Embed Size (px)
Citation preview
VRHA Health Information Technology Project
Primary Care ConferenceMay 17, 2011
What is VRHA?
• VRHA is the VT Rural Health Alliance
• VRHA is a Health Center Controlled Network
• VRHA is a program of Bi-State
• VRHA was initially funded as a Network by the Office of Rural Health Policy (with some seed money from the State Office of Rural Health).
2
VRHA Purpose
The primary purpose of VRHA is to work collaboratively on putting state and federal health policy initiatives into practice, leveraging shared resources and expertise for common benefit focused on shared missions of access to high quality health care for the medically underserved, including uninsured and underinsured, regardless of ability to pay.
3
VRHA Membership
• Bi-State Primary Care Association• VT FQHCs (8)• North Country Health Systems• Vermont Coalition of Clinics for the Uninsured (VCCU)• Vermont’s Area Health Education Center (AHEC) Network• Vermont Information Technology Leaders (VITL)• Vermont Program for Quality in Health Care (VPQHC)
Participation in the VRHA HIT Project is limited to the eight VT FQHCs. VRHA is viewed as a “statewide” HCCN because all VT FQHCs are participating in the network.
3
National HIT Initiatives
• Expansion of regional and statewide Health Information Exchange (HIE).
• Development of a National Health Information Network (NHIN).
