Embed Size (px)
Citation preview

Schuette
Clinical Case StudyPsychiatric And Cognitive Disorders
Sarah Schuette | LIU Post Dietetic Internship | March 11, 2019Clinical Site: Northwell Syosset Hospital
Preceptor: Colleen Chiariello
1

Schuette
KG is a 36-year-old single Caucasian female admitted to Northwell Syosset
Hospital on February 12, 2019 for a possible suicide attempt by drug overdose. She was
transferred from the Special Care Unit to the Inpatient Psychiatry Unit on February 12th,
and discharged February 25, 2019. KG is Roman Catholic and lives at home with her
mother and father. She was a graphic design teacher for high school students until
quitting three years ago, and is currently unemployed. She has never smoked tobacco or
used illicit drugs, but has a history of alcohol abuse.
Patient’s History
KG was diagnosed with major depression disorder and generalized anxiety
disorder in May of 2015. She stated she experienced major losses that year, but did not
elaborate. The following Fall, she quit her job as a graphic design teacher for high school
students to attend a partial program at South Nassau County after attempting suicide by
Tylenol overdose in August 2015. KG’s social history includes prior alcohol abuse from
2000-2010. She quit drinking on her own in 2010, but relapsed in 2015 and in 2018. She
states she has been sober for one year and 5 days. She reports she never smoked tobacco
or engaged in recreational drug use.
On February 12th, 2019, KG was found at home with altered mental status by her
parents. They stated she was last seen “normal” the night before and when the parents
came to see her today around 9:30am, she was found altered. They called for an
ambulance, which brought her to Syosset Hospital, where she was obtunded and not
responsive. In the ED, her labs showed positive for benzodiazepines and an elevated
salicylate level of 29.5. KG was diagnosed with an intentional drug overdose and
2

Schuette
admitted to the Special Care Unit for 1:1 monitoring after the effects of the drugs had
been reversed and her electrolytes were replenished. Once she was medically cleared, KG
was moved to the hospitals’ inpatient psychiatry unit for stabilization. She stated that she
was frustrated with her life, and was “done with life and just [wanted] to end it all.” She
stated she regretted her decision to overdose on pills, of which she swallowed an
unknown number. Originally noted as being guarded, isolative, anxious, nervous,
depressed and somewhat uncooperative, KG eventually became more social during her
time in the inpatient psychiatry unit. She participated in daily group activities, cooperated
with taking medications, and her symptoms of depression and anxiety improved. Once
evaluation showed she was at low risk for suicide (no suicidal ideations) and had more
stable mood with improved anxiety management, KG was discharged with the plan to
return to South Nassau to complete their partial program, which was discussed with her
parents and outpatient prescriber at South Nassau.
Discussion of Psychiatric and Cognitive Disorders
AnxietyBackground
According to the CDC, the prevalence rates for anxiety disorder in developed
countries range from 13.6% to 28.8% of the population. Different forms include
generalized anxiety disorder (GAD), panic disorder, obsessive-compulsive disorder
(OCD), posttraumatic stress disorder (PTSD), and social anxiety disorder. Common to all
of these are heightened and poorly controlled emotional, somatic, and neurologic
symptoms triggered by a specific type of circumstance or situation (Mahan and
Raymond, 2017, p.856).
3

Schuette
Anxiety can function as an evolutionary advantage because it is a heightened
awareness of one’s surroundings and thus can be useful in staying alert to potential
dangers. However, this quickly moves into the realm of pathology when it becomes
pervasive and difficult to control. There is a clear genetic component to anxiety, and early
life stress may constitute a significant etiologic factor for anxiety, but the overall etiology
for anxiety is not well understood.
The structure in the brain thought to generate anxiety is the amygdala, which
processes fear-related stimuli and then signals other parts of the brain to fire and release
norepinephrine corticotropin-releasing factor, which ultimately stimulates elevated
cortisol levels and other excitatory components of the sympathetic nervous system.
(Baldwin, et. al., 2012).
Difficult life circumstances that provoke stress can exacerbate underlying
anxiety disorders and may be helpful to address with counseling. Anxiety provokes
physical and emotional symptoms, including rapid heart rate, shallow breathing,
diaphoresis, hypervigilance, and sleep disorders. It also provokes physical and emotional
symptoms including increased fear and worry (Albert et. al., 2011, p.1494). KG was
diagnosed with generalized anxiety disorder in 2015 following what she described as
“significant losses in her life.” When she first arrived to Syosset, she was experiencing
poor sleep quality and increased fear and worry. These feelings were present in varying
degrees throughout her stay, and revolved around fears that she was a burden to her
parents, fear of resentment from her parents, fear that she would “always be a failure,”
worry that she would never get her thoughts or health under control, and worry she would
never healthy enough to work again.
4

