Embed Size (px)
Citation preview
Renal Radionuclide Renal Radionuclide imagingimaging
Dr.Aftab QadirDr.Aftab Qadir
• Renal perfusion and function• Obstruction (Lasix renal scan)• Renovascular HTN (Captopril renal scan)• Infection (renal morphology scan)• Pre-surgical quantitation (nephrectomy) • Renal transplant• Congenital anomalies, masses
(renal morphology scan)
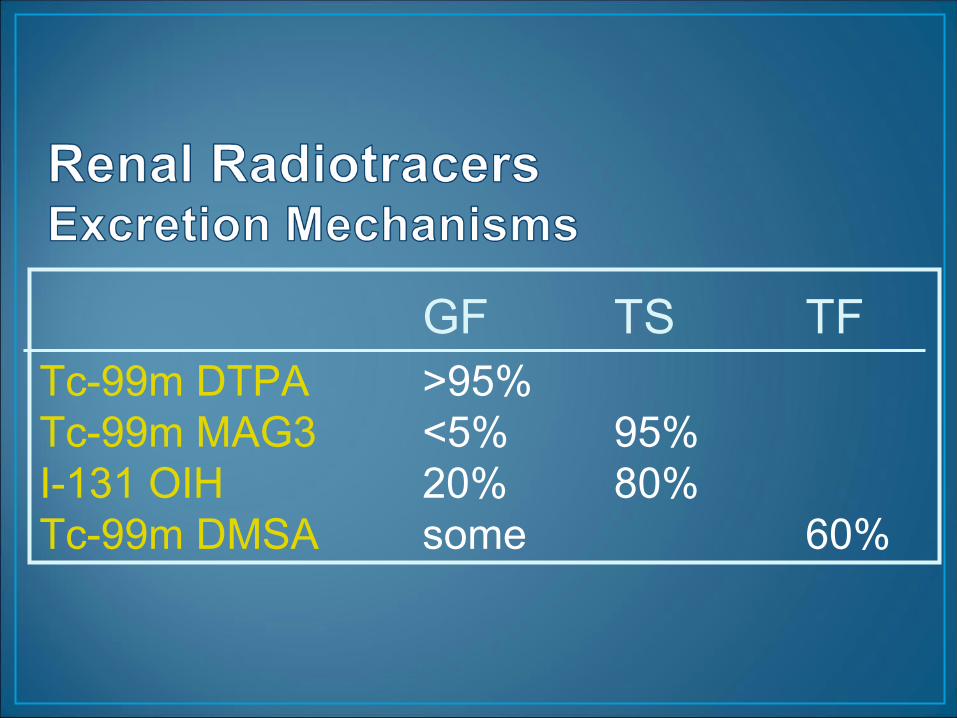
GF TS TFTc-99m DTPA >95%Tc-99m MAG3 <5% 95%I-131 OIH 20% 80%Tc-99m DMSA some 60%
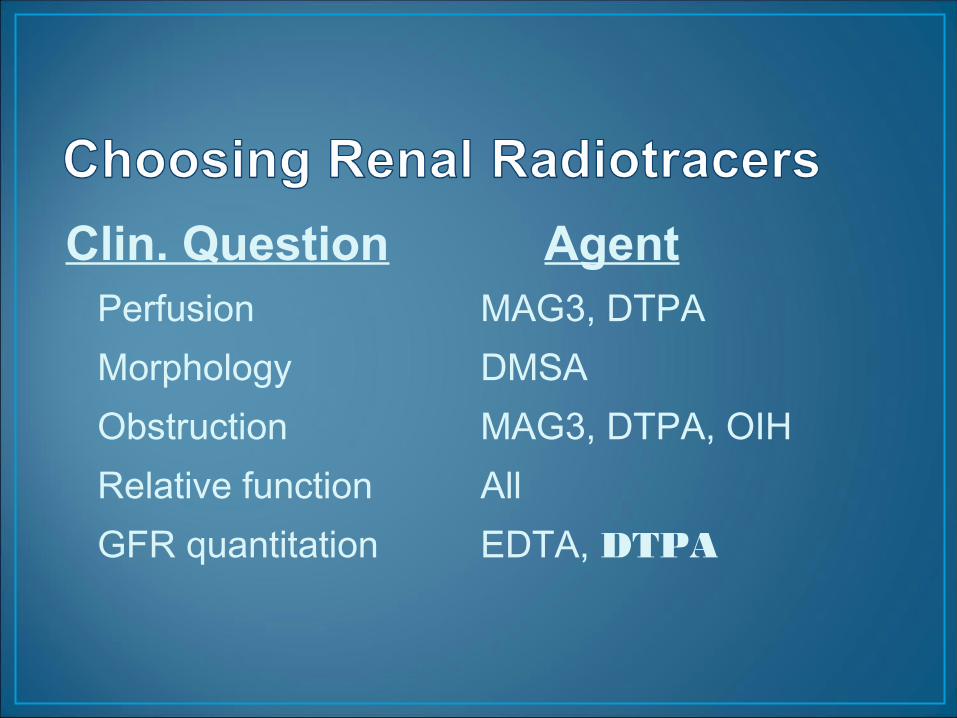
Perfusion MAG3, DTPA Morphology DMSA Obstruction MAG3, DTPA, OIHRelative function AllGFR quantitation EDTA, DTPA
Clin. Question Agent
• Tracers • Tc-99m DMSA
• Acquisition• 2-4 hrs post-injection• pinhole posterior + post. oblique (or SPECT)
