Embed Size (px)
Citation preview
Washington State Health Reform
Quarterly MeetingNorthwest Portland Area Indian Health Board
January 20, 2015
Agenda1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
Background Coming Changes Planning Calendar Possible System Models Possible Service Models Other Questions Comments – January 5, 2014
2. Accountable Communities of Health Background Comments – January 5, 2014
3. Governor’s Health Innovation Leadership Network Seeking recommendations for Tribal Representative and Urban
Indian Organization Representative2

BACKGROUND
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
3
• Since early 1990s, Medicaid transitioning beneficiaries to health plans with CMS approval
• Today, over 90% of full-benefit Medicaid eligibles covered through Apple Health Managed Care Plans
• State pays PMPM (per-member, per-month) to Plans with defined set of benefits for defined groups —each Plan is fully “at risk”* for care of assigned population
• Currently, Apple Health Managed Care Plans cover physical health care services and mental health care services below the access to care standard
*”at risk” means that the MCO is paid a per member per month (PMPM) rate to provide the full array of services they are under contract for. If the MCO spends more than it receives from HCA, the MCO loses money. If the MCO spends less than it receives, the MCO can keep a portion of this money. CMS requires the PMPM to be an actuarial rate and HCA to monitor and incentivize MCOs to ensure appropriate care is provided to clients. 4
Apple Health (Medicaid) Managed Care
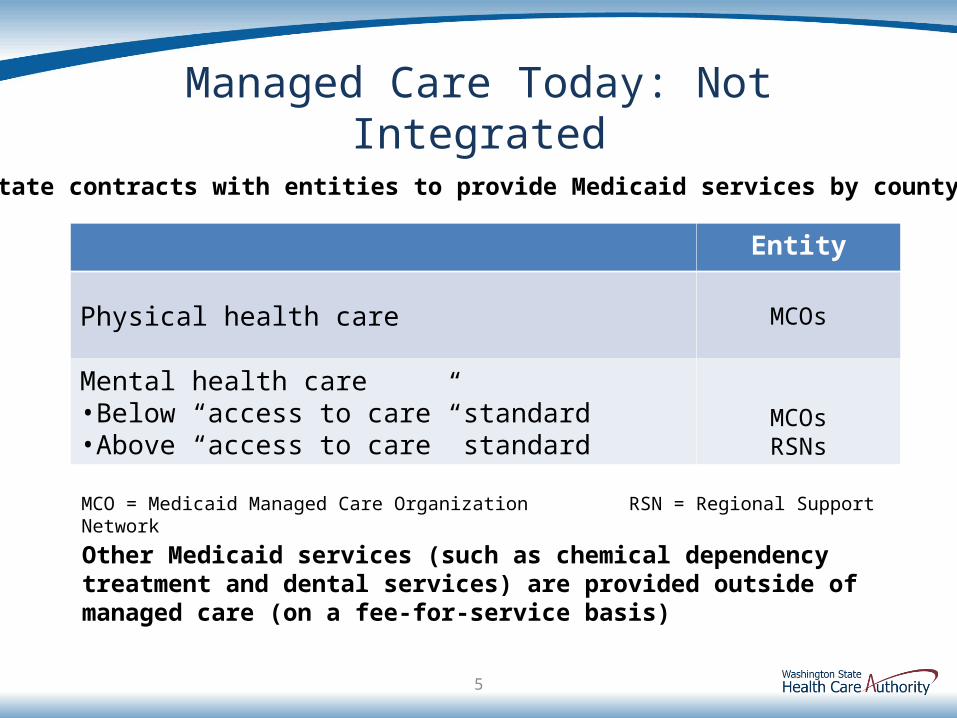
Managed Care Today: Not Integrated
5
Entity
Physical health care MCOs
Mental health care•Below “access to care” standard•Above “access to care” standard
MCOsRSNs
MCO = Medicaid Managed Care Organization RSN = Regional Support Network
State contracts with entities to provide Medicaid services by county
Other Medicaid services (such as chemical dependency treatment and dental services) are provided outside of managed care (on a fee-for-service basis)
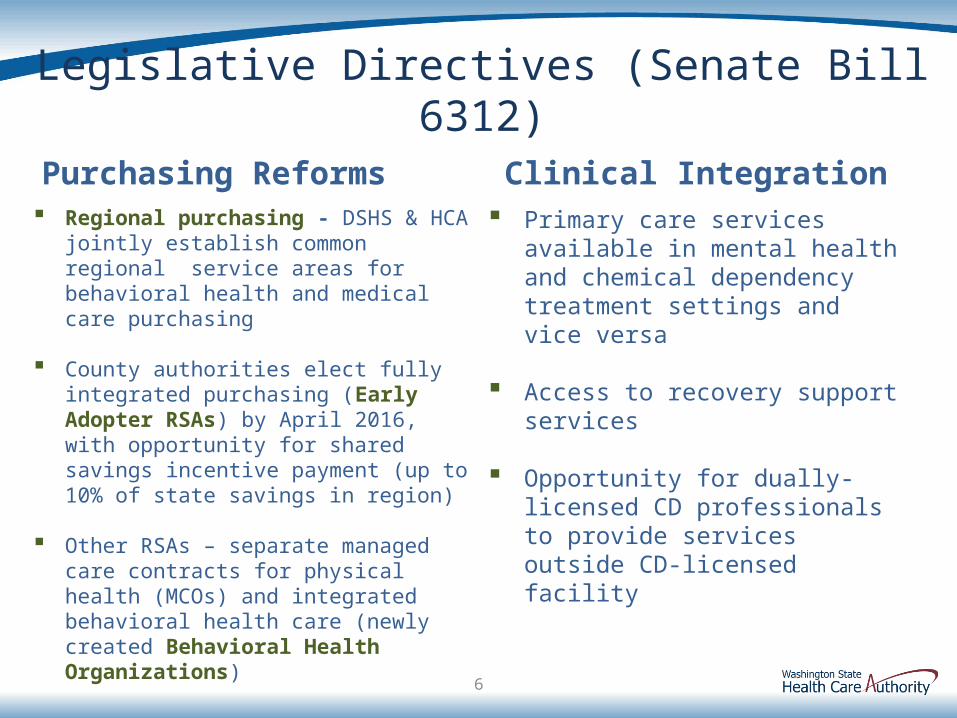
Legislative Directives (Senate Bill 6312)
Purchasing Reforms Regional purchasing - DSHS & HCA jointly
establish common regional service areas for behavioral health and medical care purchasing
County authorities elect fully integrated purchasing (Early Adopter RSAs) by April 2016, with opportunity for shared savings incentive payment (up to 10% of state savings in region)
Other RSAs – separate managed care contracts for physical health (MCOs) and integrated behavioral health care (newly created Behavioral Health Organizations)
Clinical Integration Primary care services available in
mental health and chemical dependency treatment settings and vice versa
Access to recovery support services
Opportunity for dually-licensed CD professionals to provide services outside CD-licensed facility
6
Goals: Integrated Purchasing of Managed Care
• Provide more holistic, better managed care for people with co-occurring disorders.
• Support seamless access to services with standards and medical necessity guidelines in one system, without “access to care” standard.
• Improve ability to monitor quality across all providers Quality metrics in managed care contracts
Sanctions for specific performance measures.
• Align financial incentives for expanded prevention and treatment and improved outcomes across physical and behavioral health systems.
• Create system for interdisciplinary care teams that are accountable for full range of physical and behavioral health services.
• Improve information and administrative data sharing, making relevant information more available to multidisciplinary care team.
7

COMING CHANGES
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
8
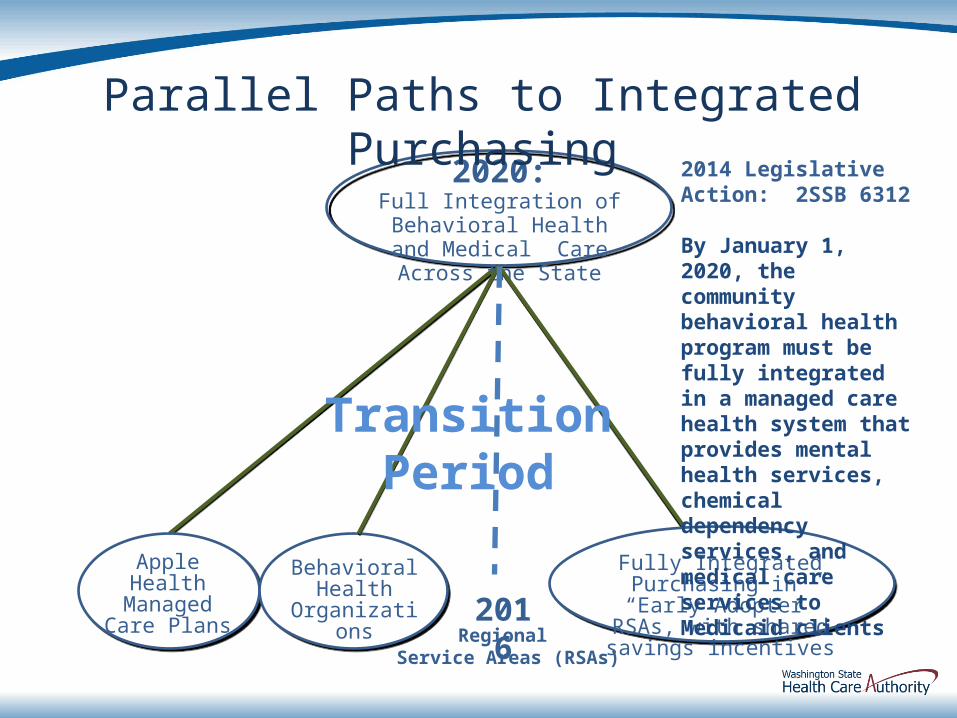
2020:Full Integration of Behavioral
Health and Medical Care Across the State
Behavioral Health
Organizations
Apple Health Managed Care
Plans 2016
Transition Period
Parallel Paths to Integrated Purchasing
Regional Service Areas (RSAs)
Fully Integrated Purchasing in “Early Adopter” RSAs, with shared savings incentives
2014 Legislative Action: 2SSB 6312
By January 1, 2020, the community behavioral health program must be fully integrated in a managed care health system that provides mental health services, chemical dependency services, and medical careservices to Medicaid clients
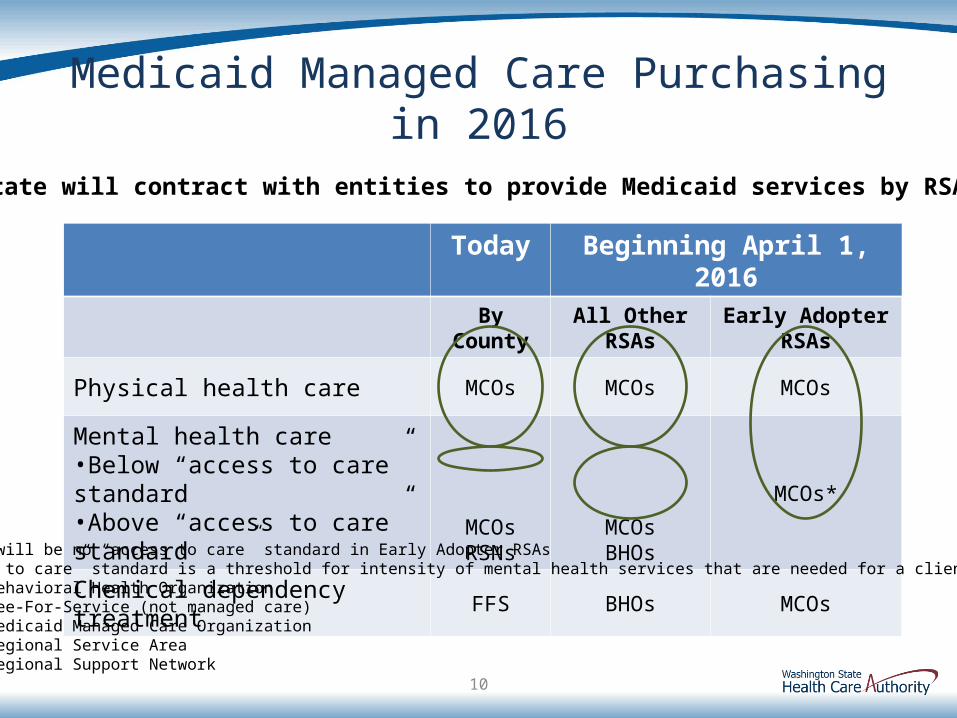
Medicaid Managed Care Purchasing in 2016
10
Today Beginning April 1, 2016
By County All Other RSAs Early Adopter RSAs
Physical health care MCOs MCOs MCOs
Mental health care•Below “access to care” standard•Above “access to care” standard
MCOsRSNs
MCOsBHOs
MCOs*
Chemical dependency treatment FFS BHOs MCOs
*There will be no “access to care” standard in Early Adopter RSAs“Access to care” standard is a threshold for intensity of mental health services that are needed for a client.BHO = Behavioral Health OrganizationFFS = Fee-For-Service (not managed care)MCO = Medicaid Managed Care OrganizationRSA = Regional Service AreaRSN = Regional Support Network
State will contract with entities to provide Medicaid services by RSA
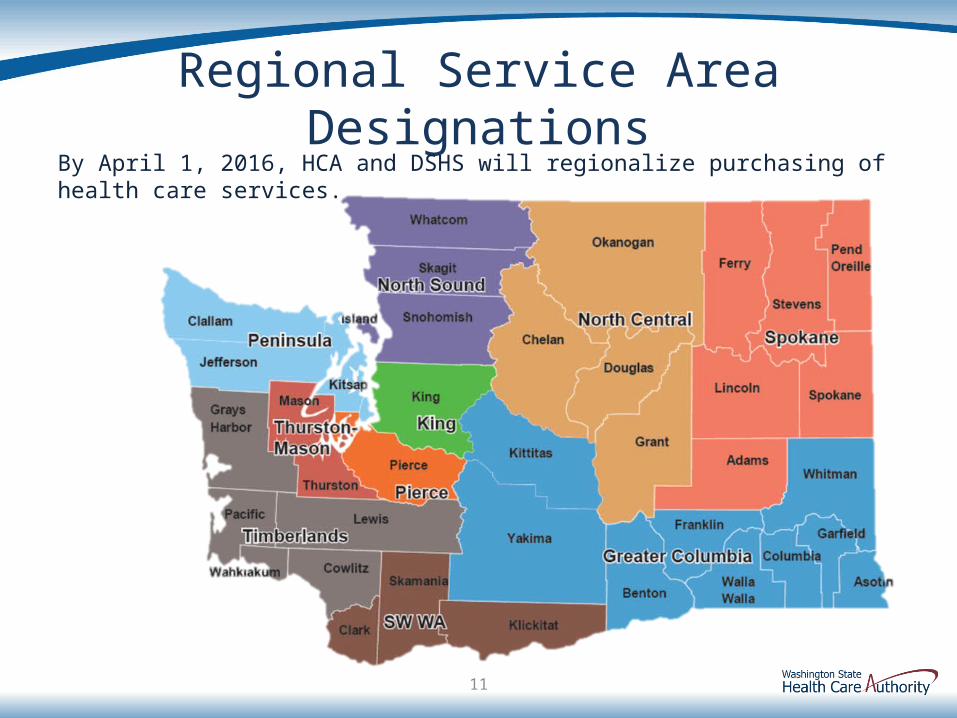
Regional Service Area Designations
By April 1, 2016, HCA and DSHS will regionalize purchasing of health care services.
