Embed Size (px)
Citation preview

3/11/2017
1
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
What’s in that wound bed? Slough, Eschar, or Biofilm?
Linda J. Cowan, PhD, ARNP, FNP-BC, CWS
Disclosures
• Employed as a Research Health Scientist, North
Florida/South Georgia Veterans Health System,
Gainesville, FL.
• Research funding received from:
– VA
– Biomonde
– Healthpoint
– Smith & Nephew
– Hollister
– Medline
• This material is the result of work supported with
resources and the use of facilities at the VA.
3/11/2017
2
Disclaimers
Speaker does not endorse any one •
particular company’s products, is not
employed by industry, has no financial
interest in the listed commercial
companies.
Contents of this presentation do • not
represent the views of the U.S.
Department of Veterans Affairs or the
United States Government
Participants will describe:
• Key characteristics of chronic non-
healing wounds
• Impediments to wound healing
• Characteristics of slough, eschar, and
biofilm in open wounds
• Evidence-based approaches to address
or remove slough, eschar, and biofilm
from open wounds
• Potential antibiofilm treatment strategies
3/11/2017
3
Chronic Wounds vs. Acute Wounds
• All chronic wounds begin as acute
wounds
• Common chronic wounds
– Venous ulcers of the lower extremities
– Diabetic foot ulcers
– Pressure ulcers
– Complex trauma and surgical wounds
Key characteristics of chronic wounds
Imbalanced at microcellular level •
Stuck in inflammatory phase• 1-4
High MMPs / Low TIMPs (inverse correlation)–
High inflammatory cytokines–
Low growth factors–
Fibroblast inhibition– 5
Does • not follow expected pathway to
healing (less than 50% improvement in 4
weeks)6
3/11/2017
4
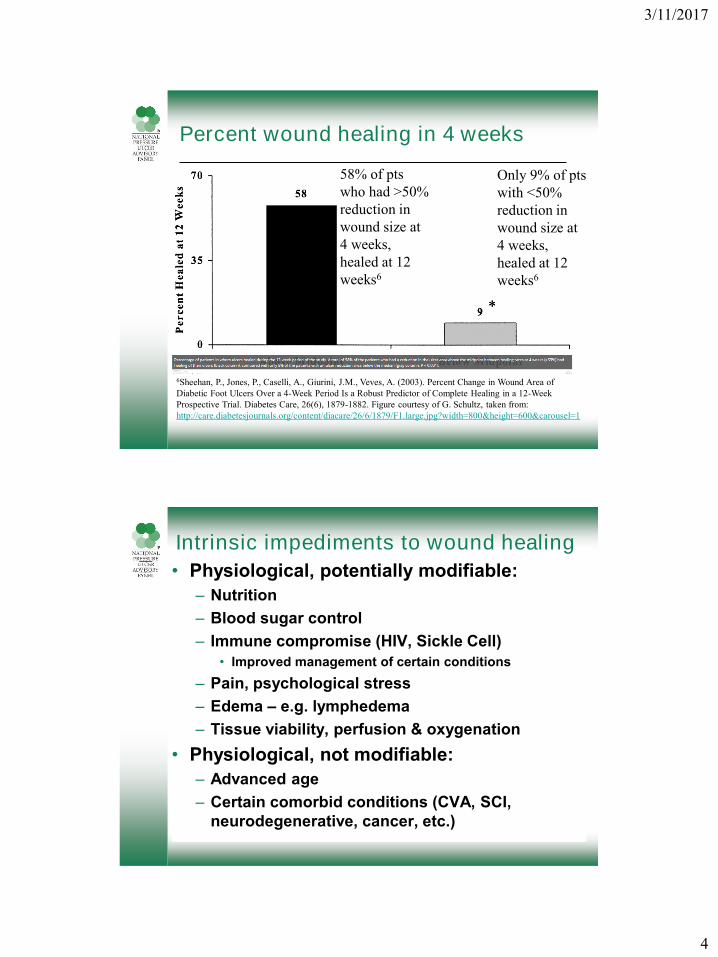
Percent wound healing in 4 weeks
6Sheehan, P., Jones, P., Caselli, A., Giurini, J.M., Veves, A. (2003). Percent Change in Wound Area of
Diabetic Foot Ulcers Over a 4-Week Period Is a Robust Predictor of Complete Healing in a 12-Week
Prospective Trial. Diabetes Care, 26(6), 1879-1882. Figure courtesy of G. Schultz, taken from:
http://care.diabetesjournals.org/content/diacare/26/6/1879/F1.large.jpg?width=800&height=600&carousel=1
58% of pts
who had >50%
reduction in
wound size at
4 weeks,
healed at 12
weeks6
Only 9% of pts
with <50%
reduction in
wound size at
4 weeks,
healed at 12
weeks6
Intrinsic impediments to wound healing
Physiological, potentially modifiable:•
Nutrition–
Blood sugar control–
Immune compromise (HIV, Sickle Cell)–
Improved management of certain conditions •
Pain, psychological stress–
Edema – – e.g. lymphedema
Tissue viability, perfusion & oxygenation–
Physiological, not modifiable:•
Advanced age –
Certain comorbid conditions (CVA, SCI, –
neurodegenerative, cancer, etc.)
3/11/2017
5
Extrinsic impediments to wound healing - potentially modifiable14
– Medications
• chemotherapy, steroids, anticoagulants
– Persistent or repetitive trauma
• immobility - failure to off-load, inappropriate shoes or
mobility devices, wet-to-dry dressings
– Exposure
• Smoking/nicotine, alcoholism
• Environmental, toxic chemicals, hygiene (personal &
environmental), parasites, pets, etc.
