Embed Size (px)
Citation preview

When working on processes consider -
Mapping the key processes as flowcharts
Identifying supporting microsystems and how they interact with core processes
Observing and measuring cycle times—how long process steps take
Professionals
Every member of the microsystem who provides or
contributes to the care of patients should be thought
of as a professional. Learning more about the staff,
what they do, when they work and what they think
and how they rate the workplace is an important part
of understanding any microsystem. A staff survey is
often a good way to find out what would make the
service better for patients and the team.
Patterns
Patterns exist in every microsystem
but often are unnoticed. Patterns exist
in many dimensions and questions to
consider are—
What are the metrics that
matter to this microsystem—
the outcome measures?
What are the trends over
time?
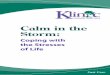
What would you want to change in Renal OPD?
0% 20% 40% 60% 80% 100%
Clinical Outcome
Customer Care
Hospital environment - Cleanliness
Hospital environment - Layout
Hospital environment - Furniture
Clinc appointment scheduling
Information available in outpatients
Waiting time for patients
Seeing the appropriate staff member
Time of day clinic held
Room use/allocation
Staff working patterns
Available equipment
% of replies
1 - No change required 2 3 4 5 - Large change required
Clinic VC147B Tuesday 1/11/11
8.3
0
8.4
5
9.0
0
9.1
5
9.3
0
9.4
5
10
.00
10
.15
10
.30
10
.45
11
.00
11
.15
11
.30
11
.45
12
.00
12
.15
12
.30
12
.45
13
.00
13
.15
13
.30
13
.45
14
.00
Patient 1
Patient 2
Patient 3
Patient 4
Patient 5
Patient 6
Patient 7
Patient 8
Patient 9
Patient 10
Patient 11
Patient 12
Patient 13
Patient 14
Patient 15
Patient 16
Patient 17
Patient 18
Patient 19
Patient 20
Patient 21
Patient 22
Patient 23
Patient 24
Patient 25
Patient 26
Patient 27
Patient 28
Patient 29
Patient 30
Patient 31
Patient 32
Patient 33
Patient 34
Patient 35
Patient 36
Patient 37
Patient 38
Patient 39
Patient 40
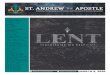
Processes—Gantt
Chart showing
cycle times
Processes
The microsystem members participate in various
processes and steps to care for patients. Often the
team have never taken the time to review these
processes and different views and perspectives
emerge when the team create a flowchart of these
core processes. This lack of knowledge often leads to
waste and unreliability
What are the communication and social patterns within the microsystem?
Do the team meet and review these patterns to improve care?
Resources
Further information about collecting and understanding the 5Ps can be found in—
Quality by Design (2007) Nelson, Batalden, Godfrey, Ch 6 & 13
Dartmouth Microsystem Academy Action guides
www.clincalmicrosystem.org CLICK Materials
www.sheffieldmca.org.uk
4 ©2013 Trustees of Dartmouth College, Sheffield Microsystem Coaching Academy
Assessing Your Microsystem using the 5Ps
‘A one page book’
‘To do things differently, we must see things differently’
John Kelsch, Xerox 1990
The 5Ps framework is a tested and useful method for microsystem members to begin to
see their microsystem in a new way and begin to ask new questions. This process should
actively involve the microsystem team to build understanding and ownership. The
discoveries made in the 5Ps help the team create and select their theme(s) for
improvement. (See resources pg 4)
Purpose
High performing microsystems have a clearly stated purpose and mission. Writing a
purpose statement during the 5Ps allow the team to consider—why does our microsystem
exist? Do we all share a common goal and aim? Active discussion of this connects
individual members with the microsystem purpose.
To promise and deliver
reliable, patient-
centered, evidence
based care for every
patient, every time. (IDCOP Berwick 2001)
To provide an essential clinical support
service to ensure local and regional
patients with an endocrine condition
receive the highest quality clinical
outcomes (EIU, STH 2012)
‘To enable people with CF to live
as normal a life as possible’
(STH CF Team 2011)
Patients
General population knowledge and facts are often not shared by all members of the
microsystem team, even though many will have individual knowledge of the patients they
provide care to. Things to consider are
What subpopulations exist within your patient group?
What are the demographics, age, gender?
Where do your patients travel from?
What do patients think about the service? What do they think we can do better?
