Embed Size (px)
Citation preview

What motivates rural men to improve their health status?
A report for the Rural Industries Research and Development Corporation by Dr Samar Aoun and Ms Lyn Johnson
October 2000 RIRDC Publication No 00/157 RIRDC Project No WAC-1A

© 2000 Rural Industries Research and Development Corporation. All rights reserved. ISBN 0 642 58187 8 ISSN 1440-6845 What motivates rural men to improve their health status? Publication No. 00/ Project No. WAC-1A The views expressed and the conclusions reached in this publication are those of the author and not necessarily those of persons consulted. RIRDC shall not be responsible in any way whatsoever to any person who relies in whole or in part on the contents of this report. This publication is copyright. However, RIRDC encourages wide dissemination of its research, providing the Corporation is clearly acknowledged. For any other enquiries concerning reproduction, contact the Publications Manager on phone 02 6272 3186. Researcher Contact Details Dr Samar Aoun WA Centre for Rural Health and Community Development 8th Floor, Bunbury Tower 61 Victoria Street Bunbury WA 6230 Phone: 08 97922520 Fax: 08 97922503: Email: [email protected]:
RIRDC Contact Details Rural Industries Research and Development Corporation Level 1, AMA House 42 Macquarie Street BARTON ACT 2600 PO Box 4776 KINGSTON ACT 2604 Phone: 02 6272 4539 Fax: 02 6272 5877 Email: [email protected]. Website: http://www.rirdc.gov.au Published in October 2000 Printed on environmentally friendly paper by Canprint

iii
Foreword To improve the health of rural men, the relationship of several intertwined factors are explored through this project: the reluctance of men to confront health issues proactively; the role of general practitioners in preventive care and their capacity for education and support for rural men; the appropriateness of the worksite as a venue to facilitate men’s access to advice on health matters; and the application of a health promotion model likely to encourage positive action towards improved health. The present study has been designed to incorporate these components with a focus on a specific health problem which is the fifth major health priority in Australia, diabetes, by bringing an education and screening program to rural industries. For men identified at high risk, referral to a general practitioner provided them with a simple first step they can take towards improving their health status. Twenty seven industries involving 525 men participated in the project in the rural South West of Western Australia. This project demonstrates the feasibility and effectiveness of worksite screening and education programs in motivating at-risk men into seeking further care from their doctor. The study highlights a gap in service provision, namely identifying those at-risk and modifying their behaviour, and suggests a collaborative model of care between industries, the region’s health services and divisions of general practice to address this gap. This report, a new addition to RIRDC’s diverse range of over 600 research publications, forms part of our Human Capital, Communications and Information Systems R&D program which aims to enhance human capital and facilitate innovation in rural industries and communities. Most of our publications are available for viewing, downloading or purchasing online through our website: • downloads at www.rirdc.gov.au/reports/Index.htm • purchases at www.rirdc.gov.au/eshop Peter Core Managing Director Rural Industries Research and Development Corporation

iv
Acknowledgements The authors wish to acknowledge the financial support of RIRDC in funding this project. The project could not have been possible without the full cooperation and valuable contribution of Jenny McDonnell, the Diabetes Nurse Educator at the Bunbury Health Service. All resources used for education and screening have been provided by the Bunbury Health Service. We wish to acknowledge the advice of Professor Rob Donovan from Curtin University and Mr Allan Huggins from Edith Cowan University on men’s health issues and for providing the relevant literature. Finally we would like to thank the industry representatives who facilitated this project on their worksites and for the men who participated and enriched the project with their feedback.
About the WA Centre for Rural Health and Community Development The WA Centre for Rural Health and Community Development is an incorporated non-profit organisation which provides an innovative approach to research, education and training services to enhance the well-being of rural people. It is located in Bunbury, in the South West of Western Australia and it aims • to improve the quality of and access to rural health and community services through conducting
strategic and priority-driven research for the development of outcome-focused services
• to foster intersectoral collaboration through participating in collaborative research projects with the academic institutions, industries and community organisations in order to reduce duplication of initiatives
• to support rural health and community service providers through education and training
• To provide expertise in the design, planning, implementation and evaluation of health programs.

v
Contents
FOREWORD III
CONTENTS V
LIST OF FIGURES vii
LIST OF TABLES vii
EXECUTIVE SUMMARY VIII
1. INTRODUCTION AND BACKGROUND 1
1.1 Diabetes risk factors 1
1.2 The health perspective of rural men 1
1.3 Health promotion by General Practitioners 2
1.4 Workplace health promotion 3
1.5 Models in health promotion 4
2. OBJECTIVES 6
3. METHODOLOGY 7
3.1 Liaison with industries 7
3.2 Phase 1: Education and Screening Program 7
3.3 Phase 2: Follow-up 8
3.4 Phase 3: 8 3.4.1 Focus groups with men 8 3.4.2 Workshop between industries and health professionals 9
3.5 Media Contact 9
4. RESULTS 10
4.1 Description of sample 10 4.1.1 Industries and men 10 4.1.2 Geographic distribution 12
4.2 Phase 1: Education and Screening Program 14 4.2.1 Risk factor assessment 14 4.2.2 Health Service Utilisation 15 4.2.3 Feedback on educational session 16
4.3 Phase 2: Follow-up 18

vi
4.4 Phase 3: Workshop between industries and health professionals 19 4.4.1 Employee perspective 19 4.4.2 Employer perspective 20 4.4.3 Perspective of GPs and other health providers 20 4.4.4 Addressing gaps in service provision 21
4.5 Media Coverage 22
5. DISCUSSION 23
5.1 Effectiveness of Health Intervention for Rural Men 23
5.2 The Extent of Susceptibility 25
5.3 Effectiveness of Workplace Health Intervention 26
5.4 Effectiveness of General Practitioner Intervention 28
5.5 Education and Support Strategies 29
6. IMPLICATIONS 31
7. CONCLUSION AND RECOMMENDATIONS 32
8. COMMUNICATIONS STRATEGY 33
9. REFERENCES 34
10. APPENDICES 37

vii
LIST OF FIGURES Figure 1: Percentage of participants with risk factors 15
LIST OF TABLES Table 1 List of participating organisations by size of organisation 10
Table 2 List of non-participating organisations 11
Table 3 Summary of number of industries and men participating in the project 12
Table 4 Percentage contribution of industries to regional product compared to their percentage representation in this project
12
Table 5 Geographic distribution of industries and their contribution to the sample 13
Table 6 Place of residence of participating men 14
Table 7 Length of residence 14
Table 8 Risk status of men by age 14
Table 9 Comparison of the number of risk factors between men below 40 years (not in target group) and those over 40 years (in target group)
15
Table 10
Reasons for accessing GP services 15
Table 11
Factors inhibiting attendance at GPs 16
Table 12
Percentage of men visiting health service and the timing of the visit 16
Table 13
Benefits of education session 17
Table 14
Results of follow-up 18
Table 15
The extent of motivation for lifestyle change by visit to GP for men high risk
19
Table 16
Intervention mapped against Health Belief Model (all men in study) 23
Table 17
Intervention mapped against the transtheoretical model (men identified at high risk)
24
Table 18
Comparison of the proportions with high blood pressure or overweight several surveys
25

viii
Executive Summary To improve the health of rural men, the relationship of several intertwined factors needed to be explored through this project: the reluctance of men to confront health issues proactively; the role of general practitioners in preventive care and their capacity for education and support for rural men; the appropriateness of the worksite as a venue to facilitate men’s access to advice on health matters; and the application of a health promotion model likely to encourage positive action towards improved health. The present study has been designed to incorporate these components with a focus on a specific health problem which is the fifth major health priority in Australia, diabetes, by bringing an education and screening program to rural industries. For men identified at high risk, referral to a general practitioner provided them with a simple first step they can take towards improving their health status. The study has been conducted in the rural South West of Western Australia in 1999/2000. Twenty seven industries participated (a response rate of 66%) in the education and screening program requiring 29 one-hour sessions, mainly on-site. There was an adequate representation of all sectors of industry such as mineral extraction, processing and manufacturing, agricultural products, processing and services (including farmers and fruit growers), timber and forest products, building and construction. A total of 525 men took part voluntarily in the education and screening sessions, with 446 in the target group of 40-65 years (men outside this age range had specifically asked to attend). The target group consisted of 55% of men in the younger age group (40-49 years) and 45% in the older age group (50-65 years). Industries were at varying stages of being able to adopt this health intervention in terms of their personal, social or financial resources and their awareness of the benefits of such interventions. Hence an essential part of the success of this intervention in the workplace has been the formal and informal communication through multiple levels in industries and understanding how varying systems can be mobilised for health. A third of industries had a health and safety officer and therefore were easier to access than those without. At the other end of the scale, this intervention has reached sectors of industries deemed too difficult to engage and hence which usually miss out on such programs like the farmers and fruit growers. These were reached by taking the program to the regular after hours meetings of their associations or social clubs in agricultural communities. From a men’s health perspective, the workplace seemed to be a well accepted place for health education and screening often the only check-ups for some men over the years. The group setting, involving participants already known to each other, sparked a camaraderie and men did not seem inhibited about sharing information about their risk factors with each other. In general, men were appreciative of the opportunity to participate in such men’s groups at the worksite. Hence worksite screenings are able to attract an otherwise disinterested audience or an audience that seeks permission to engage. The education and the health risk assessment have successfully addressed the components of the Health Belief Model: the perceived susceptibility (risk factors), the perceived severity (consequences of diabetes), the perceived benefits of and barriers to taking action and cues to action. Men were very appreciative of the education provided to them in terms of presentation, content and relevance: 94-100% found the education session interesting, useful and easy to follow; 28% found that most of the information was new to them and 67% found some of it new. Seventy five percent reported that the session had greatly increased their awareness of the consequences of diabetes, 64% have become highly aware of whether they are at risk of developing diabetes and 71% have greatly increased their awareness of what they can do to reduce their risk of getting diabetes. As a consequence, 31% reported that they were greatly motivated and 63% were partly motivated to make changes to their lifestyles as a result of the project and that the screening had served as a wake-up call that one or more aspects of their lifestyle needed attention.

ix
The screening component has revealed that the extent of susceptibility of this group to developing diabetes was significant. In the younger age group, 48% were at high risk (having 2 or more risk factors) and in the older age group, 85% were at risk (with one or more risk factors), with 64% at risk overall (287 men). Of the modifiable risk factors, 62% of men were overweight and 33% had high blood pressure. Of the non-modifiable risk factors, 26% of men had a family history of diabetes and 8% were from a predisposing ethnic background. In addition, 4% of men had a previous borderline high blood sugar test and 6% had a history of heart disease. While all men at high risk were advised to see their GP by giving them a letter of referral, 91% consented to be followed-up and 60% responded to the follow-up survey. Of these respondents, 76% visited their GP who arranged for blood glucose tests as advised in the referral letter. The feedback of men on the results of these tests in the follow-up survey revealed that 2% had undiagnosed diabetes and that 6% had impaired glucose tolerance (IGT) which indicates increased risk of progression to frank diabetes and is associated with cardiovascular risk factors. Other health problems have emerged from these tests: 32% of men discovered they had raised blood pressure and raised cholesterol needing to be medicated, with implications for heart disease. Another measure of the seriousness of these findings is the reasonably high proportion of men (40%) required seeing their doctor mostly within a short time period (2 weeks or 2 months) from initial visit, in order to monitor their risk factors. The strategy adopted has been appropriate in engaging men and then using their personal results to motivate action which is in this case to visit their doctor. The extent to which GP services have been utilised by this group of men in the past year is compatible to that of the general population of men in the area (76%). These visits were mainly due to routine checks initiated by the industry (40%) and the rest were due to symptoms, script renewal, test results or needing medical certificates. This is consistent with the concept that men will not visit a GP or undergo a health check unless they have symptoms, for insurance purposes, part of another visit or if offered at the worksite. Barriers to accessing GPs have not been a major issue for 68% of these men, with “not considering that their problem was serious enough” being the most frequent stated reason for not visiting their doctor (18%). This is related to the lack of knowledge that men have regarding health matters in general and diabetes in particular. Donovan and Egger (2000) have reported that diabetes education is urgently required for this group of men who are not aware of the link of body weight with diabetes and its association with heart disease. The positive response of GPs to this project could be interpreted in the light of their awareness of the need to deliver more of the preventive care to their patients. By identifying patients at-risk, projects like this one provided GPs with an ideal opportunity for health education as men were not presenting with an acute problem. However only 49% of men had lifestyle advice limited to lose weight and exercise more, which left men short of knowing how to take action. The reality of rural practice and its time constraints compounded by a local shortage in the number of GPs and a lack of GP training in lifestyle education and counselling, make this topic more appropriate for other health professionals to undertake. It was interesting to find out that the extent of motivation of men, to change their lifestyle as a result of this project, was not related to whether they visited their GP or not when advised to do so. Whether they were motivated or not, their visit to the GP was strictly to determine the presence or absence of disease. This is consistent with the perception that men do not seek out lifestyle information from a doctor who is seen as a quick fix for acute health problems (Donovan and Egger 2000). The project has been successful in engaging men in the preventive concept of seeking care and getting them to attend their GP to check the extent of their risk. The strategy adopted for this project had a number of strengths namely that the health risk assessment was topic-specific and personalised and it was combined with an educational component and a medical follow-up. Early detection was the main focus of the benefits of the screening thus giving men the opportunity to prevent the disease if they modify their lifestyle behaviour. The findings have however highlighted gaps in service provision in this region for those at-risk of developing diabetes. What is still lacking is ways of halting the progression of the disease as the onset of diabetes precedes actual clinical diagnosis by 4 to 7 years. In the constraints of rural practice and priorities given to those with the disease, the gap in

