Embed Size (px)
Citation preview
What are the reporting standards for abnormal findings in upper GI endoscopy?
Portuguese Oncology Institute, Coimbra Center for Health Technology and Services Research, Faculty of Medicine, Porto Portugal
Miguel Areia
Learning Objectives
1. To understand the importance of standardizing endoscopic reports;
2. To know consensus classifications on upper endoscopic diseases to report, if applicable.
• Abnormal findings can vary substantially in upper GI:
– Organ location
– Disease: • Anatomical distortions
• Congenital lesions
• Acute lesions
• Chronic lesions
• Pathologies situated outside gastrointestinal tract
– Emergency situations.
Standards for abnormal findings
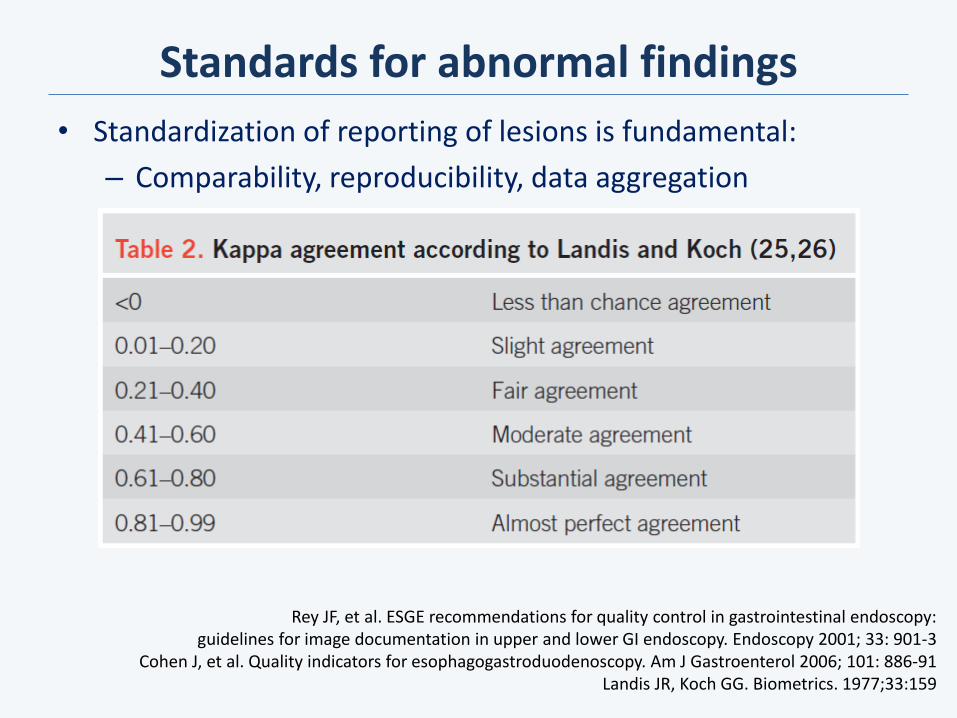
Standards for abnormal findings
• Standardization of reporting of lesions is fundamental:
– Comparability, reproducibility, data aggregation
Rey JF, et al. ESGE recommendations for quality control in gastrointestinal endoscopy: guidelines for image documentation in upper and lower GI endoscopy. Endoscopy 2001; 33: 901-3
Cohen J, et al. Quality indicators for esophagogastroduodenoscopy. Am J Gastroenterol 2006; 101: 886-91 Landis JR, Koch GG. Biometrics. 1977;33:159
• Location
• Size or length
• Number
• Morphology
• Homogeneity
• Clinical suspicion
• Picture documentation
• If applicable: – Signs of haemorrhage
– Previous surgery: type
– Stenosis: traversable or not
– Technique performed
• Haemostasis was achieved
Standards for abnormal findings
Park WG, et al. Quality indicators for EGD. Gastrointest Endosc. 2015;81:17 Minimal Standard Terminology for Gastrointestinal Endoscopy: World Endoscopy Organisation (WEO), 2009:1
• Protruding lesions (lump):
– Stenosis, compression or ring
– Nodule, polyp, tumor, varix, fold, ectopic pancreas.
• Excavated lesions:
– Diverticulum
– Erosion, ulcer, scar, fistula, perforation or Mallory-Weiss tear.
• Mucosa:
– Erythematous, oedematous, granular, nodular, atrophic.
