Embed Size (px)
Citation preview

Violence in mental health care:the experiences of mental health nursesand psychiatrists
Peter Nolan PhD RGN RMN
Professor of Mental Health Nursing, School of Health Sciences,
University of Birmingham
Janie Dallender MSc
Research Associate, School of Health Sciences,
University of Birmingham, Birmingham, England
Joaquim Soares PhD
Senior Researcher, Centre for the Development of Health Sciences, Stockholm
Sarah Thomsen MPH
Research Associate, National Institute for Psychosocial Factors and Health,
Stockholm
and Bengt Arnetz MD PhD
Professor of Psychosocial Medicine, National Institute
for Psychosocial Factors and Health, Stockholm, Sweden
Accepted for publication 8 January 1999
NOLANNOLAN PP., DALLENDERDALLENDER JJ., SOARESSOARES JJ., THOMSENTHOMSEN SS. && ARNETZARNETZ BB. (1999)(1999) Journal of
Advanced Nursing 30(4), 934±941
Violence in mental health care: the experiences of mental health nurses
and psychiatrists
Violence against mental health service personnel is a serious workplace
problem and one that appears to be increasing. This study aimed to ascertain the
extent and nature of violence against mental health nurses and psychiatrists,
and to identify what support, if any, they received following exposure to
violence. Mental health staff working within ®ve West Midlands Trusts in the
United Kingdom were surveyed using a postal questionnaire to investigate the
extent and nature of violence they encountered in their daily work. There was
an overall response rate of 47%, which included a response rate for psychia-
trists of 60% (n� 74) and for mental health nurses of 45% (n� 301). Though
both groups experienced violence at work, nurses were found: to have been
exposed to violence signi®cantly more during their career; to have been a victim
of violence within the previous 12 months of the survey; and to have suffered a
violent incident involving physical contact. Whilst a higher proportion of
nurses than psychiatrists received some support following a violent incident, a
large proportion of both groups did not receive any, although most felt in need
of it. The implications of this study for training and management are discussed.
Correspondence: Peter Nolan, School of Health Sciences,
The Medical School, Edgbaston, Birmingham B15 2TT, England.
Journal of Advanced Nursing, 1999, 30(4), 934±941 Experience throughout the nursing career
934 Ó 1999 Blackwell Science Ltd

Keywords: management, mental health nurses, psychiatrists, support,
training, violence, workplace
INTRODUCTION
The possible relationship between violence and mental
illness has long been the subject of interest to researchers,
although many con¯icting conclusions have been reached
(Wessely & Taylor 1991). However, in the mind of the
general public, and in the experiences of some health
professionals, this relationship remains a strong one (Scull
1979). Most mental health professionals encounter various
forms of violence at some time during their working lives.
In the United Kingdom (UK) there has been a tendency
either to ignore such incidents or accept them as an
inevitable part of mental health care. Glennister (1997)
remarks that there is an unquestioned assumption in the
literature that caring always lies at the heart of the mental
health services and consequently issues such as social
control, coercion and violence, are rarely acknowledged or
discussed.
The former General Nursing Council for England and
Wales issued a directive in 1974 stating that all mental
health nurses should be instructed in the care and
management of violent patients but gave no guidance as
to how this could be achieved (General Nursing Council
1974). Violence at work was also addressed by the Health &
Safety At Work Act (1974), in which it was stated that
employers had a statutory duty to render the work
environment safe for employees, especially those who
were likely to encounter aggression and con¯ict.
Little by way of quanti®cation of violence in health care
settings was undertaken until the Health and Safety
Commission (1987) published a report of a survey of
health service employees which asked them to specify the
extent to which they had been involved in violent
episodes. The ®ndings provided, for the ®rst time, an
estimation of the extent of violence encountered by staff in
health services. The survey stated that less than 1% of
those surveyed had suffered major injury requiring
medical assistance, but 11% had suffered minor injuries
requiring ®rst aid, 5% had been threatened with a weapon
and more than 18% had been threatened verbally. Such
was the impact of the report that the Confederation of
Health Service Employees (COHSE) considered suing
health authorities that failed to take appropriate action
to protect the well-being of their employees (Mason 1991).
