Embed Size (px)
Citation preview

Chapter 8Vascular access
Jocelyn M. De Guzman, Bryan B. Kitch, and Jeffrey D. Ferguson
IntroductionWhile discussions continue concerning the utility of obtaining prehospital vascular access, the skill remains a standard taught to EMS providers. Methods of access include peripheral and central intravenous (IV) catheterization and intraosseous (IO) access, depending on the local scope of practice and the qualifications of prehospital personnel. The medications and fluids administered through these various routes depend on local EMS protocol and the practices of the EMS medical director. Those specifics are beyond the scope of this chapter, but are discussed elsewhere in this text.
BenefitsSimilar to its benefit in the emergency department (ED) or any other acute care setting, vascular access provides an avenue for medical intervention by the EMS provider. Early prehospital initiation of treatment for cardiac arrest, cardiac arrhythmia, and sepsis has been shown to be beneficial for patients [1–3]. For the more stable yet ill or distressed patient, the initiation of an IV or IO for symptomatic treatment of nausea, pain, or dehydration can help the continuum of care that will likely progress in the ED. Treatment of potentially reversible conditions like hypoglycemia and narcotic overdose in the prehospital setting can prevent deterioration of the patient’s condition and potentially negate the need for transport. Vascular access also facilitates advanced care such as rapid sequence intubation and the administration of vasopressors and thrombolytics.
RisksObtaining vascular access involves inherent risks to the provider, including blood exposure and needlestick injury. Whether it is attempted at the scene or in transit, the prehospital environment is often characterized by poor lighting, limited space, or movement in the rear of an ambulance. This offers less than ideal conditions in which to handle lancets, IV and IO needles, and other sharps. A combative and/or confused patient can add to the difficulty. Transmission of HIV, hepatitis B, and hepatitis C remains a constant threat to the EMS provider, with the risks of infection following needlestick injury estimated at 0.3%, 6–30%, and 1.8%, respectively [4]. Consistent use of universal precautions is imperative to reduce the likelihood of occupational exposures. Potential risks to the patient include bleeding, damage to adjacent structures, infection, and thrombosis and will be discussed later.
Establishing an IV is often part of EMS protocols. In many cases, protocols allow for EMS provider assessment and judgment regarding whether or not an IV is necessary. One study revealed that while over 50% of the patients who arrived at an ED via EMS had IVs in place, almost 80% of those IVs were not used in the prehospital setting. The tendency to err on the side of caution to avoid punitive measures from perceived undertreatment seemed to contribute to the discrepancy [5]. Another study similarly found that protocols seemed to drive the decision to start an IV as opposed to an actual need for administration of medicines or fluids [6]. Medical

oversight is indicated to continually evaluate the appropriateness of “precautionary” IVs in the contexts of potential risks and costs to the system and to patients.
Several studies in the trauma setting have unveiled a lack of significant benefit regarding prehospital vascular access. The classic EMS mantra of “two large-bore IVs” for trauma patients has been muted by concern for increased on-scene times and delay of transport to definitive medical care. Nevertheless, two studies have shown high success rates when IVs were attempted in transit without delaying transport [7,8]. However, a literature review by the Eastern Association for the Surgery of Trauma resulted in a set of practice management guidelines that found no demonstrable benefit from prehospital IV placement or IV fluid administration for either penetrating or blunt injury patients [9]. Recent research in the field of trauma resuscitation suggests that routine administration of IV fluids may have no benefit and in fact can be harmful in the prehospital setting [10,11]. Another study endorsed “scoop and run” transport for EMS as it found that each prehospital procedure before ED thoracotomy led to a reduction in the odds of survival [12].
Peripheral IV accessHistoryEarly records document the use of feather quills and animal bladders for intravenous therapies with animal-to-human transfusions. These were later replaced by hollow steel needles with rubber tubing leading to glass bottles. The evolution to over-the-needle plastic catheters has been focused on operator safety and patient comfort [13].
Flow rate through the catheter is based on Poiseuille’s law, dealing with pressure and resistance. The pertinent determinants of the equation include the radius of the catheter and the catheter length. Flow is directly proportional to the radius to the 4th power (r 4), and inversely proportional to catheter length. As such, a large-gauge, short IV catheter can profoundly improve the potential flow rate over a smaller gauge, longer catheter.
Typical locations for peripheral IV access include the antecubital fossa, veins in the forearm and dorsum of the hand and foot, external jugular vein, and scalp veins.
Technique (Video Clip 8.1)1. PreparationWhen the decision to pursue vascular access is made, the preparation for the procedure is just as imperative as the skill itself. Temptations for speed in the prehospital setting, assumptions regarding the patient’s health, or other neglectful behavior deviating from the practice of universal precautions can result in occupational exposure. When possible, wash hands prior to putting on gloves.
Prepare the equipment (Figure 8.1). You will need an IV start kit (if available) or you can assemble your own (tourniquet, alcohol wipe or other cleaner, tape or a commercially available adhesive device). Select an IV needle with catheter (Figure 8.2), saline lock, saline flush, and/or IV fluids. Check the IV

