Embed Size (px)
Citation preview

Patient safety incidents and adverse events in ambulatory dental care: a systematic scoping review
Eduardo Ensaldo-Carrasco MSc, Centre of Medical Informatics, Usher Institute of Population Health Sciences and Informatics, The University of Edinburgh, Scotland, UK
Milton Fabian Suarez-Ortegon MSc, Centre for Population Health Sciences, Usher Institute of Population Health Sciences and Informatics, The University of Edinburgh, Scotland, UK
Andrew Carson-Stevens MB BCh MPhil, Patient Safety Research Lead, Primary and Emergency Care Research (PRIME) Centre, Cardiff University, Wales & Visiting Professor of Healthcare Improvement, Department of Family Practice, University of British Columbia
Kathrin Cresswell PhD, Senior Research Fellow, Centre of Medical Informatics, Usher Institute of Population Health Sciences and Informatics, The University of Edinburgh, Scotland, UK
Raman Bedi, Professor and Head Centre for International Child Oral Health. King’s College London Dental Institute at Guy’s, King’s College and St Thomas’s Hospitals, Division of Population and Patient Health, King’s College London, United Kingdom
Aziz Sheikh MD, Professor of Primary Care Research & Development and Co-Director, Centre of Medical Informatics, Usher Institute of Population Health Sciences and Informatics, The University of Edinburgh, Scotland, UK
Address for correspondence:
Eduardo Ensaldo CarrascoCentre of Medical Informatics, Usher Institute of Population Health Sciences and Informatics, The University of Edinburgh, Scotland, UKSources of support
Eduardo Ensaldo Carrasco acknowledges the support of the Mexican National Council for Science and Technology (CONACYT) and Mexico's Ministry of Education (SEP). We also gratefully acknowledge the support of Marshall Dozier, Academic Liaison Librarian at The University of Edinburgh
1
12
3
4567

AbstractBackground: There have been efforts to understand the epidemiology of iatrogenic harm in hospitals and primary care, and to improve the safety of care provision. There has in contrast been very limited progress in relation to the safety of ambulatory dental care.
Objectives: To provide a comprehensive overview of the range and frequencies of existing evidence on patient safety incidents and adverse events in ambulatory dentistry.
Methods: We searched MEDLINE and EMBASE for articles reporting events that could have or did result in unnecessary harm in ambulatory dental care. We extracted and synthesized data on the types and frequencies of patient safety incidents and adverse events.
Results: 40 articles were included. We found that the frequencies varied very widely between studies; this reflected differences in definitions, populations studied and sampling strategies. The main five PSIs we identified were errors in diagnosis and examination, treatment planning, communication, procedural errors and the accidental ingestion or inhalation of foreign objects. However, little attention paid to wider organizational issues.
Conclusions: Patient safety research in dentistry is immature since current evidence cannot provide reliable estimates on the frequency of patient safety incidents in ambulatory dental care or the associated disease burden. Well-designed epidemiological investigations are needed that also at the same time investigate contributory factors.
2
89
101112
131415
16171819
20212223242526
2728293031
32
33

IntroductionAdverse events (AEs) occur in healthcare settings worldwide; 1, 2 it is estimated that between 30-50% of these events can be prevented.2-5 This issue gained popularity in 1991 following the publication of the Harvard Malpractice Study, which provided population-based data demonstrating that substantial numbers of patients were being harmed during the provision of hospital care.6 In 2000, the Institute of Medicine (IOM) estimated, for the United States, up to 98,000 deaths per year resulted from iatrogenic harm during inpatient care.7 It is generally accepted that AEs occur in approximately 10% of hospital admissions internationally.2-5, 8 These landmark studies have spawned a growing field of patient safety (PS) research over the subsequent two decades. In 2002, the resolution 55.18 of the World Health Assembly has recognized AEs as a public health concern.9
Concepts for patient safety (PS), patient safety incident (PSI) and AEs have been developed (Table 1). Also, the field has moved on from describing the extent of harm to the underlying causes and, more recently, interventions designed to reduce harm.10 However, progress in primary care is more limited,10, 11, 12, 13 particularly in dentistry,14, 15 probably to the assumption that this sector is safer than the hospital sector.16 Nonetheless, injuries with varying degrees of harm can occur among dental patients.17-19
Table 1. Concepts developed for patient safety research in hospital settings. Concept Definition
Patient safety The reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum20
Patient safety incident An event or circumstance that could have resulted, or did result, in unnecessary harm to a patient.20
Clinical error The failure to carry out a planned action as intended or the application of an incorrect plan.21
HarmImpairment of structure or function of the body and/or any deleterious effect arising, including disease, injury, suffering and death.20
Adverse eventAn injury that was caused by medical management or complication instead of the underlying disease and that resulted in prolonged hospitalisation or disability at the time of discharge from medical care or both.20
Injury Damage to the tissues caused by an agent or event.20
Never eventsSerious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented.22
The introduction of Incident Reporting Systems (IRSs) has been recommended, 23 although only Thusu et al (2012) have studied this resource. 24 Moreover, the efficacy of current PS strategies in dentistry is unclear as they have not been tested. 25
3
34353637383940414243444546
47484950515253
54
55565758
Research into the conceptual understanding of PS and epidemiology of PSIs in dentistry is needed.25 National Dental Associations have called for more information about unsafe dental care and to learn lessons from errors. 26
However, the scope of the current field of research is not clear and no concerted efforts have been made to date to systematically scrutinize existing empirical PS research. This study focuses on the systematic scoping of the global literature about the range and frequencies of PSIs and AEs arising from ambulatory dentistry. This review is important and timely given the World Health Organization’s (WHO) emerging agenda for “Safer Primary Care”, 27 advocating for a better understanding of PSIs, AEs and key knowledge gaps in primary care patient safety.
MethodsWe undertook a systematic scoping review of the literature28, 29 based on the framework developed by Levac et al.29 and systematic review principles. In contrast to systematic reviews, this technique is recommended to map broad topics, especially where the body of evidence is still emerging. 28, 29
Data sources and search strategyA search strategy was conducted in MEDLINE and EMBASE with a set of medical subheading (MeSH) and free-text terms (Appendix 1). The year of publication of “Error in Medicine” 30 was chosen to initiate the screening period which ranged from January 1994 to January 2015. A “snowball” approach31 was used in all the eligible full-text articles to identify any missed relevant publications.
Eligibility criteriaWe included cross-sectional studies that reported any type of event that could have or did result in unnecessary harm due to ambulatory dental care. Dental ambulatory care settings included all individual, community practices, private practices and hospital outpatient clinics. 32
Articles were excluded if harm or potential harm was not the main outcome, such as papers addressing the effectiveness of treatments (e.g. bleaching procedures). Opinion studies, forensic studies, disease risk management, as well as recommendations for antibiotic prophylaxis, treating patients with pre-existing medical conditions or occupational hazards were also discarded.
Articles that reported PSIs or AEs but lacked information about their frequency were eliminated.
Types of included studiesThe following study designs were considered for inclusion:
Epidemiological studies (e.g. descriptive and analytical studies).
4
5960616263646566676869
7071727374
75767778798081
8283848586
8788899091
9293
9495
96

