Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Whole-body MR imaging with the use of parallel imagingfor detection of skeletal metastases in pediatric patientswith small-cell neoplasms: comparison with skeletalscintigraphy and FDG PET/CT
Jyoti Kumar & Ashu Seith & Atin Kumar &
Raju Sharma & Sameer Bakhshi & Rakesh Kumar &
Sandeep Agarwala
Received: 25 January 2008 /Revised: 16 May 2008 /Accepted: 29 May 2008 /Published online: 18 July 2008# Springer-Verlag 2008
AbstractBackground In pediatric patients with small-cell tumors,there is an increasing demand for accurate and early detectionof skeletal, especially bone marrow, metastases as newtreatment protocols are introduced. Whole-body MR imaging(WB-MR) and 18F-fluorodeoxyglucose PET/CT (FDG PET/CT) are new promising imaging methods that can detectmetastases before osteoblastic host response occurs, which isthe basis for detection of metastases by skeletal scintigraphy(SSC).Objective To assess the ability of WB-MR to detect marrowmetastases in children with small-cell neoplasms and compareits performance with that of FDG PET/CT and SSC.
Materials and methods During a 16-month period, 26children and adolescents with histopathologically provensmall-cell neoplasms underwent WB-MR, FDG PET/CT andTc-phosphonate-based SSC in a random order within a 25-dayperiod. Metastases were localized in relation to eight regionsof the body.Results WB-MR revealed metastases in 39 out of a total of208 regions in 26 patients (sensitivity 97.5%, specificity99.4%, positive predictive value 97.5%, negative predictivevalue 99.4%), SSC in 12 regions (sensitivity 30%, specificity99.4%, PPV 92.3%, NPV 85.6%) and FDG PET/CT in 36regions (sensitivity 90.0%, specificity 100%, PPV 100%,NPV 97.7%). Both WB-MR and FDG PET/CT showedexcellent agreement (kappa) with the final diagnosis (96.9%and 93.6% respectively), whereas SSC showed only moderateagreement (39.6%).Conclusion Our results suggest that WB-MR and FDGPET/CT studies are robust imaging modalities for screeningfor skeletal metastases, and are far more accurate than SSC.The lack of radiation is an additional advantage of WB-MR, especially in the pediatric population.
Keywords Whole-bodyMRI . FDG PET/CT.
Small-cell neoplasm .Metastases . Children
Introduction
Neuroblastoma, primitive neuroectodermal tumor (PNET),rhabdomyosarcoma and Ewing sarcoma are the mostcommon small-round-cell malignancies that occur in thepediatric population. In these patients, there is an increasingdemand for accurate and early detection of skeletal,
Pediatr Radiol (2008) 38:953–962DOI 10.1007/s00247-008-0921-y
J. Kumar (*)Department of Radiology, Maulana Azad Medical College,New Delhi, Indiae-mail: [email protected]
A. Seith :A. Kumar : R. SharmaDepartment of Radiology, All India Institute of Medical Sciences,Ansari Nagar,New Delhi, India 110029
S. BakhshiDepartment of Medical Oncology,All India Institute of Medical Sciences,New Delhi, India
R. KumarDepartment of Nuclear Medicine,All India Institute of Medical Sciences,New Delhi, India
S. AgarwalaDepartment of Pediatric Surgery,All India Institute of Medical Sciences,New Delhi, India

especially bone marrow, metastases as new therapy proto-cols are introduced. A reliable tumor staging with a highdiagnostic accuracy is essential not only for therapy butalso for prognosis. Currently, skeletal scintigraphy (SSC)based on Tc-99m methylene diphosphonate (Tc-99mMDP), unilateral or bilateral iliac crest biopsy and CT ofthe chest and abdomen are the standard methods for theinitial staging of these tumors. MR imaging is commonlyused in the evaluation of the local extent of small-celltumors, but it has not been widely used in distant staging.Although Tc-99m MDP scintigraphy is recognized as asensitive technique for skeletal metastases. It depicts bonemetastases at a relatively advanced stage when there is anosteoblastic response. However, it has limited spatialresolution and specificity, and further imaging is sometimesrequired to characterize the regions of documented abnor-mality [1]. MIBG scintigraphy is a more specific examina-tion to detect and stage neural crest tumors and plays animportant role in the evaluation of neuroblastoma. Howev-er, it is not as sensitive as Tc-99m MDP scintigraphy. Iliaccrest biopsy is another routinely used technique. Besidesbeing invasive, it carries the disadvantage that the verysmall area sampled may not include metastases, eventhough they may be present [2]. It has been reported tohave a sensitivity comparable to that of Tc-99m MDPscintigraphy [3].