Commenting on the prevalence of violence in health care,
Evans (1991) stated that it is unacceptable that a vast
health network should offer employees working under
considerable pressure less protection than is provided in
any other industry.
LITERATURE REVIEW
Despite much effort to educate all those working in health
care settings in the prevention and management of violent
incidents, it is now recognized that violence poses an
increasing problem for mental health service employees
(Hansen 1996). Estimating the exact prevalence of
violence remains elusive due to failure to agree on
operational de®nitions (Love & Hunter 1996), various
methodological problems encountered when comparing
mixed concepts and constructs (Wessely & Taylor 1991),
and the wide variation in the way violent incidents are
reported and recorded (Shah et al. 1991). The term
`violence' has been applied to behaviours ranging from
mild verbal abuse to grievous bodily harm, so it is not
surprising that studies report great variation in the
prevalence of violence depending on the settings studied
(Dublin & Lion 1992). Because of this, caution needs to be
exercised when reviewing prevalence rates, as it is highly
likely that published ®gures underestimate the extent of
the problem (Love & Hunter 1996).
Nonetheless, the number and nature of injuries
sustained by nurses as a result of violence has been
estimated to be higher than the number of injuries
reported in what are considered to be high risk industries
such as mining, forestry and heavy construction (Love &
Hunter 1996). Furthermore, there is overwhelming
evidence that nurses are more likely to be physically
assaulted, threatened and verbally abused than any other
health professional group (Whittington et al. 1996).
Weiser et al. (1994) estimated that approximately 10%
of psychiatric patients are violent towards staff. The same
study also reported that 50% of psychiatric staff have been
physically assaulted at some time during their careers.
Ruben et al. (1980) and Madden et al. (1976) concluded
that approximately 50% of psychiatrists had been assaulted
during the course of their work and, in a multinational
survey, Poster (1996) found that 75% of mental health
nurses had been physically assaulted at least once in their
careers. Whittington & Wykes (1994) found that 65% of
nurses in their sample had been violently assaulted by
patients, and Arnetz et al. (1996) concluded that 30% of
Swedish nurses experienced violence at work.
Precursors of violence
Violent behaviour is observed more frequently in some
patients than others, for example in younger patients
(James et al. 1990), those who have been violent prior to
Experience throughout the nursing career Violence in mental health care
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941 935

admission (Conn & Lion 1983), and those with severe
forms of mental illness (Pearson et al. 1986). Other
precursors of violence include confusional states, non-
compliance with medication (Whittington et al. 1996),
short hospital stays in overcrowded wards (Edwards & Reid
1983), poor staff±patient ratios (Yates 1981), increased
rates of admission (Adler et al. 1983), and especially
clients with criminal histories and personality disorders
(Hansen 1996). Martin (1984) reviewed the reports of all
psychiatric hospital inquiries in the UK published during
the 1960s and 1970s and found that amongst the conditions
likely to lead to violent incidents was the practice of
entrusting large numbers of seriously mentally ill patients
to the care of a few poorly trained staff for prolonged
periods in a therapeutically impoverished environment.
Attempting to reduce the levels of violence in mental
health care settings is problematic for, as Cahn (1995) and
Wessely & Taylor (1991) have observed, violence and
mental illness seem to coexist in some patients.
There is some evidence to support the claim that victims
of violence have certain predisposing characteristics
(Arnetz et al. 19961 ), although this has been challenged by
Whittington & Wykes (1994). Support for this claim is based
on the ®nding that approximately 5% of staff are involved
in 20% of reported violent incidents (Hodgkinson et al.
19852 ). Poster (1996) found a signi®cant difference between
those who reported previous assaults and those who did
not, the former being more likely to expect an assault than
the latter. The adoption of authoritarian attitudes, failing to
involve medical staff, poor communication (Brailsford &
Stevenson 1973), demoralization and incompetence (Depp
1983) have been found to be signi®cantly associated with
staff who reported higher rates of assault.
