Embed Size (px)
Citation preview

4/7/2013
1
Kristin Walters, MS, RD
Objectives� Overview of bariatric surgery
� Diet progression for post-op bariatric patients
� Prevention of protein malnutrition
� Common vitamin and mineral deficiencies
� Role of the Dietitian
� Current issues in post-op care and treatment
Introduction to Bariatric Surgery� Obesity is a life-threatening
disease affecting 34% of the
adults in the US; and nearly 67%
of the adults in the US are either
overweight or obese. (ASMBS,
2007)
� Between 2000 and 2005, obesity
(BMI> 30) increased by 24%,
morbid obesity (BMI>40)
increased by 50%, super obesity
(BMI> 50) increased by 75%.
(ASMBS, 2007)
Why Bariatric Surgery?� Most effective intervention for severe obesity
� Majority of bariatric surgery patients maintain loss of >50% of excess weight
� Non-surgical treatments of obesity typically results in an average weight loss of 5-10% of initial body weight
� High rates of remission of many obesity-related co-morbidities.

4/7/2013
2
Criteria for Bariatric Surgery� BMI ≥40 without comorbidities
� BMI ≥35 with comorbidities
� Diabetes, obstructive sleep apnea, chronic joint pain, coronary heart disease, hypertension, NAFLD, etc.
� Failed previous attempts at diet and exercise
� No current drug and alcohol dependence
� Free from substantive psychological disease
� Some insurance companies require pre-surgical participation in supervised weight management program.
Gastric Bypass Roux-en-Y� Gold standard (EWL 60-70%)
� Primarily restrictive with some malabsorption
� Modulation of gut hormones� Decreased Ghrelin� Effects on GLP-1, PYY, Leptin
� Strongest potential for improving Type II Diabetes
� Longer term studies available
� Potential Complications� Dumping syndrome� Malabsorption� Micronutrient Deficiencies� Risk of Ulcers (NSAIDS/smoking)� Anastomotic Ulcers
Sleeve Gastrectomy� Primarily restrictive with some malabsorption
� Modulation of gut hormones
� Potential change in Ghrelin and other gut hormones
� Less complicated surgery with no intestinal involvement
� Shorter term studies available
� Weight loss appears to be somewhere between the Roux-en- Y and the gastric band
� Potential Complications
� Gastro-esophageal Reflux Disease
� Nausea/vomiting
� Gastric Ulcers
Adjustable Gastric Band� Purely Restrictive Procedure
� Major marketing promoting surgery
� Less significant weight loss
� Adjustments made via subcutaneous port
� Should be considered permanent if long-
term weight loss is to be achieved.
� Potential Complications� Obstruction
� Ulcers
� Gastro-esophageal Reflux Disease
� Slippage/migration
� Erosion

4/7/2013
3
Biliopancreatic Diversion with Duodenal Switch
� Primarily malabsorptive with some
restriction
� Complicated surgical procedure
� Rarely done at this time
� Significant complications
N. Engl J Med. 2007;357:714-752
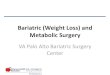
Bariatric Food Guide Pyramid General Diet Progression Guidelines
Stage 1: Clear liquids
- Duration: 1-3 days (hospitalization)
- Low calorie beverages, no sugar, no carbonation, no caffeine
Stage 2: Full liquids
- Duration: Weeks 1-2
- Aim for high protein, low sugar (<15gm) beverages
- Protein shakes, sugar-free pudding, yogurt, and other fuller liquid type foods should
be included to provide appropriate texture, healing, and gut mobility
- Goals:
- Aim for 4-6oz fluids every hour
- 60-80gm protein
- 45-64oz fluids total daily