Schuette
Diagnostic Criteria
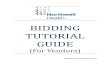
Diagnostic criteria for Generalized Anxiety Disorder include meeting all of the
following criteria outlined by the Diagnostic and Statistical Manual of Mental Disorders,
or DSM-5, pictured below:
(Image via American Psychiatric Association, 2013)
KG met the all of the criteria, including items 2, 3, and 4 under Diagnostic
Criteria item C. Unlike other mental disorders, the focus of worry in those with GAD
5

Schuette
shifts over time. Common worries include work or family responsibilities, money, health,
or safety. As mentioned above, KG experienced a number of these common worries.
Labs that should be assessed in those with anxiety include vitamin D,
Magnesium and B vitamin status (Mahan and Raymond, 2017, p.852). KG’s magnesium
was found to be within normal range at 1.8, and her vitamin D status and B vitamin status
were not assessed during her admission.
Medical Interventions
Medical interventions include using drugs (antidepressants, benzodiazepines),
psychotherapy (cognitive behavioral therapy) and providing the patient with support
(provide reassurance and verbal rewards for successes, promote gradual changes,
support blood sugar stability) (Mahan and Raymond, 2017, p.848). KG received all of
these treatments during her admission.
Nutritional Implications
Nutrition related interventions include reducing caffeine intake, reducing intake
of sucrose and other forms of sugar, adding a multivitamin containing high doses of B
vitamin and minerals plus 200mg per day of magnesium, and increasing high-quality
protein intake throughout the day (Mahan and Raymond, 2017, p.852). KG was
consuming about 70g of added sugar from the Ensure Enlive cans she was consuming
daily, so finding ways for her to reduce her added sugar intake, such as consuming more
fiber-rich whole foods sources to obtain nutrients, might prove beneficial.
6

Schuette
DepressionBackground
Depression is a mood disorder that causes persistent feelings of sadness and loss
of interest or pleasure in activities (Albert, et. al., 2011, p. 1538). According to the World
Health Organization, Major Depressive Disorder is one of the most common causes of
disability worldwide. Persons with Major Depressive Disorder have had at least one
major depressive episode for 14 days or longer, and it may be recurrent throughout their
lives. About 40% of risk for major depression is inherited, and 60% is from
environmental factors. Multiple genes are recognized as playing a role in depression,
most notably the C>T type of the MTHFR allele is said to indicate a higher risk for
developing depression. Other theories on what may cause depression include a chronic
deficiency of omega-3 fatty acids, and the monoamine deficiency theory, which suggests
that a deficiency of serotonin, dopamine, and norepinephrine is the main
pathophysiologic factor in depression (Mahan and Raymond, 2017, p. 856).
Diagnostic Criteria
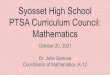
Diagnostic criteria for Major Depressive Disorder (also called Persistent
Depressive Disorder, or Dysthymia) include meeting five of the following criteria
outlined by the Diagnostic and Statistical Manual of Mental Disorders, or DSM-5,
pictured below:
7

Schuette
(Image via American Psychiatric Association, 2013)
Patient history that should be assessed includes height, weight, BMI, weight
changes, dietary/intake history, blood pressure, food pica, I&O, and constipation.
While there are no lab findings that are specifically indicative for major depressive
disorder, lab work is needed to exclude physical conditions that may cause depression,
such as pernicious anemia. Labs that should be assessed include H&H, serum Fe, Alb,
8

Schuette
Ca++, serum Mg++, serum zinc and copper, glucose, serotonin, thyroid tests, Na+, and
K+, N balance, serum folate and B12, serum vitamin D.
(Escott-Stump, 2015, p.289).
Medical Interventions
Provide adequate nutritional intake.
Monitor weight at least twice monthly to evaluate status and changes.
(Consequences from antidepressants may cause weight gain)
Assess usual eating habits and related problems, which may include poor sleep
habits. Adequate drug therapy usually helps appetite improve.
Assure adequate intake of key nutrients, including amino acids, omega-3 fatty
acids, and vitamins D and B12.
Reduce stress, which elevates protein kinase C levels in the brain
Promote physical activity and exposure to sunshine
(Escott-Stump, 2015, p.289).
KG was meeting her estimated calorie needs and the majority of her micronutrient
needs, but was not consuming enough omega-3’s. In the past, she had experienced weight
gain related to her medications, but after switching to another medication and reducing
her PO intake, she was able to bring her weight back down to close to her IBW/UBW of
120lb. Her usual eating habits were assessed and became the main focus of our sessions,
as she was an extremely picky eater at baseline.
Nutritional Implications, Counseling/Education, & Care Management
Use a diet providing high quality protein. Inadequate protein intake may reflect
decreased intake of iron, thiamine, riboflavin, niacin and B6 and B12.
9

