Such situations can be much more fre-
quent than we think, from herd immunity to climate
change. In general, we can say that the different meas-
ures related to the original NNT can also be used as
proxies of the adherence of an intervention to the ethical
principles of beneficence and utility.
Acknowledgements
We are grateful to Michael Parker (Ethox, Oxford) for
useful suggestions.
Conflict of interest
None declared.
References
Andriole, G. L., Crawford, E. D., Grubb, R. L. 3rd, Buys,
S. S., Chia, D., Church, T. R., Fouad, M. N.,
Gelmann, E. P., Kvale, P. A., Reding, D. J.,
Weissfeld, J. L., Yokochi, L. A., O’Brien, B., Clapp,
J. D., Rathmell, J. M., Riley, T. L., Hayes, R. B.,
Kramer, B. S., Izmirlian, G., Miller, A. B., Pinsky,
P. F., Prorok, P. C., Gohagan, J. K. and Berg, C. D.
(2009). Mortality Results from a Randomized
Prostate-cancer Screening Trial. New England
Journal of Medicine , 360, 1310–1319.
Table 1. Properties of the different measures described in the text
Measure Components Range Examples
NNTreat Relative risk frequency of outcome 1 to infinity Surgery for acute
appendicitis
NNTest Same plus prevalence of disease
in symptomatic persons
>1 to infinity MRI for joint pain
NNScreen Same plus prevalence of pre-clinical
condition in asymptomatic persons
>1 to infinity Mammography
NNPrevent Relative Risk Frequency of outcome 1 to >1 Herd immunity
FROM FIGURES TO VALUES 27

7/28/2019 VINEIS__From Figures to Values the Implicit Ethical Judgements in Our Measures of Health
http://slidepdf.com/reader/full/vineisfrom-figures-to-values-the-implicit-ethical-judgements-in-our-measures 7/7
Morris, Z., Whiteley, W. N., Longstreth, W. T. Jr,
Weber, F., Lee, Y. C., Tsushima, Y., Alphs, H.,
Ladd, S. C., Warlow, C., Wardlaw, J. M. and
Al-Shahi Salman, R. (2009). Incidental Findings on
Brain Magnetic Resonance Imaging: Systematic
Review and Meta-analysis. BMJ , 339, b3016.
Schroder, F. H., Hugosson, J., Roobol, M. J., Tammela,
T. L., Ciatto, S., Nelen, V., Kwiatkowski, M., Lujan,
M., Lilja, H., Zappa, M., Denis, L. J., Recker, F.,
Berenguer, A., Maattanen, L., Bangma, C. H., Aus,
G., Villers, A., Rebillard, X., van der Kwast, T.,
Blijenberg, B. G., Moss, S. M., de Koning, H. J. and
Auvinen, A. (2009). Screening and Prostate-cancer
Mortality in a Randomized European Study. New
England Journal of Medicine , 360, 1320–1328.
Schulzer, M. and Mancini, G. B. (1996). ‘Unqualified
Success’ and ‘unmitigated Failure’: Number-
needed-to-treat-related Concepts for Assessing
Treatment Efficacy in the Presence of Treatment-
induced Adverse Events. International Journal of
Epidemiology , 25, 704–712.
Vineis, P., Ahsan, H. and Parker, M. (2005).
Genetic Screening and Occupational and Environ-
mental Exposures. Journal of Occupational and
Environmental Medicine , 62, 657–662, 597.
Walter, S. D. (2001). Number Needed to Treat (NNT):
Estimation of a Measure of Clinical Benefit. Statistics
in Medicine , 20, 3947–3962.
Walter, S. D. and Sinclair, J. C. (2009). Uncertainty in
the Minimum Event Risk to Justify Treatment was
Evaluated. Journal of Clinical Epidemiology , 62,
816–824.
Zulman, D. M., Vijan, S., Omenn, G. S. and Hayward,
R. A. (2008). The Relative Merits of Population-
based and Targeted Prevention Strategies. Milbank
Quarterly , 86, 557–580.
28 VINEIS AND SATOLLI