Outcome measuresThe primary outcomes were PSIs and AEs as defined in Table 1.
Study selectionTwo reviewers (EEC & FSO) independently reviewed the articles for inclusion. The citations were imported into EndNote x6 (Thomson Reuters; http://www.endnote.com) where all duplicates were deleted. Initially, only the title and abstracts were screened. Then, full-text copies were obtained and assessed for eligibility. If not available, authors were contacted and a copy was requested. In case of a disagreement, a third reviewer (AS) was consulted. The reporting of the results followed the Preferred Reporting Items for Systematics Reviews and Meta-analyses (PRISMA) checklist. 33
Data extraction and analysisData were extracted into a customized form in Microsoft Excel 2011 (Microsoft Corporations, Redmond, WA). The main categories for data extraction (Table 3) were agreed by the reviewers. They met after extracting the first five articles to determine if the extraction approach was consistent with the objectives of the study. Working definitions for PSIs and AEs were recorded.
Table 3. Main categories for data extraction
Authors Measurement method
Publication year Types of patient safety incidents
Discipline Frequencies of patient safety incidents
Research design Types of adverse events
Method for data collection Frequencies of adverse events
Data summary and synthesisThe scoping review method retrieves a wide heterogeneity of articles. 34
Therefore, the estimation of frequencies or associations were not sought. Instead, the findings were described and synthesized into two main conceptual domains: 1) the types and frequencies of PSIs and 2) the types and frequencies of AEs.
ResultsA total of 8386 potentially relevant articles were retrieved from which 40 were included (Figure 1).
5
979899
100101102103104105106107108
109110111112113114115
116
117
118119120121122123
124
125126127

Figure 1. PRISMA diagram
Included
Eligibility
Screening
Identification
40 articles included in the scoping review
48 full text articles excluded (non empirical work)
578 records excluded as duplicates
88 full-text articles assessed for eligibility
7721 records excluded:non relevant (n=7708),
duplicates (n=13)
After de-duplication, 7808 potentially relevant papers were included for title and abstract
screening
8386 potentially relevant papers were identified
35 records identified from reference lists
6166 records retrieved from MEDLINE and 2185 from
EMBASE
6
128

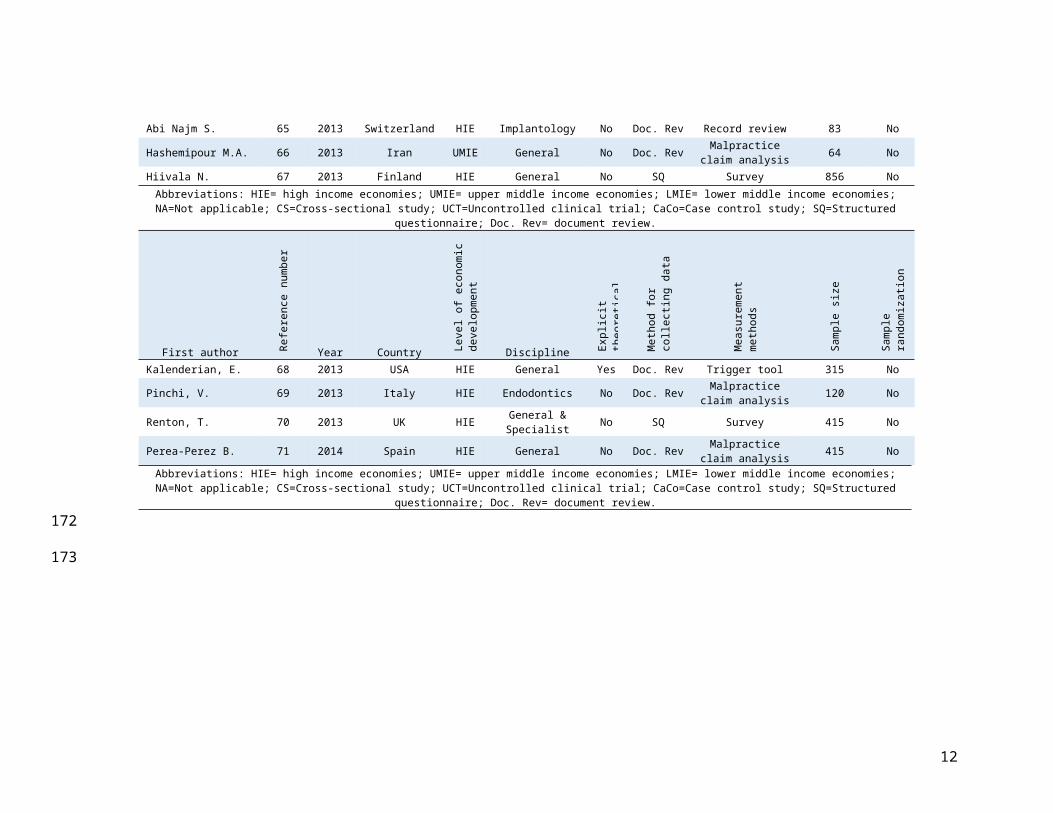
The general characteristics of these articles are displayed in Table 4. The relative percentage of publications substantially increased from 15% (n=6) in the first four years (1994-1998) to 37.5% (n=15) in the last four years (2011-2015). Healthcare systems within high-income economies were the source of the majority of the publications (92.5%, n=37) in which general dentistry ranked as the top discipline (27.5%, n=11), followed by endodontics, legal medicine and studies reporting various disciplines (15% n=6 each). Fewer articles were found for oral surgery (12.5% n=5), pediatric dentistry (7.5% n=7.5), implantology (5.0% n=2) and orthodontics (2.5% n=1).Most studies concerned private practices (72.5%, n=29) and dental schools (22.5%, n=9), whereas only 5% were in outpatient hospital clinics (n=2).
Documentary review (75%, n=30) and structured questionnaires (25%, n=10) were the only methods identified for data collection. The sample sizes varied substantially from 11 to 2830000 participants. None of the included articles used a randomized sample.
Key findingsThe results were ordered into the conceptual domains displayed in Figure 2. Each of these will be described in turn.
7
130131132133134135136137138139140
141142143144
145
146147148149

Table 4. Main characteristics of included articles.
First author Refe
renc
e nu
mbe
r
Year Country Leve
l of
econ
omic
deve
lopm
ent
Discipline Expl
icit
theo
retic
al
Met
hod
for
colle
ctin
g da
ta
Mea
sure
men
t m
etho
ds
Sam
ple
size
Sam
ple
rand
omiza
tion
Milgrom, P. 35 1994 USA HIE Various No SQ Survey 289 NoHaas, D.A. 36 1995 Canada HIE Various No Doc. Rev Malpractice
claim analysis 143 No
Lupi, J. E. 37 1996 USA HIE Orthodontics No Doc. Rev Radiographic review 88 No
Nkansah P.J. 38 1997 Canada HIE Various No Doc. Rev Survey 2830000* NoKeur I. 39 1998 Netherlands HIE General
dentistry No SQ Survey 471 No
Venta I. 40 1998 Finland HIE Legal medicine No Doc. Rev Malpractice claim analysis 237 No
Atherton G.J. 41 1999 UK HIE General dentistry No SQ Survey 1110 No
Ammar, WA.. 42 2000 Saudi Arabia HIE Legal medicine No Doc. Rev Malpractice claim analysis 32 No
Leelataweedwud, P. 43 2001 USA HIE Paediatric dentistry No Doc. Rev Record review 195 No
Givol, N 44 2002 Israel HIE Implantology No Doc. Rev Malpractice claim analysis 61 No
D´Eramo E.M. 45 2003 USA HIE Oral surgery No SQ Survey 157 NoFrangiskos, F. 46 2003 Greece HIE Oral surgery No SQ Direct
observation 250 NoTiwana k.K 47 2004 USA HIE Various No Doc. Rev Record review 36 NoOzdemir M.H. 48 2005 Turkey UMIE Legal medicine No Doc. Rev Malpractice
claim analysis 11 No
Susini, G. 49 2007 France HIE Endodontics No Doc. Rev Malpractice claim analysis 24651* No
Bjorndal, L. 50 2008 Denmark HIE Legal medicine No Doc. Rev Malpractice claim analysis 482 No
Tzanetakis G.N. 51 2008 Greece HIE Endodontics No Doc. Rev Record review 2180 NoAbbreviations: HIE= high income economies; UMIE= upper middle income economies; LMIE= lower middle income economies; NA=Not
applicable; CS=Cross-sectional study; UCT=Uncontrolled clinical trial;; CaCo=Case control study; SQ=Structured questionnaire; Doc. Rev= document review.
8