x
service provision, for both health services and GPs, seems to be at the two ends of the spectrum: identifying those at-risk and modifying their behaviour. In the light of these findings, a workshop between industries, GPs and other health professionals has highlighted the need to establish a lifestyle counselling service as a support strategy for those at-risk. Industries indicated that they would be prepared to sponsor their employees to use the service and GPs would be prepared to refer patients to the service. This service works by moving contemplating men to the stages of action (where behaviour change is initiated) and maintenance (where the change is sustained and predictable health gains are achieved). Men need concrete advice on how to translate knowledge into action in their daily lives. Lifestyle counselling would mainly target weight through nutrition and physical activity as men would be much more willing to do something about their weight because it is visible than about other less obvious risk factors (Egger 2000). In fact dietary modification and increased physical activity can lead to 40%-50% reduction in the rate of progression to diabetes. The program would work as follows: an individualised program for change will be determined between the client and the lifestyle counsellor ie an action plan for weight loss and exercise which is monitored closely at regular intervals through routine follow-up sessions. Regular feedback on progress and health gains would be provided to employers and GPs. This lifestyle counselling service would be expected to be a collaborative venture between industries, the divisions of general practice and health services for it to be sustained on the long-term. As a conclusion, this study has fulfilled its objectives in terms of establishing that this health initiative is appropriate for engaging men in the preventive concept of seeking health care, that is getting them to attend their GP when they only have the risk factors but not the disease. The adopted strategy of screening combined with education on the worksite and conducted in the context of a medical follow-up has dealt successfully with the issues of how and where to intervene in the case of a disease like diabetes which often goes undiagnosed. Once equipped with the knowledge of their risk, the consequences of the disease and what action they need to take to reduce their risk, these men were not reluctant to use the health services, particularly those with a supportive work culture. Hence the majority of these men would be responsive to further support in order to modify their lifestyle behaviour and sustain the change. Since local health services can not offer this support at this stage, it needs to be provided through an innovative venture between industries and health services. It is recommended that: The strategy tested in this project be applied to cover all the workforce in the industries targeted
in order to assess the true extent of undiagnosed diabetes and to reach the less accessible groups such as blue collar workers. The industries need to be committed to organise screening for everyone on site combined with education and a medical follow-up, particularly in the light of the high proportions at-risk.
The GPs instead of the men report on the follow-up test results which would provide a more
accurate and complete picture of morbidity. For this to happen, The Divisions of General Practice need to be actively and collaboratively involved with industries at the planning phase of the project.
Umbrella organisations for farmers and fruit growers and others in the agricultural sector need to
be more actively involved in encouraging their members to participate in education and screening programs.
Strategies be determined to enable the program of education and screening to be taken to
employees whose organisations are not currently well placed to facilitate health initiatives at the workplace, such as those with a small number of employees, no dedicated occupational health and safety personnel, or a mobile work location.

xi
The feasibility of the proposed lifestyle counselling service as a support strategy needs to be explored by stakeholders soon in order to capitalise on the awareness and interest generated by this project. Such long-term interventions have more impact on health related behaviour than the one-off single intervention. For this service to be sustainable, GPs, health services and industries need to collaborate.

1
1. Introduction and Background 1.1 Diabetes risk factors Diabetes is now listed as the fifth major health priority area, an estimated 780,000 Australians having diabetes. Of these, approximately 430,000 have diagnosed diabetes and another 350,000 have undiagnosed diabetes (Colagiuri et al. 1998). While rates of hospitalisation and deaths directly attributed to diabetes are low, diabetes is often mentioned as a contributory cause on death certificates and has a major impact on quality of life. Type 2 diabetes is usually diagnosed in people aged 40 and over and is the most common type of diabetes. The treatment for Type 2 often involves weight reduction, increased exercise and weight modification. However, in more severe cases, insulin or oral medications may be needed. Impaired Glucose Tolerance (IGT) is a precursor to type 2 diabetes and is characterised by glucose levels intermediate between normal values and those diagnostic of diabetes. Type 2 diabetes (and IGT) is an appropriate disease for screening and early detection because it represents a sizeable burden in the population, it can be identified in the preclinical (asymptomatic) phase, and the prognosis may be improved if it is detected and treated early (Engelgau et al 1995). Early detection of diabetes provides opportunities for tertiary prevention of blindness, renal failure, and amputations and for cardiovascular risk factor detection and treatment. The prevalence of undiagnosed diabetes is high and is estimated to represent half the total prevalence of diabetes (Commonwealth Department of Health & Aged Care 1999). The onset of Type 2 diabetes has been reported to occur 9-12 years before clinical diagnosis (Harris et al 1992). Lead time is the period between detection of a disease by screening and ordinary clinical diagnosis. Diabetes detected in asymptomatic individuals through screening, results in a gain in lead time. During this preclinical state, diabetes can be diagnosed and treatment started. The early detection of undiagnosed diabetes is a key intervention point in reducing the personal and community burden of diabetes (WA Diabetes Services Taskforce 1999). The major risk factors or high-risk groups for Type 2 diabetes include a family history of diabetes; obesity i.e. more than 20% over desired body weight; Aboriginal or ethnic origins; age greater than 40; high blood sugar on testing; hypertension; elevated cholesterol level; physical inactivity (Colagiuri et al. 1998; American Diabetes Association 1997). A community diabetes surveillance study should identify individuals who are likely to meet the diagnostic criteria for diabetes. Individuals who have two or more of the above indicators of the disease should be referred for appropriate medical evaluation. Identifying individuals at high risk from diabetes is a focus at both national and state levels. The National Diabetes Strategy 2000-2004 has as its second goal to “prevent or delay the development of Type 2 diabetes” (Commonwealth Department of Health & Aged Care 1999: 8). In Western Australia, formulating clinical goals and targets has identified that each health region should have a diabetes plan and a coordinated mechanism for diabetes prevention and management (Dobson et al. 1994).
1.2 The health perspective of rural men Both national and state levels of government acknowledge the disadvantage faced by rural people in availing themselves of all aspects of diabetes management, from screening to regular assessment and education (WA Diabetes Services Taskforce 1999; Commonwealth State Diabetes Forum 1999), yet the need for such access is apparent. In the rural South West of Western Australia, for example,

2
diabetes is a public health concern, particularly for men. According to a health needs analysis commissioned by the Greater Bunbury Division of General Practice (Aoun and Stone 1997), the local reported prevalence rate of diabetes (5.6%) was nearly double that reported in the State (2.6%). The prevalence of diagnosed diabetes in men compared to women was nearly three times higher. The local needs analysis further highlighted that men were three times more likely than women to use outpatient services in hospitals, possibly as a substitute to attending general practice or as a consequence of waiting until their condition is so critical that they need emergency care. Men’s reluctance to utilise GP services is confirmed in a study by Burkitt (1999), who found that men aged 20-60 years consult general practitioners half as often as women, a number of reasons for this being speculatively advanced. Some are about logistics: that GP facilities are not readily accessible when men are available, nor are delays in a waiting room acceptable unless the inconvenience can be justified by a functional purpose such as acquiring a doctor’s certificate to cover absence. Consultation rates are affected by aspects such as the appointment system used by general practitioners, the proximity of an Accident and Emergency Department seen as an alternative to GP consultation, and a person’s distance from a general practitioner, with rural males having reduced rates of consultation for both serious and trivial conditions (Campbell & Roland 1996: 79). Most reasons for reluctance to visit a GP revolve around the social conditioning of males (Huggins, Somerford & Rouse 1996), especially rural males in whom the male gender role is argued to be particularly strong: that men view seeking help as a sign of weakness and to expose vulnerabilities or to disclose intimacies is inappropriate. When symptoms are manageable, it is preferable to ‘soldier on in silence’; when they become severe, it is acceptable to seek help, especially when ‘pushed’ by one’s partner, but the delay means that males tend to visit the GP for life-threatening conditions for which they are hospitalised (Huggins, Somerford & Rouse 1996: 1.10). Debate about the claim that men delay seeking help for medical conditions (Hartford et al. 1990 in Fletcher 1995: 112) highlights that little is empirically known about men’s views about their health concerns or how they would improve existing health services, with rural men in particular being overlooked (Fletcher 1995). The differing views of men and women towards health were examined in a study of attitudes to coronary heart disease amongst employed people in Ireland. The sample of 74 included groups formed by permutation of three variables: gender, age and occupational group. Men were generally less motivated to change health behaviours than women, older men thinking it was too late and younger men thinking it was too soon. Barriers to change were identified to include aspects like the difficulty of changing routines and lack of personal discipline. Motivation to change was principally undermined by scepticism about apparently contradictory medical advice. Despite this, specific education and clear advice from doctors was sought: ‘More exposure to how bad it [illness] is’; ‘Until you go to a doctor and you’re told that you have high cholesterol or whatever, its only then you’ll have to get down to doing something about it’ (Gabhainn et al. 1999: 624).
1.3 Health promotion by General Practitioners The perception that general practitioners are the most reliable and credible source of health information and advice is commonly held (Oldenburg & Owen 1995) and has been empirically demonstrated. In a study of the importance of information sources for preventive health care in rural Australia, doctors were rated as the most important and chemists as the second most important compared to other sources such as family and friends, field days and media: print-based, television and radio (Humphreys, Rolley & Weinand 1993). Further, there is an expectation on the part of the population in general that lifestyle issues should be discussed as a routine part of medical consultations (Ashenden, Silagy & Weller 1997). What is less clear is whether the general practitioners themselves need to be involved or whether the provision of advice in a practice setting is adequate. Nurse-based lifestyle advice given in a GP setting yielded little change in patient outcomes in one study (Ashenden, Silagy & Weller 1997). Conversely, a lifestyle project undertaken

3
in rural Western Australia in which a dietitian provided lifestyle counselling on referral of a GP in a range of GP practices impacted positively on patients’ risk factors, such as reduced weight, cholesterol and blood sugar (Potter 1999). Despite this, preventive care is argued to be underutilised by general practitioners in the primary care setting (Oldenburg & Owen 1995; Ashenden, Silagy & Weller 1997). Although 80% of all adults in Australia consult a general practitioner annually, with an average of four visits per annum, the average consultation is 10.5 minutes, leaving little time to do other than address the primary health concern and chronic conditions that prompted the visit (Bonevskie, Sanson-Fisher & Campbell 1996: 22, 27). Limited time in consultations coupled with remuneration problems are further compounded by the lack of training provided to medical practitioners in preventive care, such as the counselling and education skills needed to encourage lifestyle modification by patients and the competencies needed in moving from a paternalistic model of determining treatment options to one of shared decision-making between GP and patient ((Oldenburg & Owen 1995: 307; Charles, Whelan & Gafni 1999; Towle & Godolphin 1999). To facilitate behaviour change for patients, general practitioners would need to be informed not only clinically about such matters as causes of and preventive strategies for particular diseases, but also about the individual patient as a person: “about his or her experience of illness, social circumstances, habits and behaviour, attitudes to risk, values and preferences” (Coulter 1999: 719). If the opportunity to undertake health prevention is constrained in the GP setting, particularly for men who visit less frequently, how can males at-risk be accessed with a view to addressing modifiable behaviours that contribute to disease? To meet this challenge, focused workplace health intervention was advocated by Gabhainn et al. (1999) in their study of attitudes to cardiovascular disease. Such a strategy was seen as appropriate for older men (>45 years) who were generally well informed but unlikely to perceive themselves as willing or able to take action, this impaired self-efficacy being exacerbated for blue-collar groups of employees.
1.4 Workplace health promotion Worksites have been identified as a suitable setting in which to conduct health promotion, providing a grouping of people at a single location in which formal and informal communication channels, the latter providing support networks, are usually established (Veitch, Owen, Burns & Salles 1997). In the United States, for example, over 60% of adults can be accessed via worksites, offering the opportunity to raise lifestyle factors with the majority of the adult population and the diversity within that population, with the aim of reducing preventable chronic disease (Emmons et al. 1999). In Australia, health promotion in the workplace is being increasingly embraced and is seen to be most effective when integrated with an occupational health and safety program (Steggall 2000), such change suggesting awareness by senior managers and adoption by the ‘gatekeepers’ of occupational health and safety (Nutbeam & Harris 1998: 57-58). Organisations that are at the forefront of health promotion in the workplace may be regarded in terms of the diffusion of innovation model as innovators and early adopters: respectively, those who are quick to implement a new approach and those who are similarly proactive yet have more community credibility (Nutbeam & Harris 1998: 40). Manufacturing worksites are of particular interest for initiatives in health promotion because they provide access to blue-collar workers, in whom higher levels of multiple risk factors such as excessive weight and elevated blood pressure have been demonstrated, compared to white collar-counterparts (Veitch, Owen, Burns & Salles 1997; Heaney & Goetzel 1997). Bringing a health promotion intervention to the workplace overcomes the recognised difficulty that few high risk individuals voluntarily seek out health improvement services (Pelletier 1999: 341).

4
Despite methodological limitations, research into clinical and cost-effectiveness of worksite health promotion is increasingly favourable, although not conclusive (Heaney & Goetzel 1997: 305). Most promising appear to be initiatives in which participation in health education classes is coupled with individual counselling for high risk employees as determined by physiological measures such as blood pressure, weight and height plus self-assessment of risk behaviours (Heaney & Goetzel 1997; Pelletier 1999). This might be further enhanced by the availability of print material to participants, given the finding that, for general rather than patient populations, adding a pamphlet to an existing intervention may increase the likelihood of desired action being taken (Paul & Redman 1997). Evidence is weak that a single-component intervention such as assessment of health risk alone impacts on health-related behaviours. Conversely, comprehensive approaches undertaken over an extended period of 1- to 2- years are identified as more effective, although it is not clear whether the finding that ‘more is better’ relates to number of strategies employed or number of personal contacts with program staff (Anderson & Staufacker 1996:506; Emmons et al. 1999).
1.5 Models in health promotion Models of change in health behaviour offer some insight into the results of worksite health promotion. Multi-component health interventions conducted over a period of time may accommodate both the stages (when) and processes (how) of change identified in the transtheoretical model (Prochaska & DiClementi 1984 in Nutbeam & Harris 1998). For example, education can raise awareness of health issues and foster recognition of the benefits of change, while individual counselling can help employees to identify barriers to change and to determine an action plan for change, helping employees to move through the different stages of change: precontemplation (no intention to change), contemplation (considering a change), preparation (committing to change), action (making changes) and maintenance (sustaining changes). However, as Greene et al. (1999) caution, the transtheoretical model also incorporates processes of change, so interventions need to be designed which facilitate a shift in decisional balance (pros of change outweighing the cons) and an improvement in self-efficacy: the confidence that one can engage in the desired behaviour. Another model that can account for results in worksite health promotion which involve multiple components such as general education and personalised assessment is the Health Belief Model (Janz & Becker 1984 in Nutbeam & Harris 1998). The Health Belief Model (HBM) is generally acknowledged as both the genesis of a systematic, theory-based approach to research in health behaviour (Brown 1999) and the most frequently cited and researched model (Harrison, Mullen & Green 1992). It comprises four main components, arguably galvanised by a fifth, which may be applied as follows: • Perceived susceptibility: Assisting an individual to recognise their susceptibility to a disease, that
is, their likelihood of experiencing an adverse condition or contracting a given disease, for example by confronting them with the risk factors applicable to that disease.
• Perceived severity: Assisting an individual to understand the seriousness of a particular disease, that is, its likely impact on their circumstances: physical, emotional, relational and financial, for example by alerting them to health problems arising from the disease.
• Perceived benefits of taking action: Providing a forum in which an individual can assess the benefits which should flow from taking action, such as reducing susceptibility to a disease or reducing its impact if contracted.
• Perceived barriers to taking action: Providing a forum in which an individual can determine the impediments to taking action, such as inconvenience, cost, or lack of support, for example, in disruption to family routine.