• ARRA funding to drive Electronic Health Record (EHR) adoption through incentive programs and grants.
• Achieve pervasive use of data to support quality improvement and accountability.
• Create standards and implementation guides for a robust privacy and security infrastructure
5
Vermont HIT Initiatives
• Expanding the Vermont Health Information Exchange (VHIE) to encompass data exchange between hospitals, ambulatory providers, long term care, mental health and home health.
• Implementing a statewide Clinical Data Repository (CDR) to support expansion of the Vermont Blueprint for Health medical home payment reform model.
• Enabling adoption of Electronic Health Records by primary care providers and critical access hospitals throughout the state through the ARRA funded Regional Extension Center.
• Connecting the statewide Immunization Registry to the VHIE.
6
Project Goals
• Patient data in each FQHC’s Electronic Health Record is structured, reliable, complete and reportable.
• Clinical Data Repository is populated with data from all FQHCs
• Clinical UDS reporting is automated in EHR or CDR
• Network-wide comparative reporting is available through the CDR
• HIE connectivity is implemented at each FQHC
• FQHCs complete EHR implementation and achieve Meaningful Use
• Workflow redesign and Continuous Quality Improvement are used to ensure lasting benefits
7
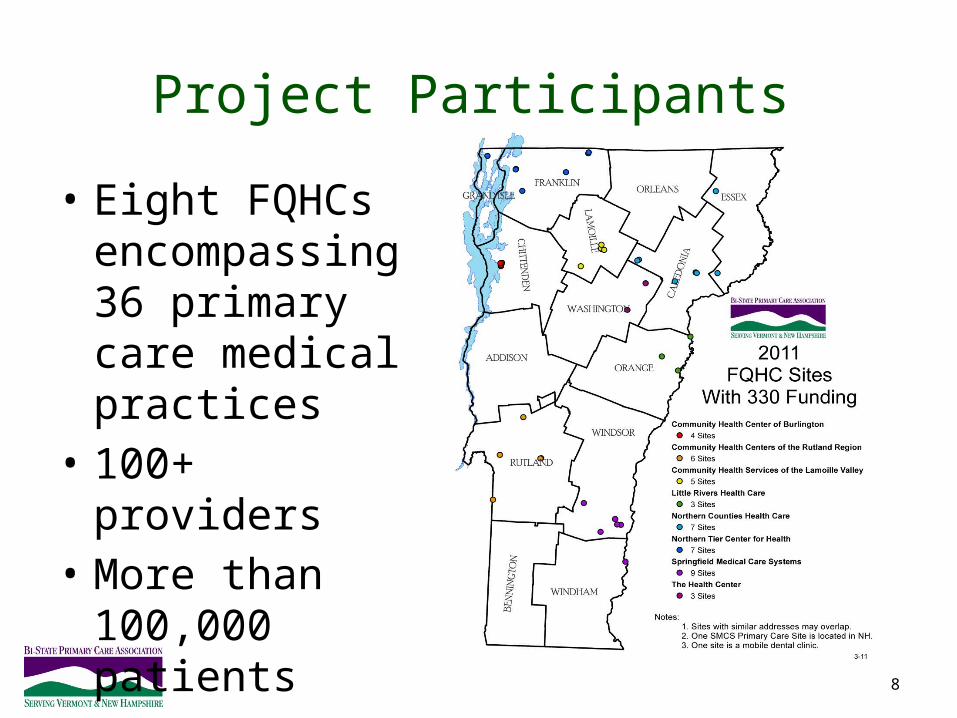
Project Participants
8
• Eight FQHCs encompassing 36 primary care medical practices
• 100+ providers• More than
100,000 patients
Project Funding and Timeline• Project is funded by a $2.2M Health Resources and Services Administration
(HRSA) grant and with over $500K from Vermont’s HIT Fund.• Federal funds are allocated for:
– Data integrity work– Data Feed to the VT Health Information Exchange (VHIE) & Clinical Data Repository
(CDR) - DocSite– Creation of additional DocSite registry reports for UDS clinical data (beyond the
Blueprint) – EHR templates, workflow design and training as needed
• State funds are allocated for Incentive payments to health centers for achieving project goals
• HRSA Grant runs through May 2012.
9
Project Outcomes
– Reporting UDS Data without Chart Pulls
– Blueprint Medical Home Participation
– CMS Meaningful Use Incentive Payments
– Data sharing with hospitals and other health care providers
– Clinical Benchmarking / Network-level QI Activities
10
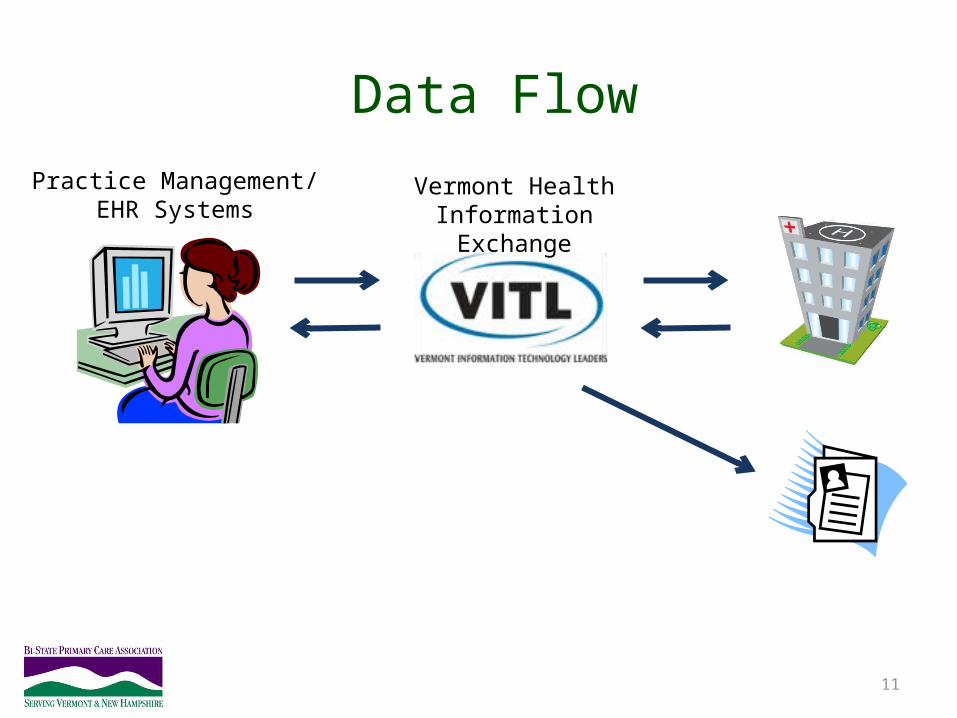
Data Flow
11
Practice Management/EHR Systems
Vermont Health Information Exchange

Who’s On First, What’s on Second…
12
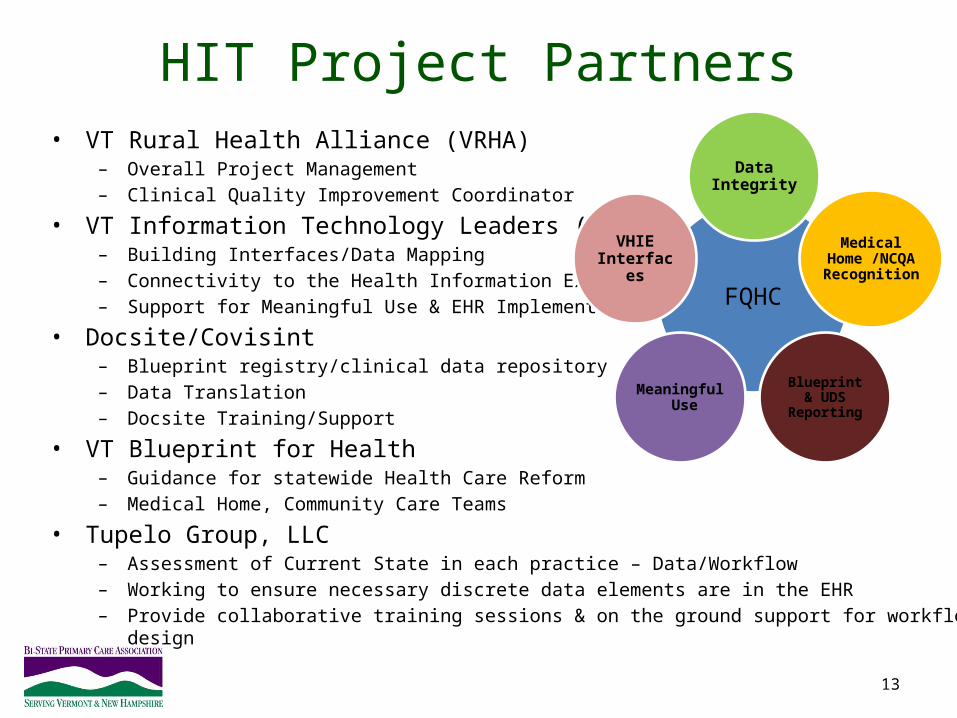
HIT Project Partners• VT Rural Health Alliance (VRHA)
– Overall Project Management– Clinical Quality Improvement Coordinator