Standards for abnormal findings
Cohen J, et al. Quality indicators for esophagogastroduodenoscopy. Am J Gastroenterol 2006; 101: 886-91 Minimal Standard Terminology for Gastrointestinal Endoscopy: World Endoscopy Organisation (WEO), 2009:1-45
Validated or consensus
classifications

• Barrett oesophagus (Prague C & M classification)
Validated or consensus classifications
Armstrong D. Aliment Pharmacol Ther. 2004;20 Suppl 5:40 Sharma P, et al. Gastroenterology 2006;131:1392
Tytgat GNJ, Tytgat HAJ. Grading and Staging in Gastroenterology. Thieme Verlag, 2009:81 Minimal Standard Terminology for Gastrointestinal Endoscopy: World Endoscopy Organisation (WEO), 2009:1
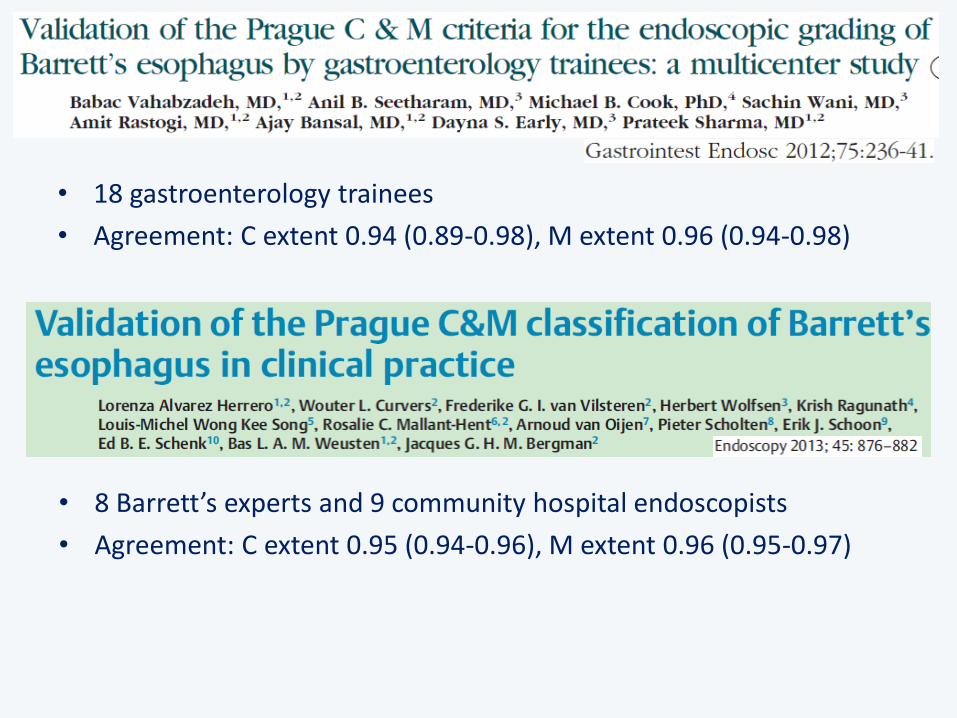
• 18 gastroenterology trainees
• Agreement: C extent 0.94 (0.89-0.98), M extent 0.96 (0.94-0.98)
• 8 Barrett’s experts and 9 community hospital endoscopists
• Agreement: C extent 0.95 (0.94-0.96), M extent 0.96 (0.95-0.97)