11
North Central RSA in Transition
Transitional two-RSA approach for counties presently served by the Chelan-Douglas and Spokane RSNs:
• Apple Health Managed Care: New North Central RSA separate from Spokane RSA
• BHO: Single BHO will serve new North Central and Spokane RSAs during the transition
• 2020 Full Integration: Fully integrated managed care is required in 2020 by Senate Bill 6312. North Central and Spokane RSAs will be separate regions for purposes of integrated physical and behavioral health managed care systems in 2020.
12
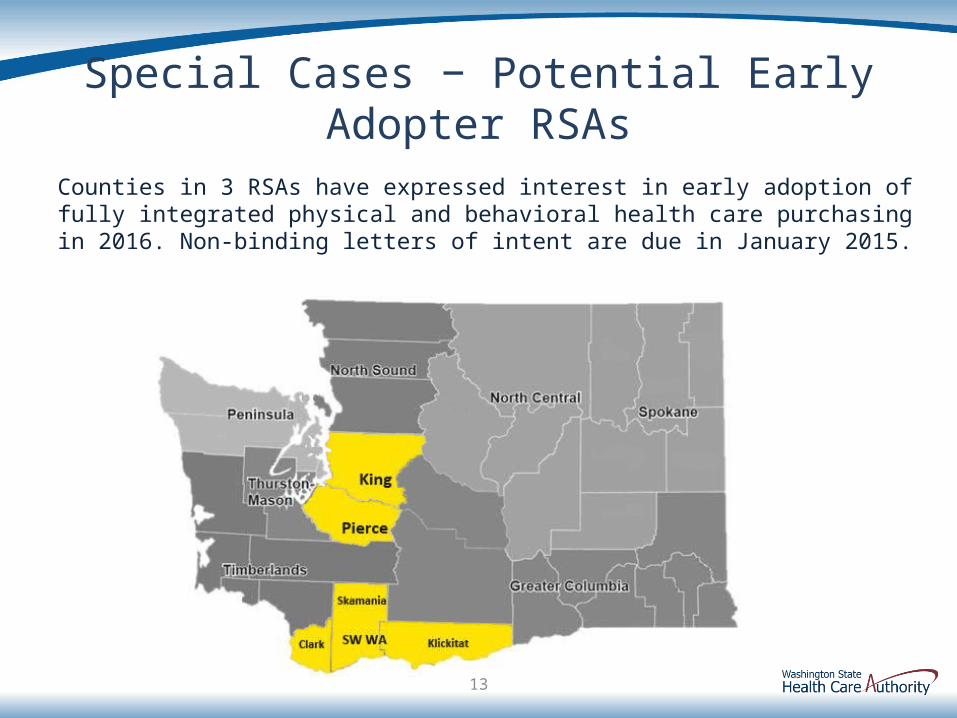
Special Cases − Potential Early Adopter RSAs
Counties in 3 RSAs have expressed interest in early adoption of fully integrated physical and behavioral health care purchasing in 2016. Non-binding letters of intent are due in January 2015.
13
Medicaid Purchasing in “Early Adopter” RSAs• Standards being developed jointly by HCA and DSHS• County authorities in an RSA must agree to
become Early Adopter RSAs• Procurement process will be necessary to select
MCOs• Compliance with Medicaid and State managed care
contracting requirements• Shared savings incentives
• Payments to Early Adopter counties targeted at 10% of savings realized by the State, based on outcome and performance measures
• Available for up to 6 years or until fully integrated purchasing occurs statewide
• Models continue to be discussed broadly
Some Criteria for MCO Early Adopter Participation
Managed care organizations must:
•Meet network adequacy standards established by HCA and pass readiness review
o Provide full continuum of comprehensive services, including critical provider categories (e.g., primary care, pharmacy, and behavioral health)
o Ensure no disruption to ongoing treatment regimens
•Be licensed as an insurance carrier by the Office of the Insurance Commissioner
•Meet quality, grievance and utilization management and care coordination standards and achieve NCQA accreditation by December 2015
15
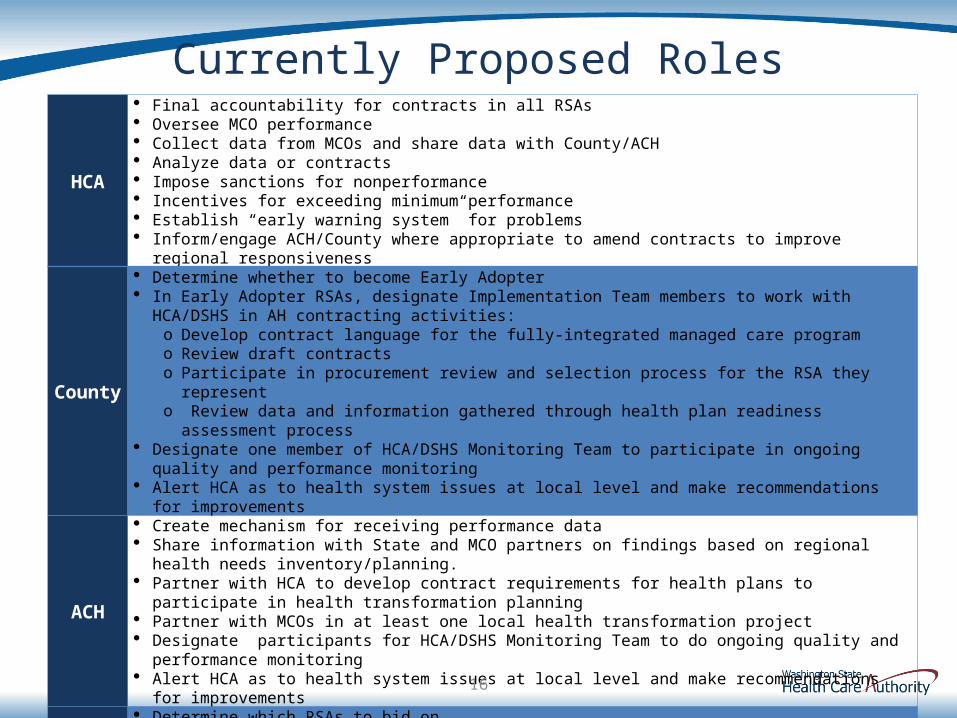
Currently Proposed Roles
HCA
Final accountability for contracts in all RSAs Oversee MCO performance Collect data from MCOs and share data with County/ACH Analyze data or contracts Impose sanctions for nonperformance Incentives for exceeding minimum performance Establish “early warning system” for problems Inform/engage ACH/County where appropriate to amend contracts to improve regional responsiveness
County
Determine whether to become Early Adopter In Early Adopter RSAs, designate Implementation Team members to work with HCA/DSHS in AH contracting
activities: o Develop contract language for the fully-integrated managed care program o Review draft contractso Participate in procurement review and selection process for the RSA they represento Review data and information gathered through health plan readiness assessment process
Designate one member of HCA/DSHS Monitoring Team to participate in ongoing quality and performance monitoring
Alert HCA as to health system issues at local level and make recommendations for improvements
ACH
Create mechanism for receiving performance data Share information with State and MCO partners on findings based on regional health needs inventory/planning. Partner with HCA to develop contract requirements for health plans to participate in health transformation planning Partner with MCOs in at least one local health transformation project Designate participants for HCA/DSHS Monitoring Team to do ongoing quality and performance monitoring Alert HCA as to health system issues at local level and make recommendations for improvements
MCO
Determine which RSAs to bid on Supply network information in all RSAs Supply response to RFP in Early Adopter RSAs Pass readiness review Partner with ACH in at least one local health transformation project Participate in ongoing meetings of ACH
16
PLANNING CALENDAR
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
17
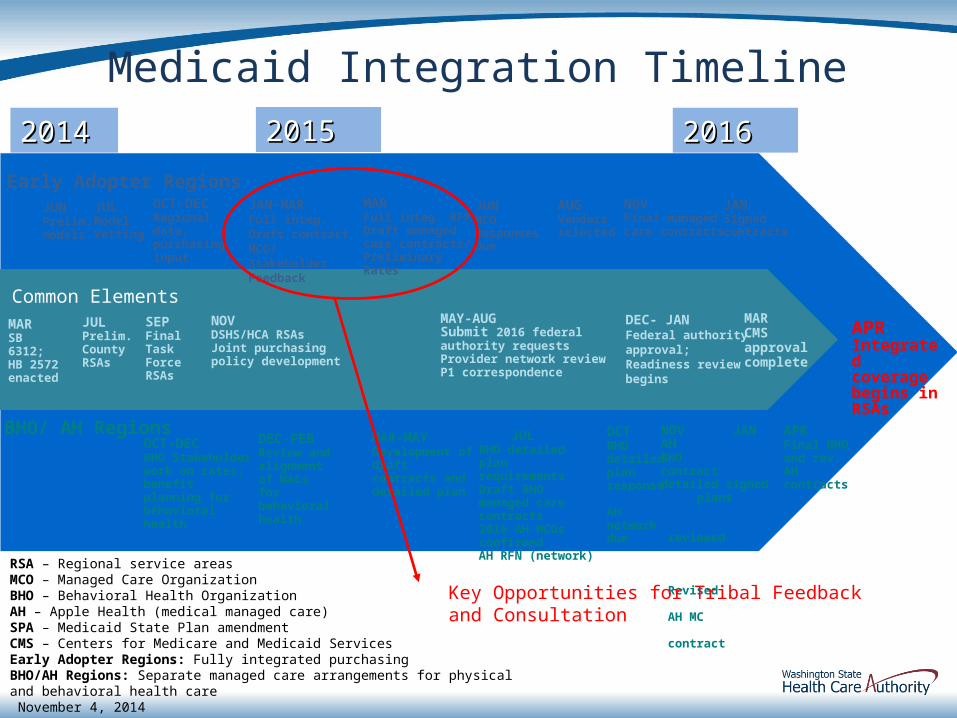
RSA – Regional service areasMCO – Managed Care OrganizationBHO – Behavioral Health OrganizationAH – Apple Health (medical managed care)SPA – Medicaid State Plan amendmentCMS – Centers for Medicare and Medicaid ServicesEarly Adopter Regions: Fully integrated purchasingBHO/AH Regions: Separate managed care arrangements for physical and behavioral health care November 4, 2014
Early Adopter RegionsJUNPrelim. models
20142014
JULModel Vetting
JAN-MARFull integ. Draft contract MCO/Stakeholder Feedback
MAR SB 6312; HB 2572 enacted
JULPrelim.County RSAs
SEPFinal Task Force RSAs
20152015
MAY-AUGSubmit 2016 federal authority requests Provider network reviewP1 correspondence
DEC- JANFederal authority approval; Readiness review begins
MAR Full integ. RFP Draft managed care contracts/ Preliminary Rates
JUNMCO Responses Due
NOVFinal managed care contracts
JANSignedcontracts
JULBHO detailed plan requirementsDraft BHO managed care contracts2016 AH MCOs confirmedAH RFN (network)
OCTBHO detailed plan response
AH network due
APR Integrated coverage begins in RSAs
BHO/ AH Regions
NOVDSHS/HCA RSAsJoint purchasing policy development
20162016
NOV JANAH BHO contract detailed signed plans reviewed
Revised AH MC contract
MARCMS approval complete
APRFinal BHO and rev. AH contracts
Common Elements
OCT-DECRegional data; purchasing input
AUGVendors selected
OCT-DECBHO Stakeholder work on rates; benefit planning for behavioral health
DEC-FEB Review and alignment of WACs for behavioral health
MAR-MAYDevelopment of draft contracts and detailed plan
Medicaid Integration Timeline
Key Opportunities for Tribal Feedback and Consultation
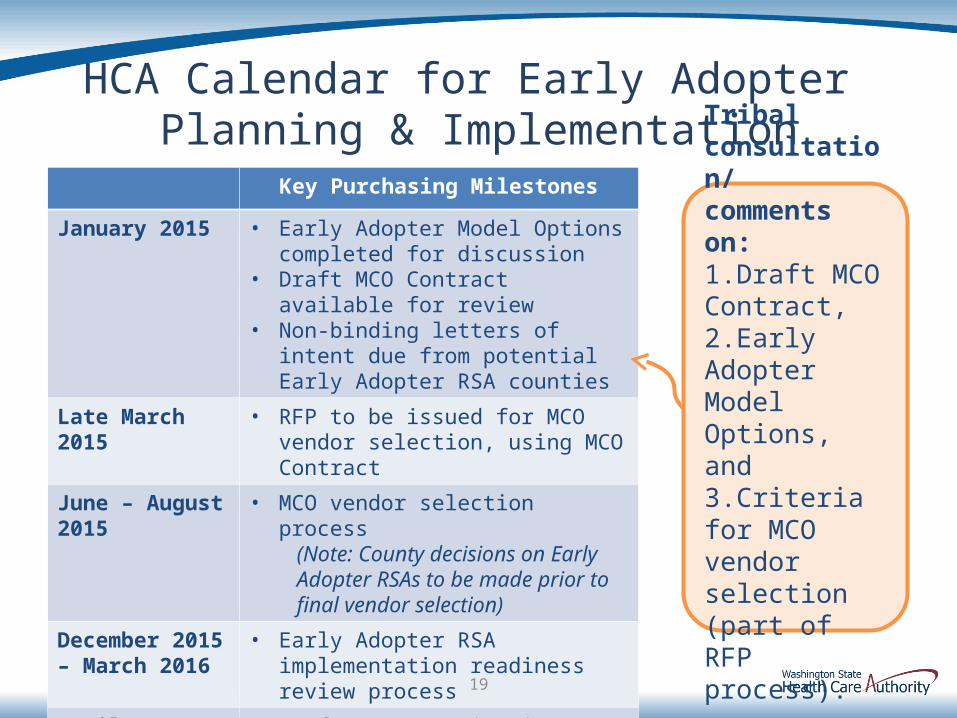
HCA Calendar for Early Adopter Planning & Implementation
Key Purchasing Milestones
January 2015 • Early Adopter Model Options completed for discussion
• Draft MCO Contract available for review • Non-binding letters of intent due from
potential Early Adopter RSA counties
Late March 2015 • RFP to be issued for MCO vendor selection, using MCO Contract
June – August 2015 • MCO vendor selection process (Note: County decisions on Early Adopter RSAs to be made prior to final vendor selection)
December 2015 – March 2016
• Early Adopter RSA implementation readiness review process
April 2016 • Performance monitoring begins
19
Tribal consultation/comments on: 1.Draft MCO Contract, 2.Early Adopter Model Options, and 3.Criteria for MCO vendor selection (part of RFP process).