– Physical barriers
• Rolled wound edges, non-viable tissue (slough, fibrin,
eschar)
– Invasion – virulent pathogens (biofilm)
T-I-M-E-(s) Principle for WBP1,8,9
T - remove non-viable Tissue in wound
I - address Infection (prevent, treat,
remove problematic organisms/biofilm)
M – manage Moisture34
E – address wound Edges
S – address Surrounding Skin
3/11/2017
6
Documenting wound assessments
Location•
Suspected etiology, contributing factors•
Size (W X L X D in cm)•
Undermining, tunneling (clock method)•
Exudate (color, amount, odor)•
Wound bed tissue (color, amount viable)•
Wound edges and surrounding tissue•
Last treatments used, compliance, •
wound response, patient/CG education
Describing wound tissue
• Color of wound bed (in percentages)
• Viable (living tissue with good perfusion)
• Non-viable (dead/dying host tissue)
• Boggy (wet spongy consistency)
• Fluctuant (moving in waves, movable &
compressible, variable/unstable)
• Friable (bleeds easily with light touch)
• Hypergranulating (overgrowing baseline)
• Pale (anemic looking)
3/11/2017
7
Characteristics of slough in wounds
• What it is13
– Non-viable host tissue (or “avascular fat”)
– Typically it is moist, white, yellow, grey, or tan
dead tissue; loose or adherent; includes white
blood cells, fibrin, and other proteins
– May have “chicken fat” appearance
• What it is not
– Alive – slough by itself is not living tissue
• Slough will not “grow” on dressings
– Biofilm - may have bacteria/biofilm on it
– ?Blood clot, dried exudate, softened scab?
Fibrin35
Fibringen• is a glycoprotein in vertebrates
that helps in formation of blood clots.
Fibrin• is an insoluble, non-globular protein
formed from fibrinogen during the clotting of
blood. It is formed by the action of the
protease thrombin (clotting enzyme) on
fibrinogen which causes it to polymerize.
The polymerized • fibrin, together with
platelets form a hemostatic plug or clot over a
wound site. 35Laurens, N., Koolwijk, P., DeMaat, M/P. (2006). Fibrin Structure and wound healing. Journal
of Thrombosis and Haemostasis, 4:932-939.
3/11/2017
8
Slough
• Best ways to remove
Characteristics of eschar in wounds
• What it is
– Dry, dead host tissue
• What it is not
– Scab / crust (dried exudate)
– Dry Gangrene (condition where tissue dies
caused by ischemia due to underlying illness,
injury, and/or infection). Fingers, toes, & limbs
most often affected.
• When not to remove
– If providing reliable protective barrier
3/11/2017
9
Eschar
• When to remove
– Integrity is compromised (no longer acting as
body “bandaid”)
– Impediment to healing
• Best ways to remove
Biofilm – What is it?
• “Any group of microorganisms in which cells stick to
each other and often these cells adhere to a
surface. These adherent cells are frequently
embedded within a self-produced matrix of
extracellular polymeric substance (EPS).” Wikipedia
• “Van Leeuwenhoek, using his simple microscopes,
first observed microorganisms on tooth surfaces
and can be credited with the discovery of microbial
biofilms.” Rodney Donlan (2002). Biofilms: Microbial
Life on Surfaces. Emerging Infectious Diseases, 8(9),
881-890.
3/11/2017
10
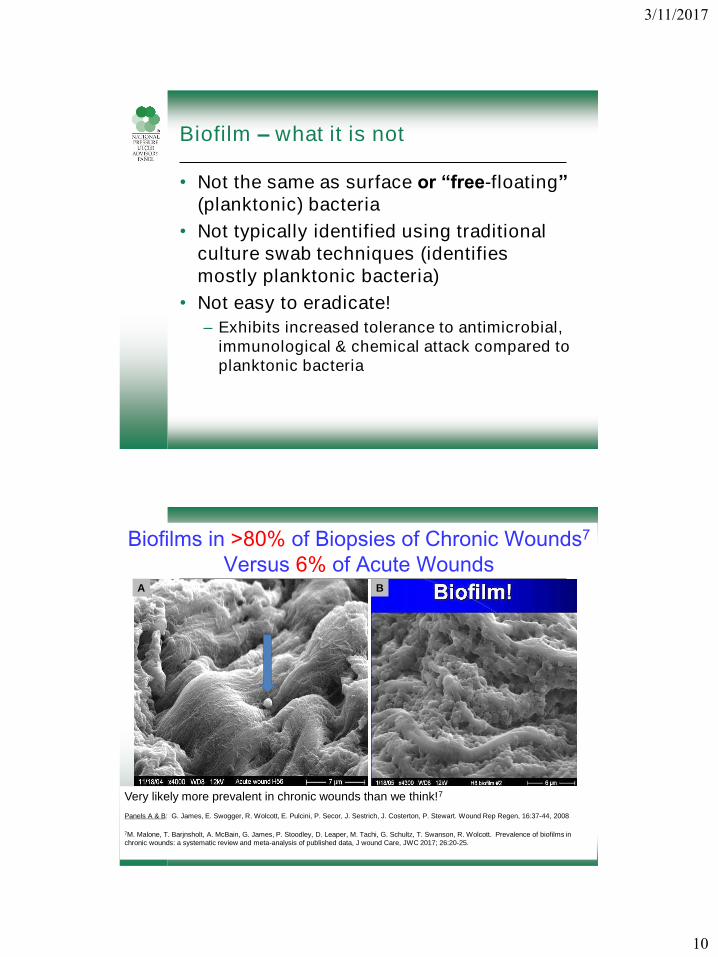
Biofilm – what it is not
• Not the same as surface or “free-floating”
(planktonic) bacteria
• Not typically identified using traditional
culture swab techniques (identifies
mostly planktonic bacteria)
• Not easy to eradicate!
