Embed Size (px)
Citation preview

www.elsevier.com/locate/ygyno
Gynecologic Oncology
Whole abdominal radiotherapy in the adjuvant treatment of patients with
stage III and IV endometrial cancer: A Gynecologic Oncology
Group study
Gregory Suttona,*, Janice H. Axelrodb,1, Brian N. Bundyc, Tapan Royd, Howard D. Homesleye,
John H. Malfetanof,2, Borys R. Mychalczakg, Mary E. Kingh
aDivision of Gynecologic Oncology, St. Vincent’s Hospital and Health Services, 2001 W. 86th Street, Indianapolis, IN 46260, USAbGynecologic Oncology, Western Pennsylvania Hospital, Pittsburgh, PA 15224, USA
cStatistics, Gynecologic Oncology Group, Roswell Park Cancer Institute, Buffalo, NY 14263, USAdDepartment of Radiation Oncology, St. Louis University Health Science Center, St. Louis, MO 63110, USA
eWake Forest School of Medicine, Brookview Research, Inc., Winston-Salem, NC 27103, USAfGynecologic Oncology, Albany Medical College, Albany, NY 12208, USA
gDepartment of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, NY 10021, USAhClinical Pathology, Columbia University, New York, NY 10027, USA
Received 21 July 2004
Abstract
Objective. To evaluate toxicity, survival, and recurrence-free interval in women with loco-regionally advanced endometrial carcinoma
treated with postoperative whole abdominal radiation therapy.
Methods. Whole abdominal irradiation with pelvic plus or minus para-aortic boost was initiated within 8 weeks of total abdominal
hysterectomy, bilateral salpingo-oophorectomy, pelvic washings, and selective pelvic and para-aortic node sampling in eligible, consenting
patients.
Results. Of 180 evaluable patients entered on the study with surgically staged III and IV endometrial carcinoma maximally debulked
to less than 2 cm, 77 had typical endometrial adenocarcinoma and 103 had high-risk histology, either papillary serous or clear cell
carcinoma. Patients with typical endometrial adenocarcinoma were significantly younger and had significantly fewer poorly differentiated
cancers. Proportionally, there were twice as many non-Whites with high-risk histologies as non-Whites with typical endometrial
adenocarcinoma. Forty-five percent of patients with typical endometrial adenocarcinomas had positive pelvic nodes compared to 51% of
those with high-risk histologies. Both histologic groups had similar distribution for performance status, para-aortic node positivity, site
and extent of disease, and International Federation of Gynecology and Obstetrics (FIGO) stage. The frequency of severe or life-
threatening adverse effects among 174 patients evaluable for radiation toxicity included 12.6% with bone marrow depression, 15% GI,
and 2.2% hepatic toxicity. The recurrence-free survival rates were 29% and 27% (at 3 years) for the typical endometrial adenocarcinoma
and high-risk histologies, respectively. The survival rates were 31% and 35%, respectively. No patient with gross residual disease
survived.
Conclusion. Whole abdominal irradiation in maximally resected advanced endometrial carcinoma has tolerable toxicity, and it is
suggested that the outcome may be improved by this adjunctive treatment in patients with completely resected disease.
D 2005 Published by Elsevier Inc.
Keywords: Whole abdominal radiotherapy; WAR
0090-8258/$ - s
doi:10.1016/j.yg
* Correspondi
E-mail addr1 Current addr2 Current addr
97 (2005) 755 – 763
ee front matter D 2005 Published by Elsevier Inc.
yno.2005.03.011
ng author. Fax: +1 317 415 6749.
ess: [email protected] (G. Sutton).
ess: New Jersey Gynecologic Oncology, Little Silver, NJ 07739, USA.
ess: Associates in Gynecological Care, P.C., Albany, NY 12208, USA.

G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763756
Introduction
Endometrial cancer is the most common malignant neo-
plasm arising in the female reproductive tract. Although it has
the lowest death-to-case ratio of all gynecologic malignan-
cies, 6600 women die of advanced, recurrent, or metastatic
endometrial cancer every year in the United States [1].
Extirpative surgery followed in selected cases by pelvic
radiation therapy is capable of controlling stage I and II
disease in the majority of cases. Adjuvant therapy in stage III
and localized stage IV disease has not been well defined,
however, and appropriate treatment for patients with aggres-
sive papillary serous and clear cell cancers awaits delineation.
Based upon early favorable experience with ovarian
cancer at the M.D. Anderson Hospital, Greer and Hamburger
[2] suggested that whole abdominal radiotherapy utilizing a
moving-strip technique might be beneficial in treating
patients with endometrial cancer whose tumors had spread
to the abdominal cavity. They reported corrected and abso-
lute 5-year survivals of 80% and 63%, respectively, among
27 women with intraperitoneally-disseminated endometrial
cancer, none with residual disease greater than 2 cm in
diameter, who received whole abdominal moving-strip
radiotherapy with a pelvic boost. Of patients who developed
recurrent disease, three had within-field failures alone and
one had simultaneous abdominal and distant relapses.
Toxicity was limited to early severe enteritis and two
cases of ‘‘late’’ partial bowel obstruction and a vaginal ulcer.
Subsequent reports [3] of substantial small bowel toxicity
among patients with ovarian cancer treated with the
moving-strip technique led to the abandonment of this
procedure in favor of the whole abdominal ‘‘open-field’’
procedures in use at the present time.
Hendrickson et al. [4] first demonstrated that papillary
serous cancers of the endometrium were associated with an
extraordinary risk of relapse characterized by abdominal
failures, which were fatal in the vast majority of patients.
They were the first authors to suggest the use of adjuvant
abdominal radiotherapy in this disease entity.
