Embed Size (px)
Citation preview

Visual Diagnosis
Joseph A Zenel, MDOregon Health & Science University
October 2005

7-year, 8-month-old male with complaints...
Mother brings the
“Note”

Problem List
• 10/13/89 Age 6 yrs, Sinusitis/pharyngitis
• 12/20/89 Acute left otitis media
• 1/29/91 Pharyngitis (TC negative)

Further History• 5/7/90 Age 6 yr, 8 mos – Leg pains/ drinking a lot
– Ht 49.25 in (90%) –Wt 46 lb (50%)
– PE normal, BP 80/60– Vision 20/40 R, 20/50 L
– Urine dipstick normal• SG 1.015, pH 5.0

Further History
• 12/4/90 Age 7 yr, 4 mos– Sharp, intermittent chest pain for 3 weeks– Stomach ache 1X/wk– Active in basketball
– PE: tenderness over sternum
– DX: Chostochondritis– RX: Ibuprofen

Further History
• 1/2/91 One month later– Still complains of chest pain– Appetite poor
– PE: normal• Heme test stool negative X4
– DX: GE Reflux?– RX: Antacid

Further History
• 1/29/91 3 weeks later– Low grade fever– Sore throat
– PE: Pharynx injected– TC negative
– DX: Pharyngitis

Today• Congested– Gasping during sleep
• Stomach ache/ poor appetite• Vomits 3 X every morning• Occasional headaches for 2 weeks• Lower right backache • Constipated– Dark, hard stools
• Thirsty

Vital Signs
• T 97.5° F
• P 88
• R 24
• BP 90/62
• HT 49.25 in (45%)• WT 45 lb (5%)

Physical Exam
• Poor posture
• Generalized weakness
• DTR’s 1+
• Otherwise normal

Key Features• Poor appetite• Vomiting• Thirst• Constipation• Stomach ache• Backache • Poor Ht, Wt gain• DTRs 1+, weakness

Anorexia
• Stress• Reflux esophagitis• Infection• Depression• Constipation• Drugs• Malignancy• Iron deficiency
• Hypothyroidism• Hypercalcemia• Diabetes insipidus• Lead poisoning• Inflammatory
bowel disease• Other

Vomiting• GE reflux• Gastroenteritis• Appendicitis• Intestinal
obstruction• Peptic ulcer• Systemic infection• Pancreatitis• Pyelonephritis
• CNS infection, tumor• Migraine• Electrolyte, Mg, Ca
abnormalities• DKA• Congenital adrenal
hyperplasia• Cough• Drugs/ingestion• Amino, organic
acidurias

Polydipsia?
• Psychogenic polydipsia• Diabetes mellitus• Diabetes insipidus• Hypercalcemia• Hypokalemia• Renal tubular acidosis• Neuroblastoma

Constipation: Common
• Chronic idiopathic
• Dietary causes
• Painful defecation

Constipation: Other• Hirschsprung Disease• Meconium ileus equivalent• Spinal dysraphism• Lead poisoning• Hypokalemia• Hyper- and hypocalcemia• Muscular weakness• Hypothyroidism • Diabetes mellitus

Myalgia• Trauma
• Febrile infection
• Myositis • Myoglobinopathies• Dermatomyositis• Systemic lupus erythematosis• Fibromyalgia
• Hyponatremia• Hypercalcemia

Growth Chart
• If ↓Ht ≥ ↓ Wt:– Suspect endocrine etiology
• If ↓Wt > ↓ Ht:– Suspect poor calorie intake– Suspect ↑calories
expenditure– Suspect ↑calorie elimination

Growth Chart
• If ↓Ht ≥ ↓ Wt:– Suspect endocrine etiology
• If ↓Wt > ↓ Ht:– Suspect poor calorie intake– Suspect ↑calories
expenditure– Suspect ↑calorie elimination

Decreased Reflexes, Weakness
• Myopathy
• Neuropathy– Guillain-Barre Syndrome
• Hypothyroidism
• Hypokalemia• Hypercalcemia

Laboratory
• Uric Acid 6.6 (2.2-7.7 mg/dL)
• Calcium 15 (8.5-10.8 mg/dL)• Phosphorus 2.7 (3.8-5.4 mg/dL)
• Total protein 7.0 (6.0-8.5 g/dL)• Albumin 4.1 (3.0-5.5 g/dL)
• AST, ALT normal

Laboratory• UA– Sp grav 1.012– pH 5.0– Ketones trace– Glucose neg– 0 rbc– 4-6 wbc– Nitrites neg– Bact neg– Calcium oxalate crystals, occasional

Hypercalcemia• Listlessness• Irritability • Depression
• Headache • Weakness
• Anorexia• Constipation • Vomiting• Polydipsia, polyuria• Weight loss

Hypercalcemia• Pancreatitis• Gastritis, peptic ulcer
• Renal stones• Renal failure• Nephrogenic DI
• Bone pain
• Bradycardia• Hypertension
• Gait disturbance• Hyporeflexia• Proximal muscle weakness