Younger staff, those with limited experience of health
care and especially those who work permanently on night
duty, have been found to be particularly vulnerable to
violence in the workplace (Whittington et al. 1996), as are
those who express dissatisfaction with their work and
those who suffer from work-related musculo-skeletal
injuries (Arnetz et al. 1996). The study by Arnetz et al. also
found signi®cant correlations between violence and the
age of staff, their gender, smoking habits, coffee consump-
tion at work, and their use of alcohol to relax after work.
These factors explained 17% of the variance amongst staff
who reported being victims of violence and 13% of the
variance among those who had been threatened, although
Whittington & Wykes (1994) found the only signi®cant
differences between staff who had been assaulted and those
who had not were age and grade. They also found that staff
who had been assaulted more than once were usually
assaulted by the same patient, indicating problematic
relationships rather than `dif®cult' patients as being an
important factor. Community psychiatric nurses have been
found to be more likely to encounter violent situations than
other nurses (Morning 1994) and Love & Hunt (1996)
concluded that male mental health nurses with managerial
responsibilities were particularly at risk.
Prevention
Managing violence has become a priority for mental health
nurses, although very little attention has been given to a
critical analysis of methods and outcomes. Hansen (1996)
proposed that by identifying hazards and other environ-
mental factors, attacks on and injuries to staff could be
reduced or eliminated. An occupational health perspec-
tive underscores the need for proactive monitoring and
heightens incentives for prevention through the introduc-
tion of external regulation (Love & Hunter 1996). It has
been claimed that training staff in skills to cope with
violence can signi®cantly reduce the incidence of injury
(Infantino & Musingo 1985).
However, it has also been shown that nurses who had
attended a course in managing violence were twice as
likely to be assaulted as those who had not (Fischer 1988).
Attempting to explain this phenomenon, Whittington
et al. (1996) observed that staff who had attended training
sessions on managing violence were more likely to
precipitate violence than non-attendees. Merely focusing
on the techniques of restraint and control in such courses
is insuf®cient. Instead, emphasizing the importance of
therapeutic relationships, client-centredness, negotiation
and collaboration should be central in training sessions
(Harris & Morrison 1995).
DEFINITION OF VIOLENCE
Berkowitz (1989) pointed out that `violence' is a term used
to refer to a variety of different actions, while Buss (1961)
stated that the term subsumed a large number of responses
that varied in topography, energy expenditure and conse-
quences. The operational de®nition of violence accepted
within the context of this study was: `displaying aggres-
sive behaviour, including spitting, scratching, deploying
physical force, or using an object as a weapon, either to
threaten or physically assault'.
AIMS OF THE STUDY
This study aimed:
1 To ascertain the extent and nature of violence against
mental health employees.
2 To identify the support received by staff following
exposure to violence.
P. Nolan et al.
936 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941

METHOD
Setting and subjects
Between November 1996 and March 1997, all quali®ed
and trainee psychiatrists and ®rst level mental health
nurses currently working with mental health clients
from ®ve National Health Service Trusts in the West
Midlands region of England were sent a postal ques-
tionnaire. The sample was drawn from the staf®ng lists
held by the Personnel and Human Resource Managers of
the Trusts. Overall, 47% of mental health employees
returned the questionnaire. The response rate for
psychiatrists was 60% (n� 74) and for nurses, 45%
(n� 301) (Table 1).
The questionnaire
The questionnaire contained 20 items which sought to
elicit the number, type and severity of violent incidents or
threats of violence against staff, and whether support was
offered after such incidents. Items in the questionnaire
had previously been validated by Arnetz et al. (1996).
Procedure
Psychiatrists, trainee psychiatrists and ®rst level mental
health nurses were sent a questionnaire and covering
letter to their workplace via their Personnel or Human
Resource Manager. The letter stated that subjects'
responses would be completely con®dential and that the
West Midlands Trusts would receive a report summariz-
ing the main ®ndings of the study. Stamped addressed
envelopes were enclosed for return of the questionnaire to
the researchers. A reminder was sent to all subjects 4
weeks after the initial mailing of the questionnaire, again
through their Personnel Managers.
