Embed Size (px)
Citation preview
Original Article
Vitrectomy without postoperative posturing for idiopathicmacular holesAdrian Rubinstein MRCSEd, Alan Ang FRCOphth and Chetan Kantibhai Patel FRCOphthOxford Eye Hospital, Radcliffe Infirmary, Oxford, UK
ABSTRACT
Purpose: To determine the success of vitrectomy with ILMpeeling and C3F8 tamponade for macular holes without theneed for postoperative face-down posturing.
Methods: Twenty-four eyes of 24 consecutive patientsundergoing pars plana vitrectomy with indocyanine green-assisted ILM peeling and C3F8 tamponade without proneposturing were included in the study. All patients had followup on 1 day, 2 weeks and 3 months postoperatively. Biomi-croscopy and optical coherence tomography were used toassess macular hole closure at 3 months postoperatively.Snellen visual acuity was compared pre- and postoperatively.
Results: Of the 24 eyes recruited, two (8%) had stage II, 17(71%) had stage III and five (21%) had stage IV macularholes. Nineteen (79%) eyes were phakic and five (21%) eyeswere pseudophakic at the time of surgery.The macular holeshad been present for an average of 7.5 months (range3–18 months). At 3-month follow up, 22/24 (91.6%) holeswere closed. Both of the two holes that failed to close werestage IV macular holes. Preoperative visual acuity rangedfrom 6/18 to 6/60 (mean 6/36). Postoperative visual acuityranged from 6/9 to 6/60 (mean 6/18). Eighteen eyes hadimprovement of visual acuity of at least one line on theSnellen chart, six eyes had no improvement. No eyes hadworse vision postoperatively.
Conclusion: Macular hole surgery without face-down pos-turing provides anatomical and functional results compa-rable to those with prone posturing. Combinedphacovitrectomy is not essential to avoid prone posturing.
Key words: face-down posturing, gas tamponade, macularhole, OCT.
INTRODUCTION
After macular hole surgery, patients are required to postureface down for 7–10 days postoperatively,1–6 which can be adaunting and uncomfortable experience. For those patientsunable to posture prone, either silicone oil tamponade orcombined phacovitrectomy with gas tamponade have beendescribed.4–6 In this paper, we present the results of phakicand pseudophakic patients undergoing vitrectomy with ILMpeeling and gas tamponade with neither postoperative face-down posturing nor combined cataract surgery for macularhole.
METHODS
All patients undergoing non-posturing macular hole surgerybetween 1 April 2005 and 31 March 2006 were identified.Patients were excluded from the study if they had any sig-nificant ocular comorbidity (glaucoma, diabetic retinopathy,previous retinal surgery or age-related macular degenera-tion), previous failed macular hole surgery, secondarymacular holes (trauma, myopia > 5.00D), combined cataractsurgery, or if silicone oil was used during the procedure. Allpatients gave informed consent.
The macular holes were diagnosed clinically by slit-lamp biomicroscopy and in most cases confirmed by opticalcoherence tomography (OCT). Grading of macular holeswere performed according to Gass� classification.7,8 Otherpreoperative data collected included patient demographics,lens status of the eye, estimated duration of symptoms andbest corrected Snellen visual acuity.
Surgery consisted of standard three-port approach usingthe BIOM system. Staining of vitreous with 0.1 mL of filteredtriamcinolone was used to aid identification of a successfulinduction of posterior vitreous detachment. Indocyaninegreen diluted with 5% dextrose at a concentration of 0.1%was used to aid ILM peeling which was performed using
� Correspondence: Dr Chetan Kantibhai Patel, Oxford Eye Hospital, Radcliffe Infirmary, Oxford, UK. Email: [email protected]
Received 31 October 2006; accepted 20 February 2007.
Clinical and Experimental Ophthalmology 2007; 35: 458–461doi: 10.1111/j.1442-9071.2007.01532.x
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists
end-gripping forceps. Eighteen per cent C3F8 gas tamponadewas used in all cases.
Postoperatively, patients were advised to avoid supineposture for 7 days. All patients were reviewed at 2 weeks and3 months postoperatively. OCT was performed at the3-month follow up to confirm postoperative macular holestatus. Primary and secondary outcome measures were ana-tomical closure of the hole and postoperative Snellen visualacuity, respectively.
