Embed Size (px)
Citation preview
JANUARY/FEBRUARY 2019Volume 19, Issue 1
A Vertical Health, LLC publication | PracticalPainManagement.com
Also in this Issue• Why Pain Catastrophizing Matters
• Vibration for Various Pain Conditions • Explaining Opioid-Induced Hyperalgesia
• Get Patients to Do Home Exercises
AN EXPERTS’ ROUNDTABLE
FAST FORWARDWHAT PAIN CARE MAY LOOK LIKE
IN THE FUTURE
FAST FORWARDWHAT PAIN CARE MAY LOOK LIKE
IN THE FUTURE
JANUARY/FEBRUARY 2019Volume 19, Issue 1
A Vertical Health, LLC publication | PracticalPainManagement.com
Also in this Issue• Why Pain Catastrophizing Matters
• Vibration for Various Pain Conditions • Explaining Opioid-Induced Hyperalgesia
• Get Patients to Do Home Exercises
AN EXPERTS’ ROUNDTABLE
FAST FORWARDWHAT PAIN CARE MAY LOOK LIKE
IN THE FUTURE
FAST FORWARDWHAT PAIN CARE MAY LOOK LIKE
IN THE FUTURE
media kit 2020
JUNE 2019Volume 19, Issue 4
Also in this Issue
NGF Antagonists: Game-Changing Agents?
The Data Behind Gabapentinoid Abuse
Provider Perspectives on the Inter-Agency Task Force Report
MIGRAINE
REFRACTORYHEADACHE &
AN HCP GUIDE TO DIAGNOSIS AND CARE
A Vertical Health, LLC publication | PracticalPainManagement.com
JUNE 2019Volume 19, Issue 4
Also in this Issue
NGF Antagonists: Game-Changing Agents?
The Data Behind Gabapentinoid Abuse
Provider Perspectives on the Inter-Agency Task Force Report
MIGRAINE
REFRACTORYHEADACHE &
AN HCP GUIDE TO DIAGNOSIS AND CARE
A Vertical Health, LLC publication | PracticalPainManagement.com
SPINE, SHOULDER& NECK PAIN cases in treatment cases in treatment
SPINE, SHOULDER& NECK PAIN
JULY/AUGUST 2019Volume 19, Issue 5
Also in this Issue
IV Formulations of the Future
Talking to Patients about Stress
False Positives in UDM Screens
Can I Call Myself a Pain Specialist?
A Remedy Health Media, LLC publication | PracticalPainManagement.com
SPINE, SHOULDER& NECK PAIN cases in treatment cases in treatment
SPINE, SHOULDER& NECK PAIN
JULY/AUGUST 2019Volume 19, Issue 5
Also in this Issue
IV Formulations of the Future
Talking to Patients about Stress
False Positives in UDM Screens
Can I Call Myself a Pain Specialist?
A Remedy Health Media, LLC publication | PracticalPainManagement.com
practicalpainmanagement.com
practicalpainmanagement.com
overview
For 20 years, Practical Pain Management has provided evidence-based strategies for the treatment of chronic pain to both healthcare professionals and patients in an easy-to-digest practical format.
Online: PracticalPainManagement.com (PPM) offers its professional audience case reports, research insights, medical meeting highlights, and in-depth analysis of key pain care topics. It serves as a critical resource for a variety of physician specialties looking for practical advice to help patients manage challenging, painful conditions. The patient focused area of PPM provides must-know information on chronic pain conditions and symptoms, actionable advice on treatment options, and empowering stories of people overcoming pain to live better lives.
At Point-of-Care: The Practical Pain Management print Journal is the nation’s leading teaching journal for practitioners that covers the assessment and treatment of chronic pain. PPM journal articles are written by leading experts and reviewed by an editorial board of highly regarded pain management experts.
practicalpainmanagement.com
reaching professionals and patients
Offering Patients:
• A deep-dive into more than 20 chronic pain conditions
• Doctor-reviewed and trusted condition and treatment centers
• True-life success stories from fellow patients and advocates
• Resources and support through PPM’s SMART Patient Guide series
Offering Healthcare Professionals:
• Strategies for practical applications of new treatments, such as CGRP inhibitors for migraine prevention, disease modifiers for arthritis, and cannabis for overall pain management
• Developments in pain care models, including the role of mental and emotional health
• Advances in pharmacological and non-pharmacological approaches, including drug delivery, devices, and diagnostics
• Field Tips and Retrospective Case Studies that address complex pain conditions, comorbidities, unique patient populations, and assessment strategies
• Frequent updates on regulatory changes, including their impact on practice management
• Meeting coverage from all of the major pain conferences across the U.S.
• Expert-written literature reviews that provide insight into the latest pain research
• Reviewed by a 30-plus multi-specialty, clinician-based Editorial Advisory Board that lends expertise, trust, and authority to all content
Align your Brand with expert pain management content through our professional and patient programs.
Patient Social Communities
OnlinePain Stories &
Solutions eNewsletter
Patient Education Guides
JUNE 2019Volume 19, Issue 4
Also in this Issue
NGF Antagonists: Game-Changing Agents?
The Data Behind Gabapentinoid Abuse
Provider Perspectives on the Inter-Agency Task Force Report
MIGRAINE
REFRACTORYHEADACHE &
AN HCP GUIDE TO DIAGNOSIS AND CARE
A Vertical Health, LLC publication | PracticalPainManagement.com
The Journal
PainScans
Online
Pain Monitor eNewsletter
Pain News for Your Practice View this email in your browser.
For Healthcare Professionals
Join the Conversation
NEUROPLASTICITY
The Potential to Change PainResponseA chat with Joseph Wielgosz, PhD.
View Article
EMGALITY
FDA Approves Lilly’s Galcanezumabfor Episodic Cluster HeadacheWill become the only CGRP antibody to date forthe preventive treatment of the disorder.
View Article
DED
Possible Link Between Dry EyeDisease and MigraineOlder adults of both sexes may be at higher risk.
View Article
This Month's Survey
Take our New Poll
What do you find most challenging about interventional pain Physician Education Guides and Primers
Meeting and Conference Highlights
Professional Social Community
practicalpainmanagement.com
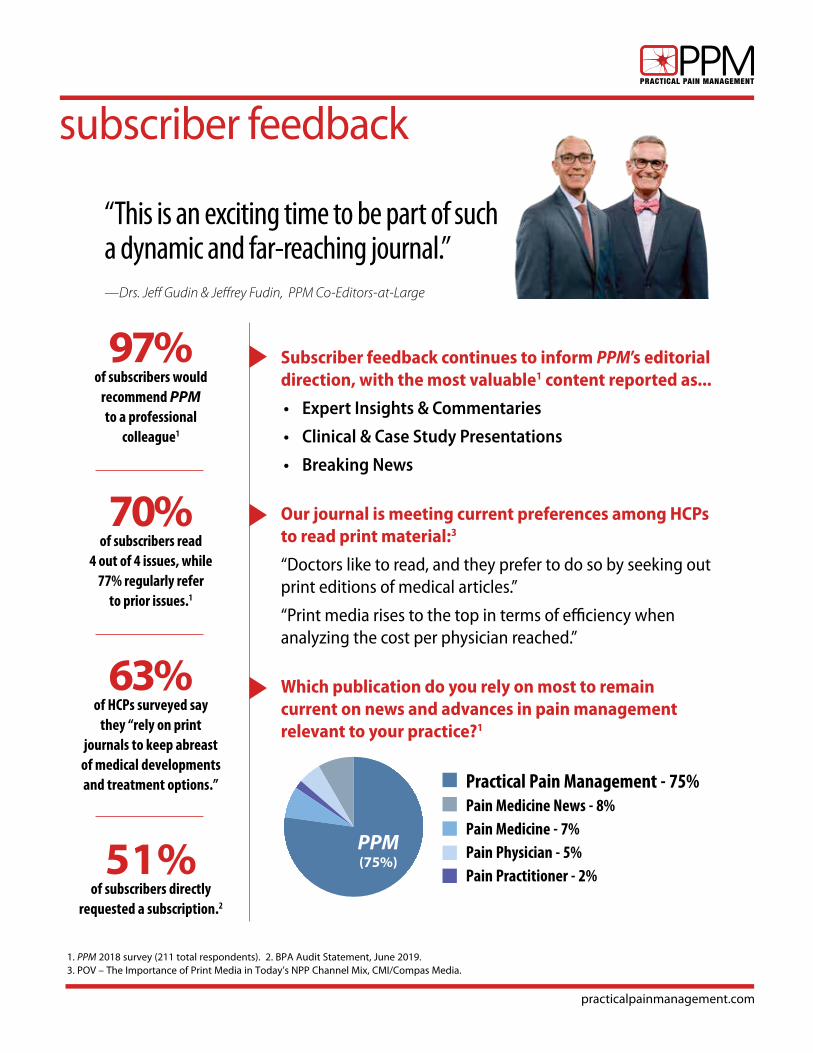
subscriber feedback
“This is an exciting time to be part of such a dynamic and far-reaching journal.”—Drs. Jeff Gudin & Jeffrey Fudin, PPM Co-Editors-at-Large
1. PPM 2018 survey (211 total respondents). 2. BPA Audit Statement, June 2019. 3. POV – The Importance of Print Media in Today’s NPP Channel Mix, CMI/Compas Media.
Practical Pain Management - 75%Pain Medicine News - 8% Pain Medicine - 7% Pain Physician - 5%Pain Practitioner - 2%
PPM(75%)
97% of subscribers would
recommend PPM to a professional
colleague1
70% of subscribers read
4 out of 4 issues, while 77% regularly refer
to prior issues.1
63% of HCPs surveyed say
they “rely on print journals to keep abreast
of medical developments and treatment options.”
51% of subscribers directly
requested a subscription.2
Subscriber feedback continues to inform PPM’s editorial direction, with the most valuable1 content reported as...
• Expert Insights & Commentaries
• Clinical & Case Study Presentations
• Breaking News
Our journal is meeting current preferences among HCPs to read print material:3
“Doctors like to read, and they prefer to do so by seeking out print editions of medical articles.”