POSSIBLE SYSTEM MODELS
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
20
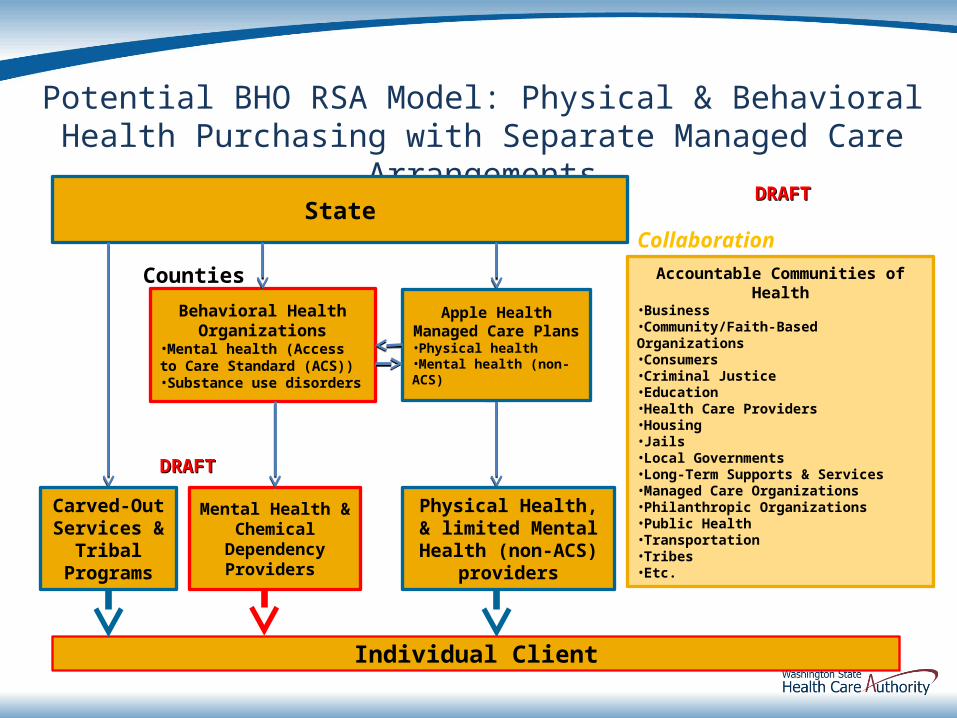
Potential BHO RSA Model: Physical & Behavioral Health Purchasing with Separate Managed Care Arrangements
State
Mental Health & Chemical
Dependency Providers
Individual Client
Collaboration
Behavioral Health Organizations
•Mental health (Access to Care Standard (ACS))•Substance use disorders
Apple HealthManaged Care Plans
•Physical health•Mental health (non-ACS)
Counties
DRAFTDRAFT
DRAFTDRAFT
Physical Health, & limited Mental Health (non-ACS) providers
Carved-Out Services &
Tribal Programs
Accountable Communities of Health•Business•Community/Faith-Based Organizations•Consumers•Criminal Justice•Education•Health Care Providers•Housing•Jails•Local Governments•Long-Term Supports & Services•Managed Care Organizations•Philanthropic Organizations•Public Health•Transportation•Tribes•Etc.
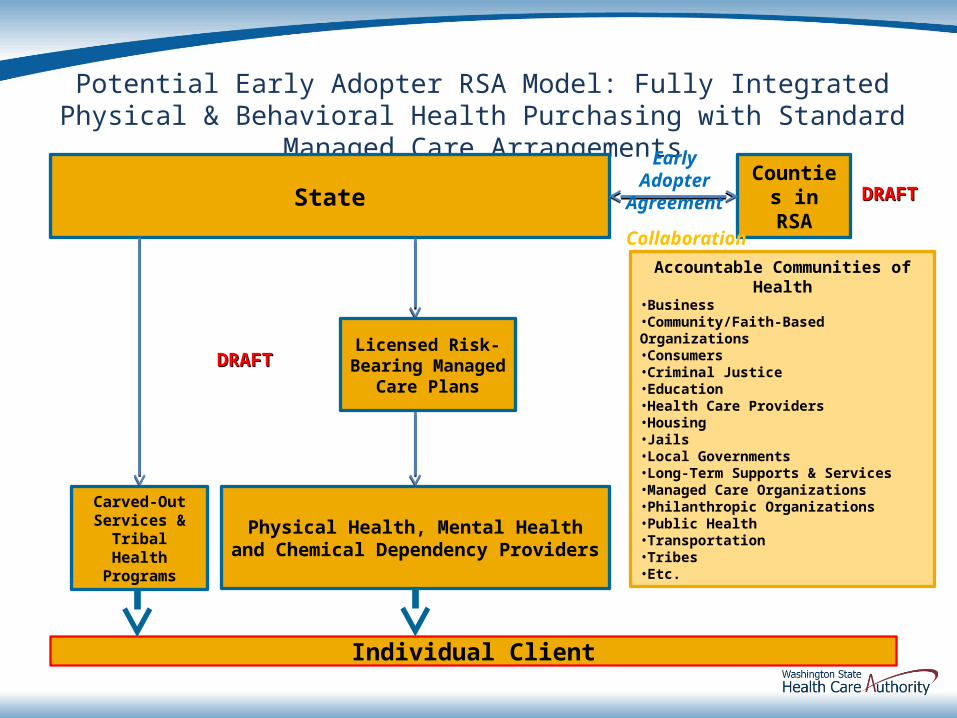
Potential Early Adopter RSA Model: Fully Integrated Physical & Behavioral Health Purchasing with Standard Managed Care Arrangements
State
Physical Health, Mental Health and Chemical Dependency Providers
Accountable Communities of Health•Business•Community/Faith-Based Organizations•Consumers•Criminal Justice•Education•Health Care Providers•Housing•Jails•Local Governments•Long-Term Supports & Services•Managed Care Organizations•Philanthropic Organizations•Public Health•Transportation•Tribes•Etc.
Individual Client
Licensed Risk-Bearing Managed
Care Plans
Carved-Out Services &
Tribal Health Programs
DRAFTDRAFT
DRAFTDRAFTCounties in RSA
Collaboration
Early Adopter Agreement
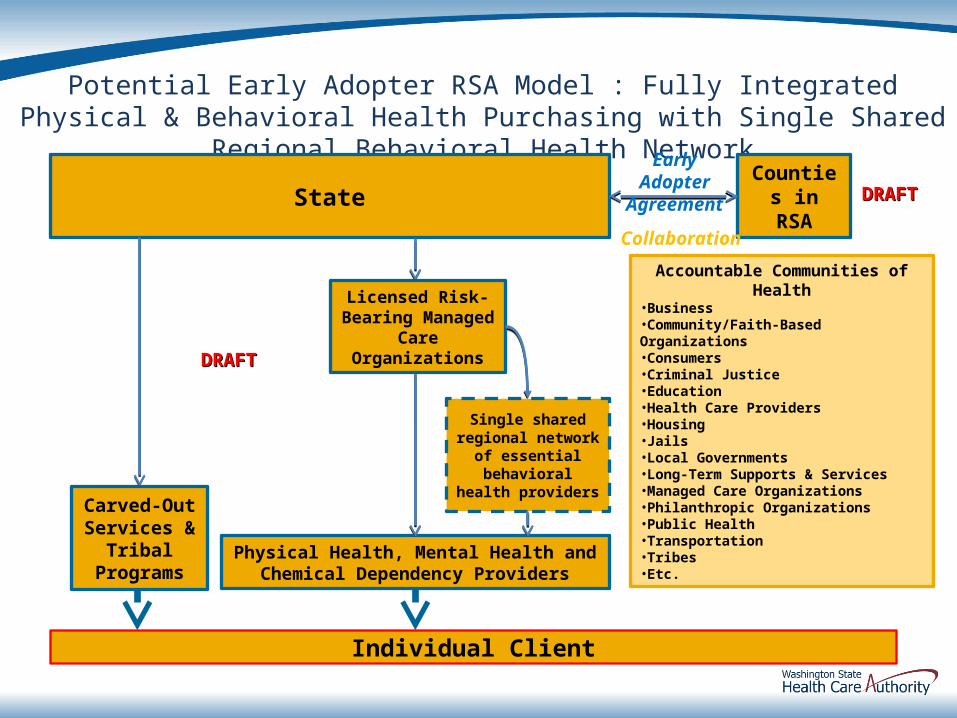
Potential Early Adopter RSA Model : Fully Integrated Physical & Behavioral Health Purchasing with Single Shared Regional Behavioral Health Network
State
Physical Health, Mental Health and Chemical Dependency Providers
Accountable Communities of Health•Business•Community/Faith-Based Organizations•Consumers•Criminal Justice•Education•Health Care Providers•Housing•Jails•Local Governments•Long-Term Supports & Services•Managed Care Organizations•Philanthropic Organizations•Public Health•Transportation•Tribes•Etc.
Individual Client
Licensed Risk-Bearing Managed
Care Organizations
Carved-Out Services &
Tribal Programs
DRAFTDRAFT
DRAFTDRAFTCounties in RSA
Collaboration
Early Adopter Agreement
Single shared regional network
of essential behavioral health
providers

POSSIBLE SERVICE MODELS
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
24
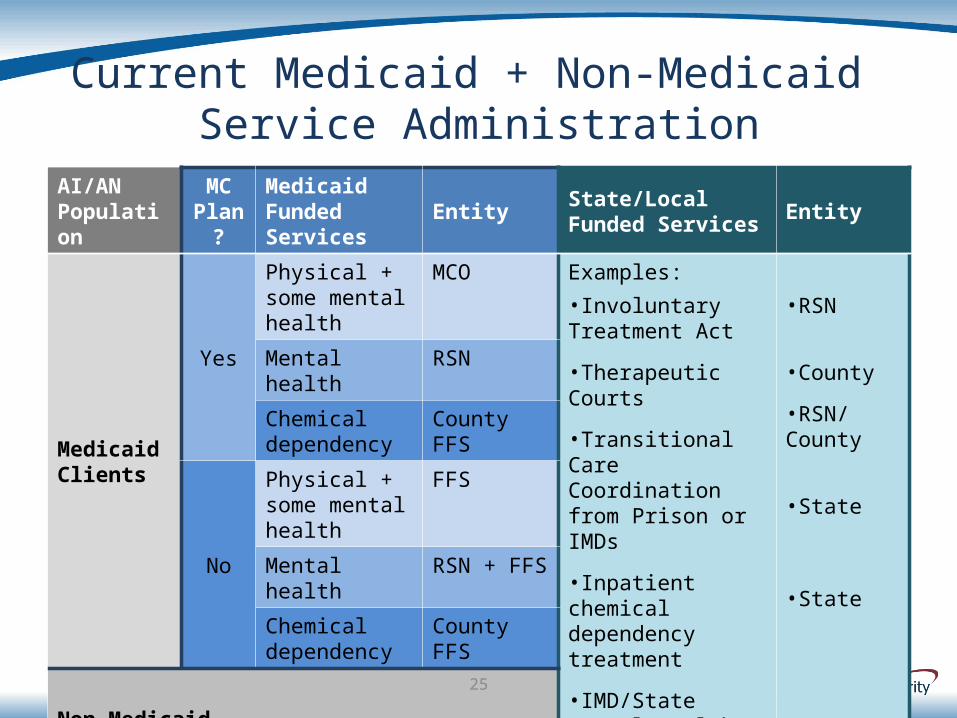
Current Medicaid + Non-Medicaid Service Administration
AI/AN Population
MC Plan?