RESULTS
A total of 24 eyes of 24 consecutive patients with idiopathicmacular holes were included in the study (Table 1). Sixteenpatients (66%) were female with a mean age of 71 years(range 63–79). Among the 24 eyes, two (8%) had stage II, 17(71%) had stage III and five (21%) had stage IV macularholes. The macular holes had been present for an average of7.5 months (range 3–18 months). Nineteen eyes (79%) werephakic and five (21%) eyes were pseudophakic. Surgery wasperformed in 19/24 (79%) eyes by the consultant (CKP), and5/24 (21%) eyes by the fellow (AA).
Twenty-two out of 24 (91.6%) holes were closed at3-month follow up. Both of the two holes that failed to closewere stage IV macular holes, with an estimated duration of7 months for the first, and 9 months for the second. Botheyes were phakic.
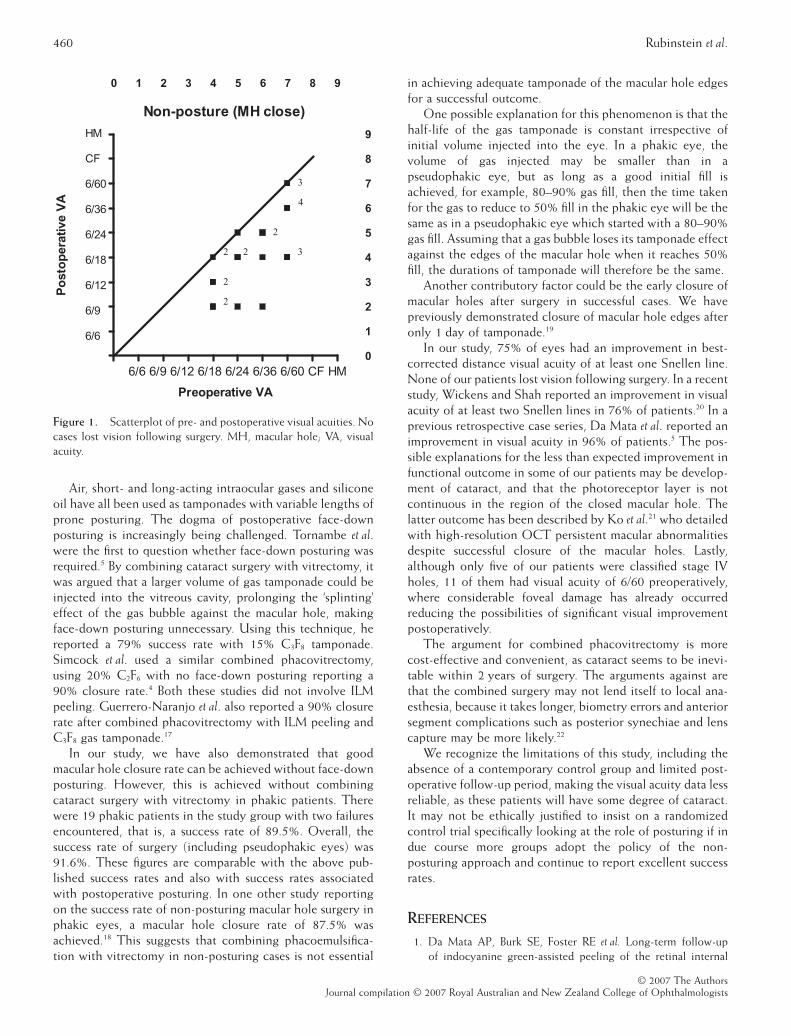
Preoperative visual acuity ranged from 6/18 to 6/60 (mean6/36). Postoperative visual acuity ranged from 6/9 to 6/60(mean 6/18). Eighteen eyes had improvement of visual acuityof at least one line on the Snellen chart, six eyes had noimprovement. No eyes had worse vision postoperatively. Fiveeyes had improvement of at least three Snellen lines (Fig. 1).
Five patients had cataract surgery within 7 months (range6–9 months) following the vitrectomy. Peripheral retinalbreaks were treated with cryotherapy in 8/24 (33%) eyes. Noretinal detachments were observed postoperatively. Three(12.5%) eyes had raised intraocular pressure on day 1postoperatively. Two (8%) eyes had lens touch during theprocedure.