– Exhibits increased tolerance to antimicrobial,
immunological & chemical attack compared to
planktonic bacteria
Biofilms in >80% of Biopsies of Chronic Wounds7
Versus 6% of Acute Wounds
Very likely more prevalent in chronic wounds than we think!7
Panels A & B: G. James, E. Swogger, R. Wolcott, E. Pulcini, P. Secor, J. Sestrich, J. Costerton, P. Stewart. Wound Rep Regen, 16:37-44, 2008
7M. Malone, T. Barjnsholt, A. McBain, G. James, P. Stoodley, D. Leaper, M. Tachi, G. Schultz, T. Swanson, R. Wolcott. Prevalence of biofilms in
chronic wounds: a systematic review and meta-analysis of published data, J wound Care, JWC 2017; 26:20-25.
A B
3/11/2017
11
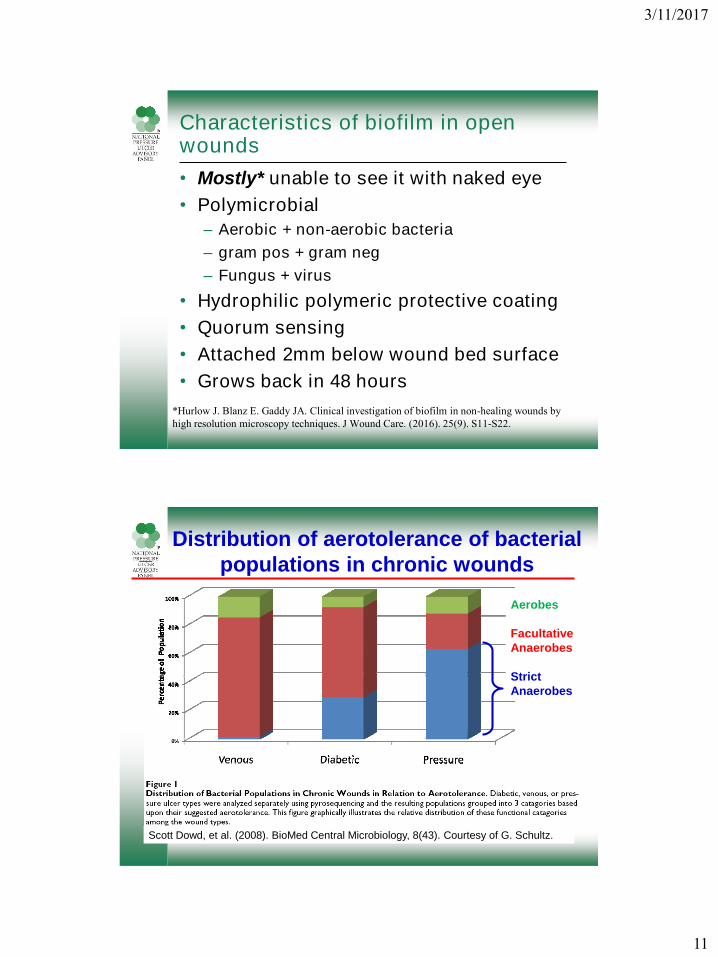
Characteristics of biofilm in open wounds
• Mostly* unable to see it with naked eye
• Polymicrobial
– Aerobic + non-aerobic bacteria
– gram pos + gram neg
– Fungus + virus
• Hydrophilic polymeric protective coating
• Quorum sensing
• Attached 2mm below wound bed surface
• Grows back in 48 hours
*Hurlow J. Blanz E. Gaddy JA. Clinical investigation of biofilm in non-healing wounds by
high resolution microscopy techniques. J Wound Care. (2016). 25(9). S11-S22.
Scott Dowd, et al. (2008). BioMed Central Microbiology, 8(43). Courtesy of G. Schultz.
Distribution of aerotolerance of bacterial
populations in chronic wounds
Aerobes
Facultative
Anaerobes
Strict
Anaerobes
3/11/2017
12
Why are bacteria in biofilms so difficult to kill?
1. Extracellular polymeric substance (EPS) of
biofilm • Dense matrix impairs diffusion of large antibodies
• EPS materials chemically react (neutralize) microbicides
• Negative charges of polysaccharides and DNA bind
cationic molecules like Ag+, antibiotics, PHMB+