4/7/2013
4
General Diet Progression Guidelines
� Stage 3A: Pureed diet
� Durations: Weeks 3-4
� Always consume protein foods first
� Do not drink fluids for 30 minutes before and after meals
� Foods to include: protein shakes, pureed meat/poultry, yogurt, cottage cheese,
pureed/peeled fruit and vegetables, sugar-free pudding, cream of wheat/rice
� Stage 3B: Soft diet
� Duration: Weeks 5-6
� Foods to include: ground lean meat, ground skinless poultry (moist!), fish, cottage
cheese, yogurt, low-fat cheese, well-cooked vegetables, fruit (start with peeled)
� Continue with 4-5 small meals per day
General Diet Progression Guidelines
� Stage 4: Regular diet
� Maintenance phase
� Continue with 4-5 small meals per day
� Balanced Meals: protein first, vegetables/fruit, starches (whole
grains), and healthy source of fat
� Avoid rice, bread, and pasta until patient is comfortably consuming at
least 60gm protein
� Chew food thoroughly to the consistency of applesauce
� Take at least 30 minute to complete meals
� Long-term Goal: Reduction of fat mass while maintaining lean body
mass and body composition
Risk of Protein Malnutrition in Bariatric Patient
� Importance of protein� Preserves lean muscle mass
� Plays role in satiety
� Helps with wound healing
� Malabsorption from surgical procedure� Rare
� Length of intestinal limb
� Re-routing of intestine
� Inadequate protein intake� Decreased quantity of food due to pouch size
� Dislike or intolerance to quality protein sources
� Clinical Signs of Protein Malnutrition� Alopecia; Anemia; Impaired wound healing;
Edema
Protein Requirements for the Bariatric Patient
� ASMBS recommend at least 60-80 gm protein per day
� 1.1 – 1.3 g/kg for body weight at BMI of 25
� Example Calculation:
� 40 y/o female
� Ht: 5’6”
� Wt: 198 lbs/ 90 kg
� BMI at 25: 155 lbs/ 70.45kg
� 1 – 1.3 g/kg X 70.45kg = 70 -90 g of Protein/ day

4/7/2013
5
Treatment and Prevention of
Protein Malnutrition
� Diet
� Determine protein needs
� Identify high-quality protein sources
� Food
� Always include protein at every meal and snack
� Protein supplements
� Deficiency may occur within 3-6 months after surgery
� Degree of PM may require hospitalization (rare)
� Enteral nutrition
� Parenteral nutrition
Protein Supplements� Considerations when recommending a protein supplement
� Protein source should be the main ingredient in the product
� Whey protein (isolate and concentrate)
� Soy protein isolates
� Soy
� Egg
� Avoid collagenic protein
� Nutrition profile of product should include:
� Less than 200 calories
� Less than 6 g of sugar
� Less than 4 g of fat
� Between 20 - 30 g of protein
Potential Nutrition-related
Complications� Dumping Syndrome
� Loss of pyloric sphincter actions
� Symptom include: diarrhea, nausea, dizziness, weakness, rapid pulse, cold sweats, fatigue, and
cramps
� Prevention: avoid high sugar/fat foods, chew food well, eat slowly, watch portion sizes, and avoid
liquids with meals
� Nausea and vomiting� Most likely eating/drinking related (meal size, chewing, speed of eating, fluids with meals)
� Less likely: stenosis, pregnancy, obstruction
� Dehydration� Signs: dark urine, dizziness, nausea, fatigue
� 48-64oz fluids daily
� Diarrhea� Lactose Intolerance
� Food Sensitivity
� Dumping Syndrome
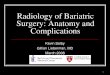
Micronutrient Deficiencies
Strohmayer 2010