Medicaid Funded Services Entity State/Local
Funded Services Entity
Medicaid Clients
Yes
Physical + some mental health
MCO Examples:•Involuntary Treatment Act
•Therapeutic Courts
•Transitional Care Coordination from Prison or IMDs
•Inpatient chemical dependency treatment
•IMD/State Mental Health Hospital inpatient care
•RSN
•County
•RSN/County
•State
•State
Mental health RSN
Chemical dependency
County FFS
No
Physical + some mental health
FFS
Mental health RSN + FFS
Chemical dependency
County FFS
Non-Medicaid Clients
25
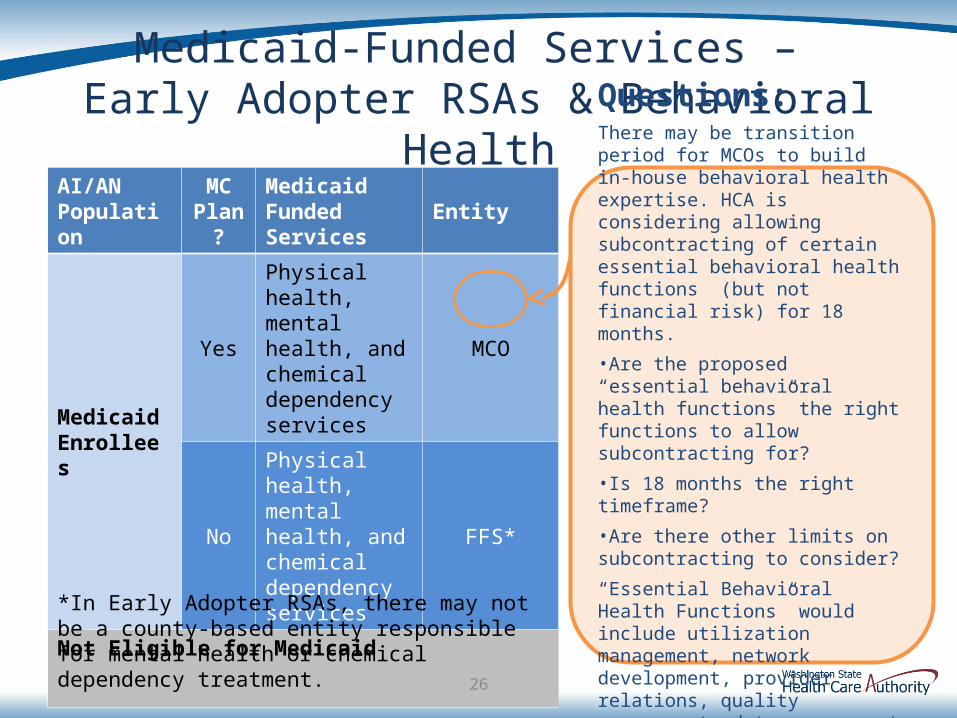
Medicaid-Funded Services – Early Adopter RSAs & Behavioral
HealthAI/AN Population
MC Plan?
Medicaid Funded Services Entity
Medicaid Enrollees
Yes
Physical health, mental health, and chemical dependency services
MCO
No
Physical health, mental health, and chemical dependency services
FFS*
Not Eligible for Medicaid
26
Questions:There may be transition period for MCOs to build in-house behavioral health expertise. HCA is considering allowing subcontracting of certain essential behavioral health functions (but not financial risk) for 18 months.•Are the proposed “essential behavioral health functions” the right functions to allow subcontracting for? •Is 18 months the right timeframe? •Are there other limits on subcontracting to consider?
“Essential Behavioral Health Functions” would include utilization management, network development, provider relations, quality management, data management and reporting.
*In Early Adopter RSAs, there may not be a county-based entity responsible for mental health or chemical dependency treatment.
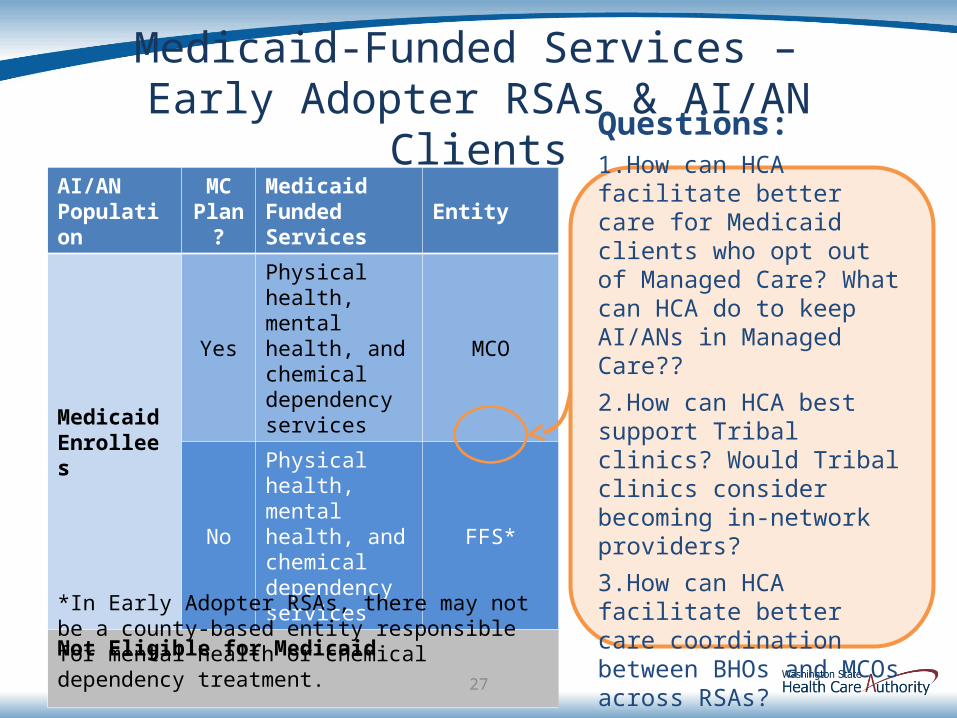
Medicaid-Funded Services – Early Adopter RSAs & AI/AN Clients
AI/AN Population
MC Plan?
Medicaid Funded Services Entity
Medicaid Enrollees
Yes
Physical health, mental health, and chemical dependency services
MCO
No
Physical health, mental health, and chemical dependency services
FFS*
Not Eligible for Medicaid
27
Questions:1.How can HCA facilitate better care for Medicaid clients who opt out of Managed Care? What can HCA do to keep AI/ANs in Managed Care??
2.How can HCA best support Tribal clinics? Would Tribal clinics consider becoming in-network providers?
3.How can HCA facilitate better care coordination between BHOs and MCOs across RSAs?*In Early Adopter RSAs, there may not be a county-
based entity responsible for mental health or chemical dependency treatment.
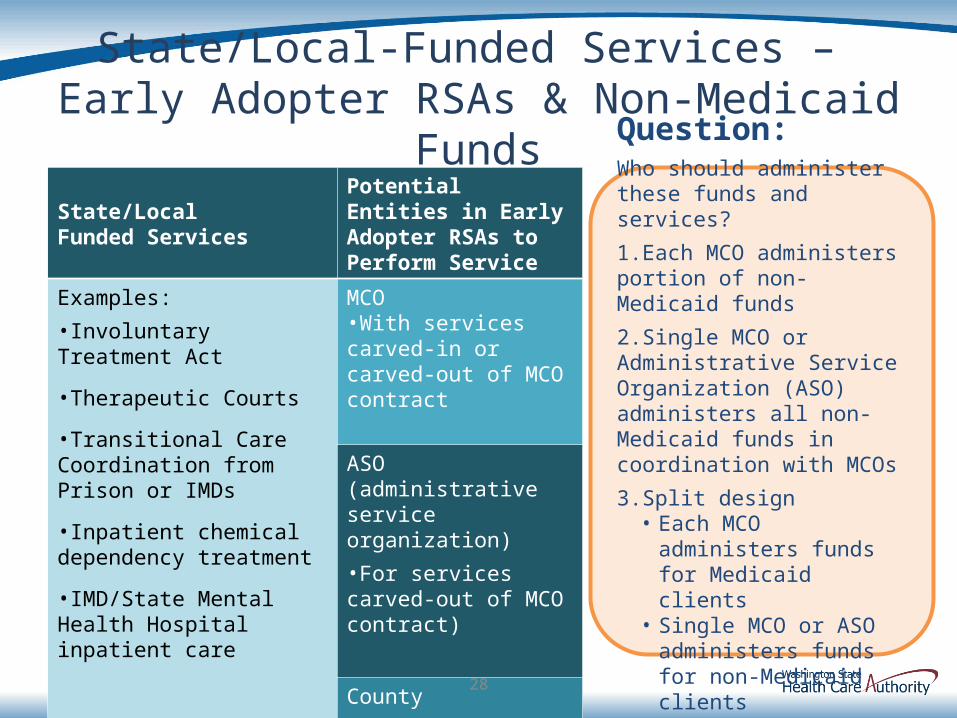
State/Local-Funded Services – Early Adopter RSAs & Non-Medicaid
FundsState/Local Funded Services
Potential Entities in Early Adopter RSAs to Perform Service
Examples:•Involuntary Treatment Act
•Therapeutic Courts
•Transitional Care Coordination from Prison or IMDs
•Inpatient chemical dependency treatment
•IMD/State Mental Health Hospital inpatient care
MCO •With services carved-in or carved-out of MCO contract
ASO (administrative service organization) •For services carved-out of MCO contract)
County•Alternative to ASO
28
Question:Who should administer these funds and services?
1.Each MCO administers portion of non-Medicaid funds
2.Single MCO or Administrative Service Organization (ASO) administers all non-Medicaid funds in coordination with MCOs
3.Split design • Each MCO administers funds
for Medicaid clients• Single MCO or ASO
administers funds for non-Medicaid clients
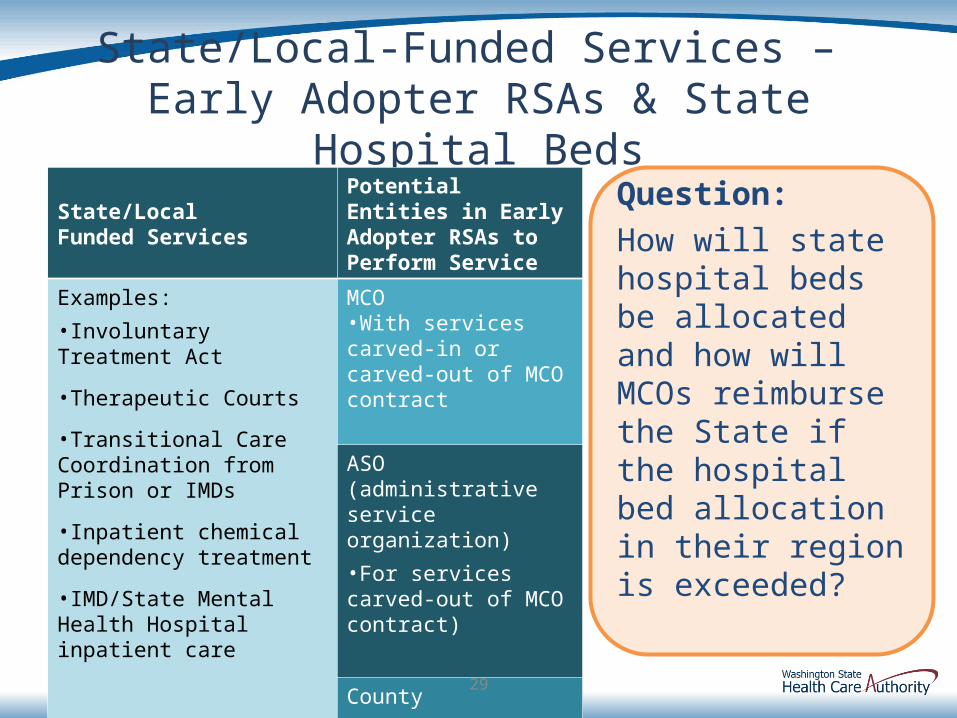
State/Local-Funded Services – Early Adopter RSAs & State Hospital
BedsState/Local Funded Services
Potential Entities in Early Adopter RSAs to Perform Service
Examples:•Involuntary Treatment Act
•Therapeutic Courts
•Transitional Care Coordination from Prison or IMDs
•Inpatient chemical dependency treatment
•IMD/State Mental Health Hospital inpatient care
MCO •With services carved-in or carved-out of MCO contract
ASO (administrative service organization) •For services carved-out of MCO contract)
County•Alternative to ASO
29
Question:How will state hospital beds be allocated and how will MCOs reimburse the State if the hospital bed allocation in their region is exceeded?