2. Persister bacteria have low metabolic activity• Antibiotics only kill metabolically active bacteria
3. Oxygen diffusion to center of biofilm is limited• Promotes growth of anaerobic bacteria
4. Synergism between different bacteria• MRSA secrete resistance proteins
• Pseudomonas secrete catalase that destroys H2O2
Slide material: Courtesy of G. Schultz, PhD
Biofilm
• When to remove
– When biofilm presence has negative
consequences
– When interferes with wound healing
– When especially virulent (β hemolytic
streptococci)
– To prevent re-growth
• Best ways to remove
– DEBRIDEMENT
– Total kill
3/11/2017
13
Evidence for debridement methods
• Sharp
– Scalpel, scissors, curette
• Enzymatic (collagenase)
– Pros (gentle) Cons (slow)
• Autolytic (exudate/MMPs)
– Pros (gentle) Cons (slow)
• Ultrasonic (low and high frequency)
– With and without forced water
• Mechanical (debriding gauze, wet-to-dry)
– Surfactants (w/wo mechanical wiping)
• Larval/biological – medicinal maggots
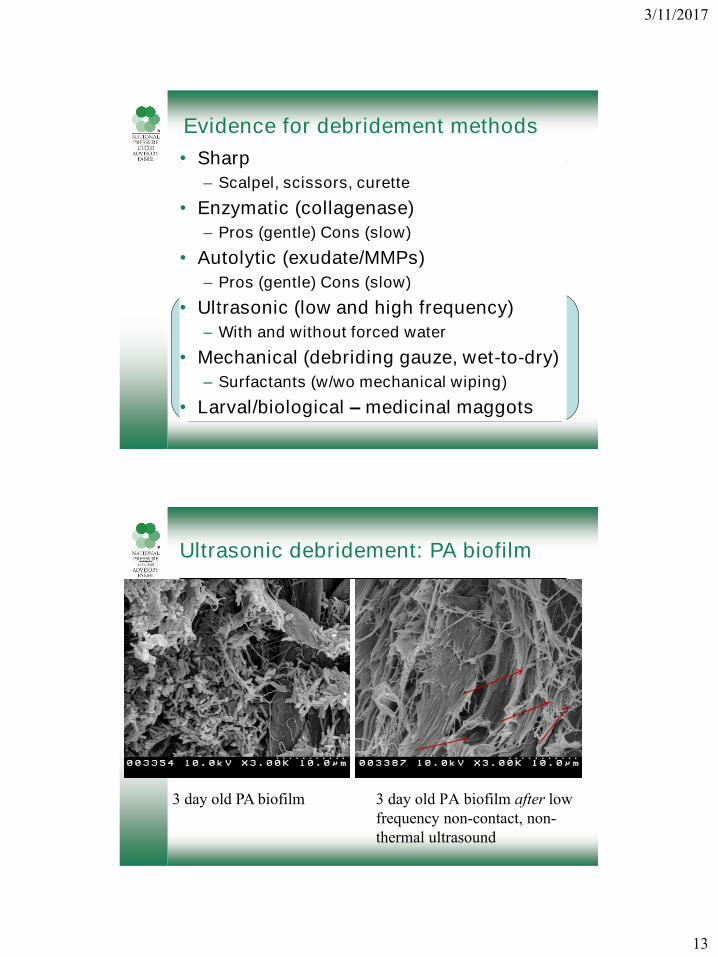
Ultrasonic debridement: PA biofilm
3 day old PA biofilm 3 day old PA biofilm after low
frequency non-contact, non-
thermal ultrasound
3/11/2017
14
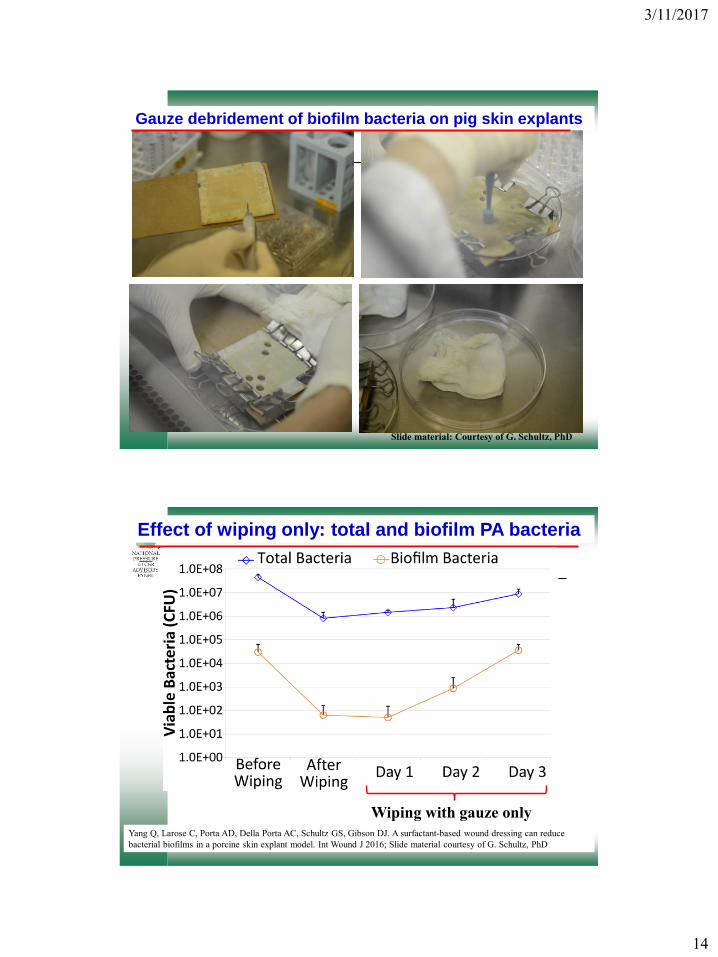
Gauze debridement of biofilm bacteria on pig skin explants
Slide material: Courtesy of G. Schultz, PhD
Effect of wiping only: total and biofilm PA bacteria
Wiping with gauze only
Yang Q, Larose C, Porta AD, Della Porta AC, Schultz GS, Gibson DJ. A surfactant-based wound dressing can reduce
bacterial biofilms in a porcine skin explant model. Int Wound J 2016; Slide material courtesy of G. Schultz, PhD
3/11/2017
15
Yang Q, Larose C, Porta AD, Della Porta AC, Schultz GS, Gibson DJ. A surfactant-based wound dressing