Schuette
Encourage an anti-inflammatory diet, such as the Mediterranean diet.
Increase omega-3 fatty acids
Vitamin D supplementation should be provided
Liquid supplements may be useful if preparing meals is overwhelming.
Encourage full involvement with psychotherapy, cognitive behavioral therapy,
or interpersonal therapy. These are helpful adjuncts for medication.
Teach creative menu planning and food preparation methods that address
the side effects and symptoms the patient is experiencing
Promote use of whole foods (fruits, vegetables). Discourage regular use of
fried foods, processed foods, rich desserts, processed meats.
Promote exercise
Limit caffeine
(Escott-Stump, 2015, p.289-290).
While KG was consuming adequate protein from chicken and her Ensure Enlives,
her food choices were very limited. Promoting a Mediterranean style diet with a higher
intake of whole foods sources like fruits and vegetables was encouraged, and while the
liquid supplements could be useful, KG wanted to move towards eating whole foods and
keeping the Ensure Enlives as a back-up instead of her go-to meal. Cognitive behavioral
therapy was utilized both by myself and the inpatient psychiatric unit to aid KG in her
recovery. The psychiatric unit utilized self monitoring by having KG report any feelings
of suicidal ideation, social support through daily group activities including dance, food
demonstrations, art projects and group therapy, stress management through having KG
identify her stressors/triggers such as medications or sharp objects, and relapse
10

Schuette
prevention through use of therapy, coping mechanisms, identifying stressors, and having
KG agree to go back to the South Nassau partial program upon discharge and to alert
staff, family or friends if she experienced more suicidal ideations. There has been a
plethora of evidence supporting the use of cognitive behavioral therapy in those with
anxiety and depression. One study showed that 44% of participants who participated in
cognitive behavioral therapy-centered group therapy experienced significant
improvement in depression (Thimm, et. al., 2014). The strategies I utilized with KG
included creative meal planning through self monitoring using a food and feelings
journal, problem solving through alternative ways to consume produce, goal setting by
helping KG set the goal of trying three smoothies recipes I provided to her, social support
by helping KG identify how her parents could assist her in meeting her goal, and stimulus
control by identifying ways KG could meet her goal without experiencing potentially
triggering things such as sharp objects (knives for cutting produce).
Suicidal Behavior
Background
Suicide ranks 11th among causes of deaths in the US. An estimated 700,000
Americans attempt suicide every year, though the true incidence is likely underestimated,
as statistics on suicidal behavior are based mainly on death certificates and inquest
reports. 3.5-12.5% of those who make an attempt eventually die by suicide because so
many people make repeated attempts. About 20-30% of people who attempt suicide
try again within one year (Albert, et. al., 2011, p.1579). KG had made a prior suicide
attempt by overdosing on Tylenol pills in 2015.
11

Schuette
Diagnostic Criteria
Suicidal behavior includes three types of self-destructive acts: completed suicide
(resulting in death), attempted suicide (an act intended to be self-lethal, but that does not
result in death. Typically involves some ambivalence about wishing to die and may be a
cry for help) and suicide gestures (attempts that involve an action with a very low lethal
potential, such as superficial scratching. These should not be dismissed, as they are a cry
for help). Thoughts and plan about suicide are referred to as suicidal ideations. (Albert,
et. al., 2011, p.1579). KG has attempted suicide twice, once in 2015 and once before her
current admission on 2/12/19.
Medical Interventions
If an overdose of a potentially lethal drug is confirmed, immediate steps are
taken to prevent absorption and expedite excretion, administer any available
antidote, and provide supportive treatment.
All patients require psychiatric assessment.
After an attempt, patients may deny any problems because the depression that led
to the suicidal act may be followed by an elevation in mood. Still, the risk of later,
completed suicide is high, and patients should be admitted to a psychiatric unit
until medically cleared as low risk for suicide.
Prevention is the number one form of medical intervention. The National Suicide
Hotline is an easily accessible way for people having suicidal ideations to obtain
immediate help. Proven psychotherapies for treatment/prevention include
cognitive behavioral therapy (CBT) for suicide attempters, and dialectical
12

