-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
1/22
Visualizing the Relationship between Human Error and
Organizational Failure
Chris Johnson
Department of Computing Science,
University of Glasgow, Glasgow G12 8QQ.
Fax: 0141 330 4913, Telephone: 0141 330 6053,
Email:[email protected],
http://www.dcs.gla.ac.uk/~johnson
Managerial failure plays an important role in major accidents
and
incidents. Operators have been authorized to deliberately remove
safety
mechanisms. They have also been instructed to guide
application
processes into dangerous operating environments. Given the
consequences
of such intervention, it is surprising that so little attention
is paid to therelationship between organizational failure and
operator error. One
explanation for this is that tools and techniques, which have
been
developed to analyze human and system failures, cannot easily be
applied
to reason about organizational problems. This paper argues that
Fault
Trees help to visualize the ways in which organizational
failures create the
necessary preconditions for human failure. This approach is also
used to
focus on the organizational problems that can exacerbate the
consequences
of those errors in the aftermath of an accident. It is argued
that too much
attention has been paid upon human errors in the causes of
accidents and
not enough attention has been paid to organizational failure in
post-accident events. A collision between a Maryland Commuter train
and an
American National Railroad Passenger Corporation train on
February 16th,
1996 is used to illustrate this argument.
Keywords: human error; organizational failure; fault trees;
safety;
accidents.
1. Introduction
Many accident reports cite human failure as a primary cause
(Johnson, 1998). The
workers at the Bhopal chemical plant pumped Methyl-isocyanate
into a leaking tank(Morehouse and Subamaniam, 1986). The officers
and crew of the Herald of Free
Enterprise set to sea with their bow doors open (Sheen, 1987).
The pilot and co-pilot
throttled back their one working engine rather than the failed
engine during the Kegworth
air crash (AAIB, 1990). The first line of fire-fighting
operations was delayed by
communications failures between various operators during the
Channel Tunnel Fire
(Department of the Environment, 1996). This paper explains why
operator error is such a
mailto:[email protected]:[email protected]:[email protected]
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
2/22
prevalent cause of major accidents: insufficient attention is
being paid to the managerial
weaknesses that make systems vulnerable to human failure.
There has been a considerable amount of research into the causes
of human error. Much
of this has stressed the psychological and physiological
influences that shape operator
performance. There has been a focus on the effects of high
workload on a users ability torespond to warning messages (Woods,
1994). Other research has focussed on the impact
of noise and vibration on an operators decision making
processes. There has also been a
focus on individual attitudes to risk taking (Stanton and
Glendon, 1996). Unfortunately,
much of this work focuses on the symptoms of human error rather
than its underlying
causes (van Vuuren, Shea, and van der Schaaf, 1997). Relatively
little work
has focussed on the underlying organizational and regulatory
weaknesses that lead to
high workload or noise in an operators environment (Hale,
Wilpert and Freitag, 1997).
These less direct forms of human failure help to establish the
working practices that result
in operator error (Reason, 1997). Unless we understand the
managerial and regulatory
causes of human failure then there is little prospect that we
will ever be able to reduce the
number of accidents and incidents that are being blamed on
operator error.Unfortunately, there are few techniques that can be
used to reason about the interaction
between organizational failure and human error. Cognitive models
cannot easily be
extended to represent regulatory requirements. Conversely, it is
difficult to reason about
individual responses to particular system failures using
optimization models from
operations research (Johnson, 1995). This paper, therefore,
shows how fault trees help to
visualize the relationship between organizational problems and
human failure. This
notation is appropriate because it reveals that:
1. organizational failures create the necessary preconditions
for human error;
2. organizational failures also exacerbate the consequences of
those errors.
Fault trees can also be integrated into other analytical tools
that support process
improvement, such as Management Oversight and Risk Trees (MORT).
A further benefit
is that the fault tree notation is well understood by existing
generations of engineers.
There are, however, many reasons why the standard fault tree
notation is not appropriate
for our purpose. These issues are discussed in more detail in a
previous paper (Love and
Johnson, 1997). In contrast, the remainder of this paper
demonstrates that the approach
can be used to analyze the complex, "messy" blend of operator
errors and organizational
failures that characterize real world accidents. A collision
between a Maryland Commuter
train and an American National Railroad Passenger Corporation
train on February 16 th,1996 is used to illustrate this
argument.
1.1 The MARC 286 Case Study
The National Transportation Safety Board (NTSB) report provides
the following
executive summary of the collision that forms the case study for
this paper:
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
3/22
"About 5:39 pm on February 16, 1996, Maryland Rail Commuter
(MARC) train 286
collided with National Railroad Passenger Corporation (Amtrak)
passenger train 29 near
Silver Spring, Maryland. En route from Brunswick Maryland to
Union Station,
Washington DC, MARC train 286 was travelling under CSX
Transportation Inc (CSXT)
operation and control on CSXT tracks. MARC train 286 passed an
APPROACH signal
before making a station stop at Kensington, Maryland; proceeded
as if the signal hadbeen CLEAR; and then, could not stop for the
STOP signal at Georgetown Junction,
where it collided with Amtrak train 29. All 3 CSXT operating
crew members and 8 of the
20 passengers on MARC train 286 were killed in the derailment
and subsequent fire.
Eleven passengers on MARC train 286 and 15 of the 182
crewmembers and passengers
on AMTRAC train 29 were injured. Estimated damages exceeded $7.5
million" (page vii,
NTSB, 1997).
This accident provides an appropriate case study because at
first sight it appears to have
been caused by a relatively simple instance of operator error.
The engineer on-board
MARC train 286 forgot that the previous signal had been APPROACH
instead of
CLEAR. They, therefore, reached the Georgetown Junction with a
velocity that preventedthem from stopping in time to avoid AMTRAC
train 29. Later sections will argue,
however, that such a superficial analysis ignores the managerial
and regulatory factors
that contributed this accident. These organisational factors
helped to create a system that
relied upon the crewmembers memory of a signal that they had
seen minutes before an
unscheduled stop.
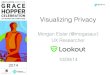
1.2 Using Fault Trees to Support Accident Analysis
This paper uses fault trees to represent and reason about the
relationship between
organisational failure and human error. This notation provides a
simple graphical syntaxbased around circuit diagrams. Figure 1
presents a brief overview of this approach.
Andrews and Moss (1993) provide a more detailed
introduction.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
4/22
Figure 1: Fault tree components
Fault trees are, typically, used pre hoc to analyse potential
errors in a design. They have
not been widely used to support post hoc accident analysis. They
do, however, offer
considerable benefits for this purpose. The leaves of the tree
can be used to represent the
initial causes of the accident (Leplat, 1987). The gates in
Figure 1 can be used to
represent the ways in which those causes combine. For example,
the combination of
operator mistakes, hardware/software failures and managerial
problems might be
represented using an AND gate. Conversely, a lack of evidence
about user behaviour orsystem performance might be represented
using an OR gate. Basic events can be used to
represent the underlying failures that lead to an accident
(Hollnagel, 1993).
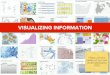
Figure 2 uses a fault tree to represent some of the findings in
the NTSB report:
"The MARC train 286 engineer apparently forgot the signal
aspect, which
required him to be prepared to stop at Georgetown Junction, due
to interference
caused by various events, including performing an unscheduled
station stop, that
occurred between the presentation of the APPROACH aspect at
signal 1124-2 and
the STOP signal at Georgetown Junction." (NTSB, 1997, Conclusion
4, page 73)
"Neither the conductor nor the assistant conductor while in the
cab control
compartment appeared to have effectively monitored the engineers
operation of
MARC train 286 and taken action to ensure the safety of the
train" (NTSB, 1997,
Conclusion 5, page 73)
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
5/22
Figure 2 also shows that there is no direct means of translating
from natural language into
the structures of a fault tree. Analysts must identify key
events from the prose. These
events must then be structured using the gates that were
introduced in the previous
paragraph. Later sections will integrate the first three
conclusions from the NTSB report
into the fault tree shown in Figure 2.