can reduce bacterial biofilms in a porcine skin explant model. Int Wound J 2016; Slide material courtesy of
G. Schultz, PhD
Wiping + Surfactant
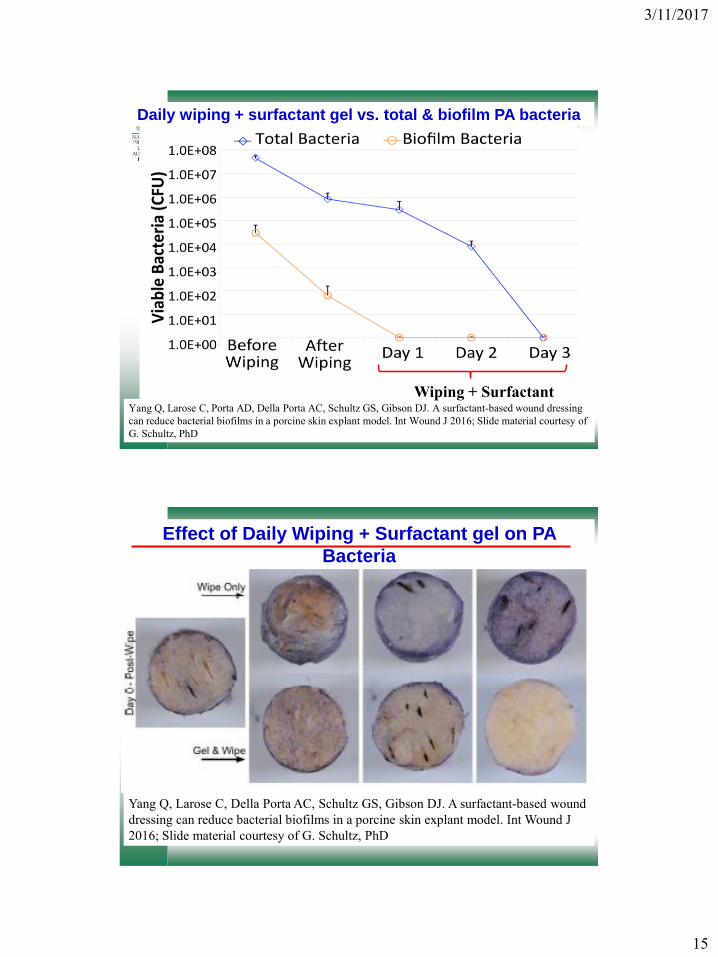
Daily wiping + surfactant gel vs. total & biofilm PA bacteria
Effect of Daily Wiping + Surfactant gel on PA
Bacteria
Yang Q, Larose C, Della Porta AC, Schultz GS, Gibson DJ. A surfactant-based wound
dressing can reduce bacterial biofilms in a porcine skin explant model. Int Wound J
2016; Slide material courtesy of G. Schultz, PhD
3/11/2017
16
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
1.0E+00
1.0E+01
1.0E+02
1.0E+03
1.0E+04
1.0E+05
1.0E+06
1.0E+07
1.0E+08
Before Wiping After Wiping Day 1 Day 2 Day 3
Via
ble
Bacte
ria (
CF
U)
Total Bacteria Biofilm Bacteria
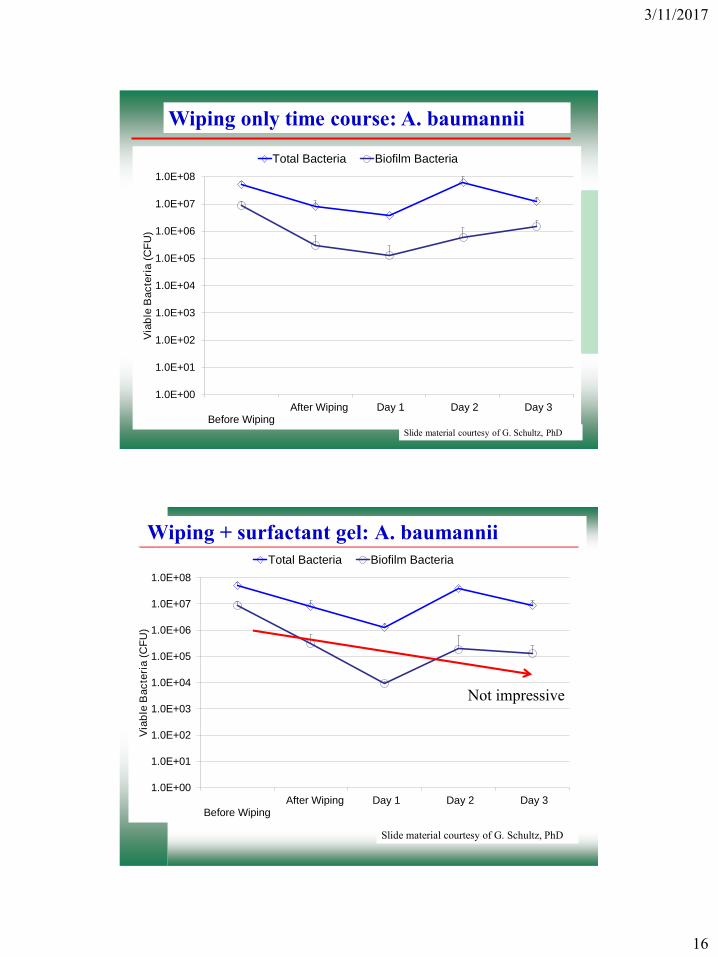
Wiping only time course: A. baumannii
Slide material courtesy of G. Schultz, PhD
1.0E+00
1.0E+01
1.0E+02
1.0E+03
1.0E+04
1.0E+05
1.0E+06
1.0E+07
1.0E+08
Before Wiping After Wiping Day 1 Day 2 Day 3
Via
ble
Bacte
ria (
CF
U)
Total Bacteria Biofilm Bacteria
Wiping + surfactant gel: A. baumannii
Not impressive
Slide material courtesy of G. Schultz, PhD
3/11/2017
17
1.E-01
1.E+00
1.E+01
1.E+02
1.E+03
1.E+04
1.E+05
1.E+06
1.E+07
1.E+08
0 24 48 72 96
Hours
Gauze Surfactant Gel
Surfactant Gel with 2% Mupirocin Surfactant Gel with 8.5% Mafenide Acetate
Co
lon
y Fo
rmin
g U
nit
s
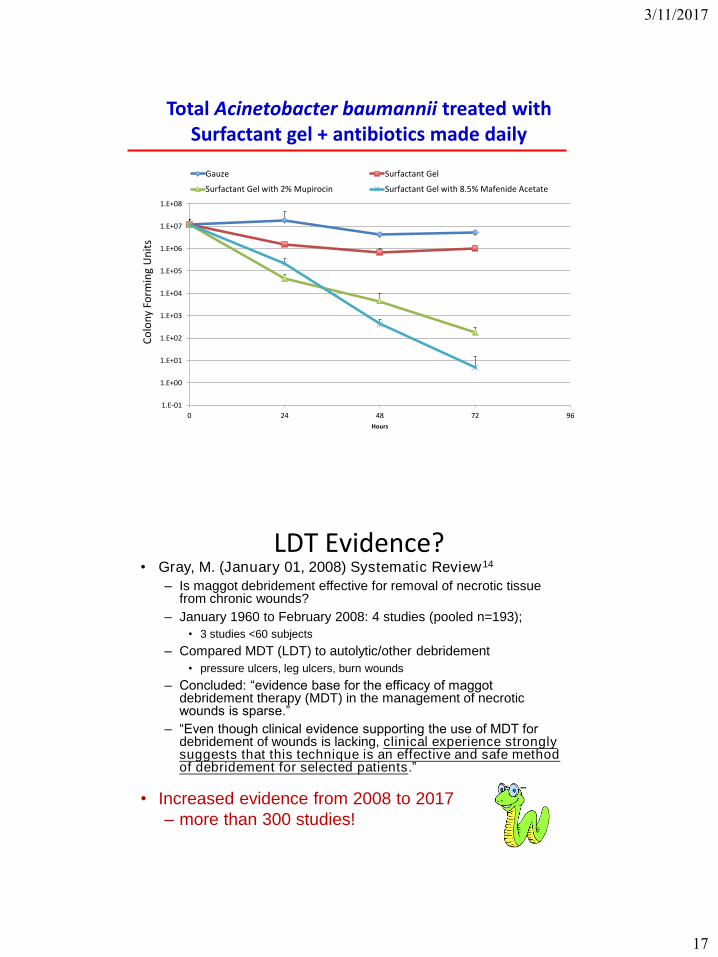
Total Acinetobacter baumannii treated withSurfactant gel + antibiotics made daily
LDT Evidence?• Gray, M. (January 01, 2008) Systematic Review14
– Is maggot debridement effective for removal of necrotic tissue from chronic wounds?