• Reflux oesophagitis (Los Angeles classification)
Validated or consensus classifications
Armstrong D, et al. Gastroenterology 1996;111:85 Lundell LR, et al. Gut 1999;45:172
Tytgat GNJ, Tytgat HAJ. Grading and Staging in Gastroenterology. Thieme Verlag, 2009:81 Minimal Standard Terminology for Gastrointestinal Endoscopy: World Endoscopy Organisation (WEO), 2009:1
• 46 endoscopists, experts and trainees, Europe, USA, Japan, Australia
• LA agreement: 0.40 (0.22–0.51); all other < 0.10
• 4 experts, 5 trainees
• Los Angeles and Hetzel-Dent classifications
• Experts: κ = 0.55 vs. 0.55, Trainees: κ = 0.44 vs. 0.39

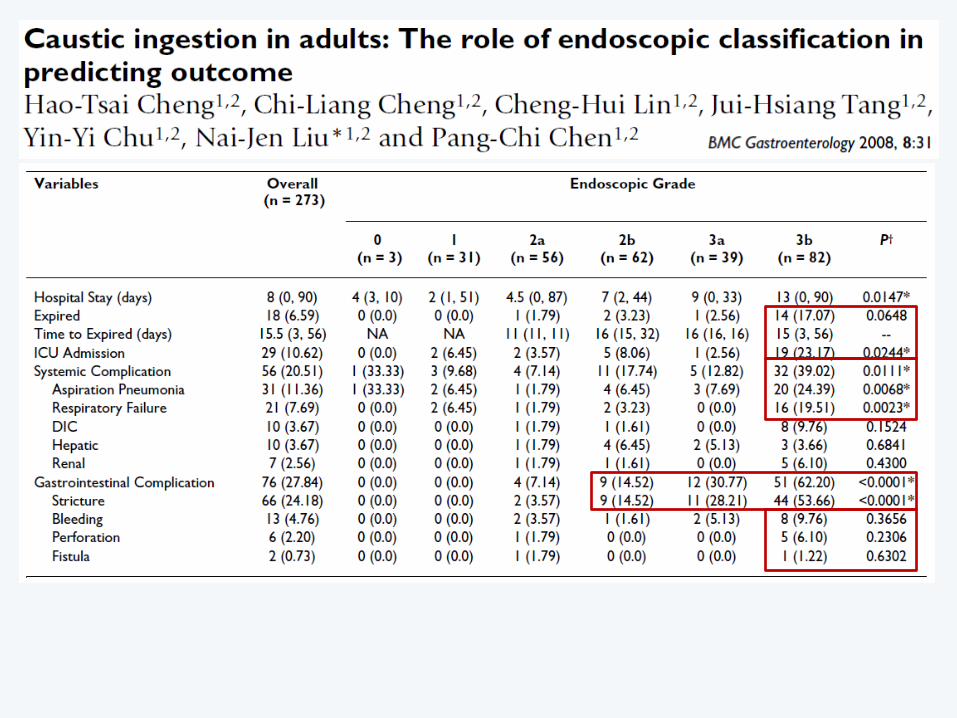
• Caustic injury (Zargar scale)
Validated or consensus classifications
Zargar SA, et al. Gastroenterology. 1989;97:702 Zargar SA et al. Gastrointest Endosc 1991;37:165
Tytgat GNJ, Tytgat HAJ. Grading and Staging in Gastroenterology. Thieme Verlag, 2009:1-80
Grade Description Prognosis
I Oedema, hyperaemia