New imaging techniques such as whole-body MR imag-ing (WB-MR) and positron emission tomography (PET)can identify bone metastases at an earlier stage of growth,before the host osteoblastic reactions occur. WB-MR, withits excellent soft-tissue contrast, lack of radiation and highspatial resolution, is a promising method that allows imag-ing of the entire body in a reasonable time. The use of MRfor whole-body imaging has been limited by cost and acqui-sition time. Longer imaging time is particularly problematicin younger children because they often require sedation.Also, it has been difficult to integrate the different anatomicregions into a single comprehensive scan.
Recent developments in MR imaging, such as thedevelopment of fast turbo sequences, matched by advancesin software technology have led to renewed interest in MRimaging as a potential whole-body screening tool. Anotherimportant development has been the introduction of parallelimaging (parallel acquisition technique, PAT). PAT involvesthe acquisition of a reduced dataset in the phase encodingdirection(s) of k-space to shorten acquisition time. With thistechnique, image data are acquired simultaneously by twoor more receiver coils with different spatial sensitivities andreconstructed to form the image. During the image recon-struction, the missing data are generated with the spatialinformation for the different coil sensitivity profiles, thusavoiding aliasing artifacts. The images are reconstructedusing two different algorithms: either by calculation of the
missing k-space lines before Fourier transformation (GRAPPA)or by later fusion of the generated incomplete images(SENSE). The former was applied for the examinations inour study. The resulting improvements in imaging speed canbe used in various ways, including shortening long exami-nations, improving spatial resolution and/or anatomic cov-erage, improving temporal resolution, enhancing imagequality, overcoming physiological constraints and detectingand correcting for physiological motion [4]. The lack ofradiation exposure is an additional advantage over scintig-raphy and CT, especially in children.
WB-MR has been described in adults for evaluatingskeletal metastases, detecting an unknown primary, andstaging malignancy in pregnant patients [5]. It has also beenused in assessment of multifocal disease such as poly-myositis, Langerhans cell histiocytosis, multifocal osteo-myelitis, child abuse, extensive vascular malformations andfor the staging of small round-cell tumors in the pediatricpopulation [6]. There have been very few studies to assessthe ability of fast MR sequences to reveal metastatic diseasein children [1, 7].
The dual modality PET/CT scan has emerged as anotherpotential whole-body screening tool and combines theadvantages of both modalities—functional informationfrom PET along with anatomic information from CT scan.This fusion improves lesion localization and diagnosticaccuracy [4].
In this study, we assessed the ability of WB-MR todetect bone marrow metastases in children with small-cellneoplasms and compared its performance with that of 18F-fluorodeoxyglucose (FDG) PET/CT and SSC.
Materials and methods
Patients
During a 16-month period, 28 children and adolescentswith histopathologically proven small-cell neoplasms werereferred to us for metastatic work-up. These patientsunderwent WB-MR, SSC and FDG PET/CT in a randomorder. Two of these patients who could not undergo all ofthese investigations were excluded from the study. Theremaining 26 patients who formed the study group werealso subjected to iliac crest biopsy. The interval for com-pletion of all the imaging modalities and iliac crest biopsywas 25 days or less. Also, these were completed before orduring the first 10 days of chemotherapy. Informed consentwas obtained from the parents for each of these procedures.Institutional review board approval was not obtained as itwas not a mandatory prerequisite in our institution. Contra-indications to sedation and the presence of a cardiacpacemaker or intracranial vascular clips were criteria for
954 Pediatr Radiol (2008) 38:953–962

exclusion from the study. However, none of our patientshad any of these exclusion criteria.
The patient population included 20 males and 6 femaleswho ranged in age from 7 months to 16 years. Primarytumors comprised Ewing sarcoma/PNET (11 patients),rhabdomyosarcoma (5 patients), ganglioneuroblastoma (1patient), neuroblastoma (8 patients) and granulocytic sarco-ma (1 patient).
Whole-body MR imaging
For each patient, MR imaging was performed on a 1.5-Twhole-body MR scanner (Magnetom Avanto; Siemens,Erlangen, Germany). The patients were imaged in thesupine position with arms placed next to the thorax andabdomen, using the total imaging matrix (TIM) coil systemfor older children. The smallest possible coils were used forvery young patients. Patients under 6 years of age weresedated by an anesthesiologist. Oxygen saturation, heartrate, respiratory rate and blood pressure were monitoredcontinuously during the MR examination.