• VT Information Technology Leaders (VITL)– Building Interfaces/Data Mapping– Connectivity to the Health Information Exchange– Support for Meaningful Use & EHR Implementation
• Docsite/Covisint– Blueprint registry/clinical data repository– Data Translation– Docsite Training/Support
• VT Blueprint for Health– Guidance for statewide Health Care Reform – Medical Home, Community Care Teams
• Tupelo Group, LLC– Assessment of Current State in each practice – Data/Workflow– Working to ensure necessary discrete data elements are in the EHR– Provide collaborative training sessions & on the ground support for workflow design
13
FQHC
Data Integrity
Medical Home /NCQA Recognition
Blueprint & UDS ReportingMeaningful Use
VHIE Interfaces

On The Ground Activity
14
15
“DATA YOU CAN TRUST ”Data integrity:
• Structured• Reliable• Complete• Reportable
Achieved through: • Collaborative learning• Gap analysis• Workflow redesign• Technology optimization
16
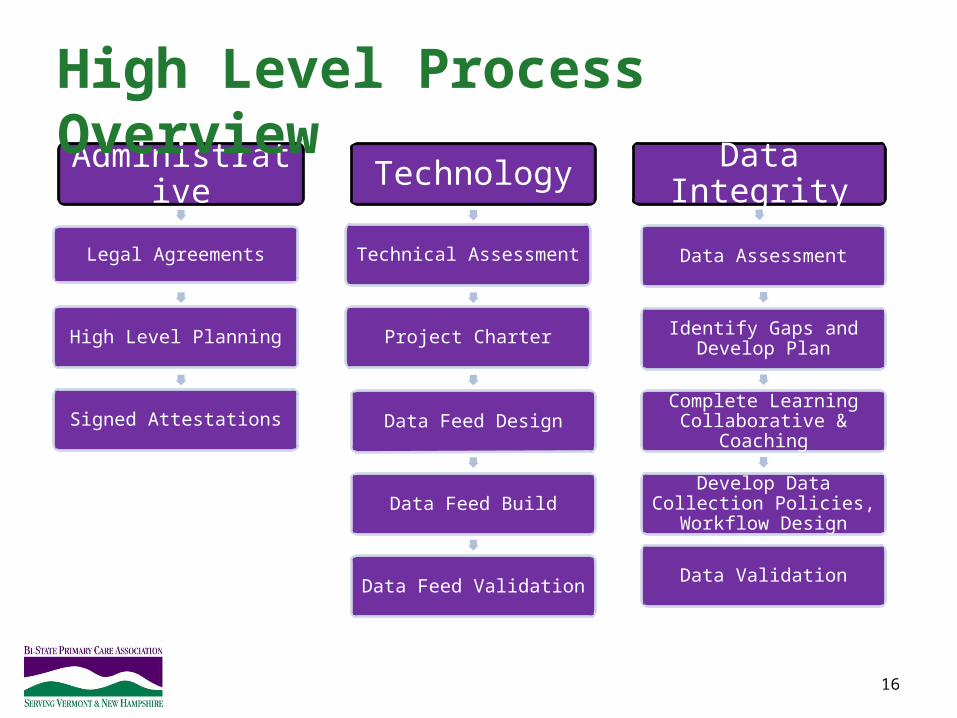
Technology
Technical Assessment
Project Charter
Data Feed Design
Data Feed Build
Data Feed Validation
Administrative
Legal Agreements
High Level Planning
Signed Attestations
Data Integrity
Data Assessment
Identify Gaps and Develop Plan
Complete Learning Collaborative & Coaching
Develop Data Collection Policies, Workflow Design