Hypercalcemia: Neonatal
• Neonatal primary hyperparathyroidism
• Secondary hyperparathyroidism– Maternal hypocalcemia
• Familial hypocalciuric hypercalcemia
• Autosomal recessive hypophosphatasia
• Idiopathic infantile hypercalcemia

Hypercalcemia: Neonatal
• Excessive calcium supplementation
• Subcutaneous fat necrosis
• Williams syndrome– Transient hypercalcemia– Elfin facies– Mental retardation– Supravalvular aortic stenosis– Deletion chromosome 7

Hypercalcemia: School-aged Children
• Hyperparathyroidism– Parathyroid adenoma
• Autosomal dominant hereditary hyperparathyroidism
• Multiple endocrine neoplasia (MEN) type I• Hyperparathyroidism• Pancreatic tumor• Pituitary tumors

Hypercalcemia: Malignancy
• Lymphoma– Hodgkin, non-Hodgkin
• Ewing sarcoma• Neuroblastoma• Langerhans cell histiocytosis• Rhabdomyosarcoma• Ovarian small cell carcinoma• Renal tumors

Hypercalcemia: Other
• Thyrotoxicosis• Adrenal insufficiency• Granulomatous disease
• Drugs– TPN– Vitamin D intoxication– Vitamin A – Thiazide– Lithium– Theophylline

Hypercalcemia: Normal PTH
• Williams syndrome• Subcutaneous fat necrosis• Familial hypocalciuric hypercalcemia• Vitamin A/ Vitamin D excess• Hyperthyroidism• Malignancy• Granulomatous disease• Adrenal insufficiency

Hypercalcemia: PTH Excess
• Primary hyperthyroidism– Adenoma– Familial – Ectopic
• Secondary hyperparathyroidism– Maternal hypoparathyroidism– Renal osteodystrophy

Hypercalcemia: Workup
• History, family history• Physical examination
• Calcium, ionized calcium, phosphorus• PTH levels• Alkaline phosphatase• Urine: calcium, phosphorus, calcium/creatinine ratio• Vitamin D levels
• Imaging– X-ray– Neck, renal ultrasound, CT, MRI– Nuclear scan

Hypercalcemia: Treatment
• Hydration– Increase urinary calcium output
• Loop diuretic– Inhibit tubular reabsorption
• Calcitonin– Inhibit renal readsorption, bone resorption
• Biphosphonates– Block bone resorption

Hypercalcemia: Surgery
• Primary hyperthyroidism
• Recurrent renal stones
• Persistent calcium levels > 12.5 mg/dL

Parathyroid Adenoma
• Rare in children– Prolonged parathyroid hyperplasia– Genetic abnormality
• 80-85% primary hyperparathyoidism
• ↑PTH, hypercalcemia, hypophosphatemia, acidosis, ↑ urine calcium, ↑ urine phosphorus
• Surgery– Cure rate 95-98%

10-year-old male with acute abdominal pain

McBurney Point
• Point 1.5 - 2 inches on straight line from anterior superior iliac spine to umbilicus
• Appendix location

McBurney Sign
• Rebound tenderness and sharp pain when McBurney point is palpated
• Appendicitis

Blumberg Sign
• Rebound tenderness
• Peritoneal irritation• Appendicitis

Psoas Sign
• Pain with right leg hyperextension– Inflammation over psoas muscle
• Appendicitis• Pelvic abscess

Obturator Test
• Pain with right hip flexion, internal rotation–Pain in hypogastric area
• Ruptured appendix• Pelvic abscess

Rovsig Sign
• RLQ pain worse with LLQ palpation, percussion
• Peritoneal irritation• Appendicitis

Aaron Sign
• Pain, distress in area of patient’s heart, stomach – During palpation of
McBurney point
• Appendicitis


Hilton, Practical Pediatric Radiology

Abdominal CT Scan

Clues to Real Abdominal Pain
• Hand points to pain:
– The farther from umbilicus, the more likely pain is organic in origin
Apley Rule

Clues to Real Abdominal Pain
“Touch me not!”
• Eyes closed during examination

4-yr-old male with 12 hours acute abdominal pain &
vomiting

Pertinent Findings
• Bilious vomiting
Open eyes!
“Go ahead and touch!”