Figure 8.1 IV starting equipment.

Figure 8.2 18 and 20 gauge IV catheters with needles.
Prepare the patient for the procedure. When appropriate, discuss with the patient the reason for the procedure along with risks and benefits. Unless a true emergency exists or the patient is not able to make his/her own decisions, verbal consent should be obtained.
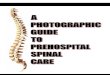
2. Site selectionPosition the patient’s extremity to help straighten the desired vein. Apply the tourniquet proximal to the targeted area (Figure 8.3). When possible, look distally first to allow additional proximal attempts on the same extremity, if necessary. Once the tourniquet is applied, you can have the patient pump his/her fist open and closed several times to help the vasculature become engorged. Feel for a soft, spongy, non-pulsatile vessel.

Figure 8.3 Position of tourniquet proximal to target vein.
3. Clean the siteUse an alcohol pad, betadine, chlorhexadine, or a similar antiseptic product to clean the proposed IV site. Allow the area to dry.
4. Insertion of the IVHold the skin taut with one hand while inserting the needle with your dominant hand. Approach the vessel as shallow as possible (less than 30° angle to the skin) with the bevel of the needle facing up or away from the patient. Once you feel a “pop” and/or see a flash of blood in the reservoir of the IV needle, advance the needle slightly further and slowly slide the catheter over the needle, cannulating the vessel with the plastic catheter while not moving the needle itself (Figure 8.4).

Figure 8.4 “Flash” of blood indicating that the needle is within the vein’s lumen and the catheter should be advanced over the needle.
5. Removing the needleHold firm pressure over the tip of the cannulated plastic catheter while you withdraw the needle from the hub of the catheter. If applicable, push the button to retract the needle to its safe position and move the needle to a safe area. The needle needs to be disposed of in a sharps container as soon as the IV is secured.
6. Securing the IVAttach the saline lock and flush the lock with saline or attach IV fluid tubing directly to the hub of the catheter. Secure the catheter hub with tape or a commercial securing device. Check for signs of infiltration (i.e. localized swelling, inability to flush catheter, pain).
External jugular vein access has a similar technique. The needle is inserted in a caudad direction, but no tourniquet is used. Instead, the index finger of the non-dominant hand can be used to apply gentle pressure to the external jugular vein just above the clavicle to facilitate venous engorgement. Care should be taken to avoid placing a needle puncture too low in the neck (i.e. at or immediately above the clavicle) to avoid lung injury. Blind attempts when the external jugular vein is not readily apparent are not advised due to potential for serious injury to surrounding structures (Figure 8.5).

Figure 8.5 External jugular vein.
Contraindications to intravenous access relate mainly to site selection. Sites with burns, cellulitis, trauma, and other conditions that compromise the integrity of the overlying skin should be avoided. Extremities on the side of a recent mastectomy or lymphatic chain removal, those that contain known thromboses, and those that contain permanent modifications for dialysis access should be used only when all other options have been exhausted. Special consideration must be given to patients with known bleeding disorders and those who are taking medications that may alter coagulation, as ensuring ease of compressibility becomes an important factor to limit excessive bleeding from cannulation attempts.
Maintenance of vascular access in the prehospital setting may often prove difficult as perspiration, mud, dirt, and water reduce the effectiveness of tape and adhesive dresssings used to secure the catheter. Combative or confused patients can also intentionally or unintentionally dislodge their IV access during transport and may require additional verbal instruction and reminders along with extra padding/support to maintain the line. Gauze wraps, elastic bandages, and arm boards are just a few examples of adjuncts used to protect and optimally position venous access.
Intraosseous accessIntraosseous devices function to access the intramedullary vessels found in the bone marrow of spongy bone that lead to the central circulation of the body. The IO needle, embedded in the bony structure, is protected by the non-collapsible periosteum, solving any problems with

