Embed Size (px)
Citation preview

W
MedicineMaps: A tool for mapping and linking evidence from experimental and clinical trial literatureNicholas J. Matiasz1,3, Wei-Ting Chen2, Alcino J. Silva, PhD3, William Hsu, PhD1
Researchers need tools to integrate find-ings from a diverse and growing literature
MedicineMaps allows translational scientists to formalize the way they summarize evidence and design clinical trials.
Randomized clinical trials (RCTs) are the de facto method for test-ing and reporting the efficacy and safety of treatments.
The literature available on even rare diseases often provides more information than any individual scientist can digest and process.
Translational scientists thus need meta-analytic tools that can: integrate primary outcomes across multiple RCTs, summarize what’s known to explain effects on a population, and compare studies methodologically to inform future study design.
We explore these issues in the domain of Neurofibromatosis type I (NF1), a genetic disorder that causes cognitive deficits in children.
This work builds off ResearchMaps [2–3], a free web application for tracking and planning research in basic science (e.g., biology).
Structuring clinical trial reports can help to make causal information more digestible
Graphical formalisms concisely encode observed statistical rela-tions while intuitively visualizing causal relations.
We use a graphical formalism to annotate literature, leading to data structures that can be explored with intuitive queries:
What are the essential elements from a study that can guide decision making?
We studied clinical trial reports to identify which of their elements are essential for understanding the context of a trial’s outcomes.
Does lovastatin improve attention in children with NF1?”
“ MATCH (p:Paper)-[]->(i:Intervention),(i:Intervention)-[r:EXCITES]->(o:Outcome)WHERE i='lovastatin' AND o='attention'AND r.age<18 RETURN p,i,r,o;
To contextualize results, MedicineMaps shows how studies differ methodologically
Bioengineering & Radiological SciencesComputer ScienceNeurobiology, Psychology, & Psychiatry
123
We will link the databases of ResearchMaps and MedicineMaps to identify etiologies
Discussion and future work
MedicineMaps.org is a free web application that you can use to annotate clinical trials
RESEARCH ARTICLE Open Access
Lovastatin improves impaired synaptic plasticityand phasic alertness in patients withneurofibromatosis type 1Florian Mainberger1, Nikolai H Jung1, Martin Zenker2, Ute Wahlländer3, Leonie Freudenberg9, Susanne Langer1,Steffen Berweck4, Tobias Winkler5, Andreas Straube5, Florian Heinen6, Sofia Granström7, Victor-Felix Mautner7,Karen Lidzba8 and Volker Mall1*
Abstract
Background: Neurofibromatosis type 1 (NF1) is one of the most common genetic disorders causing learningdisabilities by mutations in the neurofibromin gene, an important inhibitor of the RAS pathway. In a mouse modelof NF1, a loss of function mutation of the neurofibromin gene resulted in increased gamma aminobutyric acid(GABA)-mediated inhibition which led to decreased synaptic plasticity and deficits in attentional performance. Mostimportantly, these defictis were normalized by lovastatin. This placebo-controlled, double blind, randomized studyaimed to investigate synaptic plasticity and cognition in humans with NF1 and tried to answer the questionwhether potential deficits may be rescued by lovastatin.
Methods: In NF1 patients (n = 11; 19–44 years) and healthy controls (HC; n = 11; 19–31 years) paired pulsetranscranial magnetic stimulation (TMS) was used to study intracortical inhibition (paired pulse) and synapticplasticity (paired associative stimulation). On behavioural level the Test of Attentional Performance (TAP) was used.To study the effect of 200 mg lovastatin for 4 days on all these parameters, a placebo-controlled, double blind,randomized trial was performed.
Results: In patients with NF1, lovastatin revealed significant decrease of intracortical inhibition, significant increaseof synaptic plasticity as well as significant increase of phasic alertness. Compared to HC, patients with NF1 exposedincreased intracortical inhibition, impaired synaptic plasticity and deficits in phasic alertness.
Conclusions: This study demonstrates, for the first time, a link between a pathological RAS pathway activity,intracortical inhibition and impaired synaptic plasticity and its rescue by lovastatin in humans. Our findings revealedmechanisms of attention disorders in humans with NF1 and support the idea of a potential clinical benefit oflovastatin as a therapeutic option.
Keywords: Transcranial magnetic stimulation (TMS), Paired associative stimulation (PAS), Long-term potentiation(LTP), Synaptic plasticity, RAS-pathway, Developmental disorder, NF1, Attention, Lovastatin
* Correspondence: [email protected] of Pediatrics, Technical University Munich, KinderzentrumMünchen gemeinnützige GmbH, Heiglhofstrasse 63, 81377 Munich, GermanyFull list of author information is available at the end of the article
© 2013 Mainberger et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of theCreative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Mainberger et al. BMC Neurology 2013, 13:131http://www.biomedcentral.com/1471-2377/13/131
RESEARCH ARTICLE Open Access
Lovastatin improves impaired synaptic plasticityand phasic alertness in patients withneurofibromatosis type 1Florian Mainberger1, Nikolai H Jung1, Martin Zenker2, Ute Wahlländer3, Leonie Freudenberg9, Susanne Langer1,Steffen Berweck4, Tobias Winkler5, Andreas Straube5, Florian Heinen6, Sofia Granström7, Victor-Felix Mautner7,Karen Lidzba8 and Volker Mall1*
Abstract
Background: Neurofibromatosis type 1 (NF1) is one of the most common genetic disorders causing learningdisabilities by mutations in the neurofibromin gene, an important inhibitor of the RAS pathway. In a mouse modelof NF1, a loss of function mutation of the neurofibromin gene resulted in increased gamma aminobutyric acid(GABA)-mediated inhibition which led to decreased synaptic plasticity and deficits in attentional performance. Mostimportantly, these defictis were normalized by lovastatin. This placebo-controlled, double blind, randomized studyaimed to investigate synaptic plasticity and cognition in humans with NF1 and tried to answer the questionwhether potential deficits may be rescued by lovastatin.
Methods: In NF1 patients (n = 11; 19–44 years) and healthy controls (HC; n = 11; 19–31 years) paired pulsetranscranial magnetic stimulation (TMS) was used to study intracortical inhibition (paired pulse) and synapticplasticity (paired associative stimulation). On behavioural level the Test of Attentional Performance (TAP) was used.To study the effect of 200 mg lovastatin for 4 days on all these parameters, a placebo-controlled, double blind,randomized trial was performed.
