Embed Size (px)
Citation preview

What To Do After You Have Been Discharged From
Therapy?
Strategies for Returning to Work/School/Life.
Presented byFairlawn Rehabilitation Hospital
Julia Krasheninin MS CCC SLP Karla McAuliffe MA CCC SLP
What is COGNITION?
THINKING! Frontal Lobe: regulates /mediates higher
intellectual function = EXECUTIVE FUNCTION (self regulation)
It involves all the components required for conscious mental activities.

Helm Estabrooks identifies 5 major cognitive domains:
ATTENTION, MEMORY, EXECUTIVE FUNCTIONS, LANGUAGE and VISUOSPATIAL SKILLS
CLQT: Everyday Example of Cognition in Functional Activities
While getting ready for work, Sandra notes she is out of toothpaste and she has no aspirin, which she takes daily for stroke prevention. Her executive functions “kick in” and enable Sandra to both realize the consequences of being without these items and make a decision to stop at a drugstore on the way to work. She mentally plans her route to most closest drugstore on the way to work using her visuospatial representation of the neighborhoods and streets between her house and the office.
In the car Sandra uses her procedural memory for driving without having to think about the process of shifting, accelerating, breaking, etc. This enables her to turn her thoughts to a difficult project she has at work. Using her executive function skills, she thinks about all the factors and considerations involved in this projects and she arrives at a different approach to it.
At the drugstore, Sandra uses her visual perceptual and motor skills to help her parallel park. She enters the store, she recalls 2 items she needs from memory storage. To facilitate the search process she uses semantic/conceptual knowledge to mentally place the needed items in semantic categories so she can go directly to aisles where items are located ( aspirin-pain medications). Her visual perceptual skills help her negotiate the aisles and working memory helps her retain the items on the list and their location. Arriving at the aisle she needs she uses her visual perception, scanning, selective attention, and language skills in the form of reading to locate the items. Working memory helps her compare brands relative to price/size/quantity and executive skills help her to make the best decision in view of what she needs, likes and judges to be the best value.

WHAT is weak after TBI?
Common deficits:
EXECUTIVE FUNCTION!!self regulation strategic thinkinglearning new informationproblem solvingmental flexibilityinitiation attentionorganizationtheory of mind


ASHA’s Technical Report of Children and Adults with Cognitive-Communicative Disorders after Brain Injury states the following:
“The goals of cognitive and behavioral rehabilitation are to enhance the person’s capacity to process and interpret information and to improve the person’s ability to function in all aspects of family and community life.”

Goal: • Improve an individual’s performance
by eliminating or reducing underlying cognitive impairment.
Assessment:• Battery of standardized tests resulting
in judgments about area of cognitive weakness and areas of strength that can be used to compensate for weaknesses
Treatment:• De-contextualized exercises to restore
cognitive processes and skills• Goal: eliminate or reduce cognitive
impairment
Goal: •Help achieve functional objectives and participate in activities that are at least temporarily blocked by impairmentAssessment:•Standardized testing •Situational observations can substitute standardized tests•Markers of functional improvement are maintained job, independent living, school grades, etc.Treatment:•De-contextualized exercises • Practice functional tasks important to them •Practice strategic thinking and compensatory behaviors in functional contextsGoal: restore function through repeated successful performance of functional tasks with external mediation/self regulation or support
Traditional Paradigm Contextualized Paradigm