patency that may be encountered with IVs during vasoconstriction and low-flow states found in sepsis and cardiac arrest.
Intraosseous access is currently attainable with manual, impact-driven, and powered drill methods. The gauge and length of some of the commercially available products will vary for the adult and pediatric patient. The commonly available EZ-IOTM uses a 15 mm long needle for children under 39 kg while 25 mm and 45 mm lengths are available for patients 40 kg or greater; all are 15 gauge. The sites of insertion vary by manufacturer recommendations but locations may include the proximal tibia, distal tibia, proximal humerus, and sternum. Contraindications to IO access are generally site specific and include infection of the overlying skin, fracture at or above the IO site, vascular compromise, and previous surgery or significant deformity of the bone. Previous sternotomy, suspected sternal fracture, and CPR with chest compressions exclude use of sternal IO access. Potential complications include osteomyelitis, fat emboli, fracture, growth plate injury, compartment syndrome, infection, and extravasation resulting in local tissue injury and swelling [14–16].
Drinker and Lund in the 1920s were the first to use IO vascular access in the sternum of animal models, demonstrating that the fluid given did indeed reach intravascular circulation. Josefson followed in 1934, reporting the first IO use in humans. Soon after, in the 1940s, the first use of the IO was documented in the pediatric population. While its use with military personnel during World War II was advocated when IV access was delayed or difficult, the development of the over-the-needle PVC IV catheter by Massa in the 1950s temporarily curtailed use of the IO. The reemergence of the IO in the 1980s in the Pediatric Advanced Life Support and Advanced Pediatric Life Support courses supported its use after failed IV attempts. More recent guidelines from the American Heart Association advocate for the use of IOs as first-line access in pediatric emergencies and as first alternative in adult cardiac arrest, including in out-of-hospital settings [13–15,17].
Several recent studies have shown the success of obtaining vascular access through IOs after failed or difficult attempts at IV access. IO vascular access has demonstrated high first-attempt success rates and overall success rates of 90% and greater in adults and children [16]. The advantages of the commercially available battery-powered driver used in the study included its short learning curve, ability to easily penetrate thick cortical bone given its power source, and rapid drug delivery into the systemic circulation [18]. IO access has been proven to be as quick and effective as IV access [19]. In patients with inaccessible peripheral veins, IO access is faster and more successful than central IV lines [20].
Most medications given through the peripheral IV can be given through an IO, with bioequivalence proven between the two routes [21]. IO has been shown to have clinically comparable times to peak drug concentration compared to central IV access [17].
Wilderness, tactical, disaster, and other specialty EMS groups may encounter situations requiring early consideration of the use of the IO for vascular access. Austere conditions, limited access to an entrapped patient, or cumbersome gear and clothing of both patient and provider can obstruct efforts to initiate peripheral IV access. One study showed significantly shorter times to IO access compared to IV access in providers wearing chemical, biological, radiological, and nuclear (CBRN) protective equipment [22]. IO access is recommended during any resuscitation when IV access is not readily attainable [15].
Technique (Video Clip 8.2)