Pertinent Findings
• Dry mouth, sunken eyes
• Apley rule– Pain away from umbilicus
• RUQ pain

Pertinent Findings
• No rebound tenderness
• ? Right CVA tenderness

DDX: Bilious Vomiting
• Intestinal obstruction– Anatomical• Malrotation with volvulus• Duodenal stenosis• Annular pancreas• Mass • Other
– Functional ileus• Infection• Drug

Malrotation
• Malposition
• Right-sided duodenum
• Right-sided proximal jejunum

Malrotation
Normal

Malrotation1:6000 births
• Failure of normal rotation of embryonic intestine
– Cecum on left
– Small bowel on right
– Little or no fixation of bowel
– Duodenum frequently truncated and fused to colon

Malrotation
Volvulus
Normal

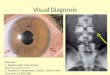
Brushfield Spots
• Speckled iris
• Elevated white spots on iris in a concentric ring with pupil– Iris connective tissue aggregates
• Associated with Down syndrome– Can be normal

Kayser-Fleischer Ring• Copper deposition on inner surface of
Descemet membrane – Outer margin of cornea
– Pathognomonic for Wilson disease

Tuberous Sclerosis
• Skin– Hypopigmented spots– Ash leaf (95% infants)– Adenoma sebaceum
(angiofibromas)– Shagreen patch
• Brain– 95% subependymal nodules,
parenchymal hamartomas
• Eyes– Retinal phakoma
• Other– Renal hamartoma– Heart rhabdomyoma

Aniridia •Wilms Tumor
• Aniridia
• Hemihypertrophy
• Cryptorchidism
• Hypospadias
• Mental retardation

Pupil Size
• Dilation– Neuroblastoma (catecholamines)– Atropine
• Constriction–Morphine

Leukokoria • Retinoblastoma
• Corneal opacity
• Congenital cataract
• Hyphema– Anterior chamber
fluid
• Retinal disease

Ectopia Lentis
• Displacement ormalposition of crystalline lens of eye
• Marfan syndrome– Most frequent cause
of heritable ectopia lentis
– Tall stature, arachnodactyly, joint laxity, mitral valve prolapse, aortic dilatation
eMedicine

Iritis, Uveitis • JRA
• Kawasaki disease
• Sarcoidosis
• Herpetic keratitis
• Corneal ulcer
• Trauma

Oculocutaneous Albinism
• Pigment absence, dilution– Hair, skin and eyes
• Common features– Strabismus– Photophobia– Decreased visual acuity– Absent binocular vision

Herpes Zoster
• Grouped vesicles on anerythematous base– Dermatome distribution– Does NOT cross midline
• Reactivation 1-3 dermatomes– Latent virus in dorsal root
ganglion
• Most common distribution T3-L2, facial (Trigeminal)

Impetigo
• Vesicles, bullae
• Multiple lesions generally at same site
• Different sizes
• Often coalesce
AAP

• Preseptal cellulitis– Erythema, edema
may extend over superior orbital rim onto brow
• Orbital cellulitis– Erythema, edema
does NOT extend over superior orbital rim onto brow• Orbital septum
prevents edema from extending over brow

Angioedema • Edema extending into deep dermis or subcutaneous tissue– Mast cell
degranulation, dilated venules, dermal edema
• Causes– Allergens– Insect venom– Infections– Blood products, IVIG

Neuroblastoma• Periorbital ecchymoses– Obstruction of palpebral vessels by tumor tissue
in & around orbits
• Clues:– Abdominal, mediastinal mass– HTN– Orbit displacement
• DDX:– Trauma, orbital fracture– Abuse

• Classic hemophilia– Hemarthroses– Deep muscle hematomas
• Trauma– Battered child– Bruises on multiple facial
planes
AAP

Kawasaki Disease
• Fever for 5 days
• 4/5 conditions:– Bilateral, non-exudate
conjunctivitis– Mucous membrane
changes– Edema, erythema
peripheral extremities – Polymorphous,
nonvesicular rash – Cervical
lymphadenopathy• Node > 1.5 cm
Limbic sparing

SJS• Serious systemic disorder– Fever, respiratory &/or GI
symptoms 10%-30% cases
• 2 mucous membranes and skin– Purulent conjunctivitis, uveitis– Skin rupture with denuded skin
• Skin lesions– Small blisters, purpuric
macules or atypical target lesions

4-month-old male with cough and “wheeze”

Past History• Full-term gestation, NSVD
• Apgars 5, 8– Limp, weak cry, blue extremities– Brief blow-by oxygen
• 15-year-old G1P0 mom – Good prenatal care
• Birth weight 3.8 kg

Age Day 12• Wt 3.9 kg
• T 36.8°C (98.2°F) HR 160 R 80
• Physical exam–Mild subcostal retractions– Clear breath sounds– No murmur, grunting, or flaring

3-weeks of age
• Wt 4.3 kg
• T 36.6°C (97.8°F) HR 140 R 96
• Physical exam– Pink, mild subcostal retractions– Clear breath sounds– No murmur, grunting, or flaring

Normal Respiratory Rates
• Newborn 30 - 80 bpm
• 1 year 20 - 40 bpm
• 3 year 20 - 30 bpm
• 6 years 16 - 22 bpm

Respiratory Effort
• Neonates primarily use diaphragm for respiratory effort
• Infants may also use abdominal musculature
• Intercostal muscle use by age 6-7 years

Tachypnea in Infant
• Fever• Cardiac insufficiency• Pain• Hypoxemia• Pulmonary disease• Anemia• Metabolic acidosis• CNS lesion