First author Refe
renc
e nu
mbe
r
Year Country Leve
l of
econ
omic
deve
lopm
ent
Discipline Expl
icit
theo
retic
al
Met
hod
for
colle
ctin
g da
ta
Mea
sure
men
t m
etho
ds
Sam
ple
size
Sam
ple
rand
omiza
tion
Kleier, DJ 52 2008 USA HIE Endodontics No SQ Survey 314 NoGaffen, A. S. 53 2009 Canada HIE General No Doc. Rev Malpractice
claim analysis 182* No
Kiani, M. 54 2009 Iran UMIE Legal medicine No Doc. Rev Malpractice claim analysis 157 No
Lee, JJ 55 2009 Taiwan HIE Oral surgery No Doc. Rev Malpractice claim analysis 2,223,971 No
Peleg O. 56 2010 Israel HIE General No Doc. Rev Malpractice claim analysis 48 No
Tsesis, I. 57 2010 Israel HIE Endodontics No Doc. Rev Radiographic review 56175* No
Hisanaga, R 58 2010 Japan HIE Various No Doc. Rev Record review 37 NoGivol, N 57 2010 Israel HIE Endodontics No Doc. Rev Malpractice
claim analysis 720 No
Ashkenazi, M. 59 2011 Israel HIE Paediatric dentistry No SQ Survey 85 No
Obinata K. 19 2011 Japan HIE General No Doc. Rev Record review 23 NoPerea-Perez B. 60 2011 Spain HIE Legal medicine No Doc. Rev Malpractice
claim analysis 63 NoSoehardi A. 61 2011 Netherlands HIE Oral surgery No SQ Survey 157 NoHillerup, S. 62 2011 Denmark HIE Oral surgery No Doc. Rev Record review 241 & 115 NoChicka M.C. 63 2012 Canada HIE Paediatric
dentistry No Doc. Rev Malpractice claim analysis 17 No
Schwamburger N.T. 64 2012 USA HIE General No Doc. Rev Record review 1,468 NoThusu, S. 24 2012 UK HIE General No Doc. Rev Incident reports 2,012 NoAbi Najm S. 65 2013 Switzerland HIE Implantology No Doc. Rev Record review 83 NoHashemipour M.A. 66 2013 Iran UMIE General No Doc. Rev Malpractice
claim analysis 64 NoHiivala N. 67 2013 Finland HIE General No SQ Survey 856 No
Abbreviations: HIE= high income economies; UMIE= upper middle income economies; LMIE= lower middle income economies; NA=Not applicable; CS=Cross-sectional study; UCT=Uncontrolled clinical trial; CaCo=Case control study; SQ=Structured questionnaire; Doc. Rev=
document review.
9

First author Refe
renc
e nu
mbe
r
Year Country Leve
l of e
cono
mic
deve
lopm
ent
Discipline Expl
icit t
heor
etica
l fra
mew
ork
Met
hod
for c
olle
ctin
g da
ta
Mea
sure
men
t m
etho
ds
Sam
ple
size
Sam
ple
rand
omiza
tion
Kalenderian, E. 68 2013 USA HIE General Yes Doc. Rev Trigger tool 315 NoPinchi, V. 69 2013 Italy HIE Endodontics No Doc. Rev Malpractice
claim analysis 120 No
Renton, T. 70 2013 UK HIE General & Specialist No SQ Survey 415 No
Perea-Perez B. 71 2014 Spain HIE General No Doc. Rev Malpractice claim analysis 415 No
Abbreviations: HIE= high income economies; UMIE= upper middle income economies; LMIE= lower middle income economies; NA=Not applicable; CS=Cross-sectional study; UCT=Uncontrolled clinical trial; CaCo=Case control study; SQ=Structured questionnaire; Doc. Rev=
document review.
10
150
151

Figure 2. Conceptual model for the activity in patient safety research in community dental care. Abbreviations: GA=General anaesthesia, LA=Local anaesthesia.
Systemic effects of LA, GA & sedation
Oral cavity and surrounding structures
Systemic adverse
outcomes
Local adverse outcomes
Adverse events
Drug prescription errors and lack of follow-up
Errors in the implementation of the procedure & cognitive errors
Errors in documentation, diagnosis, initial clinical assessment, referral,
treatment planning & informed consent
Pre-operative stage
Intra-operative stage
Post-operative stage
Performance
Types and frequencies of PSIs
and associated consequences
Patient safety research activity in ambulatory dental care
11
152
153
Types and frequencies of PSIs Initially, PSIs were organized across three stages that were conceptualized as the period before clinical treatments were carried out (pre-operative stage), the period of clinical treatment (intra-operative stage) and the period after the clinical treatment (post-operative stage). Then, PSIs and their frequencies were grouped and presented across the main three identified measurement methods (Table 5). Based on this, our results show that malpractice cases and surveys were the methods that contributed the most to identify diverse types of PSIs.
Errors concerning administrative processes,35 examination and diagnosis, 35, 54, 57, 59, 67,
71 treatment planning, 48, 54, 56, 57, 59, 66, 71 communication, 54, 66, 67 informed consent42, 48, 50, 57, 59 and referral54, 56, 66 were identified pre-operatively. Examples of errors in referrals and treatment planning resulted in wrong tooth extractions56, 72 and jaw fractures61 respectively. Intra-operatively, confusion of the operator led to wrong-tooth extractions.56 Procedural errors included technical errors, broken instruments and tooth perforations. 35, 42, 44, 45, 50, 51, 59, 67, 69, 71 Inhalation and ingestion of foreign objects were related to broken instruments and flaws in handling small objects. 58 Drug prescription errors emerged post-operatively, 35, 50, 59, 71 along with flaws in follow-up in patients seeking legal assistance.35
12
154155156157158159160161
162163164165166167168169170171
172