Ethical permission was sought at the beginning of the
study from senior managers in the Trusts. Assurances
were given that once the data had been analysed, the
questionnaires would be destroyed. The researchers had
no direct contact with the respondents and were unknown
to them prior to and during the study.
Statistical analyses
The data were stored on the SPSS for Windows program
(version 6á1) and analysed using Pearson's chi-square
statistical test (v2). This is a test frequently used when
examining whether there is a difference between the
responses of two independent groups of respondents, in
this case nurses and psychiatrists, when those responses
are in a categorical form (i.e. yes/no or male/female). All
tests were two-tailed and statistical signi®cance was
assumed at P < 0á05.
RESULTS
Characteristics of the victims of violence
Signi®cant differences were found between employees
who had been victims of violence (or threats of violence)
at work during the course of the last year and those who
had not. Three-quarters of victims were aged 39 years or
under compared to half of non-victims (v2(d.f. 4)� 13á6,
P < 0á01). Most employees in the sample had worked in
mental health care for over 10 years. Yet, a signi®cantly
higher proportion of victims (21%) had only between 6
and 10 years experience compared to non-victims (12%)
(v2(3)� 8á4, P < 0á05). Ten per-cent of victims reported
being satis®ed with their work compared to 21% of
non-victims (v2(3)� 11á3, P < 0á05). Furthermore, 70% of
victims felt they had little control over their work
compared with 55% of non-victims (v2(3)� 14á9,
P < 0á01).
Victims of violence received information regarding their
duties more regularly than non-victims; 8% of victims
said the information was unclear compared to 18% of
non-victims (v2(4)� 11á6, P < 0á05). Victims (25%) had
more feedback from their line manager when they had
done a poor job compared to non-victims (10%; v2(4)�18á6, P < 0á001).
Exposure to violence
Table 2 shows how exposure to violence or the threat of
violence had been experienced by a higher percentage of
senior psychiatric registrars and hospital-based mental
health nurses than other groups working in mental health
care. However, due to the low number of senior psychi-
atric registrars, signi®cance testing was not applied.
Figure 1 shows that just over half of the psychiatrists
reported that they had been exposed to violence during
Table 1 Number of respondents from each professional group
Professional category
Number of
employees
replying
Percentage
of ®nal
sample
Consultant psychiatrists 46 12
Senior psychiatric
registrars
4 1
Trainee psychiatrists 24 6
Community psychiatric
nurses
95 26
Hospital-based nurses 201 54
Unknown category 5 1
Total 375 100
Experience throughout the nursing career Violence in mental health care
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941 937

the course of the last year compared to three-quarters of
the nurses.
Nurses were signi®cantly more likely to have been
exposed to violence either `several times' or `very often'
(v2(4)� 21á0, P < 0á001). This pattern was also found for
exposure to violence throughout subjects' careers,
whereby nurses had been exposed to violence signi®cant-
ly more often than psychiatrists (v2(3)� 21á7, P < 0á05).