1.DMSA scintigraphy1.DMSA scintigraphy
Renal Morphology ScanRenal Morphology Scan
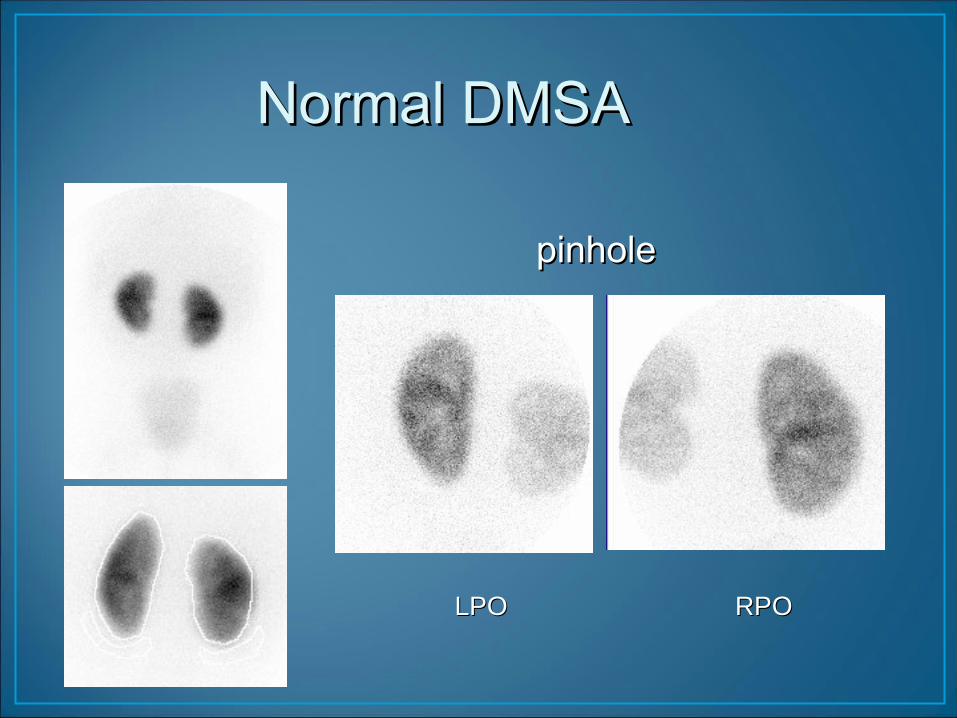
Normal DMSA Normal DMSA
pinholepinhole
LPO RPOLPO RPO
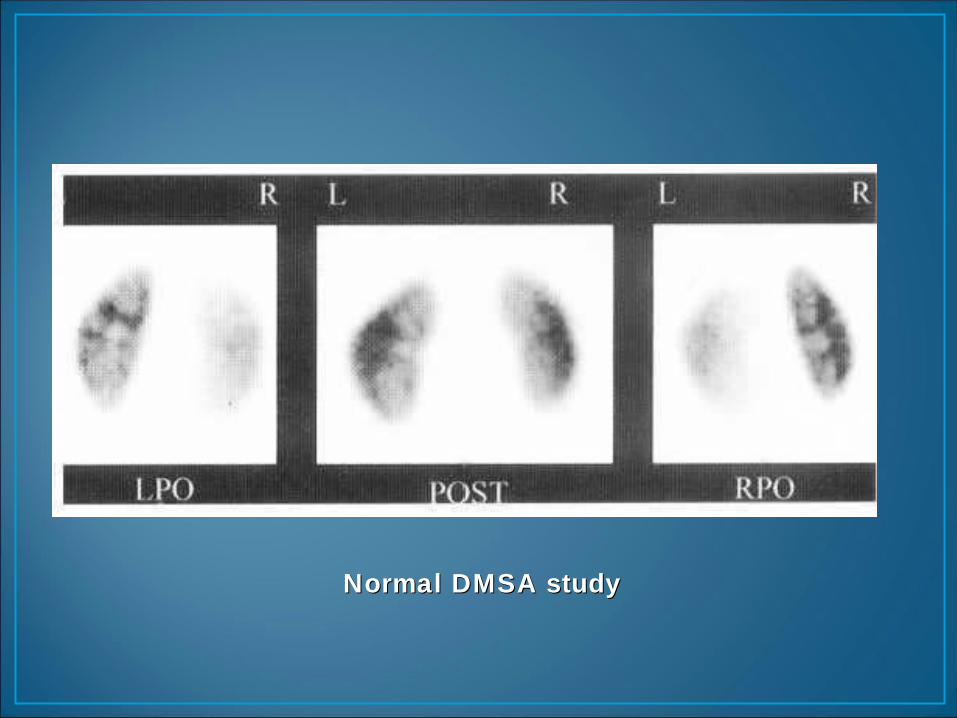
Normal DMSA studyNormal DMSA study
Applications of DMSA Applications of DMSA scintigraphyscintigraphy
1.Renal ectopia and anomalies1.Renal ectopia and anomalies
2.Renal masses and pseudomasses2.Renal masses and pseudomasses
3.Infection and scarring3.Infection and scarring
• Agenesis• Renal ectopia
• Fusion (horseshoe)• Multicystic dysplastic kidney
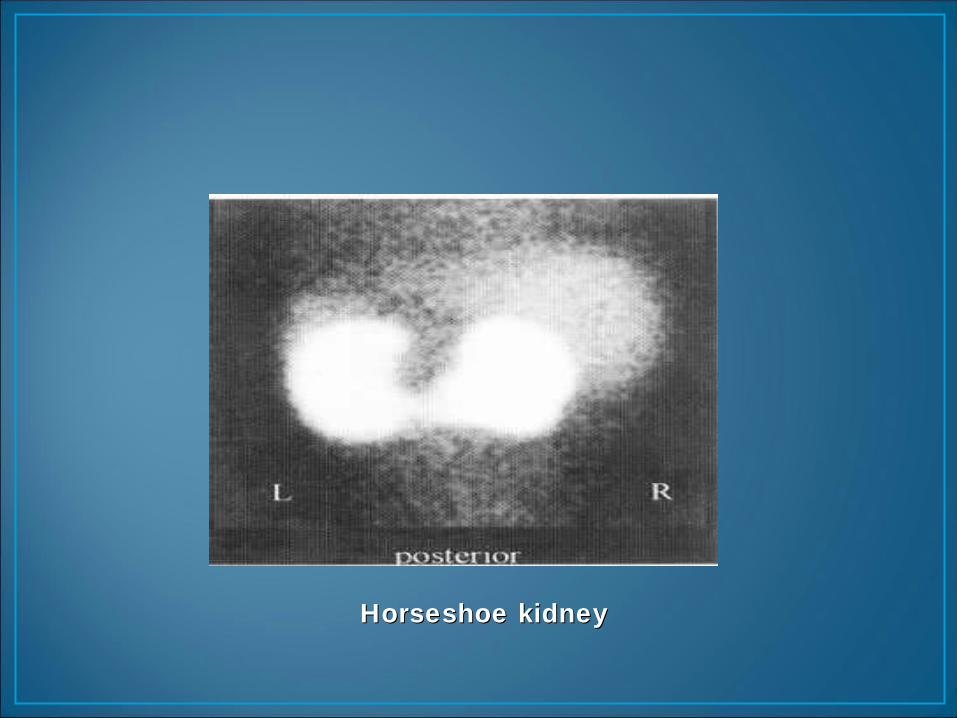
Horseshoe kidneyHorseshoe kidney
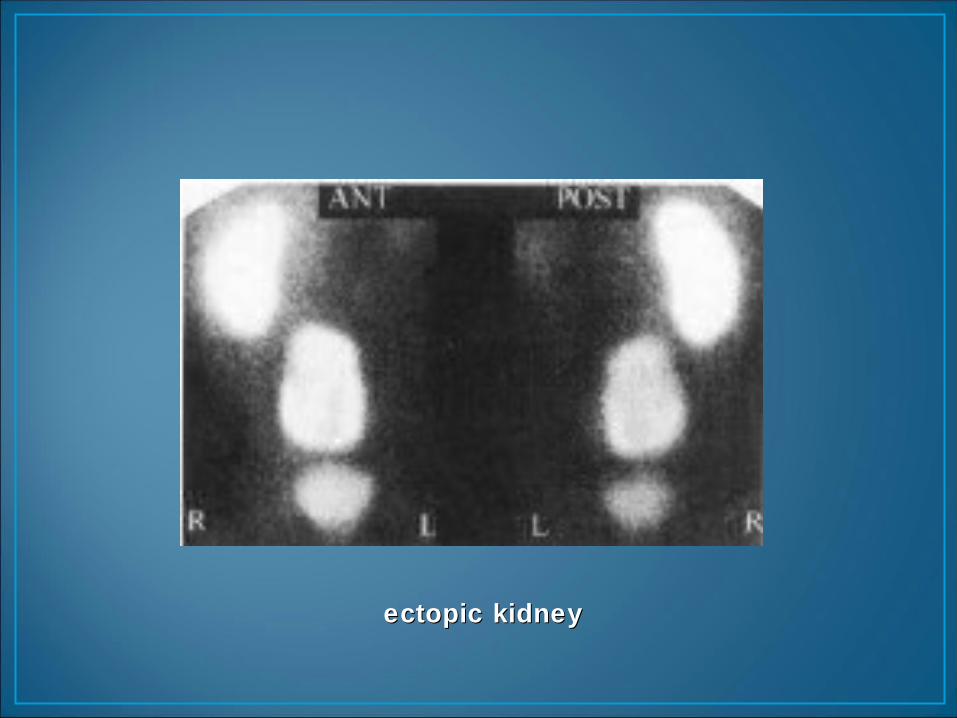
ectopic kidney ectopic kidney