Age 2 months
• Wt 6.1 kg
• T 36.2°C (97.1°F) HR 148 R 60– No retractions– Clear breath sounds– No murmur
• “Occasional wheeze when cry”

Now at 4 months of age:
• Occasional cough, clear rhinorrhea
• Occasional audible wheeze

Vital Signs
• T 36.2°C – 97.1°F
• HR 120
• R 60
• Sat 98% (RA)
• Wt 8.1 kg, Ht 68 cm

Physical Exam
• No retractions
• Clear breath sounds, occasional expiratory wheeze
• No murmur

Stridor
• Inhalation accompanied by high-pitched sound
• Indicates high degree of laryngeal or tracheal obstruction
–Croup–Epiglottitis–Tracheitis–Foreign body–Laryngotracheal malacia, stenosis

Wheeze• Musical noise sounding like a squeak– Often heard continuously during inspiration
or expiration– Usually louder during expiration
• Whistling of air through narrowed airways– Asthma– Bronchiolitis– FB– Airway compression

DDX: Wheeze, Infants• Bronchiolitis• GE reflux• Asthma• Bronchopulmonary dysplasia• FB• Airway compression– Vascular ring/aberrant vessel
• Cystic fibrosis

DDX: Cough, Infants
• Asthma• GE reflux• Respiratory infection• Airway compression
• Vascular ring, aberrant vessel
• FB• Cystic fibrosis

CXR
• Opacification, right lower lobe– Superior and/or– Posterior
segments– Probable
volume loss

Diaphragmatic Hernia
• Left side – 90% cases
• Bowel gas pattern in chest
• Heart pushed into right side

Mediastinal Mass
• Smooth or sharply defined midline mass
• Displacing trachea

DDX: Opacification
• Pulmonary abscess
• Congenital lung anomaly– Bronchogenic cyst– Cystic adenomatoid malformation– Pulmonary sequestration

Pulmonary Sequestration
• 3 cm soft tissue mass– Azygoesophageal recess
• Atelectasis of RLL
• Hyperexpansion of RUL, RML

Pulmonary Sequestration
Separate blood supply

Pulmonary Sequestration
• Nonfunctional mass of embryonic and cystic pulmonary tissue– Does not communicate with airway– Separate blood supply
• Intralobar– Lower lobe (presents as “infection”)
• Extralobar– Left sided (often with diaphragmatic hernia)

Pulmonary Sequestration
Surgical resection–Prevent recurrent infection

Cystic AdenomatoidMalformation
• Cysts communicate with main tracheobronchial tree
• Vascular supply from the bronchial circulation
• Proliferation of terminal bronchioles with suppression of alveolar growth and development

Tic
Involuntary repeated contraction of a certain
group of associated muscles

Tic
• No loss of consciousness or amnesia
• Disappear during sleep
• Conscious control can be achieved for short period

Tourette’s Syndrome
•Multiple tics
• Compulsive barking, grunting
• Shouting obscene words

Tourette’s Syndrome
• True “tic” occurs during voluntary movement
• False “tic” does not occur during conscious voluntary movement

RX: Tourette’s Syndrome• Clonidine
• Clonazepam
• Carbamazepine
• Haloperidol
• Pimozide

Conversion Disorder
• Repetitive patterns of voluntary movement or sensory deficit that suggest medical condition–Not intentionally produced
• Initiation/exacerbation preceded by conflict/stressors

Conversion Disorder
• The more medically naive, the more implausible the symptoms
• “Side to side”
• No flexion

Conversion Disorder• Repetitive
voluntary motor behavior
• Always facing camera– Factitious?–Malingering?

Chorea
Irregular, spasmodic, involuntary movements of the
limbs or facial muscles

Sydenham Chorea• Usually associated with juvenile acute rheumatic
fever.
• Characterized by involuntary, irregular, jerky movement by the face, neck, and limbs– Can be unilateral
• Movement intensified by voluntary effort but disappear in sleep

Sydenham Chorea
• May appear months after strep pharyngitis
• Usually resolves within month
• IVIG, valproic acid, haloperidol

14-year-old female with fever, rash

Petechiae • Red-purple, nonblanchable discoloration < 0.5 cm diameter
• Cause:– Intravascular
defects– Infection– Thrombocytopenia Meningococcemia

DDX: Fever, Petechiae
• Meningococcemia
• Rocky Mountain Spotted Fever
• Scarlet Fever
• Pneumococcal septicemia
• Enteroviral infectionPneumococcal sepsis
Scarletina

Meningococcemia
• Neiseria meningitidis – Gram negative diplococci
• URI prodrome followed by high fever, headache
• Two forms (1.2 cases/100,000)– Septicemia - petechiae, purpura, shock– Septicemia and meningitis
• WBC ↓ or ↑• Thrombocytopenia with or w/o DIC

