Embed Size (px)
Citation preview
OPEN INFORMATION ITEM SCRUTINY
Agenda Item No. 8
Wolverhampton City Council OPEN INFORMATION ITEM
Health Scrutiny Panel Date 5 July 2012
Originating Service Group(s) WCPCT Risk and Quality Team
Contact Officer(s)/ Sarah Southall Rebecca Brown
Telephone Number(s) 01902 444666
Title Risk Register Report
SUMMARY
The full report details all risks held on WCPCT risk register. The report is broken down into the following
1. Red Risks 2. Risks by speciality/All open risks 3. Risk Reduction 4. Risk Increase 5. New Risks
OPEN INFORMATION ITEM SCRUTINY
1. PURPOSE
1.1 To inform the Scrutiny Board of risks appertaining to Commissioning.
2. BACKGROUND
2.1 WCPCT advocates that all managers are responsible for assessing risks to their service and using a systematic and proactive approach. Identified risks are recorded on organisations risk register,
3. FINANCIAL IMPLICATIONS
3.1 Actions appertaining to risk assessments are assessed for financial implications; significant financial implications are escalated to the appropriate Head of Service and Director.
4. LEGAL IMPLICATIONS
4.1 As with all risks the consequence of not mitigating against known risks or having robust actions in place to manage the risk may lead to legal sanctions beig applied to individual or the organisation.
5. EQUAL OPPORTUNITIES
5.1 N/A