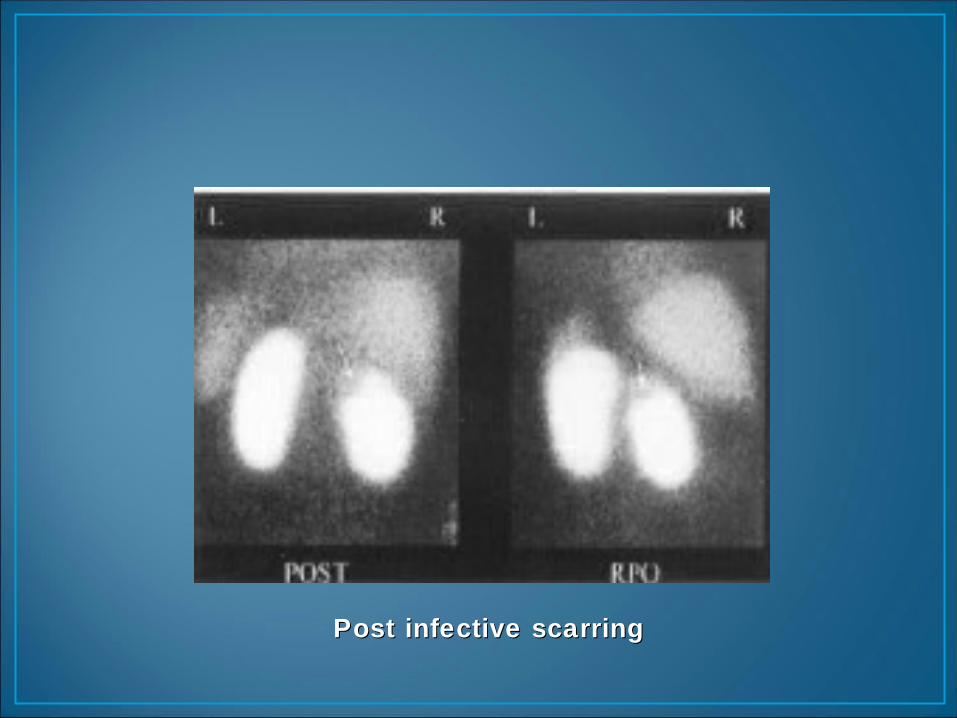
Post infective scarring Post infective scarring
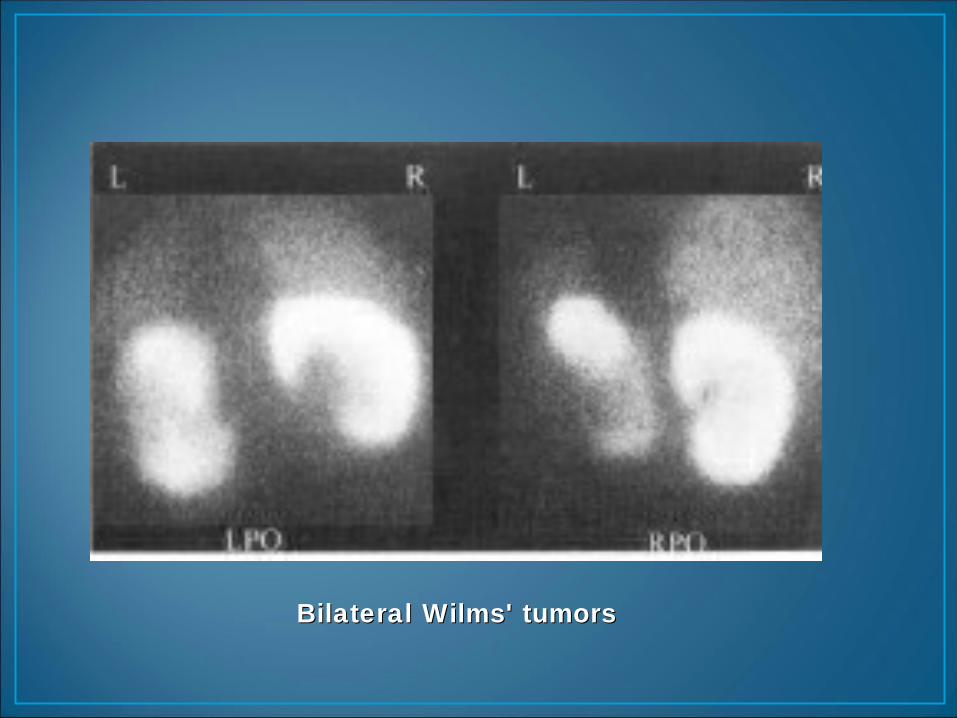
Bilateral Wilms' tumorsBilateral Wilms' tumors
• Acute or chronic pyelonephritis• Hydronephrosis• Cyst• Tumors• Trauma (contusion, laceration, rupture, hematoma)• Infarct• Abscesses
• Acute pyelonephritis• single or multiple “cold” defects• renal contour not distorted• diffuse decreased uptake• diffusely enlarged kidney or focal bulging
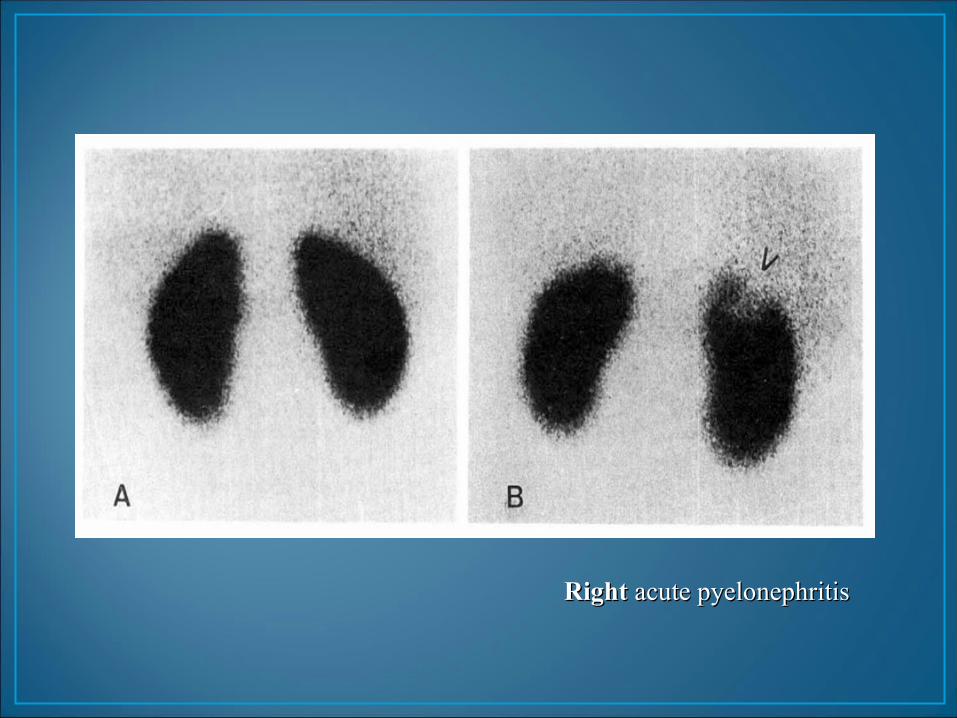
Right Right acute pyelonephritis acute pyelonephritis
• Tracer: MAG3, (DTPA)• Labeling with technetium- 99m gives a lower
radiation dose • better imaging and measurement statistics
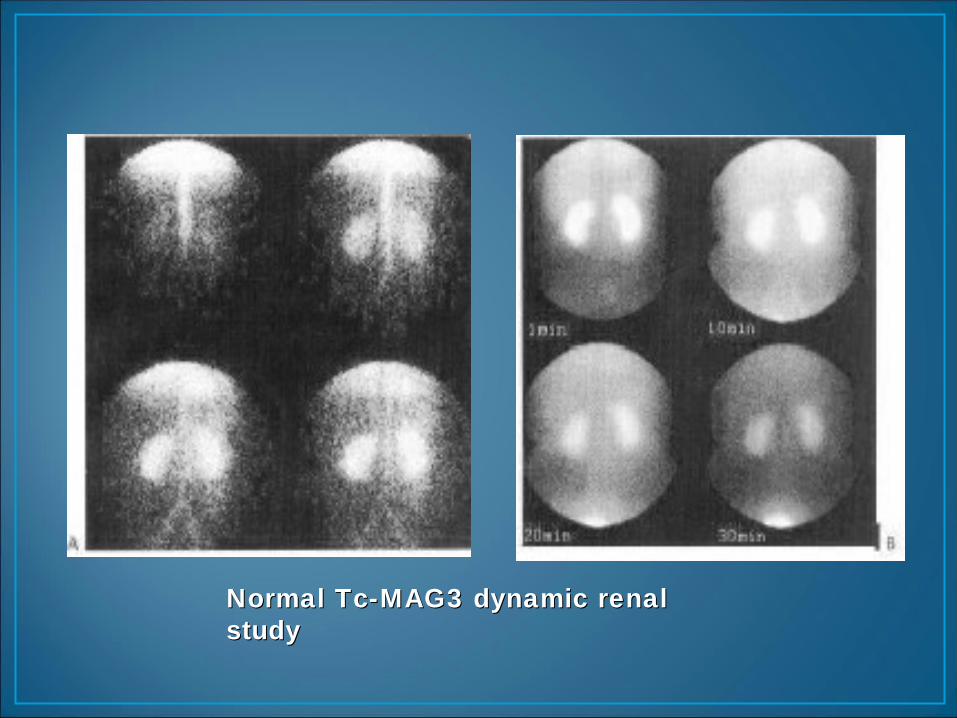