Schuette
behavioral therapy (DBT) for those with borderline personality disorder and
recurrent suicidal ideation.
If an overdose of a potentially lethal drug is confirmed, immediate steps are
taken to prevent absorption and expedite excretion, administer any available
antidote, and provide supportive treatment.
All patients require psychiatric assessment.
After an attempt, patients may deny any problems because the depression that led
to the suicidal act may be followed by an elevation in mood. Still, the risk of later,
completed suicide is high, and patients should be admitted to a psychiatric unit
until medically cleared as low risk for suicide.
Prevention: National Suicide Hotline. Proven psychotherapies for
treatment/prevention include cognitive behavioral therapy (CBT) for suicide
attempters, and dialectical behavioral therapy (DBT) for those with borderline
personality disorder and recurrent suicidal ideation.
(Albert, et. al., 2011, p.1580-1581).
KG’s admitting diagnosis was an intentional drug overdose, and corrective
measures were immediately taken to stabilize her. Once this was accomplished, she
received a psychiatric assessment which concluded that she needed to be admitted to
Syosset Hospital’s inpatient psychiatry unit until she could demonstrate she was no
longer at risk for suicide. Cognitive behavioral therapy was utilized throughout her stay
to promote overall wellness and decrease symptoms of suicidal ideations.
13

Schuette
KG’s Present Admission
Anthropometrics
At time of admission 2/12/19:
Weight: 116.16lb. 52.8kg
IBW: 120lb. UBW: 120lb. BMI: 20.6
Height: 5’3” 160.02cm
%IBW: 96.8% %UBW: 96.8% Classification: Normal
Current Admission Weights
Date Weight
2/12/19 52.8kg/116.16 #
2/20/19 53.0 kg/ 116.6 #
At time of admission, KG stated her weight had been stable between 115-120lb.
since 9/2018. Prior to this, KG experienced a significant unintended 37.5% weight gain
from 120lb. to 165lb. between 6/2016 to 10/2016 secondary to unspecified psychiatric
related medications. KG consulted with her physician, switched to taking 2mg of
Klonopin BID, and reduced her PO intake to achieve a significant intended 45lb (30%)
loss in 3 years.
Upon performing a nutrition-focused physical exam (NFPE), KG appeared to
have no notable fat loss or muscle wasting, and appeared well nourished overall. As per
nursing documentation, KG’s skin was WDL and she had no edema or pressure injuries
during her length of stay.
Diet History
At baseline, KG identifies herself as a picky eater, defining her eating style as
“like a 5-year-old”, which she explained meant she survives mainly on “bread products,
14

Schuette
cheese, and chicken.” KG struggles with certain textures and consistencies, mainly those
in fruits and vegetables. KG refuses to eat any fruits or vegetables in their whole foods
form. She states her dislike of fruits and vegetables worsened when she vomited a fruit
salad she was served during her hospital admission after her last suicide attempt in 2015.
She tried juicing produce three years ago and loved it, but found it to be too labor-
intensive, so she stopped one year ago and reports she has not had a fruit or vegetable
since winter of 2017 except for orange juice and potatoes. A typical intake at home
includes a plain bagel, waffles or pancakes with one glass of orange juice for breakfast,
followed by a sandwich with Skippy creamy peanut butter or a grilled cheese sandwich
with two slices of American cheese and two pouches of Welches fruit snacks for lunch.
Alternatively, if she is not hungry, KG will have 1 vanilla Ensure Enlive can for lunch.
For dinner, KG typically consumes 3-4 chicken tenders and French fries. KG’s fluid
intake includes the glass of orange juice at breakfast plus 2-3 12oz. bottles of water
throughout the day.
In the hospital, KG’s diet order was initially non-existent. During our first
interview when she did not have a diet order, she stated she was hungry and willing to try
food, but fearful that it would cause GI distress, and requested a vanilla Ensure Enlive.
Later that day (the 12th), her diet order was put in as “regular,” and this remained her
order for her length of stay. Her typical intake in the hospital mirrored that of her intake
at home, and as reported by herself and the diet technician, the only variance between her
daily meals was whether she ate a bagel or 2 pancakes at breakfast. The following tables
provide a more in depth analysis of her hospital meals, and demonstrate that, while the
food sources were less than optimal, KG was indeed meeting the majority of her nutrient
15

Schuette
needs, mostly due to consuming 2 Ensure Enlive cans daily. However, they were also
providing her with an excessive 70g of added sugar/day, which could possibly exacerbate
her anxiety and depression symptoms. Her oral intake is significantly deficient in fiber,
potassium, vitamin K, omega-3 fatty acids, iron, magnesium and manganese, and she is
slightly over-consuming her recommended amount of protein. These all could be
corrected with a more diverse and higher quality diet, and I discussed this with KG once
she indicated she wanted to attempt to add produce back into her diet. Regarding fluids,
KG reported that she consistently consumed 4-6 cups of water daily in addition to a glass
of orange juice. By this measure, she was not meeting her estimated fluid needs of 1.3-
1.5L fluid/day. I encouraged greater fluid intake, and KG stated she would try harder, but
it was clear this was not a high priority for her. Since her electrolytes remained within
normal range throughout her length of stay, I did not feel this needed to be more seriously
addressed at the time.
16