Table 5. Variability of frequencies of patient safety incidents across three main measurement methods
Patient safety incidents Malpractice analysis (n=17) Surveys (n=10) Record review (n=8)
Ranges (%) References Ranges (%) References Ranges
(%) References
Pre-
oper
ativ
e st
age
Administrative errors ------ ------ 8.3 35 ------ ------Error in examination or diagnosis 11.4-24 35, 54, 57, 71 6.72-55 PSIs
6.5-8 NMs35, 59, 67 ------ ------
Errors in treatment planning 9.09-26.6 48, 54, 56, 57, 66, 71 2.4 59 ------ ------
Documentation errors 3.2-55 54, 66, 69 42 PSIs12 NMs
59 ------ ------
Communication errors 3.2-12.4 35, 54, 57, 66, 71 6.29 PSIs15.49 NMs
35, 59, 67 ------ ------
Informed consent errors 3.1-59.4 42, 48, 50, 57 6.2-11 PSIs4 NMs
35, 59 ------ ------
Referral 3.1-12 54, 56, 66 ------ ------ ------ ------
Intra
-ope
rativ
e st
age
Cognitive failure / action lapse/ confusion 13-26.2 56, 57 ------ ------ ------ ------
Procedural errors 5.9-49 42, 44, 50, 69, 71 <1-49 PSIs5 NMs
35, 45, 59, 67 1.83 51
Local anesthesia administration errors 41 63 <1 PSIs
1.26 NMs67 ------ ------
Inhaled & ingested objects <1-18.2 48, 49, 54, 66 <1-12 PSIs9-13.9 NMs
41, 45, 59, 67 <1 19, 47, 58
Failure to appropriately treat medically compromised patients
3.8 54 ------ ------ ------ ------
Equipment failure 4.5-7.95 54, 66, 71 30 PSIs18.73 NMs
59, 67 ------ ------
Multiple exposure to x-rays 3.7 54, 66, 71 5.63-89 PSIs1-5 NMs
59, 67 ------ ------
Sedation errors ------ ------ <1-33 PSIs1.2-6 NMs
35, 45, 59, 67 ------ ------
Infection control ------ ------ <1 PSIs5.82 NMs
67 ------ ------
Post
-ope
rativ
e
Drug prescription errors 1.68-2.9 50, 71 3.5-32 PSIs5-19 NMs
35, 59 ------ ------
Lack of follow-up 1.63 44 4.8 35 ------ -----
Abbreviations: PSIs= patient safety incidents; NMs= near misses
Types and frequencies of AEsA distinction is apparent between local AE outcomes which concerned the oral cavity and surrounding areas, and systemic AE outcomes which involved the systemic effects of local anaesthesia (LA), general anaesthesia (GA) and
13
174
175
176
177
178
179180181182

sedation. 41, 43, 45, 63 This finding was considered to group the identified AE outcomes shown in Table 6.
Then, the variety of PSIs and their frequencies were grouped and presented across the main three identified measurement methods (Table 6). Based on this, our results show that malpractice studies again contributed the most to the identification of AEs. However, the outcomes concern mostly to local AEs with little attention to systemic AEs. The latter were generally identified by surveys and record reviews. Within local AE outcomes, nerve damage emerged after LA administration or after surgical procedures.36, 53, 73 For systemic AEs, cardiovascular events included angina pectoris, myocardial infarction, and stroke41, 45, 64 Death was reported as a consequence of flaws in LA administration, sedation and GA. 36, 38, 48, 60, 63, 71
14
183184
185186187188189190191192193194
195

Table 6. Variability of frequencies of adverse event outcomes across three main measurement methods
Adverse event outcomes
Malpractice analysis (n= 17) Surveys (n= 10) Record review (n= 8)
Ranges (%) References Ranges
(%) References Ranges (%) References
Loca
l adv
erse
out
com
es
Injuries 1-1940, 44, 48, 54, 60,
66, 71
<1–14.1 AEs
2.02 NMs45, 59, 67 14.46 65
Accidental injection of sodium hypochlorite ----- ----- 2.03 52 ----- -----
Tooth damage ----- ----- 10.62 AEs2.5 NMs
67 ----- -----
Alveolar bone loss 1.63 44, 71 ----- ----- ----- -----
Nerve damage <1-5936, 40, 44, 53, 54,
60, 66, 71 <1 70 75.1 62
Wrong tooth 3.1-5.7 54, 66 7-31 AEs1-8 NMs
59 ---- ----
Wrong treatment 5.7-15.6 50, 54, 66 1.08 AEs1.5 NMs
67 ----- -----
Wrong patient ----- ----- <1 AEs6.07 NMs
67 ----- -----
Wrong body part 3.1-5.7 4.5 AEs3.5 NMs
67 ----- -----
Tooth loss 8.8-29.4 50, 54, 60, 66, 71 ----- ----- ----- -----
Tooth fracture 1.58-8.8 40, 50, 60 52 61, 67 ----- -----Infection after treatment <1-16.8
40, 44, 48, 50, 54, 55, 60, 71
58 AEs1 NMs
45, 59, 67 ----- -----
Peri implantitis ----- ----- ----- ----- 2.40 65
Treatment failure 29.7-37 57, 66 ----- ----- ----- -----Temporomandibular joint complication 3.1-14.4 54, 60, 66, 71 ----- ----- ----- -----
Prolonged pain 2-13.3 42, 50, 54, 66 ----- ----- ----- -----Prolonged or additional treatment 3.3-30 50, 54 ----- ----- ----- -----
Syst
emic
adve
rse
outc
omes
Adverse reactions to local anesthesia <1-4.5 54, 66, 71 <1 41 <1 64
Allergic reactions <1 71 <1 39, 41, 67 ----- -----
Cardiovascular events ----- ----- <1 41, 45 <1 64
Diabetic events ----- ----- <1 39, 41 ----- -----Vasovagal collapse /syncope ----- ----- <1-3.3 39, 45, 67 <1-3.3 64, 73
Dizziness, Headache, Nausea or vomiting ----- ----- ----- ----- <1 43, 64
Fits/Seisures ----- ----- <1 41, 45 ----- -----Asthma or apnea events ----- ----- <1-5.5 39, 41 <1 43
Desaturation ----- ----- ----- ----- <1 43
Prolonged sedation ----- ----- ----- ----- 1.53 43
Brain damage 53 63 ----- ----- ----- -----
Death <1-53 36, 48, 60, 63, 71 <1 38 ----- -----Abbreviations: AEs= adverse events; NMs= near misses
15
196
197

DiscussionPS research has been largely unexplored in dentistry,14, 15, 25 and the epidemiology of PSIs, 15 AEs and PS concepts in this field are poorly understood. 15, 25, 26, 74 This work is, to our knowledge, the first systematic approach to scope the type and frequency of PSI and AEs in ambulatory dentistry. We found that PS research is still immature as most of the current work is descriptive. It is also difficult to generalize from such studies due to differences in underlying definitions, varying methodological approaches, and differing patient populations. The majority of existing work also comes from a limited number of high-income countries. However, this study also demonstrates a growing interest in PS research in ambulatory dental care contexts, and provides an insight into existing approaches that have begun seeking to understand the reasons underpinning PSIs.
Types of PSIsThe main five PSIs we identified were errors in diagnosis and examination, treatment planning, communication, procedural errors and the accidental ingestion or inhalation of foreign objects. The main source for these were malpractice cases and surveys which represented almost 50% of the articles. On the other hand, record review was the method that less contribution had to characterize PSIs. This highlights the lack of case note review methods to describe the epidemiology of harm in ambulatory dentistry.
Due to the scarcity of research in dentistry, our results cannot be compared within the same discipline. However, our findings were similar to the findings reported by Rees et al. after analyzing PSI-reports in primary care. 75 However, PSIs and AEs are not limited to individual performance. 76 The framework developed by Vincent et al. (1998) for analysing risk and safety in clinical medicine, 77 and the model of organisational safety developed by Reason, 21
differentiate errors made by people (active errors) from errors within the organisational structure of healthcare delivery (latent errors). These have been further integrated into other frameworks such as the Yorkshire Contributory Factors Framework of PSIs in hospital settings. 78 Our results show research gaps in organisational factors such as flaws within the physical environment, scheduling and patient management, lines of responsibility, and the influence of policies.
Our findings also extend those from Bailey et al. 25 confirming that no agreed standardised terminology has been used for the past 20 years. As Ioannidis pointed out: “The greater the flexibility in designs, definitions, outcomes and analytical modes in a scientific field, the less likely the research findings are to be true.” 79 Therefore, evidence from large-scale epidemiological studies with robust methods should now be considered for generating more reliable findings. 80
16
198199200201202203204205206207208209210
211212213214215216217218
219220221222223224225226227228229230231
232233234235236237238
239
240

