Embed Size (px)
Citation preview

CASE REPORT
‘Watered down’ renal colic: Using tapwater mixed with blood to simulatemacroscopic haematuriaJoseph TingDepartment of Emergency Medicine, Mater Public Hospitals, South Brisbane, Queensland, Australia
Abstract
Renal colic is a frequent presentation to the emergency department. Although most casesare genuine, up to 0.6% of cases are factitious, representing attempts to procure parenteralnarcotic medication or rarely, to attain unnecessary investigation or invasive treatment.Urethral catherization has been recommended to procure an untampered urine sample, butis viewed as invasive. Calculi analysis has no relevance to acute management. We report acase of factitious renal colic which was definitively proven to be so using sample biochem-istry to confirm a tap water sample contaminated with blood. This is diagnostically usefulif tap water or normal saline is used to produce an alleged urine sample.
Key words: drug seeking, factitious, renal colic.
Case report
A 38-year-old man presented with sudden severe rightflank pain radiating to the groin of 3 h duration. Para-medics had administered a total of 10 mg of IV mor-phine through a left hand IV cannula en route to the ED.
The patient was apparently distressed with severepain. He has had similar previous episodes of renal colic,a congenital solitary right kidney and an appendecec-tomy. Medications include sodium citotartrate sachetsand he is allergic to buscopan.
He is seen by an ED Junior House Officer, who ordersthe administration of a further 12.5 mg of IV morphine,100 mg of IV tramadol and 10 mg of IV ketorolac. Thepatient was afebrile with blood pressure 121/70 mmHg,pulse 70/min and respiratory rate 18/min. Pain intensitywas still rated at 10/10. Clinical examination revealed
subjective deep tenderness without guarding in theright lower quadrant, and the patient described ongoingsevere right flank pain.
At different times, two uniformly blood-stained urinesamples were volunteered by the patient on his returnfrom the toilet. Urinalysis showed 3+ blood on eachoccasion. His left hand drip site has been tampered withand the IV cannula is now dislodged on his first returnfrom the toilet.
A second IV cannula was placed in his right hand andconnected to a bag of normal saline. A second urinesample was requested as there is uncertainty regardingthe veracity of the patient’s claims of ongoing severepain. Another blood-stained sample was volunteered tonursing staff on his return. Blood was noted to bepresent on the patient’s shirt and the IV giving setconnection has been loosened.
Correspondence: Dr Joseph Ting, Department of Emergency Medicine, Mater Public Hospitals, Raymond Terrace, South Brisbane, Old4101, Australia. Email: [email protected]
Joseph Ting, MB BS, B Med Sci, Postgrad Dip Epidemiology (LSHTM).
doi: 10.1111/j.1742-6723.2007.01050.x Emergency Medicine Australasia (2008) 20, 85–86
© 2008 The AuthorJournal compilation © 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine

In order to confirm factitious renal colic, sample bio-chemistry was ordered to assess whether electrolytesare consistent with urine. With sodium <6 mmol/L andpotassium <1 mmol/L, the sample is probably consis-tent with tap water that has been mixed with thepatient’s blood. This was confirmed by analysing asample of water from the same toilet tap, which yieldedan identical electrolyte profile. Urine microscopyshowed >2000 ¥ 106 erythrocytes (reference range,RR < 10 ¥ 106), 15 ¥ 106 leucocytes (RR < 10 ¥ 106),occasional epithelial cells and no crystals.
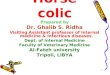
In view of the patient’s claim of having a solitaryfunctioning kidney, an urgent non-contrast CT-KUBwas performed. This showed a solitary right kidneywith no hydronephrosis, focal mass or perinephricstranding (Fig. 1). There was no ureteric calculus visibledown to the pelvic brim and no other intra-abdominalpathology was demonstrated. The patient’s white cellcount was 6.2 (RR 4.5–11.0 ¥ 109/L) and serum creati-nine 108 (RR 70–120 mmol/L).
The diagnosis of a factitious disorder and drug-seeking behaviour was discussed with the patient, whothen elected to leave the ED.
Discussion
Factitious renal colic in an attempt to procure parenteralnarcotic medication1,2 and attain unnecessary investiga-tions or invasive treatment3,4 is well-known, with anincidence of up to 0.6% of cases of acute renal colic.1
Patients have been reported to mix their own blood witha urine sample to produce factitious haematuria,1,3
although these cases were not conclusively proven. Onepatient seeking parenteral narcotics implanted metalinto the anterior abdominal wall to simulate a calculuson abdominal X-ray2 whereas another patient misrepre-sented gravel as calculi.5
Several ways have been suggested to prove a case ofrenal colic factitious. A non-haematuric bladder urinespecimen obtained by insertion of a urinary cathetermakes renal colic unlikely.1,4 Aside from patient discom-fort, urethral catherization that is traumatic produces ahaematuric specimen in the absence of calculi, and ure-thral calculi may not give rise to haematuria in bladderurine. Supervised witnessed urine collection1 is not idealfor patient modesty or privacy. Alleged calculi havebeen analysed and proven to be of non-human origin.5
Our patient’s proven attempt to produce a haematuricurine sample using tap water and his own blood repre-sents a novel method to deceive the treating doctor. Thishas not been previously reported. A sample electrolyteprofile consistent with tap water (or saline solution)definitively proves that the sample is not human urine.However, this strategy will not work if the patientmanipulates a true urine sample.
Accepted 10 July 2007
References
1. Reich JD, Hanno PM. Factitious renal colic. Urology 1997; 50:858–62.
2. Attar K, Lee G, Rowe E, Hudd C. The secret of the phantom stone:a case report. Int. Urol. Nephrol. 2004; 36: 27–8.
3. Gluckman GR, Stoller M. Munchausen’s syndrome: manifesta-tion as renal colic. Urology 1993; 42: 347–50.
4. Mydlo JH, Macchia RJ. Munchausen’s syndrome: a medico-legaldilemma. Med. Sci. Law 1997; 37: 198–201.
5. Chettouh-Harrache D, Amar A, Taleb S, Bouhacina N, AuberthieR. Factitious lithiasis: case report from Western Algeria. Sante2004; 14: 257–60.
Figure 1. Right congenital solitary kidney with no evidence ofnephrolithiasis.
J Ting
86 © 2008 The AuthorJournal compilation © 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine