Embed Size (px)
Citation preview
“What were they doing for me really?”;
experiences of ward-based rehabilitation following prolonged
critical illness.
Pam Ramsay RGN, PhD Research Manager
Critical Care
Royal Infirmary of Edinburgh
Overview
The long-term patient population
(Qualitative) health services research Theory
Generalisability
“What were they doing for me, really?” Methods
Analysis
Biographical disruption (Bury, 1982)
“System-induced setbacks” (Hart, 2001)
How is prolonged critical illness defined?
≥48 hours mechanical ventilation (Chelluri et al, 2004)
≥29 days mechanical ventilation (Gracey et al, 1992)
Tracheostomy and/or mechanical ventilation
for ≥4 days (Cox et al, 2007)
≥21 day’s mechanical ventilation for ≥ 6hours a day (MacIntyre et al, 2005)
≥ 14 days ICU stay; as a point at which “family members and clinicians begin to wonder about the “worthwhileness” of continuing care” (Heyland et al, 1998:
193)***
The “costs” of prolonged critical illness
Highest costs (in terms of bed days utilised)
Disproportionate use of scarce ICU resource
Impact upon the wider ICU patient population
Refused admissions
Increased illness severity
Reduced ICU length of stay
Untimely or premature discharge
Prolonged hospital stays
Increased demand for scarce rehabilitative resource
Increased mortality
The symptom burden: physical
Recovering organ impairment Reduced cardiovascular and pulmonary reserve Muscle wasting Profound weakness Fatigue Joint stiffness Peripheral neuropathy Severe weight loss Loss of appetite Alopecia Pruritis Adapted from Griffiths et al (1999) BMJ; 319: 427-429
The symptom burden: psychosocial