“Print media rises to the top in terms of efficiency when analyzing the cost per physician reached.”
Which publication do you rely on most to remain current on news and advances in pain management relevant to your practice?1
practicalpainmanagement.com
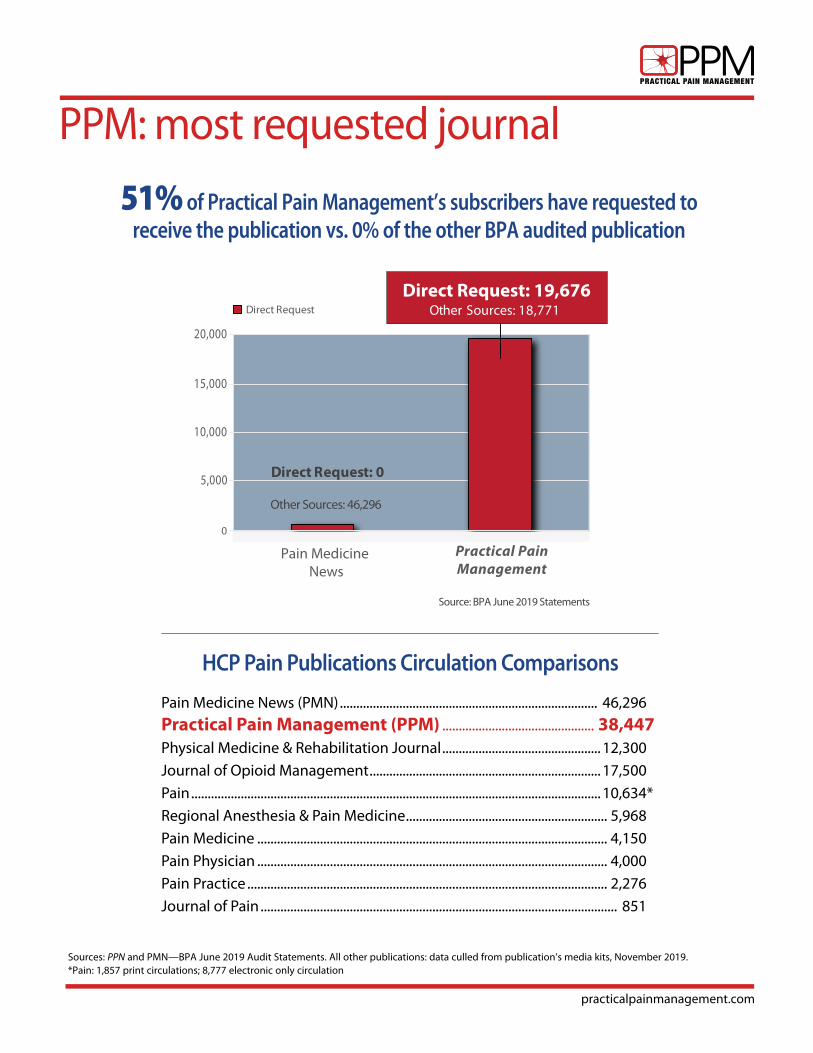
PPM: most requested journal
0
5,000
10,000
15,000
20,000
Pain Medicine News
Practical PainManagement
Direct Request Other Sources: 18,771
Source: BPA June 2019 Statements
Direct Request: 19,676
Direct Request: 0
Other Sources: 46,296
51% of Practical Pain Management’s subscribers have requested to receive the publication vs. 0% of the other BPA audited publication
Sources: PPN and PMN—BPA June 2019 Audit Statements. All other publications: data culled from publication’s media kits, November 2019.*Pain: 1,857 print circulations; 8,777 electronic only circulation
HCP Pain Publications Circulation Comparisons
Pain Medicine News (PMN) .............................................................................. 46,296
Practical Pain Management (PPM) .............................................. 38,447Physical Medicine & Rehabilitation Journal ................................................ 12,300
Journal of Opioid Management ...................................................................... 17,500
Pain ............................................................................................................................ 10,634*
Regional Anesthesia & Pain Medicine ............................................................. 5,968
Pain Medicine .......................................................................................................... 4,150
Pain Physician .......................................................................................................... 4,000
Pain Practice ............................................................................................................. 2,276
Journal of Pain ............................................................................................................ ,851
practicalpainmanagement.com
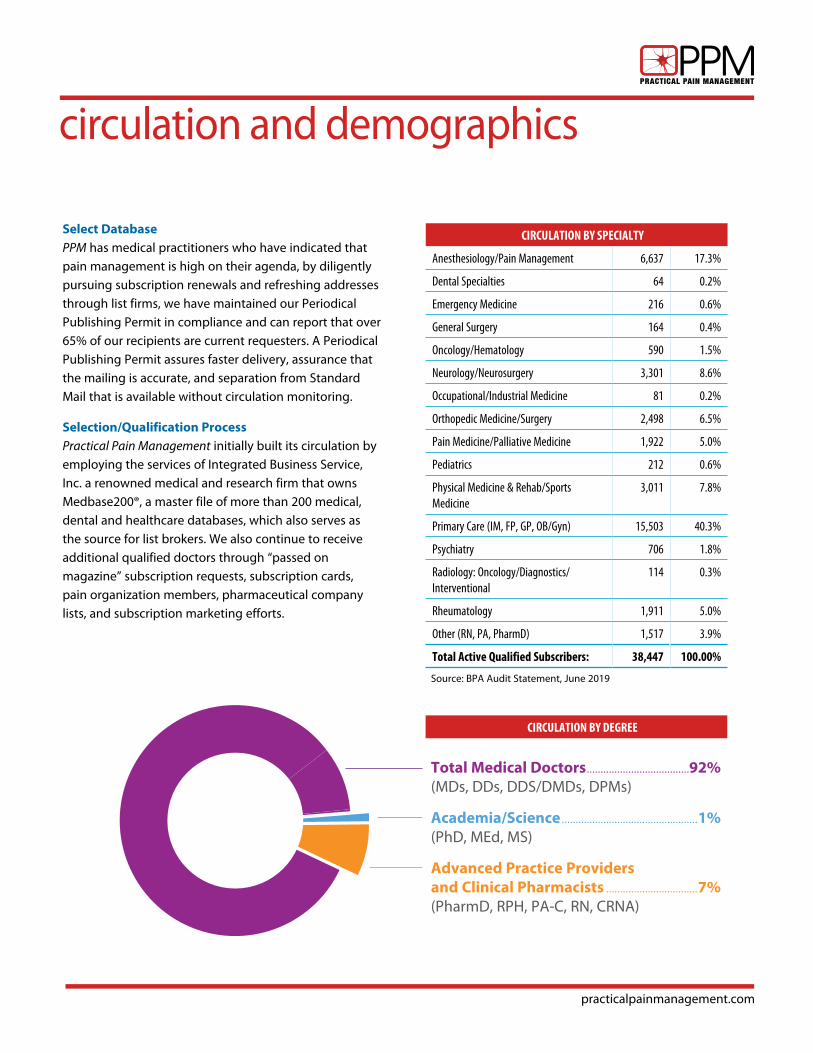
circulation and demographics
Select DatabasePPM has medical practitioners who have indicated that pain management is high on their agenda, by diligently pursuing subscription renewals and refreshing addresses through list firms, we have maintained our Periodical Publishing Permit in compliance and can report that over 65% of our recipients are current requesters. A Periodical Publishing Permit assures faster delivery, assurance that the mailing is accurate, and separation from Standard Mail that is available without circulation monitoring.
Selection/Qualification ProcessPractical Pain Management initially built its circulation by employing the services of Integrated Business Service, Inc. a renowned medical and research firm that owns Medbase200®, a master file of more than 200 medical, dental and healthcare databases, which also serves as the source for list brokers. We also continue to receive additional qualified doctors through “passed on magazine” subscription requests, subscription cards, pain organization members, pharmaceutical company lists, and subscription marketing efforts.
CIRCULATION BY SPECIALTY
Anesthesiology/Pain Management 6,637 17.3%
Dental Specialties 64 0.2%
Emergency Medicine 216 0.6%
General Surgery 164 0.4%
Oncology/Hematology 590 1.5%
Neurology/Neurosurgery 3,301 8.6%
Occupational/Industrial Medicine 81 0.2%
Orthopedic Medicine/Surgery 2,498 6.5%
Pain Medicine/Palliative Medicine 1,922 5.0%
Pediatrics 212 0.6%
Physical Medicine & Rehab/Sports Medicine
3,011 7.8%
Primary Care (IM, FP, GP, OB/Gyn) 15,503 40.3%
Psychiatry 706 1.8%
Radiology: Oncology/Diagnostics/Interventional
114 0.3%
Rheumatology 1,911 5.0%
Other (RN, PA, PharmD) 1,517 3.9%
Total Active Qualified Subscribers: 38,447 100.00%
CIRCULATION BY DEGREE
Total Medical Doctors .....................................92%(MDs, DDs, DDS/DMDs, DPMs)
Academia/Science .................................................1% (PhD, MEd, MS)
Advanced Practice Providers and Clinical Pharmacists .................................7% (PharmD, RPH, PA-C, RN, CRNA)
Source: BPA Audit Statement, June 2019

practicalpainmanagement.com
2020 edit calendar & due datesMONTH SPECIAL REPORT CASE STUDIES & CORE TOPICS
MEETING/ BONUS DISTRIBUTION
MEETING HIGHLIGHTS
AD CLOSEAD MATERIAL
DEADLINE
JANUARY/FEBRUARY
Mails 2/4
The Obesity Factor in Pain Care
• Sickle Cell Crisis• Cancer-Related Pain• Phantom-Limb Pain
American Academy of Pain Medicine (AAPM) Feb 26-March 1, National Harbor
ACR 2019 1/10 1/17
MARCH/APRIL
Mails 4/2
Low Back Pain: Finding a Consensus on Treatment
• Migraine: Have the CGRPs Won?