Types of AEsOur findings also suggest that the main concern for reporting PSIs and AEs is the severity of harm. 36, 40, 42, 44, 48, 50, 53, 54, 60, 63, 66, 71 As harm itself might need to be severe enough to raise sufficient concern for patients to seek legal and financial compensation.74, 81 Similarly, we identified other AEs such as nerve damage, 36, 40, 44,
53, 54, 60, 62, 66, 70, 71 post-treatment infection, 40, 44, 45, 48, 50, 54, 55, 59, 60, 67, 71 prolonged pain42, 50, 54, 66 and temporomandibular complications54, 60, 66, 71 that are non-immediate AEs, and which can take weeks or months to be detected following treatment. These represent a challenge to be identified and associated with error.
On the other hand, reported AEs may constitute the tip of the iceberg as near-misses and less severe AEs can remain highly unreported.80 In this regard, our findings demonstrate that little is known in relation to PSIs leading to less severe harm or no harm. We only identified two surveys that reported near misses. 59, 67
However, these studies also reported participation rates of 54% and 75%. Nevertheless, these events also represent a valuable source of information and learning, which can be obtained from incident reporting systems.75, 82 These data can then be used for understanding the nature of error and what typically happens in order to cause harm to patients.
Thusu et al.24 identified injuries, medical emergencies, inhalation and ingestion of foreign objects, adverse reactions and wrong tooth extractions as the main areas of concern in ambulatory dental practices within the National Health Service in England and Wales. In addition, the Council of European Dentists has recommended the introduction of Patient Safety Incident Reporting Systems for “…voluntarily and anonymously reporting adverse events, near misses and problems with medical devices, to enable all dentists to learn from their own and others’ experiences.”23 Therefore, developing such reporting systems for dentistry is a necessary next step.
Our results also show a distinction between local and systemic AEs. This finding compares well with a similar distinction made by Obadan et al. (2015), after analyzing dental adverse case reports (published after the period covered in our study).83 We believe this distinction should be considered for reporting further primary research and for the development or adaptation of taxonomies for PSIs and AEs in ambulatory dental care. As it reinforces the need for the development and use of standardized working definitions and classification systems for PSIs and AEs. We believe that agreed standardized definitions and terms will enable further comparisons between studies as new evidence is reported. A common PS taxonomy, such as the WHO’s International Classification for Patient Safety,20 will support such comparisons to be made.
17
241
242
243
244
245246247248249250251252253
254255256257258259260261262
263264265266267268269270271
272273274275276277278279280281282

Potential contributory factorsCompliance with patient-safety-focused protocols, simplification of tasks and procedures, adequate PS training, fatigue management and the availability of adequate informational resources are other potentially transferable strategies obtained from human factors research in medicine.84
Implications for policy and practiceAdministrators, dental associations and policymakers should begin deliberating how to reduce risk in dentistry.85 For this, a formal national PS agenda is needed that takes into account how dentistry is organized and financed within countries. Standardized concepts of PSI, AE and particularly NEs need to be implemented across the profession, and ensuring appropriate clinical governance to monitor and learn from NEs, can help to promote commitment to PS. Policies like the Framework for the Identification and Management of Never Events22, 86 from the NHS should be developed and introduced in dentistry.
Also, advocates for observatories by specialty are needed87 and dentistry is no exception. In response to the WHO Safer Primary Care report, 27 unsafe dental care needs recognition and all efforts should work under a similar agenda to primary care, identify priority areas and key knowledge gaps, and develop interventions for reducing preventable harm. 88, 89 We believe our findings can inform these deliberations as it has identified the main threats to PS, 85, 90 and the existing reported nature and scale of harm. These can now be used to set priorities for action. 91
Dentistry has been a challenge for measuring the quality of care as many treatments do not follow clear established evidence-based guidelines. 92 These should be developed for further implementation and evaluation. Moreover, a national regulatory body for PS practices is needed supported by the law and agreed standards of performance. 93
Data from IRSs needs to be part of this continuous quality improvement agenda94 and these now need to be developed for dentistry. 23, 95 An ongoing study for the characterization and development of classification systems of PSIs through the efficient interrogation of unstructured text96 shows how data from IRSs can be used in dentistry. However, a likely difficulty exists around how to most effectively foster an environment receptive to change.91 Facilitators for a PS culture include the recognition of the risks of oral healthcare delivery through all health sectors and dental associations, as well as the integration of PS into the curricula of dental schools and within the organizational structure of dentistry. 85
The multi-professional guide for PS developed by the WHO, 97 and online courses such as those provided by the Institute for Healthcare Improvement Open School, 98-100 are valuable resources to help dental schools to integrate PS education into the professional curricula in dentistry. This should be developed and integrated within a national PS strategy that will need to also consider the policy-making process in order to find the best way to work within the health sector to improve PS at a local and national level. 91
18
283284285286287
288289290291292293294295296
297298299300301302303304
305306307308309
310311312313314315316317318
319320321322323324325

Strengths and limitationsThis study has provided a comprehensive overview of an under-explored field through systematic methods following published guidelines.28, 29 Due to the lack of standardized terminology, the search strategy comprised broad terms to retrieve as many potential articles as possible. Quality assessment is not a component of scoping reviews and this step was therefore not undertaken.34 We anticipated to retrieve a wide variety of studies as the scoping review method allowed us to cover broad area of the literature.34 However, the heterogeneity of evidence also posed challenges for the interpretation of data. In order to address this, the emerging AEs and PSIs were grouped into the major concepts shown in Figure 2. Individually, the gathered data from each article was generated for specific and narrow objectives, which represented a challenge for data extraction and to conceptually map and organize the PSIs and AEs. These were also synthesised101 and integrated in Tables 5 and 6. Moreover, we did not identify enough evidence to either justify a systematic review, metanalysis or to provide pooled estimates. A subsequent systematic review would require to report estimates of prevalence of high quality observational studies. The Checklists developed by the Critical Appraisal Skill Programme (http://www.casp-uk.net/) can be used to support the quality assessment of the articles.
Recommendations for further researchFuture research must embrace robust primary research designs and methods with agreed working definitions20 and theoretical frameworks already developed in medicine. 21, 77 Subsequent research should also focus on the characterization of PSIs and AEs through the analysis of data already available from incident reporting systems or other surveillance systems.
The results from this should be taken into consideration for the development of a classification system to maximize learning from reports describing PSIs and AEs.87, 96, 102 In addition, existing reporting systems such as the National Reporting Learning System contain free-narrative descriptions24 and natural language processing offers a set of informatics tools capable of transforming text into a structured format that can be used to extract data.103 Also, a set of never events is for ambulatory dentistry is needed.14 We recommend that this list should be validated through formal consensus developing techniques. Further work also needs to be done to agree which of these areas should be focused on for future descriptive, in-depth and interventional research.
ConclusionsThis systematic scoping review demonstrates that the accumulated knowledge for the past 20 years on PSIs and AEs is immature. As our findings suggest, there is a pressing need for high quality primary research studies to help further develop the still relatively nascent field of PS research in dentistry. Our result also provide an evidence-based baseline to characterize PSIs and AEs and identify key areas for further descriptive, in-depth, consensus-building and experimental research in order to move the field on. We expect our findings to raise awareness on patient safety in dentistry and encourage researchers from
19
326327328329330331332333334335336337338339340341342343344
345346347348349350
351352353354355356357358359360
361362363364365366367368369