Results: In patients with NF1, lovastatin revealed significant decrease of intracortical inhibition, significant increaseof synaptic plasticity as well as significant increase of phasic alertness. Compared to HC, patients with NF1 exposedincreased intracortical inhibition, impaired synaptic plasticity and deficits in phasic alertness.
Conclusions: This study demonstrates, for the first time, a link between a pathological RAS pathway activity,intracortical inhibition and impaired synaptic plasticity and its rescue by lovastatin in humans. Our findings revealedmechanisms of attention disorders in humans with NF1 and support the idea of a potential clinical benefit oflovastatin as a therapeutic option.
Keywords: Transcranial magnetic stimulation (TMS), Paired associative stimulation (PAS), Long-term potentiation(LTP), Synaptic plasticity, RAS-pathway, Developmental disorder, NF1, Attention, Lovastatin
* Correspondence: [email protected] of Pediatrics, Technical University Munich, KinderzentrumMünchen gemeinnützige GmbH, Heiglhofstrasse 63, 81377 Munich, GermanyFull list of author information is available at the end of the article
© 2013 Mainberger et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of theCreative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Mainberger et al. BMC Neurology 2013, 13:131http://www.biomedcentral.com/1471-2377/13/131
p = 0.089) or perceptual threshold (NF1-placebo: 0.71 ±0.35 mA; NF1-lovastatin: 0.73 ± 0.26 mA; p = 0.749)between off and on medicated patients with NF1.RmANOVA of resting motor threshold data revealed nosignificant main effects or interaction (TIME: F[3;60] = 1.720,p = 0.175; GROUP: F[1;20] = 0.306, p= 0.586; TIME*GROUP:F[3;60] = 0.785, p = 0.502).
Exp. 2b: intracortical inhibitionHere we examined the influence of lovastatin and pla-cebo on intracortical inhibition in patients with NF1.Comparing SICI after a four day course of lovastatin andafter a four day course of placebo patients with NF1 didshow lower SICI after lovastatin compared to placebo(inter-stimulus-intervall of 2 ms: 0.58 ± 0.30 to 0.52 ± 0.22(p = 0.415); 3 ms: 0.66 ± 0.34 to 0.51 ± 0.24 (p = 0.221);5 ms: 0.99 ± 0.24 to 0.69 ± 0.20 (p = 0.017); all: 0.74 ± 0.34to 0.57 ± 0.23 (p = 0.011; see Figure 2). Furthermoredifferences in SICI between patients after a 4-daycourse of lovastatin compared to healthy controls werenot seen (2 ms: 0.75 ± 0.33 to 0.58 ± 0.30 (p = 0.315);3 ms: 0.77 ± 0.46 to 0.66 ± 0.34 (p = 0.684); 5 ms: 0.95 ±0.41 to 0.99 ± 0.24 (p = 0.481); all: 0.82 ± 0.40 to 0.74 ± 0.34(p = 0.734).
Exp. 2c: attention as measured with TAP in patients withNF1, intervention with lovastatinIn experiment 2c we tested the effect of lovastatin onattentional performance in patients with NF1. Here pa-tients with NF1 demonstrated faster reaction times afteradministration of the drug in the case of the conditionwith a warning tone but not without the warning tone(see Figure 5). In the condition with the warning tone,the reaction time was significantly shorter (from 240.5 ±21.69 ms at baseline to 226.9 ± 18.3 ms after lovastatinadministration, p = 0.004, (level of significance afterBonferroni-Holm adjustment: p ≤ 0.007), whereas pla-cebo had no effect (baseline: 233.1 ± 13.45 ms to 235.4 ±17.91 ms).
DiscussionThe main finding of the present placebo-controlled, ran-domized double blind study is that lovastatin normalizesLTP-like plasticity, decreases intracortical inhibition andimproves phasic alertness in patients with NF1.Impaired LTP-like plasticity, has also been described
in neuropsychiatric conditions such as Alzheimer’s dis-ease [24], in patients with schizophrenia [25] as well asin patients with Parkinson’s disease [26,27]. Taking into
ISIall ISI5 ms3 ms2 ms
Mea
n in
hib
itio
n
1.20
1.00
0.80
0.60
0.40
0.20
0.00
NF1-LovastatinNF1-PlaceboControls
Figure 2 SICI in healthy controls and patients with NF1 in on/off medication. Depicted are data of 10 patients of NF1 and healthy controlsin on/off medication. Mean inhibition at 60% resting motor threshold (for more details see methods) of the conditioning stimulus was built for ISIof 2, 3, 5 ms and over all ISI. Here, a trend towards increased inhibition in patients with NF1 (treated with placebo but not with lovastatin)compared to healthy controls can be observed. Error bars represent ± standard error of the mean.
Mainberger et al. BMC Neurology 2013, 13:131 Page 4 of 12http://www.biomedcentral.com/1471-2377/13/131
p = 0.089) or perceptual threshold (NF1-placebo: 0.71 ±0.35 mA; NF1-lovastatin: 0.73 ± 0.26 mA; p = 0.749)between off and on medicated patients with NF1.RmANOVA of resting motor threshold data revealed nosignificant main effects or interaction (TIME: F[3;60] = 1.720,p = 0.175; GROUP: F[1;20] = 0.306, p= 0.586; TIME*GROUP:F[3;60] = 0.785, p = 0.502).
Exp. 2b: intracortical inhibitionHere we examined the influence of lovastatin and pla-cebo on intracortical inhibition in patients with NF1.Comparing SICI after a four day course of lovastatin andafter a four day course of placebo patients with NF1 didshow lower SICI after lovastatin compared to placebo(inter-stimulus-intervall of 2 ms: 0.58 ± 0.30 to 0.52 ± 0.22(p = 0.415); 3 ms: 0.66 ± 0.34 to 0.51 ± 0.24 (p = 0.221);5 ms: 0.99 ± 0.24 to 0.69 ± 0.20 (p = 0.017); all: 0.74 ± 0.34to 0.57 ± 0.23 (p = 0.011; see Figure 2). Furthermoredifferences in SICI between patients after a 4-daycourse of lovastatin compared to healthy controls werenot seen (2 ms: 0.75 ± 0.33 to 0.58 ± 0.30 (p = 0.315);3 ms: 0.77 ± 0.46 to 0.66 ± 0.34 (p = 0.684); 5 ms: 0.95 ±0.41 to 0.99 ± 0.24 (p = 0.481); all: 0.82 ± 0.40 to 0.74 ± 0.34(p = 0.734).