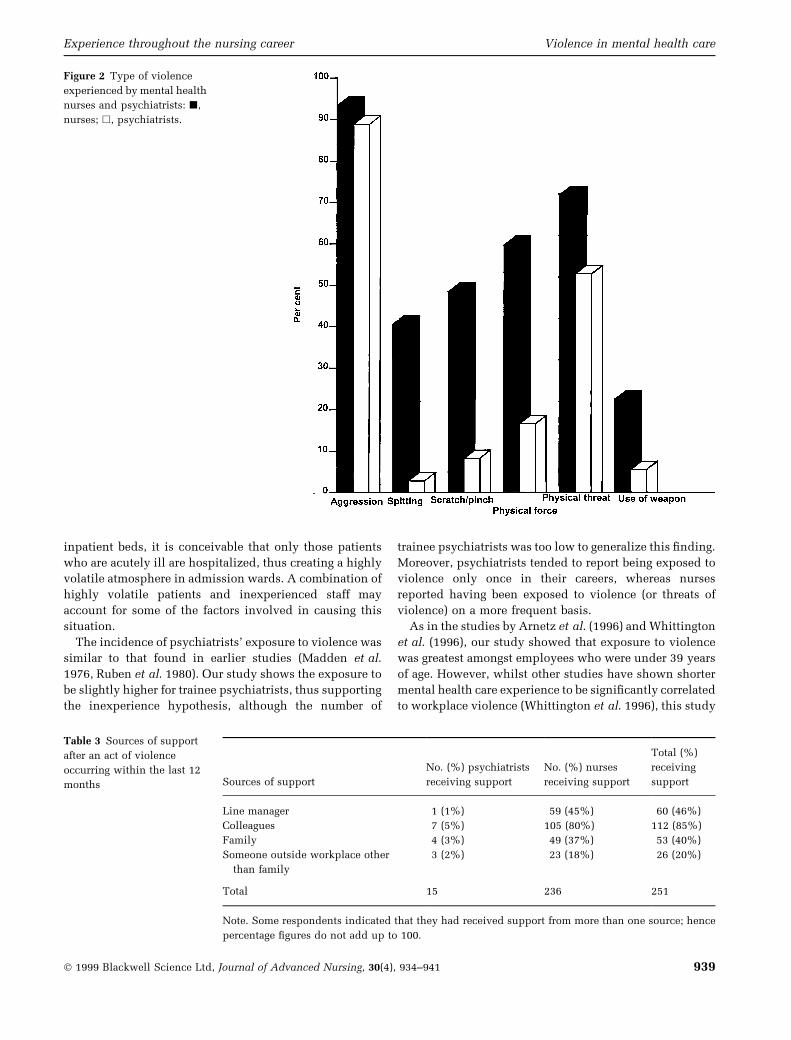
Figure 2 shows how nurses were signi®cantly more
likely to have been spat at (v2(1)� 19á5, P < 0á001),
scratched or pinched (v2(1)� 20á4, P < 0á001), slapped,
punched or kicked (v2(1)� 22á9, P < 0á001), physically
threatened (v2(1)� 5á3, P < 0á05), or hit by a weapon than
psychiatrists (v2(1)� 5á6, P < 0á05).
Perpetrators of violence
Respondents who had been victims of violence during the
last year were asked to identify their aggressor as `patient',
`patient's family', `colleagues' or `other'. Ninety-six per
cent of nurses and 95% of psychiatrists said their patients
had been aggressive towards them. A signi®cantly higher
proportion of psychiatrists (33%) than nurses (19%)
reported aggression from patients' relatives (v2(1)� 4á0,
P < 0á05). A higher proportion of psychiatrists (11%)
than nurses (6%) reported enduring aggressive behaviour
from their colleagues, although this difference was not
signi®cant.
Severity of violent act
Eighty-six per cent of psychiatrists compared to 50% of
nurses said that they had sustained no injuries as a result
of violence against them. Forty-four per cent of nurses
sustained minor injuries, whilst 6% reported serious
injuries compared to 11% of psychiatrists who sustained
minor injuries and 3% of psychiatrists who sustained
major injuries (v2 (2)� 16á8, P < 0á01).
Sources of support after exposure to violence
Half the nurses and 27% of psychiatrists who had been
the victims of violence during the course of the last year
received support after the incident. Thirty-two per cent
of psychiatrists felt no need for support compared to
17% of nurses (v2 (2)� 8á6, P < 0á05). Table 3 shows that
colleagues were the main source of support for both
groups.
DISCUSSION
The study shows how the frequency of violent incidents
involving mental health employees varies between these
professional groups. Indeed, even within our sample of
nurses, there was a large variation in the exposure to
violence (or threat of violence). A far greater proportion of
hospital-based nurses reported an incidence of violence
within the last 12 months compared with their commu-
nity-based counterparts. Hence exposure to violence (or
threat of violence) against hospital-based nurses in our
study was found to be higher than in previous studies,
such as Poster (1996) and Whittington & Wykes (1994).