5
• Cues to action: Providing a discrete, concrete, low-risk first step to initiate action and thus capitalise on the momentum generated by the perceived susceptibility, pursuing the path suggested by the benefits whilst overcoming the barriers.
The model has been criticised for uncertain predictive validity and for a failure of associated research to address systematically the interaction of the four principal dimensions (susceptibility, severity, benefits and barriers), yet the model has not been rejected as an important tool in health behaviour (Harrison, Mullen & Green 1992: 113). It continues to have been applied, for example, in explaining differential consultation rates and the ‘symptom iceberg’ – that not all experience of symptoms translates into a demand for care (Campbell & Roland 1996). The HBM has further been used in conjunction with research about specific diseases, for example as a framework for understanding and predicting adherence to a medical regime amongst diabetic amputees (Pham, Fortin & Thibadeau 1996) and in guiding the development of questions and interviews used to examine the barriers faced by diabetic college students in engaging in appropriate self-care behaviour (Wdowik, Kendall & Harris 1997). To improve the health of rural men, several elements need to be successfully intertwined: the reluctance of men to confront health issues proactively; their ambivalence about consulting general practitioners; the appropriateness of the worksite as a venue to facilitate men’s access to advice on health matters; and the application of a health promotion model likely to encourage positive action towards improved health. The present study has been designed to incorporate these components with a focus on a specific health problem, diabetes, by bringing an education and screening program to rural industries. For men identified at high risk, referral to a general practitioner provides them with a simple first step they can take towards improving their health status.

6
2. Objectives Undertaking a creative health initiative to cater for the special needs of rural men and using
diabetes screening as a mechanism for health promotion
Increasing the understanding of what motivates at-risk but asymptomatic men to seek care from general practitioners
Identifying proportions at-risk and proportions diagnosed with Type 2 or IGT after screening undiagnosed men
Adding to the body of research on the effectiveness of risk factor and symptom assessment as brief health intervention
Suggesting education and support strategies for those identified in the sample as being at-risk, involving workplaces and medical services.

7
3. Methodology
3.1 Liaison with industries This study was conducted in the rural South West of Western Australia in 1999/2000. A list of industries to contact was obtained from the South West Development Commission and a media release was issued describing the project and inviting industries to participate (Appendix 1). A phone call to introduce the project to the manager of the industry was followed by a detailed letter to the Occupational Health and Safety Officer or Health Nurse or another identified contact suggested by the manager of some smaller industries. The letter explained the phases of the project and enlisted the industry participation and support in contacting the men and organising the date and venue for education and screening (Appendix 2). To help with this organisation, a flyer was designed to be attached to the workers’ pay slips or pinned on notice boards, inviting them to attend and to register their response through the tear-off reply section of the flyer (Appendix 3). Posters on the Diffuse Diabetes Campaign were supplied by Diabetes Australia and were sent to advertise the project on the worksites well beforehand. A total of 41 industries/ organisations were contacted. On average, five contact attempts per industry were made (by phone, fax, post or e-mail) to organise the logistics of the sessions. The project was conducted in three phases:
Phase 1: Delivering the Education and Screening Program
Phase 2: Following-up men identified at-risk in phase 1.
Phase 3: Conducting a workshop involving industries and health service providers to explore education and support strategies for prevention of diabetes.
3.2 Phase 1: Education and Screening Program The project coincided with the 1999 Diffuse Diabetes Campaign by Diabetes Australia who provided the latest guidelines on screening and the posters, educational material and pamphlets needed. The program of the educational sessions was tailored to the need of men in the target group 40-65 years. The presentations included information on what is diabetes, who is at-risk, what are the symptoms, what are the long-term problems from diabetes, ways to reduce the risk factors and the healthy lifestyle recommendations. Three questionnaires were completed by participants after they had attended the educational session:
1) The risk assessment test which included a list of symptoms of diabetes, family history, ethnic background, measurement of blood pressure and height and weight by screening staff, waist circumference, history of heart disease or a previous borderline high blood sugar test. 2) The use of health services which included whether men had a regular GP, the last time they visited a GP, Accident and Emergency at the hospital or any other health professional, the reason for their visit, reasons that prevent them from visiting a GP when they have a health problem . 3) Evaluation of the educational program included whether it was interesting, useful, easy to follow, the least and the most useful components, whether it has motivated them to make any changes to their lifestyles and the extent to which it has affected their awareness of the consequences of diabetes, of whether they are at risk of developing diabetes and what they can do to reduce their risk of getting diabetes.

8
The three questionnaires are in Appendix 4. Display boards with posters and educational literature were available for display before each session. A range of handouts was made available to take home on smoking, alcohol, diet and exercise (Appendix 5).
At the end of the screening session, men who were identified to be at risk were given a letter of referral to their GP signed by the diabetes educator (Appendix 6). The letter listed the risk factors found and recommended that the GP do a medical review and a venous plasma glucose test to screen for type 2 diabetes. Men were identified to be at-risk if they were 40-49 years and having scored 2 or more risk factors, or they were 50 years and over with one or more risk factor. The blood pressure was a risk factor if it was greater than 140/90mmHg or is treated with medication. The screening team took weight and height measurements and men checked in which zone their measurements fell in the weight for height chart. They could be in one of four zones: obese or overweight or healthy or underweight. The chart indications were checked against and coincided with the Body Mass Index (overweight having a BMI exceeding 25). The waist circumference measurement was another visual indication of being overweight (100cm or over). In most situations, the waist circumference measurement was compatible with the weight for height chart. Where it conflicted, the waist measurement was taken as an indication of being overweight, as advised by Garry Egger from the Gutbusters program (personal communication).
3.3 Phase 2: Follow-up All GPs in the geographic areas of the project were informed about the project through an individual letter and via the newsletter of the Greater Bunbury Division of General Practice (Appendix 7). Contact lists of GPs were obtained from the two divisions of general practice covering the area of study. To take part in the follow-up phase, men identified at-risk in phase 1 were invited to sign a consent form for the project team to contact them regarding the outcome of their visit to the GP (Appendix 8). The participants were followed-up one-month after the screening session, either by sending them the questionnaire with a reply-paid envelope or by a telephone call. In larger industries, Occupational Health and Safety Officers assisted in distributing and collecting the follow-up forms. For some respondents, up to three contact attempts were needed to complete the follow-up questionnaire on the outcome of the visit to the GP. The follow-up questionnaire collected information on whether the respondent had visited a GP as a result of the screening session, whether a blood glucose test was done, did the result of the test show if diabetes was likely, unlikely or unclear requiring further investigation, what other tests did the GP arrange, whether the GP had provided any healthy lifestyle advice, whether the respondent was asked to attend another appointment and how soon. For those who did not make a visit to a GP, they were asked if they still intended to and if not, to specify a reason (Appendix 9).
3.4 Phase 3: 3.4.1 Focus groups with men This project has coincided with the Healthy Blokes project funded by Healthway, mainly metropolitan based with a small rural component in Bunbury. Focus groups for men 40-60 years old were conducted in April 2000 and documented in a report entitled “Men’s Health Beliefs: A Qualitative Research Report”. The main objectives of the focus groups were to assess men’s understanding/knowledge of the relationship between various risk factors and heart disease, cancer and diabetes; to identify men’s major health concerns, their sources of information and influence with respect to health, their likely participation in community-based meetings and participation in health checks and preventative maintenance. The authors of the report, Donovan and Egger, stated that” Bunbury was chosen because a men’s health project was being undertaken by Dr Samar Aoun, and it was felt that both projects would

9
benefit from the opportunity to exchange information”. While similar focus groups had been planned for this project, it was felt unnecessary to duplicate efforts. Instead, a workshop was added to explore implications for collaboration between industries and health professionals and “where to from here?” The qualitative findings from the focus groups will be discussed in the light of the combination of quantitative and qualitative findings from this project under the section on discussion. 3.4.2 Workshop between industries and health professionals Invitations were sent out (June 2000) to eleven industries with Occupational Health and Safety Officers (mainly the larger industries), a representative of the South West Development Commission, four GPs who represent their colleagues on the executive of the Division of General Practice, the program coordinator of the Division, two diabetes educators, the nutrition coordinator and the physical activity coordinator from the South West Population Health Unit and a fitness expert currently providing a service to one of the major industries (Appendix 10). Each Occupational Health and Safety Officer was asked to invite from their industry one man at-risk who participated in the program. The aims of the workshop were: • To present the preliminary findings on the education and screening sessions and use the findings
as a basis for discussion for the points that follow
• A feedback on the education and screening program from the perspective of the employer (industries) and employees (men who participated)
• To explore issues of how and where to intervene in the case of a disease like diabetes which often goes undiagnosed
• To explore issues of men’s access to and participation in health services as a factor in improving men’s health
• To recommend education and support strategies for those identified at-risk as a collaborative initiative between industries, GPs and other health providers
3.5 Media Contact The project was advertised in the local newspapers, radio and television in its different stages to give updates on its progress, keep the community informed and to encourage men through their workplaces to take part. High profile local personalities were involved to give greater credibility for the target audience.

10
4. Results
4.1 Description of sample 4.1.1 Industries and men Overall 41 industries were contacted of which 27 agreed to participate (66% response rate). These industries had different periods of the year where a training program could not be accommodated depending on the nature of the work (production, processing, farming, agriculture, timber, mining, manufacturing), hence the screening program has spanned a period of nine months (October 1999 to June 2000) to allow time for the special circumstances of each industry. The industries ranged from large, mainly mining industries (workforce over 100) to the medium (30-100) and the small (less than 30). Most of the sessions were conducted on-site. Combined off-site sessions were held for organisations that either did not have a training facility or anticipated only a small number of participants. The larger industries had two or three sessions each. In total, 29 sessions were conducted (Tables 1&2) Table 1: List of participating organisations by size of organisation and by type and date of sessions
Organisation/Industry Size Type of Session(s) Date of session(s)
Millennium Inorganic Chemicals
Large On-site 27/10/1999
WESFI Large On-site x 2 sessions 9/11/1999 Cable Sands Large On-site x 3 sessions 12/11/1999 Vasse Zone Farmers Federation
Small Session during regular meeting
9/12/1999
Agriculture Department of WA
Medium On-site 10/12/1999
Wesfarmers Dalgety Small Session during regular meeting
16/03/2000
Muja Power Station (Western Power)
Large On-site x 2 sessions 17/03/2000
Donnybrook Orchard Improvement Assoc. (fruit growers)
Medium Session during regular meeting (after hours)
20/03/2000
Simcoa Large On-site session 24/03/2000 Australia Post Small Combined off-site
(after hours) 4/04/2000
Bunbury Council Medium Combined off-site (after hours)
4/04/2000
Brunswick Lions Club (mainly farmers)
Small Session during regular meeting (after hours)
18/04/2000
Geographe Enterprises Medium On-site 19/04/2000 Pine Hauliers Medium Combined off-site 19/04/2000 Main Roads Small Combined off-site 19&27/4/00 Meadow Lea Small Combined off-site 27/04/2000 Government Departments/Agencies: • Bunbury District Police
Office
Small Combined off-site 27/04/2000

11
Organisation/Industry Size Type of Session(s) Date of session(s)
• Bush Fire Service • Construction &
Management Services • Ministry for Housing • Ministry for Planning • Ministry of Sport &
Recreation • Valuer-General’s Office • Worksafe Australia Iluka/Westralian Sands Large On-site x 2 sessions 28/04/2000 RCR Tomlinson Medium On-site 4/05/2000 Worsley Alumina Large On-site x 2 sessions 8/05/2000 Bunbury Port Authority Small Combined off-site 10/05/2000 P& O Ports Small Combined off-site 10/05/2000 Conservation & Land Management (CALM)
Medium On-site 10/05/2000
Sons of Gwalia Large On-site 19/05/2000 V & V Walsh Abattoir Small On-site 25/05/2000 Readymix Quarry Medium On-site 9/06/2000 De Vaugh Construction Medium On-site 9/06/2000
Table 2: List of non-participating organisations
Organisation/Industry Dardanup Butchering Company E.G. Greene’s Abattoir Griffin Coal Harvey Zone Farmers’ Federation J & P Construction Malatesta Pacific Western/Collie Power Station Peter’s Dairy Piacentene Earthmovers Sotico (formerly Bunnings) Table Grape Growers’ Association Wespine Industries Wesfarmers Coal Government Departments/Agencies: Ministry of Justice Bunbury District Education Department of Commerce & Trade Department of Environmental Protection Department of Land Administration Department of Transport Family & Children’s Services Fisheries Department Ministry of Fair Trading
Men from each industry were recruited on a voluntary basis. Industry representatives selected a suitable month, day and time that did not interfere greatly with other operations on site and advertised the session accordingly. Appendix 11 is comprised of samples of industry newsletters advertising the project to their workforce. Industry representatives informed the research team of the number of men who registered interest for the sessions, that is in total the anticipated number was 561. However, 6% of men could not make it for the session on the day and so the total number who were educated and screened was 525. Fifteen