DISCUSSION
Kelly and Wendel published a 58% success rate of holeclosure following peeling of the posterior cortical vitreousfor the treatment of idiopathic full-thickness macular holes.9
Better understanding of the pathogenesis of the disease andmodifications to the original technique, such as peeling ofepiretinal membranes,9 removal of ILM,10 the aid of stains,11
different types of internal tamponades1–13 and adjuvants14,15
have all contributed in improving those results to >90%. Ourgroup reported hole closure rates of 91.2% with the use ofindocyanine green-assisted ILM peeling matching thesuccess rates reported by others.16
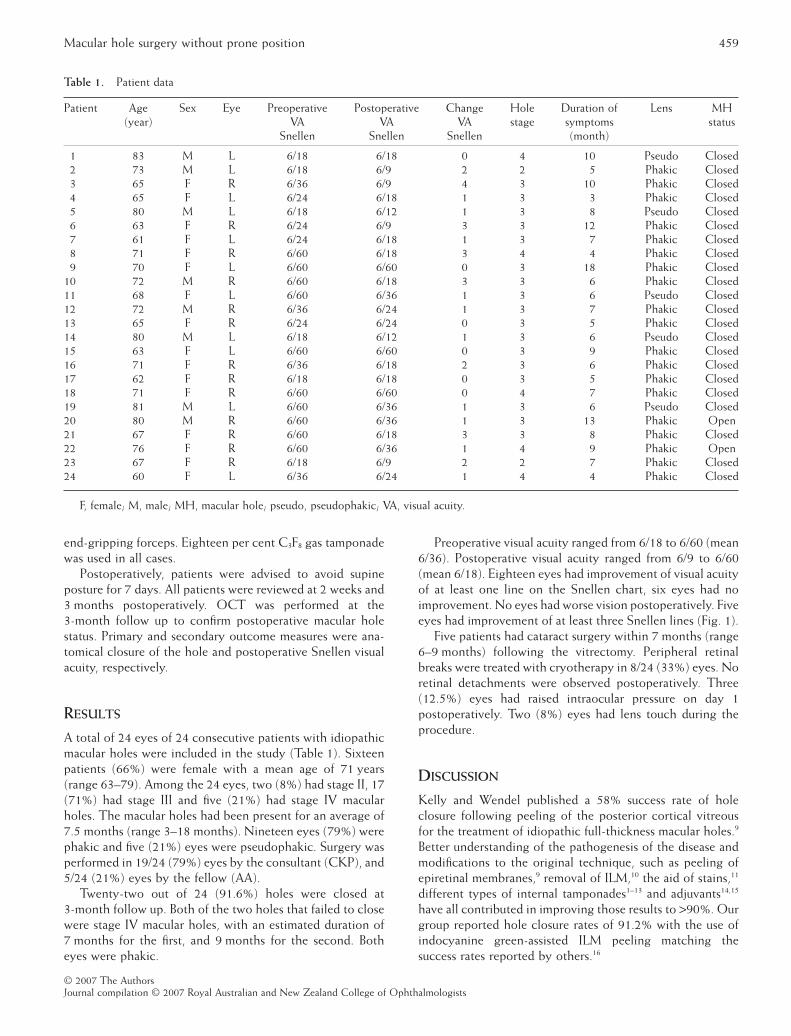
Table 1. Patient data
Patient Age(year)
Sex Eye PreoperativeVA
Snellen
PostoperativeVA
Snellen
ChangeVA
Snellen
Holestage
Duration ofsymptoms(month)
Lens MHstatus
1 83 M L 6/18 6/18 0 4 10 Pseudo Closed2 73 M L 6/18 6/9 2 2 5 Phakic Closed3 65 F R 6/36 6/9 4 3 10 Phakic Closed4 65 F L 6/24 6/18 1 3 3 Phakic Closed5 80 M L 6/18 6/12 1 3 8 Pseudo Closed6 63 F R 6/24 6/9 3 3 12 Phakic Closed7 61 F L 6/24 6/18 1 3 7 Phakic Closed8 71 F R 6/60 6/18 3 4 4 Phakic Closed9 70 F L 6/60 6/60 0 3 18 Phakic Closed
10 72 M R 6/60 6/18 3 3 6 Phakic Closed11 68 F L 6/60 6/36 1 3 6 Pseudo Closed12 72 M R 6/36 6/24 1 3 7 Phakic Closed13 65 F R 6/24 6/24 0 3 5 Phakic Closed14 80 M L 6/18 6/12 1 3 6 Pseudo Closed15 63 F L 6/60 6/60 0 3 9 Phakic Closed16 71 F R 6/36 6/18 2 3 6 Phakic Closed17 62 F R 6/18 6/18 0 3 5 Phakic Closed18 71 F R 6/60 6/60 0 4 7 Phakic Closed19 81 M L 6/60 6/36 1 3 6 Pseudo Closed20 80 M R 6/60 6/36 1 3 13 Phakic Open21 67 F R 6/60 6/18 3 3 8 Phakic Closed22 76 F R 6/60 6/36 1 4 9 Phakic Open23 67 F R 6/18 6/9 2 2 7 Phakic Closed24 60 F L 6/36 6/24 1 4 4 Phakic Closed
F, female; M, male; MH, macular hole; pseudo, pseudophakic; VA, visual acuity.