Anxiety
Depression
Disturbed sleep
Recurrent persecutory nightmares
Panic attacks
Fear of dying
Guilt
Social isolation
Altered family relationships
Adapted from Griffiths et al (1999) BMJ; 319: 427-429
Others
Reduced/poor quality of life (Herridge et al, 2003)
For many years following ICU/hospital discharge
Remains below population norms
Caregiver strain (Cameron et al (2006), Pelt et al (2007)
Psychological morbidity (anxiety, depression, PTSD)
Lifestyle disruption (e.g. employment, leisure activities)
Delayed return to work (Herridge (2003), Cheung
(2006))
(Qualitative) health services research
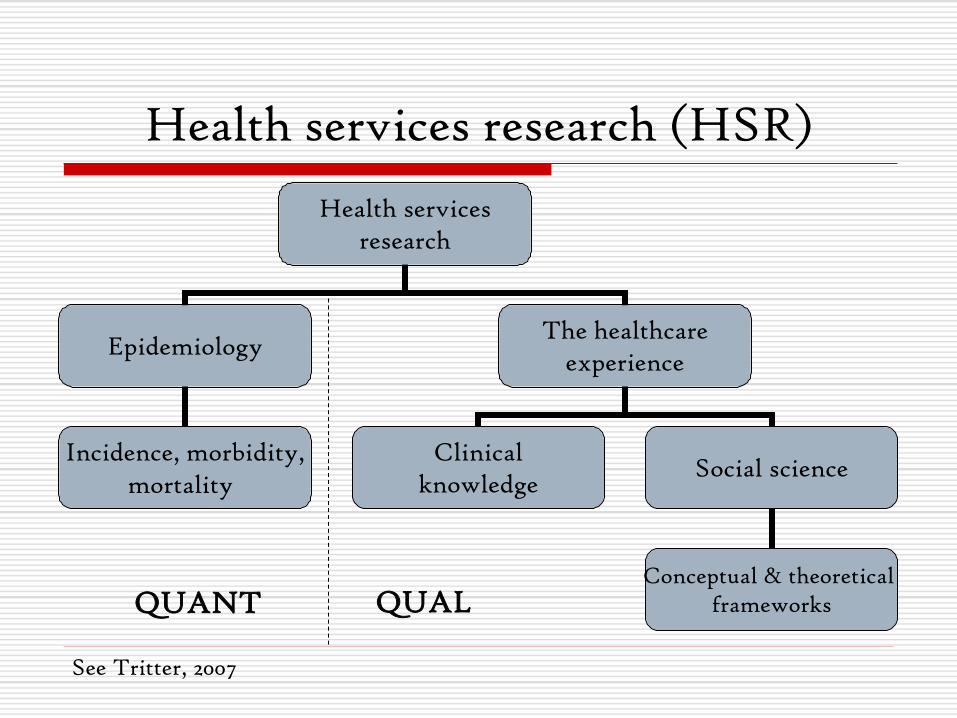
Health services research (HSR)
Health services research
Epidemiology The healthcare
experience
Incidence, morbidity, mortality
Clinical knowledge
Social science
Conceptual & theoretical frameworks
See Tritter, 2007
QUANT QUAL
Qualitative methodology: an untidy business*
“Insider” or patient perspective
Inductive approach
Data collection
Data analysis
Repeated (re)reading of the data
Emergence of themes
Coding (axial)
Deviant case analysis, etc
*See Koller (1983), Pope and Mays (1995)
Researcher as “bricoleur”
“Cycling back and forth” with the literature
Qualitative HSR: “light” in theory?
Problem/process oriented approach
Pragmatic, localised concerns
Emphasis on method
“Generic”, “slavish cook book” or “pick and mix” approach
“Empirical” data which is limited in analytical and explanatory potential, and in terms of its
ability to advance knowledge
See Harding and Gantley (1998), Appleton and King (2002),Katz and Mischler (2003)
Theory