6. ENVIRONMENTAL IMPLICATIONS
6.1 NA
7. SCHEDULE OF BACKGROUND PAPERS Risk Management Report
RM Report July 2012.doc 1
WOLVERHAMPTON CITY PRIMARY CARE TRUST
Meeting: Health Scrutiny Board/Panel
Subject: Risk Register Report
Report of: Director of Public Health
Date: 19 July 2012
1. Purpose of Report To inform the Scrutiny Board/Panel of risks appertaining to Commissioning.
2. Recommendation
For the Scrutiny Board/Panel to note the content of the report.
3. Detail
3.1 Risk Profiling Exercise The risk profiling exercise has now concluded, all teams have profiled risks and entered onto the register. Work has progressed with Primary Care contracting team who have shared the Black Country Cluster risk register which holds all risks relevant to primary care contracts and risks identified during the transition stage. Assurance has been given that the primary care risk register is reviewed monthly at cluster meetings, whilst an overall summary will be entered onto datix to acknowledge the existence of the risk register it is not recommended that all risks are entered from the risk register. This would be duplication of Primary Care contracting teams existing register and would not support the requirement for the risks to be managed and owned by the Cluster Primary Care contracting team in preparation for the transition to working as the NHS Commissioning Board.
3.2 Risk Register
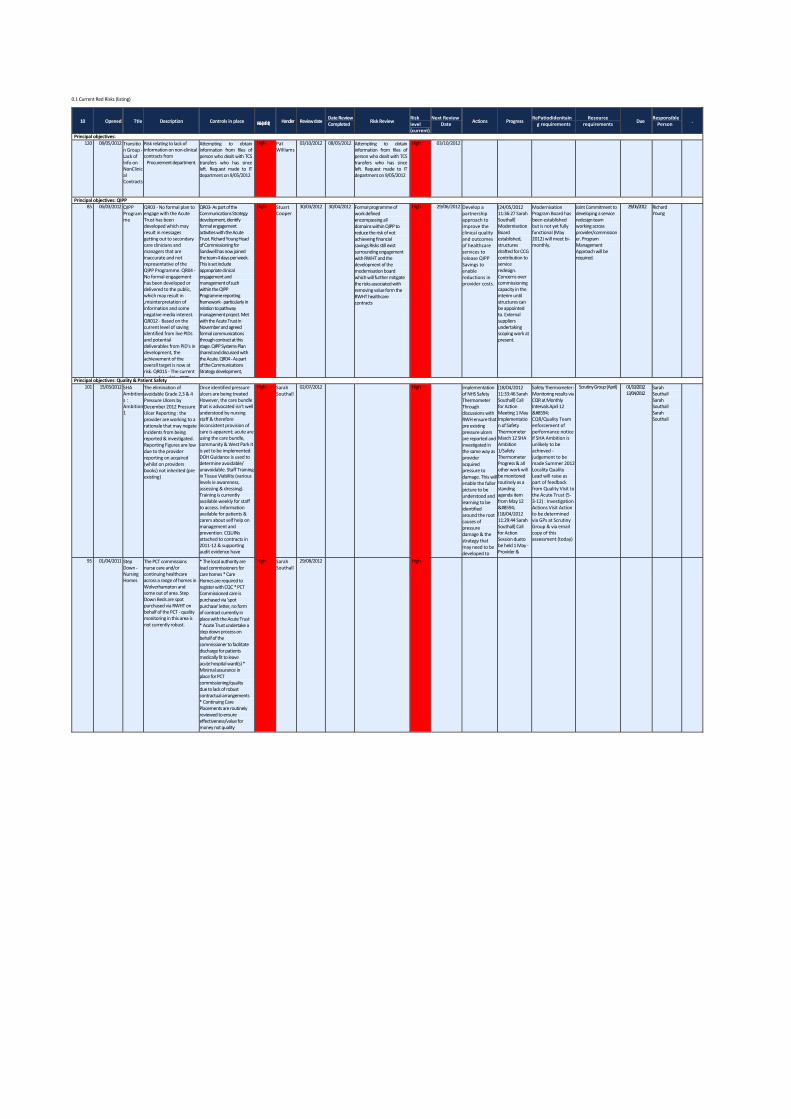
Red Risks
There are currently 3 on-going and 1 new red risks on the register as follows: 1. QIPP 2. SHA Ambition 1 – Elimination of grade 2, 3 & 4 pressure ulcers 3. Step Down Beds – Inadequate quality monitoring
1 new red risk has been added to the register regarding lack of information on non-clinical contracts - this was recognised in May, however not entered onto the register until June 2012. Full details of red risks and associated information and actions can be seen in attachment 1.
RM Report July 2012.doc 2
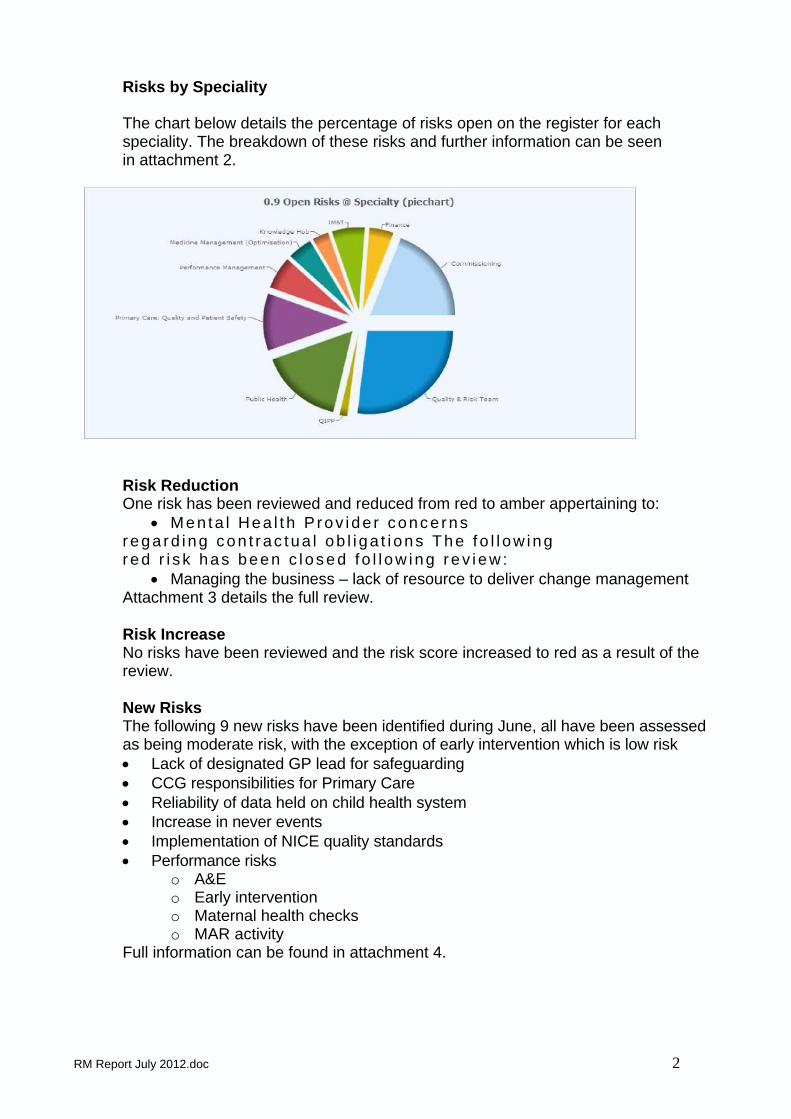
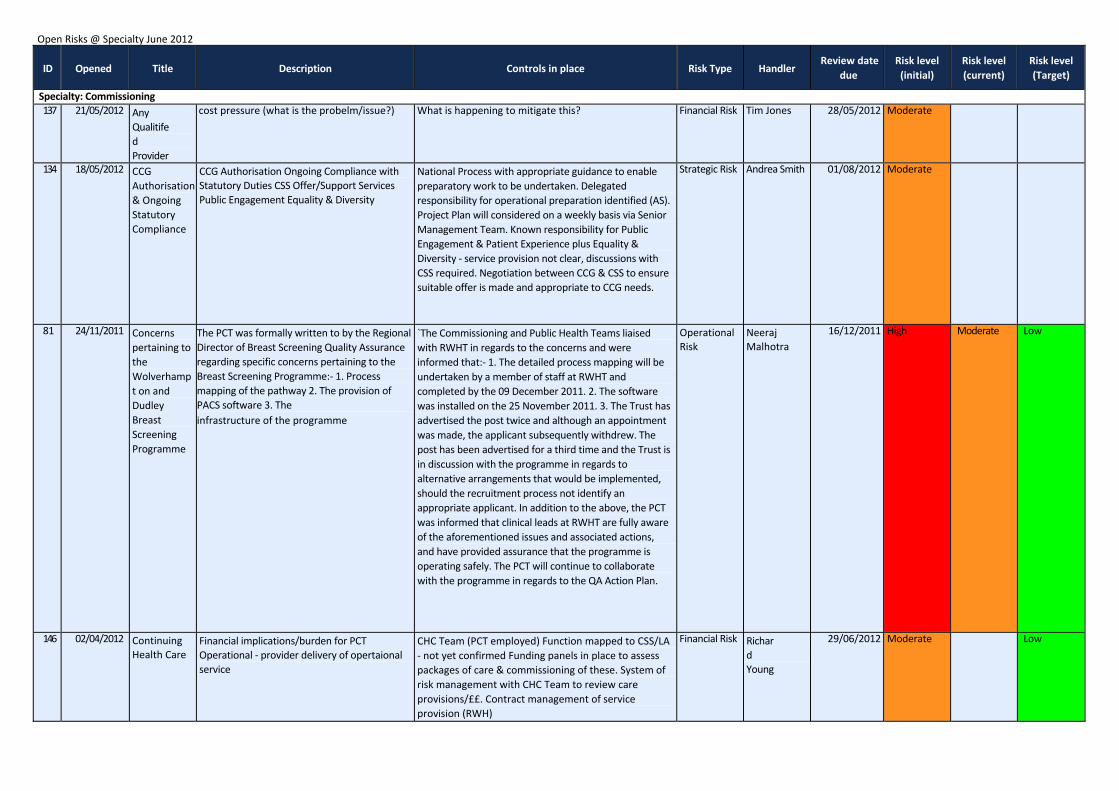
Risks by Speciality
The chart below details the percentage of risks open on the register for each speciality. The breakdown of these risks and further information can be seen in attachment 2.
Risk Reduction One risk has been reviewed and reduced from red to amber appertaining to:
• Men ta l Hea l t h P rov i de r conce rns r ega r d ing c on t r ac tua l ob l i ga t i ons T he f o l l ow ing r ed r i s k has been c l os ed f o l l ow ing r ev i ew :
• Managing the business – lack of resource to deliver change management Attachment 3 details the full review.
Risk Increase No risks have been reviewed and the risk score increased to red as a result of the review.