– January 1960 to February 2008: 4 studies (pooled n=193);
• 3 studies <60 subjects
– Compared MDT (LDT) to autolytic/other debridement
• pressure ulcers, leg ulcers, burn wounds
– Concluded: “evidence base for the efficacy of maggot debridement therapy (MDT) in the management of necrotic wounds is sparse.”
– “Even though clinical evidence supporting the use of MDT for debridement of wounds is lacking, clinical experience strongly suggests that this technique is an effective and safe method of debridement for selected patients.”
• Increased evidence from 2008 to 2017
– more than 300 studies!
3/11/2017
18
Evidence for larval debridement
Multiple actions of • Lucilia sericata larvae in hard-to-heal wounds: Larval
secretions contain molecules that accelerate wound healing, reduce
chronic inflammation and inhibit bacterial infection.
Cazander, G., Pritchard, D. I., Nigam, Y., Jung, W., & Nibbering, P. H. (– 2013).
Bioessays, 35(12), 1083-1092.
A • randomized controlled trial of larval therapy for the debridement of leg
ulcers: Results of a multicenter, randomized, controlled, open, observer
blind, parallel group study.
Mudge– , E., Price, P., Neal, W., & Harding, K. G. (2014). Wound Repair and
Regeneration, 22, 1, 43-51.
Selective • Antibiofilm Effects of Lucilia sericata Larvae Secretions /
Excretions against Wound Pathogens. Bohova, Jana, Majtan, Juraj,
Majtan– , Viktor, & Takac, Peter. (2014). Hindawi Publishing Corporation.
Antimicrobial • peptides expressed in medicinal maggots of the blow fly
Lucilia sericata show combinatorial activity against bacteria.
– Poppel, A. K., Vogel, H., Wiesner, J., & Vilcinskas, A. (2015). Antimicrobial Agents and
Chemotherapy, 59(5), 2508-14.
LDT – mechanisms of action
• Larval enzymes: protease, collagenase, ammonia, allantoin
and urea, lysozymes20,22,25,26,28,33
• Increase in alkalinity - breaks down necrotic tissues26-28,31,33
• Antimicrobial action of LDT secretions: peptides (diptericins,
lucifensin); chymotrypsin disrupts protein adhesion-
mediated biofilm formation; crude methanol extract21-25, 29-31
• Improved antibiotic effectiveness (re-susceptibility to
antimicrobials observed after LDT)29
• Stimulate fibroblast proliferation and promote fibroblast
motility; may improve angiogenesis (amino acid derivatives),
vascular perfusion, and tissue oxygenation; may reduce
scarring; reduces inflammation20, 26-28, 32, 33
3/11/2017
19
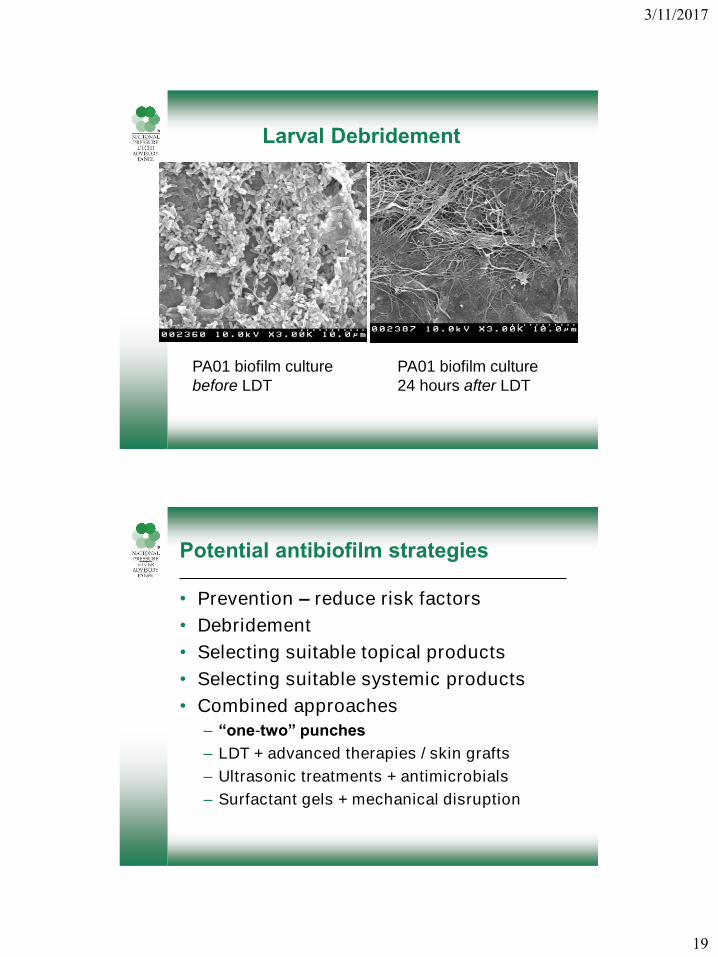
Larval Debridement
PA01 biofilm culture
24 hours after LDT
PA01 biofilm culture
before LDT
Potential antibiofilm strategies
• Prevention – reduce risk factors
• Debridement
• Selecting suitable topical products
• Selecting suitable systemic products
• Combined approaches
– “one-two” punches
– LDT + advanced therapies / skin grafts
– Ultrasonic treatments + antimicrobials
– Surfactant gels + mechanical disruption
3/11/2017
20
What is in that chronic wound bed?Slough, Eschar, Biofilm?
