Embed Size (px)
Citation preview
Abstract The object of this study was to investigate thefetal biparietal diameter/kidney length ratio in normaland hyperechogenic kidneys during the 3rd trimester ofgestation. Screened pregnancies were chronically hyp-oxic [i.e. intrauterine growth retardation (IUGR)]. De-pending on the renal manifestation of the intrauterinechronic hypoxia, the cases were divided into two studygroups. Group I was composed of 28 fetuses with IUGRand hyperechogenic renal medullae. Group II consistedof 62 fetuses with IUGR and normal echoic kidney. Bothstudy groups included pregnant women from the 3rd trimester. Fetal renal hyperechogenicity is an indicator of depression of fetal renal perfusion, correlated withpathological growth in the fetal kidney development.The fetal biparietal diameter/kidney length ratio was sig-nificantly higher in hyperechogenic cases. This may alsobe an in utero indicator of subsequent intrauterine andneonatal complications. Detailed ultrasound examina-tions of renal parenchyma and length appear to be usefulin the prenatal diagnosis of reduced renal perfusion andof intrauterine hypoxia, allowing detection of possiblepathological fetal conditions in utero.
Keywords Biparietal diameter/kidney length ratio · Fetus · Intrauterine growth retardation · Renal hyperechogenicity · Ultrasonography
Introduction
The benefits of sonographic evaluation of urinary tractdisease in children are well documented [1]. It is knownthat changes in kidney length may precede renal echo-texture changes in certain renal diseases [2]. Evaluationof fetal kidney biometry must be included in the guide-lines for an early transvaginal scan, and measurement ofthe kidney parameters is recommended in all cases.
Some authors have proposed ratios, in different stagesof pregnancy, as a screening tool for the detection of ab-normal kidney growth [3, 4]. Normal standards estab-lished for kidney length in term infants, premature in-fants, and children as measured with ultrasonographyhave facilitated accurate evaluation of abnormal kidneys[3, 4, 5, 6, 7, 8].
Pathological kidney dimensions mean pathologicalfunction. There are larger than normal kidney measure-ments in polycystic kidney, thrombosis of renal vein, tu-mor, acute inflammations, etc. There are smaller thannormal kidney measurements in dysplasia, hypoplasia,intrauterine obstructions (Prune-Belly syndrome, ure-throcele, etc.), renal failure, oligomeganephronia, chron-ic inflammation, etc. [9].
In fetuses with intrauterine growth retardation(IUGR), normal standards for biparietal diameter/kidneylength ratio have not, to our knowledge, been comparedwith gestational age in hyperechoic cases with no ana-tomical alteration. Fetal renal hyperechogenicity with noanatomical alteration is the indirect sign of intrauterinehypoxia (e.g. IUGR) [9, 10, 11, 12, 13]. Therefore, wemeasured biparietal diameter/kidney length ratio with ul-trasonography in fetuses to establish whether the renalhyperechogenicity correlates with pathological size inIUGR due to intrauterine hypoxic conditions.
Materials and methods
Ninety IUGR cases from a group of routinely scanned pregnantwomen were included in our prospective study. The study lasted
A. Surányi (✉) · A. PálDepartment of Obstetrics and Gynecology, Albert Szent-Györgyi Medical University, Szeged, Hungarye-mail: [email protected].: +36-62-545491, Fax: +36-62-545711
T. NyáriDepartment of Medical Informatics, Albert Szent-Györgyi Medical University, Szeged, Hungary
A. SurányiDepartment of Obstetrics and Gynecology, University of Szeged, 1, Semmelweis, P.O. Box 438, 6725 Szeged, Hungary
Pediatr Nephrol (2003) 18:14–17DOI 10.1007/s00467-002-1004-1
O R I G I N A L A RT I C L E
Andrea Surányi · Tibor Nyári · Attila Pál
What is biparietal diameter/kidney length ratio in cases with renal hyperechogenicity?
Received: 18 April 2002 / Revised: 19 August 2002 / Accepted: 24 August 2002 / Published online: 14 November 2002© IPNA 2002
15
for 8 months. Both normal and pathological cases were investi-gated during routine scans, so the stages of the pregnancies werethe 1st, 2nd, and 3rd trimesters. The gestational age was calculat-ed according to Naegele’s rule and the 1st trimester ultrasoundexamination. IUGR was established by Hansmann’s weight esti-mation, based on biparietal and transverse trunk diameters [14,15, 16].