Factors that contribute to recovery:• Premorbid personality, goal direction of individual, length of coma, areas of
brain damaged, family support, age, course of therapy, emergency medical services (trauma center vs. nearest hospital), funding for services.
Did I (caregiver) attend the therapy sessions?????
WHAT IS THE PROBLEM? WHAT TO DO if THIS HAPPENS? • Can we list our strategies=solutions?? Have we been practicing and
integrating our strategies into our daily routines?? CHECK LIST : At the time of discharge, caretakers should go to each discipline
with questions regarding adapting the home environment. • PT/OT: Required equipment? Physical modifications?• Neuropsychology: Home safety issues? What to do if behavioral issues
arise? • ST: Communication/Cognitive strategies? Swallowing guidelines?• Case manager: home care, outpatient services, support groups.
Discharge Plan/ Are we ready? Preparing for lifetime commitment
What is the problem? Learn the weaknesses, know the strengths! Organized home= place for everything. Change the room arrangement for easy
access, label and thoughtfully arrange drawers, notebook or cue cards with specific steps for completing tasks/routines i.e. shower, personal care. Keep it simple!
Establish a schedule and Use alarms to keep on schedule. Calendar and visual aids when necessary.
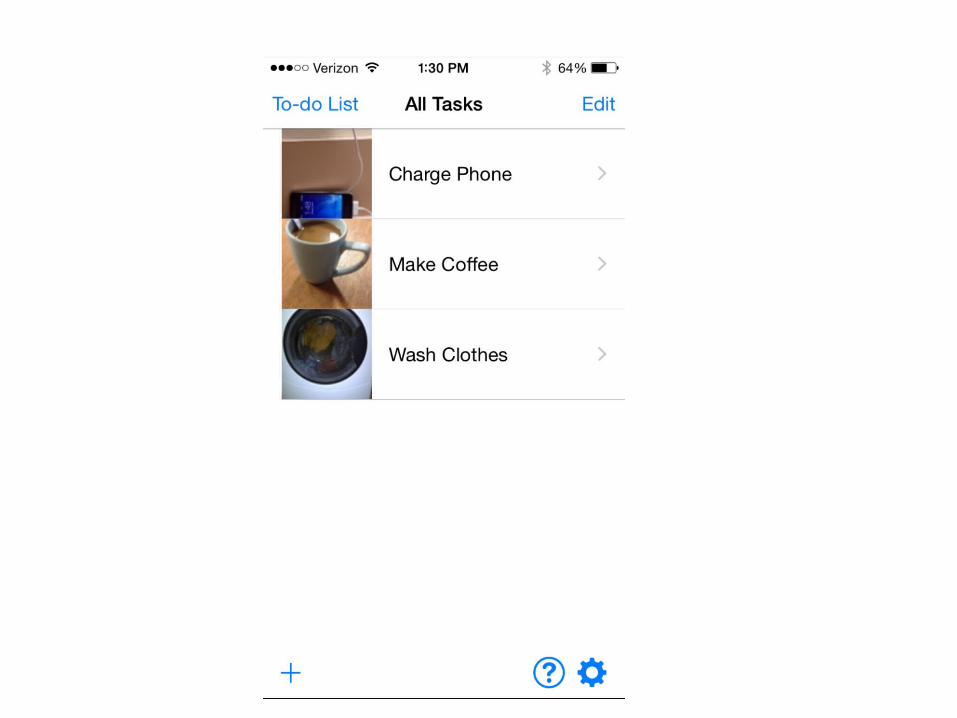
External cues-Visual/graphic aids: to do lists, calendars, alarm clocks. Limit “nagging.”
Family members reactions need to be consistent. Share your routines with all caregivers.
Same instructions, consistency in approach or feedback, repetition to ensure recall. Visual/Graphic /clear and concrete!
Always check with your physician when behavioral changes occur! Proactive! Positive!
Seek support for social problems i.e. drugs/alcohol.
CHECKLIST for DISCHARGE

STRUCTURE CONSISTENCY REPETITION
BRAIN LOVES ORGANIZATION! Order in the house! Order in Words/Thoughts!
MODEL ,TEACH, and PRACTICE VISUAL/GRAPHIC SUPPORTS
“In my house, meticulous neatness is imperative. If you move my leather coat from a hook to the closet, I may forget I own it.”“Lost In My Mind – Recovering From TBI”

Anticipating or dealing with barriers to independent living
Initiation impairment
“ It’s like I need to turn on the engine even for basic needs. “ –caregiver.
Initiation= starting an activity or thought; part of self regulatory system
WHAT IS THE PROBLEM ?Initiation deficits can be misconstrued for behavior issues or emotional problems.
Initiation Skills/Executive Function Deficits
Accommodations and environmental supports:
Well established and understood daily routines. Initiation deficits often require frequent cueing. Reduce nagging by
external cues! Alarms, schedules. Encourage individuals to write or record their own cues/lists/schedules
to foster self sufficiency and reduce resistance. Multistep tasks may require cues for each distinct step Plan to start early and allow for slow, steady completion. Double the
time! Plan to request help “could you help me get started on this after
lunch?” MODEL, TEACH, PRACTICE: visual or graphic supports
Self Regulation Skills/Executive Functions Deficits
Signs of self regulation difficulties may include any of the following:
Decreased understanding of own abilities/needs =weak self monitoring/evaluation/insight
Difficulty with goal setting; coming up with reasonable goals or steps to accomplish goals =weak problem solving, initiation
Difficulty with inhibiting impulses =weak flexibility in thinking Difficulty organizing thoughts, language, behaviors =weak problem solving Difficulty shifting from one activity to another =weak cognitive flexibility Difficulty learning from consequences =weak self evaluation
What is different since the brain injury??
Is there Insight?“ I felt like there was a storm going on in my head.”
WHAT is the PROBLEM?
o Self regulation issues may be misidentified as behavior problems or lack of concern for the quality of their work.
o As caregivers, clinicians, teachers, and coworkers we should be specific with our observations and reporting of behaviors.
Instead of :“ he does not care, she is depressed, he is lazy”
Try : “he is not doing the laundry like I asked; she is in bed until 12 pm.”