Figure 2: An example of a fault tree representing part of the
MARC accident
A number of important differences distinguish this use of fault
trees from their more
conventional application. The output from an AND gate is true if
and only if all of its
inputs are true. It is difficult to analyse an accident in this
way. For example, Figure 2
shows that the collision was the result of four events. The
derailment would have been
prevented if any one of these events had been prevented from
happening. In accident
analysis, however, it is difficult to be certain that an event
would actually have been
avoided in this way. The derailment may or may not have been
avoided if the Conductor
had intervened. This potential conflict between the pre hoc use
of fault trees to support
risk assessment and their post hoc use to support accident
analysis can be resolved. In the
post hoc application of fault trees we are building our model
upon a known set of events.
Any inferences that depend upon events that are not part of that
set must be regarded as
speculation unless further evidence can be provided. In the
previous example, this might
involve empirical or observational studies of the interaction
between Conductors and
Engineers on MARC trains.
2.0 Immediate Causes
Figure 2 focussed on the immediate causes of the MARC collision
as they were described
in the concluding section of the NTSB report. These findings
focus upon the operator
errors that directly caused the derailment. This analysis can be
extended to provide a
more complete overview of the events that led to the accident.
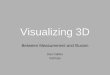
Figure 3 provides an
overview of the findings in the NTSB report. It accurately
reflects the direction and focus
of the argument in the concluding section. Most of the findings
relate to the Engineers
error rather than to the monitoring activities of the Conductor
or their assistant. This is
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
6/22
shown by the way in which the left-hand branch of the tree is
developed from the
intermediate event in which MARC 286 approaches Georgetown
Junction as if signal
1124-2 was set to CLEAR. The lack of intervention by the
Conductor and Assistant
Conductor is less of a focus than the Engineers error.
Figure 3: An Extended Fault Tree Showing Events Leading to the
MARC Collision
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
7/22
The previous fault tree provides a graphical representation of
the focus in the NTSB
report. This offers a number of important benefits:
1. Fault trees provide an overview of the events that an analyst
believes contributed
to an accident. This is important because many reports are
lengthy and detailed.
The NTSB account is approximately 150 pages in length. The
analysts findingsare, typically, summarised in the concluding
section of an accident report.
However, it can often be difficult to piece together individual
conclusions into a
coherent account of human error and systems failure;
2. Fault trees also suggest alternative hypotheses and questions
about the analysis
that is presented in an accident report. Readers can further
develop the
intermediate events in a tree to explore alternative
conclusions. For example, the
relative lack of attention that was paid to the Conductor and
the Assistant
Conductor can be contrasted with similar reports in the aviation
industry that
focus on cockpit communications rather than individual errors
(AAIB, 1990).
Figure 4 focuses on part of the fault tree presented in Figure
3. In particular, it representsome of the non-contributory factors
that were mentioned in the previous section:
"Neither the three MARC train 286 crewmembers nor the two Amtrak
train 29
locomotive crewmembers were impaired by alcohol or drugs. All
train
crewmembers were in good health, had no evidence of fatigue, and
were
experienced in and qualified for their duties." (NTSB, 1997,
Conclusion 1, page
73)
These non-contributory factors are represented as house events.
They can either be
"turned" on or off during the analysis of a fault tree. The NTSB
report indicated thatneither drugs nor illness affected the
Engineer in the MARC collision. Technically, this
can be represented by assigning a probability of 1 to the two
house events in Figure 4.
However, the ability to switch events on and off also provides
analysts with means of
exploring alternative hypotheses about the course of an
accident. For instance, a house
event can be turned off if it is assigned a probability of 0.
This can be used to explore
what might have happened if the Engineers performance had been
impaired by drugs or
by alcohol. The OR gate would then indicate that the Engineer
could forget the
APPROACH aspect of signal 1124-2 even if their memory were not
impaired by the
unscheduled stop. This specific example illustrates how the
non-contributory factors in
the NTSB report help readers to identify alternative scenarios
or hypotheses about the
events that might have led to the accident. The level of
analysis presented in Figure 4might seem simplistic. However, it is
important to point out that this is the level at which
the NTSB report was written. Fault trees simply help to reason
about the consequences of
the alternative scenarios that were implicit in the conclusions
of the report.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
8/22
Figure 4: Using House Events to Represent Alternative
Scenarios
Inhibit gates provide an extension to the approach discussed in
the previous paragraph.