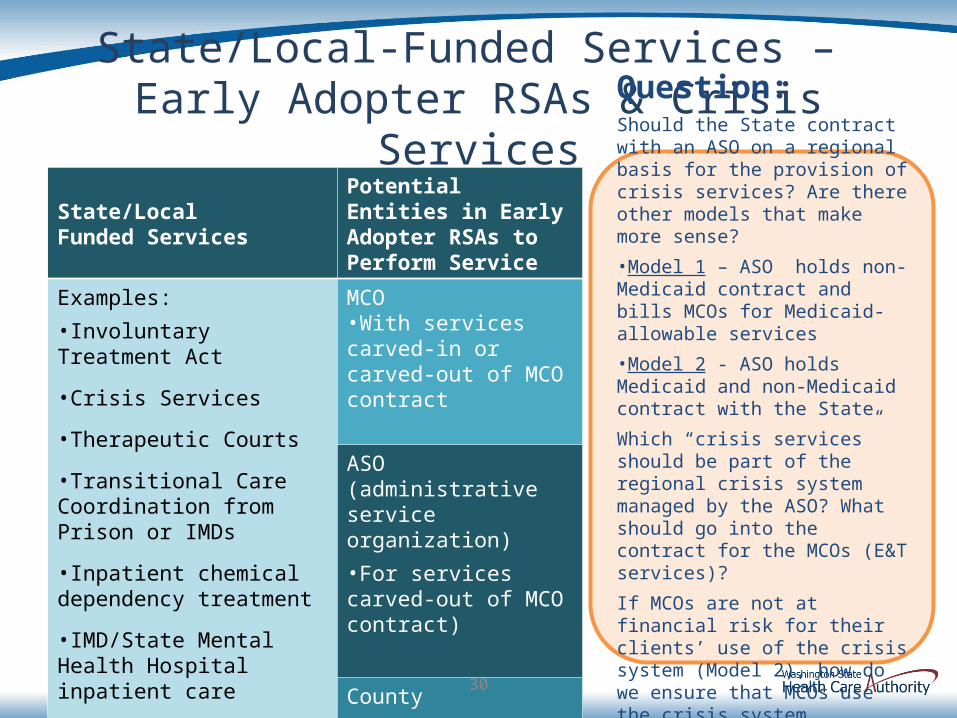
State/Local-Funded Services – Early Adopter RSAs & Crisis Services
State/Local Funded Services
Potential Entities in Early Adopter RSAs to Perform Service
Examples:•Involuntary Treatment Act
•Crisis Services
•Therapeutic Courts
•Transitional Care Coordination from Prison or IMDs
•Inpatient chemical dependency treatment
•IMD/State Mental Health Hospital inpatient care
MCO •With services carved-in or carved-out of MCO contract
ASO (administrative service organization) •For services carved-out of MCO contract)
County•Alternative to ASO
30
Question:Should the State contract with an ASO on a regional basis for the provision of crisis services? Are there other models that make more sense?
•Model 1 – ASO holds non-Medicaid contract and bills MCOs for Medicaid-allowable services
•Model 2 - ASO holds Medicaid and non-Medicaid contract with the State
Which “crisis services” should be part of the regional crisis system managed by the ASO? What should go into the contract for the MCOs (E&T services)?
If MCOs are not at financial risk for their clients’ use of the crisis system (Model 2), how do we ensure that MCOs use the crisis system appropriately?
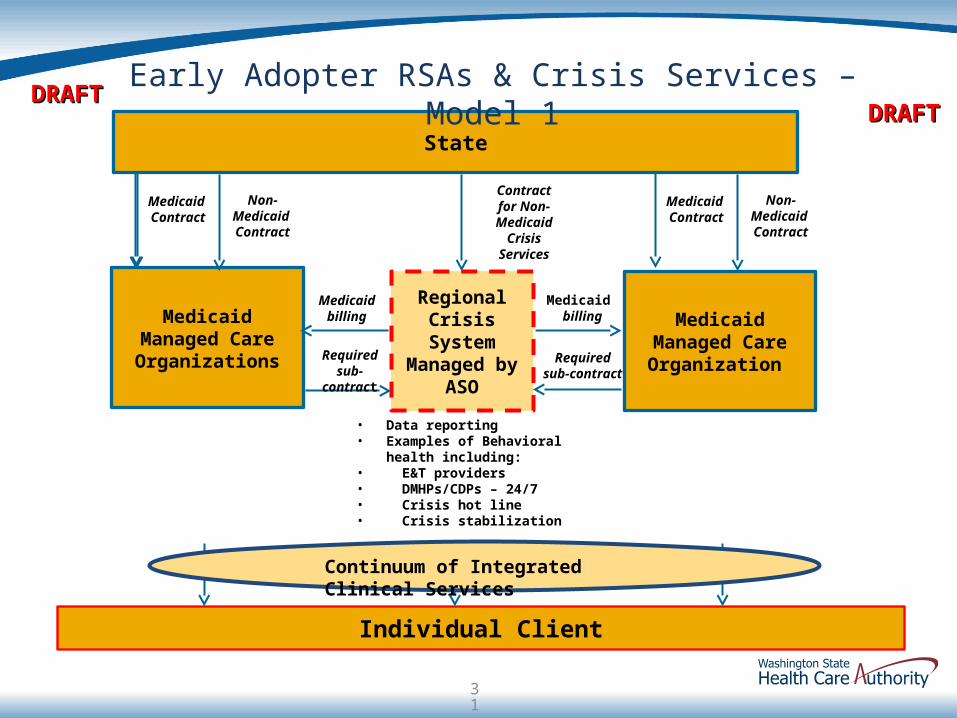
State
Individual Client
Medicaid Managed Care Organizations
Regional Crisis System
Managed by ASO
Early Adopter RSAs & Crisis Services – Model 1DRAFTDRAFT
Medicaid Managed Care Organization Required
sub-contract
Medicaid billing
Requiredsub-contract
Medicaid billing
Continuum of Integrated Clinical Services
DRAFTDRAFT
31
Medicaid Contract
Non-Medicaid Contract
Contract for Non-
Medicaid Crisis
Services
Medicaid Contract
Non-Medicaid Contract
• Data reporting • Examples of Behavioral health
including: • E&T providers• DMHPs/CDPs – 24/7• Crisis hot line• Crisis stabilization
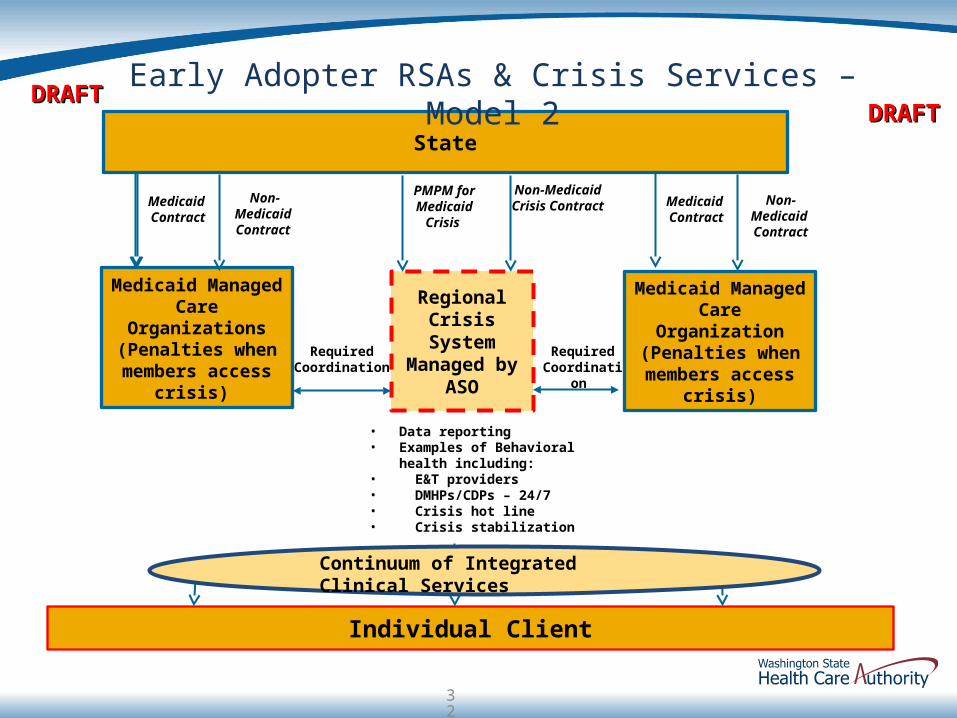
State
Individual Client
Medicaid Managed Care Organizations
(Penalties when members access
crisis)
Regional Crisis System
Managed by ASO
DRAFTDRAFT
Medicaid Managed Care Organization (Penalties when members access
crisis)
• Data reporting • Examples of Behavioral health
including: • E&T providers• DMHPs/CDPs – 24/7• Crisis hot line• Crisis stabilization
Continuum of Integrated Clinical Services
DRAFTDRAFT
32
Medicaid Contract
Non-Medicaid Contract
Medicaid Contract
Non-Medicaid Contract
Required Coordination
Required Coordination
Non-Medicaid Crisis Contract
PMPM for Medicaid
Crisis
Early Adopter RSAs & Crisis Services – Model 2

Potential Crisis System Models: DescriptionsModel 1
• Single regional behavioral health crisis system, managed by an Administrative Service Organization, (ASO) subcontracts with an established regional behavioral health crisis provider system, for the delivery of Medicaid and non-Medicaid crisis services to Medicaid and non-Medicaid individuals on a cost-reimbursement basis.
• The ASO holds a contract with the State for all non-Medicaid services, provided to both Medicaid and non-Medicaid enrollees.
• MCOs in the region are required to subcontract with the ASO for the provision of Medicaid/non-Medicaid crisis services to their enrollees. In this model, the ASO would bill the MCO for Medicaid-allowable services provided to their enrollees, which would be included in the MCO’s Medicaid PMPM.
• The ASO’s contract with the State would fund the non-Medicaid services provided to the Medicaid enrollees and non-Medicaid individuals. The State-ASO contract would also include funding (as in the case of RSNs today) for the ASO to reimburse the county for court costs.
Model 2 • Single regional behavioral health crisis system,
managed by an Administrative Service Organization (ASO), subcontracts with an established regional behavioral health crisis provider system, for the delivery of Medicaid and non-Medicaid crisis services to Medicaid and non-Medicaid individuals on a cost-reimbursement basis.
• ASO holds a contract with the State for all non-Medicaid services, provided to both Medicaid and non-Medicaid enrollees. The ASO also receives a PMPM for all Medicaid crisis services provided to Medicaid enrollees.
• The cost for Medicaid crisis services is not
included in the PMPM for Medicaid managed care organizations (MCOs). MCOs are required, in contract, to coordinate with the crisis system and are penalized when their members access the crisis system or held at performance risk for their members use of crisis services.
33
OTHER QUESTIONS
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
34
Behavioral Health Provider Network
What behavioral health provider types should be included in the Essential Community Provider Network?CMHAs, state-owned and operated hospitals, crisis
providers, inpatient and outpatient SUD providersOpioid treatment programsMobile crisis, crisis residential, respite beds
35
Model of Care
• Draft Model of Care available for review
• Draft Model of Care will be background for procurement
• Questions:• What needs to be strengthened?• Is any section overly prescriptive?• Has anything been left out?• Does the framework (4 quadrant adaptation) help with
understanding of program goals?36
COMMENTS - JANUARY 5
1. Integrated Purchasing of Medicaid Physical and Behavioral Health Care
37
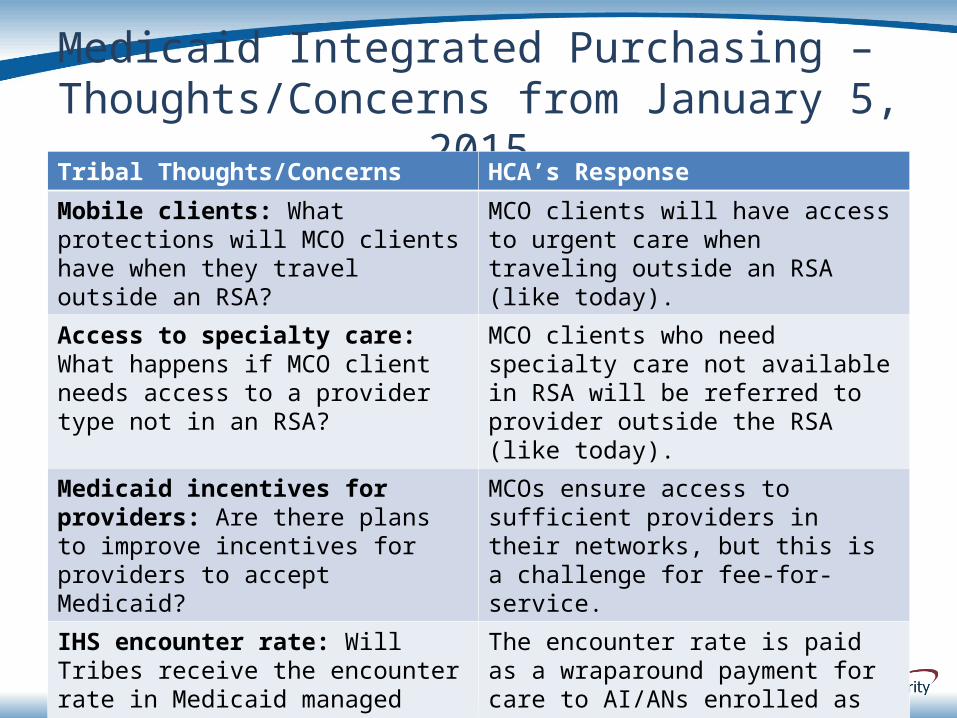
Medicaid Integrated Purchasing – Thoughts/Concerns from January 5,
2015
38
Tribal Thoughts/Concerns HCA’s Response
Mobile clients: What protections will MCO clients have when they travel outside an RSA?