What is it like in daily life to have the condition(s) you treat
16-25 26-35 36-45 46-55 56-65 66-75 76-85 86+
Age 0.6% 2.2% 9.0% 20.2% 28.1% 27.0% 10.7% 2.2%
0.6%2.2%
9.0%
20.2%
28.1%27.0%
10.7%
2.2%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
What is your age group?55 years old
Married
3 children—1 at University
Still at work
Husband not very supportive
Only 2 treatment options—
no option for operation
Referred straight to hospital
for chemotherapy
Anxious and fearful
Has no nurse specialist or
other support
Rosie— A typical patient (fictional)
1

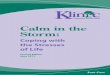
An example 5Ps—Cystic Fibrosis at Sheffield Teaching Hospitals
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
CF OPD Purpose - To enable people with CF to live as normal a life as possibleTotal number of patients
0
20
40
60
80
100
120
140
2003/
04
2004/
05
2005/
06
2006/
07
2007/
08
2008/
09
2009/
10
2010/
11
Band 6
Band 5
Band 4
Band 3
Band 2
band 1
Do you have any comments regarding the CF Outpatient Service?
”Less waiting around please”“I feel the clinic could do with updating”
“The unit is old-the rooms are small”“Dated room requires some TLC”
“Would prefer it to be quicker”“Not enough rooms as when busy have to wait in waiting room not separate room.”“CF unit is small for the amount of patients…the no. of patients have outgrown the facilities.”
“Written and formalized Annual Review results and summary from clinics allows patients to track own health; essential!”
“A good comprehensive service delivered by friendly & supportive staff.”“All the staff are caring and lovely, even the cleaners. They exceeded expectations.”“Having the new ward has made it a lot easier to stay in hospital.”
“All staff are lovely, helpful, experienced and patient.”“I think the ward is very good, all the nurses were great and made me feel really welcome and the
facilities were really good!”“Outpatient facility could be improved. The rooms are too small and outdated.”“ Not enough Community support”
“long wait for admission – at least 3 days”“Can’t always see the physiotherapist. psychologist and social worker when you want to”
Where do your patients come from?
How do we compare—registry data
What do your patients think? - Survey
PROCESSES
Diagnosis at Birth
Managed by SCH until
aged 16
Visit Outpa-
tients, vari-able fre-
quency
Annual Re-view on Birth-
day
PFT Weight—BMI Sputum Sam-
ple/Swab
GTT Test
Dr or SPR Re-view
Dietician Re-view (Most
Patients)
Nurse, Port Flush, Blood
Sample
Physio (Some Patients)
Visit Phar-macy for
Meds
Admission to CF Ward, ITU
or HDU
X Ray Social Worker Ultra Sound Bone Scan (Metabolic
Bone)
Pharmacy
Combined
clinics, Diabe-tes, Met
Bone,
Lung Trans-
plant (Newcastle/
Papworth/
Elsewhere)
Transition Clinic
Psychologists
Cashiers Of-fice (Some)
Patient Trans-port
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
Role Name Role Name Role Name
Respiratory Consultant Frank Edenborough Physiotherapy manager Cheryl Harman Ward/Outpatient CF Matron Ruth Marrison
Respiratory Consultant Martin Wildman Physiotherapy Clinical Specialist Ward Manager Susan Lloyd
Secretary to Frank Wendy Skelton Psychologist Gemma Field Ward Matron Alison Lee
Secretary to Martin Joanne Andrews SpR Sally Davies Health Care Assistant Michelle Lowther
Nurse Specialist Yvonne Locke SpR Aldrin Adeni Volunteer (HCA’s mum) Shelia Foster
Nurse Specialist Shirley Murray SpR Kate Gasgoyne Senior Dietician Sarah Thornton
Nurse Specialist Julie Boadle Social Worker Dorothy Langman Dietician Alisia Milne
Patient representative Lynsey Morton Social Worker Louise Martin Dietician Nina Singaroyan
Service Manager Lisa Needham Pharmacist Amanda Plummer Dietician Jenny Leyland
Assistant Service Manager Claire Walker Pharmacist Tim Gleeson Clerical Officer Marjorie Frater
Pathway Coordinator Julie Key Medicines Management Technician Suzanne Wilkinson
Role Name Role Name Role Name
Respiratory Consultant Frank Edenborough Physiotherapy manager Cheryl Harman Ward/Outpatient CF Matron Ruth Marrison
Respiratory Consultant Martin Wildman Physiotherapy Clinical Specialist Ward Manager Susan Lloyd
Secretary to Frank Wendy Skelton Psychologist Gemma Field Ward Matron Alison Lee
Secretary to Martin Joanne Andrews SpR Sally Davies Health Care Assistant Michelle Lowther
Nurse Specialist Yvonne Locke SpR Aldrin Adeni Volunteer (HCA’s mum) Shelia Foster
