Embed Size (px)
Citation preview

CASE REPORTS
Viscoelastic displacement of fibrous ingrowth: a new surgical approach to retrocorneal membranes
Mark Mandelcom, MD, eM, FRCSC; Garnze Men, MD
R etrocorneal membrane fo.~atio? following anterior segment surgery or Injury IS the most com
mon presenting sign of epithelial downgrowth 1 but may also be due to fibrous ingrowth.2 In cases of epithelial downgrowth, invading epithelial cells proliferate on the iris, ciliary body, trabecular meshwork, vitreous, retina and, most frequently, back of the cornea, causing corneal decompensation, glaucoma, progressive anterior synechiae, intraocular inflammation, vitreous traction, retinal detachment, phthisis and, eventually, blindness. I,3 In contrast, fibrous ingrowth remains confined to the cornea and anterior chamber angle and causes visual loss most often by creating an opacity in the visual axis or, more infrequently, by damage due to glaucoma.4,5
After surgical or accidental injury, fibroplasia takes place as a necessary part of the reparative process. Several factors, such as prolonged inflammation, poor wound apposition and damaged corneal endothelium, may lead to uncontrolled fibroplasia.6- 8
Fibroblasts in fibrous ingrowth may originate from subepithelial connective tissue or corneal stromal fibroblasts, posterior keratocytes, metaplastic corneal endothelium and blood mononuclear cells. &-8
There is no specific treatment for fibrous ingrowth other than management of complicating sequelae. Unlike the treatment of epithelial downgrowth, it may not be necessary to eradicate all fibroblastic tissue.9
From the Department of Ophthalmology, Toronto Western Hospital, University Health Network, University of Toronto. Toronto, Ont.
Originally received Jan. 15, 2001 Accepted for publication May 25, 2001
Reprint requests to: Dr. Mark Mandelcorn, Department of Ophthalmology, Toronto Western Hospital, Suite EC 6-028, 399 Bathurst St., Toronto ON M5T 2S8
Can J Ophthalmo/2001;36:34l-3
Retrocorneal membrane surgery-Mandelcom et al
We describe a new and relatively atraumatic surgical technique for correcting fibrous ingrowth obstructing the visual axis.
CASE REPORT
A 72-year-old black woman with non-insulindependent diabetes mellitus presented with a 6-month history of visual loss following left extracapsular cataract extraction with posterior chamber implant. Her medications were glyburide (20 mg/d) and enalapril maleate (20 mg twice a day).
The visual acuity in the patient's left eye was counting fingers at I m. There was a healed conjunctival incision from a fornix-based flap. The back of the cornea was covered by a grey, fibrous retrocorneal membrane that extended vertically to just below the visual axis and horizontally from the cataract wound limits between 10 0' clock and 2 o'clock, leaving a 2-mm sector of clear cornea on the temporal and nasal sides of the membrane. The anterior chamber was deep and clear. A posterior chamber implant was in the ciliary sulcus. The iris looked normal, with no rubeosis and no pupillary distortion. There was no red reflex.
Careful gonioscopy to rule out extension of the retrocorneal membrane onto the iris or over the anterior chamber angle showed no smoothing out of iris architecture, no anterior iris or anterior chamber angle membrane, and no rubeosis iridis. No fistulous tract could be found at the cataract incision.
The intraocular pressure was 18 mm Hg bilaterally. Ultrasonography of the posterior segment showed
vitreous hemorrhage with attached retina. A three-port pars plana vitrectomy procedure was set
up, but visibility was so poor through the retrocomeal membrane that the membrane had to be dealt with. A paracentesis incision was made at the limbus at 3 o'clock, and a 27 -gauge cannula attached to a syringe containing viscoelastic (Viscoat, Alcon Canada Inc., Mississauga, ant.) was advanced through the paracentesis incision
341