Exp. 2c: attention as measured with TAP in patients withNF1, intervention with lovastatinIn experiment 2c we tested the effect of lovastatin onattentional performance in patients with NF1. Here pa-tients with NF1 demonstrated faster reaction times afteradministration of the drug in the case of the conditionwith a warning tone but not without the warning tone(see Figure 5). In the condition with the warning tone,the reaction time was significantly shorter (from 240.5 ±21.69 ms at baseline to 226.9 ± 18.3 ms after lovastatinadministration, p = 0.004, (level of significance afterBonferroni-Holm adjustment: p ≤ 0.007), whereas pla-cebo had no effect (baseline: 233.1 ± 13.45 ms to 235.4 ±17.91 ms).
DiscussionThe main finding of the present placebo-controlled, ran-domized double blind study is that lovastatin normalizesLTP-like plasticity, decreases intracortical inhibition andimproves phasic alertness in patients with NF1.Impaired LTP-like plasticity, has also been described
in neuropsychiatric conditions such as Alzheimer’s dis-ease [24], in patients with schizophrenia [25] as well asin patients with Parkinson’s disease [26,27]. Taking into
ISIall ISI5 ms3 ms2 ms
Mea
n in
hib
itio
n
1.20
1.00
0.80
0.60
0.40
0.20
0.00
NF1-LovastatinNF1-PlaceboControls
Figure 2 SICI in healthy controls and patients with NF1 in on/off medication. Depicted are data of 10 patients of NF1 and healthy controlsin on/off medication. Mean inhibition at 60% resting motor threshold (for more details see methods) of the conditioning stimulus was built for ISIof 2, 3, 5 ms and over all ISI. Here, a trend towards increased inhibition in patients with NF1 (treated with placebo but not with lovastatin)compared to healthy controls can be observed. Error bars represent ± standard error of the mean.
Mainberger et al. BMC Neurology 2013, 13:131 Page 4 of 12http://www.biomedcentral.com/1471-2377/13/131
medical imagingINFORMATICS
Animal models [1] suggest that statins could treat cognitive deficits caused by NF1, but studies in humans have shown mixed results.
To explore this issue, we used MedicineMaps to annotate studies of statins’ effects on various cognitive measures in NF1 patients.
With each study’s metadata, MedicineMaps visualizes method-ological differences across studies to contextualize their results.
These visualizations can help researchers to design new studies.
LTPCA1adult
hippocampal learningmiceadult
GABA inhibitionCA1Adult
K-rasmice
germ line0.063 ↓
0.063 ↓
NF1mice
germ line
0.125 ↓
0.063 ↓
0.063 ↓
PPFCA1Adult
0.063 ↓
I/OCA1Adult
0.063 ↓ N-rasmice
germ line
0.063 ↓
Farnesyl transferasemiceadult
0.063 ↓
Causal graphs model causal relationsand can help scientists plan experiments
Number of system variables Number of possible DAGs123456
13
25543
29,2813,781,503
The number of possible DAGs rises super-exponentially in the number of system variables.
Causal relations can be represented by directed graphs.
Causal models may assume acyclicity (a lack of feedback) and are thus modeled by directed acyclic graphs (DAGs).
The model space for causal mechanismsis very large
Research maps’ scoring of evidencequantifies consistency and convergence
Medicine maps represent and synthesize evidence from clinical trial literature
The graph databases of the ResearchMaps and MedicineMaps apps will be linked, allowing the user to explore the biological mechanisms underlying the results from clinical trials.
Research maps and medicine maps can be used to derive formal causal graphs
literature map constraints causal graphs
An ASP solver finds the causal graphs that satisfy the constraints.
The constraints are represented with answer set programming (ASP).
The maps’ edges are translated into causal-structure constraints.
ResearchMaps
MedicineMaps
X Y Z
X Y Z
X Y Z
ORIGINAL ARTICLE
HCN channels are a novel therapeutic target for cognitivedysfunction in Neurofibromatosis type 1A Omrani1,2,10, T van der Vaart1,2,3, E Mientjes1,2, GM van Woerden1,2, MR Hojjati1,4, KW Li5, DH Gutmann6, CN Levelt7, AB Smit5,AJ Silva8, SA Kushner2,9 and Y Elgersma1,2
Cognitive impairments are a major clinical feature of the common neurogenetic disease neurofibromatosis type 1 (NF1). Previousstudies have demonstrated that increased neuronal inhibition underlies the learning deficits in NF1, however, the molecularmechanism underlying this cell-type specificity has remained unknown. Here, we identify an interneuron-specific attenuation ofhyperpolarization-activated cyclic nucleotide-gated (HCN) current as the cause for increased inhibition in Nf1 mutants.Mechanistically, we demonstrate that HCN1 is a novel NF1-interacting protein for which loss of NF1 results in a concomitantincrease of interneuron excitability. Furthermore, the HCN channel agonist lamotrigine rescued the electrophysiological andcognitive deficits in two independent Nf1 mouse models, thereby establishing the importance of HCN channel dysfunction in NF1.Together, our results provide detailed mechanistic insights into the pathophysiology of NF1-associated cognitive defects, andidentify a novel target for clinical drug development.