12
percent of these men fell outside the target group, ie younger than 40 years or older than 65 years. Some industries requested if their younger men could attend as they expressed an interest, having had a family history of diabetes. The older men were present in the farmers’ and fruit growers’ regular meetings and chose to participate with the others. Therefore the total number of men in the target group (40-65 years) was 446 (Table 3). Table 3: Summary of number of industries and men participating in the project
Characteristic of sample Number Total number of industries contacted 41 Total number of industries participating 27 Total number of sessions conducted 29 Total number of men anticipated to attend 561 Total number of participants educated/screened 525 Total number of men in target group (40-65 years) 446
Every effort was made to involve industries from varied sectors in the South West, mainly the major ones such as mineral extraction, processing and manufacturing, agriculture, timber and forest products and building and construction. Table 4 compares the percent contribution of these industries to the value of regional product (South West Development Commission 1999) with the percent representation of these industries in this project. Table 4: Percentage contribution of industries to regional product compared to their percentage
representation in this project
Industry Group (excluding tourism & retail)
% contribution to value of regional product
% representation in sample
Mineral extraction, processing & manufacturing
51% 44%
Agricultural products, processing & services
21% 26%
Timber & forest products 19% 14% Building & construction 9% 10% Government services - 6%
4.1.2 Geographic distribution Participating industries were spread across the South West. Table 5 presents the geographic distribution of the location of these industries and their contribution to the project sample. Table 6 and appendix 12 present the geographic distribution of men according to their place of residence. Nearly 40% of participating men resided in Bunbury, the regional centre for the South West, followed by the two areas of Greater Bunbury, Australind (18%) and Dardanup (10%). About 60% of men have been resident in their areas for over 10 years, with about 3% as recent residents for less than one year (Table 7). Table 5: Geographic Distribution of industries and their contribution to the sample

13
Organisation Location Number of
men anticipated
Number of participants
Number of men in target group
Millennium Inorganic Chemicals
Australind 34 32 32
WESFI Dardanup 24 23 23 Cable Sands Bunbury 45 45 31 Vasse Zone Farmers Federation
Busselton 21 21 15
Agriculture Department of WA
Bunbury 22 21 20
Wesfarmers Dalgety Boyanup 19 19 10 Muja Power Station Collie 24 20 20 Donnybrook Orchard Improvement Association
Donnybrook 42 42 25
Simcoa Kemerton 20 20 19 Bunbury Council/ Australia Post
Bunbury 19 11 10
Brunswick Lions Club Brunswick 25 23 18 Geographe Enterprises Bunbury 11 8 7 Pine Hauliers Bunbury 13 13 12 Main Roads Bunbury 10 10 10 Meadow Lea Bunbury 5 5 5 Government Agencies/ Departments
Bunbury 16 16 16
Iluka Resources Capel 45 31 28 RCR Bunbury 18 16 15 Worsley Collie 55 59 51 Port Authority/ P&O Ports
Bunbury 14 12 12
Department of Conservation & Land Management
Bunbury 14 21 17
Sons of Gwalia Greenbushes 23 19 16 V&V Walsh Bunbury 10 9 7 Readymix Quarry Gelorup 17 14 14 De Vaugh Construction Bunbury 15 15 13 Total 561 525 446

14
Table 6: Place of residence of participating men
Location Frequency Percentage Bunbury 161 36.5 Australind / Binningup 79 17.9 Dardanup / Eaton 44 10.0 Boyanup / Donnybrook 40 9.1 Capel / Stratham / Gelorup 30 6.8 Busselton / Margaret River 22 5.0 Brunswick / Roelands 21 4.8 Greenbushes / Bridgetown / Manjimup / Nannup / Boyup Brook
20 4.5
Collie 13 2.9 Waroona / Mandurah / Perth 6 1.4 Harvey / Yarloop 5 1.1 Total 441 100 Did not respond to question 5 - Total 446 -
Table 7: Length of residence
Length of residence Frequency Percentage Less than one year 15 3.4 From one to five years 71 16.2 From six to ten years 79 18.1 More than ten years 272 62.2 Total 437 100 Did not respond to question 9 - Total 446 -
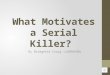
4.2 Phase 1 4.2.1 Risk factor assessment The target group consisted of 55% of men in the younger age group (40-49 years) and 45% in the older age group (50-65 years). In the younger age group, 48% were at high risk and in the older age group, 85% were at risk, with 64% at risk overall (Table 8). Of the modifiable risk factors, 62% of men were overweight and 33% had high blood pressure. Of the non-modifiable risk factors, 26% of men had a family history of diabetes and 8% were from a predisposing ethnic background (Figure 1). In addition, 4% of men had a previous borderline high blood sugar test and 6% had a history of heart disease. One or more symptoms associated with diabetes were reported by 32% of participants. Table 8: Risk status of men by age
Age Group Low risk Number (Percent)
High risk Number (Percent)
Total Number (Percent)
40-49 years 128 (52%) 118 (48%) 246 (55%) 50-65 years 31 (15%) 169 (85%) 200 (45%) Total 159 (36%) 287 (64%) 446 (100%)
Figure 1: % of participants with risk factors
8.31%Ethnic background

15
Twenty-eight participants below the age of 40 years chose to complete the risk factor assessment. It is worth noting that 54% of them were at high risk and were referred to their doctor, with all being overweight (half were obese) and 67% with a family history of diabetes. Nearly half of them had three or more risk factors compared to 19% of those over 40 years (Table 9). Table 9: Comparison of the number of risk factors between men below 40 years (not in target group)
and those over 40 years (in target group)
Total risk factors % Men <40 years % Men 40-65 years One 6.67 34.82 Two 46.67 46.43 Three or more 46.67 18.75
4.2.2 Health Service Utilisation Seventy five percent of men stated that they personally have a regular GP. This percentage increased with the number of years of residence in the area: 47% for those resident for less than a year, 67% for those who have been resident in the area for the last ten years, and 80% for over 10 years. The reasons for accessing GP services are listed in Table 10. The most important reason was a routine check, possibly industry-initiated. It is worth noting that one industry provides a yearly medical check-up (company sponsored test) for its employees and another one provides it every two years. Table 10: Reasons for accessing GP services
Reason for access Percentage Routine check 40 Symptoms or complaints 24 Illness 15 Injury 15 Script renewal 10 Test results 7 Other (e.g. flu vaccine) 7
Total does not add up to 100% due to multiple responses

16
If they knew they had some risk factors for developing diabetes, 99.5% of men indicated that they would visit a GP for further medical care. Further, 68% of men indicated that nothing prevents them from attending a GP. Of those who identified factors inhibiting them from attending a GP, 12% gave multiple reasons. The most frequent factor preventing men from visiting a GP when they have a health problem was that they think their problem is not serious enough (Table 11). Apart from the reasons identified in Table 11, 23 respondents (5%) offered their own comments, relating to difficulty in securing a timely appointment with a GP, dissatisfaction with their experiences with GPs and do not attend unless needing a medical certificate for work purposes. Table 11: Factors inhibiting attendance at GPs
Factors inhibiting attendance Percentage Nothing prevents from visiting GP 68 Problem not serious enough 18 A lot of time waiting 7 Not enough time to attend 6 Surgery times inconvenient 5 Can’t be bothered 3 Cost a problem 2 Other (e.g. difficulty in securing timely appointments)
5
Total does not add up to 100% due to multiple responses The last visit to a GP at a surgery occurred for 76% of men in the past year, for 14% between 1 and 2 years ago and for 8% over 2 years ago (Table 12). Thirty-six percent of men had visited the Accident and Emergency Department at the hospital with over a half having done the visit over 5 years ago, mainly for injury-related reasons. Thirty-four percent had visited a health professional, with 70% of them in the last two years (Table 12). The main reasons for the visit were for an injury, symptoms or complaints or a routine check. The health professionals most frequently visited were the dentist, the chiropractor, the physiotherapist, the optician, the surgeon and the orthopaedic specialist. Table 12: Percentage of men visiting health services and the timing of the visit
Timing of visit GP A&E (Hospital) Other health professional
Less than one year ago 76 7.6 19.7 From one to two years ago 13.7 4.0 4.5 From two to five years ago 6.5 4.9 4.0 More than five years ago 1.3 18.8 5.2 Timing of visit not known 0.4 0.4 0.7 Total 97.9 35.9 33.6
4.2.3 Feedback on educational session All men found the educational session easy to follow, 95% found it interesting and 96% found the information useful. Most of the information was new to 28%, some of it was new to 67% and 5% found none of it new, although respondents in this group offered explanatory comments such as “my wife has type 2 diabetes so I am full bottle on the complications”. The session had greatly increased awareness of the consequences of diabetes for 75% of respondents, of whether they are at risk of developing diabetes for 64% of respondents and of what they can do to reduce their risk of getting diabetes for 71% of respondents. As a consequence, 31% and 63%

17
respectively were greatly or partly motivated to make some changes to their lifestyles as a result of the project (Table 13). Thirty seven percent of those at high risk were greatly motivated compared to 22% of those at low risk (p=0.0005). Table 13: Benefits of education session
Benefit Very much Partly Not at all Increased awareness of • Consequences of diabetes • Personal risk • How to reduce risk
75% 64% 71%
22% 32% 26%
3% 4% 3%
Increased motivation to change lifestyle
31% 63% 6%
The most useful aspects were identified by 65% of men, with two principal themes emerging: the knowledge acquired and the personal application through assessment. In relation to raised awareness about diabetes and its consequences, comments such as the following were typical of what participants saw as most useful: “reaffirming the prevalence and consequences of diabetes”; “fat vs sugar risk explained”; “how the body produces insulin”; “link to other illnesses particularly heart disease”; “narrowing of arteries”; “blood viscosity”; “clear connection with food and lifestyles”; “display of the 2kg of fat”; “diet factors”; “awareness of symptoms”. Respondents also indicated that the opportunity for assessment and exposure to means to reduce risk was most useful too them, reflected in comments such as the following: “finding out I was at risk – some of the factors I wasn’t aware of”; “how susceptible I am with my lifestyle”: “accurate height and weight measurement”; “blood pressure checks”; “practical measurements”; “appreciation of volumes of fat needed to lose”; “reminder to exercise regularly and importance of exercise”; “getting the information to reinforce the action”; “reinforce healthy lifestyle as a timely reminder of what we know we should be doing”; “confirming it is time to act”. The majority responded “nothing” or “all interesting” or “all value adding” to the least useful aspects of the session. Two were disappointed as they thought they would have a blood test done (finger prick) as well in the session. However, most of the participants volunteered further comments, commending the presentation itself and the process applied to men’s health. Typical of the former were comments consistently made such as “excellent”, “very good”, “very useful and informative”, “well presented and concise”, “interesting” and “thanks for taking the time for us”. More reflective of the process were comments such as the following: “great concept”; “should be more of it”; “what a pity that more men did not take up the offer”; “timely presentation as the overall cost to the community needs to be reined in and this sort of information can assist that”; “directed at appropriate level for workforce”; “keep up these classes”; “a very good idea to have several men gathering to hear the same message and possibly helping each other get through any difficulties if and when it occurs”; and “bloody good idea to participate in such a men’s group”. Five respondents sought more information on diet management and the amount of food required for healthier lifestyle; conversely, two found information about diet the least useful part of the presentation. Other comments included the desirability of having more lifestyle information available from GPs, advocating regular check-ups by a GP, considering providing information on other areas relevant to men’s health such as prostate, starting with a younger age group and complementing the information provided with “maybe a motivational element …to help lazy people like myself improve my lifestyle”.

18
4.3 Phase 2: Follow-up Of the 446 men in the target group, 287 of the sample (64%) were identified as being at high risk from type II diabetes and were advised to visit their GP. Of these, 261 (91%) were given a letter of referral to the GP from the diabetes educator and consented to be followed-up. The remaining 9% included four participants who indicated they were already diagnosed as diabetic, a further four who did not accept the referral letter since they had recently seen their GP and 18 who did not sign the consent for follow-up form. Responses to the follow-up surveys, results of which are summarised in Table 14, were received from 60% of the men who had consented to follow-up. Of these, 76% had visited their GP, representing 46% of all those referred. As suggested in the referral letter, 87% of men visiting their GP had a blood glucose test and a further 5% had had a blood glucose test within the previous 12 months. For the remaining 8%, the GP did not see the need for such a test. As a result of the blood test, 2% of men discovered they had diabetes and 6% had raised IGT levels. For 85% of respondents, one or more tests apart from the blood glucose test were conducted: cholesterol and triglycerides (lipid profile), blood pressure, kidney function and prostate. Problematic test results were reported by 32%. For example, 27% had raised blood pressure, with a further 10% having raised blood pressure resulting in medication being prescribed or increased; 20% had raised cholesterol levels and 17% had problematic prostate test results. As a result, 40% of men who visited their GP were asked to attend for another appointment; of these, 13% were asked to come back within two weeks, 53% within one-two months, 25% within six months and 9% within a year. Table 14: Results of Follow-up
Aspects of Follow-Up Frequency % Men identified as at high risk 287 100 High risk men accepting referral to GP and consenting to follow-up
261 (out of 287) 91
Men responding to follow-up survey 158 (out of 261) 60 Men who have visited GP (out of those responding) 120 (out of 158) 76 Men who have visited GP (out of those referred) 120 (out of 261) 46 Men sent for blood glucose test 104 (out of 120) 87 Men with diabetes 2 (out of 104) 2 Men with raised IGT levels 6 (out of 104) 6 Men given tests other than blood glucose test 102 (out of 120) 85 Problematic other tests, e.g.: Raised blood pressure Raised cholesterol Enlarged prostate
33 (out of 102) 22 (out of 59) 16 (out of 79) 2 (out of 12)
32 37 20 17
Another appointment required Within two weeks Within one-two months Within six months Within one year
48 (out of 120) 6 (out of 48) 25 (out of 48) 12 (out of 48) 4 (out of 48)
40 13 53 25
9 GP was informed about the project 80 (out of 120) 76 GP gave lifestyle advice 57 (out of 120) 49
Of those visiting their GP with the referral letter, 76% reported that the GP was informed about the project and 49% were given lifestyle advice by the GP. The majority of respondents indicated that the advice they had been given was limited to one or more general comments like increasing