No sequel IIa Superficial ulceration, erosions,
friability, blisters, exudates, hemorrhages, whitish membranes
IIb Grade 2a plus deep discrete or circumferential ulcerations
Scar
IIIa Multiple small ulceration and areas of necrosis with brown-black or grayish discoloration
IIIb
Multiple and deep ulcerations Extensive necrosis
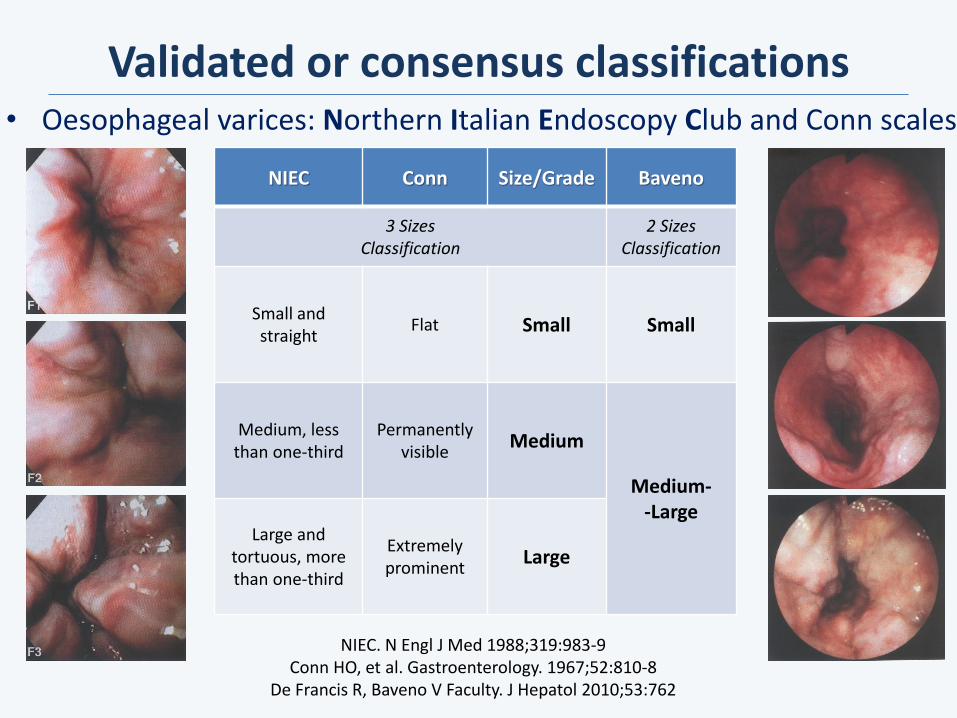
• Oesophageal varices: Northern Italian Endoscopy Club and Conn scales
Validated or consensus classifications
NIEC. N Engl J Med 1988;319:983-9 Conn HO, et al. Gastroenterology. 1967;52:810-8
De Francis R, Baveno V Faculty. J Hepatol 2010;53:762
NIEC Conn Size/Grade Baveno
3 Sizes Classification
2 Sizes Classification
Small and straight
Flat Small Small
Medium, less than one-third
Permanently visible
Medium
Medium- -Large
Large and tortuous, more than one-third
Extremely prominent
Large
• Agreement for size (kappa = 0.59) and red signs (kappa = 0.60)