• TMJ, Orofacial Pain• hATTR
American Headache Society (AHS) June 4-7, San Diego
AAPM 3/6 3/13
MAY/JUNE
Mails 6/2
Complicated Pain Disorders: CRPS, MS Fibromyalgia, EDS
• Pelvic Pain and Related Syndromes
• Psychopharmacology
American College of Rheumatology (ACR) TBD
APS 5/8 5/15
SPECIAL ISSUE: JULY/AUGUST
Mails 8/4
The Evolution of Clinical Pain Management: Two Decades of Pain Medicine, Regulation & Transformation
• Biologics as the End-Game: Future Therapeutic Targets
• Emerging Uses for Ketamine, Methadone, Buprenorphine, Cannabinoids
• Pain Prevalence and Changing Populations
PAINWeek Sept. 8-12, Las Vegas
AHS 7/10 7/17
SEPTEMBER/OCTOBER
Mails 10/2
Arthritis & Inflammation Complex Spine Care
• What’s New in Topical and OTC Analgesics
• Polymyalgia Rheumatica• Arachnoiditis and Ankylosing
Spondylitis• Interventional Technique
Advances
• North American Spine Society (NASS) Oct 7-10, San Diego• American Society for
Regional Anesthesia & Pain Medicine (ASRA) Nov. 19-21, Las Vegas
PAINWeek 9/10 9/18
NOVEMBER/DECMEBER
Mails 12/2
Prescribing Considerations for Comorbidities
• Veterans in Pain• Diabetic Neuropathy• Post-Herpetic Neuralgia
NASS
ASRA11/6 11/13
All content is subject to change
Every issue of PPM also includes the following columns: Editorial, Letters to the Editor, News & Research, Ask the Experts, Mental Health, Emerging Drugs/Product Reviews, Tips from the Field, Law & Ethics
ANALGESICS OF THE FUTURE: 2020 COVERAGE Tumor Necrosis Factor (TNF) Inhibitors | Peripheral Kappa Opioid Receptors Agonists TRPV-1 Agonists / Alpha 2 Agonists | Biased Opioid Ligands | Abuse-Deterrent Formulations hATTR & Peripheral Nerve Disease Treatments
ASK THE PHARM-D: 2020 COVERAGE OnabotulinumtoxinA | Benzodiazepines | Topicals | Natural products and vitamins Metabolism factors | Over-the-counter pain options
practicalpainmanagement.com
2020 bonus opportunities
SPECIAL REPORTS & EDUCATION GUIDES
The Evolution of Pain Management As part of the brand’s 20th Anniversary, PPM will publish* a 2020 Special Report, tentatively titled: “Two Decades of Pain Management Evolution: From Diagnosis and Diagnostics, to Disease-Modifying and Preventive Care, to Interventional and Integrated Care.” The report will include a roundtable of pain management experts across disciplines discussing how key tests and therapies have changed since the year 2000. Plus: a look at emerging and novel classes of drugs (eg, CGRP and NGF inhibitors); shifts in the understanding of complex chronic conditions like fibromyalgia and CRPS; and where the pain management community stands with opioid prescribing and monitoring.
Biologics as Analgesics of the Future As the industry seeks opioid alternatives, biologics such as monoclonal antibodies may offer the next turn in the pain management roadmap; this guide will help clinicians navigate. Content will discuss recent research and discoveries around pain pathways, including the expression of specific proteins and their role in inflammation and chronic pain. Reviews and case studies will report on best practice for managing chronic pain conditions, ranging from low back pain and migraine to osteo- and rheumatoid arthritis. New classes of game-changing, disease-modifying, and preventive drugs to be covered will include agents targeting nerve growth factor (NFG), tumor necrosis factor (TNF), and calcitonin gene-related peptide (CGRP).
Risk Mitigation and Integrated CareThis special report will focus on the new dynamic facing HCPs across the country: integrated care. As primary care providers, advanced practice providers, pain specialists, clinical pharmacists, physical therapists, psychologists, and more continue to be bound together in the long-term management of individuals with chronic pain, they must adjust their communication strategies, assess-ment and REMS approaches, as well as their treatment plans. Content will provide tips from the field, expert commentaries, and case studies on maneuvering this evolving landscape, which includes drug monitoring and the management of comorbidities, such as emotional and mental health challenges.
PAINSCANS
HCPs can get a quick grasp on popular—and sometimes controversial—pain management topics through our PainScans. These literature reviews dig deep into existing case reports and surveys to cull out the practical take-aways for practicing clinicians while also providing expert commentary on the subject at hand. PainScans are written by KOLs and are available on the PPM site.
PAIN MONITOR
PPM’s twice-weekly HCP newsletter features breaking news and research insights, including practical takeaways and commentary from our board members and other pain management experts. In addition, online exclusives from our PPM Journal and results from our clinical-reader polls are featured.

practicalpainmanagement.com
specialized columns*
Analgesics of the Future What’s next in pain medicine approaches? From novel drug classes to improved drug delivery systems, this column digs into Phase 2 and 3 trial data to highlight new and emerging products in both the pharma and non-pharmacologic space. Launched in 2019, Analgesics of the Future covered glial-cell modulators, nerve growth factor antagonists, cannabinoids, IV formulations, dermatological patches, microtablets, and more. In 2020, look for:
• Tumor Necrosis Factor (TNF) Inhibitors
• Peripheral Kappa Opioid Receptors Agonists
• TRPV-1 Agonists
• Alpha 2 Agonists
• Biased Opioid Ligands
• IR Abuse-Deterrent Opioids
• hATTR & Peripheral Nerve Disease Treatments
Reported by clinical research pharmacists, each column includes a discussion-based review and star rating by PPM’s Editors-at-Large.
Ask the APPThere’s no doubt that advanced practice providers (e.g., APRNs, NPs, PAs) continue to grow as crucial players in acute and chronic pain management, from monitoring multimodal analgesia plans to optimizing interdisciplinary teams to leading in palliative care. This expert column addresses key questions and challenges faced by the advanced pain management community, such as how manage a new high-dose patient, training consideration, and integrating into the interdisciplinary team model.
Written by Theresa Mallick-Searle, MS, RN-BC, ANP-BC, a nurse practitioner in the Division of Pain Medicine at Stanford Health Care in California. Mallick-Searle is a CO*OR REMS Education faculty member with the Nurse Practitioner Healthcare Foundation and a Master Faculty member of Advanced Pharmacology with the American Society for Pain Management Nursing. She is the 2019 receipient of Point of Care Network Top Nurse Practitioners.
5555
OverviewNew insights into the pathophysiology of pain have given rise to novel targets for addressing chronic pain. Advancements in clinical research on the role of nerve growth factors (NGFs) in pain conditions has led to the development of anti-NGF monoclonal antibodies (mAbs) that have the potential to specifically target pain at the cellular transcriptional level. Studies have shown that NGF protein expression is typically increased at sites of inflamma-tion and we now understand it plays a role in nociceptor sensitization.1,2 NGF is a neutrophin with a high binding affinity to the tropomyosin-related kinase (trk) family of receptors and low-binding affin-ity to p75 receptors, both playing import-ant roles in the growth and function of sensory neurons.1-4 The binding of NGF to trk-A in particular, activates the down-stream expression of key proteins involved in pain sensitization. By preventing NGF binding to TrKA and p75, mAbs can in-hibit downstream signaling pathways that lead to pain-related hypersensitivity.1,3-4
The first humanized immunoglobulin G2 NGF antibody to be developed was
Inside the Potential of Nerve Growth Factor Antagonists
Image: Shutterstock
Reported by M. Tatjana A. Ramos, PharmD, MPH, and Timothy J. Atkinson, PharmD, BCPS, CPE, with a review by PPM’s Editors-at-Large.
Analgesics of the
Future
New Biological Entities: Anti-nerve growth factor (NGF) monoclonal antibodies (mAbs) have the potential to target pain at the cellular transcriptional level. Since NGF protein expression is typically increased at sites of inflammation and plays a role in nociceptor sensitization, researchers have found that by preventing NGF binding to TrKA and p75, mAbs may inhibit the downstream signaling pathways that lead to pain-related hypersensitivity. Potential indication: Treatment of osteoarthritis, chronic low back pain, and cancer pain (due to bone metastases). Products in development: • Tanezumab, available at 2.5 mg and 5 mg every 8 weeks from Pfizer and Eli Lilly and Company has been fast-tracked by FDA for the treatment of osteoarthritis (OA) and moderate-to-severe chronic back pain. • Fasinumab, available at 1 mg and 3 mg every 4 or 8 weeks from Regeneron Pharmaceuticals and Teva Pharmaceutical Industries, is being pursued for the treatment of chronic pain due to hip or knee OA.
Potential market entry: Pfizer and Eli Lilly are in the process of analyzing results from their most recent Phase III trials to determine potential next steps for further development of tanezumab. Regeneron and Teva have only recently completed Phase III studies of fasinumab.
PPM Rating: 3.5 out of 5 stars, see page 57 ★★★★★
Pract icalPainManagement.com | June 2019
5555
OverviewNew insights into the pathophysiology of pain have given rise to novel targets for addressing chronic pain. Advancements in clinical research on the role of nerve growth factors (NGFs) in pain conditions has led to the development of anti-NGF monoclonal antibodies (mAbs) that have the potential to specifically target pain at the cellular transcriptional level. Studies have shown that NGF protein expression is typically increased at sites of inflamma-tion and we now understand it plays a role in nociceptor sensitization.1,2 NGF is a neutrophin with a high binding affinity to the tropomyosin-related kinase (trk) family of receptors and low-binding affin-ity to p75 receptors, both playing import-ant roles in the growth and function of sensory neurons.1-4 The binding of NGF to trk-A in particular, activates the down-stream expression of key proteins involved in pain sensitization. By preventing NGF binding to TrKA and p75, mAbs can in-hibit downstream signaling pathways that lead to pain-related hypersensitivity.1,3-4
The first humanized immunoglobulin G2 NGF antibody to be developed was
Inside the Potential of Nerve Growth Factor Antagonists
Imag
e: S
hutte
rsto
ck
Reported by M. Tatjana A. Ramos, PharmD, MPH, and Timothy J. Atkinson, PharmD, BCPS, CPE, with a review by PPM’s Editors-at-Large.