Rather than assigning Boolean probabilities to house events,
these gates can be associated
with a wider range of probabilities. Figure 5 exploits inhibit
gates as a means of
describing further hypotheses about the potential impact of
non-contributory factors in
future accidents and incidents. In this case the hypotheses
relate to the effects of bad
weather and signal failure on the course of the collision:
"The weather conditions did not impair the ability of the MARC
train 286
crewmembers to distinguish the indication of the Kensington
signal 1124-2."
(NTSB, 1997, Conclusion 2, page 73)
"The signal system functioned as designed." (NTSB, 1997,
Conclusion 3, page
73)
Figure 5 uses probabilistic inhibit gates because the Engineers
ability to view signal
1124-2 need not be impaired every time that there was bad
weather. Similarly, a
signalling failure need not always lead to an incorrect
indication for 1124-2. This ability
to assign probabilities to representations of human error should
not be underestimated. It
provides the opportunity for Monte Carlo simulation techniques
in which analysts can
investigate probable and improbable, frequent or infrequent,
traces of interaction. Theobvious pitfall is that there must be
some means of validating the statistics that are used
to prime models such as that shown in Figure 5. The most
appropriate means of obtaining
these figures after an accident is through reconstruction and
empirical tests with other
operators. Of course, these studies are inevitably biased by the
individuals knowledge
that their performance is being monitored in the aftermath of an
accident. These studies
have, however, been widely used in previous accident reports
(AAIB, 1990).
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
9/22
Figure 5: Using Inhibit Gates to Represent Alternative
Scenarios
The previous paragraphs have argued that fault trees can be used
to provide an overview
of the immediate human errors that contribute to accidents.
House events and inhibit
gates can also be used to analyse the non-contributory factors
that did not play a part in
past failures but which might lead to similar errors during the
future operation of thesystem. The following section builds on this
analysis and shows how our fault tree model
can be extended to capture the managerial and regulatory factors
that created the potential
for the direct human error in Figures 3 to 5.
3.0 The Organisational Origins of Direct Human Error
The first five findings in the NTSB report focused on
non-contributory factors and the
interaction between the Engineer, the Conductor and the
Assistant Conductor. The
remaining twenty-two findings centred on the organisational
factors that contributed to
the accident. These organisational problems involve both
managerial and regulatory
failure. Many of them stemmed from a failure to review the human
factors implicationsof increasing the capacity on the Brunswick
line. Increasing the capacity implied
reducing the train headway to 15 minutes during dense scheduling
periods. This, in turn,
implied changes to the signalling system. In consequence, the
Engineer had to remember
the aspect of signal 1124-2 both before and after any stop at
Kensington station:
"Additionally, signal 100 was less than the 11,000 feet minimum
braking
requirement from the EAS-2 signals at CP Georgetown Junction. As
a result of
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
10/22
the signal modifications, signal 100 was replaced by signal
1124-2, which was
now the last automatic wayside signal before EAS-2 for
Georgetown Junction and
was west of the Kensington station platform" (NTSB, 1997, page
43).
The NTSB report summarised the managerial and regulatory
failures that created this
situation in the following conclusions from their accident
report:
"Had the Federal railroad Administration and the Federal Transit
Administration
required the CSX Transportation Inc. to perform a total signal
system review of
the proposed signal changes that included a human factors
analysis with
comprehensive failure modes and effects analyses, this accident
may have been
prevented". (NTSB, 1997, Conclusion 7, page 73)
"Federal funds granted for the signal modifications on the CSXT
Brunswick Line
to accommodate an increase in the number of Maryland Rail
Commuter trains did
not ensure that the safety of the public was adequately
addressed" (NTSB, 1997,
Conclusion 8, page 73)
"The Federal Railroad Administration relied on the need for
increased vigilance
of wayside signals and special actions in operating rules, such
as the crew
communication rule of emergency order 20, does not adequately
safeguard the
public" (NTSB, 1997, Conclusion 10, page 73)
"Had a train control system that could utilise the cab signal
equipment on the
Maryland Rail Commuter cab control car been a part of the signal
system on the
Brunswick Line, this accident may not have occurred." (NTSB,
1997, Conclusion
11, page 73)
Figure 6 illustrates how these findings can be integrated into
the fault tree model. A
cursory inspection reveals the additional complexity that is
introduced when investigators
consider the deeper sources of organisational failure that
contribute to major accidents
and incidents.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
11/22
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
12/22
Figure 6: Using Fault Trees to Represent the Organisational
Precursors to Human Error
Previous sections have introduced non-contributory causes into
our fault tree model of
human error and organisational failure. Drugs and illness were
rules out as influences on
the operators behaviour. By considering these causes, analysts
can identify alternative
scenarios that might lead to similar accidents in the future.