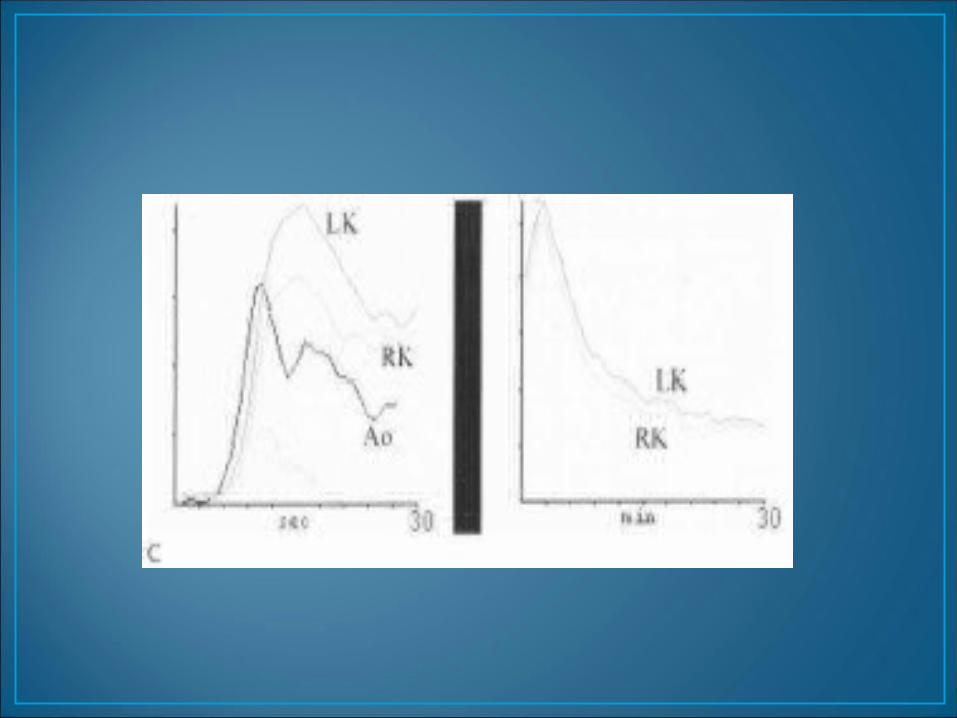
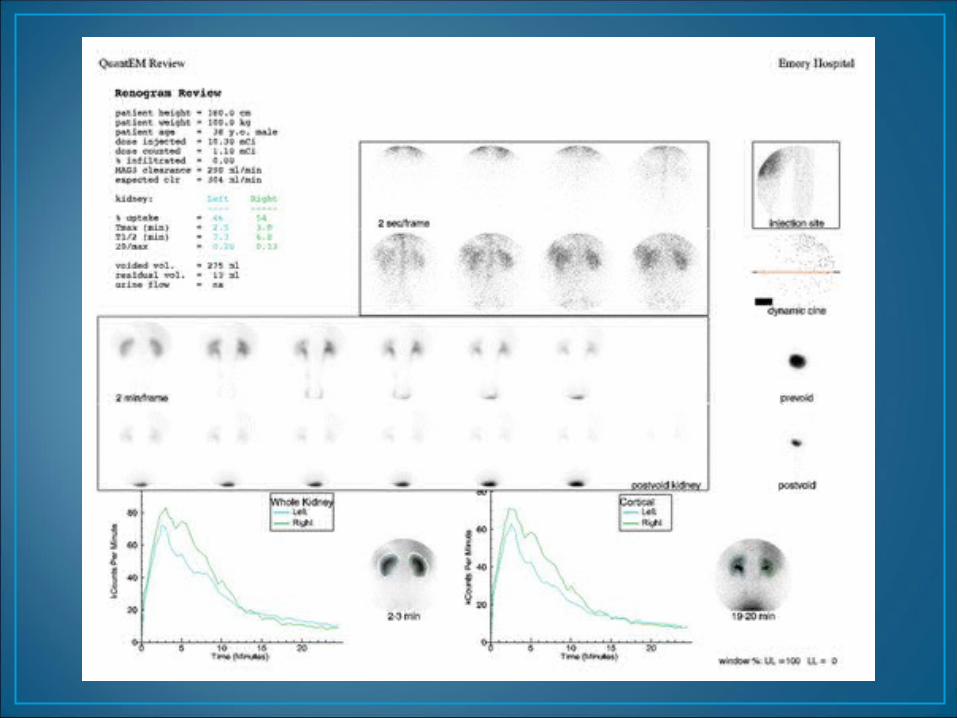
Normal Tc-MAG3 dynamic renal Normal Tc-MAG3 dynamic renal studystudy
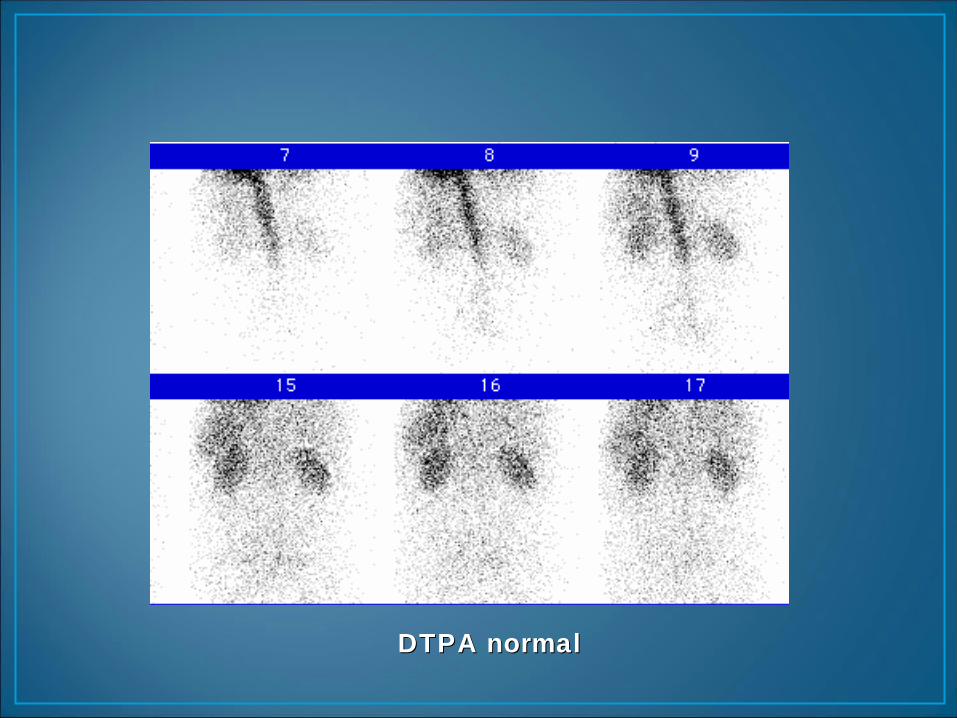
DTPA normalDTPA normal
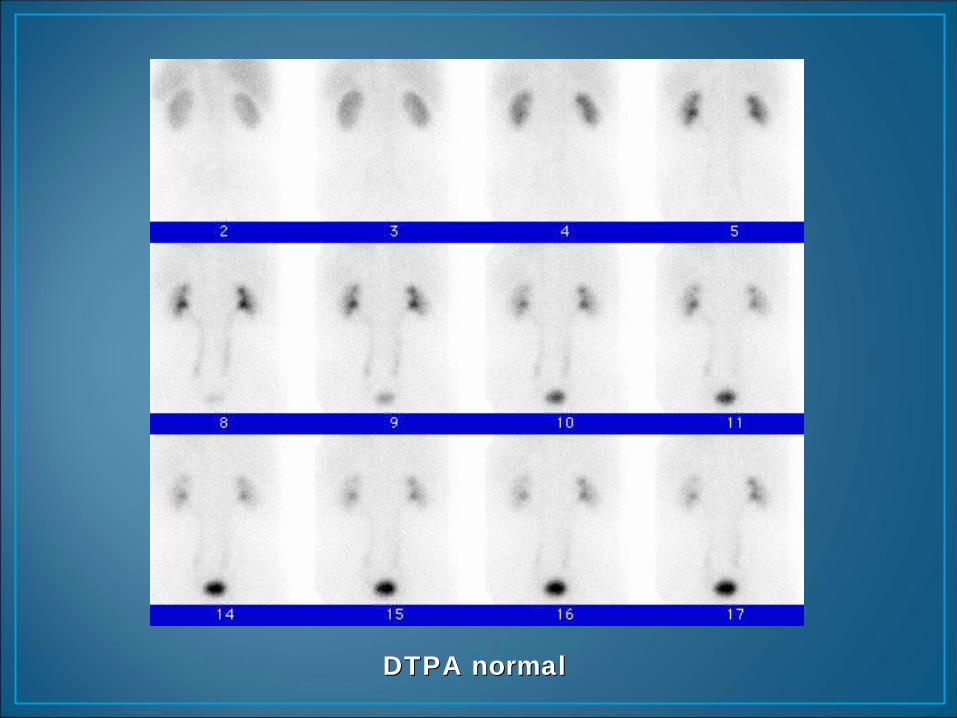
DTPA normalDTPA normal
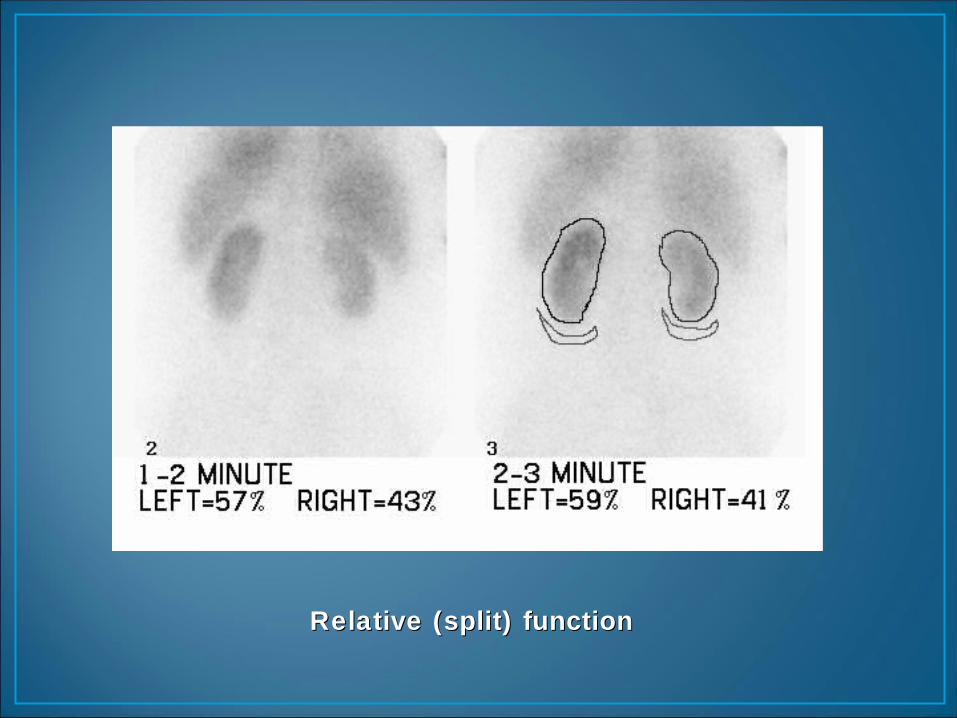
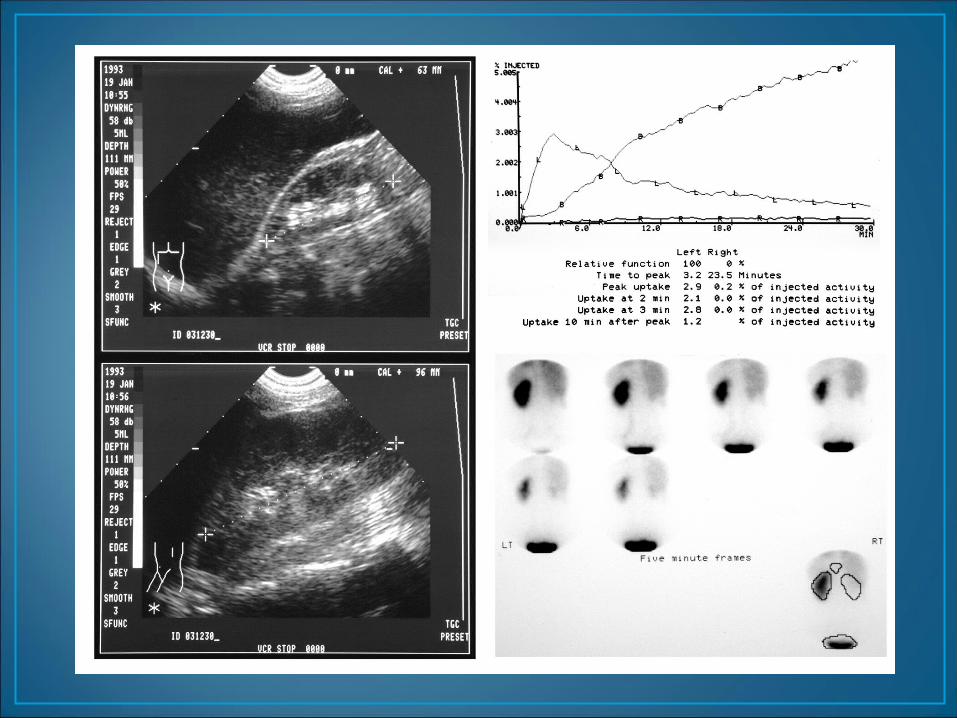
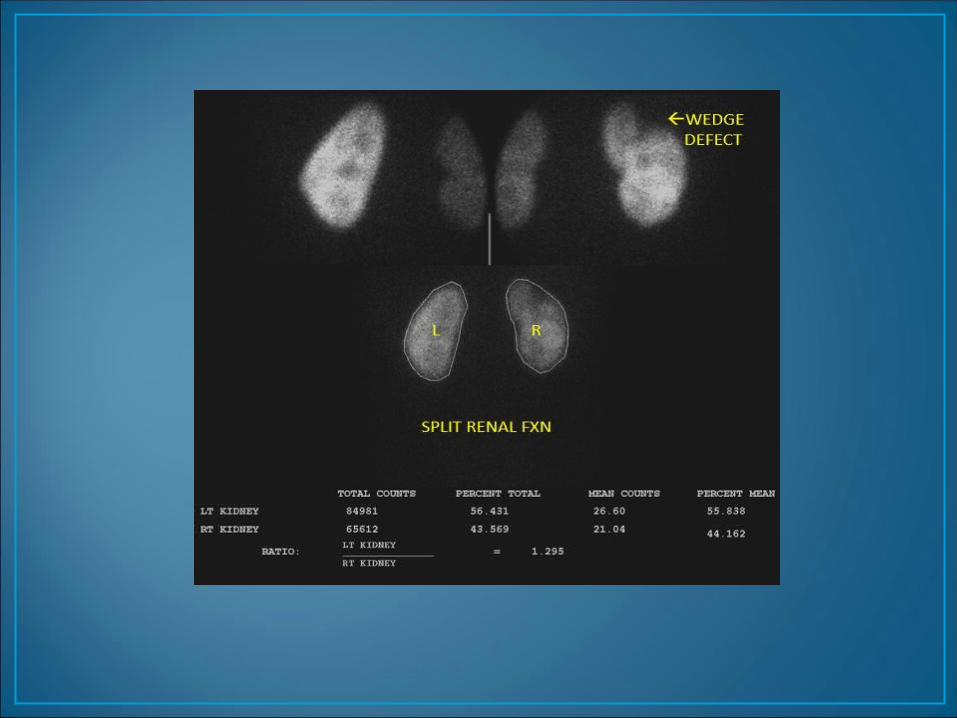
Relative (split) functionRelative (split) function
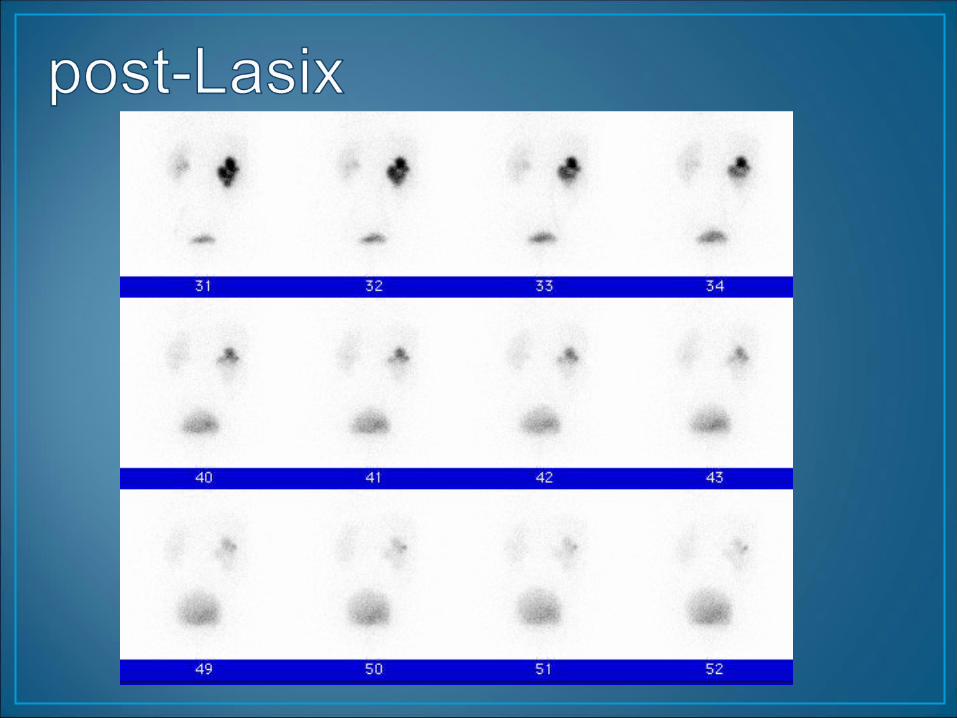
Diuretic (Lasix) Renal Scan
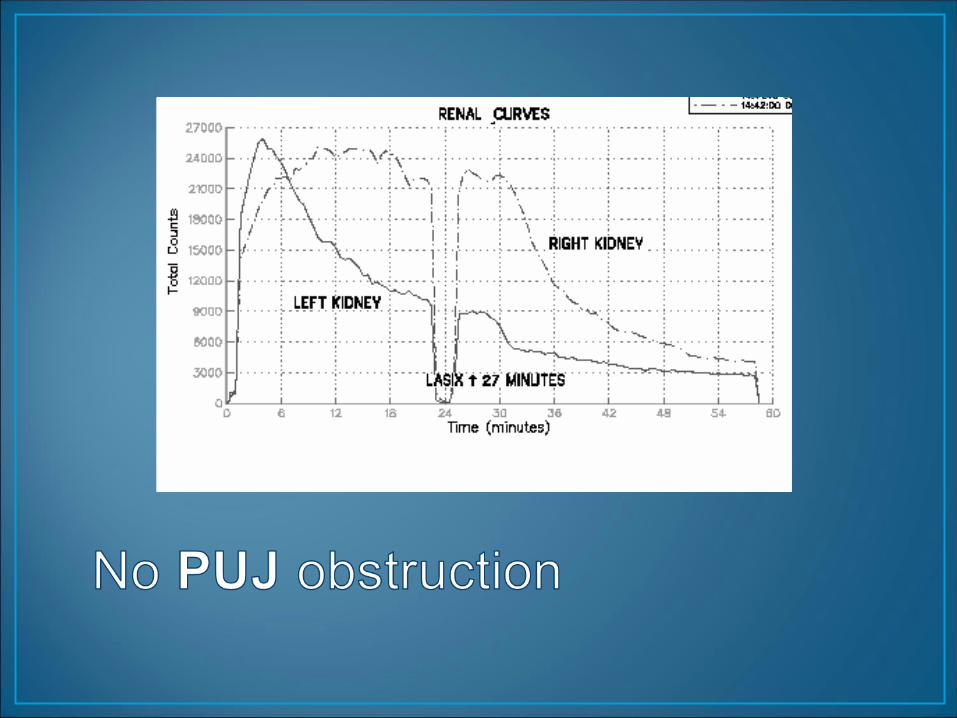
• Hydronephrosis - tracer pooling in dilated renal pelvis• Lasix induces increased urine flow• If obstructed >>> will not wash out
• If dilated, non-obstructed >>> will wash out