Besides the routine scan we investigated fetal medullary echo-genicity and the size of the kidneys. Renal ultrasound studies werecarried out using a Combison 530 machine with a 3 to 5 MHztrans-abdominal transducer. We calculated the biparietal diameter/kidney length ratio.
Hyperechogenic medullae were diagnosed when the fetal renal medullae displayed an echogenicity similar to that of the surrounding bone, but higher than that of the liver or spleen[17].
The lengths of fetal kidneys were examined from the posterioraspect. The kidneys were scanned with the transducer parallel tothe vertebral column. This orientation was used uniformly for bothkidneys in all fetuses. We measured the maximal length: superiorto inferior perimeter. Two measurements (right and left kidneylength parameters) were made at each examination and averaged,because there was no statistically significant difference in thelength between the right and left kidneys. Our data are supportedby previous work [18].
We compared our nomogram for biparietal diameter/kidneylength ratio plotted against gestational age with data from Callanet al. [3] and Guariglia Rosati [4]. Our nomogram was not signifi-cantly different from the previous data [3, 4]. The values appear tobe fairly constant throughout pregnancy, with a slight decrease.
IUGR fetuses were divided into two groups: those with fetalmedullary hyperechogenicity (group I) and those without (groupII). The 28 fetuses (21 girls and 7 boys) with renal medullary hyperechogenicity were compared with the remaining IUGR cases(62 cases) as a control group. Some cases were excluded, becauseof renal anatomical alteration, from the analysis leaving 90 babiesfor study.
The renal function was followed in the immediate postnatal period (2 weeks). Renal function parameters were blood urea nitrogen, serum creatinine, serum acid-base parameters (pH, par-tial oxygen, and carbon dioxide, standard bicarbonate), and urineoutput. The results were analyzed using Fisher’s exact test and t-test.
Results
There were no significant differences in right and leftkidneys or between kidneys in boys and girls. Fetal development was established with biparietal diameter/kidney length ratio.
We used Fisher’s exact test to analyze the ratio of nor-mal and pathological cases in boys and girls in bothgroups. There was no significant difference in boys andgirls in groups I and II with this test.
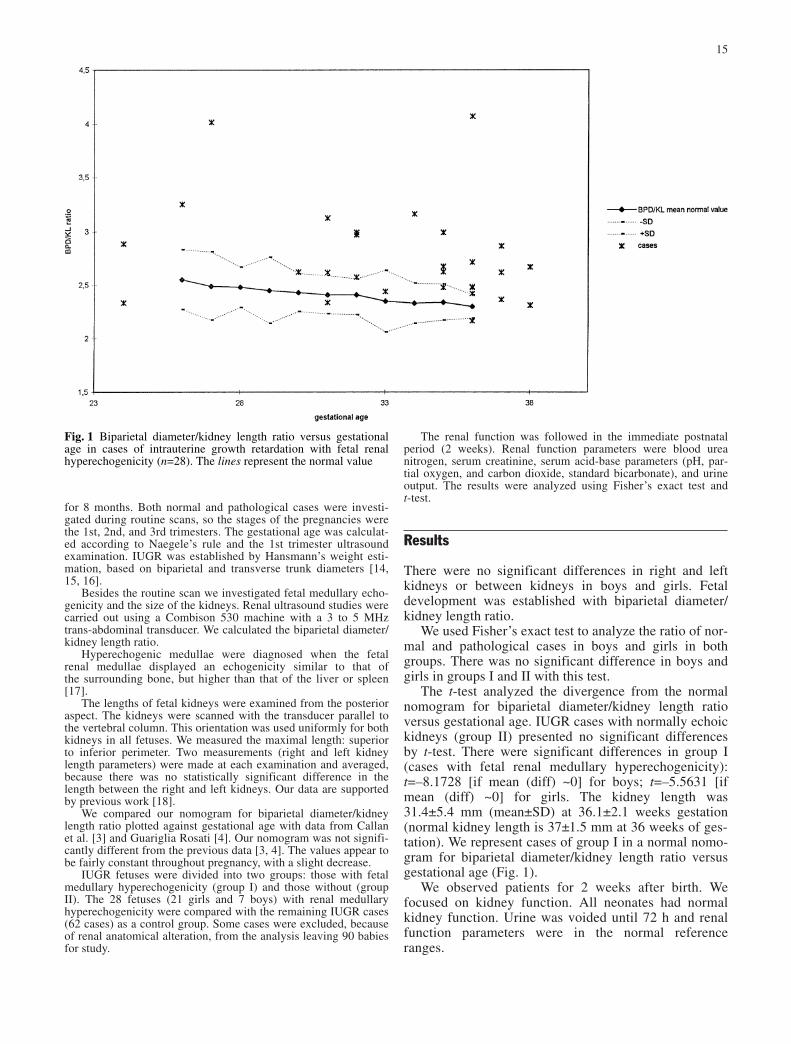
The t-test analyzed the divergence from the normalnomogram for biparietal diameter/kidney length ratioversus gestational age. IUGR cases with normally echoickidneys (group II) presented no significant differencesby t-test. There were significant differences in group I(cases with fetal renal medullary hyperechogenicity):t=–8.1728 [if mean (diff) ~0] for boys; t=–5.5631 [ifmean (diff) ~0] for girls. The kidney length was31.4±5.4 mm (mean±SD) at 36.1±2.1 weeks gestation(normal kidney length is 37±1.5 mm at 36 weeks of ges-tation). We represent cases of group I in a normal nomo-gram for biparietal diameter/kidney length ratio versusgestational age (Fig. 1).