Conversely, accident reportsoften speculate about events that might
prevent similar accidents in the future:
"A fully implemented positive train separation control system
might have
prevented this accident by recognising that MARC train 286 was
not being
operated within allowable parameters, based on other authorised
train operations,
and would have stopped the train before it could enter into the
unauthorised track
area" (NTSB, 1997, Conclusion 12, page 73)
Figure 7 captures this finding. The diagram again illustrates
the relationship between the
natural language comments of the NTSB report and the formal
analysis techniques that
can be applied to fault tree diagrams. In this case, the house
events are assigned a
probability of 1 to simulate the events leading to the
collision. The Federal Railroad
Administration and the Federal Transit Administration allowed
the proposed signal
changes without a comprehensive failure modes and effects
analysis. According to figure
7, if the house events had been false and an analysis had been
conducted then a positive
train separation control system would have been introduced. In
consequence, the highest
level conjunction would not have been true. The derailment would
not have taken place.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
13/22
Figure 7: Using Fault Trees to Represent the Organisational
Precursors to Human Error
The previous analysis raises many questions about the role of
organisational failure in
major accidents. It is not certain that a failure modes and
effects analysis would have led
to the introduction of a positive train separation system, as
suggested in Figure 7. This
objection can be represented by replacing the house events with
an inhibit gate. Analysts
could then assign a probability to the introduction of a train
separation system given thata failure modes and effects analysis
had been conducted. This approach, in turn, raises
further questions about quantified approaches to group decision
making. It is unclear how
reliable data might be obtained and validated for such an
analysis. What figure would an
accident investigator be justified in assigning to a particular
outcome of the failure modes
and effects analysis? Such questions point towards a need to
explore the relationship
between economics or management theory and cognitive science
(Johnson, 1995). The
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
14/22
former approaches provide accounts of group decision making
under uncertainty. The
latter provides more qualitative insights into individual
instances of human error.
4.0 The Aftermath
Previous sections have shown that fault trees provide one means
of integratingobservations about organisational failure into an
analysis of more direct forms of human
error. Previous diagrams have, however, suffered from a weakness
that is common in
many human factors investigations. There is a preoccupation with
the causes rather than
the consequences of an incident. This is a significant
limitation because most lives are
lost in the aftermath of an accident than are lost through its
immediate effects. In the
MARC case study, at least eight of the eleven fatalities were
caused by events that
occurred after the immediate collision. Figure 8 alters the
perspective of previous fault
trees by focussing on the immediate aftermath of the collision.
It represents the following
conclusions from the NTSB report:
"The emergency egress of passengers was impeded because the
passenger cars
lacked readily accessible and identifiable quick-release
mechanisms for the
exterior doors, removable windows or kick panels in the side
doors, and adequate
emergency instruction signage." (NTSB, 1997, Conclusion 13, page
73)
"The catastrophic rupture of the Amtrak unit 255 fuel tank in
the collision with
the MARC cab control car 7752 released fuel, which sprayed into
the interior of
the cab control car, and resulted in the fire and at least 8 of
the 11 fatalities."
(NTSB, 1997, Conclusion 18, page 74)
"Even though the Montgomery County Fire and Rescue Service
personnelresponded promptly to the emergency, they could do nothing
to save the lives of
the accident victims because passenger coach cab control car
7752 was already
completely engulfed in flames when the fire fighters arrived on
the scene."
(NTSB, 1997, Conclusion 21, page 74)
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
15/22
Figure 8: Fault Tree Showing Events Following the MARC
Collision
As can be seen, there is an even greater emphasis on
organisational problems in the
aftermath of an accident than in its immediate causes. This
analysis highlights an
important distinction between two different forms of
organisational failure:
1. Managerial failure. This relates to the ways in which
companies organise and
manage their working practices.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
16/22
2. Regulatory failure. This relates to the ways in which
governments and other
statutory bodies govern and monitor the working practices of
companies and
industries.