19
exercise, reducing alcohol intake, quitting smoking, controlling weight and adopting a low fat diet. Some 20% were given more specific information, either explanations or suggestions for action: “discussed diet”; “explained three components making up cholesterol and what effect diet and exercise had on these components”; “lose about 5kg”; “see a dietitian to modify diet and lose weight”; “HeartSmart program”. Of the 24% of respondents to the survey who have not visited their GP, 7% intend to make an appointment and a further 5% intend to discuss the results of the screening at their regular GP visits, for example “I will go when I am due for a prescription” and “I go to doctor once a year because of strong history of diabetes in family”. The remaining 12% have indicated they will not visit their GP, either because they have visited their GP shortly prior to the screening (3%) or for reasons such as the following: “I am too busy at present”; “I am not concerned about risk as it is only weight”; “I have modified my diet”; “I was only just overweight and I am attending gym classes and have lost the weight”. The extent to which men were motivated to make changes to their lifestyles is independent of whether they make a visit to the GP or not. As indicated in Table 15, similar proportions of those highly and partly motivated have visited the GP (46% and 42% respectively), while 86% of those stating not to be motivated at all have visited their GP. Of the six men who were not motivated but visited GP, three had symptoms associated with diabetes, five were aged 50 or over and five had either one or two other risk factors. The remaining unmotivated person who has not visited the GP had the most risk factors of this group: three, and was aged over 50 which is an additional risk factor. Table 15 : The extent of motivation for lifestyle change by visit to GP for men at high risk
Extent of motivation for lifestyle change
Visited GP Number Percent
Did not visit GP Number Percent
Total Referred Number Percent
Very much 41 (46%) 49 (54%) 90 100% Partly 63 (42%) 86 (58%) 149 100% Not at all 6 (86%) 1 (14%) 7 100% Not known 10 (67%) 5 (33%) 15 100% Total 120 (46%) 141 (54%) 261 100%
4.4 Phase 3: Workshop between industries and health professionals The workshop was attended by 16 participants: three representatives from the local Division of General Practitioners, four other health professionals (two diabetes educators, one dietitian and one physical activity consultant), seven industry representatives and three ‘at risk’ employees, one of whom was also an industry representative. The workshop started with a presentation of the preliminary findings as a basis for discussion, in which the following points emerged. 4.4.1 Employee perspective Employees indicated that they had found the screening and education very valuable. Being conducted at the worksite or having attendance otherwise facilitated by the employer meant that men, who would not usually seek out information about specific diseases like diabetes, were exposed to such information in a convenient way. They appreciated the personal application which was emphasised by the accompanying screening. The group setting, involving participants already known to each other, sparked a camaraderie and almost competition about risk factors that facilitated discussion in areas of men’s health usually

20
regarded as ‘taboo’. For some, the screening served as a ‘wake up call’ that one or more aspects of their lifestyle needed attention. 4.4.2 Employer perspective Employer representatives also indicated that they had found the screening and education session very useful, complementing the ongoing attempts of their industries to raise awareness of lifestyle issues such as weight management and exercise in order to improve the health of employees. Concern was expressed that the voluntary nature of the program meant that employees most in need of the information and screening opportunity may not attend. However, industries would be interested to conduct the same program on a regular basis to reach more of their workforce. Industry programs were identified as encompassing a range of activities, with some industries having one or more of the following activities and others having none: paying for an annual check-up by a GP for employees
conducting clinical assessments by occupational health nurses and having these results available
for discussion by a GP, brought on-site for individual contact with employees
providing one training day every two months
facilitating lifestyle change by having fitness equipment and the services of an exercise physiologist available on-site, as an adjunct to workplace rehabilitation strategies. The exercise physiologist cautioned from sponsoring men to join community gyms for the first time without expert supervision. This has caused more harm than good to some men particularly those over 50 years.
It was acknowledged that such strategies, pursued consistently and in an integrated manner, were designed over time to increase staff awareness of and propensity to act on health issues, with results being monitored in subsequent screenings/activities. Modest gains, sustained and improved progressively, were anticipated rather than major change as a result of a one-off intervention. A challenge recognised by industry representatives was that of striking the balance between facilitating employee health yet minimising the situation in which the individual employee shifts responsibility for their health from themselves to their employer or elsewhere such as to their GP or their partner. A further challenge identified was that of managing the links between the potential stakeholders in an individual’s health, for example their partner, their GP and other health professionals such as dietitians, in a way which best facilitates action by the employee at a key, opportune time. 4.4.3 Perspective of GPs and other health providers General Practitioners were positive about the diabetes screening and education program, viewing the initiative as one that encouraged men, who would otherwise not do so, to visit the GP for a medical check-up. Having the patient bring with him the screening results has saved the GP’s time and hence time was better spent on health education. Workshop participants viewed the GPs as a credible source of information and the GPs themselves were keen to retain overall case management of their patients. It was acknowledged, however, that time and resource constraints meant that, when confronted by patients at risk from disease rather than currently suffering disease, lifestyle advice was limited to what should be done (‘lose weight’, ‘exercise more’) rather than how this should be undertaken. It was recognised that ongoing follow-up was desirable but the onus was left to individual patients to make another appointment at the time recommended during the initial consultation with the doctor. However, when patients did re-visit the GP, it was often triggered by a specific complaint, with the

21
result that ongoing follow-up of general risk factors was overlooked in the face of a more pressing immediate matter. Further, given the perceived shortage of GPs in the area and thus the difficulty of scheduling appointments for ‘sick’ patients, there was reluctance to use a practice-initiated recall system, which might overtax the availability of appointment times. As one GP put it “there is no more doctor time available in Bunbury” and “in general GPs are not skilled at giving dietary advice” and other health professionals need to take on this role. However it is hard to get access to dietary advice from other health professionals. Dietitians and other health professionals at the Bunbury Health Service agreed they had waiting lists for patients already with the disease whose priority for lifestyle counselling is higher than the at-risk people. The ideal situation for GPs is to have a practice nurse, located at the GP’s surgery, with access to a database identifying an individual’s age and risk factors for a range of diseases. Thus GPs can keep in touch with what is happening to their patients. The practice nurse could take the time needed to provide adequate lifestyle counselling, capitalising if necessary on programs already available locally such as HeartSmart and more generally such as Gutbusters. 4.4.4 Addressing gaps in service provision It was agreed that the principal gap in service provision is in the management of men at high risk from, but yet to contract, diabetes. These men were identified through screening and were referred to their GPs, who arranged tests to determine whether they currently have the disease. For men who did not have the disease, little was offered by GPs in the way of lifestyle counselling, nor were these men qualified to access established services such as those offered by the diabetes nurse educator, other than in the education session conducted with the initial screening. It was considered that men would be reluctant to pay for private services, such as from a nutritionist. The question begging was what next? How do we keep these men motivated to modify their behaviour in order to reduce their risk of future onset of diabetes? The provision of a lifestyle counselling service was suggested as a strategy to address the service gap. A structured group program, conducted (during or after hours) over a period of weeks by health professionals with expertise in the relevant areas, was suggested as a means to raise and discuss issues of lifestyle change such as exercise and weight control, consistently reinforcing and progressively monitoring such aspects amongst participants. The program was envisaged as being conducted in a similar vein to employee assistance programs; that is, able to be utilised by employees and their partners on a voluntary basis but sponsored by the employer, which would meet the cost of aspects such as venue hire and payment to health professionals delivering the program. A neutral venue was preferred, rather than a location such as the hospital, which was seen to reinforce a ‘sickness’ rather than ‘wellness’ model. One example of how this could work by involving GPs and workplaces would be to have a pre-printed, carbonised form available, on which results for clinical screening conducted at the worksite could be recorded, a copy to be retained by the employer, a second for retention by the employee and a third for transmission to the GP. The form could also include checklists for potential action such as goals to be set, for example reduction in waist circumference by x centimetres over y weeks, and referral sources such as local programs and specialist health providers, to act as a stimulus for discussion between the GP and the patient. To demonstrate the efficacy of the program to sponsoring employers, aggregated data (rather than that for individual employees) would be provided to employers, indicating the number of participants from their organisation and the progress achieved in lifestyle change. However as a precursor to this initiative, industry representatives strongly recommended that the findings from the current study be presented to the higher levels of their management.

22
As a conclusion, should a community-based lifestyle counselling be established to fill the gap in service provision, GPs would be prepared to refer patients to the service and industries would be prepared to sponsor their employees to use the service.
4.5 Media Coverage The community was kept informed about the progress of the project through local newspapers (South West Times, Bunbury Mail), ABC radio, and Golden West Network television news (Appendix 13). In each of these items, role models and community leaders were selected to help accelerate the rate of adoption of this intervention by other men in the community. For example, Ron Fenn , one of the screened men, was in a newspaper article having lost thirty kg since he was identified as being at high risk of developing diabetes. Some of his comments in the paper were “ the screening and the visit to the doctor really brought it home to me about how close I was to trouble”, “now I know the scale of the problem”, after losing weight “I have a lot more energy now, I’m not as agro and I’m definitely happier in life”, “it’s funny, I don’t miss it at all- you don’t notice there’s no butter in your sandwich, it’s all in your head”. The article was a real success in the community judging by the positive feedback from lay people and health professionals. Men in the community could identify with Mr Fenn as the article was more of a testimonial of a typical men who has tried for years to lose weight and change his diet and has finally succeeded. The Mayor of the City of Bunbury and the Bunbury Police Superintendent were two prominent local personalities who participated in the screening and education session and were shown on TV news being tested for their risk factors. In his weekly write-up in Bunbury Mail, the Mayor reported that the session was a good opportunity for him to take stock. He found the screening session very informative and “would strongly recommend that men in the susceptible over 40 category make the effort to attend the screening both as a check-up and an education forum about diabetes and other health issues".

23
5. Discussion This project is about establishing if the adopted education and screening strategy for diabetes prevention has motivated men to visit their GP in order to establish the presence or absence of disease and to monitor risk factors. This can be explained in the light of three models of health promotion whose applications in this project are intertwined: the health belief model, the transtheoretical model and the diffusion of innovation theory.
5.1 Effectiveness of Health Intervention for Rural Men The Health Belief Model explained the factors contributing to increased motivation as summarised in the framework below. Table 16: Intervention mapped against Health Belief Model (for all men in study)
Component Application in Intervention Susceptibility/awareness of risk increased greatly for 64% of men “Finding out I was at-risk-some
of the factors I wasn’t aware of”
“how susceptible I am with my lifestyle”
Education: in a group session, informing participants about risk-factors
Screening: - Self-assessment of risk factors such as
family history using a questionnaire - Objective individual assessment of
physiological measures of risk such as blood pressure and weight
Severity/awareness of consequences increased greatly for 75% of men “Now I know two things that
make you go blind” “the consequences of doing
nothing about it”
Education: in a group session, informing participants about potential consequences of the disease
Benefits/awareness of reducing risk increased greatly for 71% of men “diet and exercise- getting information to reinforce action”
Education: • In a group session, informing participants
about options to reduce risk via lifestyle changes such as in diet and exercise.
• After the session, having print material available such as brochures on healthy eating for participants to take if desired.
Barriers/impeding change Regarding lifestyle “I love beer and meat” “I am too busy” Regarding GP access “delays in securing appointments
Discussion: • In group education session, providing
opportunity for discussion about impediments to change
• For individuals identified at high risk, interacting informally on one to one basis with Diabetes Educator during discussion of results of risk factor questionnaire
Cues to action • Acknowledgement of awareness &

24
Component Application in Intervention 31% of all men were highly motivated to change lifestyle and 63% were partly motivated “the session has confirmed it’s time to act and do not wait for the day” “timely reminder of what we know we should be doing”
commitment: In survey evaluating education session, asking participants to indicate to what extent they had learned something and were motivated to make lifestyle changes.
• Referral: Giving individuals at high risk of contracting the disease a letter of referral to GP requesting further investigation.
• Anticipation of follow-up: Informing participants given a letter of referral that, with their consent, they would be contacted about the outcome of their GP visit.
This intervention can also be mapped against the transtheoretical model which puts men at varying stages of motivation or readiness to change. Table 17: Intervention mapped against the transtheoretical model (men identified at high risk) Stages of change In terms of Visit to GP In terms of Lifestyle change Pre-contemplation 287 men at high risk were
advised to visit GP 287 aware of the need for a lifestyle change
Contemplation 158 men responding to follow-up survey
149 reported to be partly motivated
Determination or preparation 120 actually visiting GP 90 reported to be highly motivated
Action Action taken by GP (To be explored later in report) Maintenance (follow-up) 48 men needed a follow-up by
GP (To be explored later in report)
As presented in Table 17, men who participated in this project were moved from the pre-contemplation stage to contemplation to preparation stage at different levels. The study fulfilled its brief in terms of the visit to GP but stopped short of the action stage where behaviour change is initiated. How this can be achieved is discussed later on in the report under education and support strategies. According to Donovan and Egger (2000), there is a clear association between interest/action and problems in the immediate social circle of men which can move them from pre-contemplation direct to action. Factors are “death of a friend or work acquaintance, personal health scare, constant pushing by partner or GP, age at death of father and type of death”. For instance in this project, although younger men were not targeted, they chose to participate on the basis that they had a family history of diabetes (67% of them compared to 26% in the total sample) or they knew an acquaintance with the complications of diabetes. The strategy adopted for the project had a number of strengths worth replicating in similar studies aiming to motivate men to improve their health status. Furthermore, this strategy has been supported by the findings of the focus groups conducted by Donovan and Egger (2000). The health risk assessment was combined with an educational component and a medical follow-
up. This is in line with Becker and Janz’s suggestion (1987) that health risk assessments are