Summary
• Examine – not only with naked eye
• Determine - what is it?
• Address – targeted treatment
• Evaluate treatment effectiveness, wound progress
• Prevent regrowth
Special Thanks
To our US Veterans and their families
Micah Flores, PhD
Gregory Schultz, PhD
Dan Gibson, PhD
Qingping Yang, MS
Josh Yarrow, PhD
Gary Wang, MD, PhD
Randall Wolcott, MD
Cynthia Garvan, PhD
Alessandra Della Porta (UF Student)
Meg Kincaid, BS
Casey Bopp, RN

3/11/2017
21
Questions?
• Contact information:
Specific References
1. Schultz, G. S., Sibbald, R. G., Falanga, V., Ayello, E. A., Dowsett, C.,
Harding, K., Romanelli, M., ... Vanscheidt, W. (2003). Wound bed
preparation: a systematic approach to wound management. Wound Repair
and Regeneration: Official Publication of the Wound Healing Society [and]
the European Tissue Repair Society, 11, 1-28.
2. Trengove, N.J., Stacey, M.C., Macaulley, S., Bennett, N., Gibson, J.,
Burslem, F., Murphy, G., Schultz, G. (1999). Analysis of the acute and
chronic wound environments: the role of proteases and their inhibitors.
Wound Repair and Regeneration, 7, 442-452.
3. Demidova-Rice, T., Hamblin, M.R., Herman, I.M. (2012). Acute and Impaired
Wound Healing: Pathophysiology and Current Methods for Drug Delivery,
Part 1: Normal and Chronic Wounds: Biology, Causes, and Approaches to
Care. Adv Skin Wound Care, 25(7), 304–314.
4. Schultz, G. (2014). Molecular and cellular regulation of wound healing: What
goes wrong when wounds fail to heal or heal too much?. London: Henry
Stewart Talks. http://hstalks.com/lib.php?t=HST186.3834&c=252.
5. Harding, K. G., Moore, K., & Phillips, T. J. (2005). Wound chronicity and
fibroblast senescence - implications for treatment. International Wound
Journal, 2(4), 364-368.

3/11/2017
22
Specific References
Sheehan6. , P., Jones, P., Caselli, A., Giurini, J.M., Veves, A. (2003). Percent
Change in Wound Area of Diabetic Foot Ulcers Over a 4-Week Period Is a
Robust Predictor of Complete Healing in a 12-Week Prospective Trial.
Diabetes Care, 26(6), 1879-1882.
Malone7. , M., Barjnsholt, T., McBain, A.J., James, G.A., Stoodley, P.,
Leaper, D., Tachi, M., Shultz, G., Swanson, T., Wolcott, R.D. (2017). The
prevalence of biofilms in chronic wounds: a systematic review and meta-
analysis of published data. Journal of Wound Care, 25(12), 1-5.
Schultz8. , G. S., Barillo, D. J., Mozingo, D. W., & Chin, G. A. (April 01, 2004).
Wound bed preparation and a brief history of TIME. International Wound
Journal, 1(1), 19-32.
Leaper9. , D. J., Schultz, G., Carville, K., Fletcher, J., Swanson, T., & Drake,
R. (January 01, 2012). Extending the TIME concept: what have we learned
in the past 10 years? International Wound Journal, 9, 1-19.
Granick10. , M., Boykin, J., Gamelli, R., Schultz, G., & Tenenhaus, M.
(January 01, 2006). Toward a common language: surgical wound bed
preparation and debridement. Wound Repair and Regeneration, 14.
Specific References
11. Cowan, L., Phillips, P., Stechmiller, J., Yang, Q., Wolcott, R. & Schultz, G.
(2013). Antibiofilm Strategies and Antiseptics (Chapter 4) in Antiseptics in
surgery: Scientific basis, indications for use, evidence based
recommendations, vacuum instillation therapy; Willy, C., & Alt, V. (editors),
33 tables. Berlin: Lindqvist Book Publ.
12. Cowan, L., Phillips, P., Liesenfeld, B., Mikhaylova, A., Moore, D., Stechmiller,
J., & Schultz, G. (June 01, 2011). Caution: When Combining Topical Wound
Treatments, More Is Not Always Better. Wound Practice & Research: Journal
of the Australian Wound Management Association, 19(2), 60-64.
13. Swanson, T., Hurlow, J., Schultz, G., & Fletcher, J. (2014). Slough: What is
it? How do we manage it? International Wound Infection Institute.
http://www.woundinfection-institute.com/wp-
content/uploads/2014/11/Slough_AWMA_2014.pdf
14. Gray, M. (2008). Systematic Review: Is maggot debridement effective for
removal of necrotic tissue from chronic wounds? Journal of Wound, Ostomy,
and Continence Nursing, 35(4).