different disciplines to engage further research opportunities than can be translated into effective evidence-based interventions.
20
370371
372

References
1. Jha A. Summary of the evidence on patient safety: implications for research Spain: World Health Organiszation; 2008. Available from: http://www.who.int/patientsafety/information_centre/20080523_Summary_of_the_evidence_on_patient_safety.pdf.2. Jha AK, Prasopa-Plaizier N, Larizgoitia I, Bates DW. Patient safety research: an overview of the global evidence. Qual Saf Health Care. 2010;19(1):42-7.3. de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17(3):216-23.4. Organization WH. IBEAS: a pioneer study on patient safety in Latin America. Towards safer hospital care. Geneva, Switzerland: World Health Organization, 2011.5. Bartlett G, Blais R, Tamblyn R, Clermont RJ, MacGibbon B. Impact of patient communication problems on the risk of preventable adverse events in acute care settings. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2008;178(12):1555-62.6. Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324(6):370-6.7. Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human:: Building a Safer Health System: National Academies Press; 2000.8. Organization WH. Global Priorities for Patient Safety Research Better knowledge for safer care. 2008 December 2008. Report No.9. Organisation WH. World Health Assembly Resolution WHA 55.18 2012. Available from: http://www.who.int/patientsafety/about/wha_resolution/en/index.html.10. Sheikh A, Panesar SS, Larizgoitia I, Bates DW, Donaldson LJ. Safer primary care for all: a global imperative. The lancet global health. 2013;1(4):e182-e3.11. Sheikh A, BatesMD DW. Iatrogenic harm in primary care. Harvard Health Policy Review. 2014;4(1):4-8.12. Carson-Stevens A, Hibbert P, Avery A, Butlin A, Carter B, Cooper A, et al. A cross-sectional mixed methods study protocol to generate learning from patient safety incidents reported from general practice. BMJ open. 2015;5(12):e009079.13. Panesar SS, Carson-Stevens A, Cresswell KM, Salvilla SA, Slight SP, Javad S, et al. How safe is primary care? A systematic review. BMJ quality & safety. 2015:bmjqs-2015-004178.14. Ramoni RB, Walji MF, White J, Stewart D, Vaderhobli R, Simmons D, et al. From good to better: toward a patient safety initiative in dentistry. Journal of the American Dental Association (1939). 2012;143(9):956-60.15. Bailey E, Tickle M, Campbell S. Patient safety in primary care dentistry: where are we now? Br Dent J. 2014;217(7):339-44.16. Webster JS, King HB, Toomey LM, Salisbury ML, Powell SM, Craft B, et al. Understanding quality and safety problems in the ambulatory environment: seeking improvement with promising teamwork tools and strategies. 2008.17. Oncel M, Apiliogullari B, Cobankara FK, Apiliogullari S. Accidental swallowing of the head of a dental mirror: Report of a rare case. Journal of Dental Sciences. 2012;7(2):199-202.18. da Costa Monini A, Maia LGM, Jacob HB, Gandini LG. Accidental swallowing of orthodontic expansion appliance key. American Journal of Orthodontics and Dentofacial Orthopedics. 2011;140(2):266-8.19. Obinata K, Satoh T, Towfik AM, Nakamura M. An investigation of accidental ingestion during dental procedures. J Oral Sci. 2011;53(4):495-500.
21
373374
375376377378379380381382383384385386387388389390391392393394395396397398399400401402403404405406407408409410411412413414415416417418419420421

20. World Alliance For Patient Safety Drafting G, Sherman H, Castro G, Fletcher M, World Alliance for Patient S, Hatlie M, et al. Towards an International Classification for Patient Safety: the conceptual framework. International journal for quality in health care : journal of the International Society for Quality in Health Care / ISQua. 2009;21(1):2-8.21. Reason J. Human error : models and management. 2000;320(March):4-6.22. Department of Health N. Revised Never Events Policy and Framework Lodon: National Health Service, 2015 March. Report No.23. Dentists CoE. Resolution on Patient Safety. Council of European Dentists, 2008.24. Thusu S, Panesar S, Bedi R. Patient safety in dentistry - state of play as revealed by a national database of errors. Br Dent J. 2012;213(3):E3.25. Bailey E, Tickle M, Campbell S, O’Malley L. Systematic review of patient safety interventions in dentistry. BMC oral health. 2015;15(1):1.26. Yamalik N, Dijk W. Analysis of the attitudes and needs/demands of dental practitioners in the field of patient safety and risk management. Int Dent J. 2013;63(6):291-7.27. Group TSPCEW. Safer Primary Care: A Global Challenge. Switzerland: World Health Organization, 2012.28. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. International journal of social research methodology. 2005;8(1):19-32.29. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):1-9.30. Leape LL. Error in medicine. Jama. 1994;272(23):1851-7.31. Webster J, Watson RT. Analyzing the past to prepare for the future: Writing a literature review. Management Information Systems Quarterly. 2002;26(2):3.32. Panesar S, Carson-Stevens A, Cresswell KM. Global burden of unsafe primary care: a systematic review and meta-analysis. BMJ Quality & Safety. 2016.33. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine. 2009;151(4):264-9.34. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Information & Libraries Journal. 2009;26(2):91-108.35. Milgrom P, Fiset L, Whitney C, Conrad D, Cullen T, O'Hara D. Malpractice claims during 1988-1992: a national survey of dentists. Journal of the American Dental Association (1939). 1994;125(4):462-9.36. Haas DA, Lennon D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. Journal (Canadian Dental Association). 1995;61(4):319-20, 23-6, 29-30.37. Lupi JE, Handelman CS, Sadowsky C. Prevalence and severity of apical root resorption and alveolar bone loss in orthodontically treated adults. Am J Orthod Dentofacial Orthop. 1996;109(1):28-37.38. Nkansah PJ, Haas DA, Saso MA. Mortality incidence in outpatient anesthesia for dentistry in Ontario. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics. 1997;83(6):646-51.39. Keur I, Smeets EC, de Jong KJ, Abraham-Inpijn L. [Medical accidents in the dental practice. Survey of 471 dentists in the Netherlands]. Ned Tijdschr Tandheelkd. 1998;105(5):162-5.40. Venta I, Lindqvist C, Ylipaavalniemi P. Malpractice claims for permanent nerve injuries related to third molar removals. Acta odontologica Scandinavica. 1998;56(4):193-6.41. Atherton GJ, McCaul JA, Williams SA. Medical emergencies: Medical emergencies in general dental practice in Great Britain Part 1: their prevalence over a 10-year period. Br Dent J. 1999;186(2):72-9.42. Al Ammar W, Guile EE. A one-year survey of dental malpractice claims in Riyadh. Saudi Dental Journal. 2000;12(2):95-9.
22
422423424425426427428429430431432433434435436437438439440441442443444445446447448449450451452453454455456457458459460461462463464465466467468469470