Analgesics of the
Future
New Biological Entities: Anti-nerve growth factor (NGF) monoclonal antibodies (mAbs) have the potential to target pain at the cellular transcriptional level. Since NGF protein expression is typically increased at sites of inflammation and plays a role in nociceptor sensitization, researchers have found that by preventing NGF binding to TrKA and p75, mAbs may inhibit the downstream signaling pathways that lead to pain-related hypersensitivity. Potential indication: Treatment of osteoarthritis, chronic low back pain, and cancer pain (due to bone metastases). Products in development: • Tanezumab, available at 2.5 mg and 5 mg every 8 weeks from Pfizer and Eli Lilly and Company has been fast-tracked by FDA for the treatment of osteoarthritis (OA) and moderate-to-severe chronic back pain. • Fasinumab, available at 1 mg and 3 mg every 4 or 8 weeks from Regeneron Pharmaceuticals and Teva Pharmaceutical Industries, is being pursued for the treatment of chronic pain due to hip or knee OA.
Potential market entry: Pfizer and Eli Lilly are in the process of analyzing results from their most recent Phase III trials to determine potential next steps for further development of tanezumab. Regeneron and Teva have only recently completed Phase III studies of fasinumab.
PPM Rating: 3.5 out of 5 stars, see page 57 ★★★★★
Pract icalPainManagement.com | June 2019
23
As a nurse practitioner who has focused her career on pain management and seen trends both in outpatient clinics as well as acute care hospitals, I get this question
asked often. Depending on the stakeholder’s point of view, the question may take a different form, but the meaning is the same. Hospital administrators, for example, may focus on the Joint Commission’s indicators for pain assessment and management,1 or the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey concerning communication about pain during a hospital stay.2 Bedside nurses and non-pain specialist clinicians may want to focus on best practices for building interprofessional teams that can meet the pain management needs of their growingly complex patient populations (eg, the homeless, opioid tolerant, addicted, or those with mental health issues).
In the 1990s, names like Betty Ferrell, Chris Pasero, and Christine Miaskowski were touted as the trailblazers in estab-lishing the importance of the pain resource nurse as well as the need for continued training and improved outcomes in pain management.3-5 Cindie Lou Roger, an independent consul-tant at CL Roger Healthcare Consulting in Georgia, shared with me that, in 1996, she created the position of a Pain Management CNS/NP/Practice Specialist at the Gwinnett Hospital System, and just a couple of years later, a formal pain service was created. “I thought the Pain Resource Nurse program created by Betty Ferrell should be implemented in all accredited institutions,” she told me.
The growing regulations and patient complexities in today’s acute care settings have gone beyond what the bedside nurse, pain resource nurse, or medical intern can handle alone. Every healthcare organization should have a dedicated pain manage-ment team—and yes, Advanced Practice Providers, or APPs, can take the lead. Acute Pain Services (APS) are becoming available in many hospitals worldwide because of the numer-ous advantages they hold for patients and healthcare systems. The hope is that, as formalized systems are recognized as best practice and APS are introduced, these changes will lead to a greater appreciation for pain issues and education among all healthcare providers.6 In turn, pain practice will improve.
APP Training: The Skill Sets Are ThereAdvanced Practice Registered Nurses (APRNs) have the skills and training to assess, manage, and create guidelines for pain management. They have, through their specific training, the skills to place and/or manage regional anesthesia, as well as interpersonal skills suited to interprofessional collaboration. Most APRNs have, at some point, spent time taking care of patients at the bedside, worked within complex systems, and participated in systems improvement committees.
Physician Assistants (PAs) typically enter their training with a background in healthcare and have experience with healthcare systems. Through their primary training, they develop the skills and experience to assess and recognize poorly managed pain. Although there are few PA residencies devoted to the specialty of pain management, PAs that participate in residencies that focus on intensive training in specialties such as surgery, trauma, acute care, critical care, and/or emergency medicine,7 develop the skill set to manage the complexities of acute pain in compromised patients.
APPs in ActionBelow are a few examples of best practices already being put into play by APPs in the acute care setting.
Mechele Fillman, NP, Acute Pain Service“I started an acute pain service at Saint Joseph’s Hospital, in Denver, in 2008, because I recognized that surgery patients were experiencing inadequate pain relief with opioids. In some cases, the patients’ pain management was inadequate, and they were experiencing side effects such as over-sedation and respiratory depression, causing them to have a much longer ICU stay. The pain service was started to provide pain relieving and opioid-sparing techniques, such as epidurals and ketamine infusions.
I came to Stanford HealthCare in 2012 and expanded the acute pain service from 1.5 FTEs to 5 FTEs, allowing for 24-hour pain consult coverage. Additionally, during my tenure, we saw the addition of a regional anesthesia service that allows for state-of-the-art multimodal pain management
Advanced Practice Provider Q&A
FOR THE APP
Theresa Mallick-Searle, RN-BC, ANP-BC, of Stanford Health Care’s Division of Pain Medicine, answers this question: Is there value in having an Acute Pain Service, and can APPs take the lead?
Pract icalPainManagement.com | March 2019
23
As a nurse practitioner who has focused her career on pain management and seen trends both in outpatient clinics as well as acute care hospitals, I get this question
asked often. Depending on the stakeholder’s point of view, the question may take a different form, but the meaning is the same. Hospital administrators, for example, may focus on the Joint Commission’s indicators for pain assessment and management,1 or the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey concerning communication about pain during a hospital stay.2 Bedside nurses and non-pain specialist clinicians may want to focus on best practices for building interprofessional teams that can meet the pain management needs of their growingly complex patient populations (eg, the homeless, opioid tolerant, addicted, or those with mental health issues).
In the 1990s, names like Betty Ferrell, Chris Pasero, and Christine Miaskowski were touted as the trailblazers in estab-lishing the importance of the pain resource nurse as well as the need for continued training and improved outcomes in pain management.3-5 Cindie Lou Roger, an independent consul-tant at CL Roger Healthcare Consulting in Georgia, shared with me that, in 1996, she created the position of a Pain Management CNS/NP/Practice Specialist at the Gwinnett Hospital System, and just a couple of years later, a formal pain service was created. “I thought the Pain Resource Nurse program created by Betty Ferrell should be implemented in all accredited institutions,” she told me.
The growing regulations and patient complexities in today’s acute care settings have gone beyond what the bedside nurse, pain resource nurse, or medical intern can handle alone. Every healthcare organization should have a dedicated pain manage-ment team—and yes, Advanced Practice Providers, or APPs, can take the lead. Acute Pain Services (APS) are becoming available in many hospitals worldwide because of the numer-ous advantages they hold for patients and healthcare systems. The hope is that, as formalized systems are recognized as best practice and APS are introduced, these changes will lead to a greater appreciation for pain issues and education among all healthcare providers.6 In turn, pain practice will improve.
APP Training: The Skill Sets Are ThereAdvanced Practice Registered Nurses (APRNs) have the skills and training to assess, manage, and create guidelines for pain management. They have, through their specific training, the skills to place and/or manage regional anesthesia, as well as interpersonal skills suited to interprofessional collaboration. Most APRNs have, at some point, spent time taking care of patients at the bedside, worked within complex systems, and participated in systems improvement committees.
Physician Assistants (PAs) typically enter their training with a background in healthcare and have experience with healthcare systems. Through their primary training, they develop the skills and experience to assess and recognize poorly managed pain. Although there are few PA residencies devoted to the specialty of pain management, PAs that participate in residencies that focus on intensive training in specialties such as surgery, trauma, acute care, critical care, and/or emergency medicine,7 develop the skill set to manage the complexities of acute pain in compromised patients.
APPs in ActionBelow are a few examples of best practices already being put into play by APPs in the acute care setting.
Mechele Fillman, NP, Acute Pain Service“I started an acute pain service at Saint Joseph’s Hospital, in Denver, in 2008, because I recognized that surgery patients were experiencing inadequate pain relief with opioids. In some cases, the patients’ pain management was inadequate, and they were experiencing side effects such as over-sedation and respiratory depression, causing them to have a much longer ICU stay. The pain service was started to provide pain relieving and opioid-sparing techniques, such as epidurals and ketamine infusions.
I came to Stanford HealthCare in 2012 and expanded the acute pain service from 1.5 FTEs to 5 FTEs, allowing for 24-hour pain consult coverage. Additionally, during my tenure, we saw the addition of a regional anesthesia service that allows for state-of-the-art multimodal pain management
Advanced Practice Provider Q&A
FOR THE APP
Theresa Mallick-Searle, RN-BC, ANP-BC, of Stanford Health Care’s Division of Pain Medicine, answers this question: Is there value in having an Acute Pain Service, and can APPs take the lead?
Pract icalPainManagement.com | March 2019
* Subject to change
practicalpainmanagement.com
specialized columns* (continued)
Ask the PharmDTimely questions on the minds of HCPs are addressed through this regular Q&A column. Topics have ranged from false positives on urine drug screens to the abuse potential of gabapentinoids to emerging uses for ketamine.
Led by McKenzie C. Ferguson, PharmD, BCPS, an associate professor in the Pharmacy Practice Drug Information & Wellness Center at Southern Illinois University Edwardsville in Illinois. Dr. Ferguson is a board-certified pharmacotherapy specialist.
Mental & Emotional HealthAs pain management increasingly becomes interdisciplinary and integrated, clinicians need to understand and assess for psychological comorbidities, and in many cases, refer their patients to mental health professionals. This column digs into DSM classifications and offers best practice and program overviews for clinicians managing patients who may be facing stress, anxiety, depression, workplace challenges, malingering, and more.
Written by David Cosio, PhD, ABPP, a psychologist in the Pain Clinic and the CARF-accredited, interdisciplinary pain program at the Jesse Brown VA Medical Center, in Chicago. He holds specialist certification in clinical health psychology from the American Board of Professional Psychology. Dr. Cosio is the author of the recent book, Pain Relief: Managing Chronic Pain Through Traditional, Holistic, & Eastern Practices.
Considerations in Law & Ethics From the latest rules on prescribing to managing the pharmacist-provider relationship, this column takes a detailed look at the current regulations impacting daily pain practice. In addition, the author reviews recently finalized judicial cases to offer lessons learned and forward-thinking for today’s pain practitioners.