After obtaining localizing sequences, the entire bodywas covered from vertex to heels by coronal turbo STIRsequences acquired at two to six overlapping stations usingPAT. The general advantages of PAT are increased spatialand temporal resolution for a given scan time and a de-crease in scan time at a fixed resolution. The section thicknesswas chosen so that complete anterior to posterior coveragewas possible within 15–30 sections per station. The typicaltechnical parameters used for the fast SE STIR sequence wereTR 5,100 ms, TE 87 ms and TI 130 ms. The coronal STIRimages of these overlapping stations were then composedusing built-in software. The TIM coil system enables parallelimaging with whole-body coverage. A T1-weighted (T1-W)sagittal sequence of the spine was also acquired in one to threeoverlapping stations (TR 400 ms, TE 15 ms). No intravenouscontrast agent was administered. By imaging in the coronalplane while performingWB-MR, we achieved complete bodycoverage from head to toe in multiple overlapping stationsduring a period of 40–60 min (average 50 min) in all patients,including patient positioning and sedation.
PET/CT
FDG PET/CT was performed on a Biograph 2 PET/CTscanner (Siemens, Erlanger, Germany). Patients fasted forat least 4 h and blood glucose levels <200 mg/dl wereensured. Immediately prior to the PET/CT scan, patientswere asked to empty their bladder. Younger patients weresedated prior to the examination. Scanning was initiated45 min after intravenous administration of 0.142 mCi/kg ofFDG. Low-dose CT scan was done following PETacquisition. Iodine contrast agent was not administered.
CT transmission data were used to correct for attenuationdifferences and the PET and CT data were fused. The studywas completed in an average of 50 min.
Tc-99m MDP bone scintigraphy
Conventional whole-body bone scintigraphy was performed2–4 h after injection of Tc-99m MDP using a large field ofview camera with parallel-hole high-resolution collimators.Multiple overlapping spot images were obtained over theentire body, including the head, trunk and extremities in anaverage time of approximately 10min. The dose of radiotracerwas adjusted according to the body weight of the patient.
Image interpretation
Each WB-MR study was reviewed independently by twoexperienced radiologists and discrepancies were resolvedby consensus. Metastatic lesions at each site were consid-ered present or absent, rather than numerically quantified.SSC and FDG PET/CT images were also analyzedindependently by two experienced nuclear medicine physi-cians in a random order. Reviewers were unaware of theresults of other imaging modalities. Clinical data includingthe primary tumor, and age and sex of the patient wereavailable to all reviewers.
For each patient, metastases were recorded according tobody region. The body was divided into the following eightregions for the purpose of localization of metastases: skulland head and neck region, rib cage (including sternum andshoulder girdle), cervical spine, dorsal spine, lumbar spine,pelvis, upper extremity, and lower extremity. The presenceof either single or multiple lesions in each region weresimply recorded as involvement in that region. Althoughlimited, this method overcomes the difficulty of countinglesions in diffuse bone marrow metastases. A total of 208regions were evaluated in 26 patients on each of theimaging modalities.
The histology was proven only for the primary lesion.Patients with incongruence in findings between the imagingmodalities were further evaluated by clinical outcome(minimum follow-up of 11 months), dedicated MR imag-ing, imaging follow-up as well as iliac crest biopsy, and thegold standard for each patient was established. Using theestablished gold standard, sensitivity, specificity and posi-tive predictive values were calculated for each technique.The following equations were used in these calculations:sensitivity (%) = [true positives/(true positives + falsenegatives)] × 100; specificity (%) = [true negatives/(truenegatives + false positives)] × 100; positive predictive value(%) = [true positives/(true positives + false positives)] × 100;negative predictive value (%) = [true negatives/(true nega-tives + false negatives] × 100. The statistical significance of
Pediatr Radiol (2008) 38:953–962 955

agreement/differences between data from the three imagingmodalities was tested using kappa analysis.
On turbo STIR images, skeletal metastases were definedas: focal or diffuse hyperintensity of marrow, greater thanor equal to the signal intensity of CSF; focal or heteroge-neous marrow signal variations; or destruction of corticalbone. On T1-W images, marrow metastases were defined asareas of hypointensity, less than or equal to the signalintensity of skeletal muscle or as heterogeneous marrowsignal variations. With SSC or FDG PET, metastatic diseasewas defined as an area of focal increased radionuclideuptake relative to adjacent and/or contralateral normaltissue not located in a region of physiologically increaseduptake.