43. Leelataweedwud P, Vann WF, Jr. Adverse events and outcomes of conscious sedation for pediatric patients: study of an oral sedation regimen. Journal of the American Dental Association. 2001;132(11):1531-9; quiz 96.44. Givol N, Taicher S, Halamish-Shani T, Chaushu G. Risk management aspects of implant dentistry. The International journal of oral & maxillofacial implants. 2002;17(2):258-62.45. D'Eramo E M, Bookless SJ, Howard JB. Adverse events with outpatient anesthesia in Massachusetts. J Oral Maxillofac Surg. 2003;61(7):793-800; discussion 46. Frangiskos F, Stavrou E, Merenditis N, Tsitsogianis H, Vardas E, Antonopoulou I. Incidence of penetration of a blood vessel during inferior alveolar nerve block. Br J Oral Maxillofac Surg. 2003;41(3):188-9.47. Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: a 10-year institutional review. Journal of the American Dental Association. 2004;135(9):1287-91.48. Ozdemir MH, Saracoglu A, Ozdemir AU, Ergonen AT. Dental malpractice cases in Turkey during 1991-2000. J. 2005;12(3):137-42.49. Susini G, Pommel L, Camps J. Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. International Endodontic Journal. 2007;40(8):585-9.50. Bjorndal L, Reit C. Endodontic malpractice claims in Denmark 1995-2004. International Endodontic Journal. 2008;41(12):1059-65.51. Tzanetakis GN, Kontakiotis EG, Maurikou DV, Marzelou MP. Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: a five-year retrospective clinical study. Journal of endodontics. 2008;34(6):675-8.52. Kleier DJ, Averbach RE, Mehdipour O. The Sodium Hypochlorite Accident: Experience of Diplomates of the American Board of Endodontics. Journal of Endodontics. 2008;34(11):1346-50.53. Gaffen AS, Haas DA. Retrospective review of voluntary reports of nonsurgical paresthesia in dentistry. J Can Dent Assoc. 2009;75(8):579.54. Kiani M, Sheikhazadi A. A five-year survey for dental malpractice claims in Tehran, Iran. J Forensic Leg Med. 2009;16(2):76-82.55. Lee JJ, Hahn LJ, Kao TP, Liu CH, Cheng SJ, Cheng SL, et al. Post-tooth extraction sepsis without locoregional infection--a population-based study in Taiwan. Oral diseases. 2009;15(8):602-7.56. Peleg O, Givot N, Halamish-Shani T, Taicher S. Wrong tooth extraction: root cause analysis. Quintessence Int. 2010;41(10):869-72.57. Givol N, Rosen E, Taicher S, Tsesis I. Risk management in endodontics. Journal of Endodontics. 2010;36(6):982-4.58. Hisanaga R, Hagita K, Nojima K, Katakura A, Morinaga K, Ichinohe T, et al. Survey of accidental ingestion and aspiration at Tokyo Dental College Chiba Hospital. The Bulletin of Tokyo Dental College. 2010;51(2):95-101.59. Ashkenazi M, Bijaoui E, Blumer S, Gordon M. Common mistakes, negligence and legal offences in paediatric dentistry: a self-report. Eur Arch Paediatr Dent. 2011;12(4):188-94.60. Perea-Perez B, Santiago-Saez A, Labajo-Gonzalez ME, Albarran-Juan ME. Professional liability in oral surgery: legal and medical study of 63 court sentences. Med Oral Patol Oral Cir Bucal. 2011;16(4):e526-31.61. Soehardi A, Meijer GJ, Manders R, Stoelnga PJ. An inventory of mandibular fractures associated with implants in atrophic edentulous mandibles: a survey of Dutch oral and maxillofacial surgeons. Int J Oral Maxillofac Implants. 2011;26(5):1087-93.62. Hillerup S, Jensen RH, Ersboll BK. Trigeminal nerve injury associated with injection of local anesthetics: needle lesion or neurotoxicity? Journal of the American Dental Association. 2011;142(5):531-9.63. Chicka MC, Dembo JB, Mathu-Muju KR, Nash DA, Bush HM. Adverse events during pediatric dental anesthesia and sedation: a review of closed malpractice insurance claims. Pediatric dentistry. 2012;34(3):231-8.
23
471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502503504505506507508509510511512513514515516517518519520521

64. Schwamburger NT, Hancock RH, Chong CH, Hartup GR, Vandewalle KS. The rate of adverse events during IV conscious sedation. Gen Dent. 2012;60(5):e341-4.65. Abi Najm S, Malis D, El Hage M, Rahban S, Carrel JP, Bernard JP. Potential adverse events of endosseous dental implants penetrating the maxillary sinus: long-term clinical evaluation. Laryngoscope. 2013;123(12):2958-61.66. Hashemipour MA, Movahedi Pour F, Lotfi S, Gandjalikhan Nassab AH, Rahro M, Memaran Dadgar M. Evaluation of dental malpractice cases in Kerman province (2000-2011). J Forensic Leg Med. 2013;20(7):933-8.67. Hiivala N, Mussalo-Rauhamaa H, Murtomaa H. Patient safety incidents reported by Finnish dentists; results from an internet-based survey. Acta odontologica Scandinavica. 2013;71(6):1370-7.68. Kalenderian E, Walji MF, Tavares A, Ramoni RB. An adverse event trigger tool in dentistry: A new methodology for measuring harm in the dental office. Journal of the American Dental Association. 2013;144(7):808-14.69. Pinchi V, Pradella F, Gasparetto L, Norelli GA. Trends in endodontic claims in Italy. Int Dent J. 2013;63(1):43-8.70. Renton T, Janjua H, Gallagher JE, Dalgleish M, Yilmaz Z. UK dentists' experience of iatrogenic trigeminal nerve injuries in relation to routine dental procedures: why, when and how often? Br Dent J. 2013;214(12):633-42.71. Perea-Perez B, Labajo-Gonzalez E, Santiago-Saez A, Albarran-Juan E, Villa-Vigil A. Analysis of 415 adverse events in dental practice in Spain from 2000 to 2010. Medicina oral, patologia oral y cirugia bucal. 2014;19(5):e500-5.72. Peleg O, Givot DMDN, Halamish-shani T, Taicher S. Wrong tooth extraction: root cause analysis. Br Dent J. 2011;210(4):163-.73. Hillerup S. Iatrogenic injury to oral branches of the trigeminal nerve: records of 449 cases. Clin Oral Investig. 2007;11(2):133-42.74. Yamalik N, Perea Pérez B. Patient safety and dentistry: what do we need to know? Fundamentals of patient safety, the safety culture and implementation of patient safety measures in dental practice. Int Dent J. 2012;62(4):189-96.75. Rees P, Edwards A, Panesar S, Powell C, Carter B, Williams H, et al. Safety Incidents in the Primary Care Office Setting. Pediatrics. 2015:peds. 2014-3259.76. Ovretveit J. Understanding and improving patient safety: the psychological, social and cultural dimensions. Journal of health organization and management. 2009;23(6):581-96.77. Vincent C, Taylor-Adams S, Stanhope N. Framework for analysing risk and safety in clinical medicine. Bmj. 1998;316(7138):1154-7.78. Lawton R, McEachan RR, Giles SJ, Sirriyeh R, Watt IS, Wright J. Development of an evidence-based framework of factors contributing to patient safety incidents in hospital settings: a systematic review. BMJ quality & safety. 2012:bmjqs-2011-000443.79. Ioannidis JP. Why most published research findings are false. Chance. 2005;18(4):40-7.80. Boxwala AA, Dierks M, Keenan M, Jackson S, Hanscom R, Bates DW, et al. Organization and representation of patient safety data: Current status and issues around generalizability and scalability. Journal of the American Medical Informatics Association. 2004;11(6):468-78.81. Sohn DH. Negligence, genuine error, and litigation. Int J Gen Med. 2013;6:49-56.82. Panesar SS, Cleary K, Sheikh A. Reflections on the National Patient Safety Agency's database of medical errors. Journal of the Royal Society of Medicine. 2009;102(7):256-8.83. Obadan EM, Ramoni RB, Kalenderian E. Lessons learned from dental patient safety case reports. Journal of the American Dental Association (1939). 2015;146(5):318-26.e2.84. Porto GG. Safety by design: ten lessons from human factors research. Journal of healthcare risk management : the journal of the American Society for Healthcare Risk Management. 2001;21(4):43-50.85. Pemberton MN. Developing patient safety in dentistry. Br Dent J. 2014;217(7):335-7.
24
522523524525526527528529530531532533534535536537538539540541542543544545546547548549550551552553554555556557558559560561562563564565566567568569570571