• Agreement grades 0 to 1 vs. 2 to 3 (kappa = 0.52)
J Pediatr Gastroenterol Nutr. 2015;61:176
• 3-degree vs. 2-degree scales: kappa = 0.34 vs. 0.38
• Red signs: kappa = 0.49
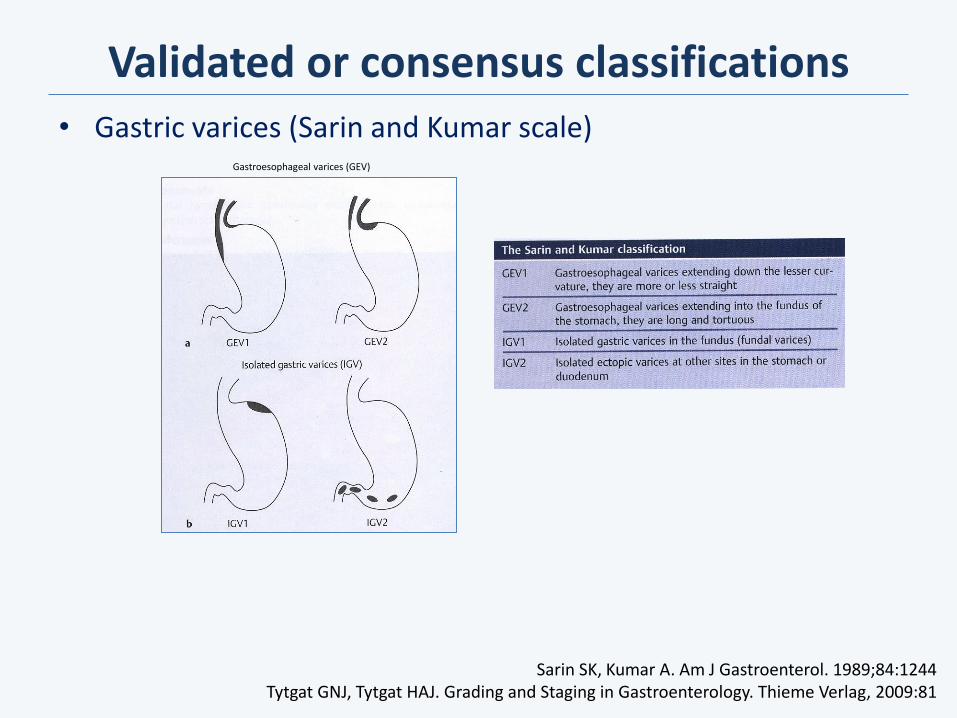
• Gastric varices (Sarin and Kumar scale)
Validated or consensus classifications
Sarin SK, Kumar A. Am J Gastroenterol. 1989;84:1244 Tytgat GNJ, Tytgat HAJ. Grading and Staging in Gastroenterology. Thieme Verlag, 2009:81
Gastroesophageal varices (GEV)
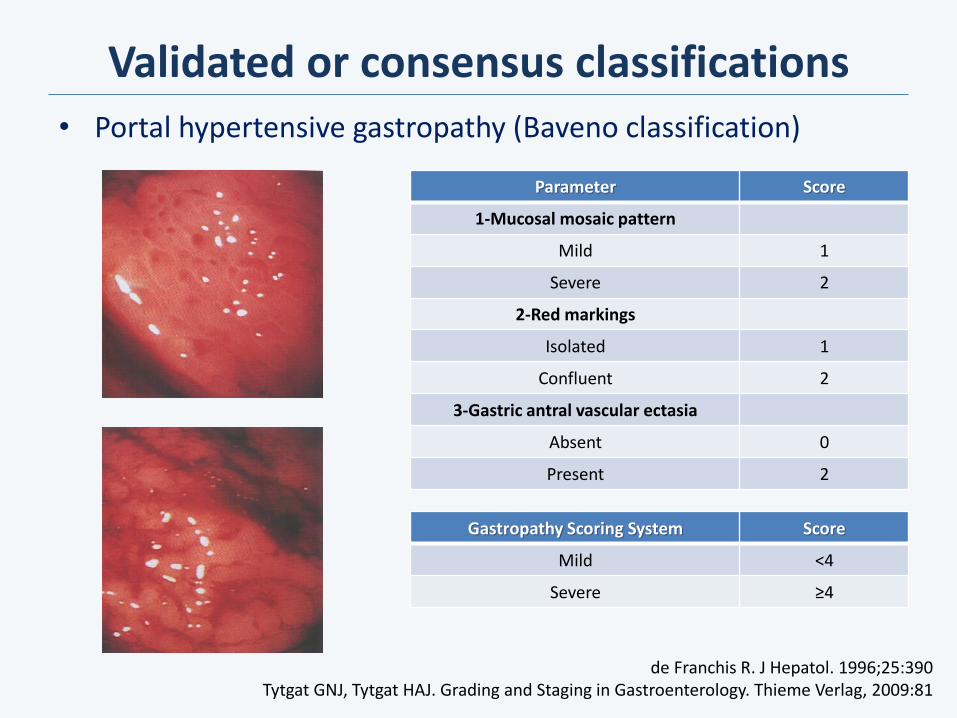
• Portal hypertensive gastropathy (Baveno classification)
Validated or consensus classifications
Parameter Score
1-Mucosal mosaic pattern
Mild 1
Severe 2
2-Red markings
Isolated 1
Confluent 2
3-Gastric antral vascular ectasia
Absent 0
Present 2
Gastropathy Scoring System Score
Mild <4
Severe ≥4
de Franchis R. J Hepatol. 1996;25:390 Tytgat GNJ, Tytgat HAJ. Grading and Staging in Gastroenterology. Thieme Verlag, 2009:81
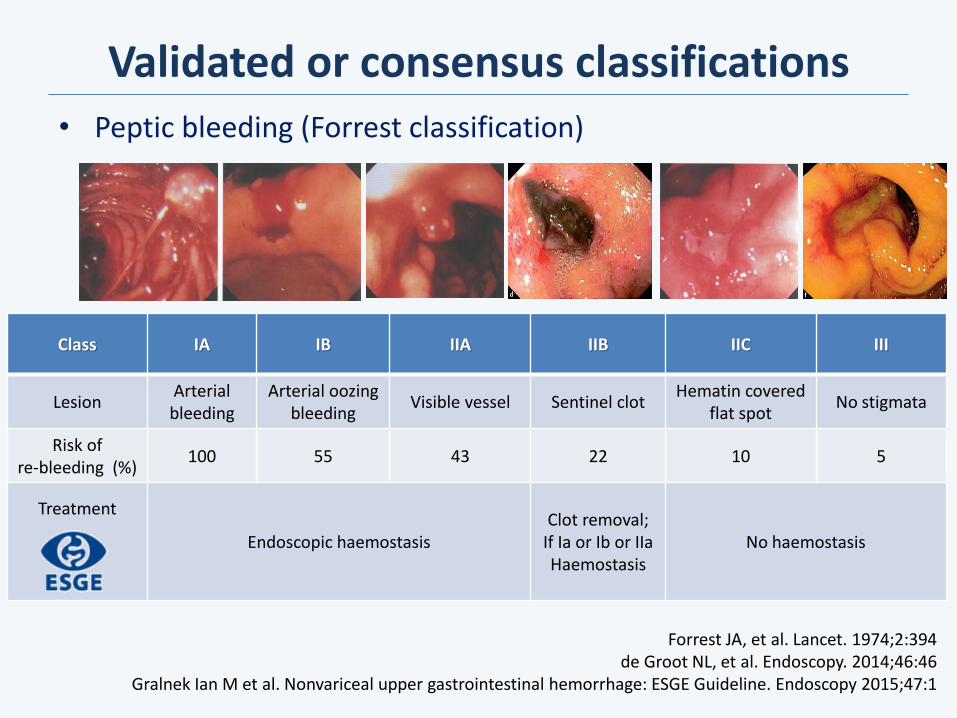