Molecular Psychiatry (2015) 20, 1311–1321; doi:10.1038/mp.2015.48; published online 28 April 2015
INTRODUCTIONNeurofibromatosis type 1 (NF1, incidence 1:3000) is caused bymutations in the NF1 gene. The NF1 gene product, neurofibromin,contains a Ras GTPase-activating protein domain, which serves asa negative regulator of Ras/ERK signaling. The clinical symptomsof NF1 include cutaneous neurofibromas, café-au-lait spots,skinfold freckling and Lisch nodules, as well as cognitive deficitsthat negatively impact school performance and quality of life.1,2
Mice with a heterozygous null mutation of the Nf1 gene(Nf1+/–mice) closely model the cognitive deficits and behavioraldifficulties experienced by human NF1 patients, includingvisual-spatial learning, working memory, attention and motorperformance deficits.3–5
Previously, it has been shown that the learning deficits of Nf1+/–
mice result from hyperactivation of Ras signaling in GABAergicneurons, despite expression of the neurofibromin/Ras in bothexcitatory and inhibitory neurons.3,6 The specificity of thisphenotype is further surprising, given that it is not recapitulatedin other mouse models in which Ras-ERK signaling is upregulated,such as mouse models for Noonan syndrome and Costellosyndrome.7 This suggests that NF1 might also have a Ras-independent function in neurons. Ras-independent targets holdsubstantial therapeutic potential, as Ras itself is difficult to target,and drugs that interfere with downstream Ras signaling have poortissue specificity and undesirable side effects, limiting their utilityfor treating cognitive dysfunction. Moreover, two randomizedcontrolled trials targeting Ras activity in NF1 patients demon-strated no evidence of clinical efficacy.8,9
In the present study, we sought to define the mechanismsunderlying the cell-type-specific pathophysiology underlying thelearning deficits of Nf1 mice. Given the widespread expression ofneurofibromin in neuronal and glial cell types, we focused ourefforts on a novel Nf1 mouse mutant with deletion of the neuron-specific NF1 exon 9a isoform (Nf19a–/9a). Exon 9a is a short 10amino-acid sequence in the amino-terminal region, the presenceof which does not influence the function of the Ras GTPase-activating protein domain.10 Expression of the exon 9a isoformbegins postnatally and is highly abundant in the septum, striatum,cortex and hippocampus.10–12 We found that Nf19a–/9a– micerecapitulate the phenotypes observed in the global Nf1+/– mice,including deficits in hippocampal synaptic plasticity and learning,as well as enhanced inhibitory synaptic transmission. Furthermore,we identified the hyperpolarization-activated cyclic nucleotide-gated channel 1 (HCN1) as a neurofibromin-interacting protein.HCN1 belongs to the family of voltage-gated ion channels thatmediate an inward cationic current (Ih),
13 which contributes tointrinsic excitability, pacemaker activity and synaptic integra-tion.14–16 Accordingly, increasing evidence has implicated Ihin activity-dependent plasticity, learning and memory, andepilepsy.17–21 Furthermore, HCN1 is enriched in cortical andhippocampal parvalbumin-expressing interneurons.22–26 We nowdemonstrate attenuation of Ih and subsequent enhancement ofexcitability in interneurons of Nf1 mutant mice. Moreover, weshow that the attenuation of Ih underlies the increased inhi-bitory neurotransmission in Nf19a–/9a– and Nf1+/– mice, such thatincreasing HCN current with lamotrigine (LTG) rescues the
1Department of Neuroscience, Erasmus Medical Center, Rotterdam, The Netherlands; 2ENCORE Center for Neurodevelopmental Disorders, Erasmus Medical Center, Rotterdam,The Netherlands; 3Department of Pediatrics, Erasmus Medical Center, Sophia Children’s Hospital, Rotterdam, The Netherlands; 4Department of Physiology, Shahrekord Universityof Medical Sciences, Shahrekord, Iran; 5Department of Molecular and Cellular Neurobiology, CNCR, Neuroscience Campus Amsterdam, VU University, Amsterdam, TheNetherlands; 6Department of Neurology, Washington University School of Medicine, St. Louis, MO, USA; 7Department of Molecular Visual Plasticity, Netherlands Institute forNeuroscience, Royal Netherlands Academy of Arts and Sciences (KNAW), Amsterdam, The Netherlands; 8Department of Neurobiology, Brain Research Institute, University ofCalifornia Los Angeles, Los Angeles, CA, USA and 9Department of Psychiatry, Erasmus Medical Center, Rotterdam, The Netherlands. Correspondence: Professor Y Elgersma,Department of Neuroscience, Erasmus Medical Center, Wytemaweg 80, PO Box 2040, CA, Rotterdam 3000, The Netherlands.E-mail: [email protected] address: Department of Translational Neuroscience, Brain Center Rudolf Magnus, University Medical Center Utrecht, Utrecht, The Netherlands.Received 3 November 2014; revised 19 February 2015; accepted 9 March 2015; published online 28 April 2015
Molecular Psychiatry (2015) 20, 1311–1321© 2015 Macmillan Publishers Limited All rights reserved 1359-4184/15
www.nature.com/mp
1736 VOLUME 17 | NUMBER 12 | DECEMBER 2014 NATURE NEUROSCIENCE
A R T I C L E S
NS, an autosomal dominant genetic disorder with an incidence of ~1 in 2,500 live births, is characterized by facial abnormalities, short stature, motor delay and cardiac defects1,2. Importantly, 30–50% of patients with NS show cognitive deficits3–6. Patients with NS also show clumsiness, motor delay, hearing loss, deficits in spatial knowledge and planning, and social and emotional problems3,4,7. Patients with NS also show impairments in hippocampal-dependent memory tasks4,8,9.
Germline mutations in genes involved in Ras-Erk signaling, such as PTPN11, SOS1, KRAS, NRAS, RAF1, BRAF, SHOC2, MAP2K1 (MEK1) and CBL, have been reported to cause NS1,10. Among those, mutations in PTPN11, which encodes SHP2, account for ~50% of NS cases1. SHP2 is a positive regulator of Ras-Erk signaling11, which has a crucial function in many cellular processes, including learn-ing and memory12. The PTPN11 mutations found in NS patients are gain-of-function alleles that upregulate this signaling cascade11,13–15. Cognitive problems such as learning disabilities and memory impair-ment are common in NS3,5,6. However, little is known about the role of PTPN11 in synaptic plasticity and learning and memory in the mammalian brain. Furthermore, there is no available treatment for cognitive deficits associated with this common genetic disorder.
Previous studies using NS mouse models derived by knock-in Ptpn11 mutations demonstrated that the heterozygous knock-in mice show phenotypes similar to those found in NS patients. These
include short stature, craniofacial abnormalities, myeloproliferative disease and multiple cardiac defects14,16. Here we first tested whether NS mice have deficits in learning and memory and synaptic plastic-ity. Then, we asked whether increasing SHP2 activity in adult brain affects synaptic function, LTP and learning and memory. Finally, we examined whether it is possible to rescue the LTP and learning deficits of adult NS mice.