We observed patients for 2 weeks after birth. We focused on kidney function. All neonates had normalkidney function. Urine was voided until 72 h and renalfunction parameters were in the normal reference ranges.
Fig. 1 Biparietal diameter/kidney length ratio versus gestationalage in cases of intrauterine growth retardation with fetal renal hyperechogenicity (n=28). The lines represent the normal value
dimensions of the kidneys. Renal hypoplasia can developbecause of intrauterine hypoxia [8]. Renal blood flow isestimated as 3% of the cardiac output under physiologi-cal conditions in the human fetal renal artery [19, 20].During hypoxemia, the renal blood flow fell by25%–50% compared with baseline values [9]. Thiswould imply that, instead of a local vasoconstriction ofthe renal vasculature, the fetal renal blood flow may bemaintained by a combination of mechanisms, includingan increase in arterial pressure and the intrarenal actionof various metabolites, which ultimately induce a similarhemodynamic change [21]. A direct relationship hasbeen reported between hypoxia and the renal artery pul-satility index (e.g., resistance) [13, 22]. The redistribu-tion of the fetal circulation results in abnormal renalflow. The redistribution of the blood flow is due to fetalhypoxemia. During this process, the fetal kidneys areamong those organs that are sometimes compromised,leading to transient renal insufficiency, usually a benigndisease [13, 23]. In theory, fetal hypoxia triggers a dis-cordant vasomotor reaction in the common carotid arteryand descending thoracic aorta. In the descending thoracicaorta, a reduction in the mean blood velocity and an in-crease in the pulsatility index of flow velocity develop.In the common carotid artery the mean blood velocityrises in parallel with a decrease in the pulsatility index inthe flow velocity waveform [24, 25]. The increased re-sistance index of the descending thoracic aorta could bea component of the centralization of the fetal circulationdue to chronic hypoxia. The fetal renal blood flow maysimilarly be affected as a result of an elevated intravas-cular resistance, leading to a decline in renal perfusion[10]. Reduced renal perfusion results in delay of the de-velopment of the fetal kidney, which is a possible causeof renal hypoplasia [8].
In those neonates where there had been renal hyper-echogenicity due to intrauterine hypoxia and redistribu-tion of fetal circulation, the kidney length was signifi-cantly less than the normal reference range. Therefore,when renal perfusion and growth were normal, kidneylength was normal in relation to body weight. Thesecases showed no significant difference from the nomo-gram for kidney length versus body weight.
The measurements of fetal renal hyperechogenicityand kidney length are simple examinations, and shouldtherefore be performed during a routine scan. Renal hyperechogenicity is a sensitive sign of intrauterine hypoxia, and measurement of kidney length is essentialbecause the changes in the length are more characteris-tic. If hyperechogenicity is found, the kidney length ismeasured with ultrasonography, in order to detect the indirect sign of redistribution of the fetal circulation, anearly sign of an intrauterine hypoxic state. Therefore, itis important to direct pregnant women to a perinatal in-tensive care center in order to detect the possible patho-logical fetal state.