The Gynecologic Oncology Group (GOG) initiated the
present study to determine feasibility, survival, and pro-
gression-free interval among patients with advanced endo-
metrial cancer of all histologic types treated with whole
abdominal radiotherapy with pelvic and, in the case of para-
aortic metastases, para-aortic boosts. A second major
objective was to determine the progression-free interval
and sites of recurrence among patients with stage I and II
papillary serous and clear cell carcinomas of the endome-
trium treated similarly. Results for this latter group of
patients will be discussed in a forthcoming publication.
Methods
This report summarizes results for patients with stage III
and IV endometrial cancer of all histologic subtypes. In the
present study, subjects were required to have pathologically-
confirmed primary endometrial cancer with clinical and/or
surgical stage III and IV disease without vaginal involve-
ment, parenchymal liver metastases, lung metastases, or
spread to extraperitoneal sites excluding retroperitoneal
lymph nodes. Papillary serous or clear cell histologies were
required to involve greater than 50% of tumor volume.
Patients with para-aortic lymph node metastases were
eligible only if scalene lymph node biopsy was negative.
Patients were ineligible if they had received pelvic or
abdominal radiation or chemotherapy, or were found to have
inadequate hematologic (WBC � 3000, platelets and
granulocytes � 1500 cells/cm), renal (creatinine > 2.0
mg%), or hepatic function (bilirubin or aspartate trans-
aminase (AST) > 2� normal). Also ineligible were patients
with GOG performance status of 4 and those with a previous
or concomitant malignancy except nonmelanoma skin
cancer. Written informed consent was obtained from all
patients prior to study entry in accord with institutional,
state, and federal regulations.
Pathology review
Peritoneal washings were to be obtained from the pelvis
and cytologically evaluated for malignant cells. The uterus
was to be evaluated for size, location of tumor, depth of
myometrial invasion, histologic type, and grade of tumor.
Lymph nodes and adnexa were also evaluated for the
presence and location of metastases. For each patient
entered, the GOG Pathology Committee reviewed appro-
priate slides documenting histological parameters. For
patients with papillary serous and clear cell histologies, all
slides were to be submitted for review.
Surgery
Enrollees were required to have total abdominal hyste-
rectomy, bilateral salpingo-oophorectomy, pelvic washings,
and selective para-aortic and pelvic lymph node sampling.
Omentectomy was not required; however, careful inspection
of the omentum was required as well as removal of sections
of the omentum with gross metastases. Tumor resection to
residual nodules of 2 cm or less was required. Previous
therapy with hormonal agents was permitted and patients
with recurrent endometrial cancer were allowed if all other
protocol requirements were met. Study entry was required
within 8 weeks of surgery.
Radiation therapy
Irradiation was to be initiated within 8 weeks of surgery;
all treatments were delivered by megavoltage equipment
ranging from that of cobalt-60 to maximum 25-MeV
photons. Minimal source-skin distance was 80 cm and dose
rates between 30 and 200 cGy/min at midplane were
required. Patients were to be treated with two pairs of
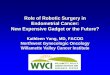
Table 1
Cell type distribution (N = 180)
Cell type Number
Clear cell 23
Papillary serous 80
Typical endometrial 77
Adenocarcinoma 10
Endometrioid 34
Glassy cell 1
Mixed epithelial 10
Adenosquamous 14
Villoglandular 7
Undifferentiated 1
Table 2
Patient characteristics
Characteristic Typical endometrial
(N = 77)
Papillary serous/clear
cell (N = 103)
No. (%) No. (%)
Age
<50 14 (18.2) 6 (5.8)
51–60 15 (19.5) 17 (16.5)
61–70 26 (33.8) 39 (37.9)
71–80 20 (26.0) 36 (35.0)
81+ 2 (2.6) 5 (4.9)
GOG performance status
0 32 (41.6) 38 (36.9)
1 41 (53.2) 58 (56.3)
2 4 (5.2) 7 (6.8)
3 0 (0.0) 0 (0.0)
Race
White 68 (88.3) 77 (74.8)
Black 6 (7.8) 21 (20.4)
Other 3 (3.9) 5 (3.9)
Grade
1 20 (26.0) 10 (9.7)
2 23 (29.9) 24 (23.3)
3 34 (44.2) 68 (66.0)
Unknown 0 (0.0) 1 (1.0)
G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763 757
parallel opposed fields (open-field technique) to the whole
abdomen and pelvis. The whole abdomen was to be treated
first, to a dose of 3000 cGy in 20 fractions of 150 cGy each.
A decrease in the daily fraction to 125 cGy per day was
allowed if gastrointestinal symptoms or leukopenia pre-
cluded use of the higher dose. After whole abdominal
radiation, the pelvis was boosted to a midplane dose of 1980
cGy at 180 cGy per fraction for eleven treatments. The
combined whole abdominal radiation and the total pelvic
radiation required 6–7 weeks.
Patients with positive para-aortic nodes were to receive
an additional boost of 1500 cGy for a total para-aortic dose
of 4500 cGy.
The whole abdominal field extended from 1 cm above
the top of the diaphragm to the bottom of the obturator
foramina. The lateral border extended 1.0–1.5 cm beyond
the lateral peritoneal margin. Full thickness posterior kidney
blocks were used throughout therapy. Blocking of the left
heart above the diaphragm was to be used and portions of
the lower lateral pelvic fields and femoral heads were also
blocked.
The pelvic field extended from the L5–S1 interspace
superiorly to the bottom of the obturator foramina inferiorly.
The lateral margins were 1.5 cm lateral to the medial rim of
the ilium.
The para-aortic boost field was bounded by the L5–S1
interspace inferiorly, the superior margin of the abdominal
field superiorly, and the lateral extent was 8 cm wide.
Interruptions in treatment exceeding 2 weeks in duration
disqualified patients from protocol therapy.
Radiation therapy and quality control were supervised by
the Radiologic Physics Center under the sponsorship of the
American Association of Physicists in Medicine. Accuracies
of T3% in source output and T5% in prescribed dose
delivery were required.