1. PreparationWash hands, don the appropriate personal protective equipment (PPE), and prepare the equipment (Figure 8.6).Figure 8.6 Intraosseous equipment.
2. Idenitify the landmarks and site Humeral head – keep the arm adducted with the palm pronated. Palpate the proximal
humerus and locate the greater tuberosity, which will be the site of insertion. Proximal tibia – identify the tibial tuberosity. The site of insertion should be two
finger breadths below and just medial to this landmark. Distal tibia – abduct and externally rotate the hip. Palpate the flat portion of bone just
proximal to the medial malleolus.
3. Clean the siteCleanse the targeted area with alcohol prep, betadine, chlorhexadine, or other antiseptic. Allow the site to dry.
4. Insert the IOInsert the IO needle into the skin overlying the desired location until bone is reached. Insert the needle through the cortex into the marrow either manually or per device-specific instructions. The needle should be relatively stable and freestanding in the bone if inserted appropriately.
5. Assess IO patencyRemove the trocar and dispose of it in a sharps container. Attach a syringe or IO-specific tubing and assess for patency of the IO. Monitor the extremity for extravasation. Attach IV fluids if indicated; use a pressure bag or manually push fluids via syringe to achieve desired infusion rates.
6. Secure the IOStabilize the IO in place with gauze and tape or a commercially available device.
In a non-urgent setting, lidocaine or other anesthetic drugs may be injected into the area of the proposed IO and infused with the fluids to reduce pain and discomfort.
Central intravenous accessPrehospital central venous access is a procedure sometimes performed by advanced-level paramedics, nurses, and EMS physicians. Usually in the form of a large 8.5 French single-lumen catheter, the route provides rapid access to the central venous circulation and a route for rapid fluid resuscitation. Central venous access may be the preferable option when attempts at peripheral and IO lines have failed and/or are contraindicated, but its use in the prehospital arena is sparsely reported (Figure 8.7). Central venous line placement by air medical transport teams has been reported [21,23]. Similarly, one report documented the performance of 115 prehospital central lines placed by field response EMS physicians over a 3-year period [24]. Critical care teams are often responsible for maintenance

of these lines during interfacility transport, so familiarity with this form of vascular access is important.Figure 8.7 Central venous catheter kit.
The internal jugular (IJ), subclavian, and femoral veins are options for central venous access. Traumatic injuries above the diaphragm often dictate a femoral location. Attempts at access in the IJ and subclavian veins have a risk of pneumothorax, which should be considered if the patient acutely decompensates during the procedure. Placement of a central line, especially in the upper body, often causes an interruption of CPR efforts [20]. Risks of bleeding from venous or inadvertent arterial puncture, infection, thrombosis, and nerve damage also exist [18]. The prehospital environment makes it nearly impossible to preserve sterile technique. Given that these lines are performed as “code” lines under emergency, semi-sterile (similar to a peripheral IV line) conditions, it should be expected that the line would be removed and another one placed if the patient survives to the ED.
Special considerationsAccessing dialysis catheters and indwelling cathetersIn the prehospital setting, dialysis catheters, infusion ports, and other long-term artificial structures should not be considered as first-line options for gaining vascular access. The health of these difficult access patients often depends on frequent IV access and medication administration; improper utilization of these routes may result in serious consequences. Alternative forms of vascular access or medication routes should be considered. In the case that the EMS provider must access these types of catheters, special attention must be paid to sterile technique and the specific proper method for accessing each individualized access point.
System medical directors may provide training and protocols for specific patient populations that may include accessing such devices earlier in the treatment algorithm.
Pediatric considerationsThe pain and anxiety in the pediatric patient associated with vascular access is often a difficult matter to address in the prehospital setting. The need for rapid vascular access in a critically ill child along with varying transport times does not typically allow for some of the pharmacological options for relieving the pain of IV insertion that are available in the ED and hospital setting. Various commercially available creams, gels, and patches often require from several minutes up to an hour of application time for effectiveness. Local infiltration of lidocaine with either a small-gauge needle or needle-free system such as the J-Tip provides quicker anesthetic delivery but requires a second, often psychologically traumatizing needle puncture or startling noise due to pressurized CO2. Often, if the child is stable enough to consider the use of these pain-reducing interventions, vascular access can be deferred until arrival to the hospital.
Medical oversight and training for pediatric patient care should focus on helping the EMS provider distinguish the stable transport from the critically ill patient who would benefit from early vascular access [25]. Additionally, attempts at IV access in young children are infrequent and often difficult. Training may be needed to improve technical skills and confidence to increase success [26].
The future: ultrasound-guided IV access