Provides a set of general, modifiable propositions which:
Explain
Predict
Interpret
causal links
confounding variables
context
phenomena of interest
See Patton (2002)
Generalisability?
“Fittingness”
“Comparability”
“Translatability”
“Naturalistic” generalisability explicit comparisons
tacit knowledge
“Analytical” or “theoretical generalisability Replication logic
similar results
contradictory results (but for predictable reasons)
“Richness” of description •phenomenon of interest •context •theoretical stance
See Schofield (1993), Yin (2004)
“What were they doing for me really?”: experiences of ward-based care and rehabilitation

Methods
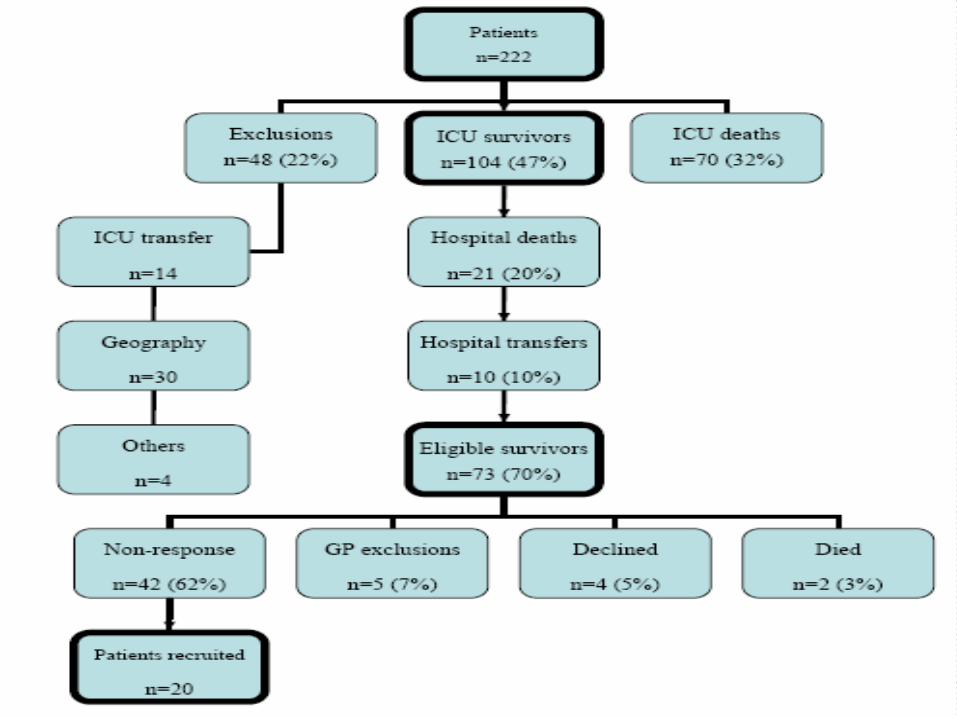
Qualitative interview at ≤6 months post ICU discharge
Access to participants
SICSAG database
General Practitioners
Sampling: convenience (purposive not always possible)
The semi-structured interview
Life before critical illnes
The ICU experience
Experiences of ward-based care and
rehabilitation
Life after critical illness
Morbidity
Adaptation
Recovery
The critical
illness “journey”
Biographical disruption
“precisely that kind of event in which the structures of everyday life and the forms of knowledge which underpin them are disrupted” (Bury,1982: 169)
Biographical shift
“predictable” life course
chaotic and uncertain
Biographical disruption following critical illness
“When I first got home, I got the shock of my life…I could put water in the kettle, but I couldn’t lift it. That’s scary…that’s when you say to yourself, “You are bad”.
(Andy (54), pancreatitis)
Biographical disruption following critical illness