Macular hole surgery without prone position 459
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists
Air, short- and long-acting intraocular gases and siliconeoil have all been used as tamponades with variable lengths ofprone posturing. The dogma of postoperative face-downposturing is increasingly being challenged. Tornambe et al.were the first to question whether face-down posturing wasrequired.5 By combining cataract surgery with vitrectomy, itwas argued that a larger volume of gas tamponade could beinjected into the vitreous cavity, prolonging the ‘splinting’effect of the gas bubble against the macular hole, makingface-down posturing unnecessary. Using this technique, hereported a 79% success rate with 15% C3F8 tamponade.Simcock et al. used a similar combined phacovitrectomy,using 20% C2F6 with no face-down posturing reporting a90% closure rate.4 Both these studies did not involve ILMpeeling. Guerrero-Naranjo et al. also reported a 90% closurerate after combined phacovitrectomy with ILM peeling andC3F8 gas tamponade.17
In our study, we have also demonstrated that goodmacular hole closure rate can be achieved without face-downposturing. However, this is achieved without combiningcataract surgery with vitrectomy in phakic patients. Therewere 19 phakic patients in the study group with two failuresencountered, that is, a success rate of 89.5%. Overall, thesuccess rate of surgery (including pseudophakic eyes) was91.6%. These figures are comparable with the above pub-lished success rates and also with success rates associatedwith postoperative posturing. In one other study reportingon the success rate of non-posturing macular hole surgery inphakic eyes, a macular hole closure rate of 87.5% wasachieved.18 This suggests that combining phacoemulsifica-tion with vitrectomy in non-posturing cases is not essential
in achieving adequate tamponade of the macular hole edgesfor a successful outcome.
One possible explanation for this phenomenon is that thehalf-life of the gas tamponade is constant irrespective ofinitial volume injected into the eye. In a phakic eye, thevolume of gas injected may be smaller than in apseudophakic eye, but as long as a good initial fill isachieved, for example, 80–90% gas fill, then the time takenfor the gas to reduce to 50% fill in the phakic eye will be thesame as in a pseudophakic eye which started with a 80–90%gas fill. Assuming that a gas bubble loses its tamponade effectagainst the edges of the macular hole when it reaches 50%fill, the durations of tamponade will therefore be the same.
Another contributory factor could be the early closure ofmacular holes after surgery in successful cases. We havepreviously demonstrated closure of macular hole edges afteronly 1 day of tamponade.19
In our study, 75% of eyes had an improvement in best-corrected distance visual acuity of at least one Snellen line.None of our patients lost vision following surgery. In a recentstudy, Wickens and Shah reported an improvement in visualacuity of at least two Snellen lines in 76% of patients.20 In aprevious retrospective case series, Da Mata et al. reported animprovement in visual acuity in 96% of patients.5 The pos-sible explanations for the less than expected improvement infunctional outcome in some of our patients may be develop-ment of cataract, and that the photoreceptor layer is notcontinuous in the region of the closed macular hole. Thelatter outcome has been described by Ko et al.21 who detailedwith high-resolution OCT persistent macular abnormalitiesdespite successful closure of the macular holes. Lastly,although only five of our patients were classified stage IVholes, 11 of them had visual acuity of 6/60 preoperatively,where considerable foveal damage has already occurredreducing the possibilities of significant visual improvementpostoperatively.
The argument for combined phacovitrectomy is morecost-effective and convenient, as cataract seems to be inevi-table within 2 years of surgery. The arguments against arethat the combined surgery may not lend itself to local ana-esthesia, because it takes longer, biometry errors and anteriorsegment complications such as posterior synechiae and lenscapture may be more likely.22
We recognize the limitations of this study, including theabsence of a contemporary control group and limited post-operative follow-up period, making the visual acuity data lessreliable, as these patients will have some degree of cataract.It may not be ethically justified to insist on a randomizedcontrol trial specifically looking at the role of posturing if indue course more groups adopt the policy of the non-posturing approach and continue to report excellent successrates.