In ED care, ultrasound technology has become a useful tool to improve the success of IV access. Previously, patients who could not be cannulated by more traditional methods were often subject to more invasive procedures such as cut-downs or central lines, posing an increased level of risk. The growing widespread availability of ultrasound technology augments the ability of providers to obtain IV access in a less invasive fashion. While detailed instruction is beyond the scope of this text, ultrasound techniques can be used in a static fashion to identify the location of a suitable vein when one cannot be seen or palpated. The vein is then accessed by the usual techniques. Alternatively, a dynamic approach is often used, wherein the provider uses ultrasound to visualize the needle tip and subsequently the catheter entering the vein, confirming placement. The materials and methods are largely similar to standard peripheral access techniques, with the exception of the need for an ultrasound machine, gel, and longer length catheters for accessing deeper veins.
Multiple studies have been performed analyzing the efficacy, speed, patency, and complications of ultrasound IV access. Across several inpatient and ED environments, ultrasound-guided peripheral access shows trends towards being a comparable or preferable modality with regard to risk of failure, number of attempts, and procedure time [27]. There is clear demonstration of reduction of central line use when ultrasound is available to facilitate peripheral IV placement [28]. Success of ultrasound peripheral IV attempts was non-inferior to the external jugular approach in those who failed traditional attempts [29].
With regard to prehospital use of this technology, there are limited data and several barriers to implementation. Ultrasound machines remain expensive, and despite advances in miniaturization, most devices require a non-trivial amount of physical space. Hand-held ultrasound devices have been produced in recent years and may allow for feasibility studies of EMS-initiated ultrasound-facilitated IV access. As other applications for ultrasound are studied and implemented for prehospital use, the ability to gain vascular access may be an added benefit of the technology, even if not purchased for that primary purpose. As several other modalities are equivalent to if not faster than ultrasound-guided peripheral IV placement, this technology may find a greater stronghold in systems permissive of longer on-scene times or for long-distance/critical care transport.
ConclusionVascular access is commonly pursued as part of prehospital emergency care. In some cases it is to facilitate administration of needed medications or resuscitative fluids. In other cases IVs are placed as a precaution in case such measures are eventually needed. Many IVs are not used prior to arrival at an ED. It is important for EMS clinicians to possess the necessary skills and equipment to initiate vascular access under myriad conditions. Further, this is an area that is appropriate for monitoring and evaluating from a quality improvement perspective, including both decision-making and technical skill domains.
References1. 1 Seymour CW, Cooke CR, Hebert PL, Rea TD. Intravenous access during out-of-hospital
emergency care of noninjured patients: a population-based outcome study. Ann Emerg Med 2012;59(4):296–303.