“I was glad to be home but very, very tired and very weak. I was…frustrated by the fact that my life was gone as I knew it. I had to rely on someone to help me get up, dress me, that sort of thing.” (Anne (77), pneumonia)
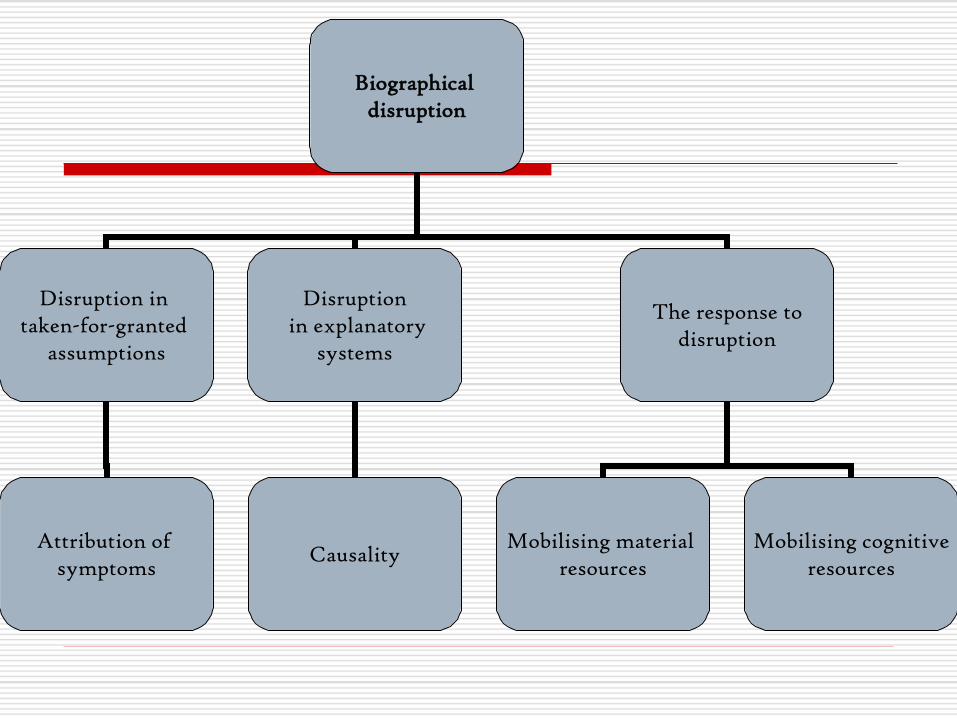
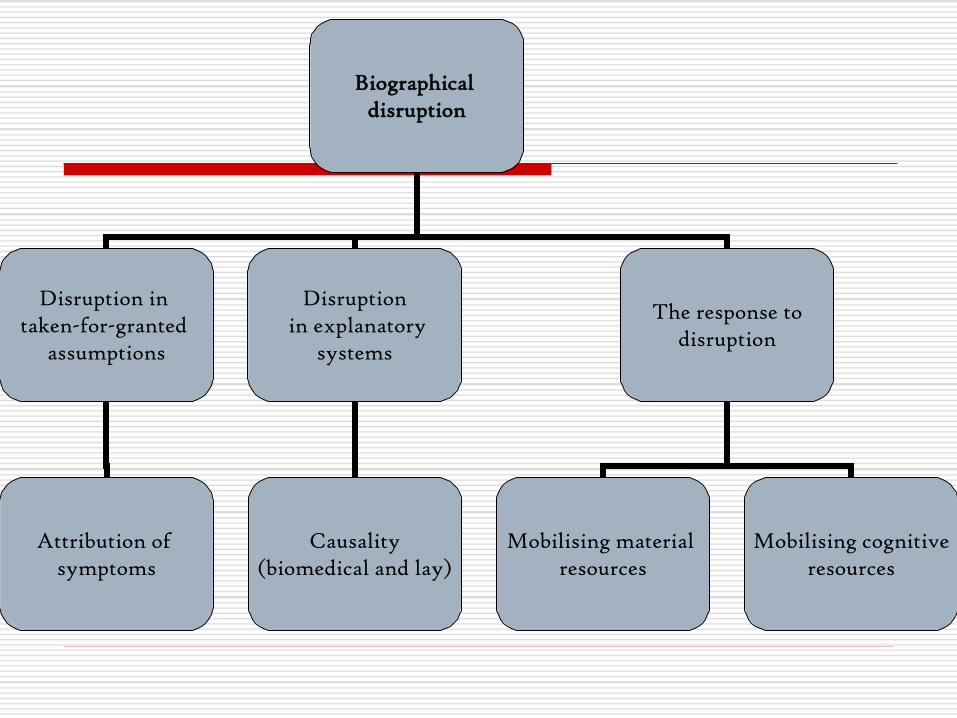
Biographical disruption
Disruption in taken-for-granted
assumptions
Disruption in explanatory
systems
The response to disruption
Mobilising material resources
Mobilising cognitive resources
Causality Attribution of
symptoms
“System-induced setbacks”
A device for making visible patterns of interaction and social process in the delivery of health…services which are screened out by “professional vision”, and obscured by routinised and medicalised ways of seeing.”
(Hart, 2001: 103)
Why explore “system-induced setbacks”?
“…system failures can undermine even the best efforts of…survivors and their families to manage their lives, forcing them to invest even more energy into “strategic management” than might otherwise be the case.” (Hart, 2001: 102)

Taken-for-granted assumptions
“I could’ve done more to help myself… my
brother asked for a sheet of exercises for me to do when I got out. I realise I could’ve been doing a lot of that. Seems obvious now, but it
wasn’t then…I think I could’ve progressed quicker.” (Jane (51), pneumonia)
Taken-for-granted assumptions
“I headed up in front of the physio, so that he didn’t see my face...because it took every ounce of strength to get up there. But once I came home, I couldn’t walk up the stairs in a oner. I had to take three goes at it. But I did it well enough to get out of hospital...”