REFERENCES
1. Da Mata AP, Burk SE, Foster RE et al. Long-term follow-upof indocyanine green-assisted peeling of the retinal internal
Non-posture (MH close)
0 1 2 3 4 5 6 7 8 9
0
1
2
3
4
5
6
7
8
9
6/6 6/9 6/12 6/18 6/24 6/36 6/60 CF HM
HM
CF
6/60
6/36
6/24
6/18
6/12
6/9
6/6
Preoperative VA
Po
sto
per
ativ
e V
A
2 2
3
3
2
2
2
4
Figure 1. Scatterplot of pre- and postoperative visual acuities. Nocases lost vision following surgery. MH, macular hole; VA, visualacuity.
460 Rubinstein et al.
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists

limiting membrane during vitrectomy surgery for idiopathicmacular hole repair. Ophthalmology 2004; 111: 2246–53.
2. Benson WE, Cruickshanks KC, Fong DS et al. Surgical manage-ment of macular holes: a report by the American Academy ofOphthalmology. Ophthalmology 2001; 108: 1328–35.
3. Johnson MW. Improvements in the understanding and treat-ment of macular hole. Curr Opin Ophthalmol 2002; 13: 152–60.
4. Simcock PR, Scalia S. Phacovitrectomy without prone posturefor full thickness macular holes. Br J Ophthalmol 2001; 85:1316–9.
5. Tornambe PE, Poliner LS, Grote K. Macular hole surgerywithout face-down positioning. A pilot study. Retina 1997; 17:179–85.
6. Thompson JT, Smiddy WE, Glaser BM, Sjaarda RN, Flynn HWJr. Intraocular tamponade duration and success of macular holesurgery. Retina 1996; 16: 373–82.
7. Gass JDM. Idiopathic senile macular holes: its stages andpathogenesis. Arch Ophthalmol 1988; 106: 629–39.
8. Gass JDM. Reappraisal of biomicroscopic classification ofstages of development of a macular hole. Am J Ophthalmol 1995;119: 752–9.
9. Kelly NE, Wendell RT. Vitreous surgery for idiopathic macularholes: results of a pilot study. Arch Ophthalmol 1991; 109:654–9.
10. Brooks HL Jr. Macular hole surgery with and without internallimiting membrane peeling. Ophthalmology 2000; 107: 1939–49.
11. Lee KL, Dean S, Guest S. A comparison of outcomes afterindocyanine green and trypan blue assisted internal limitingmembrane peeling during macular hole surgery. Br J Ophthalmol2005; 89: 420–4.
12. Goldbaum MH, McCuen BW, Hanneken AM, Burgess SK,Chen HH. Silicone oil tamponade to seal macular holes withoutposition restrictions. Ophthalmology 1998; 105: 2140–8.
13. Smiddy WE, Pimentel S, Williams GA. Macular hole surgerywithout using adjunctive additives. Ophthalmic Surg Lasers 1997;28: 713–7.
14. Paques M, Chastang C, Mathis A et al. Effect of autologousplatelet concentrate in surgery for idiopathic macular hole:results of a multicenter, double-masked, randomized trial.Platelets in Macular Hole Surgery Group. Ophthalmology 1999;106: 932–8.
15. Hoerauf H, Kluter H, Joachimmeyer E et al. Results ofvitrectomy and the no-touch-technique using autologousadjuvants in macular hole treatment. Int Ophthalmol 2001; 24:151–9.
16. Lochhead J, Jones E, Chui D et al. Outcome of ICG-assistedILM peel in macular hole surgery. Eye 2004; 18: 804–8.
17. Guerrero-Naranjo JL, Cortes-Luna C, Morales-Canton V et al.[Macular hole surgery without postoperatory <<face>> downpositioning. Pilot study]. Arch Soc Esp Oftalmol 2006; 81: 321–6.
18. Tranos PG, Peter NM, Nath R et al. Macular hole surgerywithout prone posturing. Eye advanced online publication, 31March 2006. doi:10.1038/sj.eye.6702339.
19. Satchi K, Patel CK. Posterior chamber compartments demon-strated by optical coherence tomography, in silicone-filledeyes, following macular hole surgery. Clin Experiment Ophthalmol2005; 33: 619–22.
20. Wickens JC, Shah GK. Outcomes of macular hole surgeryand the shortened face down positioning. Retina 2006; 26:902–4.
21. Ko TH, Witkin AJ, Fujimoto JG et al. Ultrahigh-resolutionoptical coherence tomography of surgically closed macularholes. Arch Ophthalmol 2006; 124: 827–36.
22. Rahman R, Rosen P. Pupillary capture after combined manage-ment of cataract and vitreretinal pathology. J Cataract RefractSurg 2002; 28: 1607–12.
Macular hole surgery without prone position 461
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists





