MCO clients will have access to urgent care when traveling outside an RSA (like today).
Access to specialty care: What happens if MCO client needs access to a provider type not in an RSA?
MCO clients who need specialty care not available in RSA will be referred to provider outside the RSA (like today).
Medicaid incentives for providers: Are there plans to improve incentives for providers to accept Medicaid?
MCOs ensure access to sufficient providers in their networks, but this is a challenge for fee-for-service.
IHS encounter rate: Will Tribes receive the encounter rate in Medicaid managed care?
The encounter rate is paid as a wraparound payment for care to AI/ANs enrolled as MCO clients.
Federal grant opportunity: There is currently a federal grant opportunity for tribal care integration.
HCA would be happy to work with Tribes on this. Please share more on this.
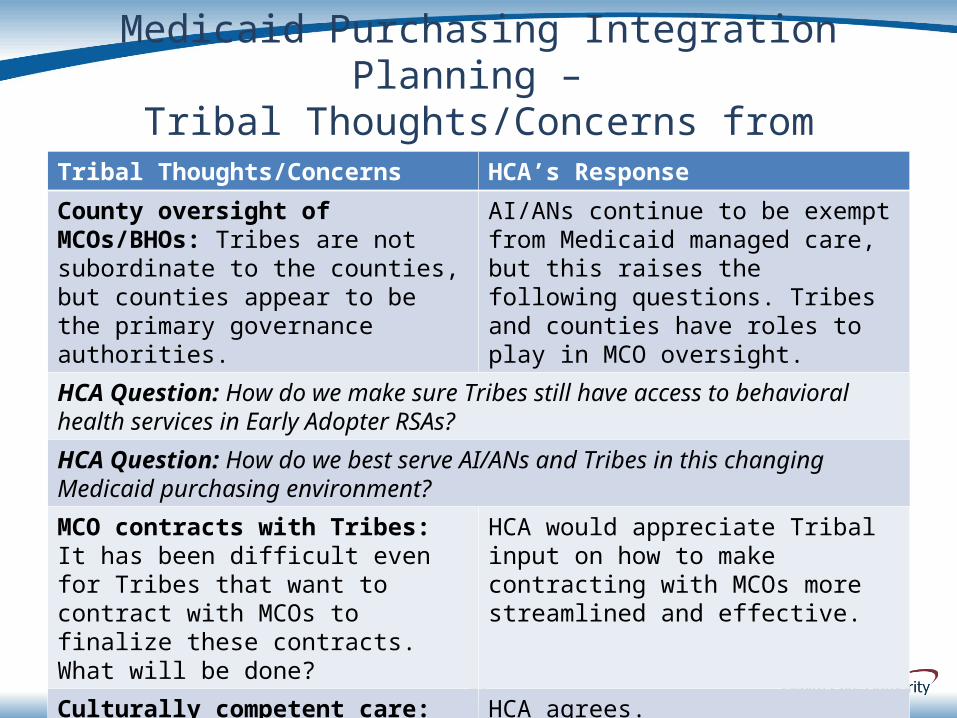
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
39
Tribal Thoughts/Concerns HCA’s Response
County oversight of MCOs/BHOs: Tribes are not subordinate to the counties, but counties appear to be the primary governance authorities.
AI/ANs continue to be exempt from Medicaid managed care, but this raises the following questions. Tribes and counties have roles to play in MCO oversight.
HCA Question: How do we make sure Tribes still have access to behavioral health services in Early Adopter RSAs?
HCA Question: How do we best serve AI/ANs and Tribes in this changing Medicaid purchasing environment?
MCO contracts with Tribes: It has been difficult even for Tribes that want to contract with MCOs to finalize these contracts. What will be done?
HCA would appreciate Tribal input on how to make contracting with MCOs more streamlined and effective.
Culturally competent care: Tribes do not want interference from MCOs.
HCA agrees.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
40
Tribal Thoughts/Concerns HCA’s Response
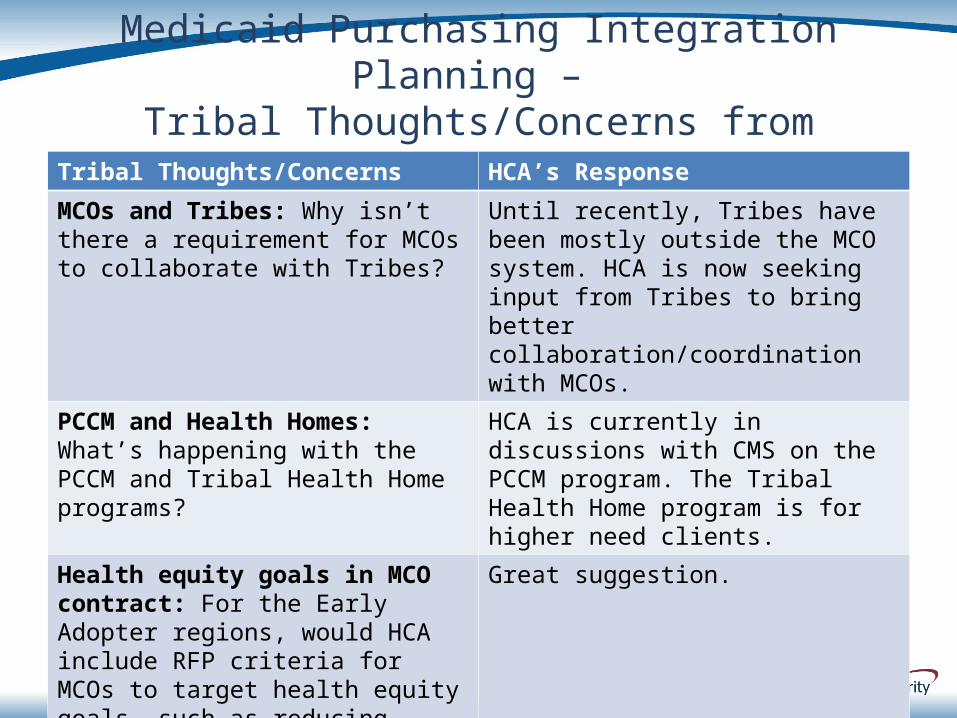
MCOs and Tribes: Why isn’t there a requirement for MCOs to collaborate with Tribes?
Until recently, Tribes have been mostly outside the MCO system. HCA is now seeking input from Tribes to bring better collaboration/coordination with MCOs.
PCCM and Health Homes: What’s happening with the PCCM and Tribal Health Home programs?
HCA is currently in discussions with CMS on the PCCM program. The Tribal Health Home program is for higher need clients.
Health equity goals in MCO contract: For the Early Adopter regions, would HCA include RFP criteria for MCOs to target health equity goals, such as reducing uninsurance among urban AI/ANs? North Sound RSN is working with Tribes on how they will meet AI/AN needs.
Great suggestion.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
41
Tribal Thoughts/Concerns HCA’s Response
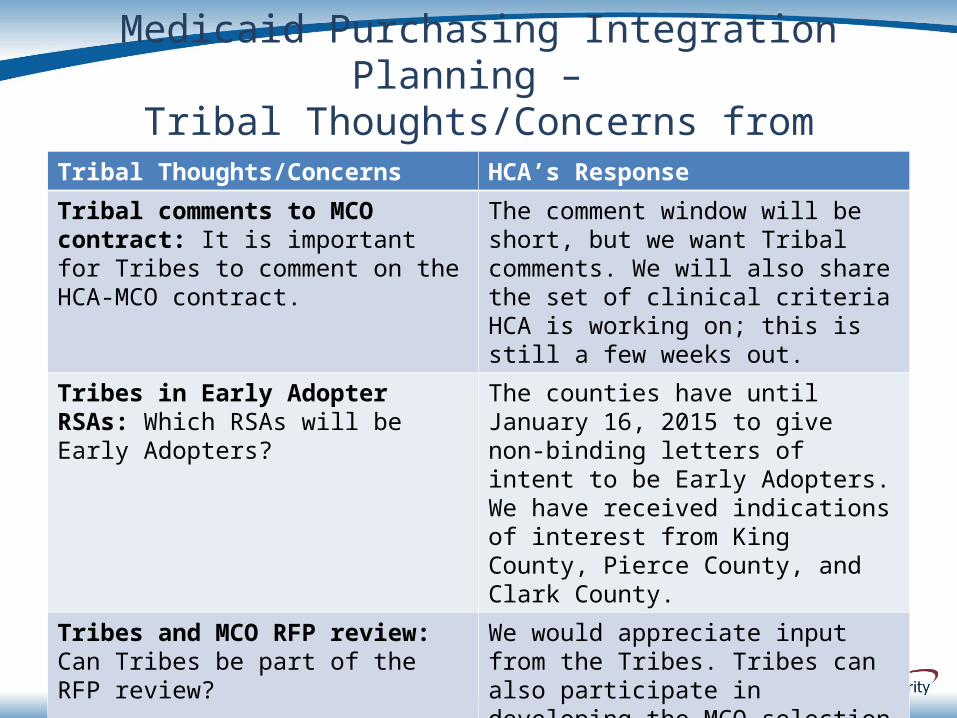
Tribal comments to MCO contract: It is important for Tribes to comment on the HCA-MCO contract.
The comment window will be short, but we want Tribal comments. We will also share the set of clinical criteria HCA is working on; this is still a few weeks out.
Tribes in Early Adopter RSAs: Which RSAs will be Early Adopters?
The counties have until January 16, 2015 to give non-binding letters of intent to be Early Adopters. We have received indications of interest from King County, Pierce County, and Clark County.
Tribes and MCO RFP review: Can Tribes be part of the RFP review?
We would appreciate input from the Tribes. Tribes can also participate in developing the MCO selection criteria that will drive the RFP review.
List of Non-Medicaid Services: Can Tribes get the full list of non-Medicaid services?
HCA will provide the full list when it is completed.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
42
Tribal Thoughts/Concerns HCA’s Response
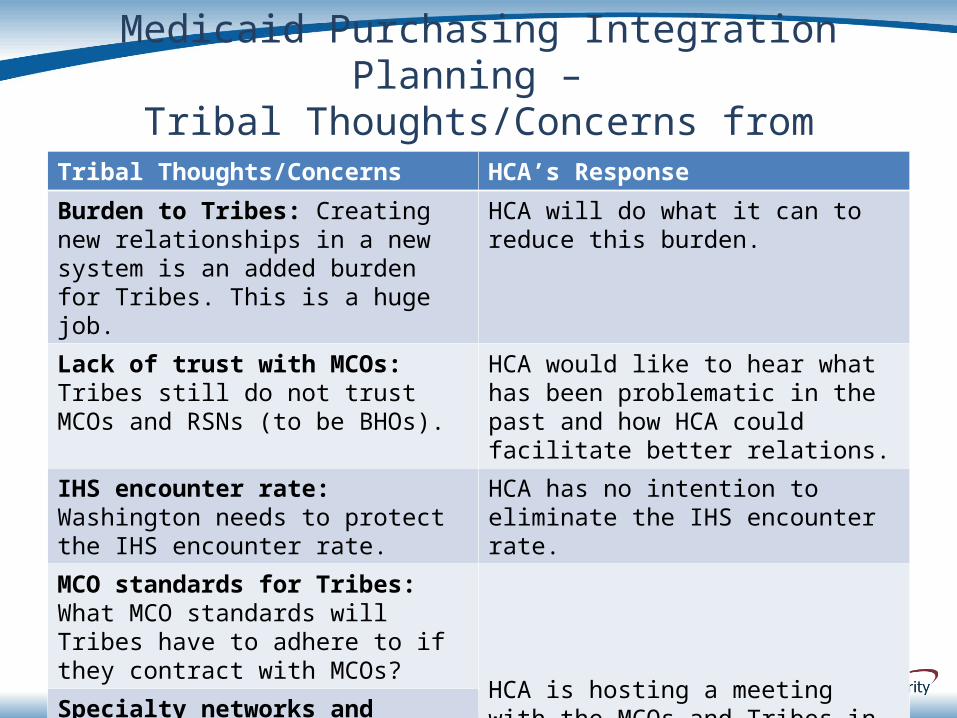
Burden to Tribes: Creating new relationships in a new system is an added burden for Tribes. This is a huge job.
HCA will do what it can to reduce this burden.
Lack of trust with MCOs: Tribes still do not trust MCOs and RSNs (to be BHOs).
HCA would like to hear what has been problematic in the past and how HCA could facilitate better relations.
IHS encounter rate: Washington needs to protect the IHS encounter rate.
HCA has no intention to eliminate the IHS encounter rate.
MCO standards for Tribes: What MCO standards will Tribes have to adhere to if they contract with MCOs? HCA is hosting a meeting with the MCOs
and Tribes in Olympia on February 13, 2015 to discuss these issues.