(John (49), pneumonia)
Taken-for-granted assumptions
“I could walk about the ward with a stick… I could see they were trying to get shut of me (laughs). I had the big talk, and I said, “I’m not ready to go home, my wife can’t look after me” and eventually I was taken out to convalescence.” (Albert (71), septic shock)
See Connolly et al (2009): the “systematisation” of patients
Taken-for-granted assumptions
“…the doctor must have okayed it, must’ve thought I was ok. They don’t discharge people
that are not capable and they let me out.” (Ken (71), ruptured aortic aneurysm)
Explanatory systems: amnesia
“The last thing I remember was…the ambulance. I don’t remember anything else until I woke up six weeks later.” (Elizabeth (61), oesophageal rupture)
Explanatory systems: delirium
“I spent a session with my parents where…I’d tell them what I thought I’d dreamt but wasn’t sure whether it was a dream or reality. They were able to say, “No, that’s complete rubbish, that was obviously a dream.”” (Dave
(32) pancreatitis)
Explanatory stems: information (general)
“Even in my fuzzed head, I was aware on a number of occasions that whoever was momentarily in charge of me had scant knowledge of who I was and how I got there.”
(John (49) pneumonia)
Explanatory stems: information (morbidity)
“I don’t know if it’s something that happens if you’ve only been in (ICU) a few days…but your body feeds off your muscles. I didn’t know any of this…Had I have had this knowledge, it would’ve been…easier for me to accept." (Jane (51), pneumonia)
Response: material
“ I won’t have a bath unless there’s someone in the house. I’m still waiting for a bath seat. It would’ve been a great help…especially when I first got home.” (Jane (51), pneumonia)
Response: material
“I don’t like to sleep downstairs…well, I’ve had to the past few months, because I’m not able to get upstairs….not even on my bum.”
(Anne (77), pneumonia)
Response: material
“I have what I call my “messy corner”…my newspaper, the remote for the telly, my pills, the phone, my grabber and what have you. I just have everything where I can reach it. I get by (laughs).” (Pat (47), post-operative pneumonia)

Response: material