Exposure to violence for community-based nurses was
found to be much less, although not as low as that
reported by Arnetz et al. (1996). With the reduction of
Table 2 Number and percentage of subjects exposed to violence
(or threat of violence) during their career by profession
Professional
category
Number of subjects
experiencing violence
% of category
sample
Consultant psychiatrist 20 44
Senior psychiatric
registrar
4 100
Trainee psychiatrist 11 50
Hospital-based mental
health nurse
163 81
Community-based
mental health nurse
47 50
Missing data 7
Figure 1 Act of violence or threat of violence against mental
health nurses and psychiatrists during the course of the last year:
j, nurses; h, psychiatrists.
P. Nolan et al.
938 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941
inpatient beds, it is conceivable that only those patients
who are acutely ill are hospitalized, thus creating a highly
volatile atmosphere in admission wards. A combination of
highly volatile patients and inexperienced staff may
account for some of the factors involved in causing this
situation.
The incidence of psychiatrists' exposure to violence was
similar to that found in earlier studies (Madden et al.
1976, Ruben et al. 1980). Our study shows the exposure to
be slightly higher for trainee psychiatrists, thus supporting
the inexperience hypothesis, although the number of
trainee psychiatrists was too low to generalize this ®nding.
Moreover, psychiatrists tended to report being exposed to
violence only once in their careers, whereas nurses
reported having been exposed to violence (or threats of
violence) on a more frequent basis.
As in the studies by Arnetz et al. (1996) and Whittington
et al. (1996), our study showed that exposure to violence
was greatest amongst employees who were under 39 years
of age. However, whilst other studies have shown shorter
mental health care experience to be signi®cantly correlated
to workplace violence (Whittington et al. 1996), this study
Figure 2 Type of violence
experienced by mental health
nurses and psychiatrists: j,
nurses; h, psychiatrists.
Table 3 Sources of support
after an act of violence
occurring within the last 12
months Sources of support
No. (%) psychiatrists
receiving support
No. (%) nurses
receiving support
Total (%)
receiving
support
Line manager 1 (1%) 59 (45%) 60 (46%)
Colleagues 7 (5%) 105 (80%) 112 (85%)
Family 4 (3%) 49 (37%) 53 (40%)
Someone outside workplace other
than family
3 (2%) 23 (18%) 26 (20%)
Total 15 236 251
Note. Some respondents indicated that they had received support from more than one source; hence
percentage ®gures do not add up to 100.
Experience throughout the nursing career Violence in mental health care
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941 939

found that the highest association was for those who had
worked between 6 and 10 years in mental health care.
Job dissatisfaction was also found to be signi®cantly
correlated to workplace violence, again supporting earlier
research (Whittington et al. 1996). Brailsford & Stevenson
(1973) concluded that under-involvement and poor
communication between staff and patients were signi®-
cantly associated with assault and our study found that
employees who perceived they had less control over their
working situation were also more likely to be victims of
violence. Yet, in this study it was found that those who
had received most information regarding what was
expected of them were more likely to be victims. The
nature of this information was often described by victims
as `negative feedback' on their work performance. This
®nding suggests that it is the speci®c nature of the
communication between line managers and staff rather
than lack of communication that appears to be linked to
incidents of violence. It is unclear whether an incident of
violence causes communication with managers to be
perceived negatively by the victims, or whether an initial
lack of clear and positive guidance predisposes employees
to potentially threatening situations. Our research tends to
indicate the latter.
Most violent attacks against both nurses and psychia-
trists were carried out by their patients. Nurses appear to
be particularly vulnerable. This may simply re¯ect the fact
that nurses spend more time with patients than other
professional groups working in mental health care and are
often involved with them in a more intimate, interactive
manner, especially in acute phases of their illness. There
are therefore more opportunities for patients to vent their
aggression on nurses and, equally, the nature of the
nurse±patient relationship may provide more triggers for
aggressive behaviour.
Psychiatrists in this study reported less exposure to
violent incidents than nurses. This may be due to the
distance they maintain from patients and the tendency
for junior staff to be more intimately involved in care
provision. Yet, psychiatrists are more vulnerable to
aggressive incidents initiated by relatives of patients
and this may re¯ect the fact that relatives see the
consultant as the person with overall responsibility for
the welfare of the patient. Further research into violence
perpetrated by patients' relatives and friends would be
instructive.