Specialty networks and Tribes: Tribes need guarantee that MCOs will work with Tribes in effective way for AI/ANs to access MCO specialty networks.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
43
Tribal Thoughts/Concerns HCA’s Response
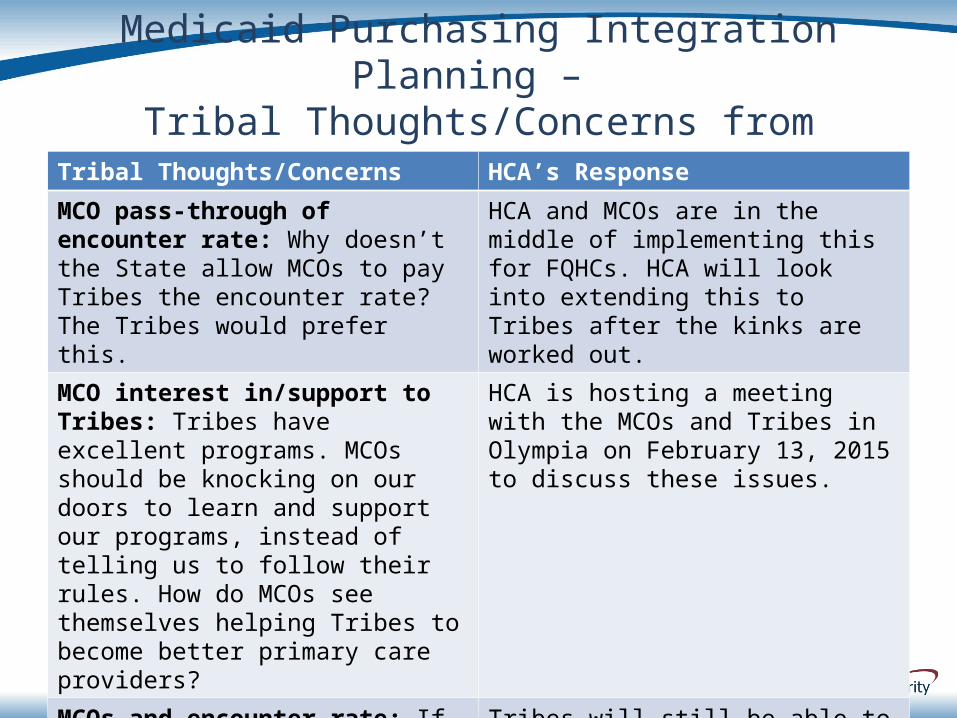
MCO pass-through of encounter rate: Why doesn’t the State allow MCOs to pay Tribes the encounter rate? The Tribes would prefer this.
HCA and MCOs are in the middle of implementing this for FQHCs. HCA will look into extending this to Tribes after the kinks are worked out.
MCO interest in/support to Tribes: Tribes have excellent programs. MCOs should be knocking on our doors to learn and support our programs, instead of telling us to follow their rules. How do MCOs see themselves helping Tribes to become better primary care providers?
HCA is hosting a meeting with the MCOs and Tribes in Olympia on February 13, 2015 to discuss these issues.
MCOs and encounter rate: If Tribes contract with MCOs, how will that affect the encounter rate?
Tribes will still be able to receive the encounter rate for services to MCO-enrolled AI/ANs. MCOs pay providers in many ways, in attempts to reward keeping clients healthy rather than encounters.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
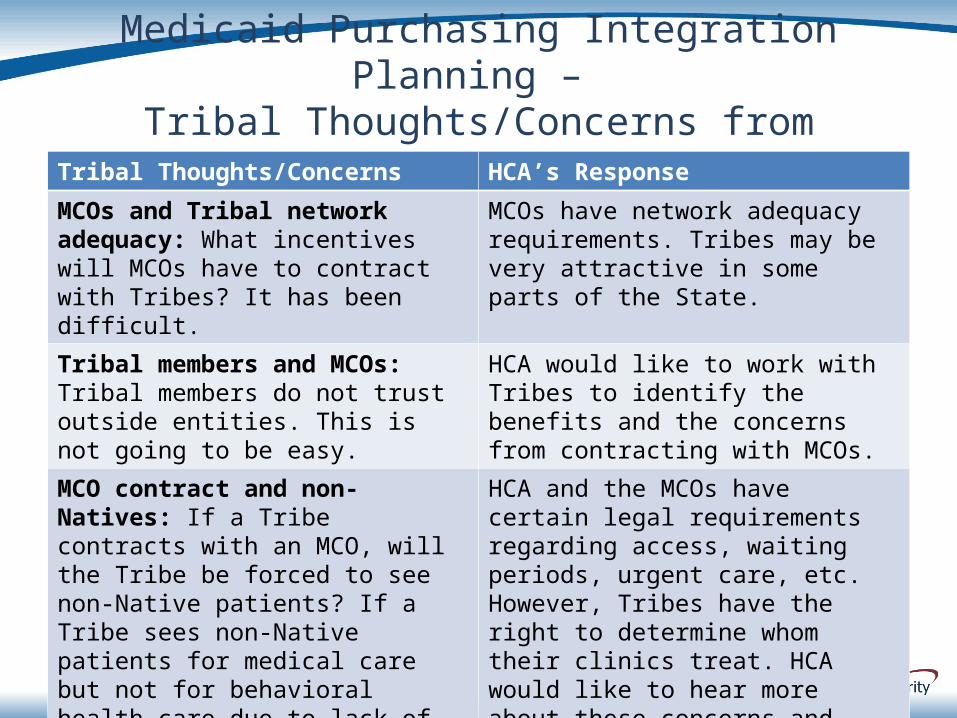
44
Tribal Thoughts/Concerns HCA’s Response
MCOs and Tribal network adequacy: What incentives will MCOs have to contract with Tribes? It has been difficult.
MCOs have network adequacy requirements. Tribes may be very attractive in some parts of the State.
Tribal members and MCOs: Tribal members do not trust outside entities. This is not going to be easy.
HCA would like to work with Tribes to identify the benefits and the concerns from contracting with MCOs.
MCO contract and non-Natives: If a Tribe contracts with an MCO, will the Tribe be forced to see non-Native patients? If a Tribe sees non-Native patients for medical care but not for behavioral health care due to lack of capacity, will contracting with an MCO interfere with the Tribe’s decision on whom to treat?
HCA and the MCOs have certain legal requirements regarding access, waiting periods, urgent care, etc. However, Tribes have the right to determine whom their clinics treat. HCA would like to hear more about these concerns and work through these issues with Tribes.
Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
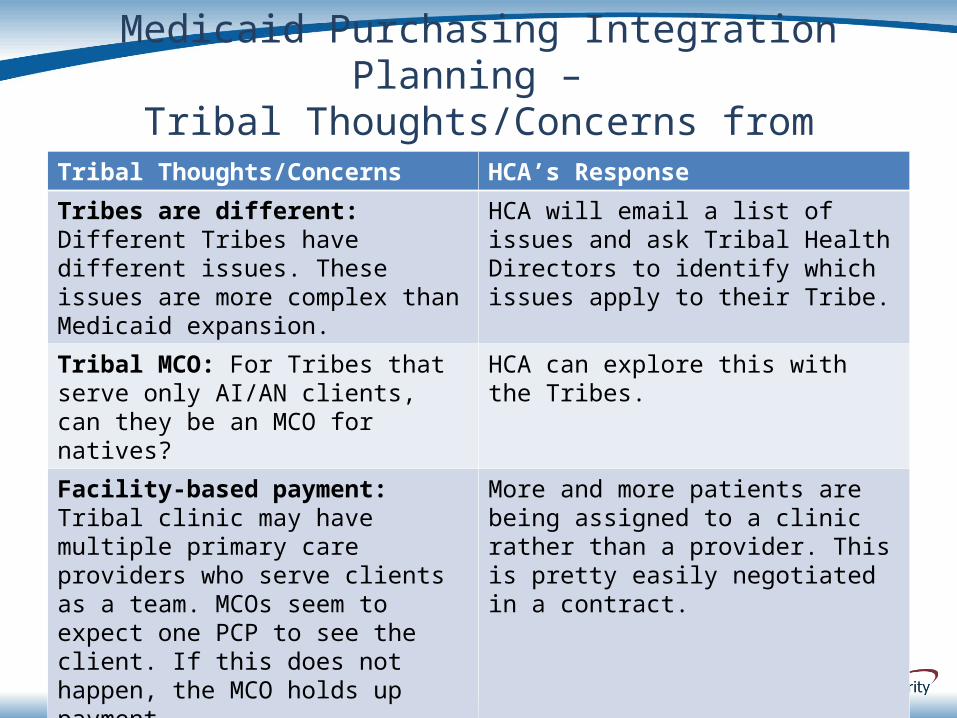
45
Tribal Thoughts/Concerns HCA’s Response
Tribes are different: Different Tribes have different issues. These issues are more complex than Medicaid expansion.
HCA will email a list of issues and ask Tribal Health Directors to identify which issues apply to their Tribe.
Tribal MCO: For Tribes that serve only AI/AN clients, can they be an MCO for natives?
HCA can explore this with the Tribes.
Facility-based payment: Tribal clinic may have multiple primary care providers who serve clients as a team. MCOs seem to expect one PCP to see the client. If this does not happen, the MCO holds up payment.
More and more patients are being assigned to a clinic rather than a provider. This is pretty easily negotiated in a contract.
MCO support for case management: We don’t get paid for case management, but it is very effective so we do it.
More and more MCOs are paying for community health workers, nurses, social workers. Many more options than before.

Medicaid Purchasing Integration Planning –
Tribal Thoughts/Concerns from January 5, 2015
46
Tribal Thoughts/Concerns HCA’s Response
Tribes that opt out: MCOs and Tribes are of two different cultures. MCOs focus on money; Tribes focus on sustainable care. How can Tribes not be pressured to contract with MCOs (opt out of the managed care system)?
AI/ANs will continue to have the federal exemption from managed care, and Tribes will continue to receive the encounter rate for services provided at the Tribal clinic.
BACKGROUND2. Accountable Communities of Health
47
Healthier WashingtonHealthier Washington
• Improving how we pay for services…so people and their providers can choose the best treatment options
• Ensuring health care focuses on the whole person…people’s physical and mental health care are integrated to better meet their needs
• Building healthier communities through a regional approach…local organizations work together to build strategies that work for their community
48
Healthier WashingtonHealthier Washington
Strategies include:
•Accountable Communities of Health to support locally-driven goals, approaches, and processes
•Redesign of provider payments*to improve the quality and value of care
•Creation of a regional extension serviceto share information about best practices
*Tribes are not participating in provider payment redesign effort.
49
Accountable Communities of Accountable Communities of HealthHealth
What is an Accountable Community of Health (ACH)?
•A group of public and private organizations and individuals working together to integrate health care and improve health in their region
•Participants include: public health, housing, and social service providers; MCOs; insurers; county and local government; Tribes; and consumers
50
Clinical CommunityACHs
Accountable Communities of Accountable Communities of HealthHealth
ACHs are intended to regionally align with Regional Service Areas (RSAs) in order to enable ACH input on Medicaid purchasing priorities to ensure they are responsive to regional health needs. ACH input will be informed by data on population health produced by HCA and DSHS and its partners and provided to the ACH for development of a health action plan.
The State proposes phased engagement of ACHs based on the evolution of the ACH Initiative and the maturation of ACHs as follows:•Statewide procurement objectives that address regional needs and perspectives; •Assessment of MCO RFP responses for the ACH’s specific region; •On-going oversight of MCO and BHO effectiveness;•Sharing of public health and managed care data to inform priorities for improving health within the ACH in partnership with public and private entities within the ACH boundary.
51
Accountable Communities of Accountable Communities of HealthHealth
An Accountable Community of Health is not intended to:
• Add approval layers
• Replace government entities
• Divert state funds
• Bear financial risk
52
Accountable Communities of Accountable Communities of HealthHealth
Two ACH Pilot Grants have been awarded to:
• CHOICE Network (Cascade Pacific Action Alliance)Counties: Mason, Thurston, Lewis, Grays
Harbor, Cowlitz, Pacific, Wahkiakum
• North SoundCounties: Snohomish, Skagit, Whatcom, San
Juan, Island
ACH Design Grants to be awarded
53
54
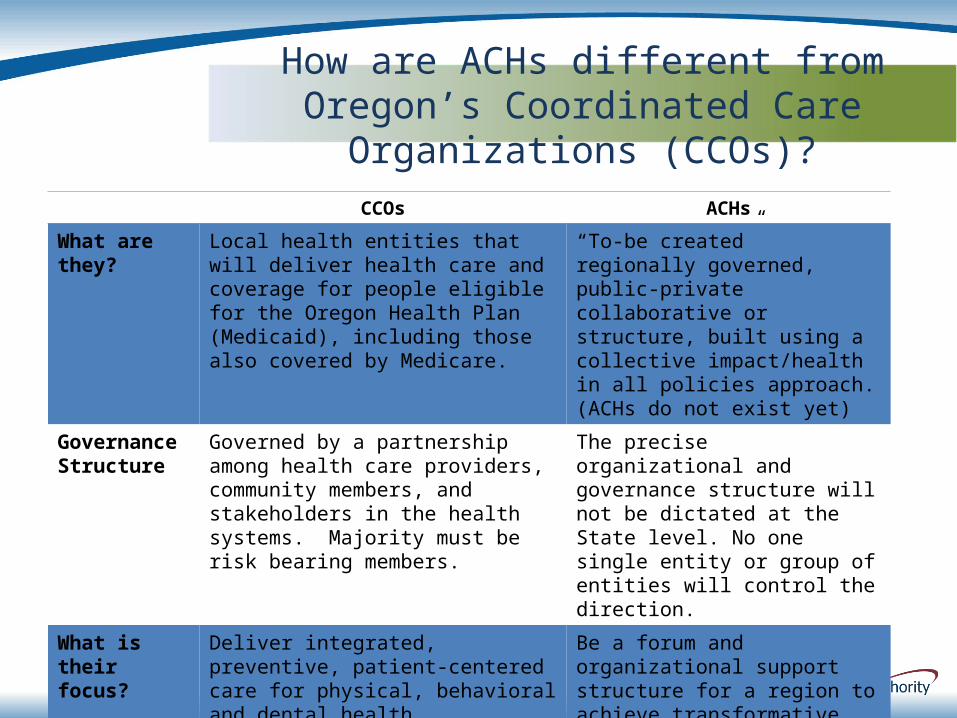
CCOs ACHs
What are they? Local health entities that will deliver health care and coverage for people eligible for the Oregon Health Plan (Medicaid), including those also covered by Medicare.