The previous diagram focussed on managerial failure. The train
operators failed to
provide adequate emergency instructions or escape mechanisms in
their passenger car.However, the NTSB report also found regulatory
problems that exacerbated the
consequences of this accident:
"The absence of comprehensive Federal passenger car safety
standards resulted in
the inadequate emergency egress conditions." (NTSB, 1997,
Conclusion 14, page
73).
"A need exists for Federal standards requiring passenger cars be
equipped with
reliable emergency lighting fixtures with a self-contained
independent power
source when the main power supply has been disrupted to ensure
passengers can
safely egress." (NTSB, 1997, Conclusion 15, page 74)
"Prescribed inspection and maintenance test cycles are needed to
ensure the
reliable operation of emergency windows in all long-distance and
commuter rail
passenger cars." (NTSB, 1997, Conclusion 16, page 74)
Figure 9 shows how these regulatory weaknesses contributed to
the managerial failures
shown in Figure 8. Such an integrated approach is critical if
readers are to gain an
overview of the relationship between operational practices and
the regulatory structures
that guide those practices.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
17/22
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
18/22
Figure 9: Representing Regulatory Problems in an Extended Fault
Tree
The previous fault tree illustrates how the lack of Federal
standards for reliable
emergency lighting combined with the lack of suitable signs in
the MARC car to prevent
passengers from finding the emergency exits. Similarly, the lack
of more general Federal
safety standards combined with the inadequate maintenance cycles
of the MARCoperators to prevent passengers from using the exits
once they had located them. Even
this level of analysis simplifies the organisational problems
that were uncovered by the
NTSB:
"Because other commuter passenger cars may also have interior
materials that
may not meet specified performance criteria for flammability and
smoke emission
characteristics, the safety of passengers in those cars could be
at risk." (NTSB,
1997, Conclusion 19, page 74).
"The Federal guidelines on the flammability and smoke emission
characteristics
and the testing of interior materials do not provide for the
integrated use of
passenger car interior materials and, as a result, are not
useful in predicting the
safety of the interior environment of a passenger car in a
fire." (NTSB, 1997,
Conclusion 20, page 74)
Each stage of this analysis takes us further and further away
from the Engineers initial
error. It also moves us further and further away from most of
the analysis techniques that
are being developed by human factors and systems engineering.
The NTSB alsoidentified a range of further management problems:
"The CSX Transportation Inc. personnel operating Maryland Rail
Commuter
passenger trains are not adequately trained to understand and,
therefore, execute
their responsibilities for passengers in emergencies." (NTSB,
1997, Conclusion
24, page 74)
Figure 10 extends the previous diagrams to introduce these
additional findings. This fault
tree provides graphic evidence both of the complexity and
diversity of organisational
factors that exacerbate the effects of an accident and can
frustrate a co-ordinated response
to any incident.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
19/22
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
20/22
Figure 10: Fault Tree Showing Organisational Failures and Direct
Operator Error.
5.0 Conclusion
This paper has extended the application of fault trees beyond
their normal use in systems
engineering. This notation provides important visualisation
properties that enable readers
to gain an overview of complex, interconnected events. For
example, the previous
diagram shows how the lack of Federal guidelines contributed to
the passengers
difficulties in escaping during the fire. Our use of fault trees
also provides visual support
for the argument that post accident events are just as
important, if not more important,
than the more immediate human errors that lead to many
accidents. Most of the fatalities
in the MARC collision could have been avoided if managerial and
regulatory structures
had ensured the provision of effective escape mechanisms.
The previous argument introduces the second focus of this paper.
It has been argued that
too little attention has been paid to the role of organisational
failure in major accidents.
The role of managerial and regulatory practices as
pre-conditions for human error has
been particularly neglected. There are some exceptions to this
criticism (Reason 1997,
Hale, Wilpert and Freitag 1997, van Vuuren, Shea and van der
Schaaf, 1997). However,
most human factors and systems engineering has focused on the
immediate causes of
operator error and system failure rather than on the
organisational context of those errors.