• Peptic bleeding (Forrest classification)
Validated or consensus classifications
Forrest JA, et al. Lancet. 1974;2:394 de Groot NL, et al. Endoscopy. 2014;46:46
Gralnek Ian M et al. Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline. Endoscopy 2015;47:1
Class IA IB IIA IIB IIC III
Lesion Arterial bleeding
Arterial oozing bleeding
Visible vessel Sentinel clot Hematin covered
flat spot No stigmata
Risk of re-bleeding (%)
100 55 43 22 10 5
Treatment
Endoscopic haemostasis Clot removal;
If Ia or Ib or IIa Haemostasis
No haemostasis
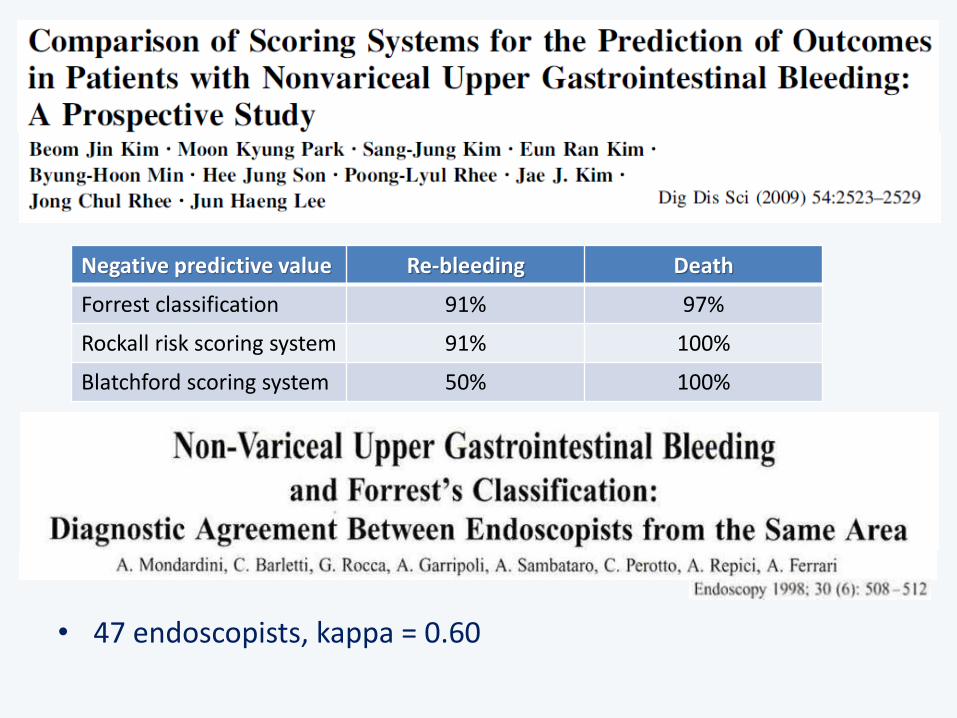
• 47 endoscopists, kappa = 0.60
Negative predictive value Re-bleeding Death
Forrest classification 91% 97%
Rockall risk scoring system 91% 100%
Blatchford scoring system 50% 100%

Validated or consensus classifications
• Duodenal polyposis in FAP (Spigelman classification)
Spigelman AD, et al. Lancet 1989;2:783 Saurin JC, et al. J Clin Oncol 2004;22:493