“To-be created” regionally governed, public-private collaborative or structure, built using a collective impact/health in all policies approach. (ACHs do not exist yet)
Governance Structure
Governed by a partnership among health care providers, community members, and stakeholders in the health systems. Majority must be risk bearing members.
The precise organizational and governance structure will not be dictated at the State level. No one single entity or group of entities will control the direction.
What is their focus?
Deliver integrated, preventive, patient-centered care for physical, behavioral and dental health.
Be a forum and organizational support structure for a region to achieve transformative health results through collaboration across sectors.
Are they risk-bearing? Yes No
How are ACHs different from Oregon’s Coordinated Care Organizations (CCOs)?
55
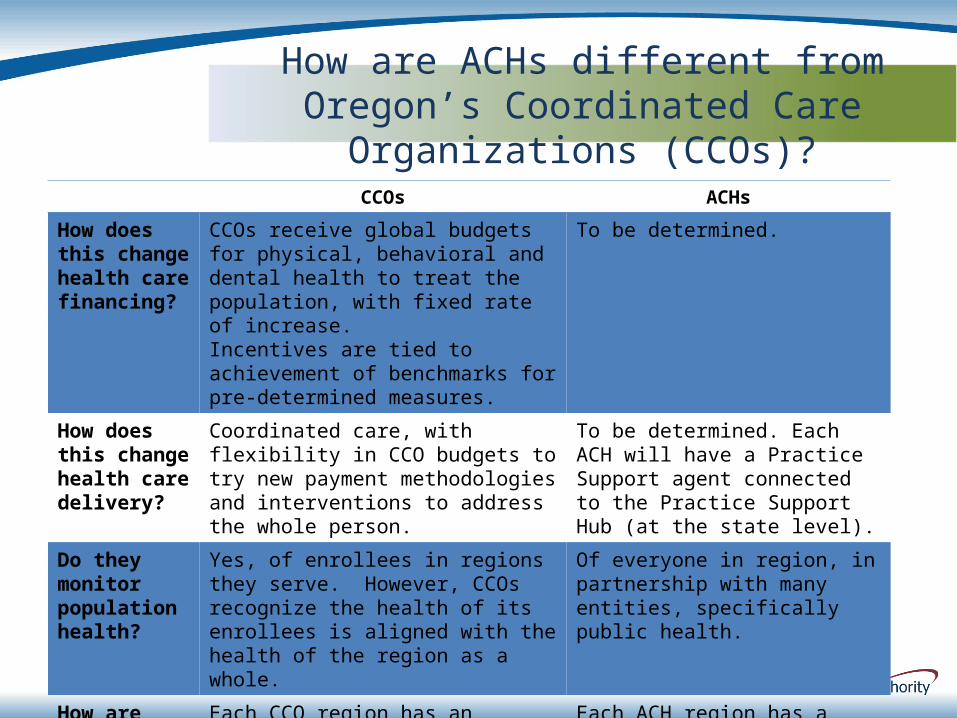
CCOs ACHs
How does this change health care financing?
CCOs receive global budgets for physical, behavioral and dental health to treat the population, with fixed rate of increase.Incentives are tied to achievement of benchmarks for pre-determined measures.
To be determined.
How does this change health care delivery?
Coordinated care, with flexibility in CCO budgets to try new payment methodologies and interventions to address the whole person.
To be determined. Each ACH will have a Practice Support agent connected to the Practice Support Hub (at the state level).
Do they monitor population health?
Yes, of enrollees in regions they serve. However, CCOs recognize the health of its enrollees is aligned with the health of the region as a whole.
Of everyone in region, in partnership with many entities, specifically public health.
How are they held accountable?
Each CCO region has an oversight panel of community members, providers, and stakeholders.
Each ACH region has a governance structure expected to include community members, providers, stakeholders, and Tribal members.
How are ACHs different from Oregon’s Coordinated Care Organizations (CCOs)?
Accountable Communities of Accountable Communities of HealthHealth
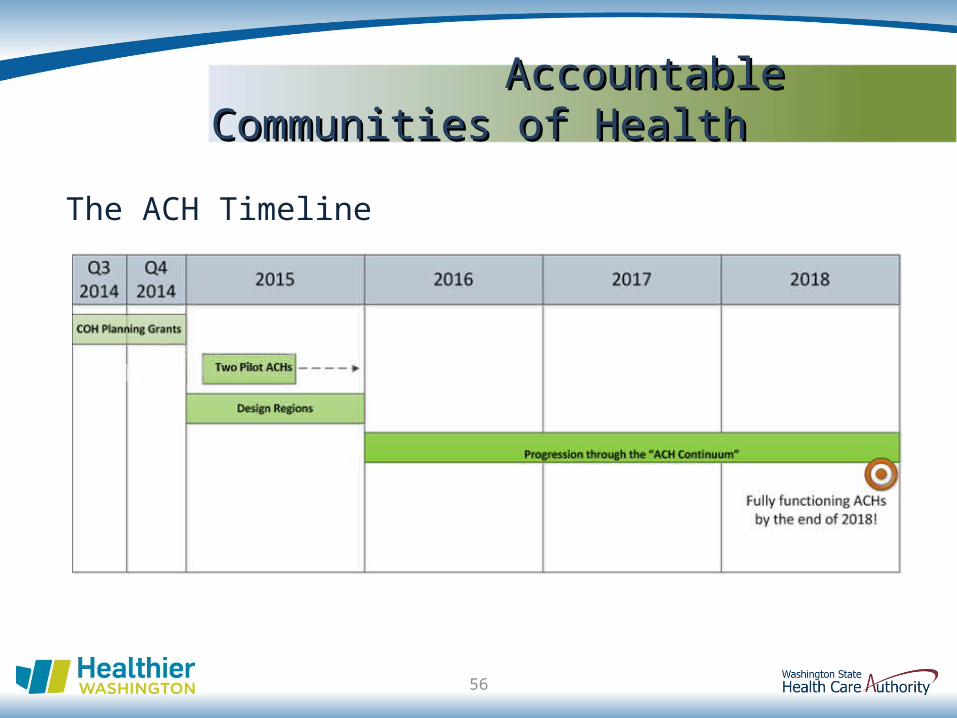
The ACH Timeline
56
Accountable Communities of Accountable Communities of HealthHealth
Total Four-Year ACH Budget: $10.8 million
•ACH Design and Implementation (including personnel, travel, consultants, grants)
Year 1
o ~ 2 Pilot ACHs
o ~ 8 Design Regions
Years 2 – 4
o ~ 10 ACHs
•ACH-Tribal Coordination
57
Accountable Communities of Accountable Communities of HealthHealth
Total Four-Year ACH-Tribal Coordination Budget: $300,000
Proposed Funding Structure for RFP:
• Year 1 (pre-implementation year): $75,000
• Year 2: $150,000
• Year 3: $50,000
• Year 4: $25,000
Proposed Contract Deliverables to HCA:
• Protocols, templates, coordination plans for ACHs to engage with Tribes in their regions
• Data analytic recommendations for ACHs
• Recommendations for maintaining ACH-Tribal coordination process
58
Accountable Communities of Accountable Communities of HealthHealth
ACH-Tribal Coordination•Principles
Health disparity reduction is a key goal of ACHs
ACH participants are expected to understand and respect the Tribal-State government-to-government relationship
•Framework
Tribal representation on local ACH governance/oversight board
Tribe may invoke right to have State participate in any ACH meetings
State must be cc’d on all written communication from ACH to Tribes
59
Accountable Communities of Accountable Communities of HealthHealth
ACH-Tribal Coordination•Financial Support
•Deliverables
•Principles
•Framework
60
How can HCA facilitate productive relationships between ACHs and Tribes/Urban Indian Organizations in order to improve the health of American Indians/Alaska Natives?
COMMENTS – JANUARY 52. Accountable Communities of Health
61

Accountable Communities of Health – Tribal Thoughts/Concerns from January 5,
2015
62
Tribal Thoughts/Concerns HCA’s Response
ACH Accountability: What is the mechanism for holding any of the participants accountable? RSNs have not worked for Tribes at all.
1. ACH is accountable for priorities community has established to its partners/participants, its community, and the State for the pilot funding for the test grant.
2. ACH is accountable through community’s sustainability plan for the ACH.
ACH-Tribal Coordination: How is the ACH meant to interface with the Tribes?
The budget described is intended to support the work needed to answer this question. These funds could enable Tribes to identify data analysis requirements and priorities (or protocols to identify priorities) specific to AI/ANs that all ACHs should use.
Accountable Communities of Health – Tribal Thoughts/Concerns from January 5,
2015
63
Tribal Thoughts/Concerns HCA’s Response
ACH Organization: What is this ACH office going to look like? Is it a board? Is it social workers who come to the Tribes? Is it one office? Multiple offices in a region?
The organization of ACHs will likely vary. HCA envisions boards of directors, including Tribal representation. If the organizational structure does not work, HCA will make adjustments.
ACH Backbone Organizations: Who is HCA looking at to begin this process? Develop these boards?
Each ACH is expected to have a backbone organization, such as non-profit community organizations or local health jurisdictions. HCA will provide link to list of backbone organizations. For example, Kitsap County Public Health will likely be the backbone organization for the ACH in Clallam, Jefferson, and Kitsap Counties.
SPIPA: Please note that SPIPA decided it would not move forward as a backbone organization.
Accountable Communities of Health – Tribal Thoughts/Concerns from January 5,
2015
64
Tribal Thoughts/Concerns HCA’s Response
ACH as Supplemental: Will ACHs compete with Tribes in providing services?
No. ACHs will supplement Tribal services.
Tribal Participation: So, a “to do” each Tribe could take care of is designating someone to link into these ACH efforts?
Yes. HCA will be available to assist Tribal designees in linking with the ACH planning efforts.
Government-to-Government Relations: RSNs have not always recognized the government-to-government relationships between the State and the Tribes. If these ACHs are non-profits, what is the take on the government-to-government relationship with the ACHs.
This is why HCA is seeking Tribal input into how to facilitate Tribal participation in ACHs that will respect Tribal sovereignty while facilitating effective regional coordination of health care and support services. While the ACHs are contemplated to be non-governmental partnerships, HCA will be responsible for ensuring that the government-to-government relationship is respected.
Accountable Communities of Health – Tribal Thoughts/Concerns from January 5,
2015
65
Tribal Thoughts/Concerns HCA’s Response
State Commitment: Are there state dollars to fund this?
The CMMI grant is supporting this effort. The legislature put up $1 million last year. State agencies are contributing in-kind support.
HCA: ACHs have more to learn from Tribes than from almost any other sector. How can we learn from Tribes about serving communities and addressing health disparities? How can ACHs bring resources to help address Tribal concerns?
ACH Sustainability: What is the plan for ACH sustainability?
The ACH initiative is a demonstration, to enable ACHs to show their value. As the ACHs show their value, various funding sources would likely become possible.
ACH Cultural Competency: Having non-Natives raise cultural competency questions would be helpful.
HCA could include requirements for ACH participants to receive cultural competency training.
GOVERNOR’S HEALTH INNOVATION LEADERSHIP NETWORK
3. Healthier Washington
66
Health Innovation Leadership Network
The Governor’s Office seeks recommendations for two people to serve 1-year terms on HILN:
•A Tribal representative, and•An Urban Indian Organization representative.
67
What is HILN?
•HILN is a public-private network to accelerate Healthier Washington efforts.
•With the award of the CMMI grant, the Governor is creating HILN from the members of the Executive Management Advisory Council (which informed the State Health Care Innovation Plan).
68
Health Innovation Leadership Network

Health Innovation Leadership Network
What is HILN intended to do?
•Monitor, inform and accelerate Healthier Washington progress
•Identify barriers and opportunities for alignment, scale and spread
69
Health Innovation Leadership Network
Please let me know if:
•You have any recommendations
•You have any questions about HILN
70

RESOURCES
71
HCA Healthier Washington:http://www.hca.wa.gov/hw/Pages/default.aspx
DSHS Developing Behavioral Health Organizations:http://www.dshs.wa.gov/bhsia/division-behavioral-heath-and-recovery/developing-behavioral-health-organizations
Washington Adult Behavioral Health System Task Force:http://leg.wa.gov/JOINTCOMMITTEES/ABHS/Pages/default.aspx