4/7/2013
6
Vitamin and Mineral Deficiencies
� Postoperatively, 28%–59% of all types of
bariatric surgical patients report symptoms
of micronutrient deficiency, including hair
loss, dry skin, muscle pain, and fatigue,
within the first year after surgery.
� Onset is often insidious
� Persistent life-long surveillance for
deficiencies is needed
� Potential causes:• Altered absorption• Decreased gastric acid • Bypass areas of absorption (RNY)• Non-compliance with supplements• Poor food tolerance• Avoidance of micronutrient rich foods Jejeeboy 2002
Vitamin B12� Prevalence: 33-75% after surgery. Able to store in large
amounts so deficiency may not show up for years.
� Incomplete digestion and release of B12 from food r/t
decrease in hydrochloric acid
� Intrinsic factor is produced by parietal cells of the stomach and
impaired production with bariatric surgery.
� Must rely on passive absorption of B12 : sublingual and IM
� Deficiency often presents with non-specific symptoms such as
weakness, fatigue, and irritability. May progress to
paresthesias in the hands or feet.
Folic Acid (Folate)� Depletion within a few months after surgery. Decreased
intake of folic acid-fortified foods.
� Deficiency can lead to macrocytic anemia, leukopenia, thrombocytopenia, and glossitis.
� Less common than B12 deficiency because adequate amounts are found in most multivitamins.
� Pregnant, and those thinking about becoming pregnant, need to be especially aware of folic acid.
Vitamin B1 (Thiamin)� Generally considered rare, but has been reported in a number
of bariatric surgery patients.
� Essential coenzyme in carbohydrate metabolism and deficiency can result in impaired nerve conduction.
� Stored in small amounts in the body. Requires daily replenishment. Acute deficiencies can occur as soon as 1 to 3 months after surgery
� Most common among all surgical patients with frequent vomiting.
� Early symptoms may include anorexia, gait ataxia, muscle cramps, or irritability. Untreated deficiency can lead to beriberi, peripheral neuropathy, Wernicke encephalopathy, and/or Korsakoff psychoses.

4/7/2013
7
Vitamin A� Involved in immunological activity, cellular proliferation
and plays a role in visual acuity
� Potential deficiency in gastric bypass and duodenal switch patients r/t bypassing upper small intestine where fat-soluable vitamins are primarily absorbed.
Calcium� Increased long-term risk of metabolic bone disease has been
well documented in gastric bypass patients.
� Fewer studies have been done with sleeve and band patients.
� Symptoms of deficiency include leg cramping, osteoporosis, and neuromuscular hyperexcitability.
� Calcium citate is more effectively absorbed than calcium carbonate by 22-27%.
Vitamin D� Most common deficiency prior to surgery. Deficiency
appears to be related to morbid obesity.
� Deficiency linked to increased risk of osteoporosis, cancers (colon, breast, prostate), chronic inflammatory diseases, metabolic disorders, and peripheral vascular disease.
Iron� Most common deficiency
� Reports of deficiency range from 20%-50% of post-op bariatric patients.
� Cause: decreased absorption and decreased intake of high iron foods after surgery.
� Symptoms: fatigue, palpitations, anemia, koilonychia (spoon nails), pica, and brittle hair.

4/7/2013
8
Zinc, Selenium, Copper� Rare deficiencies
� Zinc is absorbed in both the duodenum and proximal jejunum and is involved in over 200 enzyme systems, including wound healing and immunity.
� Selenium is a part of the enzyme glutathione peroxidase which protects cells from free radical damage.
� Copper is a trace metal that is absorbed in the stomach and proximal duodenum. Deficiency is rare and symptoms often mimic B12 deficiency.
Vitamin and Mineral SupplementationRYGB Sleeve Band Long Bypass*
Multi-vitamin (include
iron, folate, selenium,
copper, and zinc)
Two serving size daily One serving size daily One serving size daily Two serving size daily
Thiamine (B-1) 50 mg 3x/ wk 50mg 3x/wk for first 6 months
50mg 3x/wk for first 6 months
50mg 3x/wk
B-12 Sublingual 1000mcg 3x/ wk –OR-
1 (1000mcg) IM q month
Sublingual 1000mcg 3x/ wk –OR-
1 (1000mcg) IM q month
Sublingual 1000mcg 3x/ wk –OR-
1(1000mcg) IM q month
Calcium Citrate
(Divide Doses;
separate from iron)
1500-1700 mg daily 1500-1700 mg daily 1000-1200 mg daily 1800-2000 mg daily
Vitamin D 2,000 units dailyIncludes MVI, Calcium/D
1,000 units dailyIncludes MVI, Calcium/D
1,000 units dailyIncludes MVI, Calcium/D
2,000 units dailyIncludes MVI, Calcium/D
Vitamin A
(Beta Carotene)
25,0000 IU/ weekOr 5,000 IU in Multi-vitamin
25,000 IU/week
Post-op LabsYearly Post-op Labs
� CBC
� Creatinine
� BUN
� Electrolytes
� Calcium
� PTH
� Liver Panel
� Fasting Glucose
� Lipid Panel
� Iron panel
� Albumin
� Thiamine
� Vitamin A
� Vitamin D (25 OH)
� Vitamin B-12
� Thiamine
� Folic Acid
Role of the Dietitian� Essential member of bariatric team.
� Educate and counsel patients on what to expect after surgery
� Help patients set reasonable weight loss goals
� Assess and monitor dietary intake and determine whether patient is meeting nutrient goals
� Assist in selection of foods that decrease gastrointestinal symptoms and maximize weight loss
� Assist patient with food tolerance difficulties by customizing the diet progression
� Monitor for signs of micronutrient deficiencies