25
unlikely to have a sustained influence on behaviour unless conducted in the context of an ongoing medical care relationship (follow-up by a doctor in this project) and within a supportive educational process (by diabetes educator in this project).
The second strength of this project is that it was topic-specific. Donovan and Egger (2000) recommended that programs targeted towards men need to be topic-specific as general health checks would be less likely to attract compliance.
If clients are self-selecting (as is the case in this project), this may lead to those who are at risk less likely to attend (Schoenbach, Wagner and Beery 1987). However the third strength of this project is that diabetes knowledge is lacking among this group of men, compared to their knowledge of cardiovascular disease. Therefore while men have self-selected for the health checks, their ignorance of the risk factors did not deter them from attending. Donovan and Egger (2000) reported that diabetes education is urgently required for this group of men who are not aware of the link of body weight with diabetes and that diabetes is a major health problem for men in Australia and it is associated with heart disease. Therefore their superficial understanding of the links, prior to the project, was not sufficient for them to take action.
The fourth strength of this project is that the education session was based on an understanding of the characteristics of the audience in order to target the knowledge, understanding, beliefs and skills of this group of men. In addition, the education and screening were delivered by a credible scientific team. As Donovan and Egger (2000) reported, men respond to scientific facts and concrete rather than abstract concepts. In this project, the following were greatly appreciated: visual 2.3kg fat model, viscosity of blood model, plastic model of blocked artery, accurate height/weight measurements.
A fifth strength is that health information was personalised. Men were personally engaged in measuring and documenting their risk factors and comparing them to benchmark measurements, hence acquiring a sense of the extent of their risk. Early detection was the main focus of the benefits of screening thus giving men the opportunity to prevent the disease if they modify their lifestyle behaviour. The strategy adopted in this project has been acknowledged as an appropriate one to engage men and then use the results to motivate action (Donovan and Egger 2000).
5.2 The Extent of Susceptibility To assess the extent of susceptibility of this group of men, the physiological risk factors obtained in this project, high blood pressure and overweight, are compared with the following surveys for men 25-64 years in Table 18. Table 18: A comparison of the proportions with high blood pressure or overweight in several surveys
Surveys High Blood Pressure Overweight National Heart Foundation Survey (1980)* 26.7 47.6 National Heart Foundation Survey (1983)* 22.4 48.2 National Heart Foundation Survey (1989)* 18.8 51.5 National Nutrition Survey (1995)* 16.7 66.3 This Men’s Health Project (2000) 33.0 62.0
*Source: Australian Institute of Health and Welfare (2000) As this project has targeted older men than previous surveys (over 40), it is expected to include greater proportions of men with higher blood pressure and more overweight. However, the difference in blood pressure is also due to the lower threshold of 140/90 mmHg adopted in this study, compared to 160/95mmHg in all the other mentioned surveys in Table 18. With respect to weight, the determinants for overweight were the same in this project and the other surveys. However, while the trends showed an increase with time from 1980 to 1995, it is surprising that in the latest survey where

26
younger men were included, the proportions overweight (66.3%) were even higher than those in this project (62.0%). This is somehow echoed in this project, when risk factors for men younger than forty were analysed separately. All of these younger men were overweight and obviously they were interested to participate because they were concerned as 67% of them had a family history of diabetes. On the one hand, this raises the issue that such education and screening programs need to target men younger than forty as negative behaviours set in much earlier. On the other hand, Donovan and Egger (2000) recommended for health interventions to be age-sensitive as men are more receptive to health messages once they reach forty or fifty, for instance “turning forty is a major factor for men in reassessing their health and fitness, they come to realise that life is not all beer and skittles and that they are not bullet proof”. At 50, a defining turning point in life, men start feeling the significant physical effects of ageing. The screening process has detected that 2% of men at-risk who had a blood test done had developed diabetes and did not know they had it. A further 6% had raised IGT level which indicates increased risk of progression to frank diabetes and is associated with cardiovascular risk factors. It is worth noting that not all men who were advised to see their doctor actually did (46% did) and not all men who went to their GP had a blood test done (87% did). Because of the voluntary nature of participation, the rate of undiagnosed diabetes is not as high as anticipated. Some of the reasons could be: men who had undiagnosed diabetes with obvious symptoms have not probably participated. One
example is that of a man referred to the diabetes educator by his GP two months after his industry participated in the screening. Apparently, he deliberately did not attend the session at his worksite because he suspected he had diabetes. His risk was further confirmed to him by his workmates who were discussing what they have learned from the session so he decided to see his GP. His attitude is one of not wanting to know the bad news (denial).
another reason for not reporting back positive results could be related to that the identification of diabetes could influence insurance and even employment prospects. One man was concerned if his industry would be privy to the screening results.
It is likely that diabetes would have been diagnosed among the 40% who did not respond to the survey. Having the GPs instead of the men report on the follow-up results would have given a more accurate and complete picture. However this project was aiming to engage men in terms of them seeking and understanding the results of their tests.
The follow-up period needs to be extended beyond one month as it was not long enough for some men to make an appointment (which might be in two weeks time), visit GP, have blood test done and go back to GP to discuss the results of the test. As a result, some of those screened in the last two months of the project, have not been able to fulfil the follow-up component within the duration of the project.
This project has highlighted other health problems: 32% of men discovered they had raised blood pressure needing to be medicated and raised cholesterol with implications for heart disease. Another measure of the seriousness of these findings is the reasonably high proportion of men (40%) required seeing their doctor mostly within a short time period (2 weeks or 2 months).
5.3 Effectiveness of Workplace Health Intervention An essential part of the success of health intervention in the workplace was the liaison with industries. An extensive amount of time and energy was invested in applying the “diffusion of

27
innovation theory” that is the process by which an innovation (such as this project) is communicated through multiple channels and levels in industries both formal and informal. The Centre has successfully acted as the “agent of change” who facilitated the adoption of this innovation/change by industries. This has been achieved by an understanding of how varying structures and systems can be mobilised for health in this rural community. An insight as to why some industries participated and some did not, is explained by the diffusion of innovation theory (Nutbeam and Harris 1998). Industries who were contacted for this project were at different stages of being able to adopt this innovation: they fell broadly into Early Adopters 24% (have some of the personal, social or financial resources to adopt the innovation), Early Majority 24% (amenable to change and have become persuaded of the benefit of adopting the innovation), Late Majority 29% (reluctant to adopt until benefits are clearly established) and Laggards 23% (resistant to the introduction of new ideas). In general, this classification has been guided by the number of contacts needed for the industry to participate (ranging between 2 to 9 contacts) and the length of time required for adoption to take place (ranging from 1 to 6 months). Hence there was a need to collect data for most of the period this project spanned particularly when most industries would only release a small proportion of their men to attend. The main concern of most industries was the loss in production if a group of men stopped work for an hour to attend the educational/screening session. This necessitated the contact of a larger number of industries (than initially anticipated) in order to reach the target sample of approximately 500 men for this study. By consequence, the period for follow-ups had to be extended till the report writing stage. Industries were encouraged to fit the session during working hours in order to boost the response rate. It was noticeable that the response rate was lower in industries that opted to arrange for the sessions to be after-hours. However, for groups like farmers, fruit growers and others in the agriculture industry, wider attendance was secured through fitting the session within their regular after-hours meetings. Therefore in retrospect, a longer time period to undertake this project would have been more adequate to take in consideration the different needs of industries, particularly as this innovation was a first for the majority of participating industries, particularly the smaller ones. However, this innovation has reached sectors of industries deemed too difficult to engage and hence have missed out on other health promotion programs. For instance, the farmers and the fruit growers were reached through their associations or social clubs (eg the Lion’s club) for the education and screening session and were the hardest to follow-up. The Early Adopters and some of the Early Majority are those industries who had a well established health and safety program and hence either had an occupational health and safety officer or a health nurse who assisted in the screening on their sites and in the return of the follow-up surveys. Some industries were interested to participate but had a workforce younger than 40 and therefore were not included in the above mentioned classification. In discussing the industries under Laggards, it is worth noting that two sectors of the industry in the South West, the forestry and dairy industries, had major changes which impacted on their interest and ability to participate in this project. The Regional Forest Agreement reduced logging in the South West and by consequence the size of the timber workforce, and the deregulation of the dairy industry threatened the livelihood of dairy farmers. Nevertheless there was an adequate representation of all sectors of industry as presented in Table 4. The workplace seems to be a well accepted place for health education and screening often the only check-ups over the years for some men. One man in his fifties was thankful that he participated in this project as it encouraged him to have a general health check when he was referred to see a doctor. It was the first one he has ever had and he was very relieved that he had a clean bill of health so far. Hence, worksite screenings are one method of attracting an otherwise disinterested audience or an audience that seeks permission to engage (Donovan and Egger 2000). Men did not seem reluctant to participate in a health check if offered at the worksite and there is a supportive work culture. Hence their comments regarding this program as “a very good idea to have several men gathering to hear the same message and possibly helping each other get through any difficulties if and when it occurs”,

28
“sharing the learning experience with workmates makes it more comfortable”, “having the session at work”. Men seemed grateful for the opportunity to be able to discuss health problems in organised sessions “bloody good idea to participate in such a men’s group” and “thanks for taking the time for us” and “what a pity that more men did not take up the offer”. In the workshop, industries were keen to repeat such a program to reach more of their workforce as they were concerned that 64% of those screened were at high risk of developing diabetes. When it is a one off session, blue collar workers seem to be the hardest to get these sessions organised for, even in industries with a health and safety program. Hence, the percentage of blue collar men did not exceed 40% in this project with the rest made up of middle management. One way to overcome this, is for the industry to be committed to organise screening for everyone on site.
5.4 Effectiveness of General Practitioner Intervention The extent to which GP services are utilised by this group of men is compatible with the local statistics. 76% of screened men had accessed a GP in the last year which is consistent with the local 75% male attendance to GPs per year in the general population (Aoun and Stone 1997). It is also consistent with the concept that men do not visit the GP or undergo a health check if they have no symptoms. However they will do so to compare against a mate, for insurance purposes, as part of another visit, or if offered at the worksite (Donovan and Egger 2000). Hence 40% of GP visits for this group were mostly due to the industry initiated routine checks, and the rest of the visits were due to symptoms/injury/illness or script renewal, test results, vaccines or needing medical certificates for work purposes. Barriers to accessing GPs have not been a major issue for 68% of these men, with “not considering that their problem was serious enough” being the most frequent stated reason for not visiting their doctor (18%). This is related to the lack of knowledge that men have regarding health matters in general and diabetes in particular, as reported by Donovan and Egger (2000). This project has improved awareness of a health issue otherwise considered not serious by many men “just sugar in the blood”. Over 70% of men have confirmed that the program had greatly increased their awareness of consequences and links to heart disease, personal risk particularly the weight factor and the need for lifestyle changes to reduce the risk. It is interesting that 75% of men stated that they personally had a regular GP, a concept not supported by the literature. However, some men might regard the industry GP as their own, having established rapport through the industry routine health checks. This rapport may have contributed to the reduction of inhibiting factors to visiting a GP when needed. For this group of men, proportions who visit GP in one year and those with a personal GP are both positive factors for GP initiated interventions. In the follow-up phase, a significant proportion of GPs (76%) seemed informed about the project according to the participating men which is a good indication that this project had the interest of GPs. All GPs were informed about the project when it started but as the data collection spanned over a year, recall difficulties were expected within the busy schedule of rural GPs including all other competing priorities. Also another indication that the GPs considered the project referrals seriously is the high proportions of men (87%) they sent for blood tests as advised by the diabetes educator. Most of the GPs took this opportunity to do other health checks, hence 32% of men found out they had health problems other than the focus of this study. Furthermore an indication that GPs have engaged in monitoring risk factors was the need for 40% of those checked to come for a further appointment within a short time period. However the onus was on the patient to follow this advice. The positive response of GPs to this project could be interpreted in the light of their awareness of the need to deliver more of the preventive care to their patients. Local GPs are amenable to the concept of preventative care but have not been able to engage in it to a great extent due to the shortage in their numbers per population. This shortage is reflected in the difficulty men experienced in securing timely appointments, with some men waiting up to two weeks to get an appointment with their GP.

29
In a needs analysis conducted in 1997 (Aoun and Stone), 86% of GPs felt they would be required to deliver more of preventive care in the next 5 years (95% indicated health screening and 73% health education). Nevertheless, opportunities for education are still minimal in the overall concept of preventive care. By identifying patients at risk, projects like this one provided GPs with an ideal opportunity for health education as men were not presenting with any acute problem. As this project highlighted, only 49% of men at-risk discussed lifestyle factors with their GPs and the advice was limited to lose weight and exercise more, which left men short of knowing how to achieve this and take action. However as reported in the literature (Oldenberg & Owen 1995 and Bonevski et al 1996) and by GPs who attended the workshop, time limitations compounded by a lack of GP training, make the lifestyle counselling, education and support the role of other health professionals. Even in the regular industry health checks, the opportunity for education is minimal as the GP would feedback negative or positive results of blood tests. It was interesting to find out that the extent of motivation of men to change their lifestyle was not related to whether they visited their GP or not (Table 15). Whether they were motivated or not, their visit to the GP was strictly to determine the presence or absence of disease. This is consistent with the perception that men do not seek out lifestyle information from a doctor who is seen as a quick fix for acute health problems (Donovan and Egger 2000). Some of those highly motivated men who did not visit their GP mentioned that they have already taken measures to reduce their weight. This project had a positive impact on service delivery. The diabetes educator has noticed a marked increase in GP referrals to her services whereas they were under-utilised previous to the project. The reluctance of GPs to refer to and share the management of their patients with support services in the area was a shortcoming for service delivery (Aoun and Stone 1997). This project has highlighted the role of the diabetes educator through referrals for screening from the project and hence increased GPs’ awareness of the need to refer their diagnosed diabetic patients for further education and support.
5.5 Education and Support Strategies Quantitative and qualitative results so far have highlighted gaps in service provision in this region for those at-risk of developing diabetes. The project has been successful in engaging men in the preventive concept of seeking care and getting them to attend their GP to check the extent of their risk. Once this rapport between GP and patient has been established in the context of preventing diabetes, GPs are in a good position to monitor risk factors and manage the treatment side of it. What is still lacking is ways of halting the progression of the disease as the onset of diabetes precedes actual clinical diagnosis by 4 to 7 years. As stated by Welborn, Australian GPs are in a commanding position to 1) identify people at risk, 2) recommend screening, 3) follow up positive screening results with diagnostic testing, 4) and provide appropriate advice on lifestyle and management of risk factors. This is the ideal situation but realistically in the constraints of rural practice and dealing with rural men, the gap in service provision seems to be at the two ends of the spectrum: identifying those at-risk and modifying their behaviour. The workshop between industries and health professionals has highlighted that even health professionals working within the local health services can not meet the need for prevention as there is a waiting list for their services for those with diabetes, heart disease and other conditions. Therefore, the workshop recommended establishing a lifestyle counselling service as a support strategy for those at-risk. A lifestyle counselling program works by moving contemplating men to the stages of action (where behaviour change is initiated) and maintenance (where the change is sustained and predictable health gains are achieved) . These stages of change (“to be explored” in Table 16) address the need expressed by a participant to incorporate “ a motivational element” to the education and screening session in order “to help lazy people like myself improve my lifestyle”. One example of an initiated behaviour change as a result of this project was highlighted in the media (Appendix 13). By