Results
WB-MR revealed metastases in 39 of 208 regions in 26patients (sensitivity 97.5%, specificity 99.4%, positivepredictive value 97.5%, negative predictive value 99.4%),SSC in 12 regions (sensitivity 30%, specificity 99.4%,positive predictive value 92.3%, negative predictive value85.6%) and FDG PET/CT in 36 regions (sensitivity 90.0%,specificity 100%, positive predictive value 100%, negativepredictive value 97.7%; Table 1). There were 40 true-positive bone marrow lesions according to the established“gold standard.” The agreement (kappa) between the WB-MR and final diagnosis was 96.9% (P<0.001), betweenPET/CT and final diagnosis was 93.6% (P<0.001) andbetween SSC and final diagnosis was 39.6% (P<0.001).
WB-MR detected more lesions than SSC in all regions.WB-MR and PET/CT identified concordant lesions in most
regions except in the region of the spine where WB-MRdetected more lesions than PET/CT (Table 2). Iliac crestbiopsy was attempted in all patients included in the study. Itwas false-negative in three patients: two patients had dis-seminated metastatic lesions on WB-MR, FDG PET/CTand SSC, and in the third patient with Ewing sarcoma, fewmetastatic lesions were detected by WB-MR and FDGPET/CT. There were no false-positive iliac crest biopsies.Since not all skeletal lesions were biopsied, histologicalconfirmation was not possible for most of the marrowmetastases.
In a 4-year–old boy with biopsy-proven PNET of the leftfemur, WB-MR and FDG PET/CT showed multiplemetastases involving the lumbar vertebrae, the upper andlower extremity and the pelvic bones (Fig. 1) while SSCdid not reveal any marrow metastases (Fig. 1). Iliac crestbiopsy confirmed marrow metastases.
In a 10-year-old boy with biopsy-proven Ewing sarco-ma, WB-MR detected metastatic disease in the pelvis anddorsal spine (Fig. 2). FDG PET/CT only detected the pelviclesion and failed to identify the spinal metastases (Fig. 2).On a retrospective analysis, it was felt that the markedactivity due to paraspinal brown fat in this patient obscuredthe small lesion that was present in the dorsal vertebralbody. SSC did not reveal any metastatic lesions (Fig. 2).Iliac crest biopsy did not reveal marrow metastases.
In an 8-year-old boy with biopsy-proven neuroblastoma,while disseminated metastases were identified on WB-MRin the skull, dorsal and lumbar vertebrae, extremities, tho-racic cage and pelvis (Fig. 3), PET/CT detected additionalFDG-avid lesions in the cervical spine (Fig. 3). SSC alsodetected multiple sites of metastases, but was negative forthe cervical spine and upper extremity metastases (Fig. 3).Iliac crest biopsy failed to detect any marrow metastases.
A 4-year-old girl with biopsy-proven neuroblastoma hadtwo bone marrow biopsies for metastases, but both werenegative. However, as the WB-MR (Fig. 4), FDG PET/CT(Fig. 4) and SSC (Fig. 4) images showed diffuse marrow
Table 1 Sensitivities, specificities, positive predictive values andnegative predictive values along with 95% confidence intervals fordetection of bone metastases using WB-MR, Tc-99m MDP SSC andFDG PET/CT.
Category WB-MR(n=208)
SSC(n=208)
PET/CT(n=208)
True positive 39 12 36True negative 167 167 168False positive 1 1 0False negative 1 28 4Sensitivity (%) 97.5 30 90Confidence interval 85.3–99.9 17.1–46.7 75.4–96.7Specificity (%) 99.4 99.4 100Confidence interval 96.2–100 96.2–100 97.2–100Positive predictive value (%) 97.5 92.3 100Confidence interval 85.3–99.9 62.1–99.6 88–100Negative predictive value (%) 99.4 85.6 97.7Confidence interval 96.2–100 79.7–90.1 93.8–99.3
Table 2 Distribution of true bone marrow metastases detected byWB-MR, Tc-99m MDP SSC and FDG PET/CT.