Syngal S, et al. ACG guideline. Am J Gastroenterol 2015;110:223
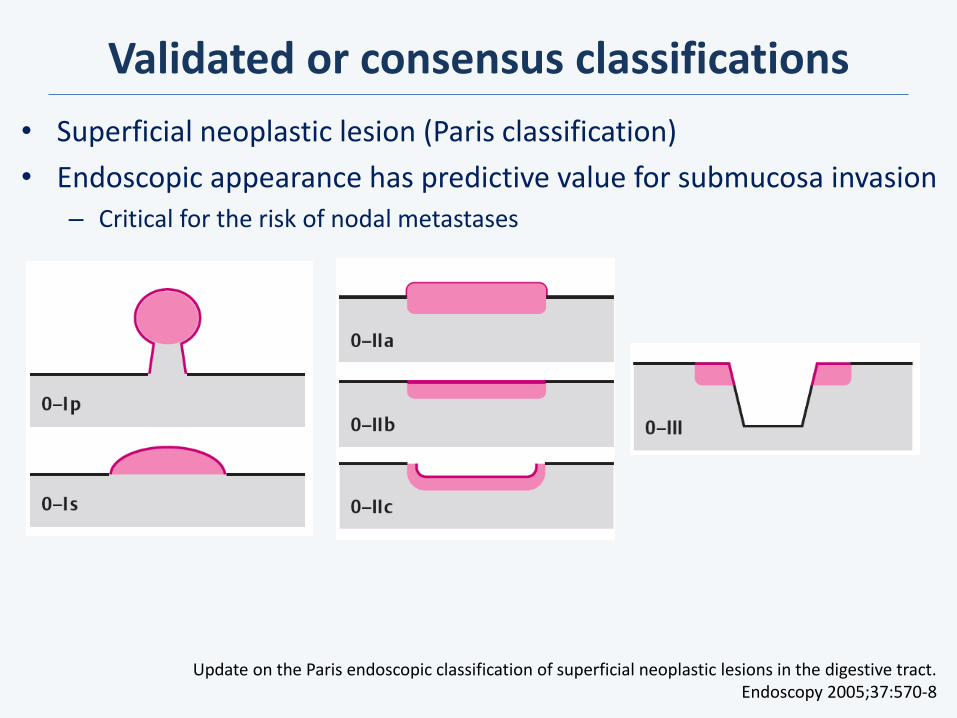
• Superficial neoplastic lesion (Paris classification)
• Endoscopic appearance has predictive value for submucosa invasion – Critical for the risk of nodal metastases
Validated or consensus classifications
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
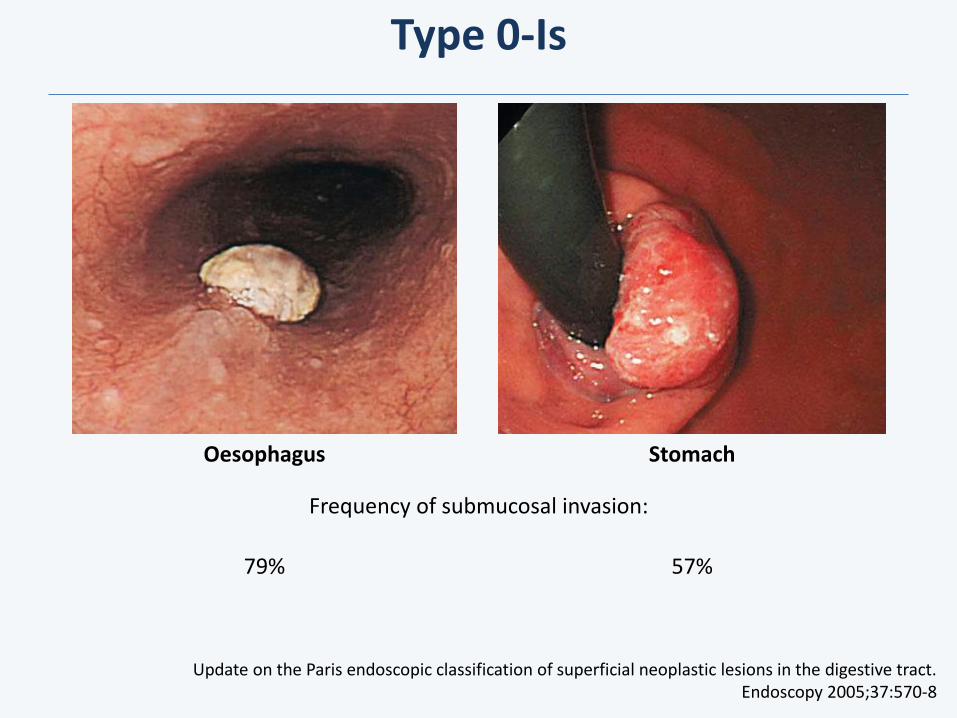
Type 0-Is
Oesophagus Stomach
Frequency of submucosal invasion:
79% 57%
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
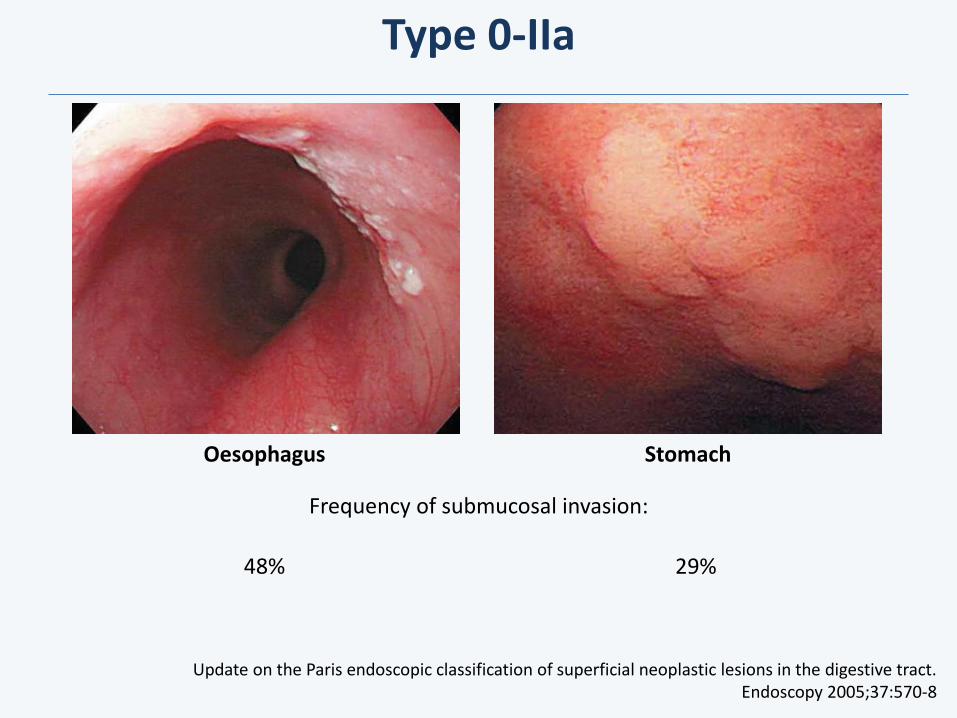
Type 0-IIa
Oesophagus Stomach
Frequency of submucosal invasion:
48% 29%
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
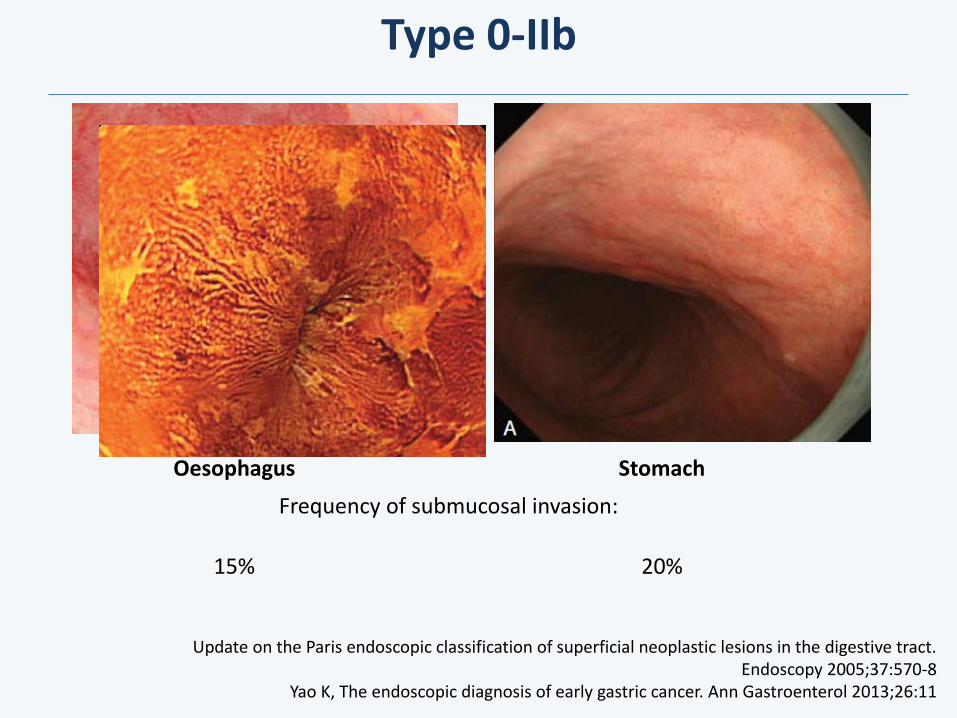
Type 0-IIb
Oesophagus Stomach
Frequency of submucosal invasion:
15% 20%
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
Yao K, The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol 2013;26:11