Retrocorneal membrane surgery-Mande1corn et al
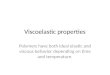
Fig. I-Slit-Iamp photograph 6 weeks after surgery, showing a clear cornea centrally and a scrolled retrocorneal membrane in the superior anterior chamber angle.
into the anterior chamber until the cannula engaged the temporal edge of the retrocorneal membrane. The cannula was moved slowly back and forth against the edge of the membrane until the edge was disengaged from the back of the cornea. A small amount of viscoelastic was then injected until the edge of the membrane was displaced posteriorly away from the cornea. The cannula was then advanced farther into the pocket thus created, and more viscoelastic was injected. The cannula was directed inferiorly so that viscoelastic could first dissect the membrane away from its inferiormost attachment to the cornea just below the visual axis. In this way, the membrane was forced to curl posteriorly as it was progressively stripped from its inferiormost to its superiormost attachment to the cornea. A scroll of retrocorneal membrane was left curled up in the superior portion of the anterior chamber angle. This created a residual opacity of the cornea of 1.5 mm just below the healed cataract incision.
Visibility was now adequate for pars plana vitrectomy to be performed. Retained vitreous blood was removed; areas of neovascularization of the retina were then segmented and delaminated, and laser endophotocoagulation was administered.
The visual acuity 6 weeks postoperatively was 20/200. The corneal opacity caused by the scrolled retrocorneal membrane measured 1 mm at the limbus (Fig. 1). The rest of the cornea was clear, as was the vitreous cavity. The retina exhibited panretinal photocoagulation scars and diabetic macular edema.
COMMENTS
Histopathological studies of specimens from a
342 CAN J OPHTHALMOL-VOL. 36, NO.6, 2001
patient with fibrous downgrowth suggested that the membrane originated from the corneal stroma at the cataract wound margin, where Descemet's membrane and endothelial cells were missing. lO Cockerham and Hidayat2 showed that there is a direct connection between the retrocorneal membrane and the cataract wound through a gap in Descemet's membrane. Histopathological examination in cases of retrocorneal membrane showed no invasion of corneal stroma by either epithelial or fibrous tissue cells outside the wound margin. 10-12 In an immunohistochemical and ultrastructural study, contractile myofibroblasts were observed in some of the 11 retrocorneal membranes studied.2
These findings suggested that, since in general there is no invasion of the cornea by the retrocorneal membrane but, rather, growth of membrane onto the surface of corneal endothelium, it might be possible to surgically create a plane of dissection between the membrane and corneal endothelium so as to disengage the membrane from the endothelium and redirect its growth as a scroll back to the cataract wound. In addition, successful viscoelastic dissection to separate a posterior capsular scar from an off-axis, subluxated intraocular lens implantl3 suggested that a similar technique might work in our case of retrocorneal membrane.
REFERENCES
1. Weiner MJ, Trentacoste J, Pon DM, Albert DM. Epithelial downgrowth: a 30 year clinicopathological review. Br J OphthalmoI1989;73:6-11.
2. Cockerham GC, Hidayat AA. Retrocorneal membrane with myofibroblasts after perforating injury: an immunohistochemical and ultrastructural study of II cases. Cornea 1999;18:700-6.
3. Shields CL, Brucker AJ. Epithelial downgrowth following the removal of iris inclusion cysts. Ophthalmic Surg 1991; 22:330--5.
4. Sherrard ES, Rycroft PV. Retrocorneal membranes: I. Their origin and structure. Br J Ophthalmol 1967;51: 379-86.
5. Sherrard ES, Rycroft PV. Retrocorneal membranes: II. Factors influencing their growth. Br J Ophthalmol 1967; 51:387-93.
6. Swan KC. Fibroblastic ingrowth following cataract extraction. Arch OphthalmoI1973;89:445-9.
7. Chiou AGY, Chang C, Kaufman SC, Ohta T, Maitchouk D, Beuerman RW, et al. Characterization of fibrous retrocorneal membrane by confocal microscopy. Cornea 1998; 17:669-71.
8. Baum J. The origin of retrocorneal membranes. Cornea 2000; 19: 124.
9. Lytle RA, Simmons RJ. Epithelial and fibrous proliferation. In: Albert DM, Jakobiec FA, editors. Principles and

practice of ophthalmology: clinical practice. Philadelphia: W.B. Saunders Company; 1994. p. 1483.
10. Kremer I, Zandbank J, Barash D, Ben-David E, Yassur Y. Extensive fibrous downgrowth after traumatic corneoscleral wound dehiscence. Ann OphthalmoI199l;23:465-8.
11. Knauf HP, Rowsey n, Margo CEo Cystic epithelial downgrowth following clear corneal cataract extraction. Arch OphthalmoI1997;115:668-9.
12. Holliday IN, Buller CR, Bourne WM. Specular micros-
Retrocorneal membrane surgery-Mande1com et al
copy and fluorophotometry in the diagnosis of epithelial down growth after a sutureless cataract operation. Am J OphthalmoI1993;116:238-40.
13. Mandelcorn M. Viscoelastic dissection for relocation of off-axis intraocular lens implant: a new technique. Can J OphthalmoI1990;30:34-5.
Key words: retrocorneal membrane, epithelial downgrowth, fibrous ingrowth, viscoelastic dissection
CAN J OPHTHALMOL-VOL. 36, NO.6, 2001 343