Meningococcemia• Complications– CNS damage– Skin necrosis– Adrenal insufficiency– GI hemorrhage
• Treatment:– IV cefotaxime, ceftriaxone initially– IV PCN G, once sensitivity known– Fluids, supportive care– Treat contacts• Rifampin, ceftriaxone, ciprofloxacin

Rocky Mountain Spotted Fever
• Rickettsia rickettsii– Tick-borne illness– Tick attached >6 hours
• 500-1000 cases/yr USA– Eastern seaboard– Southeastern states
• Incubation 3-12 days– Mean 7 days

Rocky Mountain Spotted Fever
• High fever (> 40° C)
• Abrupt onset – Myalgia, severe headache,
photophobia, vomiting, diarrhea
• 85-90% rash– 2-6 days after fever onset– Macules/papules on palms, soles – Becomes petechial and spreads
centrally

Rocky Mountain Spotted Fever
• Thrombocytopenia
• Hyponatremia
• Proteinuria
• Abnormal LFTs
• CSF pleiocytosis
• Conjunctivitis,splenomegaly, edema, meningismus
• Dx: Acute and convalescent titres
• Rx: Doxycycline– Treat if suspect
disease, particularly if in endemic area

Acute Foot Pain
A 7-year-old male
complains of left foot pain for one day

• 10/9/03 Children face growing danger from so-called community acquired staphinfections.

Osteomyelitis • Young children• Male: female 2:1
• Hx of minor blunt trauma orintercurrent illness (eg URI)
• Usually hematogenous origin– Penetrating trauma or surgery,
adjacent infection
• Staph aureus• Strep pyogenes• Other:– Strep pneumoniae (< 3 years of
age)– Group B strep -Neonates– Pseudomonas - puncture wounds

Osteomyelitis • Infants– Failure to move extremity– Pain on passive movement
• Children– Fever– Refusal to use extremity– Intense pain on palpation– Muscle spasm– Joint in position of most
comfort, slight flexion
• Skin findings LATE– Swelling, erythema, heat

10-year-old female with low-grade fever, rash

Physical Examination
• Skin:– Scattered papules on neck,
trunk, arms
– Vesicle clusters on right buttock with large bullous lesions and surrounding erythema
– No induration
– clustered vesicles right inner thigh, leg, foot

L5-S5
Seidel. Mosby’s Guide to Physical Examination

Definitions
• Vesicle– Elevated, circumscribed,
superficial lesion– Filled with serous fluid– NOT in dermis– < 1 cm in diameter
• Bulla– Vesicle > 1 cm in diameter

Herpes Zoster
• “Shingles”
• History of varicella
• Local paresthesias, pain prior to skin eruption
• Dermatomal distribution of grouped vesicles on an erythematous base

Herpes Zoster• Common in children– Varicella early infancy, in-utero– Immunocompromised– Latent virus in dorsal root
ganglion
• Reactivation 1-3 dermatomes– Does NOT cross midline
• Most common distribution T3-L2, facial (Trigeminal)

Herpes Zoster• Complications– 2° bacterial infection– Motor or CN paralysis– Encephalitis– Post-herpetic neuralgia– Disseminated herpes zoster
• Disseminated herpes zoster– Uncommon in
immunocompetent child

Dx: Herpes Zoster
• CBC: WBC nl or↓
• Viral culture: 48 hrs
• Tzanck smear–Giemsa stain–Wright stain

Herpes Zoster• DDX:–Linear eruption of
herpes simplex
–Contact dermatitis
– Impetigo
AAP

Rx: Herpes Zoster
• Supportive care– Control pain, pruritis
• IV acyclovir within 48-72 hours of onset
• IV acyclovir after 72 hours if:– Immunocompromised– Trigeminal involvement

8-month-old infant


• T 36 .2° C–97 .1° F
• P 148• R 20• P 110/51
Wt 5.2 kg Ht 58 cm HC 41 cm

Hypoalbuminemia: Edema
• Periorbital edema
• Scrotal edema
• Pitting edema of the lower extremities

Generalized Edema
• Accumulation of fluid in body tissues
– Increased capillary permeability
– Decreased oncotic pressure
– Increased hydrostatic pressure
– Impaired lymphatic drainage

Generalized Edema
• Increased capillary permeability
– Allergic reactions
– Infection• Staphylococcal scalded
skin syndrome
– Henoch-Schonleinpurpura
– Kawasaki disease

Generalized Edema
• Decreased oncoticpressure
(low serum albumin)
– Nephrotic syndrome
– Cystic fibrosis
– Protein-losing enteropathy
– Zinc deficiency

Generalized Edema
• Increased hydrostatic pressure
– Fluid overload
– Congestive heart failure
– Constricted pericarditis

Generalized Edema • Impaired lymphatic
drainage
– Usually localized to either one or more extremities
– Rarely generalized

Hypothyroidism: low T4
• Developmental delay
• Hair loss
• Weakness (hypotonia?)
• Impaired growth
• Hypothermia
• Myxedema
T 36 .2° C (97 .1° F)