Statistical considerations
Evaluation parameters included recurrence-free survival
(RFI), survival time, and frequency and severity of adverse
effects. Survival was defined as observed length of life from
entry into study to death, or to date of last contact.
Recurrence-free interval was defined as the date from entry
into study to date of reappearance or increasing parameters
of disease or date of last contact.
Life tables and medians were computed using the method
of Kaplan and Meier [5]. Differences in recurrence-free
interval or survival by patient characteristics were evaluated
using the log-rank test [6]. The Pearson chi-square test was
used [7] to identify correlations between the two major
categories of cell type and patient and disease character-
istics. The Wilcoxon rank sum test [8] was used for age at
diagnosis and cell type categories.
Results
A total of 274 patients were entered in this study between
December 1986 and February 1994. Of these, 58 were
ineligible. Inadequate surgery excluded 20 patients, 22 had
wrong cell type, three had disease more advanced than
protocol criteria permitted, four failed criteria for advanced
stage, eight had a second primary malignancy, and one had a
non-endometrial primary.
Of the 214 evaluable patients, 34 had stage I or II papillary
serous or clear cell cancer and are the subject of a separate
report. Of the 180 patients analyzed in this study, 77 had stage
III or IV typical endometrial cancer and 103 patients had
stage IIIor IVpapillaryserousorclearcell carcinoma(Table1).
Characteristics of this patient population are detailed in Table
2. Patients with either papillary serous or clear cell carcinoma
were significantly older (P < 0.01) than those with typical
endometrioid cancers. The median age of the latter was 63
years (range: 32–81 years) compared with median age of
68.5 years (range: 39–85 years) for patients with papillary
Table 3
Extent of disease
Sitea Typical endometrial
(N = 77)
Papillary serous/clear
cell (N = 103)
No. No.
Pos. (%) Pos. (%)
Vagina 4 (5.2) 3 (2.9)
Fallopian tube 20 (26.0) 19 (18.4)
Ovarian 28 (36.4) 36 (35.0)
Ligament 7 (9.1) 6 (5.8)
Omentum 15 (19.5) 22 (21.4)
Small bowel 8 (10.4) 5 (4.9)
Colon 12 (15.6) 11 (10.7)
Gutter 3 (3.9) 6 (5.8)
Diaphragmb 1 (1.3) 8 (7.8)
Cul-de-sac 12 (15.6) 12 (11.7)
Abdominal wall 2 (2.6) 2 (1.9)
Bladder 7 (9.1) 10 (9.7)
Otherc 12 (15.6) 13 (12.6)
Pos. = positive findings.a Patients may have two or more sites involved.b Statistically significant difference (P = 0.05).c Includes appendix, peritoneum, spleen, umbilical, liver, para-ovarian
tissue, renal artery, psoas muscle, epiploic fat, mesentery, and abdominal
lymph nodes.
Table 5
Postoperative residual disease
Residual Typical endometrial Papillary serous/clear cell
No. (%) No. (%)
Microscopic 65 (84.4) 91 (88.3)
Gross 12 (15.6) 12 (11.7)
Total 77 (100.0) 103 (100.0)
Table 6
G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763758
serous cancers and median age of 71 years (range: 45–85
years) for patients with clear cell cancers. All groups had
similar mean GOG performance status. A larger proportion of
Black patients had papillary serous or clear cell cancers (21/
27 = 78%) than did Whites (77/145 = 53%). Additionally,
two-thirds of those with papillary serous or clear cell cancers
had tumors of grade 3 but less than half (44%) of those with
typical endometrioid tumors were grade 3. In Table 3, the
extent of disease by site is enumerated. Similar frequencies of
spread between the two groups were observed except for
diaphragm (1.3% vs. 7.8%, P = 0.05); also, similar
frequencies of lymph node spread were observed (Table 4).
The frequency of gross residual disease was similar in both
groups of patients (Table 5).
Toxicity
In Table 6, adverse events for the 174 patients evaluable
for toxicity of whole abdominal irradiation are summarized.
Six patients are inevaluable for adverse events because three
Table 4
Lymph node status
Node status Typical endometrial Papillary serous/Clear cell
No. (%) No. (%)
Pelvic nodes
Negative 42 (54.5) 50 (48.5)
Microscopic 18 (23.4) 30 (29.1)
Gross 17 (22.1) 23 (22.3)
Para-aortic nodes
Negative 47 (61.0) 71 (68.9)
Microscopic 16 (20.8) 20 (19.4)
Gross 14 (18.2) 12 (11.7)
refused radiotherapy, one accepted only pelvic radiotherapy,
and two additional patients were not treated because of
declining performance status and bipolar affective disorder
with schizophrenic features, respectively.
Twenty-two patients had grade 3 or 4 hematologic toxi-
city. One patient with WBC 1900/mm3 and platelet count
29,000/mm3 complicated by an infected lymphocyst did not
receive pelvic boost therapy. Grade 4 toxicity included a
WBC of 900/mm3 (patient removed from study), a platelet
count of 14,000/mm3, and a third patient with thrombocyto-
penia of 8000/mm3 1 week before therapy ended.
Nausea and diarrhea were the most common acute
gastrointestinal toxicities. In one patient, treatment was
delayed by an episode of diverticulitis, and a second patient
had a 2-day delay in radiotherapy and a subsequent
recurrence while under treatment. A third patient developed
a bowel obstruction secondary to progressive disease in the
upper abdomen. An additional patient was taken off study
after developing severe nausea and vomiting after 2 days of
abdominal radiotherapy; she subsequently received pelvic
radiotherapy and vaginal ovoids.