Nurse Specialist Shirley Murray SpR Kate Gasgoyne Senior Dietician Sarah Thornton
Nurse Specialist Julie Boadle Social Worker Dorothy Langman Dietician Alisia Milne
Patient representative Lynsey Morton Social Worker Louise Martin Dietician Nina Singaroyan
Service Manager Lisa Needham Pharmacist Amanda Plummer Dietician Jenny Leyland
Assistant Service Manager Claire Walker Pharmacist Tim Gleeson Clerical Officer Marjorie Frater
Pathway Coordinator Julie Key Medicines Management Technician Suzanne Wilkinson
Role Name Role Name Role Name
Respiratory Consultant Frank Edenborough Physiotherapy manager Cheryl Harman Ward/Outpatient CF Matron Ruth Marrison
Respiratory Consultant Martin Wildman Physiotherapy Clinical Specialist Ward Manager Susan Lloyd
Secretary to Frank Wendy Skelton Psychologist Gemma Field Ward Matron Alison Lee
Secretary to Martin Joanne Andrews SpR Sally Davies Health Care Assistant Michelle Lowther
Nurse Specialist Yvonne Locke SpR Aldrin Adeni Volunteer (HCA’s mum) Shelia Foster
Nurse Specialist Shirley Murray SpR Kate Gasgoyne Senior Dietician Sarah Thornton
Nurse Specialist Julie Boadle Social Worker Dorothy Langman Dietician Alisia Milne
Patient representative Lynsey Morton Social Worker Louise Martin Dietician Nina Singaroyan
Service Manager Lisa Needham Pharmacist Amanda Plummer Dietician Jenny Leyland
Assistant Service Manager Claire Walker Pharmacist Tim Gleeson Clerical Officer Marjorie Frater
Pathway Coordinator Julie Key Medicines Management Technician Suzanne Wilkinson
Who are the Multidisciplinary team?
•To be more time efficient, a faster more efficient flow of patients, reduce waiting times•To have better access to the full MDT•To have flexible appointments•Nicer facilities•Things to do while waiting – TV, refreshments•Better building, complete overhaul, decent waiting room, overall nicer environment, cleaner rooms, improve decor•Closer proximity to ward•A unit administrator – to make us more organised & efficient•Less pharmacy wait, rapid access to pharmacy prescriptions•More physio input•More pharmacy input•Quicker clinic visits•Better parking facilities
•To be time efficient, more stream-lined, produce less waste•To have better scheduling of activities, job roles for individuals•To have a nicer environment to work in, better building, more space, up to date equipment and furniture •To improve staffing levels to allow better attendance at clinic for junior trainees•Improved ambulance/ patient transport efficiency – reduce late working hours, angst of patients and families •A doctors room, private room with desk to be able to dictate away from phone/chat•Sluice for dealing with specimens, urine, faeces.•To be closer to CF ward•Better integration between ward and OPD service•Better communication with CF ward•Clarity of roles with all the changes•Patient management system to improve quality of care•Improved time keeping by patients in terms of arrival times and reduced DNA
What are the key processes—flowchart
Who are your supporting microsystems?
2
An example 5Ps—Cystic Fibrosis at Sheffield Teaching Hospitals
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
CF OPD Purpose - To enable people with CF to live as normal a life as possible
PROCESSES
Diagnosis at Birth
Managed by SCH until
aged 16
Visit Outpa-
tients, vari-able fre-
quency
Annual Re-view on Birth-
day
PFT Weight—BMI Sputum Sam-
ple/Swab
GTT Test
Dr or SPR Re-view
Dietician Re-view (Most
Patients)
Nurse, Port Flush, Blood
Sample
Physio (Some Patients)
Visit Phar-macy for
Meds
Admission to CF Ward, ITU
or HDU
X Ray Social Worker Ultra Sound Bone Scan (Metabolic
Bone)
Pharmacy
Combined
clinics, Diabe-tes, Met
Bone,
Lung Trans-
plant (Newcastle/
Papworth/
Elsewhere)
Transition Clinic
Psychologists
Cashiers Of-fice (Some)
Patient Trans-port
PURPOSE
PROCESSES
PROFESSIONALS
PATIENTS PATTERNS
______________________________________
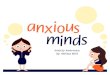
What do the staff think?—Survey
I am treated with respect every day by everyone
that works in clinic
0
2
4
6
8
10
12
14
Strongly agree Agree Disagree Strongly
Disagree
Nu
mb
er
of
res
po
nd
ers
I am given everything I need - Equipment and
encouragement to allow me to do my work to the
best of my ability
0
2
4
6
8
10
12
14
Strongly Agree Agree Disagree Strongly
Disagree
Nu
mb
er
of
res
po
nd
ers
How easy was it to ask anyone a question about the
care we provide?