Myxedema
• Relatively hard edema of subcutaneous tissue with:– Somnolence– Slow mentation– Hair loss– Hoarseness– Weakness

Growth Chart
• If ↓Ht > ↓ Wt:– Suspect endocrine etiology
• If ↓Wt > ↓ Ht:– Suspect poor calorie intake– Suspect ↑calories
expenditure– Suspect ↑calorie
elimination

Zinc Deficiency
• Mild– Poor appetite– Impaired growth
• More severe– Irritability, lethargy– Impaired immunity
• Most severe– Acro-orificial skin rash– Alopecia– Diarrhea

Zinc Deficiency
• Impaired absorption– Regional enteritis– Cystic fibrosis
• Inadequate intake
• Inborn error– Acrodermatitis
enteropathica

Infant Botulism: botulinumtoxin in stool
• Descending weakness
• Symmetric facial, truncal, extremity weakness
• “Rag doll cry”
• Bilateral ptosis
• Clostridium botulinumtoxin blocks AChrelease in peripheral synapses
– Impaired autonomic system• Constipation
– Impaired neuromuscular system

History
• Full term, NSVD– Birth weight 6 lb 7 oz (10%)– Breast fed
• Eczema, 2 months of age– Treated with vaseline
• Superinfected eczema, 3 months of age– Treated with antibiotics– Developed diarrhea
• Eczema, diarrhea persist
• 1 week ago, swelling of extremities – Acute scrotal swelling for 1 day
• Denies fever, vomiting,recurrent infections, anorexia

History• 2 month WCC only– Weight ~ 12 lbs (50%)– Received immunizations
• Diet: breast milk, fish broth
• Development:– Smiles, tracks, turns to voice– Hands to mouth– Can not lift head, sit, or roll over
• Family history:– Parents, two older sisters Healthy, average height, weight

Key Features
• Irritability
• Developmental delay/weakness
• Edema
• Excoriated, exudative, red skin– Mouth, rectum, extremities,
trunk, scalp
• Hair loss

DDX: Edema, Eczema, Weakness, Developmental Delay?
• Malnutrition, neglect• Protein sensitivity, malnutrition• Protein-losing enteropathy, malnutrition• Acrodermatitis enteropathica• Hypothyroidism• Wiskott-Aldrich syndrome• X-linked agammaglobulinemia• Phenylketonuria

Protein SensitivityAllergy to dietary proteins
• More common in infants <12 mos– FH of atopy common
• Older children have celiac-like symptoms– Steatorrhea– Hypoproteinemia– Chronic diarrhea
• Food challenge confirms – Skin test unreliable
• Usually disappears after 12 months of age
• Allergies to fish, eggs, peanuts more likely to be lifelong

Protein-losing Enteropathy
• Excessive loss of plasma proteins into GI tract in association with:
– Inflammation of bowel– Intestinal graft vs host– Acute/chronic infection– Venous or lymphatic obstruction– Malignant infiltration of bowel,
lymphatics

Protein-losing Enteropathy
• Signs and symptoms:
• Hypoproteinemia• Malabsorption
– Diarrhea– Edema– Poor weight gain– Signs of vitamin and mineral
deficiencies

Protein-losing Enteropathy
• Vascular – CHF– Constrictive
pericarditis
• Stomach– Gastritis– Polyps
• Small intestine– Celiac disease– Intestinal lymphangiectasia– Abetalipoproteinemia– Ischemia– Inflammatory bowel disease– Allergic enteropathy
• Colon– Ulcerative colitis– Hirschsprung disease

Celiac Disease
• Gluten sensitivity– Small intestine– Autoimmune response • Tissue transglutaminase
• Classic picture– Potbelly – Thin buttocks– Proximal arm and thigh muscle
wasting due to nutrient malabsorption

Celiac Disease 1:100-340
• Other signs – Irritability– Anorexia– Chronic diarrhea– FTT
• Diagnosis– 1-hour D-xylose test– 72 hour fecal fat
– Antiendomysial Ab– Antitissue transglutaminase Ab

Acrodermatitis Enteropathica• Inborn error of Zinc– Autosomal recessive– 1:500,000 Denmark
• Perioral and acral dermatitis• Alopecia• Diarrhea
• Diagnosis based on continued need for Zinc supplement

Wiskott-Aldrich Syndrome
• X-linked immunodeficiency– Low IgM, ↓CD8+ T cells
• Recurrent bacterial sinopulmonary infections• Eczema• Thrombocytopenia
• Autoimmune phenomena• Malignancies

Wiskott-Aldrich Syndrome1:1 million
• Present at birth with:– Petechiae, ecchymoses– Bloody diarrhea
• Diagnosis:– Low platelet count
– Low IgM, IgG– Normal to high IgA, IgE
– Anergy to delayed type hypersensitivity skin tests