“I filled forms in to see what height certain things were and they sent somebody up with the toilet seat and to raise the bed. These things were all done before I went home. They gave me the chair, walking sticks, the gripper, shoe horn and I’ve got a thing to put my socks on with.”
(Roy (63), pneumonia)
Response: cognitive
“You’ve got to have the will…and say, “Yes, I am
going to get better. I’m going to…get my life back”. Really having the determination…it’s not easy.” (James (65), necrotising fasciitis of the
neck)
Response: cognitive
“…one afternoon, I walked right over there (gestures out of the window). But I was so knackered later that day that I daren’t go out the next day. At first I thought, “Oh, I’ll perhaps do this every day”, but I’ve not been out since (laughs).” (Ken (71), ruptured aortic aneurysm)
Response: cognitive
“I had to go to my GP...I came out of there and got some groceries..and then I realised that I’d gone too far. I had to get a taxi home....So now it’s...I can get to distance x, but I’ve got to make sure I can get back.” (John (49), pneumonia)
Response: cognitive
“I felt the pain I get from the angina, so I had to use the spray and calm myself. Maybe doing too much too soon, I dunno. If I’m going to the shop…especially if it’s windy…it catches my breath and I feel the pain in my chest. I just put my back to the wind and have two puffs of the spray.” (Roy (63), pneumonia)
Response: cognitive
“I still get a bit breathless. It could be the first wee while…Sometimes I find if I’m walking more, it’s not as bad, funnily enough. You’d think it’d be the other way round.” (Sandra (67),
pneumonia)
Biographical disruption
Disruption in taken-for-granted
assumptions
Disruption in explanatory
systems
The response to disruption
Mobilising material resources
Mobilising cognitive resources
Causality (biomedical and lay)
Attribution of symptoms
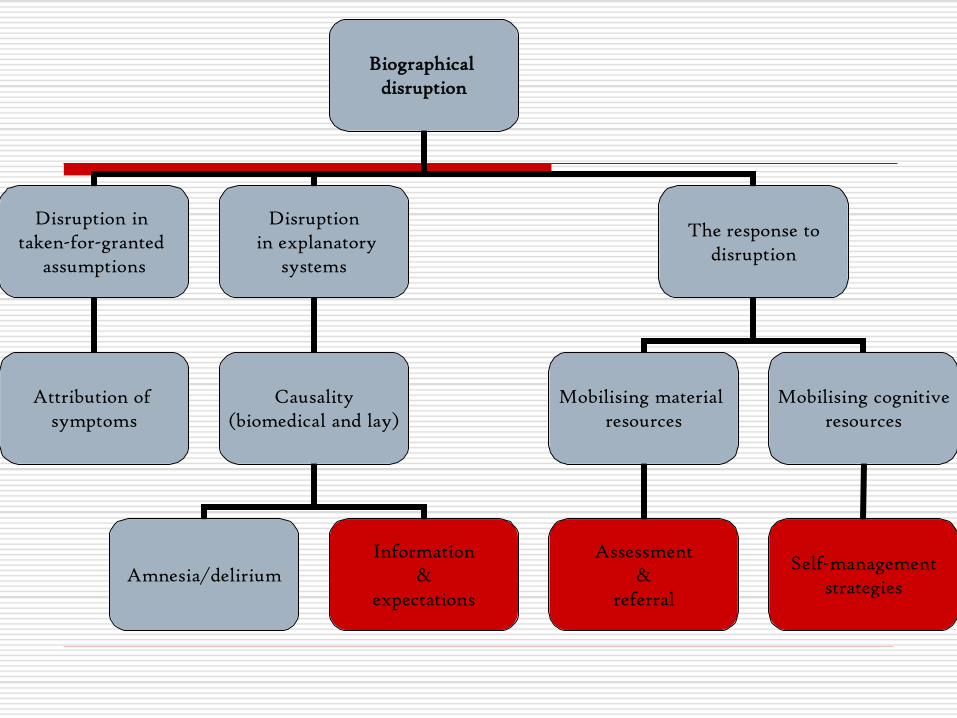
Biographical disruption
Disruption in taken-for-granted
assumptions
Disruption in explanatory
systems
The response to disruption
Mobilising material resources
Mobilising cognitive resources
Causality (biomedical and lay)
Attribution of symptoms
Amnesia/delirium Information
& expectations
Self-management strategies
Assessment &
referral
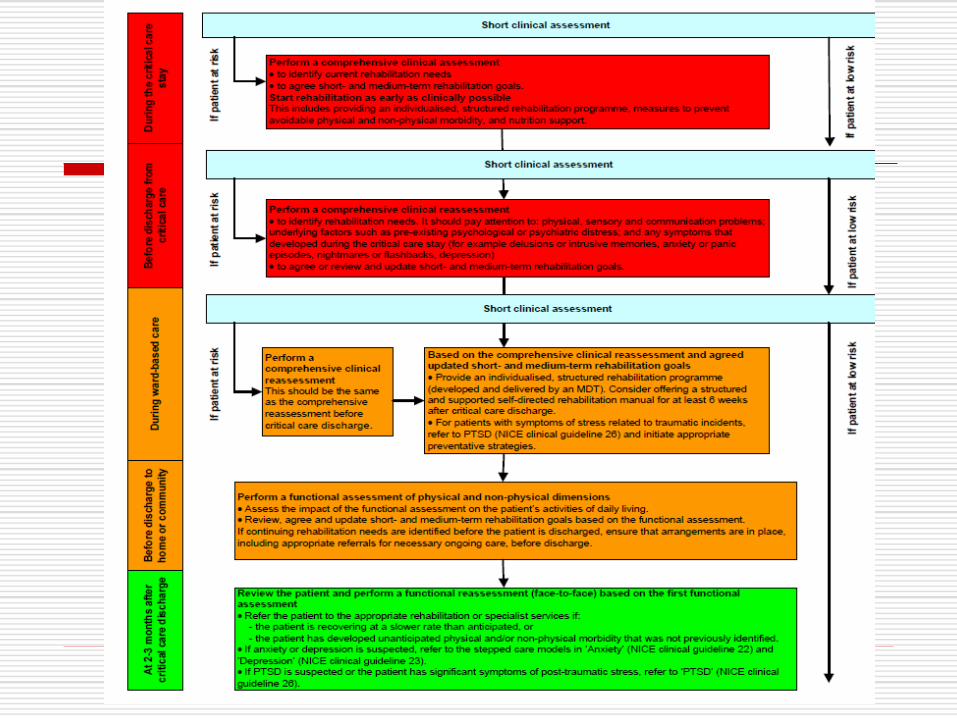
The NICE guidelines (2009)
Rehabilitation After Critical Illness (National Institute for Health & Clinical
Excellence)
Questions?