Written by Katie Duensing, JD, who previously served as the Academy of Integrative Pain Management’s director of Legislative and Regulatory Affairs. Through her extensive involvement with the development and operation of the State Pain Policy Advocacy Network, the Consumer Pain Advocacy Task Force, and the Integrative Pain Care Policy Congress, Duensing has served as a key connector of state and federal stakeholders in the pain and integrative healthcare spaces.
* Subject to change
In April 2019, in the case of US v. Littleford, a Colora-do physician was sentenced to 87 months in prison for overprescribing opioids that ultimately resulted in the
deaths of at least two patients.1 In just one day in 2012, the physician wrote one single patient prescriptions for 840 tablets of 30-mg oxycodone; 120 tablets of 80-mg oxyco-done; 360 tablets of Percocet (10 mg oxycodone/325 mg acetaminophen); 240 tablets of 100-mg morphine; 240 tablets of 2-mg Klonopin (clonazepam); and 240 tablets of 350-mg Soma (cariso-prodol). The patient’s file contained no docu-mentation of an exam, a diagnosis, or a treat-ment plan. To make matters worse, the patient had disclosed in his intake question-naire that he had pre-viously undergone opi-oid detoxification.
In most aspects, the facts of the Littleford case were egregious and have little to do with typical pain man-agement practitioners. Upon closer reading, however, the case does highlight one major issue that should concern everyone: who qualifies as a pain management specialist?
The Department of Justice (DOJ), in a press release re-garding the case, stated that Littleford “…held himself out as a practitioner in the field of ‘pain management,’ although he did not have any certification in that field and had not completed a medical residency, which would have been di-rectly applicable to the field of pain management.”2 While that may sound like an obvious red flag to an outsider to the field of pain management, those of us with a deeper un-derstanding may feel some unease at the DOJ’s statement.
Pain Specialists are in Short SupplyUnlike other medical specialties, such as pediatrics or cardi-ology, and despite what the DOJ seemingly implied, there are no independent residency training programs for the specialty of pain medicine or pain management.3 The med-ical residency referred to by the DOJ simply does not exist. Board certification in Pain Medicine is available, but a phy-sician must first complete a residency training program in an entirely different specialty, such as anesthesiology, neurology,
neurosurgery, psychi-atry, or physical medi-cine and rehabilitation. Then, prior to obtaining board certification, the physician must either: (1) complete a one-year fellowship in pain medicine; or (2) pro-vide proof of substantial training in pain medi-cine related-topics, and actively practice com-prehensive pain med-icine for a significant amount of time. This onerous path to pain specialization (in addi-
tion to the increasing scrutiny, and resulting fear, that pain practitioners face4,5) has resulted in a severe shortage of pain specialists, with nearly 30,000 Americans living with chronic pain for every one board-certified pain care physician.6
With so few board-certified pain specialists, and so many people living with chronic pain, is board certification really the only way to qualify as a pain specialist? The answer will depend upon the authority that one asks.
State Requirements MatterIf one practices in a state that has adopted laws or rules that govern pain management clinics, the answer may be
Can I Call Myself a “Pain Specialist?”
CONSIDERATIONS IN LAW & ETHICS
by Katie Duensing, JD
Who defines the role of pain specialists? Do you qualify as one, and do the courts agree? Inside the legal requirements.
64 Pract icalPainManagement.com | July/August 2019
In April 2019, in the case of US v. Littleford, a Colora-do physician was sentenced to 87 months in prison for overprescribing opioids that ultimately resulted in the
deaths of at least two patients.1 In just one day in 2012, the physician wrote one single patient prescriptions for 840 tablets of 30-mg oxycodone; 120 tablets of 80-mg oxyco-done; 360 tablets of Percocet (10 mg oxycodone/325 mg acetaminophen); 240 tablets of 100-mg morphine; 240 tablets of 2-mg Klonopin (clonazepam); and 240 tablets of 350-mg Soma (cariso-prodol). The patient’s file contained no docu-mentation of an exam, a diagnosis, or a treat-ment plan. To make matters worse, the patient had disclosed in his intake question-naire that he had pre-viously undergone opi-oid detoxification.
In most aspects, the facts of the Littleford case were egregious and have little to do with typical pain man-agement practitioners. Upon closer reading, however, the case does highlight one major issue that should concern everyone: who qualifies as a pain management specialist?
The Department of Justice (DOJ), in a press release re-garding the case, stated that Littleford “…held himself out as a practitioner in the field of ‘pain management,’ although he did not have any certification in that field and had not completed a medical residency, which would have been di-rectly applicable to the field of pain management.”2 While that may sound like an obvious red flag to an outsider to the field of pain management, those of us with a deeper un-derstanding may feel some unease at the DOJ’s statement.
Pain Specialists are in Short SupplyUnlike other medical specialties, such as pediatrics or cardi-ology, and despite what the DOJ seemingly implied, there are no independent residency training programs for the specialty of pain medicine or pain management.3 The med-ical residency referred to by the DOJ simply does not exist. Board certification in Pain Medicine is available, but a phy-sician must first complete a residency training program in an entirely different specialty, such as anesthesiology, neurology,
neurosurgery, psychi-atry, or physical medi-cine and rehabilitation. Then, prior to obtaining board certification, the physician must either: (1) complete a one-year fellowship in pain medicine; or (2) pro-vide proof of substantial training in pain medi-cine related-topics, and actively practice com-prehensive pain med-icine for a significant amount of time. This onerous path to pain specialization (in addi-
tion to the increasing scrutiny, and resulting fear, that pain practitioners face4,5) has resulted in a severe shortage of pain specialists, with nearly 30,000 Americans living with chronic pain for every one board-certified pain care physician.6
With so few board-certified pain specialists, and so many people living with chronic pain, is board certification really the only way to qualify as a pain specialist? The answer will depend upon the authority that one asks.
State Requirements MatterIf one practices in a state that has adopted laws or rules that govern pain management clinics, the answer may be
Can I Call Myself a “Pain Specialist?”
CONSIDERATIONS IN LAW & ETHICS
by Katie Duensing, JD
Who defines the role of pain specialists? Do you qualify as one, and do the courts agree? Inside the legal requirements.
64 Pract icalPainManagement.com | July/August 2019

practicalpainmanagement.com
editors-at-large
Bob Twillman, PhD The former executive director of the Academy of Integrative Pain Management (AIPM), Dr. Twillman has led national policy and advocacy efforts for the pain management community for 15 years. He maintains a volunteer faculty appointment as clinical associate professor of psychiatry and behavioral sciences at the University of Kansas School of Medicine in Kansas City and served for seven years as chair of the Prescription Monitoring Program Advisory Committee for the Kansas Board of Pharmacy. Dr. Twillman is currently employed as a pain management psychologist at St. Luke’s Health System in Kansas City, MO.
Tina L. Doshi, MD, MHS An assistant professor in the Department of Anesthesiology and Critical Care Medicine, Division of Pain Medicine, at Johns Hopkins University School of Medicine in Baltimore in Maryland, Dr. Doshi has been involved in a number of clinical trials for the treatment of neuropathic pain. She is the recipient of multiple research grants, from sponsors including the National Institutes of Health, and is a founding member and chair of the Women in Regional Anesthesia and Pain Medicine (WRAPM) Special Interest Group of the American Society for Regional Anesthesia and Pain Medicine.
Helen N. Turner, DNP, RN-BC, PCNS-BC Turner is a clinical nurse specialist and associate professor within the Pediatric Pain Management Center, Anesthesiology & Peri-Operative Medicine Department at Doernbecher Children’s Hospital/Oregon Health & Science University in Portland. In 2014-15, Turner served as President of the American Society for Pain Management Nursing (ASPMN).
Anita Gupta, DO, PharmD, MPP, National Academies of Science’s Global Forum
Beth Seickel, RN, Reflex Sympathetic Dystrophy Syndrome Association
Jaime Sanders, Coalition For Headache and Migraine Patients, The Headache & Migraine Policy Forum
Richard Lawhern, PhD, Alliance for the Treatment of Intractable Pain
Jeff Gudin, MD
An attending physician in the Department of Anesthesiology at Englewood Hospital and Medical Center in New Jersey, Dr. Gudin also serves as an associate clinical professor of anesthesiology at Rutgers-NJ School of Medicine. He is board-certified in pain medicine, anesthesiology, addiction medicine, and hospice/palliative medicine, and is a medical acupuncturist. Dr. Gudin’s clinical and research focus includes: novel non-opioid analgesics, post-operative pain management, opioid abuse and potential solutions, and increasing clinician awareness of pain assessment and risk management.
Jeffrey Fudin, PharmD, DAIPM, FCCP, FASHP, FFSM
A clinical pharmacy specialist in pain management at the Stratton VA Medical Center in Albany, NY, Dr. Fudin is also the CEO and founder of Remitigate, LLC, a software development company with a focus on opioid safety. He serves as an adjunct associate professor at Western New England University College of Pharmacy, and at the Albany College of Pharmacy and Health Sciences. He founded the ACCP Pain Pharmacy Practice Network group, and as a peer reviewer, has helped to establish several clinical practice guidelines, including for arthritis, fibromyalgia, and chronic non-cancer pain, as well as for urine drug monitoring and opioid-induced constipation.