• Can quantitate rate of washout (T1/2)
• Tracers: Tc-99m MAG3 5-10 mCi
• Acquisition: supine until pelvis full(can switch to sitting post- Lasix)
• Flow (angiogram) : 2-3 sec / frame x 1 min• Dynamic: 15-30 sec / frame x 20-30 min
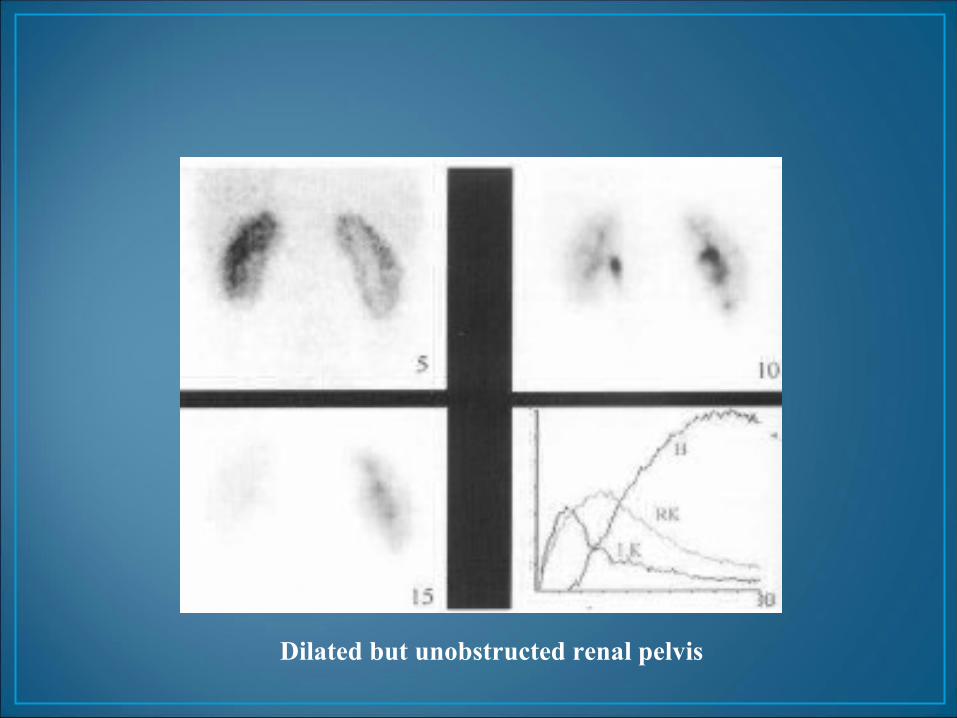
Dilated but unobstructed renal pelvis
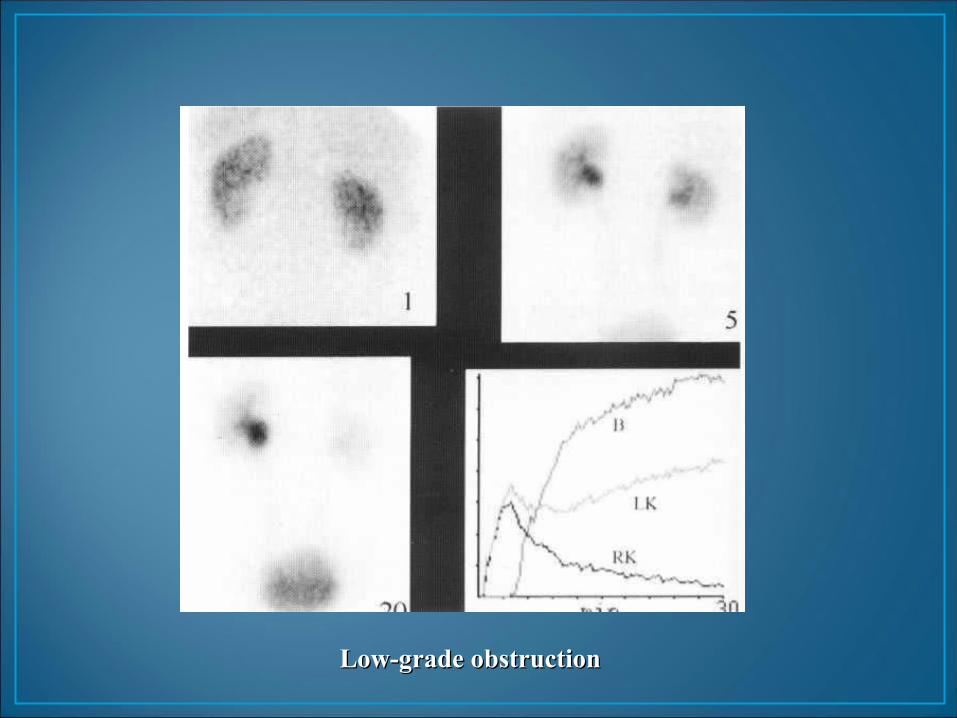
Low-grade obstructionLow-grade obstruction
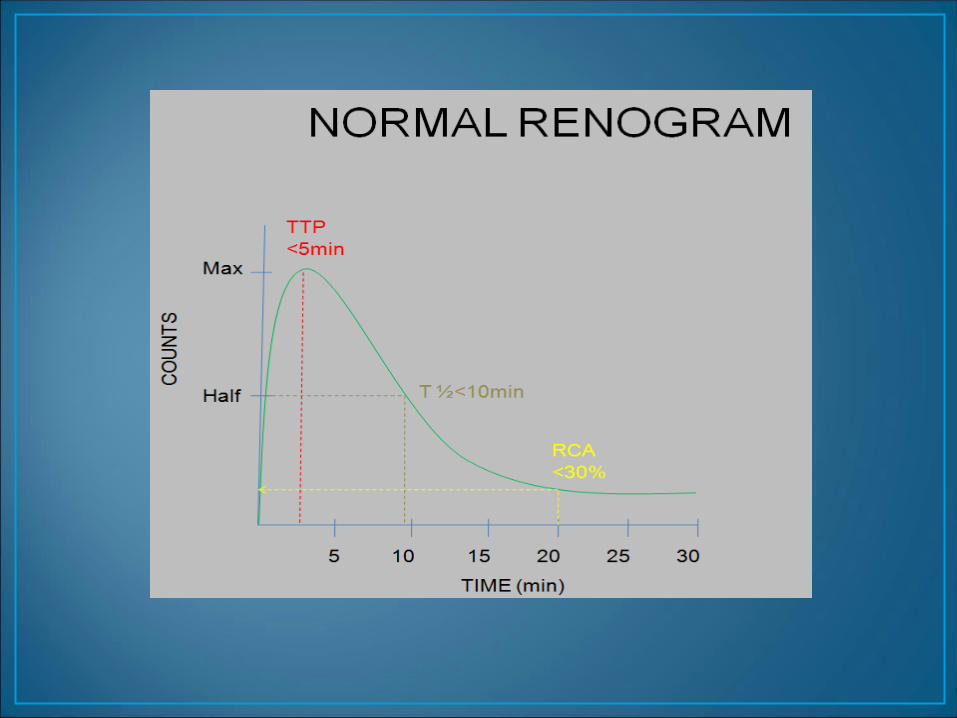
• Normal < 10 min• Obstructed > 20 min• Indeterminate 10 - 20 min
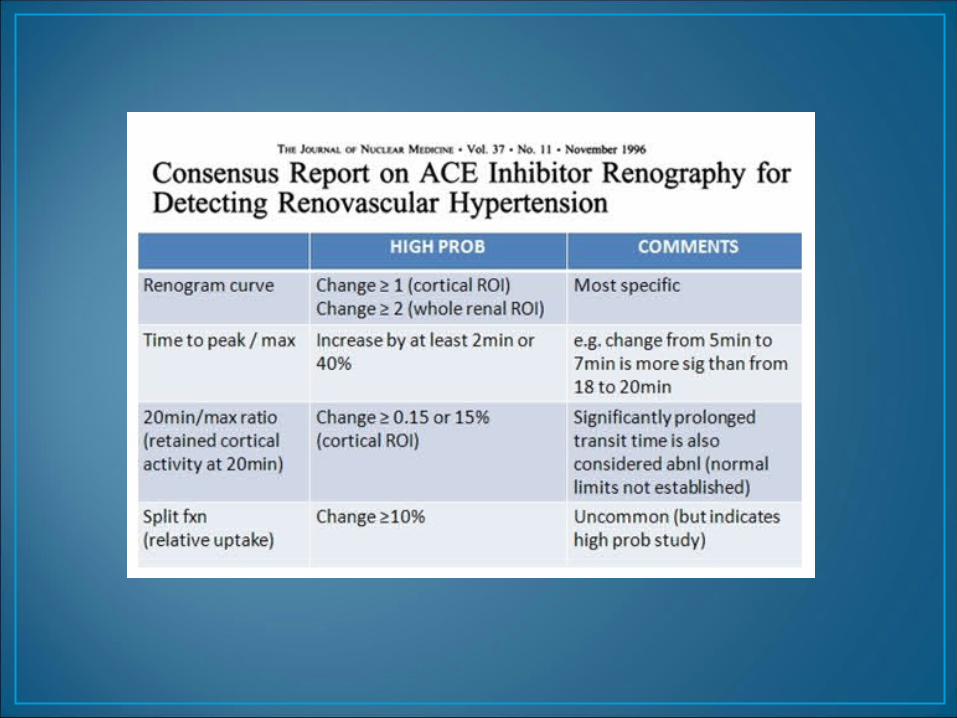
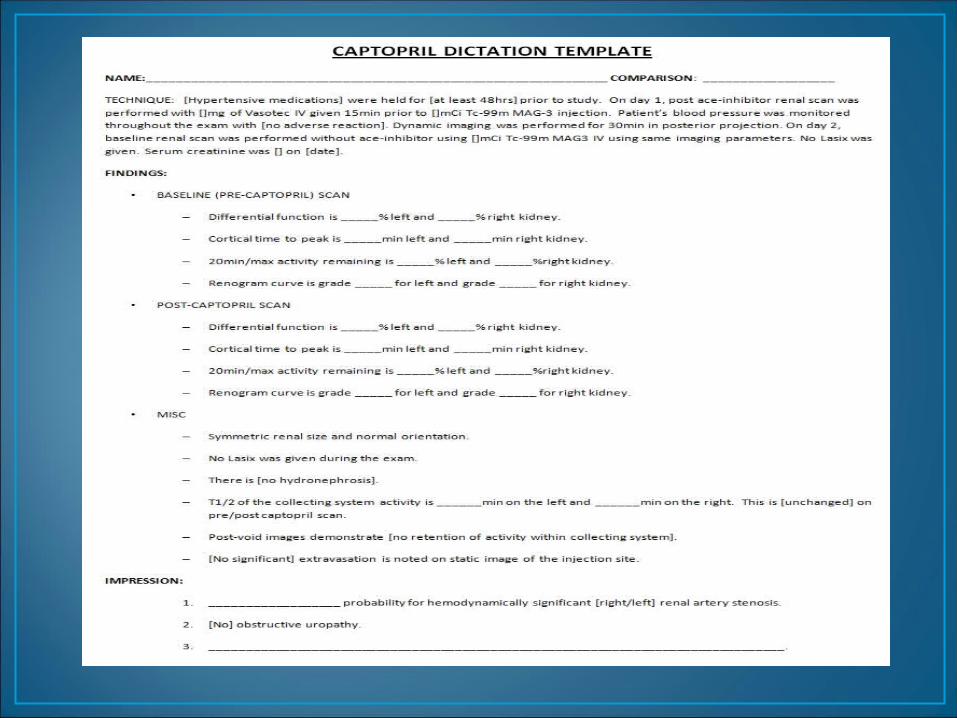
Captopril Renal ScanCaptopril Renal Scan (ACEI Renography) (ACEI Renography)
• Gold standard: angiography• Initial non-invasive tests:
• Duplex sonography• ACEI renography