Region WB-MR SSC PET/CT
Skull, head & neck 5 3 5Thoracic cage 2 1 2Pelvis 8 2 8Cervical spine 1 0 1Thoracic spine 7 2 5Lumbar spine 5 2 4Upper extremity 4 1 4Lower extremity 7 1 7Total 39 12 36
956 Pediatr Radiol (2008) 38:953–962

Fig. 1 Biopsy-proven PNET ofthe left femur in a 4-year oldboy. a WB-MR coronal STIRimage shows the primary massinvolving the left femur withassociated large soft-tissuecomponent extending into thepelvis. Hyperintense foci repre-senting metastases are seen in-volving the right femoral shaftand L2 vertebra (arrows).b FDG PET/CT MIP coronalimage shows intense uptake inthe primary tumor with multiplemetastases involving the upperand lower extremities and lum-bar vertebrae. c SSC image doesnot reveal any metastases
Pediatr Radiol (2008) 38:953–962 957
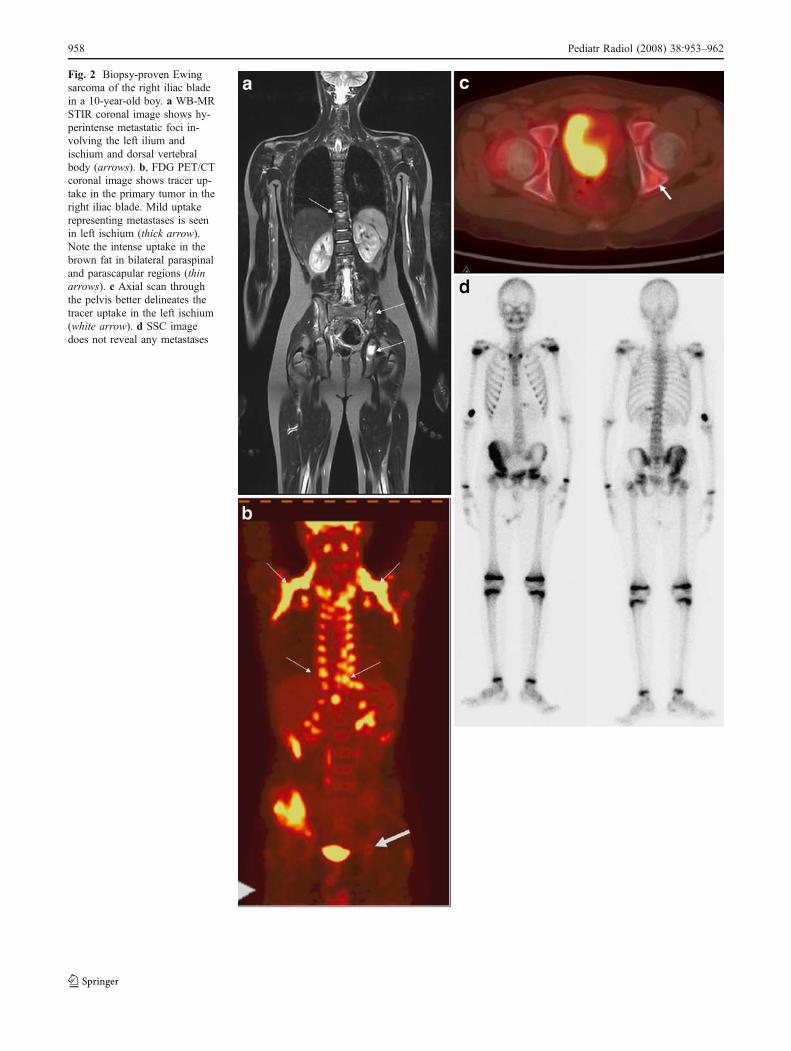
Fig. 2 Biopsy-proven Ewingsarcoma of the right iliac bladein a 10-year-old boy. a WB-MRSTIR coronal image shows hy-perintense metastatic foci in-volving the left ilium andischium and dorsal vertebralbody (arrows). b, FDG PET/CTcoronal image shows tracer up-take in the primary tumor in theright iliac blade. Mild uptakerepresenting metastases is seenin left ischium (thick arrow).Note the intense uptake in thebrown fat in bilateral paraspinaland parascapular regions (thinarrows). c Axial scan throughthe pelvis better delineates thetracer uptake in the left ischium(white arrow). d SSC imagedoes not reveal any metastases
958 Pediatr Radiol (2008) 38:953–962

metastases, the girl was not subjected to this invasive pro-cedure for a third time.
In a 16-year-old boy with biopsy-proven rhabdomyo-sarcoma involving the mandible, WB-MR detected multiplemetastases in the dorsal vertebrae, pelvis and lower
extremity. FDG PET/CT showed the pelvic and lowerextremity lesions but was negative for dorsal vertebralmetastases. SSC did not reveal any marrow metastases.Iliac crest biopsy confirmed the presence of marrowmetastases.