Grade 4 gastrointestinal toxicity was observed in seven
patients. Two had bowel obstructions associated with
progressive disease at 12 and 16 months. Three patients
who were NED developed obstructions requiring surgery at
10, 10, and 13 months; the first died of anastamotic
breakdown and sepsis postoperatively, the second patient
developed volvulus, subdiaphragmatic abscess, and sepsis at
2 months, and the third died of gastrointestinal hemorrhage,
pulmonary embolus, and congestive heart failure; both were
clinically NED. One patient died of a gastrointestinal bleed
5 months after therapy and a second died of hemorrhage
after anticoagulation for deep venous thrombosis 60 days
Adverse events
Adverse effect Grade (Frequency)
0 1 2 3 4
Hematologic 63 (36%) 35 (20%) 54 (31%) 19 (11%) 3 (2%)
Genitourinary 138 (79%) 32 (18%) 4 (2%) 0 0
Gastrointestinal 27 (15%) 42 (24%) 78 (45%) 20 (11%) 7 (4%)
Hepatic 165 (95%) 5 (3%) 0 3 (2%) 1 (1%)
Pulmonary 156 (90%) 11 (6%) 6 (3%) 1 (1%) 0
CV 159 (91%) 1 (1%) 2 (1%) 10 (6%) 2 (1%)
Neurologic 167 (96%) 3 (2%) 2 (1%) 2 (1%) 0
Cutaneous 118 (68%) 44 (25%) 10 (6%) 2 (1%) 0
Lymphatic 164 (94%) 6 (3%) 3 (2%) 1 (1%) 0
Fever 140 (85%) 26 (15%) 6 (3%) 2 (1%) 0
Other 159 (91%) 11 (6%) 2 (1%) 2 (1%) 0

Table 8
Survival by residual disease
Histology Gross Gross/Resected microscopic
Papillary 0 (2.5–33.5) 27.5 (1.3–57) 26 (1.4–141.9)
Clear cell 25 (2.6–42.1) 12.5 (2.6–17.8) 16.5 (8.8–99)
Endometrioid 0 (2.4–29) 47.3 (1.6–84) 18.4 (0.3–57.4)
G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763 759
postoperatively. A last patient developed nausea, diarrhea,
abdominal pain, malnutrition, and sepsis 9 months after
radiation therapy while being treated for disease recurrence.
She required peripheral hyperalimentation.
One patient had grade 4 and three had grade 3 hepatic
toxicity. The first patient developed cytologically-negative
ascites immediately after radiotherapy, and biopsy showed
liver necrosis. One patient developed cytologically-benign
ascites 26 days after radiotherapy and a second had a liver
biopsy demonstrating centrilobular veno-occlusive disease
felt to be consistent with radiotherapy and not viral hepatitis.
These latter two patients recovered without sequelae. An
additional patient had elevated liver function studies as well
as a pulmonary embolus and recurrent disease.
Cardiovascular adverse events included four pulmonary
emboli, two patients with congestive heart failure related to
atrial fibrillation, and one with postoperative atrial flutter.
One episode of severe hypertension occurred in a patient
who refused antihypertensive therapy. Two episodes of
hypotension occurred, one related to a postoperative epidural
anesthetic.
Patterns of failure and survival
Table 7 lists sites of failure for patients with typical
endometrial and papillary serous/clear cell cancers. Table 8
summarizes survival by residual disease.
Stage III and IV papillary serous tumors
Four subgroups were identified in patients with stage III
and IV papillary serous tumors, separated by surgical
Table 7
Site of recurrence
Sites Typical
endometrial
Papillary serous/
Clear cell
No. (%) No. (%)
NED 27 (35.1) 34 (33.0)
Recurred 50 (64.9) 69 (67.0)
Vagina 3 4
Pelvis 7 3
Abdomen 9 21
Retroperitoneal nodes 0 1
Lung 9 15
Othera 10 6
Lung and other 2 3
Abdomen and other 2 2
Pelvis and liver 1 0
Vagina and liver 0 1
Lung and pelvis 0 1
Abdomen and pelvis 1 4
Abdomen and lung 1 4
Vagina and lung 0 1
Retro. nodes and pelvis 0 1
Unknown 5 2
NED, no evidence of disease.a Includes axillary, groin, and supraclavicular lymph nodes, bone, brain,
spinal cord, liver, stomach, and bladder.
findings and residual disease. None of the eight patients
who had gross residual disease after surgery survived. Their
median disease-free survival was 4.8 months (range: 2.5–
33.5 months); six had abdominal failures while one each
had recurrences in lung and vagina and in an unknown site.
Median survival among these patients was 11.1 months
(range: 5.8–55.5 months). The longest survivor had
pulmonary metastases.
Twenty-nine patients had gross disease at the time of
surgery which was felt to be completely resected. Twenty
had malignant washings or ascites and nine had para-aortic
metastases with negative supraclavicular biopsies. Disease-
free survival ranged from 1.3 to 57 months (median: 12.0
months), and 21 (72.4%) patients died of disease from 1.6 to
72 months after therapy. Median survival for the group was
27.4 months. Failure in the abdomen (Tpelvis) occurred in
10 patients (34.5%) and seven (24.1%) had recurrences
which included the lung.
Forty-three patients qualified for the study because of
microscopic metastases. The most common site of spread
was pelvic lymph nodes (23 patients or 53.5%) either
alone or in combination with other spread. Thirteen
patients had para-aortic metastases and negative supra-
clavicular metastases and two had para-aortic metastases
without pelvic lymph node spread. Thirty-two of the 43
patients died: six of other causes, 23 of disease, 2 of
unknown causes, and 1 due to treatment. Median survival
and disease-free survival were 65 and 66 months (both
ranged 1.4–141.9 and 95 months), respectively. Among 26
patients with known recurrences, 9 (34.6%) included an
abdominal or pelvic component and six were confined to
the chest.
Stage III and IV clear cell cancers
Twenty-three patients had stage III (19) and IV (5) clear
cell cancers of the endometrium. Four patients had from 0.1
to 2.0 cm of residual disease after surgery and all but one
died of disease (one intercurrent death) between 2.6 and
42.1 months after treatment. Sites of failure included
vagina, pelvis, abdomen, and axillary lymph nodes. Four
of the five patients eligible for protocol because of
malignant peritoneal cytology alone were alive and free of
disease at 60.4 and 83 months follow-up, respectively; one
patient with malignant cytology died at 6.4 months of
abdominal failure.