Typical early morbidity
“I couldn’t walk. I was very, very weak. It took me all my time to get out of bed. I’d lost 2 and a half stone…and all my muscle was gone.”
(James (65), necrotising fasciitis of the neck)
“Inexplicable and worrying” (Jones and O’Donnell, 1994)
“A critical defining characteristic” of the distress survivors experience after ward transfer (McKinney and
Deeney, 2002)
Experiences of nursing care
“It's quite upsetting for somebody relatively young, still in their right mind, not being able to wash themselves and having to be washed, toileted and all the rest of it.”
(Christine (53),septicaemia)
See Field et al(2007)
Experiences of nursing care
“I remember one of the nurses insisting that I sit out on a chair very early on. I had no strength to sit and… she had no understanding as to my plight in that sense.” (Dave (35), pancreatitis)
See Field et al(2007)
Experiences of physiotherapy
“I said, “I never should’ve been left the way I was. I should’ve done exercises so that I wasn’t in this state.” And Dr Charmless said to me, “Well, that can’t be helped””
(Jane (51), pneumonia)

Experiences of physiotherapy
“I had to fight with them at first, but then they let me do things at my own pace. I said to them “I will walk and I will do this, but you’ve got to let me do it…if you’re pushing me, it’s not going to work.”” (Anne (77), pneumonia)
Discharge planning:professional