Fig. 3 Biopsy-proven neuroblastoma of the left adrenal in an 8-year-old boy. a WB-MR STIR coronal image shows disseminatedmetastases involving the right parietal bone with a large accompa-nying extra-axial soft-tissue mass (small arrows), multiple dorsolum-bar vertebrae, the pelvis and bilateral upper and lower extremities withminimal sparing of normal marrow (white arrows). Also note thepartially calcified left adrenal mass (black arrow). b STIR coronalimage of the head and neck region shows the normal marrow signalintensity of cervical vertebrae. Note the abnormal hyperintense
marrow involvement in bilateral proximal humeral epiphysis. c, dFDG PET/CT coronal (c) and sagittal (d) images show disseminatedlesions corresponding to the WB-MR image. The cervical vertebraealso show FDG uptake depicting metastases (arrows) that were notdetected on MR. Also note that the right parietal bone lesion showsless uptake than the adjacent intense uptake in the physiologicallyactive brain. e SSC image shows multiple metastases involving theskull, dorsal vertebrae and pelvis. Note that there is no lesion in thecervical spine
Pediatr Radiol (2008) 38:953–962 959

A 4-year-old girl with biopsy-proven PNET of the tibiashowed a STIR hyperintense lesion in the right sacral ala onWB-MR images. However, this was not seen on SSC, FDGPET/CT images nor on the iliac crest biopsy and hence was
considered a false-positive lesion on MR. Since it was closeto the iliac crest biopsy site, which was performed a weekprior to the MR examination, it probably represented amisplaced biopsy needle tract during the procedure.
Fig. 4 Biopsy-proven leftadrenal neuroblastoma in a4-year-old girl. a WB-MR STIRcoronal image shows left-sidedneuroblastoma with disseminat-ed hyperintense metastases in-volving multiple vertebrae, thepelvis and bilateral upper andlower extremities (arrows).b FDG PET/CT coronal imageshows uptake in the primarytumor with disseminated metas-tases corresponding to theregions seen on MRI. c SSCimage shows metastases in skullbone and vertebrae. The ex-tremity and pelvic bones do notshow tracer uptake
960 Pediatr Radiol (2008) 38:953–962

In another 3-year-old girl with biopsy-proven neuroblas-toma, WB-MR and FDG PET/CT detected disseminatedmetastases involving the skull, dorsal and lumbar vertebrae,extremities and the pelvis while SSC revealed only thecalvarial and upper extremity metastases and failed to demon-strate the rest. Iliac crest biopsy was positive for marrowmetastases.
Additional visceral metastases were also identified onWB-MR images. These included lung metastases that wereseen in four patients and liver metastases in one patient.Intraspinal extradural soft tissue was also delineated in twopatients on WB-MR images.
Discussion
In this study, WB-MR and FDG PET/CT showed a highersensitivity, specificity and positive predictive value thanstandard SSC for the detection of skeletal metastases inchildren and young adults (Table 1). Both WB-MR andPET/CT showed excellent agreement (kappa) with the finaldiagnosis (96.9% and 93.6%, respectively), whereas SSCshowed only moderate agreement (39.6%).
The pathological basis for early visualization of neo-plasms on WB-MR is that FSE STIR imaging allows directvisualization of tumor deposits and tumor-related edemaprior to visualization of the osteoblastic reaction, which isutilized in SSC [8]. Bone scintigraphy, although easilyperformed and the current method of choice for whole-bodyskeletal evaluation, creates a limited representation of thebody with a resultant poor spatial and contrast resolution.As technetium-based analogues are taken up by chemisorp-tion onto the phosphorus groups of calcium hydroxyapatiteproduced by osteoblasts, the concentration of isotope onscintigraphy is an indirect marker of a tumor, in effectindicating the host osteoblastic response to tumor deposits,which occurs in the advanced stage [5]. FDG PET revealsmalignant bone marrow infiltration early because of itsincreased glucose metabolism. In combination with CT, theproblem of limited spatial resolution is also overcome [7,8]. While the whole-body radiation exposure from SSC isabout 0.07 mSv, effective dose per PET/CT examination isabout 25 mSv [9, 10].