RESULTSNS mice show deficits in spatial learning and memoryTo investigate the underlying mechanism of the learning and memory deficits associated with NS, we studied two lines of heterozygous knock-in mice harboring gain-of-function mutations found in NS patients14,16: Ptpn11D61G/+ and Ptpn11N308D/+. Previous studies showed that the Ptpn11D61G/+ mutation causes more severe deficits than the Ptpn11N308D/+ mutation14,16. Because NS patients show deficits in spatial function and in memory tasks dependent on the hippocampus4,8,9, we tested both Ptpn11 mutants in the hidden-platform version of the Morris water maze17. In this task, mice learn to use spatial cues around a pool to find an escape platform hidden beneath the water’s surface. After training, memory is assessed in probe trials wherein the platform is removed and mice search the empty pool for 60 s. Ptpn11N308D/+ mice and wild-type (WT) controls showed similar latencies to find the hidden platform during training (Fig. 1a)
1Integrative Center for Learning and Memory, Departments of Neurobiology, Psychiatry and Biobehavioral Sciences, Psychology and Brain Research Institute, University of California Los Angeles, Los Angeles, California, USA. 2Department of Life Science, Chung-Ang University, Seoul, Korea. 3Department of Medicine and Microbiology, College of Medicine, Signaling Disorder Research Center, Chungbuk National University, Cheongju, Korea. 4School of Biological Sciences, College of Natural Sciences, Seoul National University, Seoul, Korea. 5Department of Neurology, University of Wisconsin-Madison, Madison, Wisconsin, USA. 6Princess Margaret Cancer Center, University Health Network, Toronto, Ontario, Canada. 7Present addresses: DZNE, German Center for Neurodegenerative Diseases, Bonn, Germany (D.E.) and Center for Neuroscience, Indian Institute of Science, Bangalore, India (J.B.). Correspondence should be addressed to A.J.S. ([email protected]) or Y.-S.L. ([email protected]).
Received 27 July; accepted 14 October; published online 10 November 2014; doi:10.1038/nn.3863
Mechanism and treatment for learning and memory deficits in mouse models of Noonan syndromeYong-Seok Lee1,2, Dan Ehninger1,7, Miou Zhou1, Jun-Young Oh3, Minkyung Kang2, Chuljung Kwak4, Hyun-Hee Ryu2, Delana Butz5, Toshiyuki Araki6, Ying Cai1, J Balaji1,7, Yoshitake Sano1, Christine I Nam1, Hyong Kyu Kim3, Bong-Kiun Kaang4, Corinna Burger5, Benjamin G Neel6 & Alcino J Silva1
In Noonan syndrome (NS) 30–50% of subjects show cognitive deficits of unknown etiology and with no known treatment. Here, we report that knock-in mice expressing either of two NS-associated mutations in Ptpn11, which encodes the nonreceptor protein tyrosine phosphatase Shp2, show hippocampal-dependent impairments in spatial learning and deficits in hippocampal long-term potentiation (LTP). In addition, viral overexpression of an NS-associated allele PTPN11D61G in adult mouse hippocampus results in increased baseline excitatory synaptic function and deficits in LTP and spatial learning, which can be reversed by a mitogen-activated protein kinase kinase (MEK) inhibitor. Furthermore, brief treatment with lovastatin reduces activation of the GTPase Ras–extracellular signal-related kinase (Erk) pathway in the brain and normalizes deficits in LTP and learning in adult Ptpn11D61G/+ mice. Our results demonstrate that increased basal Erk activity and corresponding baseline increases in excitatory synaptic function are responsible for the LTP impairments and, consequently, the learning deficits in mouse models of NS. These data also suggest that lovastatin or MEK inhibitors may be useful for treating the cognitive deficits in NS.
Reversal of learning deficits in a Tsc2+/– mouse model oftuberous sclerosisDan Ehninger1, Sangyeul Han2, Carrie Shilyansky1, Yu Zhou1, Weidong Li1, David J Kwiatkowski3,Vijaya Ramesh2 & Alcino J Silva1
Tuberous sclerosis is a single-gene disorder caused byheterozygous mutations in the TSC1 (9q34) or TSC2 (16p13.3)gene1,2 and is frequently associated with mental retardation,autism and epilepsy. Even individuals with tuberous sclerosisand a normal intelligence quotient (approximately 50%)3–5 arecommonly affected with specific neuropsychological problems,including long-term and working memory deficits6,7. Here wereport that mice with a heterozygous, inactivating mutation inthe Tsc2 gene (Tsc2+/– mice)8 show deficits in learning andmemory. Cognitive deficits in Tsc2+/– mice emerged in theabsence of neuropathology and seizures, demonstrating thatother disease mechanisms are involved5,9–11. We show thathyperactive hippocampal mammalian target of rapamycin(mTOR) signaling led to abnormal long-term potentiation in theCA1 region of the hippocampus and consequently to deficits inhippocampal-dependent learning. These deficits includedimpairments in two spatial learning tasks and in contextualdiscrimination. Notably, we show that a brief treatment with themTOR inhibitor rapamycin in adult mice rescues not only thesynaptic plasticity, but also the behavioral deficits in thisanimal model of tuberous sclerosis. The results presented herereveal a biological basis for some of the cognitive deficitsassociated with tuberous sclerosis, and they show thattreatment with mTOR antagonists ameliorates cognitivedysfunction in a mouse model of this disorder.