“I could walk about the ward with a stick… I could see they were trying to get shut of me (laughs). I had the big talk, and I said, “I’m not ready to go home, my wife can’t look after me” and eventually I was taken out to convalescence.” (Albert (71), septic shock)
Discharge planning: professional
“…there wasn’t a family meeting, there wasn’t any meeting with the doctor as such. There was a lot of interest, yes, in getting me home, but not any concrete discussion on ways to
make it easier for me.”( Lynne (25), pneumonia)
Discharge planning: professional
“I filled forms in to see what height certain things were and they sent somebody up with the toilet seat and to raise the bed. These things were all done before I went home. They gave me the chair, walking sticks, the gripper, shoe horn and I’ve got a thing to put my socks on with.”
(Roy (63), pneumonia)
Edinburgh Royal Infirmary
Mixed general ICU/HDU
19 beds (13 ICU/6 HDU)
Major trauma centre for Lothian
Specialist referral centre for liver transplant
~1,000 admissions annually
Mean/median ICU LOS
ICU mortality: ~22%
Additional hospital mortality: ~8%
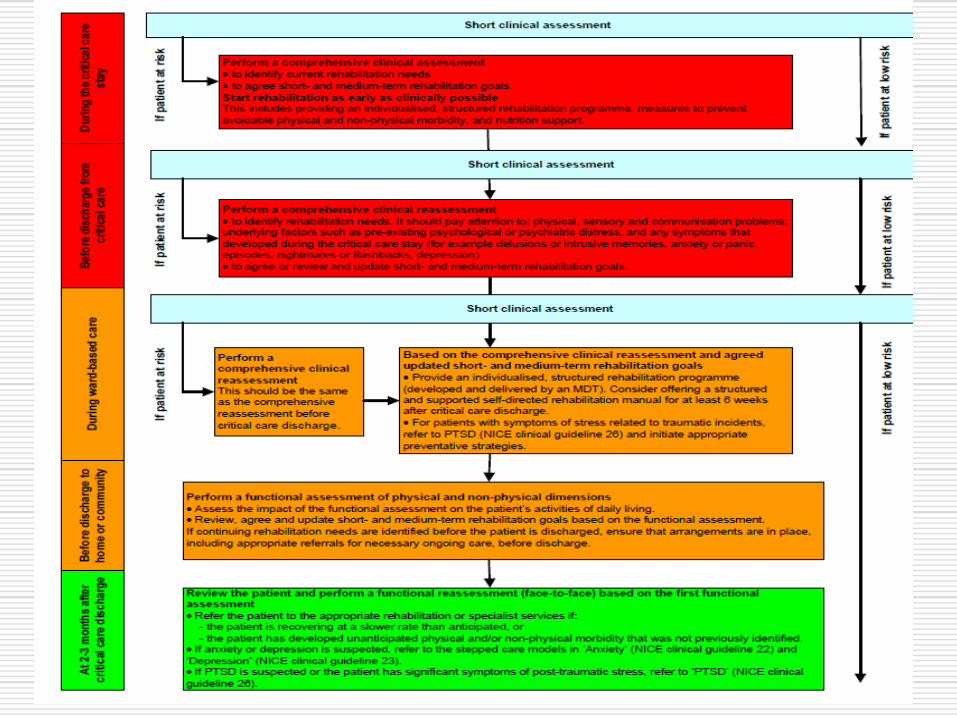
The NICE guidelines (2009)
Rehabilitation After Critical Illness (National Institute for Health & Clinical
Excellence)
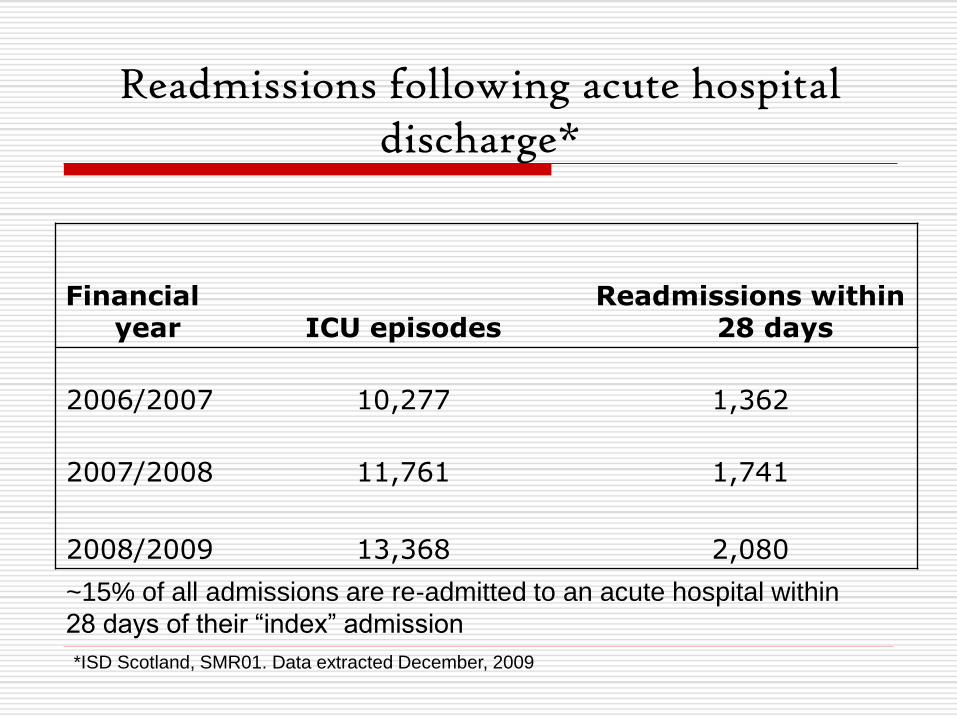
Readmissions following acute hospital discharge*
Financial year ICU episodes
Readmissions within 28 days
2006/2007 10,277 1,362
2007/2008 11,761 1,741
2008/2009 13,368 2,080
*ISD Scotland, SMR01. Data extracted December, 2009
~15% of all admissions are re-admitted to an acute hospital within
28 days of their “index” admission