What are SCRIPTS?
Words that we learn and use to help us think and self regulate!! STRATEGIC THINKING!
Cognitive strategy! “Scripts can be used as conversational routines that can be internalized as the
survivor’s own self regulatory system”
LEARN, PRACTICE, REPEAT : Self regulation scripts should be practiced through out the day in all settings!
GOAL: INDEPENDENCE with STRATEGIC THINKING! AUTOMATIC!
“this is a big deal” “I need to plan this out” “ I know its scary but I will have help”

Types of Scripts for Self Regulation
1. GOPDR2. Easy to do/Hard to do3. Ready/Not Ready4. Big deal/Little deal5. Scary /Not scary6. Choice/No Choice
Goal, Obstacle, Plan, Direction, Do, Review- strategy for any problem solving
Important to accurately estimate your abilities
Important to know what’s important
Important to know you need a plan to reduce impulsivity
Facilitates judgment and helps to understand emotions
Important to know when you have a choice and when you don’t

Progression of scripts
• Start with caregiver statements such as “I think this may be hard for you so you might need some extra help. I know that will work, ok?”
• Questions: “Do you think this will be hard or easy? What’s the plan to get this done?”
• Gestures to trigger the self regulatory script• End goal is that the script will be internalized
and serve as a self regulatory process=automatic self guidance! “This will be hard but I can do it.”

Script guidelines
• Scripts should be used under positive circumstances so they have positive associations/ avoid nagging, threats, ‘I told you so’
• Pick which script is most usefuldon’t overwhelm
• Modify language to the individual’s age, vocabulary and sensitivities
• Scripts should be used frequently
• Scripts should gradually be internalized ;supports should be faded as the individual acquires and shows use
“ Talk to your self like you would to someone you love”
GOPDR is a Cognitive Strategy!!! Goal: What is the goal?
Obstacle: Why is this hard? What is the problem?
Plan: What is the plan? What do you need for this to work?
Do : Apply the chosen solution
Review: How did it work? Any problems? What can you try next time?
“I like to sort and fold my own laundry”
“ I can’t go down to the basement and I can’t always get started. I get easily distracted.”
“ I need help. My husband will bring the washed and dried clothes to me and I will sort into piles. I will take my time. I will know I need to start it when I see the basket of clothes. I will not pay attention to the phone if it rings.”
“ I folded the clothes. It was quiet and no one distracted me. Quiet room worked well. Maybe next time I will have the news on while folding.”