3/11/2017
23
Additional Resources & ReferencesWound Bed Preparation:
15. Doughty, D. & McNichol, L. (2016). Wound, Ostomy and Continence Nurses
Society® Core Curriculum: Wound Management 1st Edition. Chapter 2:
Wound healing (Janice Beitz). Lippincott Williams & Wilkins, Philadelphia, PA.
16. Enoch, S., Harding, K. (2003). Wound Bed Preparation: The Science Behind
the Removal of Barriers to Healing. Wounds, 15(7).
http://www.medscape.com/viewarticle/459733_5
17. Moffat, C., Falanga, V, Vowden, P. European Wound Management Association
(EWMA). Position Document: Wound Bed Preparation in Practice. London:
MEP Ltd, 2004. Available at:
http://www.woundsinternational.com/media/issues/87/files/content_49.pdf
Larval Debridement Therapy:
18. Cowan, L. J., Stechmiller, J. K., Phillips, P., Yang, Q., & Schultz, G. (2013).
Chronic Wounds, Biofilms and Use of Medicinal Larvae. Ulcers, 2013, 1, 1-7.
19. Sherman et al. (2013). Chapter 2 (Maggot Therapy) in Biotherapy-History,
Principles, and Practice: A Practical Guide to the Diagnostics and Treatment
of Disease Using Living Organisms, Springer Publishers: Netherlands.
20. Cazander, G., Schreurs, M. W. J., Renwarin, L., Dorresteijn, C., Hamann, D.,
& Jukema, G. N. (2012). Maggot excretions affect the human complement
system. Wound Repair and Regeneration, 20, 6, 879-886.
21. Kawabata, T., Mitsui, H., Yokota, K., Ishino, K., Oguma, K., & Sano, S. (2010).
Induction of antibacterial activity in larvae of the blowfly Lucilia sericata by an
infected environment. Medical and Veterinary Entomology, 24, 4, 375-381.
22. Harris, L. G., Nigam, Y., Sawyer, J., Mack, D., & Pritchard, D. I. (2013). Lucilia
sericata chymotrypsin disrupts protein adhesion-mediated staphylococcal biofilm
formation. Applied and Environmental Microbiology, 79, 4, 1393-5.
23. Teh, C. H., Nazni, W. A., Lee, H. L., Fairuz, A., Tan, S. B., & Sofian-Azirun, M.
(2013). Antibacterial activity and physicochemical properties of a crude methanol
extract of the larvae of the blow fly (Lucilia cuprina). Medical and Veterinary
Entomology, 27, 4, 414-420.
24. Bohova, Jana, Majtan, Juraj, Majtan, Viktor, & Takac, Peter. (2014). Selective
Antibiofilm Effects of Lucilia sericata Larvae Secretions/Excretions against Wound
Pathogens. Hindawi Publishing Corporation.
25. Valachova, I., Takac, P., & Majtan, J. (2014). Midgut lysozymes of Lucilia sericata -
new antimicrobials involved in maggot debridement therapy. Insect Molecular
Biology, 23, 6, 779-787
26. Cazander, G., Pritchard, D. I., Nigam, Y., Jung, W., & Nibbering, P. H. (2013).
Multiple actions of Lucilia sericata larvae in hard-to-heal wounds: Larval secretions
contain molecules that accelerate wound healing, reduce chronic inflammation and
inhibit bacterial infection. Bioessays, 35, 12, 1083-1092.
27. Li, P.-N., Li, H., Zhong, L.-X., Sun, Y., Yu, L.-J., Wu, M.-L., Zhang, L.-L., ... Lv, D.-C.
(2015). Molecular events underlying maggot extract promoted rat in vivo and human
in vitro skin wound healing. Wound Repair and Regeneration, 23, 1, 65-73.

3/11/2017
24
Bexfield28. , A., Bond, A. E., Morgan, C., Wagstaff, J., Newton, R. P., Ratcliffe, N. A.,
Dudley, E., ... Nigam, Y. (2010). Amino acid derivatives from Lucilia sericata
excretions/secretions may contribute to the beneficial effects of maggot therapy via
increased angiogenesis. British Journal of Dermatology, 162, 3, 554-562.
Arora, 29. Shuchi, Baptista, Carl, & Lim, Chu. (2011). Maggot metabolites and their
combinatory effects with antibiotic on Staphylococcus aureus. BioMed Central Ltd.
Beasley, W. D., & 30. Hirst, G. (2004). Making a meal of MRSA—the role of biosurgery
in hospital-acquired infection. Journal of Hospital Infection, 56, 1, 6-9.
Bohova31. , Jana, Majtan, Juraj, Majtan, Viktor, & Takac, Peter. (2014). Selective
Antibiofilm Effects of Lucilia sericata Larvae Secretions/Excretions against Wound
Pathogens. Hindawi Publishing Corporation.
Grassberger32. , M. (2013). Biotherapy-- History, principles and practice: A practical
guide to the diagnosis and treatment of disease using living organisms. Dordrecht:
Springer.
Horobin33. , A. J., & University of Nottingham. (2004). Maggots and wound healing:
The effects of Lucilia sericata larval secretions upon interactions between human
dermal fibroblasts and extracellular matrix proteins. Nottingham: University of
Nottingham.
Sibbald34. , R.G., Elliott, J.A., Ayello, E.A., Somayaji, R. (2015). Optimizing the
moisture management tightrope with wound bed preparation 2015. Advances in
Skin & Wound, 28(10), 466-476.
Laurens35. , N., Koolwijk, P., DeMaat, M/P. (2006). Fibrin Structure and wound
healing. Journal of Thrombosis and Haemostasis, 4:932-939.














![2. Pressure Ulcer to Zero - Zena UPDATED [Read-Only] thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan,](https://img.pdfslide.net/doc/110x75/5b0720f37f8b9a5c308de997/2-pressure-ulcer-to-zero-zena-updated-read-only-thickness-tissue-loss-in-which.jpg)