4/7/2013
9
Current Issues in Bariatric Treatment� Pregnancy within the first year post-op
� Renal and/or dialysis patient and bariatric surgery
� The bariatric patient and weight regain
� Reactive hypoglycemia after bariatric surgery
� The bariatric patient and eating disorders
� Bariatric surgery and the impact on co-morbid conditions
� The bariatric patient and cross addiction
� Alcohol
� Opiates
� Hospitalization and the bariatric patient
� Improving continuum of care by increasing awareness and knowledge of medical professionals
Conclusion� Dietitians are an important member of the bariatric team
� It is important that all dietitians have a general understanding of bariatric surgery and the post-op needs.
� With an ever growing weight loss surgery population the RD is going to play a vital role in guiding the care team in terms of diet and supplementation.
ReferencesAllis,L, et al. ASMBS allied health nutritional guidelines for the surgical weight loss patient. Surgery for Obesity and Related Diseases. Vol 4, pp s73-s108, 2008.
Avinoah, E., Ovnat, A., &Charuzi, I. (1993, June). Nutritional status seven years after Roux-en-Y gastric bypass surgery. Surgery, 111(2), 137-42.
Buchwald, H. (2004). 2004 ASBS Consensus Conference Statement Bariatric surgery for morbid obesity: Health implications for patients, health professionals, and third-party payers. J
Am Coll Surg 200:593– 604.
Carlin, A.M., Rao, D.S., &Meslemani, A. (2005, December). Prevalence of vitamin D depletion among morbidly obese patients seeking gastric bypass surgery. Bone & Mineral Research
Laboratory.
Cleveland Clinic. 2005. Co-morbid Reduction after bariatric surgery. Retrieved March 13, 2011 from http://weightloss.clevelandclinic.org/images/Reduction3.gif
Dobratz JR, Earthman CP. (2006) Review of protein status and body composition after gastric bypass surgery and very low-calorie diet therapy. Bariatric Nurse Surg Pt Care.; 1 (3): 195-
204.
FAO/WHO Expert Consultation. (1991) Protein Quality Evaluation: Food and Agriculture Organization of the United Nations Rome: Food and Agriculture Organization. FAO Food and
Nutrition Paper, No. 51.
Frank, L. (2008) Protein and the Bariatric Patient. Bariatric Times.
Global Trends in Bariatric Surgery Graph. (2010). Retrieved March 13, 2011 at http:/’lukasz-marciniak.pl/hp-admin/bariatric-surgery-statistics-2010&pg6
Groff JL, Gropper SS.(2000) Advanced Nutrition and Human Metabolism. 3rd Ed. Belmont, CA: Wadsworth.
Hutter et al (2011). First Report from the American College of Surgeons – Bariatric Surgery Center Network: Laparoscopic Sleeve Gastrectomy has Morbidity and Effectiveness Positioned
Between the Band and the Bypass. Ann Surg. 254(3): 410–422.
ReferencesJacques J. (2007)Protein Basics. Bariatric Times; 4(4): 24-28.
Jacques, J. (2006) Micronutritionfor the weight loss surgery patient. Matrix Medical Communications.
Kulick, D, et al. (April 2010) The bariatric surgery patient: a growing role for registered dietitians. JADA Vol 110, no 4, pp 593-599.
Kerstyn, C.Z., Miller, W.M., & Franklin, B. (2011). Vitamin A Deficiency after Gastric Bypass Surgery: An Underreported Postoperative Complication. Journal of Obesity,
2011(760695), 4.
Kushner, R. & Neff, L. (2010). Bariatric Surgery: A Key Role for Registered Dietitians. Journal of the American Dietetic Association. Doi: 10.1016/j.jada.2009.12.030
Mechanich, J, etal. (July 2008). American association for clinical endocrinologists, the obesity society, and American society for metabolic and bariatric surgery medical
guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocrine Practice Vol 14,
No1, pp 1-60.
Manzanares, M. (2011)Protein and the Bariatric Patient. Kaiser Permanente Post- Op Bariatric Nutrition Care Webinar. 2011 1st Quarter Presentation.
Miller, R. & Choban, P. (2011). Surgical Management of Obesity: Current State of Procedure Evoluation and Strategies to Optimize Outcomes. Nutrition in Clinical
Practice, 26: 526.
O’Donnell, K. (May 2008). Small but Mighty: Selected Micronutrient Issues in Gastric Bypass Patients. Nutrition Issues in Gastroenterology, Series # 62. Practical
Gastroenterology. Pp. 37-48.
Peluso, L. (2007). Efficacy of Gastric Bypass in the Treatment of Obesity-Related Co morbidities. NutrClinPract 2007 22: 24- 28.
Radigan, A.( 2004). Post-Gastrectomy: Managing Nutrition Fall-Out. Practicial Gastroenterology: June 2004. pp. 63- 75.
Shikora, S. et al. (2007). Nutrition and Gastrointestinal Complications of Bariatric Surgery. Nutr Clinical Pract 2007 22: 29-40.