The remaining patients had either completely-resected
gross disease (8) or microscopic (6) spread at the time of
surgery. All but one patient with gross residual disease
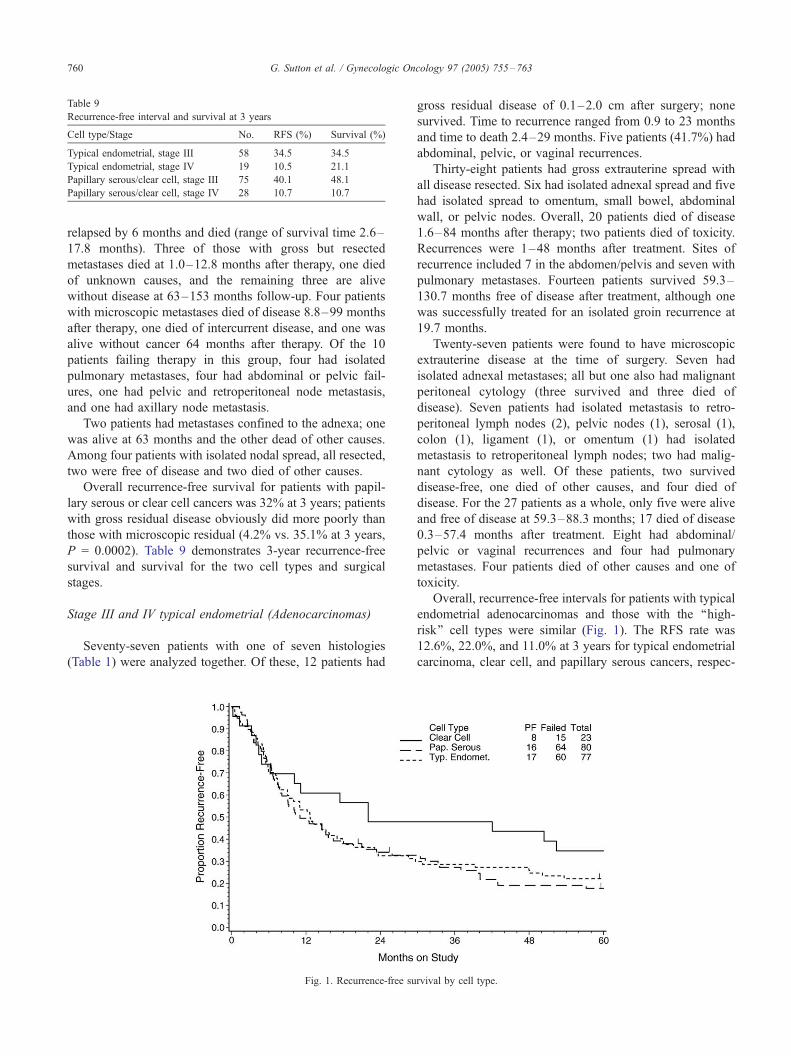
Table 9
Recurrence-free interval and survival at 3 years
Cell type/Stage No. RFS (%) Survival (%)
Typical endometrial, stage III 58 34.5 34.5
Typical endometrial, stage IV 19 10.5 21.1
Papillary serous/clear cell, stage III 75 40.1 48.1
Papillary serous/clear cell, stage IV 28 10.7 10.7
G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763760
relapsed by 6 months and died (range of survival time 2.6–
17.8 months). Three of those with gross but resected
metastases died at 1.0–12.8 months after therapy, one died
of unknown causes, and the remaining three are alive
without disease at 63–153 months follow-up. Four patients
with microscopic metastases died of disease 8.8–99 months
after therapy, one died of intercurrent disease, and one was
alive without cancer 64 months after therapy. Of the 10
patients failing therapy in this group, four had isolated
pulmonary metastases, four had abdominal or pelvic fail-
ures, one had pelvic and retroperitoneal node metastasis,
and one had axillary node metastasis.
Two patients had metastases confined to the adnexa; one
was alive at 63 months and the other dead of other causes.
Among four patients with isolated nodal spread, all resected,
two were free of disease and two died of other causes.
Overall recurrence-free survival for patients with papil-
lary serous or clear cell cancers was 32% at 3 years; patients
with gross residual disease obviously did more poorly than
those with microscopic residual (4.2% vs. 35.1% at 3 years,
P = 0.0002). Table 9 demonstrates 3-year recurrence-free
survival and survival for the two cell types and surgical
stages.
Stage III and IV typical endometrial (Adenocarcinomas)
Seventy-seven patients with one of seven histologies
(Table 1) were analyzed together. Of these, 12 patients had
Fig. 1. Recurrence-free su
gross residual disease of 0.1–2.0 cm after surgery; none
survived. Time to recurrence ranged from 0.9 to 23 months
and time to death 2.4–29 months. Five patients (41.7%) had
abdominal, pelvic, or vaginal recurrences.
Thirty-eight patients had gross extrauterine spread with
all disease resected. Six had isolated adnexal spread and five
had isolated spread to omentum, small bowel, abdominal
wall, or pelvic nodes. Overall, 20 patients died of disease
1.6–84 months after therapy; two patients died of toxicity.
Recurrences were 1–48 months after treatment. Sites of
recurrence included 7 in the abdomen/pelvis and seven with
pulmonary metastases. Fourteen patients survived 59.3–
130.7 months free of disease after treatment, although one
was successfully treated for an isolated groin recurrence at
19.7 months.