86. Department of Health N. The never events policy framework: An update to the never events policy Report. London: National Health Service, 2012.87. Carson-Stevens A, Edwards A, Panesar S, Parry G, Rees P, Sheikh A, et al. Reducing the burden of iatrogenic harm in children. Lancet. 2015;385(9978):1593-4.88. Williams H, Edwards A, Hibbert P, Rees P, Evans HP, Panesar S, et al. Harms from discharge to primary care: mixed methods analysis of incident reports. The British journal of general practice : the journal of the Royal College of General Practitioners. 2015;65(641):e829-e37.89. Rees P, Edwards A, Powell C, Evans HP, Carter B, Hibbert P, et al. Pediatric immunization-related safety incidents in primary care: A mixed methods analysis of a national database. Vaccine. 2015;33(32):3873-80.90. Pronovost PJ, Cardo DM, Goeschel CA, Berenholtz SM, Saint S, Jernigan JA. A research framework for reducing preventable patient harm. Clin Infect Dis. 2011;52(4):507-13.91. Lewis RQ, Fletcher M. Implementing a national strategy for patient safety: lessons from the National Health Service in England. Qual Saf Health Care. 2005;14(2):135-9.92. Bader JD. Challenges in quality assessment of dental care. The Journal of the American Dental Association. 2009;140(12):1456.93. Pronovost PJR, Stoll RA, Kennedy, S.B. Transforming Patient Safety: A Sector-Wide Systems Approach. World Innovation Summit for Health (WISH), 2015.
94. Brown C, Hofer T, Johal A, Thomson R, Nicholl J, Franklin BD, et al. An epistemology of patient safety research: a framework for study design and interpretation. Part 3. End points and measurement. Qual Saf Health Care. 2008;17(3):170-7.95. Williams SK, Osborn SS. The development of the National Reporting and Learning System in England and Wales, 2001-2005. The Medical journal of Australia. 2006;184(10 Suppl):S65-8.96. group TPc. Characterising the nature of primary care patient safety incident reports in England and Wales: mixed methods study. (PISA study) 2015. Available from: http://medicine.cf.ac.uk/primary-care-public-health/research/healthcare-communication/current-projects/pisa/.97. Organization WH. WHO patient safety curriculum guide: multi-professional edition.: WHO Press; 2011.98. Patel E, Nutt SL, Qureshi I, Lister S, Panesar SS, Carson-Stevens A. Leading change in health-care quality with the Institute for Healthcare Improvement Open School. British Journal of Hospital Medicine (17508460). 2012;73(7).99. Jones A, Williams A, Carson-Stevens A. Integrating quality improvement into pre-registration education. Nursing Standard. 2013;27(29):44-8.100. Ward HO, Jones A, Carson-Stevens A. IHI Open School’s quality improvement initiative. Bmj. 2013;346:f1371.101. Gough D, Oliver S, Thomas J. An introduction to systematic reviews: Sage; 2012.102. Rees P, Carson-Stevens A, Williams H, Panesar S, Edwards A. Quality improvement informed by a reporting and learning system. Archives of disease in childhood. 2014;99(7):702-3.103. Bates DW, Evans RS, Murff H, Stetson PD, Pizziferri L, Hripcsak G. Detecting adverse events using information technology. Journal of the American Medical Informatics Association : JAMIA. 2003;10(2):115-28.
25
572573574575576577578579580581582583584585586587588589
590591592593594595596597598599600601602603604605606607608609610611612613

Appendix 1. Search strategy
1. exp Dentistry/
2. dentistry.mp.
3. exp Diagnostic errors/
4. exp Medical errors/
5. exp Medication errors/
6. exp Delayed diagnosis/
7. delayed diagnosis.mp.
8. misdiagnosis.mp.
9. treatment delay*.mp.
10. exp Unnecessary Procedures/
11. exp Patient Safety/
12. exp Risk Management/
13. adverse event*.mp.
14. exp Patient Harm/
15. patient harm.mp.
16. exp Malpractice/
17. exp Accidents/
18. exp Iatrogenic Disease/
19. exp Needles/ae [Adverse effects]
20. exp Surgery, Oral/
21. dental complication*.mp.
22. systematic review*.mp.
23. "Review Literature as Topic"/
24. exp Research Design/
25. exp Research Report/
26. exp Clinical Trials as Topic/ or exp Adult/ or exp Epidemiologic Methods/ or exp Research Design/ or study design.mp.
27. exp Cross-Sectional Studies/
28. exp Intervention Studies/
29. exp Comparative study/
30. exp Follow-up Studies/
31. exp Prospective Studies/
32. exp Observational Study/
26
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640641
642
643
644
645
646
647

33. exp Cohort Studies/
34. exp Congresses as Topic/ or meeting abstract*.mp.
35. exp Meta-Analysis/
36. qualitative stud*.mp.
37. Ethnographic Research/
38. Phenomenological Research/
39. Models, Theoretical/ or Grounded Theory.mp.
40. focus group*.mp. or Focus Groups/
41. Interview/ or interview*.mp.
42. 1 or 2
43. 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21
44. 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41
45. 42 and 43 and 44
46. limit 45 to (human and medline and yr="1994 -Current")
27
648
649
650
651
652
653
654
655
656
657
658659
660661
662
663

28
664
665





