Iliac crest biopsy, which is normally the standard methodof confirming marrow involvement, as well as being aninvasive procedure, may not show metastases even if theyare present because of the small amount of tissue obtained[2]. The high sensitivity of WB-MR in detecting skeletalmetastases has previously been reported by other inves-tigators [11, 12]. A study conducted by Mentzel et al. [8]comparing WB-MR STIR imaging and Tc-99m MDPscintigraphy in the examination of children with suspectedmultifocal skeletal malignant lesions concluded that WB-
MR STIR imaging showed more lesions than conventionalscintigraphy and hence may be used as a screening tool formetastatic lesions in children. Daldrup-Link et al. [1] com-pared the accuracy of WB-MR using a conventional T1-Wspin-echo sequence, SSC, and PET in the detection of bonemetastases in a group of 39 children and young adults.They concluded that WB-MR had a higher sensitivity(82%) than SSC (71%) but a lower sensitivity than PET(90%) in the evaluation of bone marrow metastases.
Other studies in adults have also been conducted withsimilar conclusions. In a recent study by Schmidt et al. [13]comparing the diagnostic accuracy of WB-MR using paral-lel imaging and PET/CT in screening for bone metastases,WB-MR had a sensitivity of 94% and PET/CT had asensitivity of 78%. Specificities were 76% for WB-MR and80% for PET/CT, whereas diagnostic accuracy was 91%and 78%, respectively. Schmidt et al. [13] concluded that areliable MR bone marrow scan should include T1-W andSTIR imaging. We utilized coronal STIR imaging for thewhole body and sagittal T1-W imaging for the spine in ourstudy. Studies have also suggested that STIR WB-MR dueto high tissue contrast allows excellent delineation of focallesions that show no adequate FDG uptake [4]. To the bestof our knowledge, this is the first study comparing thesensitivity and diagnostic accuracy of WB-MR, SSC andFDG PET/CT in evaluating pediatric skeletal metastases.
Although the results of this preliminary study areencouraging, they need to be interpreted with caution asthe study included only a small number of patients. Thehyperintense signal noted is not specific as it may be causedby minor bone bruises that can often be observed in youngchildren. Inflammatory, infectious, traumatic and necroticchanges as well as benign lesions such as cysts and heman-giomas cannot be differentiated from malignant neoplasmby turbo STIR imaging alone [2]. As biopsy of each of themarrow lesions was not ethically justifiable, we believe thatimaging and clinical follow-up, the addition of T1-Wsequence of the spine, and the iliac crest biopsy establishedthe validity of findings in patients whose results wereincongruent between the various imaging modalities.Moreover, none of the patients had a well-documentedhistory of trauma or infection at the suspicious sites. Thespecificity may also be reduced by highly cellular hemato-poietic bone marrow typically found in children. However,hematopoietic marrow can be correctly identified when thehyperintensities are bilaterally symmetrical or diffuse. Aknowledge of the distribution of normal hematopoieticmarrow in children is important for the interpreting radio-logist [14–16]. Also while the hematopoietic marrow showsminimal hyperintensity as compared to skeletal muscle,tumor infiltration produces a marked hyperintense signalchange much greater than muscle [2]. Also, posttherapymarrow signal alterations due to edema, necrosis, fibrosis or
Pediatr Radiol (2008) 38:953–962 961

red marrow hyperplasia are difficult to differentiate fromresidual tumor on follow-up MR examinations.
In some patients PET/CT can be misinterpreted, e.g. inareas of physiologically increased uptake such as the brain.Wrong lesion localization can result from inadequate fusionof the PET and CT data resulting from breathing artifacts,although misregistrations can usually be recognized bychecking the uncorrected and unfused data. A false-negative result may be obtained if lesions are smaller thantwice the size of the spatial resolution of the PET scanner(usually 6 mm) [4]. In our study, we found that in at leasttwo patients FDG PET/CT gave a false-negative result inthe dorsal and lumbar vertebrae due to obscuration byintense uptake in the adjacent paraspinal brown fat in onepatient and hydroureteronephrosis in the other. The sensi-tivity of the technique is impaired after the start of therapybecause of reconverted FDG-avid marrow.
Imaging costs and availability must also be considered inchoosing the optimal modality. At our institution, whilebone scintigraphy is the cheapest, the cost of MR examina-tion is less than half that of FDG PET/CT. In general, WB-MR is currently more widely available than PET/CT, atleast in the present scenario.
Conclusion
Although this study included a small number of patients,our results suggest that WB-MR and FDG PET/CT studiesare robust, and are promising imaging modalities for thesystemic screening for skeletal metastases. PAT allows WB-MR screening at a high spatial resolution and speed, with asensitivity superior to that of skeletal scintigraphy. SinceWB-MR is currently more widely available than PET/CTand does not involve exposure to ionizing radiation, itappears to be a promising screening method in this sub-group of pediatric oncology patients. On the other hand,developments in PET/CT are directed towards the goal ofusing it as a “one-stop shop” for whole-body staging oftumors by delineating the primary tumor as well as lymphnodal, visceral and marrow metastases. Our results alsoindicate that WB-MR or PET/CT should be used for stagingof patients with solid malignancies, especially when iliaccrest biopsies are negative. However, larger prospectivetrials are needed to determine if WB-MR and PET/CT canreplace the routine staging procedures for staging ofpediatric malignancies [17].