Schuette
Hospital PO Intake Analysis 1: 1 plain bagel, 1 cup orange juice, 2 cans Ensure
Enlive, 1 grilled cheese sandwich, 1 3oz. serving grilled chicken breast
17

Schuette
Hospital PO Intake Analysis 2: 2 buttermilk pancakes, 1 cup orange juice, 2 cans
Ensure Enlive, 1 grilled cheese sandwich, 1 3oz. serving grilled chicken breast
18

Schuette
Medications
KG was prescribed the following medications during her length of stay:
1. Haloperidol tabletIndication: AntipsychoticDrug: take with food or milk to decrease GI distress. Diet: Do not mix with coffee or tea—drug may precipitate.Oral/GI: Dry mouth, dyspepsia, N/V, constipation, diarrheaS/Cond: avoid alcohol.Blood/serum: Increases prolactin, increases or decreases WBC, anemia, increases or decreases glucose, decreases Na+Monitor: CBC with long-term use
2. Lorazempam tablet (Benzodiazepine: Comparable to Klonopin)Indication: antianxietyDrug: may take with food if GI distress occursDiet: limit caffeine. Caution with grapefruit/related citrus, caution with herbal products or stimulant productsNutr: Anorexia, decrease weight, increase appetite, increase weight, increase thirstOral/GI: dry mouth, increased salivation, N/V, constipation, diarrheaS/Cond: avoid alcoholOther: Ataxia, sedation, slurred speech, fatigue, drowsiness, dizziness, confusion, headache, depression, palpitations.Blood/serum: Increases AST, ALT, LDH, bil, alk phos.Monitor: CBC with long-term use
3. BuspironeIndication: antianxietyDrug: food increases bioavailabilityDiet: Avoid grapefruit/related citrus, avoid St. John’s Wort.Oral/GI: Sore throat, nausea, diarrheaS/Cond: avoid alcohol. Blood/serum: May increase AST, ALT 4. Aluminum hydroxide/magnesium hydroxide/simethicone suspensionIndication: antacid, anti-flatulentDrug: take 1 hour after mealsDiet: Take Fe or Fol supplement separately by 2 hoursOral/GI: Chalky tasteBlood/serum: decreases P, K, Ca, increases Mg
5. Zolpidem Indication: sleep aidDiet: Do not take right after a meal, as food decreases absorption.Oral/GI: Dry mouth, pharyngitis, N/V, hiccups, diarrhea, constipation
19

Schuette
S/Cond: Avoid alcohol.Other: Drowsiness, dizziness. May increase anxiety and depression
6. Venlafaxine XRIndication: Antidepressant, antianxietyDrug: take with food to decrease GI upset.Diet: Avoid St. John’s WortNutr: May cause anorexia, decrease weight, increase appetite, increase weightOral/GI: dry mouth, taste changes, N/V, dyspepsia, constipation, diarrhea, flatulence S/Cond: Avoid alcohol.Other: Drowsiness, dizziness, sexual dysfunction, weakness, nervousness, anxiety, confusion, suicidal thinking and behaviorBlood/serum: Increase chol, increase or decrease glucose, increase uric acid, increase AST, increase alk phos, decrease K.Monitor: BP
The side effects KG experienced from these medications are underlined. When
she was first admitted, she was experiencing slurred speech and confusion, which can be
caused by Lorazepam as well as other benzodiazapines. In KG’s case, the side effects
were due to Klonopin, which was the medication she overdosed on. Because of this
history, she was not allowed to take Klonopin for the majority of her length of stay and
repeatedly reported “feeling terrible” on the Lorazepam. Two days before she was
discharged, a compromise was made with her doctor to try Klonopin at 1.5mg PO BID,
and KG reported decreased anxiety and nervousness within a day. Upon discharge, her
Klonopin dose was titrated to 2mg PO BID, which was the dosage she was prescribed
before her admission. Overall, she reported consistently feeling drowsy and weak.
Initially she still had suicidal ideations, though these subsided completely by 2/20/19. She
also reported generalized anxiety, depression, occasional nervousness and dizziness.
Lab Values
Date Benzodiazepine Salicylate (toxic range: >30)
20