Twenty-seven patients were found to have microscopic
extrauterine disease at the time of surgery. Seven had
isolated adnexal metastases; all but one also had malignant
peritoneal cytology (three survived and three died of
disease). Seven patients had isolated metastasis to retro-
peritoneal lymph nodes (2), pelvic nodes (1), serosal (1),
colon (1), ligament (1), or omentum (1) had isolated
metastasis to retroperitoneal lymph nodes; two had malig-
nant cytology as well. Of these patients, two survived
disease-free, one died of other causes, and four died of
disease. For the 27 patients as a whole, only five were alive
and free of disease at 59.3–88.3 months; 17 died of disease
0.3–57.4 months after treatment. Eight had abdominal/
pelvic or vaginal recurrences and four had pulmonary
metastases. Four patients died of other causes and one of
toxicity.
Overall, recurrence-free intervals for patients with typical
endometrial adenocarcinomas and those with the ‘‘high-
risk’’ cell types were similar (Fig. 1). The RFS rate was
12.6%, 22.0%, and 11.0% at 3 years for typical endometrial
carcinoma, clear cell, and papillary serous cancers, respec-
rvival by cell type.
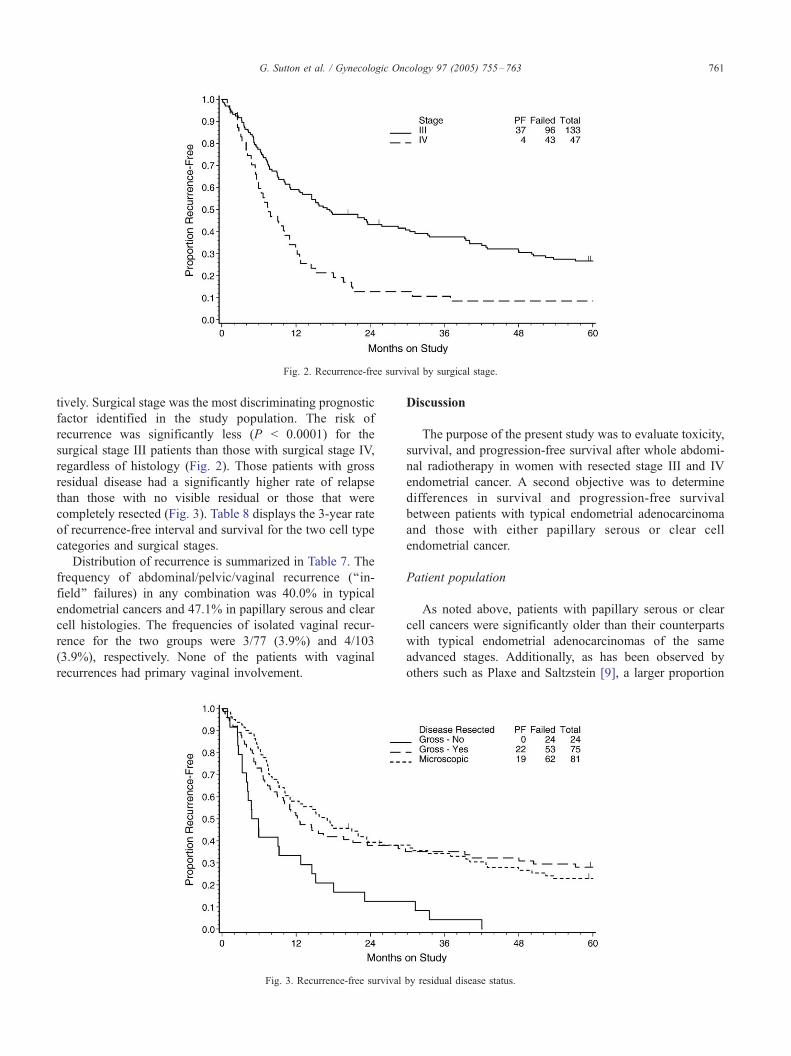
Fig. 2. Recurrence-free survival by surgical stage.
G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763 761
tively. Surgical stage was the most discriminating prognostic
factor identified in the study population. The risk of
recurrence was significantly less (P < 0.0001) for the
surgical stage III patients than those with surgical stage IV,
regardless of histology (Fig. 2). Those patients with gross
residual disease had a significantly higher rate of relapse
than those with no visible residual or those that were
completely resected (Fig. 3). Table 8 displays the 3-year rate
of recurrence-free interval and survival for the two cell type
categories and surgical stages.
Distribution of recurrence is summarized in Table 7. The
frequency of abdominal/pelvic/vaginal recurrence (‘‘in-
field’’ failures) in any combination was 40.0% in typical
endometrial cancers and 47.1% in papillary serous and clear
cell histologies. The frequencies of isolated vaginal recur-
rence for the two groups were 3/77 (3.9%) and 4/103
(3.9%), respectively. None of the patients with vaginal
recurrences had primary vaginal involvement.
Fig. 3. Recurrence-free survival
Discussion
The purpose of the present study was to evaluate toxicity,
survival, and progression-free survival after whole abdomi-
nal radiotherapy in women with resected stage III and IV
endometrial cancer. A second objective was to determine
differences in survival and progression-free survival
between patients with typical endometrial adenocarcinoma
and those with either papillary serous or clear cell
endometrial cancer.
Patient population
As noted above, patients with papillary serous or clear
cell cancers were significantly older than their counterparts
with typical endometrial adenocarcinomas of the same
advanced stages. Additionally, as has been observed by
others such as Plaxe and Saltzstein [9], a larger proportion
by residual disease status.

G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763762
of Black women had papillary serous cancers than did
White women. The proportion of those with lymph node
metastases was similar between the papillary serous or clear
cell and typical endometrial adenocarcinoma groups.
Toxicity
Given the advanced stage and, in many cases, age of the
cases treated in this series, toxicity was acceptable.
Hematologic toxicity was moderate, usually self-limited,
and did not interrupt or prevent therapy except in one case.
It should be appreciated that the treatments reported herein
occurred before the widespread availability of hemato-
poietic growth factors for supportive care.