Our study suggests the combined use of echogenicityof the fetal renal parenchyma and length measurement ofthe fetal kidney in order to detect pathological changes
16
Discussion
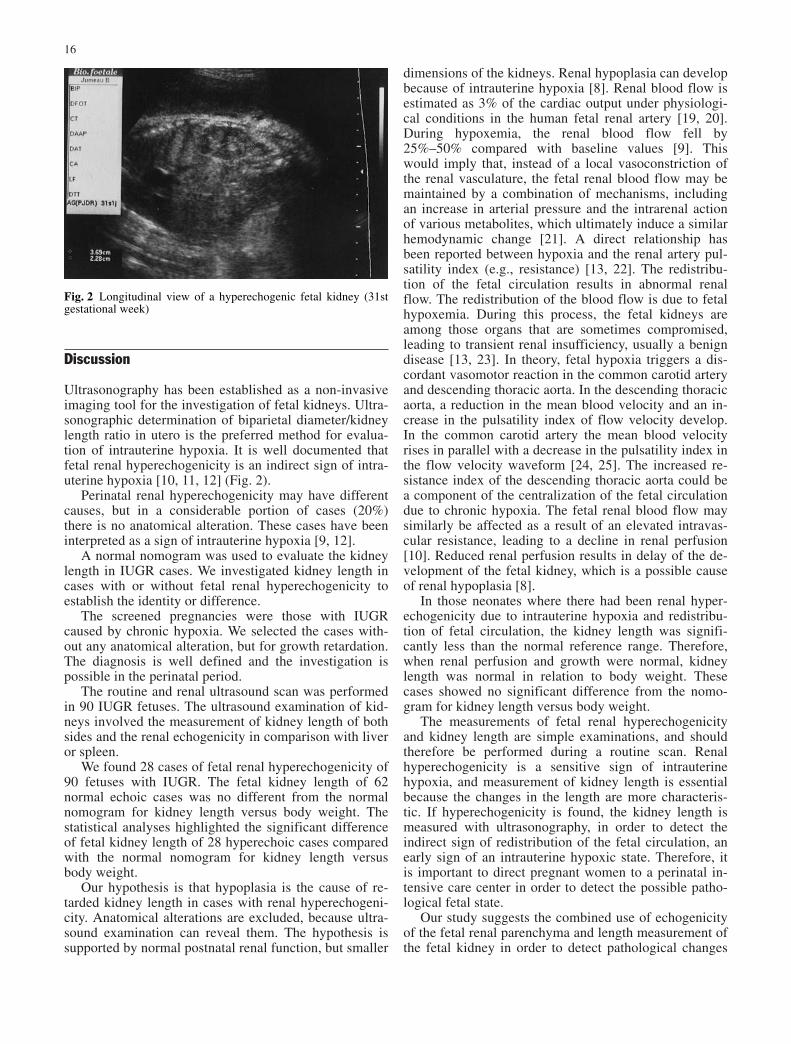
Ultrasonography has been established as a non-invasiveimaging tool for the investigation of fetal kidneys. Ultra-sonographic determination of biparietal diameter/kidneylength ratio in utero is the preferred method for evalua-tion of intrauterine hypoxia. It is well documented thatfetal renal hyperechogenicity is an indirect sign of intra-uterine hypoxia [10, 11, 12] (Fig. 2).
Perinatal renal hyperechogenicity may have differentcauses, but in a considerable portion of cases (20%)there is no anatomical alteration. These cases have beeninterpreted as a sign of intrauterine hypoxia [9, 12].
A normal nomogram was used to evaluate the kidneylength in IUGR cases. We investigated kidney length incases with or without fetal renal hyperechogenicity to establish the identity or difference.
The screened pregnancies were those with IUGRcaused by chronic hypoxia. We selected the cases with-out any anatomical alteration, but for growth retardation.The diagnosis is well defined and the investigation ispossible in the perinatal period.
The routine and renal ultrasound scan was performedin 90 IUGR fetuses. The ultrasound examination of kid-neys involved the measurement of kidney length of bothsides and the renal echogenicity in comparison with liveror spleen.
We found 28 cases of fetal renal hyperechogenicity of90 fetuses with IUGR. The fetal kidney length of 62 normal echoic cases was no different from the normalnomogram for kidney length versus body weight. Thestatistical analyses highlighted the significant differenceof fetal kidney length of 28 hyperechoic cases comparedwith the normal nomogram for kidney length versusbody weight.