To address the mechanisms of tuberous sclerosis–related cognitivedeficits, we first determined whether Tsc2+/– mice had learning andmemory impairments. Because the tuberous sclerosis genes are highlyexpressed in adult brain, including hippocampus12, and hippocampaldysfunction could contribute to the tuberous sclerosis phenotype, westudied spatial learning in the Morris water maze. Initially, mice weretested in a hippocampus-dependent version of the Morris water maze,in which they use distal spatial cues to navigate and locate a hiddenescape platform (Fig. 1a). To assess whether the mice had learned theposition of the escape platform, we gave a probe trial (during whichthe platform was removed from the pool) at the end of training. Probe
trial data show that searches from wild-type (WT) mice were moreselective than those from Tsc2+/– mice, indicating spatial learningdeficits in these mutants (Fig. 1a). Studies with the hippocampus-independent, visible version of the water maze (SupplementaryTable 1 online) revealed no differences between Tsc2+/– mice andWT controls, suggesting that motivational, perceptual or motordifferences are unlikely to account for the observed spatial learningphenotype. Moreover, additional behavioral characterization revealednormal motor skills, anxiety, exploratory activity and social approachbehavior in Tsc2+/– mice (Supplementary Table 1). These results showthat spatial learning in the Morris water maze was poorer in Tsc2+/–
mice than in WT controls.Because humans affected by tuberous sclerosis may have working
memory deficits7, and because the hippocampus can contribute toworking memory13, we next tested Tsc2+/– mice on a hippocampus-dependent win-shift version of the eight-arm radial maze (Fig. 1b), acommonly used working memory task14. In this task, food-deprivedmice were first allowed to retrieve food pellets from four accessiblearms of an eight-arm maze (phase A). After a retention interval of2 min, mice were brought back to the maze (phase B) and given accessto all eight arms (only the four previously blocked arms were nowbaited). In this task, mice can commit two types of errors: within-phase errors are committed when mice enter an arm previously visitedin the same phase, and across-phase errors are committed when miceenter an arm in phase B that they had already visited in phase A.Although Tsc2+/– mice did not differ from wild-type controls in thenumber of within-phase errors (data not shown), they did makesignificantly more across-phase errors (P ¼ 0.0364; Fig. 1b). Thispattern of errors in the radial arm maze is consistent with deficits inhippocampal function13,14.Discriminating between similar contexts is known to also depend
on hippocampal function15. Mice were trained in context condition-ing with three 0.75-mA shocks and tested in the training context or anovel context (detailed in Methods). WTmice showed clear discrimi-nation between both contexts (Fig. 1c). The freezing responses ofTsc2+/– mice, however, lacked context specificity, confirming hippo-campal dysfunction in these mutants15.
Received 19 November 2007; accepted 27 May 2008; published online 22 June 2008; doi:10.1038/nm1788
1Departments of Neurobiology, Psychiatry & Biobehavioral Sciences, Psychology and the Brain Research Institute, University of California, Los Angeles, 695 Charles E.Young Drive South, Los Angeles, California 90095, USA. 2Center for Human Genetic Research, Massachusetts General Hospital, Harvard Medical School, Richard B.Simches Research Center, 185 Cambridge Street, Boston, Massachusetts 02114, USA. 3Genetics Laboratory, Division of Translational Medicine, Brigham andWomen’s Hospital, Harvard Medical School, 221 Longwood Avenue, Boston, Massachusetts 02115, USA. Correspondence should be addressed to A.J.S.([email protected]).
NATURE MEDICINE VOLUME 14 [ NUMBER 8 [ AUGUST 2008 843
L E T T ERS
©20
08 N
atur
e Pu
blis
hing
Gro
up h
ttp://
ww
w.n
atur
e.co
m/n
atur
emed
icin
e
Effect of Simvastatin on Cognitive Functioning in Children WithNeurofibromatosis Type 1:A Randomized Controlled Trial
Lianne C. Krab, MSc, Arja de Goede-Bolder, MD, Femke K. Aarsen, MA, Saskia M. F. Pluijm,PhD, Marlies J. Bouman, MA, Jos N. van der Geest, PhD, Maarten Lequin, MD, PhD, CorieneE. Catsman, MD, PhD, Willem Frans M. Arts, MD, PhD, Steven A. Kushner, MD, PhD, AlcinoJ. Silva, PhD, Chris I. de Zeeuw, MD, PhD, Henriëtte A. Moll, MD, PhD, and Ype Elgersma, PhDNF1 Core (CognitiveResearch)Team, Departments of General Pediatrics (Ms Krab and Drs DeGoede-Bolder and Moll), Neuroscience (Ms Krab and Drs Van der Geest, De Zeeuw, and Elgersma),Pediatric Neurology (Mss Aarsen and Bouman and Drs Catsman-Berrevoets and Arts); PublicHealth (Dr Pluijm), Pediatric Radiology (Dr Lequin), and Psychiatry (Dr Kushner), Erasmus MCUniversity Medical Center, Sophia Children’s Hospital, Rotterdam, the Netherlands; Departmentsof Neurobiology, Psychiatry, and Psychology, Brain Research Institute, Los Angeles, California (DrsKushner and Silva); and Netherlands Institute for Neuroscience, Royal Academy of Sciences(KNAW), Amsterdam, the Netherlands (Dr De Zeeuw)
AbstractContext—Neurofibromatosis type 1 (NF1) is among the most common genetic disorders that causelearning disabilities. Recently, it was shown that statin-mediated inhibition of 3-hydroxy-3-methylglutaryl coenzyme A reductase restores the cognitive deficits in an NF1 mouse model.
Corresponding Author: Ype Elgersma, PhD, Department of Neuroscience, Erasmus MC, Dr Molewater-plein 50, 3015 GE Rotterdam,the Netherlands ([email protected]).Trial Registration isrctn.org Identifier: ISRCTN14965707Financial Disclosures: Drs Kushner and Silva reported being coapplicants on a US patent (No. 11/569,426) “Treating learning deficitswith inhibitors of HMG-CoA reductase.” None of the other authors reported a potential, real, or perceived conflict of interest or financialdisclosure.Author Contributions: Ms Krab had full access to all of the data in the study and takes responsibility for the integrity of the data andthe accuracy of the data analysis.Study concept and design: Krab, De Goede-Bolder, Aarsen, Pluijm, Lequin, Catsman-Berrevoets, Arts, Kushner, Silva, De Zeeuw, Moll,Elgersma.Acquisition of data: Krab, De Goede-Bolder, Bouman, Lequin, Moll.Analysis and interpretation of data: Krab, De Goede-Bolder, Aarsen, Pluijm, Van der Geest, Kushner, Moll, Elgersma.Drafting of the manuscript: Krab, De Goede-Bolder, Van der Geest, Moll, Elgersma.Critical revision of the manuscript for important intellectual content: Krab, De Goede-Bolder, Aarsen, Pluijm, Bouman, Lequin,Catsman-Berrevoets, Arts, Kushner, Silva, De Zeeuw, Elgersma.Statistical analysis: Krab, Pluijm, Van der Geest.Obtained funding: Krab, De Goede-Bolder, De Zeeuw, Moll, Elgersma.Administrative, technical, or material support: Krab, De Goede-Bolder, Bouman, Van der Geest.Study supervision: De Goede-Bolder, Aarsen, Lequin, Catsman-Berrevoets, Arts, Silva, De Zeeuw, Moll, Elgersma.Additional Contributions: We thank the patients and their parents for their participation. Also, we thank E. Steyerberg, MD, PhD,Department of Public Health, for fruitful discussions, and J. B. C. De Klerk, MD, Department of General Pediatrics and Clinical Genetics,for laboratory safety monitoring. S. J. P. M. Van Engelen, Department of Pediatric Radiology; S. M. Goorden, MSC, M. Elgersma, BSC,P. Plak, BSC, Department of Neuroscience; and A. C. Gaemers, MA, R. Wierenga, MA, E. Barendse, MA, Department of PediatricNeurology, helped in collecting the data. We appreciate the support of all other participants of the NF1 clinical workgroup and the NF1Core (Cognitive Research) Team of the Erasmus MC University Medical Center, Sophia Children’s Hospital Rotterdam, the Netherlands.None of the acknowledged participants received any form of compensation for their contributions.