Acute gastrointestinal toxicity in the form of diarrhea,
nausea, and vomiting, although common, rarely limited
therapy. It is quite clear that patients with underlying
inflammatory bowel disease such as diverticulitis tolerate
abdominal radiotherapy poorly. Similar gastrointestinal
toxicity has been reported by others such as Schray et al.
[10] and Frank et al. [11]. Two cases of fatal gastrointestinal
hemorrhage may or may not have been directly attributable
to radiotherapy. The chronic serious complication rate in
this study (12/165 or 7.3%) was similar to that observed by
other authors. Dembo [3] reported an overall 2.2%
incidence of surgical or nonsurgical bowel obstruction
among 447 patients treated with moving-strip or open-field
radiotherapy for ovarian cancer. In the treatment of intra-
peritoneally-disseminated ovarian or endometrial cancer,
liver shielding produces a safe haven under the right
hemidiaphragm. Omitting liver shielding clearly increases
the risk of hepatic injury; in this study, four patients (2.2%)
developed radiation hepatitis and one died. Fatal radiation
hepatitis is rare; Ingold [12] defined radiation hepatitis as
significant alteration of liver enzymes, hepatomegaly,
biopsy-proven histologic changes, or ascites. He determined
a safe dose to be between 3000 and 3500 cGy. Wharton et
al. [13] and Schacter et al. [14] reported a total of three cases
of fatal radiation hepatitis in patients receiving less than
2920 cGy using the moving-strip technique. Extensive
experience at the Princess Margaret Hospital in Toronto
[3] demonstrated a 0.9% incidence of radiation hepatitis
among 226 patients treated with moving-strip radiotherapy
and no cases of radiation hepatitis among 221 patients
treated with open-field technique without liver shielding.
Survival and patterns of failure
It is quite apparent from this study that patients with
gross residual disease after surgery for stage III or IV
endometrial cancer, whether typical endometrial or papillary
serous/clear cell, fare poorly despite whole abdominal
radiotherapy. Death was a near universal outcome among
24 such patients regardless of histologic subtype and 15 of
them suffered a recurrence within the treatment field.
Radiation therapy alone cannot be advocated as a curative
measure in such patients, although those with gross residual
limited to the pelvis might potentially benefit from chemo-
sensitization plus whole abdomen radiotherapy. This
approach has been piloted in a limited GOG trial [15]. On
the other hand, Corn et al. [16] showed that the presence of
para-aortic metastases in patients with advanced endome-
trioid cancers was associated with a 39% distant relapse
rate, the lungs being the most common site of failure.
Potish et al. [17] employed whole abdominal radio-
therapy in typical endometrioid cancer without gross disease
spread beyond the adnexa, but found that relapse-free
survival was extremely poor in those with gross extra-
pelvic metastases. Other series reported by Martinez et al.
[18] and Gibbons et al. [19] demonstrated that the outcome
after whole abdominal therapy was better in patients with
pathologic stage III endometrial cancer without gross
extrapelvic spread. Among small numbers of patients with
gross disease completely resected, those with clear cell
histology seemed to have the best outcome, 5/9 surviving at
last follow-up compared with 8/31 for papillary serous and
16/39 for typical endometrial adenocarcinomas.
When groups with microscopic extrauterine spread were
considered, 11/39 of patients with papillary serous, 2/6 with
clear cell, and 4/25 of those with typical endometrial
histologies survived. No particular advantage was observed
in any subgroup except patients with typical endometrial
histology and isolated adnexal metastases, where survival
was 3/7.
Several authors have evaluated the use of whole abdo-
minal radiotherapy in patients with papillary serous cancers
of the endometrium. Christman et al. [20] reported that three
of six patients with stage I–III tumors survived after
abdominal therapy (but those three were apparently stage
IA). Frank et al. [11] reported a 44% crude survival in their
patients, 56% of whom had abdominal or pelvic failures.
Employing whole abdominal radiotherapy, Grice et al. [21]
successfully treated four of six patients with stage IIIc
disease, but failed in eight of nine with stage IV disease.
Smith et al. [22] also interpreted their experience with whole
abdominal radiotherapy in high-risk patients as favorable,
but, like other reports, lacked a concurrent control arm.
Martinez et al. [23] treated 132 patients with high-risk
endometrial cancer with whole abdomen and pelvic radio-
therapy with boosts to nodal areas or the vagina over a 20-
year period and reported 5- and 10-year disease-free
survivals of 55% and 45%, respectively, for stage III
disease. First site of failure was abdomen or pelvis in 59%
of relapses and chronic grade 3 or 4 toxicity occurred in
14% of patients. Even in this single-investigator series, there
is clear room for improvement.
Whole abdominal radiation therapy as delivered in this
study appears to offer curative therapy in a minority of
patients with stage III and IV endometrial cancer, regardless
of histologic type. New techniques such as conformal or
intensity-modulated radiotherapy need to be utilized in
future studies in this group of patients. There is also a need

G. Sutton et al. / Gynecologic Oncology 97 (2005) 755–763 763
for other adjuvant therapies in these patients if a better
clinical outcome is to be realized. New treatment regimens
must have the potential to reduce both abdominal and extra-
abdominal failures. Randomized trials involving concom-
itant radiochemotherapy or sequential irradiation and
chemotherapy are clearly needed in this disease.
Acknowledgments
This study was supported by National Cancer Institute
grants of the Gynecologic Oncology Group Administrative
Office (CA 27469) and the Gynecologic Oncology Group
Statistical and Data Center (CA 37517).