X-linked Agammaglobulinemia(Bruton) 1:200,000
• Infants– Recurrent otitis media, pneumonia, sinusitis– Diarrhea (Giardia, Campylobacter)
• Atopy – Eczema– Allergic rhinitis– Asthma
• Diagnosis:– Low, absent IgM, IgG, IgA, IgE

Phenylketonuria1:15,000
• Skin– Eczema– Fair skin
• Mental retardation
• Seizures
• Extrapyramidal signs

Laboratory• Hgb 10.5 • Hct 31.4– MCV 75
• WBC 17.8– 48% seg– 29% lymph– 65 mono– 17% eos
• Plat 755 K
• Total protein 2.2 g/dL– (nl 5.0 - 7.5)
• Albumin < 1.0 g/dL– (nl 2.7 - 5.0)
• Free T4 0.90 ng/dL – Nl 0.7 - 1.8
• TSH 28.0 μIU/ml– Nl 0.28 - 5.0

Laboratory
• IgE 3864 IU/ml– Nl 0 - 230
• IgA Endomysial Ab: none detected
• Zinc 29.0 μg/L– Nl 66 - 144– Severe < 40
• RAST– Very high IgE to:• α-lactalbumin, eggwhite,
peanut, soybean, wheat
• Stool– Trace reducing
substances– Fat ↑

Diagnoses Treatment• Protein-losing
enteropathy
• Protein allergy
• Hypothyroidism?– ↑TSH, low nl T4
• Zinc deficiency – Probably nutritional
• Elemental formula
• Zinc supplement
• Refused thyroid replacement

Day 2

6 months later (14-months-old) • Total protein 4.4
– (nl 5.0 - 7.5)
• Albumin 2.5 – (nl 2.7 - 5.0)
• TSH, T4 normal
• Zinc 79.0 μg/L – (nl 66 - 144)
• Crawling, pulls to stand, cruising
• Stacks 2-3 cubes
• Babbles, “mama”

28-mos-old
• Diet– Chicken, rice, apples,
pears, sweet potatoes– Elemental formula
• No diarrhea or eczema
• Walking, running, jumping
• Eats with spoon, drinks from cup
• 100-200 words• 2 word sentences

Staph, Strep,
Either ... or Other?

Gp A Strep
• Throat culture (+)
• Scarletina rash
• Post pharyngeal cellulitis

Scarlet Fever Rash
• Diffuse erythema: neck, axillae, inguinal area– Spreads to rest of body– Toxin-producing Group A Strep
• “Sandpaper” texture
• Desquamates 7-14 days

Seven-year-old male: 10 days fever, 5 days sore throat, two days rash

EBV Infection
• Throat culture (-)• ASO titre (-)
• HSV culture negative
• Monospot (-)
• EBV Ab to Viral CapsidAg, IgG (+)

Infectious Mononucleosis
• Pharyngitis (1/3 exudative)• Generalized lymphadenopathy• Fever > 90%• Hepatosplenomegaly
• Maculopapular, red rash 3-15%– 80% rash if treated with
ampicillin, amoxicillin– Circulating IgG, IgM antibodies to
ampicillin demonstrable

Three-year-old male

StaphyloccalScalded Skin
Syndrome
• Systemic effects of exotoxin produced by Staph aureus– Causes of superficial cleavage of epidermis
• Nikolsky sign– Superficial layers of skin slide off deeper
layers when rubbed

Staphyloccal Scalded Skin Syndrome
• Treat as severe burn– Dehydration
• Vancomycin, clindamycin, oxacillin
• Toxin production suppressed with clindamycin– Binds to 50s ribosomal subunit– Interferes with protein synthesis– Suppresses monocyte synthesis of TNF

7-year-old male with fever, toe infection, rash and
hypotension

Toxic Shock Syndrome
• Fever, hypotension, rash– Circumoral pallor– Scarletina
• 3 or more systems– GI, mucous, muscular,
renal, hepatic, hematologic, CNS
• Cause:–Staph aureus– Group A Streptococcus

Lymphangitis
• Inflammation oflymphatics draining site of infection

Two-year-old female with 5 days of fever

Kawasaki Disease

Kawasaki Disease
• Fever lasting for 5 days
• Four of the five conditions:– Bilateral, non-exudate conjunctivitis– Mucous membrane changes– Changes of peripheral extremities • Edema, erythema
– Polymorphous, nonvesicular rash • Usually trunkal
– Cervical lymphadenopathy• Node > 1.5 cm

Incomplete Kawasaki“Atypical”
• 20% - 60% children with coronary aneurysms due to incomplete KD
• Consider incomplete KD in and any child with 5 days fever, no bacterial disease and 2 of following criteria:– With or w/o: 1) 2 or more classic KD criteria and
anterior uveitis (slit lamp)– Plus lab evidence of inflammation (↑WBC, ESR,
CRP, Platelets after 7 days fever, LFTs)