NEWEST BOARD MEMBERS
NEW PATIENT ADVOCATES
practicalpainmanagement.com
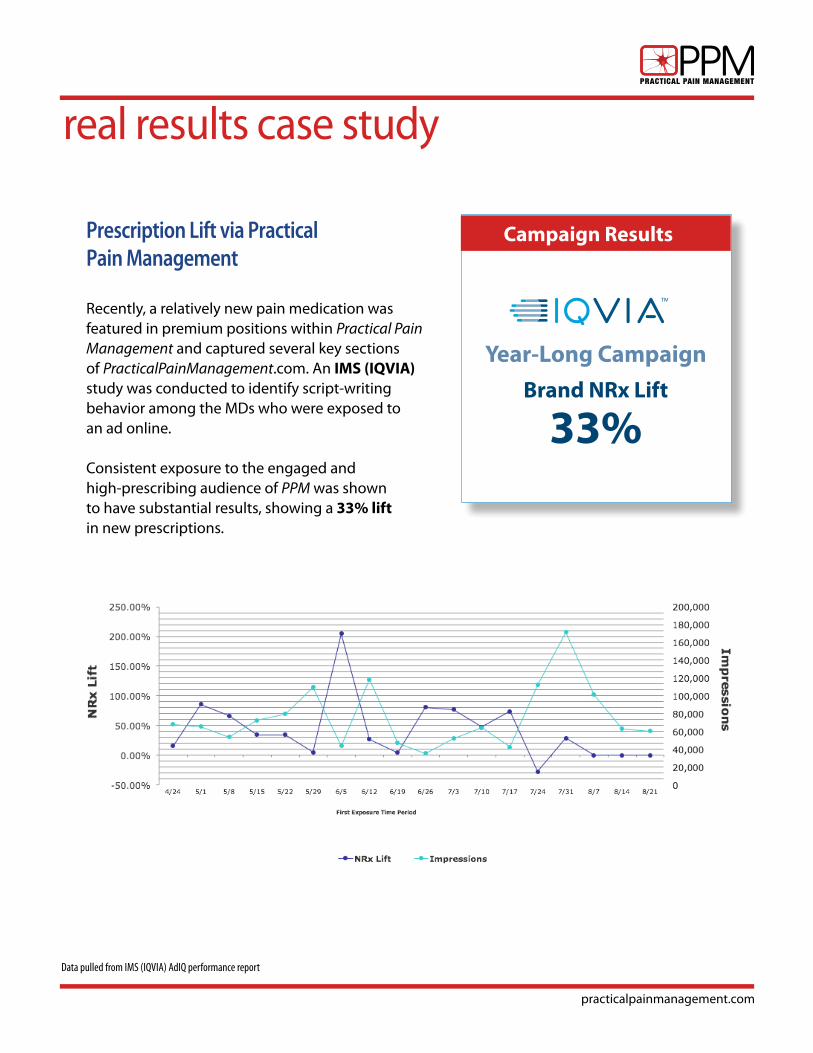
real results case study
Data pulled from IMS (IQVIA) AdIQ performance report
Prescription Lift via Practical Pain Management Recently, a relatively new pain medication was featured in premium positions within Practical Pain Management and captured several key sections of PracticalPainManagement.com. An IMS (IQVIA) study was conducted to identify script-writing behavior among the MDs who were exposed to an ad online. Consistent exposure to the engaged and high-prescribing audience of PPM was shown to have substantial results, showing a 33% lift in new prescriptions.
Brand NRx Lift
33%
Year-Long Campaign
Campaign Results
practicalpainmanagement.com
advertising & marketing tactics
Print:
1. Standard and custom print advertising in PPM, including; Outserts, Inserts, Cover Tips, Advertorials
2. Sponsorship of 2020 Special Edition a. Special Edition is mailed to PPM subscribers with bonus distribution at specific conferences/meetings b. Optional patient-focused educational piece(s) c. Extended reach-with integrated digital component(s)
3. Custom Direct Mail leveraging the PPM brand
Digital: Organic search traffic on PPM.com has increased 78% over last 12 months!
1. HCP List-Match Banner campaigns focused on PPM and run across Remedy Health Media portfolio of websites. ROS banners on:
• PracticalPainManagement.com
• OpioidCalculator.PracticalPainManagement.com
• OpioidTapering.PracticalPainManagement.com
2. Meeting Highlights: providing real-time and post-meeting updates from key industry events. For HCPs at the event, and especially for those not at the event, PPM will report on some of the most important topics and provide additional commentary from top KOLs. See examples at: practicalpainmanagement.com/meetings.
3. Patient Guides (DTC) & Best-Practice Professional Guides (HCP): Targeting DTC and/or HCP audiences with original and educational content in various mediums. See details on page 8 herein.
4. PainScan: a deep dive on a particular topic where top KOLs synthesize the most recent literature and offer 6 to 8 relevant and informative, yet more digestible, articles. See examples at: practicalpainmanagement.com/painscan.
5. Branded/Unbranded custom Resource Centers, which may include:
Videos, Research Opportunities, Articles (native and/or editorial), etc.
6. Custom email sends to PPM database and eNewsletter sponsorship to ~30K PPM HCP audience.
7. Market research from HCPs treating a myriad of conditions from migraine to RA to breakthrough cancer pain and more.
8. DTC advertising across portfolio of pain-focused patient sites including migraine, RA, OA and more.
practicalpainmanagement.com
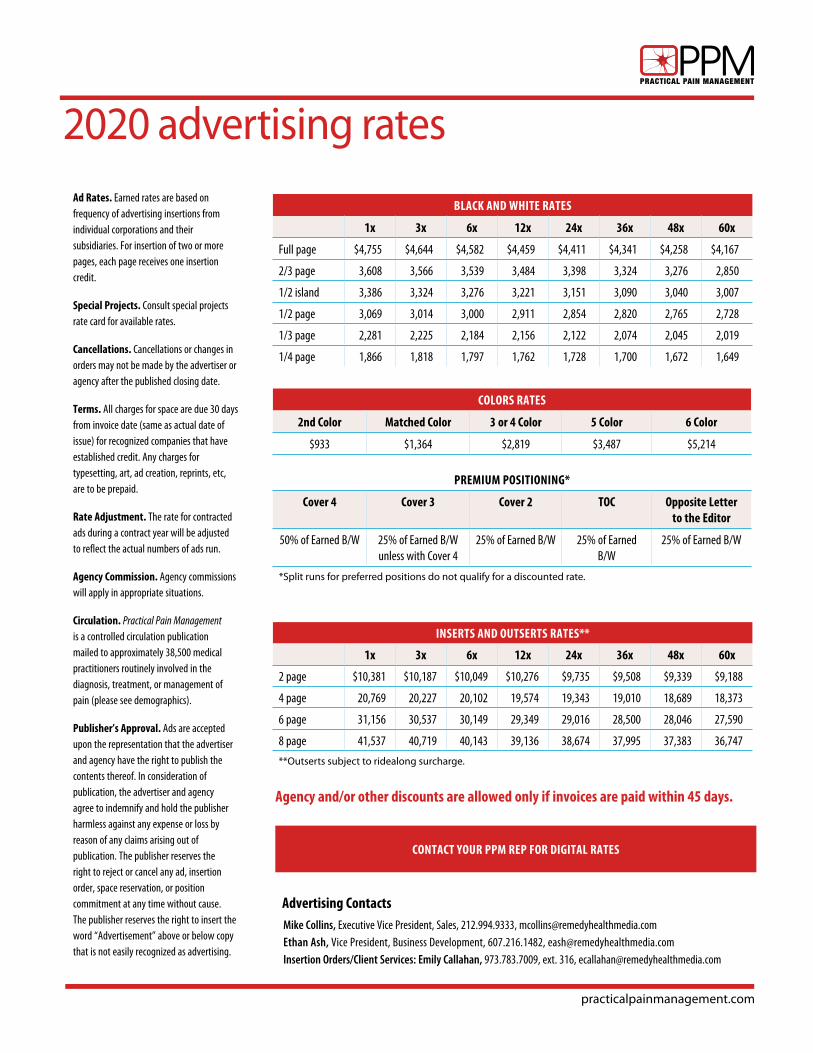
2020 advertising rates
BLACK AND WHITE RATES
1x 3x 6x 12x 24x 36x 48x 60x
Full page $4,755 $4,644 $4,582 $4,459 $4,411 $4,341 $4,258 $4,167
2/3 page 3,608 3,566 3,539 3,484 3,398 3,324 3,276 2,850
1/2 island 3,386 3,324 3,276 3,221 3,151 3,090 3,040 3,007
1/2 page 3,069 3,014 3,000 2,911 2,854 2,820 2,765 2,728
1/3 page 2,281 2,225 2,184 2,156 2,122 2,074 2,045 2,019
1/4 page 1,866 1,818 1,797 1,762 1,728 1,700 1,672 1,649
COLORS RATES
2nd Color Matched Color 3 or 4 Color 5 Color 6 Color
$933 $1,364 $2,819 $3,487 $5,214
PREMIUM POSITIONING*
Cover 4 Cover 3 Cover 2 TOC Opposite Letter to the Editor
50% of Earned B/W 25% of Earned B/W unless with Cover 4
25% of Earned B/W 25% of Earned B/W
25% of Earned B/W
*Split runs for preferred positions do not qualify for a discounted rate.
INSERTS AND OUTSERTS RATES**
1x 3x 6x 12x 24x 36x 48x 60x
2 page $10,381 $10,187 $10,049 $10,276 $9,735 $9,508 $9,339 $9,188
4 page 20,769 20,227 20,102 19,574 19,343 19,010 18,689 18,373
6 page 31,156 30,537 30,149 29,349 29,016 28,500 28,046 27,590
8 page 41,537 40,719 40,143 39,136 38,674 37,995 37,383 36,747
**Outserts subject to ridealong surcharge.
CONTACT YOUR PPM REP FOR DIGITAL RATES
Ad Rates. Earned rates are based on frequency of advertising insertions from individual corporations and their subsidiaries. For insertion of two or more pages, each page receives one insertion credit.
Special Projects. Consult special projects rate card for available rates.
Cancellations. Cancellations or changes in orders may not be made by the advertiser or agency after the published closing date.
Terms. All charges for space are due 30 days from invoice date (same as actual date of issue) for recognized companies that have established credit. Any charges for typesetting, art, ad creation, reprints, etc, are to be prepaid.
Rate Adjustment. The rate for contracted ads during a contract year will be adjusted to reflect the actual numbers of ads run.
Agency Commission. Agency commissions will apply in appropriate situations.
Circulation. Practical Pain Management is a controlled circulation publication mailed to approximately 38,500 medical practitioners routinely involved in the diagnosis, treatment, or management of pain (please see demographics).