The following Gynecologic Oncology Group institutions
participated in this study; University of Alabama at
Birmingham, Oregon Health Sciences University, Duke
University Medical Center, Abington Memorial Hospital,
University of Rochester Medical Center, Walter Reed Army
Medical Center, Wayne State University School of Medi-
cine, University of Southern California Medical Center at
Los Angeles, University of Mississippi Medical Center,
Colorado Foundation for Medical Care, University of
California Medical Center at Los Angeles, University of
Miami School of Medicine, The Milton S. Hershey School
of Medicine of the Pennsylvania State University, George-
town University Hospital, University of Cincinnati College
of Medicine, University of North Carolina School of
Medicine, University of Iowa Hospitals and Clinics,
University of Texas Southwestern Medical Center at Dallas,
Indiana University Medical Center, Wake Forest University
School of Medicine, The Albany Medical College of Union
University, University of California, Irvine Medical Center,
Tufts New England Medical Center, Rush-Presbyterian-St.
Lukes Medical Center, Stanford University Medical Center,
State University of New York Downstate Medical Center,
Eastern Virginia Medical School, Cleveland Clinic Founda-
tion, The Johns Hopkins Oncology Center, State University
of New York at Stony Brook, Pennsylvania Hospital,
Washington University School of Medicine, Memorial
Sloan-Kettering Cancer Center, Cooper Hospital University
Medical Center, Columbus Cancer Council, University of
Massachusetts Medical Center, Women’s Cancer Center,
and University of Oklahoma Health Sciences Center.
References
[1] Jemal A, Murray T, Ward E, Samuels A, Tivari RC, Ghafoor A,
Feuer EF, Thun MJ. Cancer statistics, 2005. CA Cancer J Clin
2005;55:10.
[2] Greer BE, Hamburger AD. Treatment of intraperitoneal metastatic
adenocarcinoma of the endometrium by whole-abdominal moving
strip technique and pelvic boost irradiation. Gynecol Oncol 1983;16:
365–73.
[3] Dembo AJ. Abdominal radiotherapy in ovarian cancer. Cancer 1985;
55:2285–90.
[4] Hendrickson M, Ross J, Eifel P, Kempson R, Martinez A. Uterine
papillary serous carcinoma. Am J Surg Pathol 1982;6:93–108.
[5] Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc 1958;3:457–81.
[6] Mantel N. Evaluation of survival data and two new rank order
statistics arising in its consideration. Cancer Chemother Rep 1966;50:
163–70.
[7] Snedcor GW, Cockran WG. Statistical methods. 6th ed. Ames, Iowa’
The Iowa State University Press; 1967.
[8] Hollander M, Wolf DA. Nonparametric statistical methods. New York,
NY’ John Wiley & Sons; 1999.
[9] Plaxe SC, Saltzstein SL. Impact of ethnicity on the incidence of high-
risk endometrial carcinoma. Gynecol Oncol 1997;65:8–12.
[10] Schray MF, Martinez A, Howes AE. Toxicity of open field whole
abdominal irradiation as primary postoperative treatment in
gynecologic malignancy. Int J Radiat Oncol, Biol, Phys 1989;16:
397–403.
[11] Frank AH, Tseng PC, Haffty BG, Papadopoulos DP, Kacinski BM,
Danling SW, et al. Adjuvant whole abdominal radiation therapy in
uterine papillary serous carcinoma. Cancer 1991;68:1516–9.
[12] Ingold JA, Reed GB, Kaplan HS, Bagshaw MA. Radiation hepatitis.
Am J Roentgenol 1965;93:200–8.
[13] Wharton JT, Delclos L, Gallager S, Smith JP. Radiation hepatitis
induced by abdominal irradiation with cobalt 60 moving strip
technique. Am J Roentgenol 1973;117:73–80.
[14] Schacter L, Crum E, Spitzer T, Maksem J, Diwan V, Kolli S. Fatal
radiation hepatitis: a case report and review of the literature. Gynecol
Oncol 1986;24:373–80.
[15] Reisinger RA. Phase I study of cisplatin and whole abdominal
radiotherapy for the management of stage III and IV endometrial
cancer. Gynecol Oncol 1996;63:299–303.
[16] Corn BW, Lanciano RM, Greven KM, Schultz DK, Reisinger SA,
Stafford PM, et al. Endometrial cancer with para-aortic adenopathy:
patterns of failure and opportunities for cure. Int J Radiat Oncol, Biol,
Phys 1992;24:223–7.
[17] Potish RA, Twiggs LB, Adcock LL, Prem KA. Role of whole
abdominal radiation therapy in the management of endometrial cancer:
prognostic importance of factors indicating peritoneal metastases.
Gynecol Oncol 1985;21:80–6.
[18] Martinez A, Schray M, Podratz K, Stanhope R, Malkasian G.
Postoperative whole abdomino-pelvic irradiation for patients with
high risk endometrial cancer. Int J Radiat Biol Phys 1989;17:371–7.
[19] Gibbons S, Martinez A, Schray M. Adjuvant whole abdominal pelvic
irradiation for high risk endometrial carcinoma. Int J Radiat Oncol,
Biol, Phys 1991;21:1019–25.
[20] Christman JE, Kapp DS, Hendrickson MR, Howes AE, Ballon SC.
Therapeutic approaches to uterine papillary serous carcinoma: a
preliminary report. Gynecol Oncol 1987;26:228–35.
[21] Grice J, Ek M, Greer B, Koh WJ, Muntz JG, Cain J, et al. Uterine
papillary serous carcinoma: evaluation of long-term survival in
surgically-staged patients. Gynecol Oncol 1998;69:69–73.
[22] Smith RS, Kapp DS, Chen Q, Teng NN. Treatment of high-risk
uterine cancer with whole abdominal radiation therapy. Int J Radiat
Oncol, Biol, Phys 2000;48:767–8.
[23] Martinez AA, Weiner S, Podratz K, Armin A-R, Stromberg JS,
Stanhope R, et al. Improved outcome at 10 years for serous-
papillary/clear cell or high-risk endometrial cancer patients treated
with adjuvant high-dose abdomino-pelvic irradiation. Gynecol Oncol
2003;90:537–46.