• Other tests: • MRA
• Off ACEI & ATII receptor blockers x 3-7 days
• Off diuretics x 5-7days
• No solid food x 4 hours
• Patient well hydrated• 10 ml/kg water 30-60 min pre and during test
• ACEI• Captopril 25-50 mg po (crushed), 1 hr pre-scan
Patient PreparationPatient Preparation
• Tracer: Tc-99m MAG3 (or DTPA)
• Protocol: 1 day vs. 2 day test• 1 day test: baseline scan (1-2 mCi) followed by
post-Capto scan (8-10 mCi)
• Acquisition: flow & dynamic x 20-30 min.
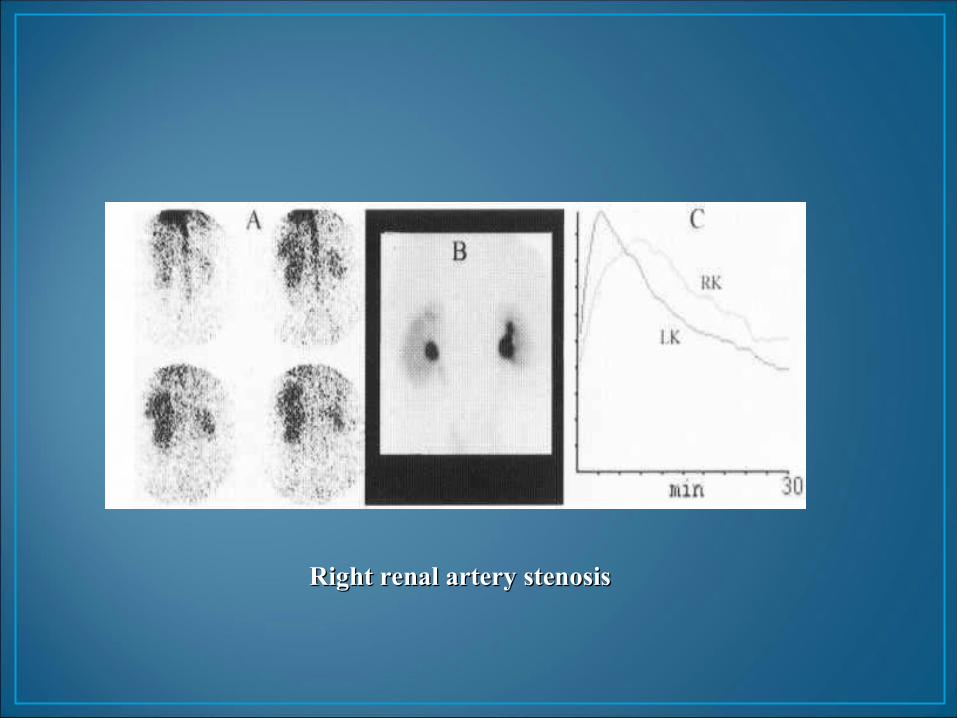
Right renal artery stenosisRight renal artery stenosis
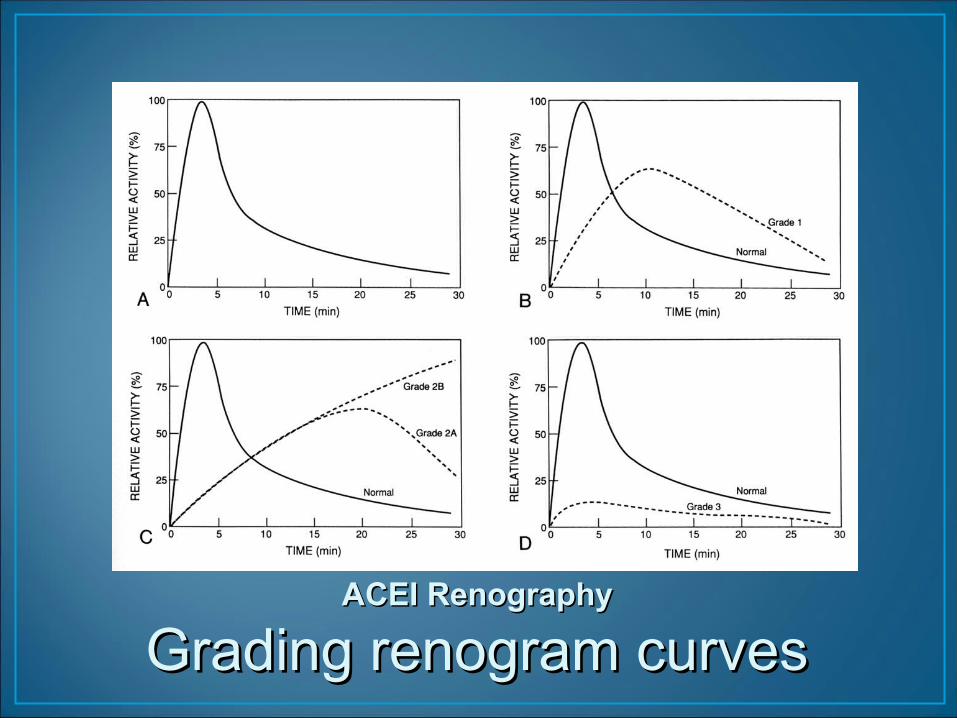
ACEI RenographyACEI Renography
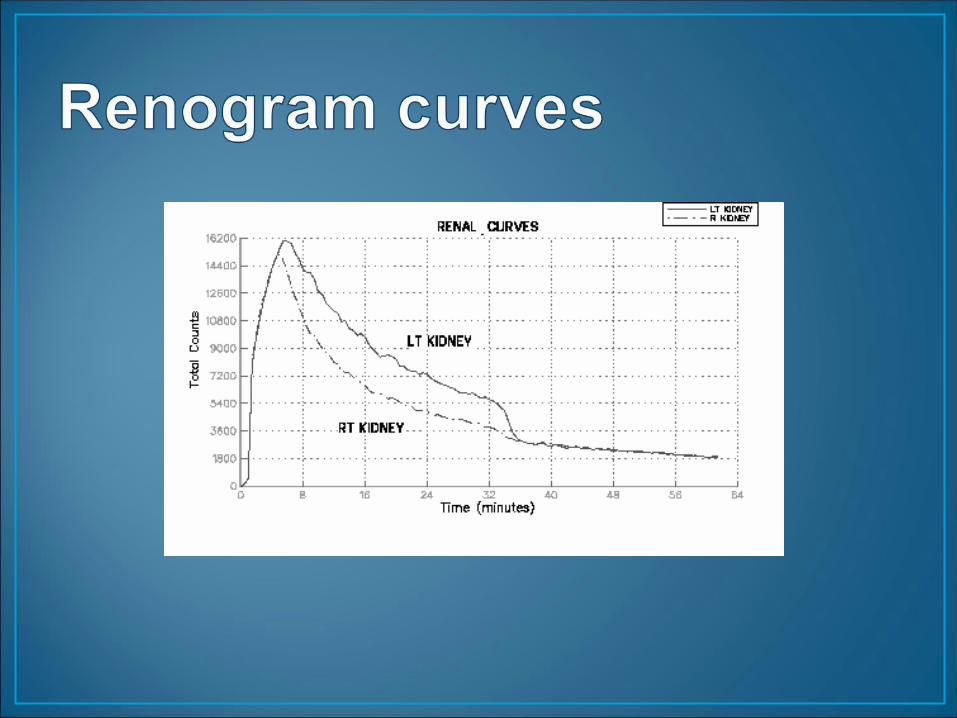
Grading renogram curvesGrading renogram curves