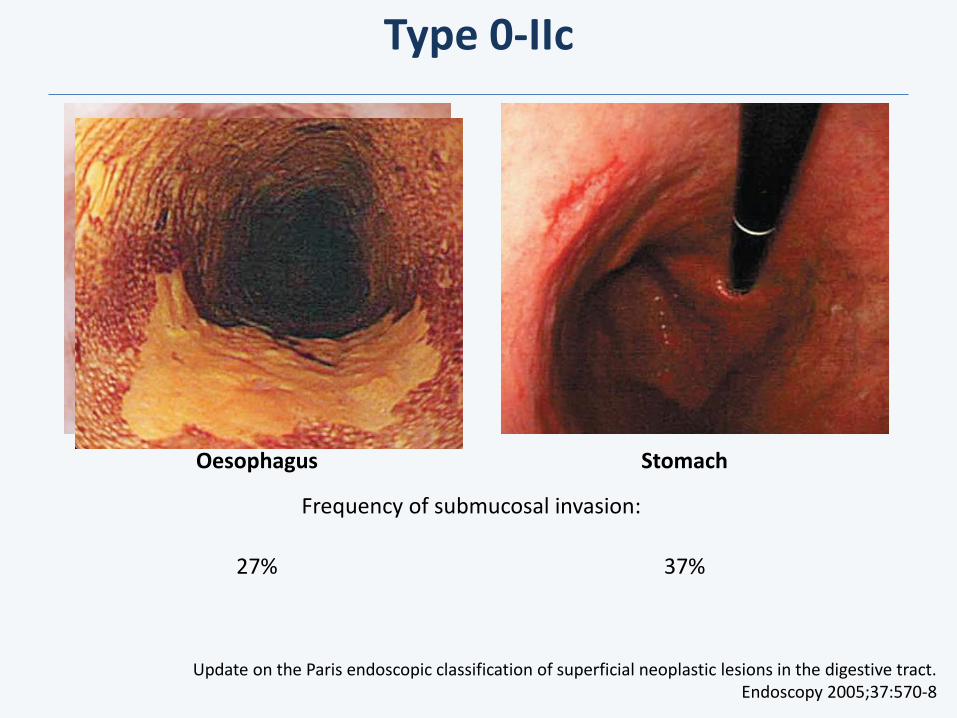
Type 0-IIc
Oesophagus Stomach
Frequency of submucosal invasion:
27% 37%
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
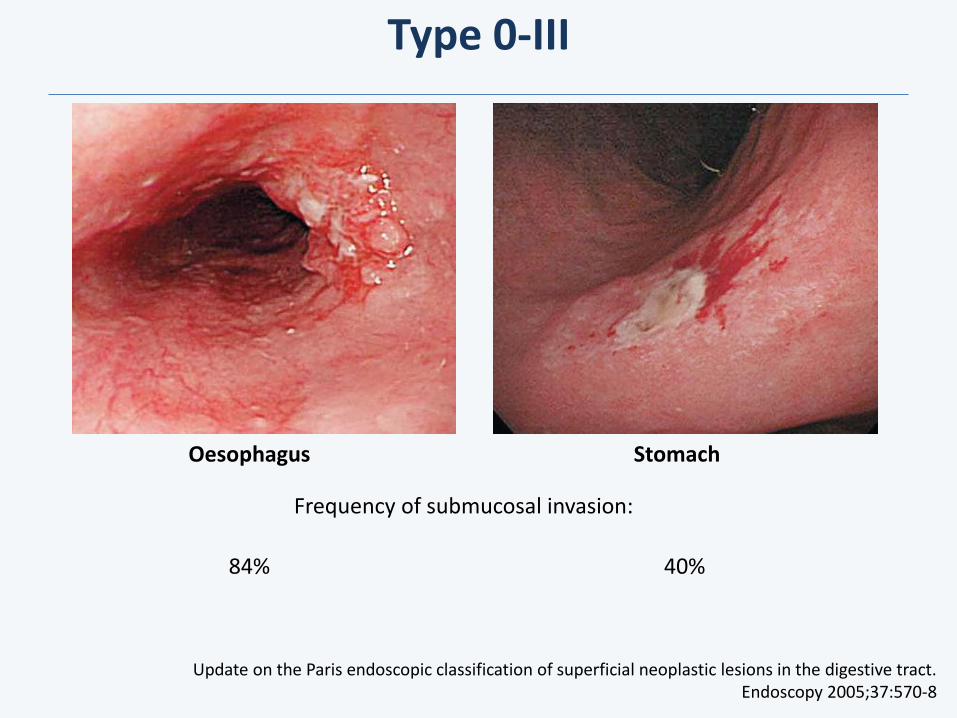
Type 0-III
Oesophagus Stomach
Frequency of submucosal invasion:
84%
Update on the Paris endoscopic classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005;37:570-8
40%
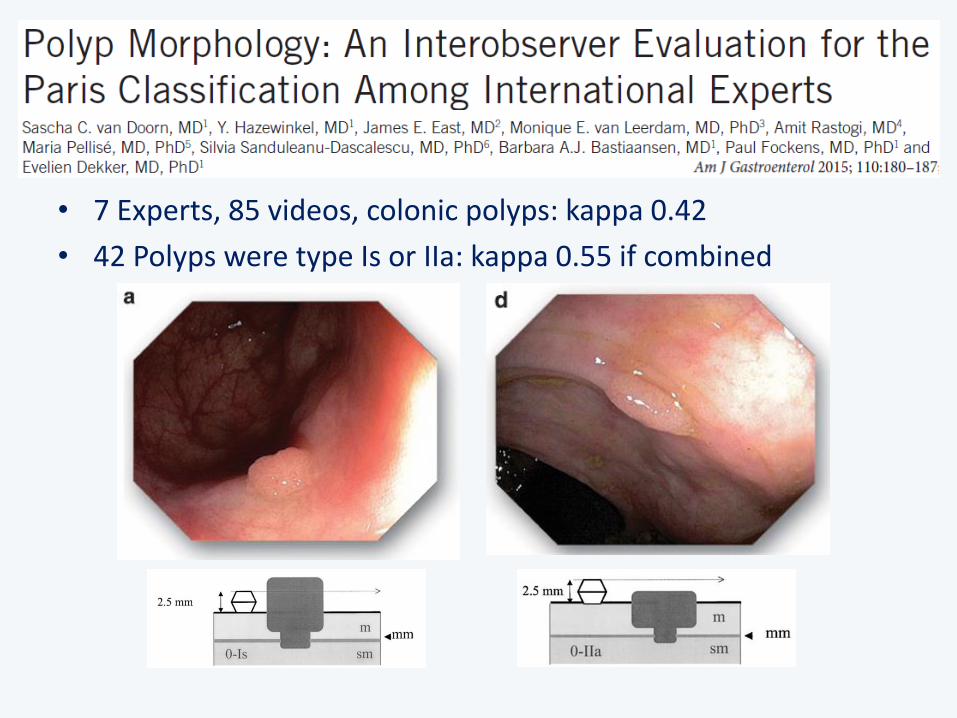
• 7 Experts, 85 videos, colonic polyps: kappa 0.42
• 42 Polyps were type Is or IIa: kappa 0.55 if combined

Conclusion
1. Use standardized language in endoscopic reports “Minimal Standard Terminology for Gastrointestinal Endoscopy”
2. If a lesion is detected Describe all you would like others to tell you
3. Use validated/consensus classifications Interobserver agreement
Related to prognosis and/or treatment options
Consensus recommended
Coimbra, Portugal
Thanks for your attention!





