CONCLUSIONS
This study makes clear that violence in the workplace is
still a key issue for mental health professionals and merits
the continued attention of researchers, educators and
managers in order to identify the causes of violent inci-
dents, minimize the risk of them occurring and protect both
staff and patients from injury and criminal proceedings.
It is recommended that training to deal with violence in
the workplace be speci®cally targeted at members of staff
who are most likely to be at risk of threats of violence and
actual physical aggression. In our study these were
young, hospital-based nurses with less than 10 years
experience. However, as other studies have shown
community rather than hospital-based nurses as being
more `at risk', we recommend that each employing
authority or Trust identify those most `at risk' within
their own district.
Our study also shows that training should include
management of aggression from patients' relatives and
from fellow colleagues; training should not simply focus
on violent patients but should consider violent and
aggressive acts in general. It is important to note that the
provision of training may be accompanied by an increase
in reported incidences of violence in the workplace, as
seen in the studies by Fischer (1988) and Whittington
et al. (1996). The reasons for this need closer attention
than they have hitherto received.
Training will doubtless prove insuf®cient unless the
underlying causes which make certain members of staff
vulnerable to aggression at the hands of their patients are
explored. The maintenance of high morale in the team,
coupled with the promotion of individuals' self-esteem,
play a signi®cant part in protecting staff from violence and
are linked to effective communication between junior and
senior members of staff. Feedback should not solely focus
on shortcomings in the person's work, but should also
identify, acknowledge and build on the individual's
strengths.
Finally, whilst not every individual who has experi-
enced a violent incident would wish to receive support
from managers or colleagues, this option should be
available for those who seek it and those who may have
no outside sources to which they can turn. Having good
quality support available can be perceived by staff as a
hallmark of the regard the organization has for them.
Moreover, this study showed that support was needed
even when the violent incident did not involve actual
bodily harm. Most psychiatrists felt they needed support
after exposure to threatening as well as aggressive
behaviour. The criteria for eligibility for support should
therefore be broad enough to encompass staff exposed to
non-physical forms of violence.
The 47% response rate from the sampling frame limits
the generalizability of the study. As there were only four
senior psychiatric registrars in the sample, comparisons
between speci®c clinical health professionals could not be
made reliably. It should also be noted that the study was
con®ned to a particular region, and its ®ndings may not be
relevant to other regions. Nonetheless, it is reasonable to
assume that the ®ndings and recommendations discussed
here have implications for other mental health workplace
settings.
P. Nolan et al.
940 Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941

References
Adler W., Kreeger C. & Ziegler P. (1983) Patient violence in a
private psychiatric warden. In Assaults Within Psychiatric
Facilities (Lion J. & Reid W. eds), Grune & Stratton, New York,
131±142.
Arnetz J., Arnetz B. & Petterson I. (1996) Violence in the nursing
profession: occupational and lifestyle risk factors in Swedish
nurses. Work and Stress 10(2), 119±127.
Berkowitz L. (1989) Frustration-aggression hypothesis. Examina-
tion and Reformulation Psychological Bulletin 106, 59±73.
Brailsford D. & Stevenson J. (1973) Factors related to violent and
unpredictable behaviour in psychiatric hospitals. Nursing
Times 18, 9±11.
Buss A.H. (1961) The Psychology of Aggression. John Wiley &
Sons, London.
Cahn T. (1995) Violence Ð an element of the psychiatric
profession. Schweizer Archives Fur Neurologie und Psychiatrie
146(3), 109±114.
Conn L. & Lion J. (1983) Assaults in a university hospital. In
Assaults Within Psychiatric Facilities (Lion J. & Reid W. eds),
Grune & Stratton, New York, pp. 61±69.
Depp F. (1983) Assaults in public mental hospitals. In Assaults
Within Psychiatric Facilities (Lion J. & Reid W. eds), Grune &
Stratton, New York, pp. 21±43.
Dublin W. & Lion J. (1992) Clinician Safety. Report of the APA
Task Force, Report 33. American Psychiatric Association,
Washington, District of Columbia.