Our hypothesis is that hypoplasia is the cause of re-tarded kidney length in cases with renal hyperechogeni-city. Anatomical alterations are excluded, because ultra-sound examination can reveal them. The hypothesis issupported by normal postnatal renal function, but smaller
Fig. 2 Longitudinal view of a hyperechogenic fetal kidney (31stgestational week)

12. Tálosi G, Streitman K, Surányi A, Pintér S, Horvath I, Mulugeta Z (1996) The possible role of uric acid in renal hyperechogencity in neonatal hypoxic acute shock. J PerinatMed 24:693–697
13. Surányi A, Pál A, Streitman K, Pintér S, Kovács L (1997) Fetal renal hyperechogenicity in pathological pregnancies.J Perinat Med 25:274–279
14. Surányi A, Streitman K, Pál A, Nyári T, Retz C, Foidart JM,Schaaps JP, Kovács L (2000) Fetal renal artery flow and renalechogenicity in the chronically hypoxic state. Pediatr Nephrol14:393–399
15. Hansmann M (1976) Ultraschallbiometrie im II. und III. Tri-mester der Schwangerschaft. Gynecologe 9:133
16. Dornan KJ, Hansmann M, Redford DHA, Witmann BK (1982)Fetal weight estimation by real-time ultrasound measurementof biparietal and transverse trunk diameter. Am J Obstet Gynecol 142:652–657
17. Kurjak A (1992) An atlas of ultrasonography in obstetrics andgynecology. (The encyclopedia of visual medicine series.)Pathenon, New Jersey, pp 64–67
18. Hayden CK, Santa-Cruz FR, Amparo EG, Brouhard B,Swischuk LE, Ahrendt DK (1984) Ultrasonographic evalua-tion of the renal parenchyma in infancy and childhood. Radi-ology 152:413–417
19. De Vries L, Levene MI (1983) Measurement of renal size inpreterm and term infants by real time ultrasound. Arch DisChild 58:145–147
20. Peeters LLH, Sheldon RE, Jones MD Jr, Makowski EL, Meschia G (1979) Blood flow to fetal organs as a function ofarterial oxygen content. Am J Obstet Gynecol 135:637–646
21. Copel JA, Kathryn L (eds) (1995) Doppler ultrasound in ob-stetrics and gynecology. Reed Raven, New York, pp 131–132
22. Robillard JE, Weitzman RE, Burmeister L, Smith FG JR(1981) Developmental aspects of the renal response to hypox-emia in the lamb fetus. Circ Res 48:128–137
23. Soothill PW, Nicolaides KH, Campbell S (1987) Prenatal asphyxia, hyperlacticemia, hypoglycemia and erythroblastosisin growth-retarded fetuses. BMJ 1:1051–1053
24. Avni EF, Spehl-Robberecht M, Lebrun D, Gomes H, Garel L(1983) Transient acute tubular disease in the newborn: charac-teristic ultrasound pattern. Ann Radiol (Paris) 26:175–182
25. Vyas S, Nicolaides KH, Campbell S (1989) Renal artery flow-velocity waveforms in normal and hypoxemic fetuses. AmJ Obstet Gynecol 161:168–172
17
in renal perfusion. This may prove to better predict theoutcome in chronically hypoxic pregnancies. For thisreason, besides the routine scan, renal ultrasonographymay be important in the diagnosis of grave fetal hypoxiaat an early stage.
References
1. Hayden CM, Sata-Cruz FR (1984) Ultrasonographic evalua-tion of the renal parenchyma in infancy and childhood. Radi-ology 152:413–417
2. Dinkel E, Ertel M, Dittrich M (1985) Kidney size in childhoodsonographic growth charts for kidney length and volume.Pediatr Radiol 15:38–43
3. Callan NA, Otis CS, Weiner S (1985) Growth of the fetal kid-ney. Ultrasonographic measurement of the ratio of averagekidney diameter to biparietal diameter. J Reprod Med30:485–488
4. Guariglia L, Rosati P (1998) Transvaginal sonographic fetalbiparietal diameter/kidney length ratio in early pregnancy as ascreening tool for renal malformations. Fetal Diagn Ther13:154–156
5. Haugstvedt S, Lundberg J (1980) Kidney size in normal children measured by sonography. Scand J Urol Nephrol14:251–255
6. Rosenbaum DM, Korngold E, Teele RL (1984) Sonographicassessment of renal length in normal children. AJR 142:467–469
7. Han BK, Babcock DS (1985) Sonographic measurementsand appearance of normal kidneys in children. AJR 154:611–
6168. Blance CE, Bookstein FL, DiPietro MA, Kelsch RC (1985)
Sonographic standards for normal infant kidney length. AJR145:1289–1291
9. Nelson WE (1995) Pediatrics handbook. Saunders, New York,pp 1337–1356
10. Chiara A, Chirico G, Comelli L (1990) Increased renal echo-genicity in the neonate. Early Hum Dev 22:29–33
11. Surányi A, Pál A, Viski S, Streitman K, Pintér S (1995) The fetal renal hyperechogenicity in chronically hypoxic preg-nancy. Ultrasound Obstet Gynecol 6:155