NIH Public AccessAuthor ManuscriptJAMA. Author manuscript; available in PMC 2009 April 2.
Published in final edited form as:JAMA. 2008 July 16; 300(3): 287–294. doi:10.1001/jama.300.3.287.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Alterations in White Matter Microstructure inNeurofibromatosis-1Katherine H. Karlsgodt1,2*, Tena Rosser4, Evan S. Lutkenhoff3, Tyrone D. Cannon1,2,3, Alcino Silva1,3,5,
Carrie E. Bearden1,2,3
1 Semel Institute for Neuroscience and Behavior, University of California Los Angeles, Los Angeles, California, United States of America, 2Center for Cognitive
Neuroscience, University of California Los Angeles, Los Angeles, California, United States of America, 3Department of Psychology, University of California Los Angeles, Los
Angeles, California, United States of America, 4Children’s Hospital Los Angeles, Los Angeles, California, United States of America, 5Department of Neurobiology,
University of California Los Angeles, Los Angeles, California, United States of America
Abstract
Neurofibromatosis (NF1) represents the most common single gene cause of learning disabilities. NF1 patients haveimpairments in frontal lobe based cognitive functions such as attention, working memory, and inhibition. Due to its well–characterized genetic etiology, investigations of NF1 may shed light on neural mechanisms underlying such difficulties inthe general population or other patient groups. Prior neuroimaging findings indicate global brain volume increases,consistent with neural over-proliferation. However, little is known about alterations in white matter microstructure in NF1.We performed diffusion tensor imaging (DTI) analyses using tract-based spatial statistics (TBSS) in 14 young adult NF1patients and 12 healthy controls. We also examined brain volumetric measures in the same subjects. Consistent with priorstudies, we found significantly increased overall gray and white matter volume in NF1 patients. Relative to healthy controls,NF1 patients showed widespread reductions in white matter integrity across the entire brain as reflected by decreasedfractional anisotropy (FA) and significantly increased absolute diffusion (ADC). When radial and axial diffusion wereexamined we found pronounced differences in radial diffusion in NF1 patients, indicative of either decreased myelination orincreased space between axons. Secondary analyses revealed that FA and radial diffusion effects were of greatestmagnitude in the frontal lobe. Such alterations of white matter tracts connecting frontal regions could contribute to theobserved cognitive deficits. Furthermore, although the cellular basis of these white matter microstructural alterationsremains to be determined, our findings of disproportionately increased radial diffusion against a background of increasedwhite matter volume suggest the novel hypothesis that one potential alteration contributing to increased cortical whitematter in NF1 may be looser packing of axons, with or without myelination changes. Further, this indicates that axial andradial diffusivity can uniquely contribute as markers of NF1-associated brain pathology in conjunction with the typicallyinvestigated measures.
Citation: Karlsgodt KH, Rosser T, Lutkenhoff ES, Cannon TD, Silva A, et al. (2012) Alterations in White Matter Microstructure in Neurofibromatosis-1. PLoSONE 7(10): e47854. doi:10.1371/journal.pone.0047854
Editor: Emanuele Buratti, International Centre for Genetic Engineering and Biotechnology, Italy
Received May 16, 2012; Accepted September 20, 2012; Published October 19, 2012
Copyright: � 2012 Karlsgodt et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This work was supported by the Carol Moss Spivak Foundation and National Institutes of Health grant MH084315 to AS, and the National Institute ofMental Health (R34 MH089299-01 to CEB). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of themanuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Neurofibromatosis Type 1 (NF1) is caused by a mutation in the
neurofibromin gene at locus 17q11.2, and is one of the most
common single-gene genetic disorders (prevalence 1:3000) affect-
ing cognitive function in humans [1]. It is also characterized by
multi-system clinical findings, including including cafe au lait
spots, neurofibromas, scoliosis, bone dysplasias, optic pathway
gliomas and Lisch nodules [2]. However, the accompanying
cognitive deficits lead to significant difficulties in functioning,
particularly in the school environment, and in fact are often the
most significant cause of lifetime morbidity in this population [3].
The NF1 cognitive profile is characterized by severe impairments
in ‘cognitive control’, or the ability to maintain attentional focus
and resist distraction, which is generally considered to be a key
function of the frontal lobe. These cognitive control deficits are
particularly notable in the areas of working memory, cognitive
flexibility, and inhibitory control [1,4,5,6].
About 65% of children with NF1 have sustained attentional
difficulties and 38–50% meet diagnostic criteria for ADHD, with
the vast majority fulfilling criteria for the inattentive subtype [7,8].
In addition, a substantial proportion of individuals with NF1
demonstrate social deficits similar to those observed in autism
spectrum disorders (ASD) [9,10]. Due to its well-characterized
genetic etiology, investigation of the neural mechanisms un-
derlying these deficits in NF1 could shed light on the pathogenesis
of attentional dysfunction and social deficits in the broader
population.