Schuette
2/12/19 Positive 29.5
Date Hgb(12-16 g/dL)
Hct(35-47%)
MCV(78-93 μm3/RBC)
Fasting Glucose(70-99 mg/dL)
Ca++ Phos BUN
2/12/19 10.7, low 32.4%,
low
96.1 103, high 8.2, low 3.9 9.0
2/20/19 10.9, low 33% 97.1 108, high 8.2, low 3.8 9.3
Date WBC RBC Creatinine Na+ Cholesterol Mg++ K+
2/12/19 5.3 3.37, low 0.59 142 189 1.8 4.1
2/20/19 5.5 3.40, low 0.61 137 185 1.8 4.2
Upon admission to the emergency room on 2/12/19, a Therapeutic
drug/toxicology screen showed positive benzodiazepine levels and an elevated salicylate
level at 29.5. These confirmed the types of medications KG had overdosed on, and
corrective measures were taken immediately so that these became normalized. Hgb and
Hct with normal MCV indicates that KG has normocytic anemia. It is likely that this is
secondary to her Haloperidol use, which she was also taking prior to admission. Her low
RBC and calcium indicate a possible vitamin D deficiency, though the low calcium could
also be secondary to her Aluminum Hydroxide medication. Given her medical history, I
would have liked to see KG’s serum vitamin D, vitamin B12, folate and iron levels
checked, but this did not occur at any point during KG’s admission. As was noted in her
charts, this was because managing her psychiatric issues was a higher priority for her
physician than correcting the anemia that was likely secondary to her psychiatric
21

Schuette
medications. Even so, I feel it would have been appropriate to start her on a vitamin D
supplement, which I suggested but was never done. Her slightly elevated glucose level
may have been secondary to long-term Haloperidol use and Venlafaxine use. Because it
was so close to the normal range for fasting blood glucose, no corrective measures were
taken, though her glucose did continue to be monitored through her length of stay.
Overall, KG’s labs throughout her hospitalization indicate that her anemia did not
improve. In her discharge note, it was documented by her physician that she was to
follow up with her primary care physician regarding managing the anemia. I focused on
encouraging intake of iron rich food sources with KG, including her chicken and plant
sources that she might include in the smoothies I suggested she try. I also stated she
should talk to her primary care physician about the possibility of taking a vitamin D
supplement.
Labs 2/12/19:
1. PhosNorm 3-4.5mg/dlIncreased associated with hypoparathyroidism and hypocalcemia.Decreased associated with hyperparathyroidism, chronic antacid ingestion, and renal failure
2. Na+Norm 136-144 mEq/LIncreased (hypernatremia) with dehydration & low fluid intake, diabetesDecreased (hyponatremia) with edema, severe diarrhea/vomiting, diuretics, hyperglycemia, malabsorption
3. BUNNorm 8-23 mg/dLIncreased with shock, dehydration, infection, DM, excessive protein intakeDecreased with malnutrition, malabsorption, overhydration
4. Creatinine
1. Phos: 3.9, WNL
2. Na+: 142, WNL
3. BUN: 9.0, WNL
22

Schuette
Norm .4-1.2 mg/dLIncreased with muscle damage, starvation, muscle mass, acute & chronic renal diseaseDecreased with pregnancy
5. GlucoseNorm (fasting) 70-99 mg/dLIncreased with DM, K deficiency, drugs (corticosteroids, high dose antihypertensives, cyclosporine), pancreatitis, sever infections, chronic hepatic dysfunction and disease.Decreased with insulin overdose, bacterial sepsis, extensive liver disease, starvation, alcohol abuse, vigorous exercise, pancreatitis
6. HgbNorm (female) 12-16g/dLIncreased with dehydration, COPD, severe burns, CHFDecreased with anemia, cirrhosis, hyperthyroidism
7. HctNorm (female) 35-47%Increased with dehydration, polycythemia, shockDecreased with anemia, blood loss, hemolysis, leukemia, hyperthyroidism, cirrhosis, over hydration
8. Mean Corpuscular Volume (MCV)Norm 78-93 mm3/RBCIncreased with megaloblastic anemia due to Fol or Vit B def, liver diseaseDecreased with Fe deficiency anemia, hereditary spherocytosis, thalassemia minor, sideroblastic anemia, lead poisoning
9. RBCNorm (female) 4.2-5.4 1012/LIn addition to nutritional deficits, may be decreased in those with hemorrhage, hemolysis, genetic aberrations, marrow failure, or renal disease.
10. Ca++Norm 8.4-10.5mg/dlIncreased (hypercalcemia) associated with endocrine disorders, malignancy, and hypervitaminosis D.Decreased (hypocalcemia) associated with Vitamin D deficiency and inadequate hepatic or renal activation of vitamin D, hypoparathyroidism, magnesium deficiency, renal failure, and nephrotic syndrome.
11. K+Norm 3.5- 5.0mEq/LIncreased (hyperkalemia) with renal failure, tissue
4. Creatinine: 0.59 WNL
5. Glucose @ 7:52am: 103. ↑
6. Hgb: 10.7, ↓
7. Hct: 32.4, ↓
8. MCV: 96.1, WNL
9. RBC: 3.37, ↓
10. Ca++: 8.2, ↓
11. K+: 4.1, WNL
23