Data Validation
High Level Process Overview
A Collaborative Approach• 4 Waves
– 2 FQHC organizations in each wave– Interdisciplinary teams from each practice/organization– 4 months of intensive data integrity work
• Focus during 4-month waves– Diabetes– Hypertension– Childhood Immunizations
• Focus through May 2012– Remainder of UDS/Blueprint measures– Clinical Outcomes
17
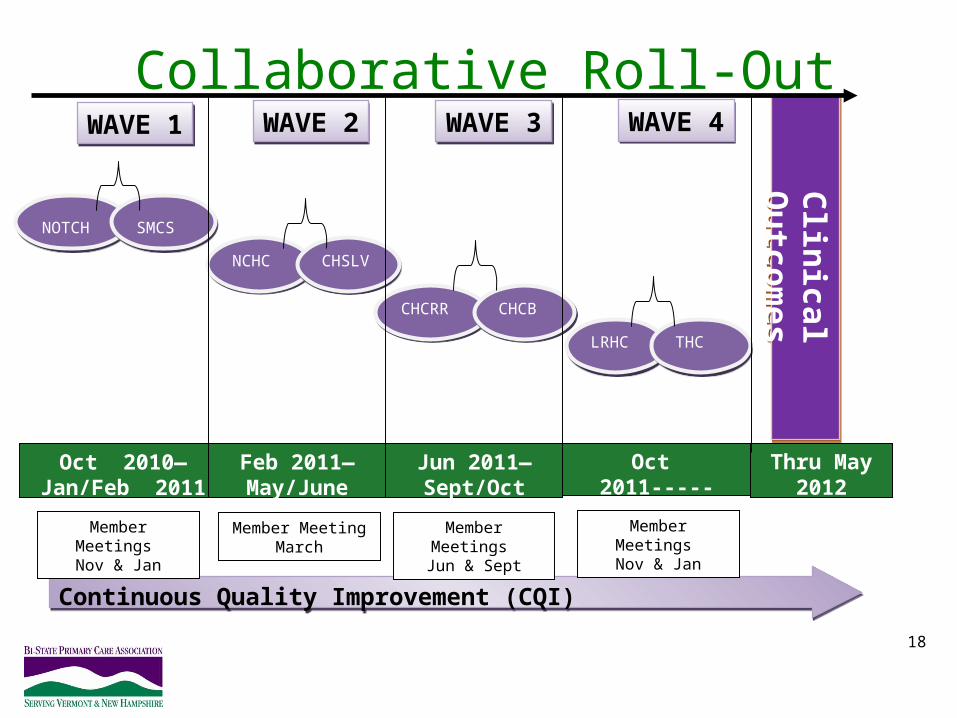
Collaborative Roll-Out
18
Clin
ical Ou
tcom
esC
linical O
utco
mes
NOTCHNOTCH SMCSSMCS
NCHCNCHC CHSLVCHSLV
CHCRRCHCRR CHCBCHCB
LRHCLRHC THCTHC
Oct 2010—Jan/Feb
2011
Feb 2011—May/June 2011
Jun 2011—Sept/Oct 2011
Oct 2011-----Jan/Feb 2012
Continuous Quality Improvement (CQI)Continuous Quality Improvement (CQI)
WAVE 1
WAVE 1
WAVE 4
WAVE 4
WAVE 3
WAVE 3
WAVE 2
WAVE 2
Member Meeting March
Member Meetings Jun & Sept
Member Meetings Nov & Jan
Member Meetings Nov & Jan
Thru May 2012
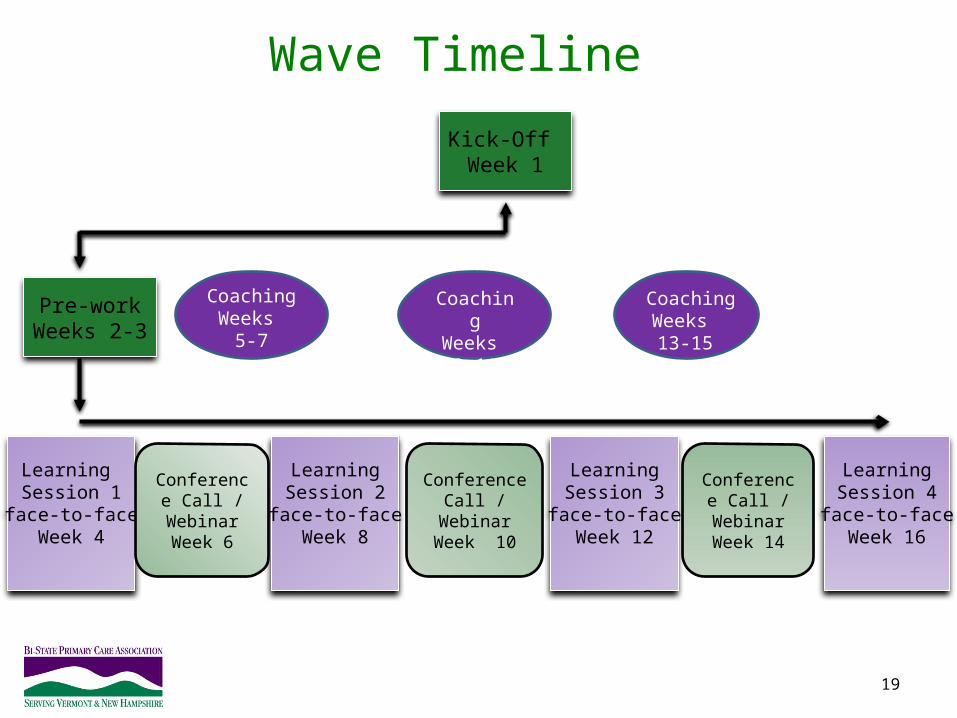
Wave Timeline
19
Learning Session 1
face-to-faceWeek 4
LearningSession 3
face-to-faceWeek 12
LearningSession 2
face-to-faceWeek 8
Kick-Off Week 1
LearningSession 4
face-to-faceWeek 16
CoachingWeeks
9-11
Pre-workWeeks 2-3
Conference Call / Webinar
Week 6
Conference Call / Webinar
Week 10
Conference Call /
WebinarWeek 14
CoachingWeeks 13-15
CoachingWeeks
5-7
Beware: We will not go away when the 4-month
collaborative is over!!!