0
2
4
6
8
10
12
14
Very Easy Easy Difficult Very Difficult
Nu
mb
er
of
res
po
nd
ers
How would you rate other people's morale and their
attitudes about working here?
0
2
4
6
8
10
12
14
Excellent Very good Good Fair Poor
Nu
mb
er
of
res
po
nd
ers
•To be more time efficient, a faster more efficient flow of patients, reduce waiting times•To have better access to the full MDT•To have flexible appointments•Nicer facilities•Things to do while waiting – TV, refreshments•Better building, complete overhaul, decent waiting room, overall nicer environment, cleaner rooms, improve decor•Closer proximity to ward•A unit administrator – to make us more organised & efficient•Less pharmacy wait, rapid access to pharmacy prescriptions•More physio input•More pharmacy input•Quicker clinic visits•Better parking facilities
•To be time efficient, more stream-lined, produce less waste•To have better scheduling of activities, job roles for individuals•To have a nicer environment to work in, better building, more space, up to date equipment and furniture •To improve staffing levels to allow better attendance at clinic for junior trainees•Improved ambulance/ patient transport efficiency – reduce late working hours, angst of patients and families •A doctors room, private room with desk to be able to dictate away from phone/chat•Sluice for dealing with specimens, urine, faeces.•To be closer to CF ward•Better integration between ward and OPD service•Better communication with CF ward•Clarity of roles with all the changes•Patient management system to improve quality of care•Improved time keeping by patients in terms of arrival times and reduced DNA
Waiting in clinic & other data
patterns?
The Sheffield CF population; the UK population and our closest neighbours (Leeds) This table identifies some outcomes and some process measures that are probably markers of quality.
I have largely used parameters available in PORT CF
Total CF population: 142 currently
PORT CF 136 patients named on end of year survey for 2010 – this value used
Characteristic Sheffield
Leeds
UK
FEV1 *65% *62.5% *64.9%
BMI *20.5 *21.8 *21.8
PEG Feeds
Proportion of adult
clinic receiving PEG
feeds
*15 patients/ 136 =
11.03%
†12% *6.8%
Number of days home
IVs over the year
(averaged across all
adult patients)
*89 pts had home iv’s
No. of iv days = 3538
Average no. iv days for
those who had iv’s=
39.75%
Ave no. iv’s across
total pt population =
26.01%
NA NA
Number of days
hospital IVS over the
year
(averaged across all
adult patients)
*52 pts had hospital
iv’s
No. iv days = 1653
Ave no. for those who
had hosp iv’s = 31.79%
Ave no. across total cf
popn = 12.15%
NA NA
Long term oxygen
prescribed to be used
continuously
*3/ 136 = 2.21% NA *1.9%
NIV (any use) *7/136 = 5.15% NA *3.5%
Treatment for CFRD
(see next table re
breakdown in CFRD)
◊*22/136 = 16.18% NA *26.8%
Patients over 16 on
DNase
*71/136 = 52.21% ¥43.6%
Patients with chronic
pseudomonas on
nebulised antibiotic ₣
*96 patients on
PORTCF with
pseudomonas
₣82%
Patients with
transiently raised
creatinine (important marker of adverse outcome)
Will need to review
hospital ICE system
Data sources *PORT CF 2009 Adults
†Leeds guide
‡ NGH data source ¥ This is an average of the % across 5 year age groups from PORT CF with tendency for older patients to receive less DNAse
₣ Unfortunately it is very difficult to accurately determine this from PORT CF since the data field includes chronic macrolides,
but the UK standard is that 90% of patients with chronic pseudomonas should be on a nebulised antibiotic so it is worth us finding these data. I have reviewed a list of those pt in 2010 with label Pseudomonas on port cF. I have then reviewed Lists of
patients on Tobramycin, and again for Colistin & then Promixin and then collated this information on the 3rd table
Notes re data collection
1. PORTCF is not very intuitive
2. PORTCF data is only as good as the data inputted
Outcome Measures?
Social Patterns
• Weekly MDT meeting discusses patients attending
clinic
• Ad hoc but regular consultant communication
• No formal CF leadership meeting (Dr, Nurse,
Management)
• Thank you‘s displayed in Nurse Area
• No regular improvement meeting
Who are your supporting microsystems?
What are the Team Patterns?
How long do they take?
3