4/7/2013
10
ReferencesShils, M. et al. (2005) Modern Nutrition in Health and Disease, 10th edition. Philadephia: Lippincott Williams and Wilken.
Stocker, DJ. Management of the bariatric surgery patient. EndocrinolMetabClin North America. 2003; 32: 437-457.
Strohmayer et al. (2010). Metabolic Management following Bariatric Surgery. Mount Sinai Journal of Medicine, 77:431-445.
Snyder-Marlow, G, et al. (April 2010) Nutrition Care for patients undergoing laproscopic sleeve gastrectomy for weight loss. JADA. Vol 110, No 4, pp 600-607.
Taylor, K.( 2007). Obesity in America. American Society for Metabolic and Bariatric Surgery. Retrieved March 13, 2011 at
http://www.asbs.org/Newsite07/media/asmbs_fs_obesity.pdf
Vetter, M.L., Cardillo, S., &Rickels, M.R. (2004). Narrative Review: Effect of Bariatric Surgery on Type 2 Diabetes Mellitus. Pysiology in Medicine, 23. Retrieved March
1, 2011 fromhttp://www.annals.org/content/150/2/94.abstract
Vitamin deficiency in gastric bypass/duodenal switch-BPD. Retrieved February 3, 2011 Message posted to http://gastricbypass.netfirms.com/vitamins.htm
Von Drygalski, A., Andris, D.A. (2009). Anemia after Bariatric Surgery: More than Just Iron Deficiency. NutrClinPract 2009 24: 217- 226.
Wikipedia. (2011). Gastric Bypass Surgery. Retrieved February 3, 2011 from http://en.wikipedia.org/wiki/Gastric_bypass_surgery