Assessing the Current State: Data Workbook
Data Workbook• Collaborative Effort from our partners• Purpose of Data Workbook
– An assessment tool for VRHA, VITL, Blueprint and practices– Provides all information about data collection capacity and...– Understand what gaps there may be – Understand where we need to focus our efforts
• Data Elements compiled from:– Vermont Blueprint for Health Data Dictionary for the Chronic Disease Registry (Covisint/DocSite)– NCQA Patient-Centered Medical Home Standards– Federal Register guidelines for Meaningful Use– CMS Physician Quality Reporting Initiative (PQRI)– Uniform Data System Clinical Measures (Added for Federally Qualified Health Centers mandated
reports)• Data Elements are mapped to specific standards as applicable• Multiple Sections (7): Demographics & Scheduling, Core Data Elements, Vital Signs, Prenatal,
Screening Tools, Misc. Data Elements, EHR Elements & Processes
22
23
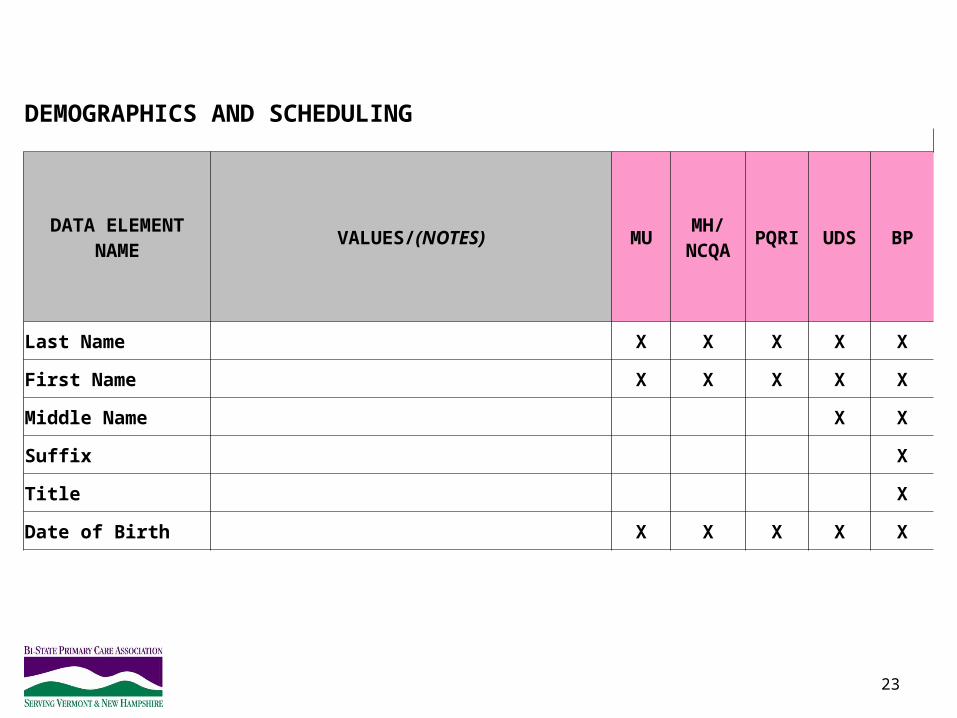
DEMOGRAPHICS AND SCHEDULING
DATA ELEMENT NAME
VALUES/(NOTES) MUMH/
NCQAPQRI UDS BP
Last Name X X X X X
First Name X X X X X
Middle Name X X
Suffix X
Title X
Date of Birth X X X X X
24
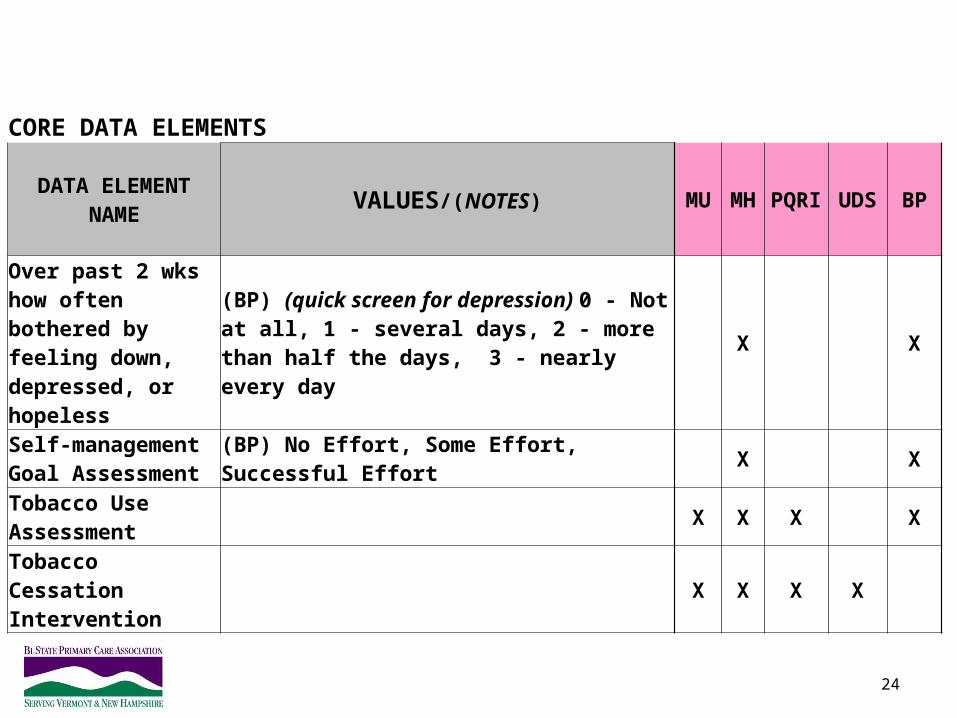
CORE DATA ELEMENTS
DATA ELEMENT NAME VALUES/(NOTES) MU MH PQRI UDS BP