Problem Solving/Executive Function Deficits
Weakness in self regulationAgain: difficulty understanding needs, setting
realistic goals, making plans to achieve goals set, initiating goal –directed behaviors, inhibiting distractions, monitoring performance, evaluating outcomes
Making adjustments is SOLVING Problems!Learn, model, practice: SCRIPTS=strategic thinking!
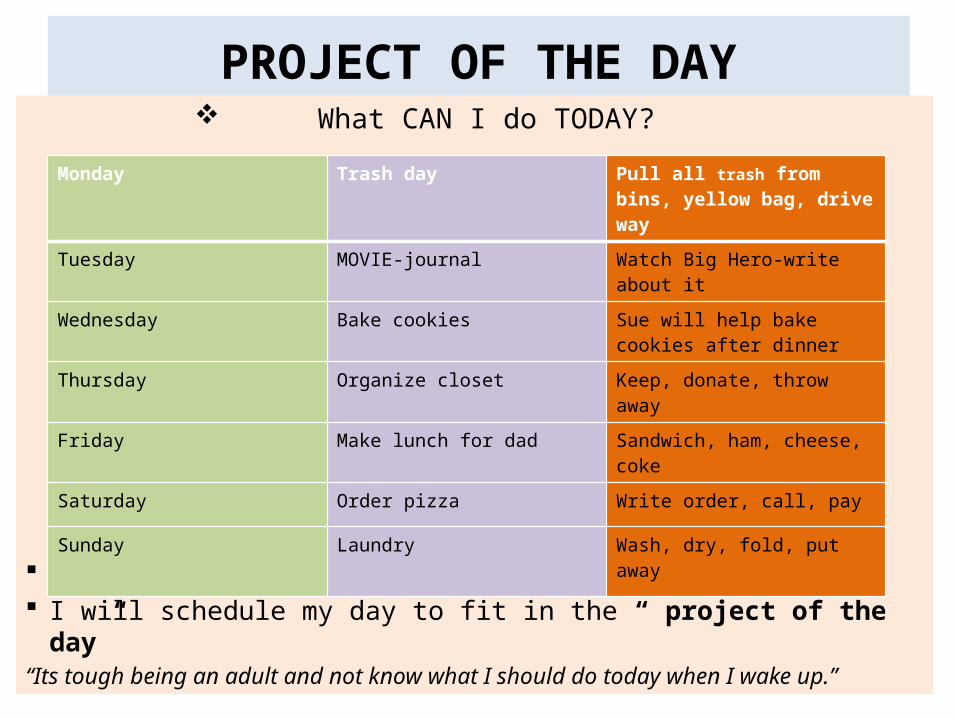
PROJECT OF THE DAY What CAN I do TODAY?
I will choose one task and complete it. I will schedule my day to fit in the “ project of the day”“Its tough being an adult and not know what I should do today when I wake up.”
Monday Trash day Pull all trash from bins, yellow bag, drive way
Tuesday MOVIE-journal Watch Big Hero-write about it
Wednesday Bake cookies Sue will help bake cookies after dinner
Thursday Organize closet Keep, donate, throw away
Friday Make lunch for dad Sandwich, ham, cheese, coke
Saturday Order pizza Write order, call, pay
Sunday Laundry Wash, dry, fold, put away

Rigidity/Inflexibility/Executive Function Deficits
Weakness in self regulationDifficulty with transitionsReduced ability to tolerate and adjust to
changeReduced ability to shift thoughts, moving on-
concrete thinkingReduced emotional flexibility

Flexibility Routines
“ My daily routine: wake up, be awesome, go back to sleep!”
Routines to change routines
Discuss the change or new routine in advance. Practice the new routine before implementing them. When change is implemented use “self talk” or “ scripts” “I don’t like
change but this will be ok” to put the survivor in best frame of mind. Use graphic or visual organizers (photo sequence of schedule in
school/work) Keep few routines the same and reassure that some routines will remain
unchanged. Peer support (pair with another student/coworker to help with transitions) “ I can be like batman kind of person.”-positive sense of self. Choose
association meaningful to individual .

Impaired Theory of Mind/EgocentrismCognitive Deficit
What is the problem?• Cognitive egocentrism is NOT moral egocentrism,
or lack of social knowledge or social skills• Can be misidentifies as as anxiety, depression,
impulsiveness, initiation impairment• It is a weakness in the ability to see alternative
perspective “ why can they take 3 AP classes but I can’t? ”or “misreadings” of others intent/emotions
Support and Strategies for weak Theory of Mind after TBI
Competent and Sensitive Social partners: practicing “mind reading” to reduce “misreadings” “Did you see the look on his face? That told me that he was just kidding.”
Explicit cues to help understand others mental state “Let me tell you a joke…”before a joke is told or “Just kidding” after a tease.
Practice interpreting “mental lives of people”, their emotions, desires, motivations-discuss during dinner or book reading. “I wonder what he thought, felt, hoped.”
Engage in helping others-discuss why someone is having difficulty, what can we do to help.
Learn few “scripts” for conversation starters.

Revised Ranchos Los Amigos Scale
Includes Theory of Mind skills!!!Level X- purposeful, appropriate
able to recognize the needs and feelings of others!!
accurately estimates abilities and independently adjusts to tasks!!

Tips for Caregiver“It’s ok not to be there for every hour of every day.”
“It takes a village and whatever works!”• Accept help when someone offers!• Take care of your Life! Love and honor
yourself!• Express your emotions!• Be informed! • Maintain a journal!• Find a support group!

Available Resources
• Projectlearnet.org• Mass Brain Injury Association• ASHA• Brainline.org• www.biausa.org• TBI Hope and Inspiration
Technology: APPs for Cognition or Brain Exercises!
HAND OUTS!

Discussion

References/Bibliography
• Projectlearnnet.org• CLQT• ASHA