Nonbullous Impetigo
• All ages– Children aged 2-5 years more often
• Group A Strep (S. Pyogenes)– Spread from skin to nose, throat
• Staph aureus
• Thin-walled vesicles or pustules on red base– Prompt rupture with serum release– Honey-colored crust– 90% lymphadenopathy

NonbullousImpetigo
Pustule
Rupture
Serous fluid
Vesicles

Bullous Impetigo• All ages– Newborns, infants more often
• Staph aureus– Phage group II type 71– Exfoliatin toxin– Spread from nose to skin
• Vesicles enlarge into bullae 1-2 cm– Rupture 1-3 days– Thin, light-brown crust– Lymphadenopathy rare
AAP

Four-month-old female with pneumonia

History
• A 4-month-old female is admitted for pneumonia and labored breathing
• URI symptoms for 2 weeks– No fever
• Parents bring to ER when fast respirations develop

ER Exam
• T 37.8° C – 100° F
• R 70 bpm
• P 170 bpm
• SaO2 93% RA

ER Exam
• Decreased breath sounds left chest– Liver 2 cm below costal margin
• CXR: Left lower lobe consolidation
• Hgb 10, Hct 29.6
• WBC 10.6 – 42 S, 3 B, 40 L

ER Treatment
• Albuterol aerosol given–SaO2 96% RA (from 93%)–Medium crackles, left lower chest
• Admit to ward
• Dx: Pneumonia, LLL

CXR• Really big heart
• Increased pulmonary vasculature
• No lung consolidation

CXR• Really big heart
• Increased pulmonary vasculature
• No lung consolidation

CXR
• Really big heart
• Increased pulmonary vasculature
• No lung consolidation

Right Axis Deviation
• Lead I (-): S wave > R wave
• Lead AVF (+): R wave > S wave

Right Axis Deviation
• Lead I (-): S wave > R wave
• Lead AVF (+): R wave > S wave

Left Atrial Enlargement
Wide, M-shaped P waves

Myocardial Damage
ST Depression

DDX: Cardiomegaly• Congestive heart
failure
• Endocardial fibroelastosis
• Glycogen storage disease
• Cardiomyopathy
• Rhabdomyoma
• Congenital heart disease– Anomalous origin of
the coronary arteries– Coarctation of the
aorta– Septal defects– Large PDA

Cardiomegaly: Laboratory
• Echocardiogram• Troponin • Adenoviral titres• Metabolic screen– Serum amino acids– Urine organic acids, mucopolysaccharides,
oligosaccharides

Troponin > 2.3 ng/mL (nl 0.0 - 2.3)
Severe LV Dysfunction

Anomalous origin of the left coronary artery
• Dye enters from aorta
• Dye appears in left coronary artery and enters pulmonary artery

Anomalous origin of the left coronary artery
• Left coronary artery arises from pulmonary artery
• Decrease mycocardial perfusion by age 2 months– LV ischemia, infarction
• Severe CHF at 2-4 months of age– LV dysfunction– Mitral insufficiency

Absence Seizure • Short staring spells
• Short duration– 5 - 15 sec
• No postictal lethargy
• Synchronous 3Hz spike-and-wave

Tonic-Clonic Seizure
• Tonic phase (Stiffening)– Slow waves with
increasing amplitude and decreasing frequency
• Clonic phase (Jerking)– Repetitive
synchronous bursts of spike activity
• Postictal lethargy

Infantile Spasms
• Quick, lightening-like jerks
• Jack-knife flexion of the trunk
• Extensor spasms
• “Hypsarrhythmia”– High voltage slow
waves, spikes, and polyspikes – Background
disorganization

Ileal Atresia• Due to intrauterine
vascular obstructive accidents
• Symptomatic 1st day:–Bilious emesis–Abdominal
distension

Ileal Atresia
• 25% Polyhydramnios
• 60-75% fail to pass meconium
• DDX:– 10% CF with meconium ileus– 5% Hirschsprung disease of
colon and terminal ileum

Small Bowel Obstruction
• Duodenal atresia– Non-bilious or bilious
vomiting 1st day– Non-distended
abdomen
• Ileal atresia– Bilious vomiting 1st day– Distended abdomen

Adactyly Absent metatarsal and proximal, middle and distal phalanx.
Due to intrauterine local mesenchymal injury
Prognosis: Supportive shoe as adult?

16-year-old male with low back pain for 6 months
• ↓ R ankle reflex
• ↓ Strength R lower leg
• ↓ Sensation R lower leg

Spinal MRI
• Focal disc protrusion
• L5 - S1– Right side– Achilles tendon reflex
Seidel. Mosby’s Guide to Physical Examination

Herniated Disc• 1/3 due to Trauma– Rare in pre-adolescence
• Most injuries L5-S1
• Signs and symptoms– Pain: sitting, back flexion, radiates down leg, foot – Extension of spine relieves pain– Weakness, paresthesia of leg, foot
• Abnormal straight-leg raising test most common finding
• Treatment: rest, exercise, steroids, surgery if neurological findings persist