30
acting on the advice given, this motivated man was reported by the health nurse at his industry to have lost thirty kg. Men need concrete advice on how to translate knowledge into action in their daily lives. Lifestyle counselling will mainly target weight through nutrition and physical activity as men would be much more willing to do something about their weight because it is visible than about other less obvious risk factors (Egger 2000). In fact dietary modification and increased physical activity can lead to 40%-50% reduction in the rate of progression from IGT to diabetes (Welborn 2000). The program would work as such: an individualised program for change will be worked out between the client and the lifestyle counsellor ie an action plan for weight loss and exercise which is monitored closely at regular intervals through routine follow-up sessions. This lifestyle counselling service would be expected to be a partnership between industries, GPs and health services for it to be sustained on the long-term. There could be a liaison role for this Centre to play between stakeholders. The role of industries would be to facilitate screening and education programs, similar to this one, but to all their workforce in conjunction with health services and Centre. Men identified at risk would be referred to their GPs who in turn would refer them to the lifestyle counselling service. The industries can also refer directly to the service if the need has been established by the health nurse. Men would be followed by the lifestyle counselling service and feedback given to them, their GP and their industry who will be kept informed about the progress. Developing the best model for the service would need further investigation by a working group of stakeholders, namely the five health services in the region and the two divisions of general practice, with the industries purchasing the service either for groups of their employees or on one-to-one basis (referred to under communications strategy).

31
6. Implications Industries have an important contribution to the continuum of care at the first stage, identification of risk, and at the fourth stage, modification of behaviour, particularly since 60% of adults can be accessed via worksites (Emmons et al 1999). Through the first stage in the continuum of care, industries need to encourage screening in the workplace within a supportive culture so that employees do not feel compromised if as a result they discover that they have health problems. In fact these employees would be at an advantage as the benefits of early diagnosis to prevent complications outweigh risks of jeopardising employment prospects. This study has identified that 64% of the industry male workforce, 40-65 years, are at risk, but no adequate service is yet available to assist these men to modify their behaviour (fourth stage in the continuum of care). The implication of a lifestyle counselling service for the employee is a better quality of life through reduced risk of developing lifestyle-preventable diseases such as diabetes and heart disease. The implication, for the employer, is improved productivity of employees through reduced days lost due to illness, reduced absenteeism and reduced insurance cover. Improving health in the workplace has obvious flow-on effects as healthier and happier people make better and more productive employees. The role of preventative health care is being better recognised and companies are embracing it (Steggall 2000). Unscheduled leave was estimated to have cost Australia 6.7 percent of payroll in 1994, with indirect costs estimated to be more than twice this figure. Poor health is related to stress and stressed workers are estimated to cost $272 million in days off and $1 billion in lost revenue between 1991 and 1997. In 1998, more than 3.5 million Australians had a disability with 3.2 million experiencing specific restrictions in core activities or employment (Steggall 2000).

32
7. Conclusion and Recommendations This study has fulfilled its objectives in terms of establishing that this health initiative is appropriate for engaging men in the preventive concept of seeking health care, that is getting them to attend their GP when they only have the risk factors but not the disease. The adopted strategy of screening combined with education on the worksite and conducted in the context of a medical follow-up has dealt successfully with the issues of how and where to intervene in the case of a disease like diabetes which often goes undiagnosed. Once equipped with the knowledge of their risk, the consequences of the disease and what action they need to take to reduce their risk, these men were not reluctant to use the health services, particularly those with a supportive work culture. Hence the majority of these men would be responsive to further support in order to modify their lifestyle behaviour and sustain the change. Since local health services can not offer this support at this stage, it needs to be provided through an innovative venture between industries and health services. It is recommended that: The strategy tested in this project be applied to cover all the workforce in the industries targeted
in order to assess the true extent of undiagnosed diabetes and to reach the less accessible groups such as blue collar workers. The industries need to be committed to organise screening for everyone on site combined with education and a medical follow-up, particularly in the light of the high proportions at-risk.
The GPs instead of the men report on the follow-up test results which would provide a more
accurate and complete picture of morbidity. For this to happen, The Divisions of General Practice need to be actively and collaboratively involved with industries at the planning phase of the project.
Umbrella organisations for farmers and fruit growers and others in the agricultural sector need to
be more actively involved in encouraging their members to participate in education and screening programs.
Strategies be determined to enable the program of education and screening to be taken to
employees whose organisations are not currently well placed to facilitate health initiatives at the workplace, such as those with a small number of employees, no dedicated occupational health and safety personnel, or a mobile work location.
The feasibility of the proposed lifestyle counselling service as a support strategy needs to be
explored by stakeholders soon in order to capitalise on the awareness and interest generated by this project. Such long-term interventions have more impact on health related behaviour than the one-off single intervention. For this service to be sustainable, GPs, health services and industries need to collaborate.

33
8. Communications Strategy Communication of Results to Key Stakeholders Preliminary results were presented in two forums of key stakeholders at a time where health services in the region were planning a coordinated approach to delivering services for diabetes. The two forums were the Bunbury Diabetes interagency group and the Regional Group for integrated Diabetes Care Program. The key stakeholders represented in these forums were the five health services, Bunbury, Wellington, Vasse-Leeuwin, Warren-Blackwood and Harvey-Yarloop (health promotion officers, dietitians and diabetes educators), the two Divisions of General Practice covering the region, the South West Population Health Unit, Silver Chain Nurses, South West Aboriginal Medical Services and two consumers from the general community. The results from this project have highlighted to the group the extent of men at-risk and the need to factor in their budget the cost of preventative services for those at high risk of developing diabetes. It was decided to establish a working group to look at the feasibility of a lifestyle counselling service which has the prospect to be a commercially significant development as a result of this project. Communication with industries Industry representatives have strongly recommended for the findings of this study to be presented to the higher levels of their management in order to highlight the risk among their employees and illicit their commitment for a lifestyle counselling service to motivate men into behaviour change and halt the progression of disease. National Rural Health Conference An abstract of this study will be submitted to the 6th National Rural Health Conference, Canberra, 4-7 March 20001

34
9. References American Diabetes Association. Screening for Diabetes. Diabetes Care 1997: 20, 1: 22-23. Aoun S, Stone G. The Greater Bunbury Division of General Practice Needs Analysis. WA Centre for Rural Health and Community Development, Edith Cowan University, Bunbury Campus, Western Australia, 1997. Anderson DR, Staufacker MJ. The impact of worksite-based health risk appraisal on health-related outcomes: a review of the literature. American Journal of Health Promotion 1996: 10, 6: 499-508. Ashenden R, Silagy C, Weller D. A systematic review of the effectiveness of promoting lifestyle change in general practice. Family Practice 1997: 14, 2: 160-176. Australian Institute of Health and Welfare (online). Available at http://www.aihw.gov.au/infobytes/health/cardiovascular-disease.html. Retrieved by Internet Explorer (3/4/2000) Becker, M. and Janz, N. (1987). On the effectiveness and utility of health hazard/health risk appraisal in clinical and non clinical settings. Health Services Research. 22 (4): 537-551. Bonevski B, Sanson-Fisher RW, Campbell EM. Primary care practitioners and health promotion: a review of current practices. Health Promotion Journal of Australia 1996: 6, 1: 22-31. Brown KM. Health Belief Model (online). Available at http://www.med.usf.edu/~kmbrown/Health_Belief_Model-Overview.htm. Retrieved by Internet Explorer (2/2/2000). Burkitt G. Strategies for dealing with men in general practice. Australian Family Physician 1999: 28, 8: 773-774 . Campbell SM, Roland MO. Why do people consult the doctor? Family Practice 1996: 13, 1: 75-83. Charles C, Whelan T, Gafni A. What do we mean by partnership in making decisions about treatment? British Medical Journal 1999: 319: 780-782 (18 September). Colagiuri S, Coagiuri R, Ward J. National Diabetes Strategy and Implementation Plan. Canberra, Diabetes Australia, 1998. Commonwealth Department of Health and Aged Care. National Diabetes Strategy 2000-2004. Canberra, Commonwealth of Australia, 1999. Commonwealth State Diabetes Forum. Highlights of Government Support for Diabetes Australia 1999. Canberra, Commonwealth Department of Health and Aged Care, 1999. Coulter A. Paternalism or partnership? British Medical Journal 1999: 319: 719-720 (18 September). Dobson SK, Penman AG et al. Clinical Health Goals and Targets for Western Australia, Vol. 1. First Report of the Western Australian Task Force on State Health Goals and Targets. Perth, Health Department of Western Australia, 1994. Donovan RJ, Egger G. Men’s Health Beliefs: A Qualitative Research Report. CBRCC Report No. 1. Bentley WA: Centre for Behavioural Research in Cancer Control, April 2000.

35
Egger, G. (2000). Intervening in men’s nutrition: Lessons from the Gutbuster men’s ‘waist loss’ program. Aust J Nut Diet, 57 (1): 46-49 Emmons KM, Linnan LA, Shadel WG, Marcus B, Abrams DB. The working health project: a worksite health-promotion trial targeting physical activity, diet and smoking. Journal of Occupational and Environmental Medicine 1999: 41, 7: 545-555. Engelgau M, Aubert R, Thompson T., Herman W. Screening for NIDDM in Nonpregnant Adults: A review of principles, screening tests, and recommendations. Diabetes Care 1995: 18, 12:1606-1618. Fletcher R Men’s health in rural New South Wales. Australian Journal of Rural Health 1995: 3: 106-113. Gabhainn SN, Kelleher CC, Naughton AM, Carter F, Flanagan M, McGrath MJ. Socio-demographic variations in perspectives on cardiovascular disease and associated risk factors. Health Education Research 1999: 14, 5: 619-628. Greene GW, Rossi SR, Rossi JS, Velicer WF, Fava JL, Prochaska JO. Dietary applications of the stages of change model. Journal of the American Dietetic Association 1999: 99, 6: 673-678. Harris MI, Klein R, Welborn TA, Knuiman MW. Onset of NIDDM occurs at least 4-7 years before clinical diagnosis. Diabetes Care 1992: 15: 815-819. Harrison JA, Mullen PD, Green LW. A meta-analysis of studies of the health Belief Model with adults. Health Education Research 1992: 7, 1: 107-116. Heaney CA, Goetzel RZ. A review of health-related outcomes of multi-component worksite health promotion programs. American Journal of Health Promotion 1997: 11, 4: 290-307. Huggins AK, Somerford P, Rouse I. A Report on Men’s Health Western Australia 1996. School of Public Health, Curtin University, in collaboration with Epidemiology Branch, Health Information Centre, Health Department of Western Australia, 1996. Humphreys J. Rural health status: what do statistics show that we don’t already know? Australian Journal of Rural Health 1999: 7: 60-63. Humphreys JS, Rolley F, Weinand HC. Evaluating the importance of information sources for preventive health care in rural Australia. Australian Journal of Public Health 1993: 17, 2: 149-157. Nutbeam D, Harris E. Theory in a Nutshell: A practitioner’s guide to commonly used theories and models in health promotion. Sydney, National Centre for Health Promotion, 1998. Oldenburg B, Owen N. Preventive care in general practice in Australia: a public health perspective. Patient Education and Counselling 1995: 25: 305-310. Paul CL, Redman S. A review of the effectiveness of print material in changing health-related knowledge, attitudes and behaviour. Health Promotion Journal of Australia 1997: 7, 2: 91-99. Peach HG, Bath NE. Prevalence and sociodemographic determinants of cardiovascular risk in a rural area. Australian Journal of Rural Health 1999: 7: 23-27.

36
Pelletier KR. A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: 1995-1998 update (IV). American Journal of Health Promotion 1999: 13, 6: 333-345. Pham DT, Fortin F, Thibadeau MF. The role of the Health Belief Model in amputees’ self-evaluation of adherence to diabetes self-care behaviors. The Diabetes Educator 1996: 22, 2:126-132. Potter E. The Lifestyle Project: Final Report. Albany, The Great Southern Division of General Practice, 1999. Schoenbach, V., Wagner, E. and Beery, W. (1987). HRA: Review of Evidence for Effectiveness. Health Services Research. 22 (4): 553-580. South West Development Commission. (1999) (online). Available at http://www.swdc.wa.gov.au/region/industry/index.asp. Retrieved by Internet Explorer (26/5/2000). Steggall V. Curing the body corporate. HR Monthly 2000: July: 16-21. Towle A, Godolphin W. Framework for teaching and learning informed shared decision making. British Medical Journal 1999: 319: 766-771 (18 September). Veitch J, Owen N, Burns J, Sallis JF. Physical activity promotion for male factory workers: a realistic option? Health Promotion Journal of Australia 1997: 7, 3: 169-174. Wdowik MJ, Kendall PA, Harris MA. College students with diabetes: using focus groups and interviews to determine psychosocial issues and barriers to control. The Diabetes Educator 1997: 23, 5: 558-562. Welborn, T. (2000). Diagnosing Australians at risk of diabetes mellitus in general practice. The Medical Journal of Australia, 173, 2: 61-62 Western Australian Diabetes Services Taskforce. Western Australian Diabetes Strategy 1999. Perth, Health Department of Western Australia, 1999.