References
1. Daldrup-Link HE, Franzius C, Link TM et al (2001) Whole-bodyMR imaging for the detection of bone metastases in children andyoung adults: comparison with skeletal scintigraphy and FDGPET. AJR 177:229–236
2. Mazumdar A, Seigel MJ, Narra V et al (2002) Whole-body fastinversion recovery MR imaging of small cell neoplasms inpediatric patients: a pilot study. AJR 179:1261–1266
3. Mirza I, Cuello B, Ramachandran A et al (2001) Bonemarrow biopsyand bone scan to detect metastases. Clin Nucl Med 26:677–679
4. Schmidt GP, Baur-Melnyk A, Herzog P et al (2005) High-resolution whole-body magnetic resonance image tumor stagingwith the use of parallel imaging versus dual-modality positronemission tomography-computed tomography: experience on a 32-channel system. Invest Radiol 40:743–753
5. Eustace S, Tello R, DeCarvalho V et al (1997) A comparison ofwhole-body turbo STIR MR imaging and planar 99mTc-methylenediphosphonate scintigraphy in the examination of patients withsuspected skeletal metastases. AJR 169:1655–1661
6. Kellenberger CJ, Epelman M, Miller SF et al (2004) Fast STIRwhole-body MR imaging in children. Radiographics 24:1317–1330
7. Kellenberger CJ, Miller SF, Khan M et al (2004) Initial experiencewith FSE STIR whole-body MR imaging for staging lymphoma inchildren. Eur Radiol 14:1829–1841
8. Mentzel HJ, Kentouche K, Sauner D et al (2004) Comparison ofwhole-body STIR-MRI and 99m Tc-methylene diphosphonatescintigraphy in children with suspected multifocal bone lesions.Eur Radiol 14:2297–2302
9. Subramanian G, McAfee JG, Blair RJ et al (1975) Technetium-99m-methylene diphosphonate – a superior agent for skeletalimaging: comparison with other technetium complexes. J NuclMed 16:744–755
10. Brix G, Lechel U, Glatting G et al (2005) Radiation exposure ofpatients undergoing whole-body dual-modality 18F-FDG PET/CTexaminations. J Nucl Med 46:608–613
11. Goo HW, Choi SH, Ghim T et al (2005) Whole-body MRI ofpaediatric malignant tumours: comparison with conventionaloncological imaging methods. Pediatr Radiol 35:766–773
12. Steinborn MM, Heuck AF, Tiling R et al (1999) Whole-body bonemarrow MRI in patients with metastatic disease to the skeletalsystem. J Comput Assist Tomogr 23:123–129
13. Schmidt GP, Schoenberg SO, Schmid R et al (2007) Screening forbone metastases: whole-body MRI using a 32-channel systemversus dual-modality PET-CT. Eur Radiol 17:939–949
14. Ricci C, Cova M, Kang Y et al (1990) Normal age related patternsof cellular and fatty bone marrow distribution in the axialskeleton: MR imaging study. Radiology 177:83–88
15. Kricun M (1985) Red-yellow marrow conversion: its effect on thelocation of some solitary bone lesions. Skeletal Radiol 14:10–19
16. Moore S, Dawson K (1990) Red and yellow marrow in the femur:age related changes in appearance at MRI. Radiology 175:219–223
17. American College of Radiology Imaging Network (2006) Protocol6660. Whole-body MRI in the evaluation of pediatric malignan-cies. Study accrual closed on 29 June 2007. http://www.acrin.org/TabID/184/Default.aspx. Accessed 27 June 2008
962 Pediatr Radiol (2008) 38:953–962









![NUCLEAR MEDICINE AND MOLECULAR IMAGING · Clinical Applications ... 3.1.4 Evaluation of [11 C]rofecoxib in a HSV encephalitis model ... 304011B Skeletal scintigraphy detail (flow](https://img.pdfslide.net/doc/110x75/5f5cf2019feb8d639340bdd0/nuclear-medicine-and-molecular-clinical-applications-314-evaluation-of-11.jpg)