Distributed cognition, situation awareness, high-workload and
mode confusion have
become part of a mantra that is being repeated with an
increasing frequency in accident
reports. Their prominence as causal factors in these documents
often obscures widerissues to do with workplace organisation and
industrial regulation. The NTSB case study
is an exception to this general criticism. It is rare to find an
official report that is so
candid in its analysis of managerial and regulatory practice.
This is a result of the
NTSBs position outside the Federal regulatory mechanisms that
protect the railroads.
Many other reporting agencies lack this independence. This
reduces the likelihood that
they will examine the managerial and regulatory practices that
create the context for
individual human errors.
Acknowledgements
Thanks go to the members of the Glasgow Interactive Systems
Group (GIST) and to theGlasgow Accident Analysis Group. This work
is supported by the UK Engineering and
Physical Sciences Research Council, grants GR/JO7686, GR/K69148
and GR/K55040.
References
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
21/22
Air Accidents Investigations Branch, Department of Transport.
Report On The Accident
To Boeing 737-400 G-OBME Near Kegworth, Leicestershire on 8th
January 1989,
number 4/90, Her Majesty's Stationery Office. London, United
Kingdom, 1990
J.D. Andrews and T.R. Moss, Reliability and Risk Assessment,
Longman Scientific and
Technical, Harlow, United Kingdom, 1993.
Department of the Environment, Transport and the Regions,
Inquiry into the Fire on a
Heavy Goods Vehicle Shuttle 7539 on 18 November 1996.
D. Busse and C.W. Johnson, Modelling Human Error within a
Cognitive Theoretical
Framework. In F.E. Ritter and R.M. Young (eds.) The Second
European Conference on
Cognitive Modelling, Nottingham University Press, 90-97,
1998.
A. Hale, B. Wilpert and M. Freitag, After the Event: From
Accident to Organisational
Learning, Pergamon Press, New York, United States of America,
1997.
E. Hollnagel, The Phenotype Of Erroneous Actions, International
Journal Of Man-
Machine Studies, 39:1-32, 1993.
C.W. Johnson, Decision Theory And Safety-Critical Interfaces. In
K. Nordby, P.H.
Helmersen, D. Gilmore and S. A. Arnesen (eds.), Interact '95,
Chapman and Hall,
London, United Kingdom, 127-132, 1995.
J. Leplat. Accidents and Incidents Production: Methods of
Analysis. In J. Rasmussen, K.
Duncan and J. Leplat (eds.), New Technology and Human Error.
John Wiley and Sons
Ltd, 1987.
L. Love and C.W. Johnson, Using Diagrams to Support the Analysis
of System 'Failure'
and Operator 'Error'. In H. Thimbleby, B. O'Conaill and P.
Thomas (eds.), People and
Computers XII: Proceedings of HCI'97, Springer Verlag, London,
United Kingdom, 245-
262, 1997.
W. Morehouse and M.A. Subamaniam, The Bhopal Tragedy. Technical
Report. Council
for International and Public Affairs, New York, United States of
America, 1986.
National Transportation Safety Board, Collision and Derailment
of Maryland Rail
Commuter MARC Train 286 and National Railroad Passenger
Corporation AMTRAKTrain 29, Near Silver Spring, Maryland on
February 16, 1996. NTSB Report RAR-97/02.
Washington, United States of America, 1997.
J. Reason,Managing the Risks of Organisational Accidents,
Ashgate, Aldershot, United
Kingdom, 1997.
-
7/28/2019 Visualizing the Relationship Between Human Error and
Organizational Failure
22/22
Sheen, Formal Investigation into the Sinking of the mv Herald of
Free Enterprise, UK
Department of Transport, Report of court 8074, Her Majestys
Stationery Office, 1987.
N. Stanton and I. Glendon, Risk Homeostasis and Risk Assessment,
In the Journal of
Safety Science (22)1-3:1-13, 1996.
W. van Vuuren, C.E. Shea, T.W. van der Schaaf, The Development
of an Incident
Analysis Tool for the Medical Field, Technical Report
EUT/BDK/85, Eindhoven
University of Technology, Faculty of Technology Management,
1997.
D. Woods, Cognitive Demands and Activities in Dynamic Fault
Management, In N.Stanton (ed.), Human Factors of Alarm Design,
Taylor and Francis, London, United
Kingdom, 1994.