37
10. Appendices

38
Appendix 1 Media release inviting industry participation


40
Appendix 2 Letter to individual industries enlisting participation

41
WA CENTRE FOR RURAL HEALTH & COMMUNITY DEVELOPMENT INC.
8th Floor, Bunbury Tower,
61 Victoria Street, Bunbury, WA 6230
Tel: (08) 9792 2520 Fax: (08) 9792 2503
e-mail: [email protected] (health officer) (name on industry) (address) (Date) Dear
Regarding Screening for Diabetes in Industries (Men’s Health Project) I am seeking the interest of your industry to be involved in this research project which is aimed to improve the health status of rural men working in industries in the South West. The project is funded by the Rural Industries Research and Development Corporation in Canberra, so there is no cost for the local industries to be involved. Men between the ages of 40 and 65 years will be asked to complete a tick-test card on risk factor and symptom assessment for diabetes, a card devised by Diabetes Australia. This screening will coincide with a campaign for community awareness by Diabetes Australia in November 1999. Before screening, participants will be required to attend a diabetes education seminar focussing on ways to reduce risk factors and improve on lifestyle issues. Participants with two or more identified risk factors will be asked to see their doctor with a letter explaining the outcome of the screening test. This will help in the early detection of undiagnosed diabetes and reduce the personal and community burden of this disease. The screening and educational seminar will require an hour and will be conducted in your meeting place or workplace by Ms Jenny McDonnell, the diabetic educator in the Bunbury Health Service. Participation is of course voluntary. Men at high risk will have the choice to be followed up after their visit to the GP and their opinion sought on how to improve men’s access to and participation in health services. If your industry is interested to participate in this project, I would appreciate if you are able to inform me of the number of men in your industry between 40-65 years. A flyer is attached to help assess the number of men interested to participate. Also, It would be helpful if you could advise me of a date, time and a place before (date), we could undertake the screening and educational session. Hoping to hear from you soon Yours sincerely Dr Samar Aoun Director WA Centre for Rural Health and Community Development

42
Appendix 3 Flyer inviting employees to participate

43
Healthy Blokes
Look Better and Live Longer
Know your risks for Diabetes • If you are a man between the ages of 40 and 65 years • and you are interested to know if you are at-risk of getting DIABETES • and how to avoid getting DIABETES You are invited to attend a short screening session, consisting of completing a questionnaire, to assess your risk factors followed by a concise information session on diabetes prevention. Date: Time: Location: Do not miss this free opportunity to improve your health, as Diabetes is on the increase for this age group and has become a major national health problem affecting men but PREVENTABLE. ……………………………………………………………………………..
Diabetes Screening and Education If you would like to participate in this project, please sign this section of the flyer and return to (name) by (date). Name of participant:…………………………. Signature:……………………………………..

44
Appendix 4 Questionnaires: 4.1 Risk assessment 4.2 Health service utilisation 4.3 Evaluation of education

45
Personal Diabetes Risk Assessment Test
Name:………………………. Age (years):………………………… Circle or tick the most appropriate response
Risk Factors Low Risk High Risk Symptoms of diabetes
Persistent/excessive thirst Excessive urination, especially
at night Recurrent infections Blurred vision Unexplained tiredness Numbness/tingling in feet or
legs
No symptoms ticked
1 or more symptoms ticked
I have a close blood relative with diabetes
No Yes
My ethnic (family or ancestral) background is
Northern European or Anglo-Celtic
Southern European Indian Asian Polynesian Aboriginal
My blood pressure is high (greater than 140/90) or is treated with medication Blood pressure … … … … … …
No
Yes
I am overweight for my height Specify height………………
Specify weight………………
(Check chart)
Waist circumference … … … …
No Yes
I have a history of heart disease No Yes I had a previous borderline high blood sugar test
No Yes
TOTAL SCORE (No of ticks in high-risk column) If you are over 40 years of age and scored 2 or more in the high risk column, you have an increased chance of developing diabetes and should be checked by your GP. If you are over 50 years of age and scored 1 or more in the high risk column, you are at risk of developing diabetes and should be checked by your GP. Those identified to be at high risk, please collect a referral letter to your GP.

46
USE OF HEALTH SERVICES (please complete or tick the appropriate responses)
Q1. Which area or town do you live in?…………………………………………. Q2. How long have you been resident in this area/town?……………………….. Q3. Do you personally have a regular GP? Yes…… No…… Q4. When was the last time you visited each of the following?
A GP at the surgery
Accident and Emergency Dept at the hospital
Other health professionals (please specify)
Less than 1 year ago 1 to 2 years ago Between 2 and 5 years More than 5 years ago Q5. What was the reason for your most recent visit to each of the following?
A GP at the surgery
Accident and Emergency Dept at the hospital
Other health professionals (please specify)
Injury Illness Symptoms or complaints Routine check Test results Script renewal Other (please specify)
Q6. Is there anything that would put you off or prevent you from visiting a GP when you have
a health problem?
I do not think my health problem is serious enough I do not seem to have enough time to see the doctor I consider the cost of going to the doctor a problem for me A lot of time waiting I do not find the surgery times convenient because I have to take time off work I find the waiting rooms at doctor’s surgery make me feel uncomfortable I feel embarrassed to be seen in the waiting room by others I just can not be bothered Any other reason…………………………………………………………….. Nothing puts me off from visiting a GP
Q7. Would you visit a GP for further medical care, if you knew you had some risk factors for developing Diabetes? Yes…… No…… IF NO, please specify your reasons………………………………………………..








54
Appendix 6 Letter of referral to GP for men identified as at risk

55
WA CENTRE FOR RURAL HEALTH & COMMUNITY DEVELOPMENT INC.
8th Floor, Bunbury Tower, 61 Victoria Street, Bunbury, WA 6230
Tel: (08) 9792 2520 Fax: (08) 9792 2503
e-mail: [email protected] Dear Doctor As part of the Men’s Health Project in the South West, we are conducting “Risk Checks for Diabetes” in the local industries to raise awareness of risk factors for developing type 2 diabetes. On (date), your patient ……………………………… was found to have the following symptoms and/or risk factors for developing type 2 diabetes:
Persistent/excessive thirst
Frequent/excessive urination Recurrent infections/skin irritations Blurred vision Unexplained tiredness Numbness/tingling in feet or legs Age 40-49 years Age 50-65 years Family history of diabetes High risk ethnic background Reported hypertension Overweight History of heart disease Previous impaired glucose tolerance
For patients at high risk, a medical review and a venous plasma glucose test are recommended to screen for type 2 diabetes. Details of risk factors and basic information on ways to improve lifestyle have been provided to your patient. If you have any queries, please contact me on 97221370. Yours sincerely Jenny McDonnell Diabetic Educator Bunbury Health Service

56
Appendix 7 Contact with GPs to inform them about project: 7.1 Letter to individual GPs

57
WA CENTRE FOR RURAL HEALTH & COMMUNITY DEVELOPMENT INC.
8th Floor, Bunbury Tower,
61 Victoria Street, Bunbury, WA 6230
Tel: (08) 9792 2520 Fax: (08) 9792 2503
e-mail: [email protected]
Dear Doctor As part of the MEN’S HEALTH Project in the South West, the Centre, in collaboration with Jenny McDonnell, Diabetes Nurse Educator, is conducting “Risk Factors Assessment for Diabetes” in the local industries to raise awareness of risk factors for developing type 2 diabetes. Men, between the ages 40-65 years, who have a high risk will be referred to see their GP with a letter explaining the outcome of the screening. The aim of the project is to: • encourage undiagnosed men to seek medical advice in good time • motivate them to make changes to their lifestyles before the condition sets in • improve men’s access to and participation in health services The research team will follow-up these men to find out the outcome of their visit to their GP. So basically this letter is to inform you about this health intervention and the background to the referral letter that you will see with your patients in the next three months (hopefully if they make the step and come and see you!). If you would like more details or would like to make suggestions, please do not hesitate to contact me on 97922520. Thanking you for your cooperation Yours sincerely Dr Samar Aoun Director WA Centre for Rural Health and Community Development

58
Appendix 8 Consent form for follow-up phase of project

59
WA CENTRE FOR RURAL HEALTH & COMMUNITY DEVELOPMENT INC.
8th Floor, Bunbury Tower, 61 Victoria Street, Bunbury, WA 6230
Tel: (08) 9792 2520 Fax: (08) 9792 2503
e-mail: [email protected]
MEN’S HEALTH PROJECT Thank you for participating in the first phase of the men’s health project: Diabetes Screening and Education. The research team will need your consent for phase 2 and 3 of the project which will deal with improving access of men to the health services in the area. Second phase: If you receive a referral letter to a GP as a result of today’s screening, the research coordinator will contact you in about a month to find out from you if you have visited a doctor and the outcome of the visit. If you did not visit a doctor, we would like to know what prevented you from doing so. Third Phase: You may be invited in about 3 months time to a meeting (focus group) to canvass your opinion on how to improve access to medical services for men like you, based on your experiences. ……………………………………………………………………………………….
CONSENT FORM I agree to participate in phase 2 and 3 of the Men’s Health Project as explained above, realising that I may withdraw at any time from taking part in this project. All information will be treated as strictly confidential. Signature:…………………………… Date:……………………………. Name of Participant: ………………………………………………………….. Phone Number: ……………………. (work) …………………….. (home) Address: …………………………………………………………… ……………………………………………………………

60
Appendix 9 Follow-up questionnaire

61
WA CENTRE FOR RURAL HEALTH AND COMMUNITY DEVELOPMENT INC.
DIABETES SCREENING AND EDUCATION FOLLOW-UP
Recently you attended a diabetes screening and education session, as a result of which you were eligible to be given a letter of referral to your General Practitioner. The purpose of this follow-up survey is to ask you whether you have yet visited your GP and if so, what the outcome was. Your name: ………………………………… Employer: ……………………... Your age (in years): …………………………….. Please tick or complete the appropriate response. Q1. Since attending the diabetes screening and education session,
have you visited your General Practitioner? Yes No If No, please go to Question 10 (over the page) If Yes, please answer Questions 2-9. Q2. Did your GP know about the diabetes project
when you handed in the referral letter? Yes No
Q3. Did your GP send you for a blood glucose (sugar) test? Yes No Q4. If Yes, did the result show diabetes to be:
Unlikely
Unclear, requiring further investigation
Diabetes likely Q5. What other tests (if any, such as another blood glucose test) did your GP arrange or perform? Please indicate the result if known. (e.g. raised blood pressure; cholesterol level) ……………………………………………………………………………………….. ………………………………………………………………………………………..

62
Q6. Did your GP give you any healthy lifestyle information e.g.
healthy diet, weight control, exercise, smoking, alcohol? Yes No Q7. If Yes, what kind of advice were you given? ………………………………………………………………………………………..
Q8. Did your GP ask you to attend for another appointment? Yes No Q9. If Yes, were you asked to come back
Within two weeks
Within one – two months
Within six months
Within a year Q10. If you have not yet attended your GP following the diabetes screening/ education session, please indicate if:
You have made an appointment with your GP
You intend to make an appointment with your GP
You do not intend to make an appointment with your GP Q11. Please give your reasons if you do not intend to see your GP about the results of the diabetes screening. ……………………………………………………………………………………….. Please return this questionnaire as soon as possible in the same envelope in which you received it. Seal the envelope and return it to (name).
Thank you for completing this questionnaire.
Keep Healthy!

63
Appendix 10 Workshop between industries & health professionals: 10.1 Invitation to participate 10.2 Workshop outline

64
WA CENTRE FOR RURAL HEALTH AND COMMUNITY DEVELOPMENT INC. Dear Last phase of the men’s health project (diabetes education and screening in industries) You are invited to participate in a workshop on men’s health and diabetes prevention involving workplaces, general practitioners and other health providers.
Thursday 8th of June 2000 12-2pm
10th Floor, Bunbury Tower (lunch provided)
The aims of the workshop are: • To present the findings on the education and screening sessions conducted in 22 industries
and for about 450 men so far, 40-65 years old, and use the findings as a basis for discussion for the points that follow
• A feedback on the education and screening program from the perspective of the employer (industries) and employees (men who participated)
• To explore issues of how and where to intervene in the case of a disease like diabetes which often goes undiagnosed
• To explore issues of men’s access to and participation in health services as a factor in improving men’s health
• To recommend education and support strategies for those identified at-risk as a collaborative initiative between industries, GPs and other health providers
Can you please RSVP by Tuesday, June 6, to Dr Samar Aoun by phone 97922520, Fax 97922503 or e-mail [email protected]

65
MEN’S HEALTH & DIABETES PREVENTION WORKSHOP
Thursday 8th June 2000 12-2pm
BUNBURY TOWER
Aims • To present interim findings on the diabetes education and screening session conducted in 31 organisations
in which 419 men aged 40-65 have participated, using the findings as a platform for further discussion. • To obtain feedback on the pros and cons of the education and screening program from the perspective of
the employer (industries) and employees (men who participated). • To explore issues of how and where to intervene in the case of a disease like diabetes which often goes
undiagnosed. • To explore issues of men’s access to and participation in health services as a factor in improving men’s
health. • To recommend education and support strategies for those identified as at-risk as a collaborative initiative
between industries, GPs and other health providers.
Session Outline
1. Welcome and introduction 2. Presentation of interim findings of program Sample
• Risk assessment • Accessing GP services • Results of follow-up
3. Feedback on the education and screening program from the men who participated and their employers 4. Employee perspective: • In addressing health concerns such as diabetes, what would men like from their GPs,
other health providers and their employers? • 5. Employer perspective • Response to employee views & suggestions of what’s feasible from an employer’s
perspective of industry OHS programs. 6. Perspective of GPs & other health providers: • Response to employee/employer views & suggestions of what’s feasible from the
perspective of GPs and other health providers. 7. Towards a resolution: • What strategies might be utilised to address gaps identified in foregoing discussion? 8. Close

66
Appendix 11 Samples of industry newsletters advertising the project