Schuette
damage, acidosis, uncontrolled DM, overuse of K supplementDecreased (hypokalemia) with GI loss, malabsorption, malnutrition, diarrhea, vomiting, chronic stress or fever, K depleting diuretic
Estimated Nutrient Needs/Hospital Diet Order
Since KG had a normal BMI of 20.6 and was 96% of her IBW and UBW at
116.16lb (52.8kg), calorie needs were determined for maintenance at
25-30kcal/kg/day:
o 52.8 kg x 25kcal = 1,320kcal/day | 52.8 kg x 30kcal = 1,584kcal/day
Protein needs were determined using 0.75-1.0 g/kg actual body weight.
o 52.8 kg x 0.75 g/kg = 39.6g | 52.8 kg x 1.0 g/kg = 52.8g
CHO needs are not determined in the hospital for patients on a “regular” diet
order. The RDA for adult females is 45-65% of total calories, or 654-944g/day.
Fat needs are not determined in the hospital. The RDA for adult females is 25-
35% of total calories, or 363-508g/day.
RDA Vitamins/Minerals Recommendationsfor adult females ages 31-50years old
Nutrient AmountVitamin A 700 mcg/dayVitamin E 15 mg/dayVtaimin D 600 IU/dayVitamin K 90 mcg/day
Folate 400 mcg/dayB12 2.4 mcg/dayIron 18 mg/day
Phosphorus 700 mg/dayZinc 8 mg/day
Sodium 1,500 mg/ddayPotassium 4,700 mg/dayCalcium 1000 mg/day
24

Schuette
Vitamin C 75 mg/day
Nutrition Care Process
Assessment
On 2/12/19, KG presented with inadequate oral intake related to psychological
causes (admitting diagnosis of suicide attempt by drug overdose, history of depression
and anxiety) as evidenced by limited food/beverage intake (patient reported not eating x2
days).
Interventions
At time of initial assessment, a diet order had not being placed so KG was NPO.
When medically feasible, her diet should be advanced as tolerated. One can Vanilla
Ensure Enlive recommended BID to help patient meet estimated nutrient needs.
Goal 1: Once diet is advanced, patient will consume 50%+ of meals plus nutrition supplement x 1 week.
Plan 1:o Diet technician will provide patient with
hospital menu and take food preferences so as to optimize PO intake.
o RD will follow up with patient in 1 week.o Nurses will monitor patient’s PO intake
and diet tolerance.
Monitoring and Evaluation:
Weight
PO intake
Appetite
Labs: Glucose, B12, vitamin D, serum iron.
Upon follow up on 2/19/19, KG’s diet order had been advanced to “Regular” with
one can Vanilla Ensure Enlive BID, and it was reported that she was tolerating the diet
25

Schuette
and meeting her calorie needs. At this point, KG provided me with her diet history prior
to admission and admitted that her intake in the hospital had been very similar. Her long-
term dependence on the Ensure Enlives fit the category of supplements acting as a
“magic answer” in therapy as described by the MNT for psychiatric disorders table
(Mahan and Raymond, 2017, p.848), and her other limited food choices of bread, cheese
and chicken fit the category of food choices resulting in suboptimal nutritional intake. We
discussed her limited food acceptance, and she stated she desired to consume more “real
foods” and felt that eating produce could help her feel better, but she just couldn’t stand
the texture. Studies have shown that increasing fruit and vegetable consumption to the
recommended five servings per day or higher can lead to decreased anxiety and
depression symptoms (Biswajit, et.al., 2017), so when KG expressed she was interested
in this, I felt it was appropriate to focus on. We used the CBT strategy of problem solving
to brainstorm ways KG could increase her produce consumption. When I brought up
making and drinking smoothies as a possibility, KG told me she had never tried a
smoothie, but was very open to trying one. Do to her limitations of not wanting to be
around sharp objects and being unable to grocery shop for herself due to the anxiety it
gave her, we problem solved ways to overcome these obstacles, utilizing the CBT
strategy of stimulus control. This included using yet another CBT strategy, social
support, through her parents, who would do the grocery shopping and prepare the
smoothies for her. Another possibility was to have her parents buy pre-cut produce that
she could then juice or blend herself, or buy pre-made juices and smoothies for her.
On 2/19/19, KG presented with limited food acceptance related to aversions to
food in mouth/throat and self-limitation of foods/food groups due to food preference as
26