Grade I Mild delay in Tmax (6-11 min using 99m Tc-DTPA) with a falling excretion phase
Grade 2 More prolonged delay in T max (greater than 11 min) but still with an excretion phase
Grade 3 with marked reduction in function of the affected kidney
• Evaluation of children with recurrent UTI• 30-50% have VUR
• Follow up after initial VCUG• Assess effect of therapy / surgery• Screening of siblings of reflux patients.
• Tc-99m
• via Foley
• can do at any age• VUR during filling
• catheterization
• Tc-99m DTPA or Tc-99m MAG3
• i.v.
• no catheter• info on kidneys
• need patient cooperation
• need good renal function
AdvantageAdvantage
Disadv.Disadv.
Direct Indirect
• Lower radiation dose(5 vs 300 mrad to ovary)
• Smaller amount of reflux detectable
• Quantitation of post-void residual volume
• Cannot detect distal ureteral reflux
• No anatomic detail
• Grading difficult
Advantages Disadvantages
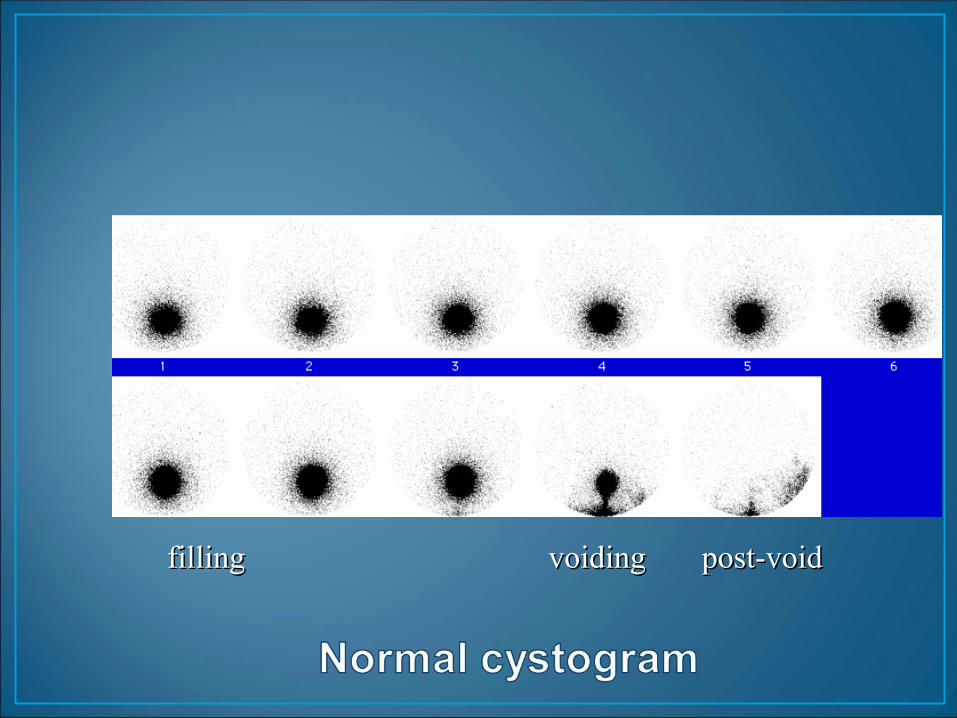
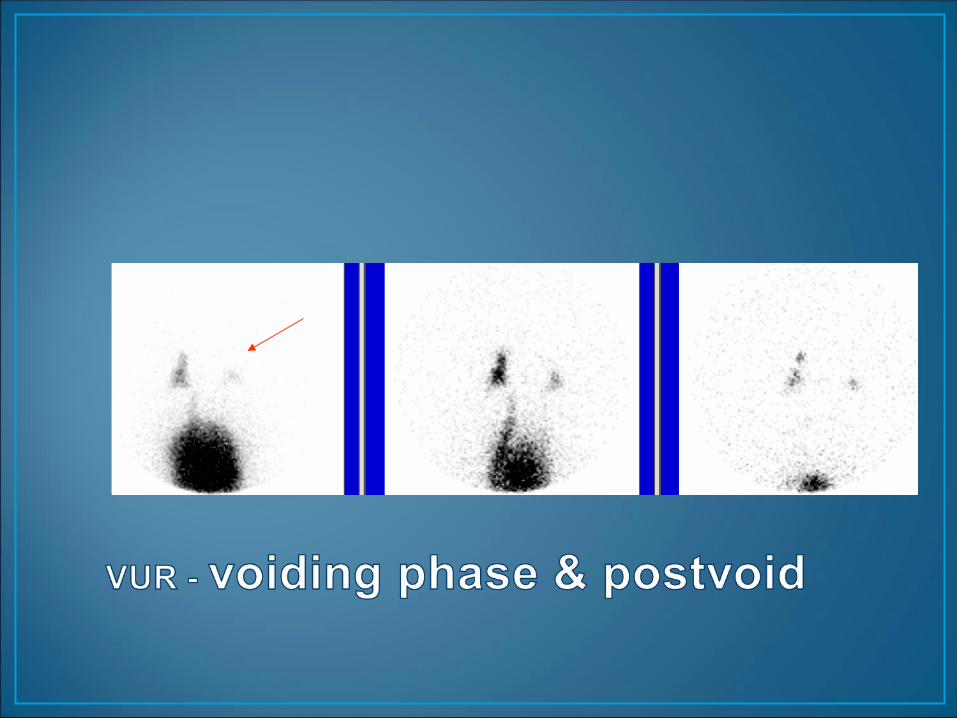
filling voiding post-voidfilling voiding post-void
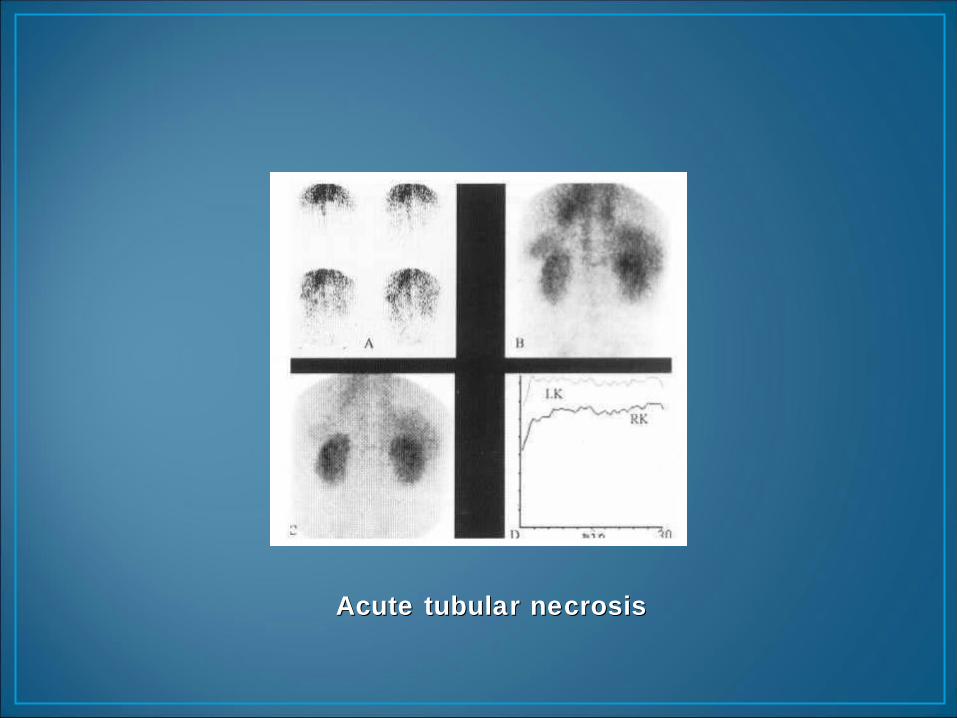
Acute tubular necrosisAcute tubular necrosis
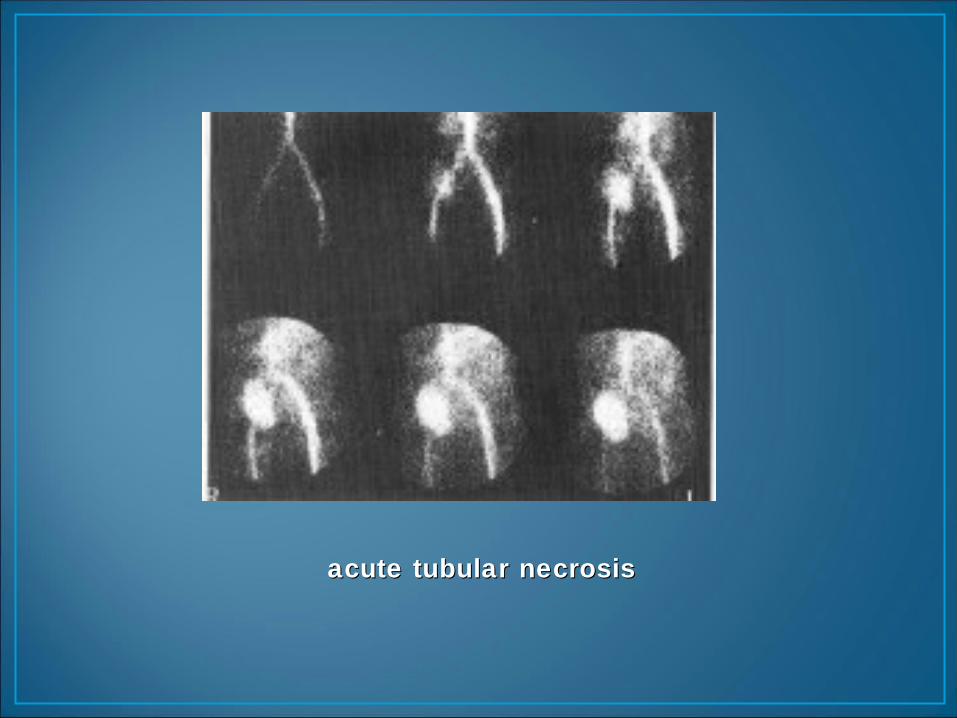
acute tubular necrosisacute tubular necrosis

Few casesFew cases
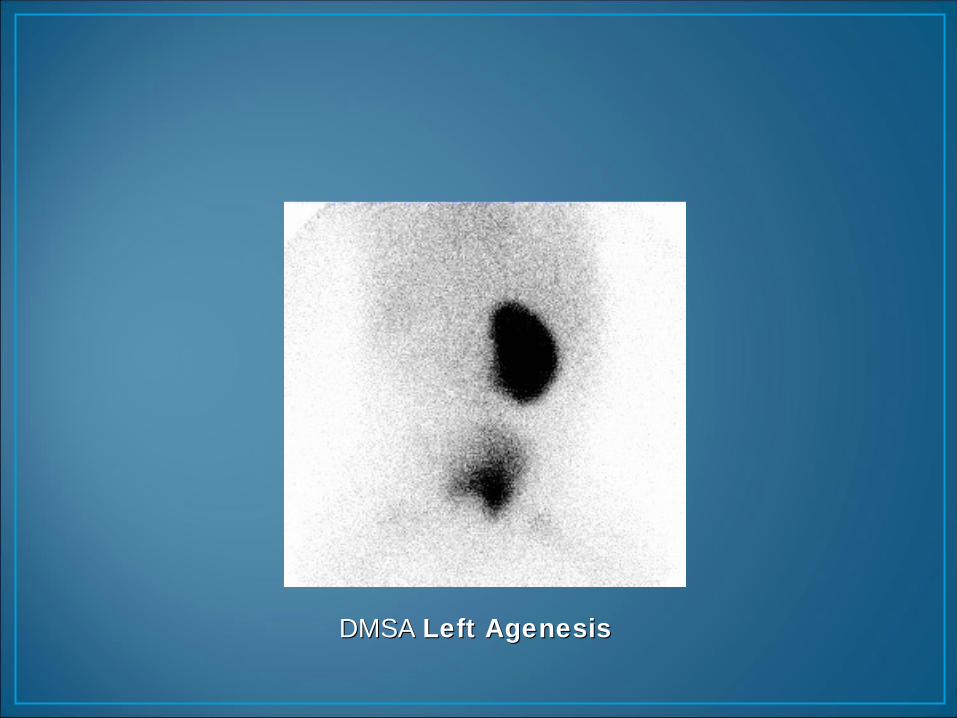
DMSA DMSA Left AgenesisLeft Agenesis
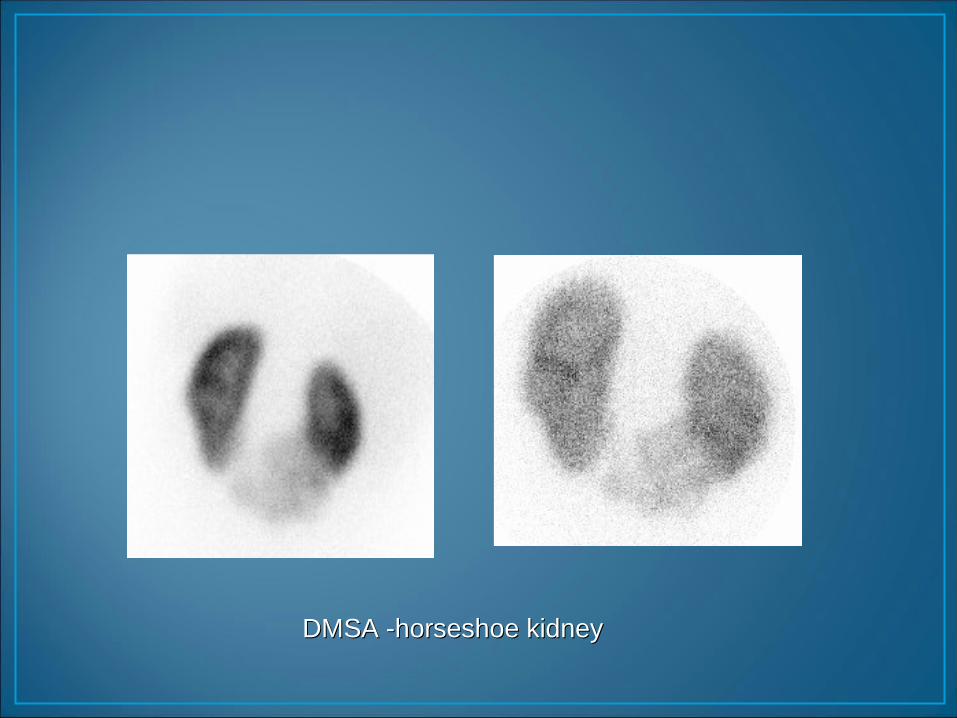
DMSA -horseshoe kidneyDMSA -horseshoe kidney
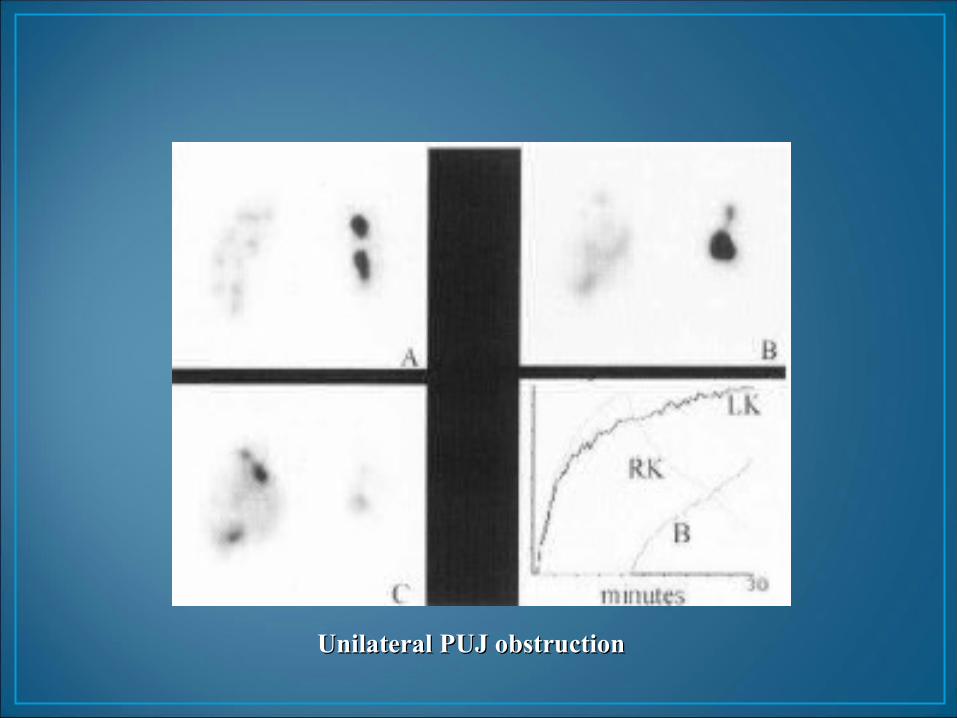
Unilateral PUJ obstructionUnilateral PUJ obstruction