Edwards J. & Reid W. (1983) Violence in psychiatric facilities in
Europe and the United States. In Assaults Within Psychiatric
Facilities (Lion J. & Reid W. eds), Grune & Stratton, New York,
pp. 131±142.
Evans R. (1991) It changed my life. Sunday Times, 23 June, p. 53.
Fischer N. (1988) The fear of assault. Bethlem Maudsley Gazette
35, 38±40.
General Nursing Council (1974) Syllabus of Subjects for Exami-
nation for the Certi®cate of Mental Nursing. GNC Publications,
London.
Glennister D. (1997) Coercion, control and mental health nursing.
In The Mental Health Nurse (Tilley S. ed.), Blackwell Science,
Oxford, pp. 43±57.3
Hansen B. (1996) Workplace violence in the hospital psychiatric
setting. An occupational health perspective. AAOHN Journal
44(12), 575±580.
Harris D. & Morrison E. (1995) Managing violence without
coercion. Archives of Psychiatric Nursing 9(4), 203±210.
Health and Safety Commission (1987) Violence to Staff in the
Health Service. Her Majesty's Stationery Of®ce, London.
Hodgkinson P., McIvor L. & Phillips M. (1985) Patient assaults on
staff in a psychiatric hospital: a two-year retrospective study.
Medicine, Science and Law 25, 288±294.
Infantino J. & Musingo S. (1985) Assaults and injuries among staff
with and without training in aggression control techniques.
Hospital Community Psychiatry 36(12), 1312±1314.
James D., Fineberg N., Shah A. & Priest R. (1990) Increase in
violence on an acute psychiatric ward: a study of associated
factors. British Journal of Psychiatry 156, 846±852.
Love C. & Hunter M. (1996) Violence in public sector psychiatric
hospitals. Benchmarking nursing staff injury rates. Journal of
Psychosocial Nursing and Mental Health Services 34(5), 30±34.
Madden D., Lion J. & Penna M. (1976) Assault on psychiatrists by
patients. American Journal of Psychiatry 133, 422±425.
Martin J.P. (1984) Hospitals in Trouble. Basil Blackwell, Oxford.
Mason P. (1991) Violent trends. Nursing Times 87(21), 16±17.
Morning D. (1994) Mental health. Coping with violence: work-
shops for CPNs. Nursing Standard 8(23), 2±8.
Pearson M., Wilmot E. & Padi M. (1986) A study of violent
behaviour among inpatients in a psychiatric hospital. British
Journal of Psychiatry 149, 232±235.
Poster E.C. (1996) A multinational study of psychiatric nursing
staff's beliefs and concerns about work safety and patient
assault. Archives of Psychiatric Nursing 10(6), 365±373.
Ruben I., Wolkon G. & Yamamoto J. (1980) Physical attacks on
psychiatric residents by patients. Journal of Nervous Mental
Disorders 168, 243±245.
Scull A.T. (1979) Museums of Madness. Penguin Books, London.
Shah A., Fineberg D. & James D. (1991) Violence among psychi-
atric inpatients. Acta Psychiatrica Scandinavica 84, 305±309.
Weiser M., Levkowitch Y., Shalom S. & Neuman M. (1994)
Emotional reactions of psychiatric staff to violent patients.
Harefuah 126(11), 642±645, 691.
Wessely S. & Taylor P.J. (1991) Madness and crime: criminology
versus psychiatry. Criminal Behaviour and Mental Health
1, 193±228.
Whittington R. & Wykes T. (1994) Violence in psychiatric
hospitals: are certain staff prone to being assaulted? Journal of
Advanced Nursing 19, 219±225.
Whittington R., Shuttleworth S. & Hill L. (1996) Violence to staff
in a general hospital setting. Journal of Advanced Nursing
24(2), 326±333.
Yates J. (1981) Staff±patient ratios and hospital enquiries. Nursing
Times 26, 2143±2145.
Experience throughout the nursing career Violence in mental health care
Ó 1999 Blackwell Science Ltd, Journal of Advanced Nursing, 30(4), 934±941 941





