Schuette
evidenced by patient reporting a diet history including limited food/beverage intake
inconsistent with nutrition reference standards for type, variety, and diet quality.
Additionally, KG made a number of comments supporting this diagnosis, including, “I
eat like a 5-year-old”, “I pretty much live on bread products, cheese and chicken
tenders”, “I don’t eat fruits and vegetables because I don’t like the texture, but I like the
flavor and want to eat more whole foods. I think that could help” and “My medications
make me not hungry sometimes.”
Goal 1: Upon discharge, patient will increase fruit and vegetable intake to 1-3 servings per week within 1 month.
Plan 1:o Nutritionist will provide patient with 5
smoothie recipes to tryo Patient will give her parents the smoothie
recipes provided to her by nutritionist, and they will prepare at least 3 of the 5 recipes for her, which she will taste
o Nutritionist will provide patient with basic oral education regarding the value of increasing whole foods intake for improved mental health.
Later that week, on 2/22/19, I informally checked in with KG to provide her with
the smoothie recipe ideas and discuss her PO intake in hospital. She stated her appetite
had been good and admitted her PO intake in the hospital was still the same as the last
time I saw her, but she was excited to try the smoothies when she was discharged because
she wanted to be healthier. At this time, I had her restate her goal and plans, and we
discussed the possibility of adding the goal of maintaining a “food and feelings diary,”
where KG would write down how she felt about each of the smoothies she tried one hour
after eating them and one more time the same day.
Monitoring and Evaluation
PO Intake
27

Schuette
Feelings regarding smoothies
Feelings throughout the day (specifically, any increase or decreased feelings of
anxiety or depression)
Progress, Prognosis and Future Plans
KG experienced significant improvement during her length of stay. Progress
reports from the hospital social worker reported that she stopped having suicidal ideations
by 2/20/19. Increasing her Venlafaxine XR and the addition of Buspirone were
documented as helping with relieving her symptoms of depression and anxiety, and the
addition of klonopin back into her regimen on 2/22/19 was noted to improve her anxiety.
An evaluation on 2/21/19 showed KG was at low risk for suicide. She was able to
identify reasons for living, including her family and her friends, and that she was learning
to live for herself. She also reported feeling hopeful about her future. Additionally, KG
was able to identify coping skills, including asking others for help, using progressive
muscle relaxation, and listening to music. Social work provided KG with phone numbers
for the LI Crisis Center, National Suicide Hotline, and the phone number and address for
Zucker Hillside Crisis Walk in Center. She reported that if she had suicidal ideations at
home, she would tell her parents, go to the nearest emergency room, call the LI Crisis
Center or Suicide Hotline, or go to Zucker Hillside Walk in Center. Finally, KG was
reported to have improved mood, and was noted to be more stable and less fragile.
On 2/25/19, KG was discharged with the following diagnoses and discharge plan:
Discharge diagnosis: Major depression disorder
Goal: Patient will report and exhibit improved, stable mood
28

Schuette
Assessment and plan of treatment: Patient reports and exhibits euthymic, stable
mood.
Secondary discharge diagnosis: Generalized anxiety disorder
Goal: Patient will report less anxiety and improved coping skills
Assessment: Patient reports less anxiety, is less fragile and reports improved
coping skills.
Discharge plan: Upon discharge, patient will go to South Nassau partial hospitalization
program, as per discussion with patient’s parents and outpatient prescriber at SNG.
Patient’s parents will keep medications under lock and key at home.
29

Schuette
References
Albert, R.K., et al. (2011). The MERCK Manual, 19th edition.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Association.
Baldwin, D, et. al. (2012). Anxiety Disorders Research Network Annual Report. European College of Neuropsychopharmacology,
Bishwajit, G., et. al. (2017). Association Between Depression and Fruit and Vegetable Consumption Among Adults in South Asia. BMC Psychiatry. 17(15). doi: 10.1186/s12888-017-1198-1
Escott-Stump, S. (2016). Nutrition and Diagnosis Related Care (8th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Mahan L.K., & Raymond J.L. (2017). Food and the Nutrition Care Process, 14th edition. St. Louis, Missouri: Elsevier
Thimm, JC, and Antonsen, L (2014). Effectiveness of cognitive behavioral group therapy for depression in routine practice. BMC Psychiatry, 14(1), 292.
30