2. 2 Band RA, Gaieski DF, Hylton JH, Shofer FS, Goyal M, Meisel ZF. Arriving by emergency medical services improves time to treatment endpoints for patients with severe sepsis or septic shock. Acad Emerg Med 2011;18(9):934–40.
3. 3 Rittenberger JC, Bost JE, Menegazzi JJ. Time to give the first medication during resuscitation in out-of-hospital cardiac arrest. Resuscitation 2006;70(2):201–6.
4. 4 Harris SA, Nicolai LA. Occupational exposures in emergency medical service providers and knowledge of and compliance with universal precautions. Am J Infect Control 2010;38(2):86–94.
5. 5 Kuzma K, Sporer KA, Michael GE, Youngblood GM. When are prehospital intravenous catheters used for treatment? J Emerg Med 2009;36(4):357–62.
6. 6 Stratton SJ. Rethinking out-of-hospital intravenous access. Ann Emerg Med 2012;59(4):304–6.
7. 7 Jones SE, Nesper TP, Alcouloumre E. Prehospital intravenous line placement: a prospective study. Ann Emerg Med 1989;18(3):244–6.
8. 8 Slovis CM, Herr EW, Londorf D, Little TD, Alexander BR, Guthmann RJ. Success rates for initiation of intravenous therapy en route by prehospital care providers. Am J Emerg Med 1990;8(4):305–7.
9. 9 Cotton BA, Jerome R, Collier BR, et al. Guidelines for prehospital fluid resuscitation in the injured patient. J Trauma 2009;67(2):389–402.
10. 10 Bickell WH, Wall MJ Jr, Pepe PE, et al. Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. N Engl J Med 1994;331(17):1105–9.
11. 11 Haut ER, Kalish BT, Cotton BA, et al. Prehospital intravenous fluid administration is associated with higher mortality in trauma patients: a National Trauma Data Bank analysis. Ann Surg 2011;253(2):371–7.
12. 12 Seamon MJ, Fisher CA, Gaughan J, et al. Prehospital procedures before emergency department thoracotomy: “scoop and run” saves lives. J Trauma 2007;63(1):113–20.
13. 13 Rivera A, Strauss K, van Zundert A, Mortier E. The history of peripheral intravenous catheters: how little plastic tubes revolutionized medicine. Acta Anaesthesiol Belg 2005;56(3):271.
14. 14 Fowler R, Gallagher JV, Isaacs SM, Ossman E, Pepe P, Wayne M. The role of intraosseous vascular access in the out-of-hospital environment (resource document to NAEMSP position statement). Prehosp Emerg Care 2007;11(1):63–6.
15. 15 Weiser G, Hoffmann Y, Galbraith R, Shavit I. Current advances in intraosseous infusion – a systematic review. Resuscitation 2012;83(1):20–6.
16. 16 Santos D, Carron PN, Yersin B, Pasquier M. EZ-IO((R)) intraosseous device implementation in a pre-hospital emergency service: a prospective study and review of the literature. Resuscitation 2013;84(4):440–5.
17. 17 Hoskins SL. Pharmacokinetics of intraosseous and central venous drug delivery during cardiopulmonary resuscitation. Resuscitation 2012;83(1):107–12.
18. 18 Gazin N, Auger H, Jabre P, et al. Efficacy and safety of the EZ-IO™ intraosseous device: out-of-hospital implementation of a management algorithm for difficult vascular access. Resuscitation 2011;82(1):126–9.
19. 19 Reades R, Studnek JR, Garrett JS, Vandeventer S, Blackwell T. Comparison of first-attempt success between tibial and humeral intraosseous insertions during out-of-hospital cardiac arrest. Prehosp Emerg Care 2011;15(2):278–81.

20. 20 Leidel BA, Kirchhoff C, Bogner V, Braunstein V, Biberthaler P, Kanz K. Comparison of intraosseous versus central venous vascular access in adults under resuscitation in the emergency department with inaccessible peripheral veins. Resuscitation 2012;83(1):40–5.
21. 21 Von Hoff DD, Kuhn JG, Burris HA III, Miller LJ. Does intraosseous equal intravenous? A pharmacokinetic study. Am J Emerg Med 2008;26(1):31–8.
22. 22 Lamhaut L, Dagron C, Apriotesei R, et al. Comparison of intravenous and intraosseous access by pre-hospital medical emergency personnel with and without CBRN protective equipment. Resuscitation 2010;81(1):65–8.
23. 23 Davis DP, Ramanujam P. Central venous access by air medical personnel. Prehosp Emerg Care 2007;11(2):204–6.
24. 24 Martin-Gill C, Roth RN, Mosesso VN. Resident field response in an emergency medicine prehospital care rotation. Prehosp Emerg Care 2010;14(3):370–6.
25. 25 Zempsky WT. Pharmacologic approaches for reducing venous access pain in children. Pediatrics 2008;122 Suppl 3:S140–53.
26. 26 Myers LA, Arteaga GM, Kolb LJ, Lohse CM, Russi CS. Prehospital peripheral intravenous vascular access success rates in children. Prehosp Emerg Care 2013;17(4):425–8.
27. 27 Heinrichs J, Fritze Z, Vandermeer B, Klassen T, Curtis S. Ultrasonographically guided peripheral intravenous cannulation of children and adults: a systematic review and meta-analysis. Ann Emerg Med 2013;61(4):444–54.
28. 28 Shokoohi H, Boniface K, McCarthy M, et al. Ultrasound-guided peripheral intravenous access program is associated with a marked reduction in central venous catheter use in noncritically ill emergency department patients. Ann Emerg Med 2013;61(2):198–203.
29. 29 Costantino TG, Kirtz JF, Satz WA. Ultrasound-guided peripheral venous access vs. the external jugular vein as the initial approach to the patient with difficult vascular access. J Emerg Med 2010;39(4):462–7