Neurofibromin, the NF1 gene product, appears early during
embryonic development, with high levels of expression in the
brain, suggesting that it is important for the orderly differentiation
of CNS neurons [11]. Gray and white matter volume increases
relative to healthy individuals have been consistently documented,
PLOS ONE | www.plosone.org 1 October 2012 | Volume 7 | Issue 10 | e47854
X
Y
0.063 ∅↑
Z
0.063 ∅↑ 0.063 ∅↓
0.063 ∅↓
X?6?Y | ? || ?
Y?6? Z | ? || ?
X?6? Z | ? || ?
X?? Z | Y || ?
memorystatin
LTPp21Ras
Funding: NIH T32 (5T32EB016640-02) to NM
Potential experiments can be ranked by the extent to which their potential constraints would reduce the set of viable causal graphs.
LTPCA1adult
hippocampal learningmiceadult
GABA inhibitionCA1Adult
K-rasmice
germ line0.063 ↓
0.063 ↓
NF1mice
germ line
0.125 ↓
0.063 ↓
0.063 ↓
PPFCA1Adult
0.063 ↓
I/OCA1Adult
0.063 ↓ N-rasmice
germ line
0.063 ↓
Farnesyl transferasemiceadult
0.063 ↓
doi:10.1038/nature711
Research maps represent and synthesize evidence from biological literature
4 experiment classes 3 causal relations
ExcitatoryNo-connectionInhibitory
Positive InterventionPositive Non-interventionNegative Non-interventionNegative Intervention
A-whatA-whereA-when
B-whatB-whereB-when
C-whatC-whereC-when
D-whatD-whereD-when
A-whatA-whereA-when
B-whatB-whereB-when
C-whatC-whereC-when
D-whatD-whereD-when
ResearchMaps.org is a web app that helps biologists to consider all possible causal interpretations of experimental results by displaying evidence in a concise and intuitive format.
3 results
IncreaseNo changeDecrease
+0−
↑∅↑∅↓↓
1234567890 1234567891 1234567892contrast/necrosis
ratiogliomaEGFR
mutation
Intervention Outcome
Agent Target
Edges in a causal graph predict which statistical (in)dependence relations will be exhibited by the variables in the model.
Unlike mere correlations, causal graphs can be used to predict how a system will behave when it undergoes an intervention.
This work has three aims:
model results in literature with research maps and medicine maps;
use these representations to derive formal causal graphs; and
quantitatively formulate experiment planning as the minimization of causal uncertainty within the model space of causal graphs.
T+ T0 T
A " 5 1 1
A?" 1 1 2
A?# 1 1 2
A # 1 1 1
P(Excitatory) = (1/4)
⇥(5/7)" + (1/4)?" + (2/4)?# + (1/3)#
⇤= 0.449
P(No-connection) = (1/4)
⇥(1/7)" + (1/4)?" + (1/4)?# + (1/3)#
⇤= 0.244
P(Inhibitory) = (1/4)
⇥(1/7)" + (2/4)?" + (1/4)?# + (1/3)#
⇤= 0.307
Edge relation = Excitatory Edge score =0.449 (1/3)
1 (1/3)
= 0.174
1
[1] doi:10.1073/pnas.0801279105
[1]
Research maps: A semantic framework for causal discovery and experiment planning mi2ucla
Nicholas J. Matiasz, MS1,2, Alcino J. Silva, PhD2, William Hsu, PhD11Medical Imaging Informatics (Bioengineering & Radiological Sciences); 2Integrative Center for Learning and Memory (Neurobiology, Psychiatry, & Psychology) — UCLA — Los Angeles, CA
ResearchMaps.org is our related web application that represents causal relations between biological agents and targets.
Linking these applications’ graph databases will allow us to explore the biological mechanisms underlying clinical trial results.
This hybrid system could facilitate collaboration across disciplines.
Intervention
This database schema is implemented in the
graph database Neo4j.
INTERVENTIONa treatment given to a patient who suffers from a condition
a directed relationship that describes an intervention’s effect on an outcome
an operationalized measure of a patient’s response to an intervention
RELATION OUTCOME
Outcome
UserPaper
Can statins treat NF1?
This optional information can contextualize results of clinical trials and possibly explain why a treatment can lead to different outcomes.
EXCITES
HAS_NO_CONNECTION_WITH
INHIBITS
ADDED
INCLUDES
MedicineMaps can show the dominant evidence for relations
Li W, et al. The HMG-CoA reductase inhibitor lovastatin revers-es the learning and attention deficits in a mouse model of neu-rofibromatosis type 1. Current Biology. 2005;15(21):1961–7.
Silva AJ, Landreth A, Bickle J. Engineering the next revolution in neuroscience: The new science of experiment planning. Oxford: Oxford University;2014.
Silva AJ, Müller KR. The need for novel informatics tools for in-tegrating and planning research in molecular and cellular cogni-tion. Learning & Memory. 2015;22(9):494–8.
[1]
[2]
[3]
MedicineMaps
ResearchMaps
MedicineMaps can show the conflicting evidence for relations
Edges in a medicine map
contain properties of the studies that
support the relation.
MedicineMaps summarizes available evidence for treatments and metadata associated with studies to aid experimental design.
By comparing trials methodologically, MedicineMaps facilitates meta-analyses that can contextualize the results of related studies.
As we further develop this app, we will perform usability studies to identify how clinical researchers can use this tool most effectively.
Currently, data is entered manually; we will use this labeled data to train our system to perform semi-automated annotation.
We invite you to visit www.medicinemaps.org to learn more.
Clinical trials on the use of statins in NF1 have had mixed results.
To systematize meta-analytic and methodological analyses, we visualize study results according to properties of their designs.
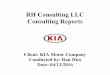
These methodological comparisons highlight, for example, the effect of different statins (lovastatin & simvastatin) on NF1 patients.
By identifying key differences/similarities in studies, researchers can design new studies to resolve unexplained results.
We acknowledge UCLA Clinical and
Translational Science Institute (CTSI) for
funding this project with a Pathfinder Award
(UL1TR000124).
dose: 200 mg
min. age: 19 yrs
This plot shows that the effects of lovastatin across
multiple studies did not differ sharply by the age of the
patient. Excitatory Noconnection
Inhibitory
Perc
enta
ge o
f find
ings
Methodological comparison:findings for lovastatin by age
≥ 18 yrs< 18 yrs
0%
10%
20%
30%
40%
50%
60%