Publisher’s Approval. Ads are accepted upon the representation that the advertiser and agency have the right to publish the contents thereof. In consideration of publication, the advertiser and agency agree to indemnify and hold the publisher harmless against any expense or loss by reason of any claims arising out of publication. The publisher reserves the right to reject or cancel any ad, insertion order, space reservation, or position commitment at any time without cause. The publisher reserves the right to insert the word “Advertisement” above or below copy that is not easily recognized as advertising.
Mike Collins, Executive Vice President, Sales, 212.994.9333, [email protected] Ash, Vice President, Business Development, 607.216.1482, [email protected] Insertion Orders/Client Services: Emily Callahan, 973.783.7009, ext. 316, [email protected]
Advertising Contacts
Agency and/or other discounts are allowed only if invoices are paid within 45 days.
practicalpainmanagement.com
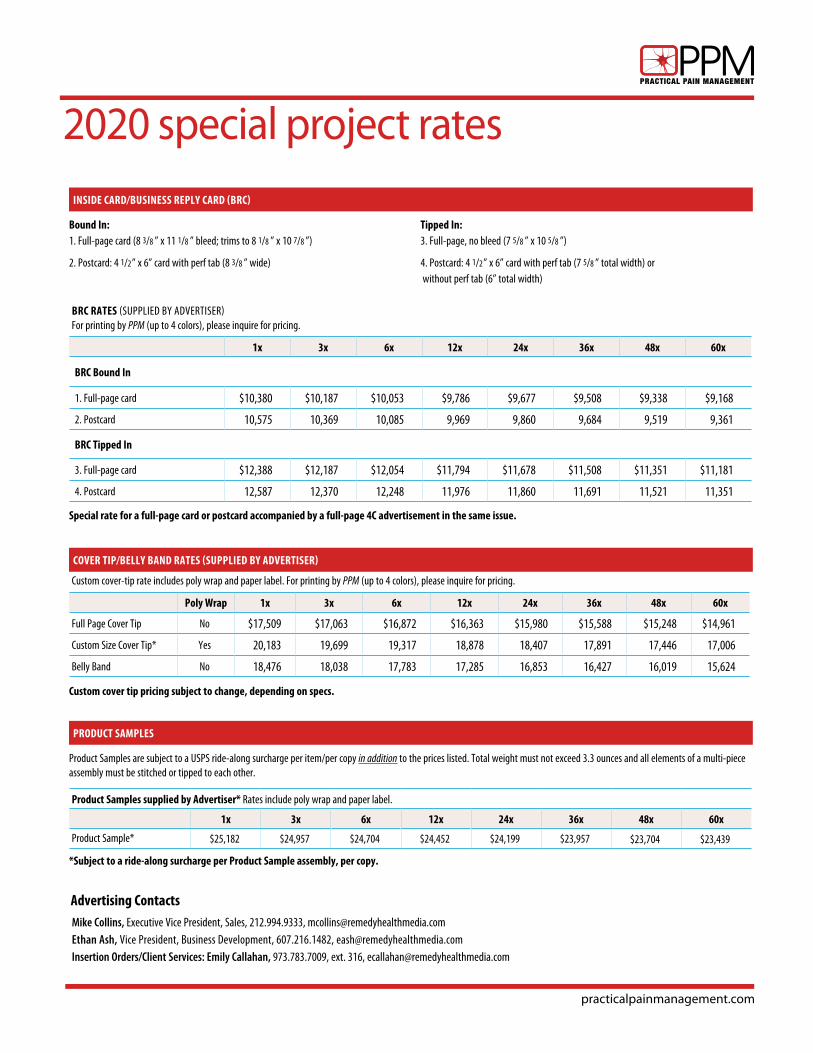
Product Samples supplied by Advertiser* Rates include poly wrap and paper label.
1x 3x 6x 12x 24x 36x 48x 60x
Product Sample* $25,182 $24,957 $24,704 $24,452 $24,199 $23,957 $23,704 $23,439
Product Samples are subject to a USPS ride-along surcharge per item/per copy in addition to the prices listed. Total weight must not exceed 3.3 ounces and all elements of a multi-piece assembly must be stitched or tipped to each other.
PRODUCT SAMPLES
*Subject to a ride-along surcharge per Product Sample assembly, per copy.
2020 special project rates
Bound In:1. Full-page card (8 3/8 ” x 11 1/8 ” bleed; trims to 8 1/8 ” x 10 7/8 ”)
2. Postcard: 4 1/2” x 6” card with perf tab (8 3/8 ” wide)
Tipped In:3. Full-page, no bleed (7 5/8 ” x 10 5/8 ”)
4. Postcard: 4 1/2” x 6” card with perf tab (7 5/8 ” total width) or without perf tab (6” total width)
INSIDE CARD/BUSINESS REPLY CARD (BRC)
BRC RATES (SUPPLIED BY ADVERTISER)For printing by PPM (up to 4 colors), please inquire for pricing.
1x 3x 6x 12x 24x 36x 48x 60x
BRC Bound In
1. Full-page card $10,380 $10,187 $10,053 $9,786 $9,677 $9,508 $9,338 $9,168
2. Postcard 10,575 10,369 10,085 9,969 9,860 9,684 9,519 9,361
BRC Tipped In
3. Full-page card $12,388 $12,187 $12,054 $11,794 $11,678 $11,508 $11,351 $11,181
4. Postcard 12,587 12,370 12,248 11,976 11,860 11,691 11,521 11,351
Special rate for a full-page card or postcard accompanied by a full-page 4C advertisement in the same issue.
Mike Collins, Executive Vice President, Sales, 212.994.9333, [email protected] Ash, Vice President, Business Development, 607.216.1482, [email protected] Insertion Orders/Client Services: Emily Callahan, 973.783.7009, ext. 316, [email protected]
Advertising Contacts
Custom cover tip pricing subject to change, depending on specs.
Custom cover-tip rate includes poly wrap and paper label. For printing by PPM (up to 4 colors), please inquire for pricing.
Poly Wrap 1x 3x 6x 12x 24x 36x 48x 60x
Full Page Cover Tip No $17,509 $17,063 $16,872 $16,363 $15,980 $15,588 $15,248 $14,961
Custom Size Cover Tip* Yes 20,183 19,699 19,317 18,878 18,407 17,891 17,446 17,006
Belly Band No 18,476 18,038 17,783 17,285 16,853 16,427 16,019 15,624
COVER TIP/BELLY BAND RATES (SUPPLIED BY ADVERTISER)
practicalpainmanagement.com
1. Mail or Delivery Service Send to:
Emily Callahan Remedy Health Media 7 North Willow Street, Suite 7A Montclair, NJ 07042 973.783.7009, ext. 316 [email protected]
2. Inserts’ Shipping Address: Practical Pain Management c/o Publishers Press 13487 South Preston Highway Lebanon Junction, KY 40150 Contact: Jeff Newton, 1.866.644.3705 [email protected]
3. Electronic Submission: For FTP server information to upload ad
submissions, please contact Emily Callahan at [email protected]
4. Accounts Receivable: Payment by Wire or ACH: PNC Bank N. A Acct Name: Remedy Health Group, LLC ABA# : 031207607 Acct# : 8026361265 Payment by Check: Remedy Health Media, LLC P.O. Box 829645 Philadelphia, PA 19182-9645 Contact: Daisy Jongoy
212.695.4316 [email protected]
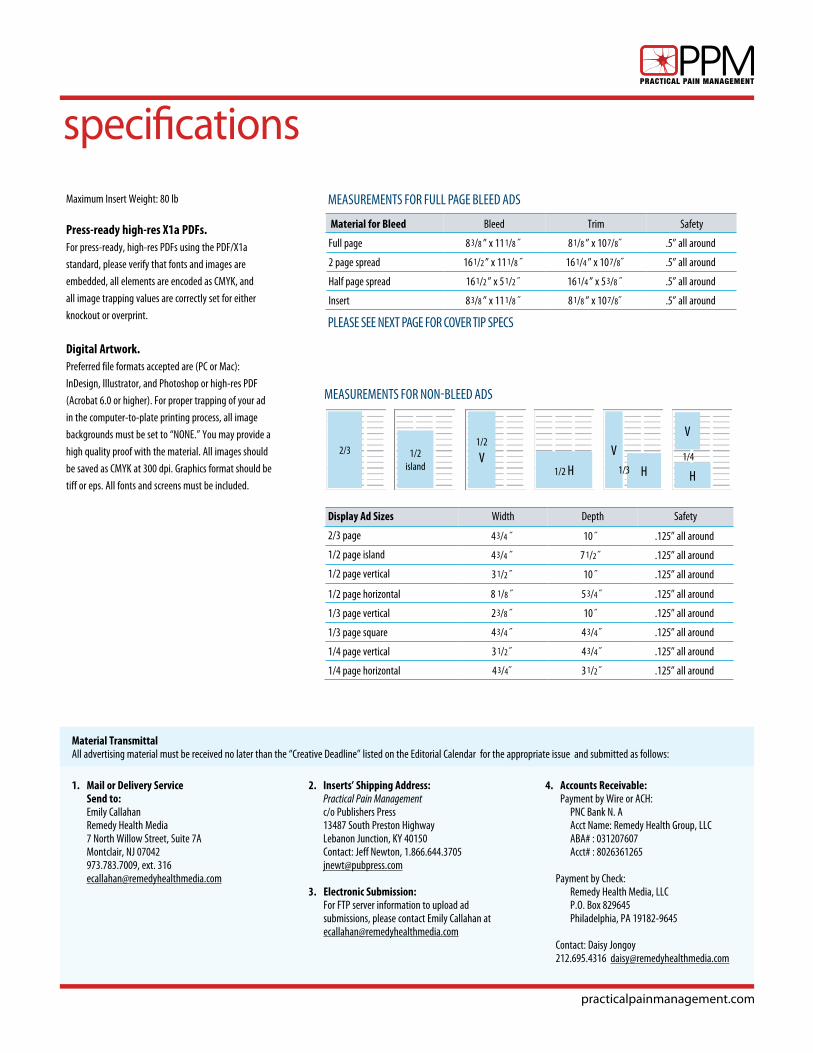
specificationsMaximum Insert Weight: 80 lb
Press-ready high-res X1a PDFs.For press-ready, high-res PDFs using the PDF/X1a
standard, please verify that fonts and images are
embedded, all elements are encoded as CMYK, and
all image trapping values are correctly set for either
knockout or overprint.