Over past 2 wks how often bothered by feeling down, depressed, or hopeless
(BP) (quick screen for depression) 0 - Not at all, 1 - several days, 2 - more than half the days, 3 - nearly every day
X X
Self-management Goal Assessment
(BP) No Effort, Some Effort, Successful Effort X X
Tobacco Use Assessment X X X X
Tobacco Cessation Intervention X X X X
25
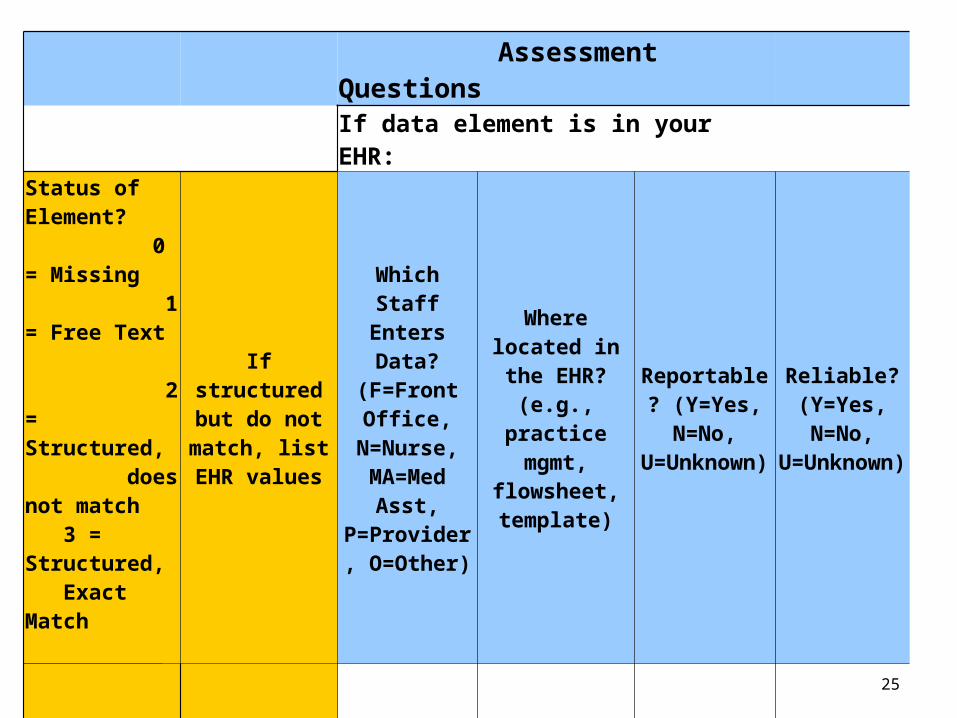
Assessment Questions
If data element is in your EHR:
Status of Element? 0 = Missing 1 = Free Text 2 = Structured, does not match 3 = Structured, Exact Match
If structured but do not match, list
EHR values
Which Staff Enters Data?
(F=Front Office,
N=Nurse, MA=Med
Asst, P=Provider,
O=Other)
Where located in the EHR?
(e.g., practice mgmt,
flowsheet, template)
Reportable? (Y=Yes, N=No,
U=Unknown)
Reliable? (Y=Yes, N=No,
U=Unknown)
Ongoing Activities• Identify gaps & issues we need to address• Determine priorities/possibilities
– Quick wins & easy fixes– New templates, flow sheets, data elements– Workflow redesign– Standardization across the system
• Testing begins in pilot sites (PDSA)• Ongoing coaching & support provided
– Site visits– Webinars & Conference Calls
• Parallel work– Data mapping/translation– Interface build/testing
• Spread changes to additional sites• Develop policies & procedures• Monthly coordinated work plan meetings
26
FQHC
Data Integrity
Medical Home /NCQA Recognition
Blueprint & UDS ReportingMeaningful Use
VHIE Interfaces
27
The first phase of grant incentive payments is underway... four FQHCs are ready to receive funds!
Good News
A Few Lessons Learned…
• Strong clinical champions & leaders among staff• Standardization is key to data integrity• Engage EHR vendors early • Many EHRs are not ready for UDS Reporting• Multiple Activities Underway
– Meaningful Use updates– Medical Home/NCQA Scoring Readiness
• Cart before the horse…• Data translation; time consuming now and into the future• Practices benefit from ongoing training on their EHR’s & report writing
capability• Monthly coordinated work plan calls with partners
28
Challenges and Successes
Challenges• Complexity
– Multiple EHRs– Many players
• Technology Change– VITL HIE Infrastructure
transition
• Evolving reporting requirements and data standards
Successes• FQHC team members
engaged• Forward momentum
maintained • Cooperation from partners
and technology vendors
29

30
Bonnie WalkerTupelo Group, LLC(802)[email protected]
Elise AmesH.I.S. Professionals, LLC(413)[email protected]