Digital Artwork. Preferred file formats accepted are (PC or Mac):
InDesign, Illustrator, and Photoshop or high-res PDF
(Acrobat 6.0 or higher). For proper trapping of your ad
in the computer-to-plate printing process, all image
backgrounds must be set to “NONE.” You may provide a
high quality proof with the material. All images should
be saved as CMYK at 300 dpi. Graphics format should be
tiff or eps. All fonts and screens must be included.
Display Ad Sizes Width Depth Safety
2/3 page 4 3/4 ˝ 10 ˝ .125” all around
1/2 page island 4 3/4 ˝ 7 1/2˝ .125” all around
1/2 page vertical 3 1/2 ˝ 10 ˝ .125” all around
1/2 page horizontal 8 1/8 ˝ 5 3/4 ˝ .125” all around
1/3 page vertical 2 3/8 ˝ 10 ˝ .125” all around
1/3 page square 4 3/4 ˝ 4 3/4˝ .125” all around
1/4 page vertical 3 1/2˝ 4 3/4˝ .125” all around
1/4 page horizontal 4 3/4˝ 3 1/2˝ .125” all around
2/3 1/2island
1/2
V1/2 H
V
H
1/4V
H1/3
Material for Bleed Bleed Trim Safety
Full page 8 3/8 ” x 11 1/8 ˝ 8 1/8 ” x 10 7/8˝ .5” all around
2 page spread 16 1/2 ” x 11 1/8 ˝ 16 1/4 ” x 10 7/8˝ .5” all around
Half page spread 16 1/2 ” x 5 1/2 ˝ 16 1/4 ” x 5 3/8 ˝ .5” all around
Insert 8 3/8 ” x 11 1/8 ˝ 8 1/8 ” x 10 7/8˝ .5” all around
MEASUREMENTS FOR FULL PAGE BLEED ADS
PLEASE SEE NEXT PAGE FOR COVER TIP SPECS
Material TransmittalAll advertising material must be received no later than the “Creative Deadline” listed on the Editorial Calendar for the appropriate issue and submitted as follows:
MEASUREMENTS FOR NON-BLEED ADS
practicalpainmanagement.com
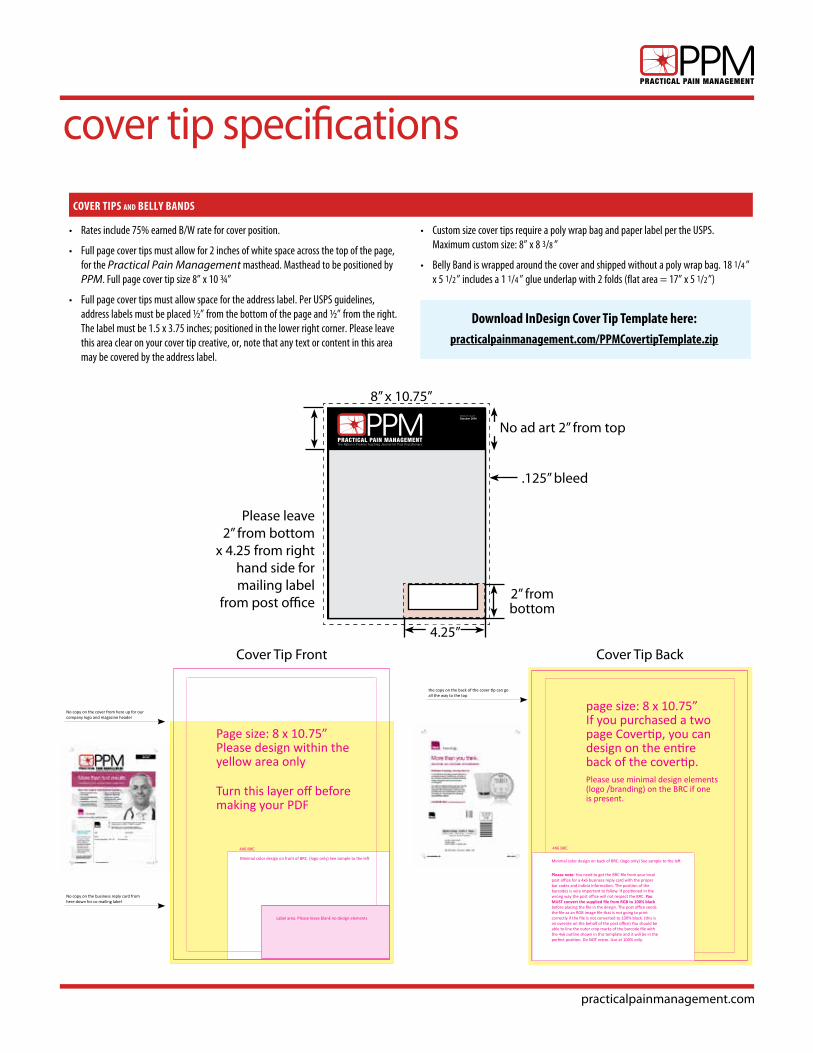
cover tip specifications
Volume 14, Issue 9October 2014
The Nation’s Premier Teaching Journal for Pain PractitionersPRACTICAL PAIN MANAGEMENT
A Vertical Health, LLC publication | www.PracticalPainManagement.com
Also In This Issue:•Sleep and Pain•Role of Endorphins in Pain Management•Highlights from PAINWeek
Cover October 2014.indd 1 10/2/14 12:06 PM
8” x 10.75”
Cover Tip Back
No ad art 2” from top
Please leave2” from bottom
x 4.25 from right hand side for mailing label
from post office2” from bottom
.125” bleed
• Rates include 75% earned B/W rate for cover position.
• Full page cover tips must allow for 2 inches of white space across the top of the page, for the Practical Pain Management masthead. Masthead to be positioned by PPM. Full page cover tip size 8” x 10 ¾”
• Full page cover tips must allow space for the address label. Per USPS guidelines, address labels must be placed ½” from the bottom of the page and ½” from the right. The label must be 1.5 x 3.75 inches; positioned in the lower right corner. Please leave this area clear on your cover tip creative, or, note that any text or content in this area may be covered by the address label.
• Custom size cover tips require a poly wrap bag and paper label per the USPS. Maximum custom size: 8” x 8 3/8 ”
• Belly Band is wrapped around the cover and shipped without a poly wrap bag. 18 1/4 ” x 5 1/2” includes a 1 1/4 ” glue underlap with 2 folds (flat area = 17” x 5 1/2”)
COVER TIPS and BELLY BANDS
Download InDesign Cover Tip Template here:practicalpainmanagement.com/PPMCovertipTemplate.zip
Cover Tip Front
No copy on the business reply card from here down for co mailing label
No copy on the cover from here up for our company logo and magazine header
Label area. Please leave blank no design elements
Turn this layer off before making your PDF
4X6 BRC
Page size: 8 x 10.75”Please design within the yellow area only
Minimal color design on front of BRC. (logo only) See sample to the left
Please note: You need to get the BRC file from your local post office for a 4x6 business reply card with the proper bar codes and indicia information. The position of the barcodes is very important to follow. If positioned in the wrong way the post office will not respect the BRC. You MUST convert the supplied file from RGB to 100% black before placing the file in the design. The post office sends the file as an RGB image file that is not going to print correctly if the file is not converted to 100% black. (this is an oversite on the behalf of the post office) You should be able to line the outer crop marks of the barcode file with the 4x6 outline shown in this template and it will be in the perfect position. Do NOT resize. Use at 100% only.
the copy on the back of the cover tip can go all the way to the top
4X6 BRC
page size: 8 x 10.75” If you purchased a two page Covertip, you can design on the entire back of the covertip.Please use minimal design elements (logo /branding) on the BRC if one is present.
Minimal color design on back of BRC. (logo only) See sample to the left
4.25”
practicalpainmanagement.com
circulation
Periodicals Mail Service Periodicals Mail Service is the publication service of the United States Postal Service (USPS)
and the most economical service for subscribers in the United States, but not all publications
can meet the stringent requirements and postal audits needed to qualify for the reduced rates.
• PPM was qualified by the USPS for a periodical license in November 2002
under the Requester Publication Category by meeting—and subsequently
have maintained current with—the following key periodical requirements:
• The publication’s circulation records are kept and are available
for USPS examination. Subscriber cards and other digital
subscriber records (web subscribers and direct subscriber new/
renewal calls) are kept in the New Jersey office.
• The publication must have a legitimate list of persons who
have requested the publication, or a member of a requesting
organization that has adopted a formal resolution that each
member receive a copy, and 50% or more of the copies must
be distributed to persons who have made such requests.
• Subscription requests that are more than 3 years old cannot
be considered valid requests. PPM flags subscriber records
in advance of expiration and submits expired requesters with
phone numbers to a marketing firm to secure renewals.
• Expiring subscriptions for which we do not have phone numbers
are submitted to a list firm to refresh the address information.
• PPM uses the USPS’ Automated Address Correction Service (ACS) for
automated address corrections and undeliverables.
• PPM also participates in a co-palletization program at our printer for
more efficient, economical, and quicker distribution to US postal sites
around the country.
PPM Subscriber List Maintenance 1. ACS records are downloaded from a secure USPS Internet site and a database
program then uses the files to automatically correct addresses in the PPM
database and remove “nixies” that are undeliverable.
2. Subscription cards, faxes, and website subscriptions are sorted into
renewals and new additions. New additions are vetted against the database
to prevent duplicate subscriptions. Questionable subscriptions are confirmed
using Internet doctor search sites before adding to the database.
3. Interactive dupe checking is then performed on the database using last
name, a few digits of the address, city, and state. Suspected duplicates are
displayed to allow database tagging of the ones to keep before purging
the dupes.
Business Publications Audit (BPA)• Audited by BPA to verify subscriptions.
• BPA audit information sheet is available by request.




