New Risks The following 9 new risks have been identified during June, all have been assessed as being moderate risk, with the exception of early intervention which is low risk • Lack of designated GP lead for safeguarding • CCG responsibilities for Primary Care • Reliability of data held on child health system • Increase in never events • Implementation of NICE quality standards • Performance risks
o A&E o Early intervention o Maternal health checks o MAR activity
Full information can be found in attachment 4.
0.1 Current Red Risks (listing)
10 Opened Ttle Description Controls in place Risk(initvell) Handler Review date Date Review Completed Risk Review
Risk level (current)
Next Review Date Actions Progress
RePatiodidenitain g requirements
Resource requirements Due
Responsible Person .
Principal objectives: 120 08/05/2012 Transitio
n Group ‐ Lack of Info on NonClinic al Contracts
Risk relating to lack of information on non‐clinical contracts from Procurement department.
Attempting to obtain information from files of person who dealt with TCS transfers who has since left. Request made to IT department on 9/05/2012
High Pat Williams
03/10/2012 08/05/2012 Attempting to obtain information from files of person who dealt with TCS transfers who has since left. Request made to IT department on 9/05/2012
High 03/10/2012
Principal objectives: QIPP 85 06/03/2012 QIPP
Program me
QR03 ‐ No formal plan to engage with the Acute Trust has been developed which may result in messages getting out to secondary care clinicians and managers that are inaccurate and not representative of the QIPP Programme. QR04 ‐ No formal engagement has been developed or delivered to the public, which may result in ,misinterpretation of information and some negative media interest. QR012 ‐ Based on the current level of saving identified from live PIDs and potential deliverables from PID's in development, the achievement of the overall target is now at risk. QR015 ‐ The current ownership of the QIPP
QR03‐ As part of the Communications Strategy development, identify formal engagement activities with the Acute Trust. Richard Young Head of Commissioning for Sandwell has now joined the team 4 days per week. This is set include appropriate clinical engagement and management of such within the QIPP Programme reporting framework ‐ particularly in relation to pathway management project. Met with the Acute Trust in November and agreed formal communications through contract at this stage. QIPP Systems Plan shared and discussed with the Acute. QR04 ‐ As part of the Communications Strategy development,
High Stuart Cooper
30/03/2012 30/04/2012 Formal programme of work defined encompassing all domains within QIPP to reduce the risk of not achieveing financial savings Risks still exist surrounding engagement with RWHT and the development of the modernisation board which will further mitigate the risks associated with removing value form the RWHT healthcare contracts
High 29/06/2012 Develop a partnership approach to improve the clinical quality and outcomes of healthcare services to release QIPP Savings to enable reductions in provider costs.
[24/05/2012 11:36:27 Sarah Southall] Modernisation Board established, structures drafted for CCG contribution to service redesign. Concerns over commissioning capacity in the interim until structures can be appointed to. External suppliers undertaking scoping work at present.
Modernisation Program Board has been established but is not yet fully functional (May 2012) will meet bi‐ monthly.
Joint Commitment to developing a service redesign team working across provider/commission er. Program Management Approach will be required.
29/06/2012 Richard Young
Principal objectives: Quality & Patient Safety 101 15/03/2012 SHA
Ambition s : Ambition 1
The elimination of avoidable Grade 2,3 & 4 Pressure Ulcers by December 2012 Pressure Ulcer Reporting : the provider are working to a rationale that may negate incidents from being reported & investigated. Reporting Figures are low due to the provider reporting on acquired (whilst on providers books) not inherited (pre existing)
Once identified pressure ulcers are being treated However, the care bundle that is advocated isn't well understood by nursing staff & therefore inconsistent provision of care is apparent; acute are using the care bundle, community & West Park it is yet to be implemented. DOH Guidance is used to determine avoidable/ unavoidable. Staff Training in Tissue Viability (various levels ie awareness, assessing & dressing). Training is currently available weekly for staff to access. Information available for patients & carers about self help on management and prevention. CQUINs attached to contracts in 2011‐12 & supporting audit evidence have
High Sarah Southall
02/07/2012
High
Implementation of NHS Safety Thermometer Through discussions with RWH ensure that pre existing pressure ulcers are reported and investigated in the same way as provider acquired pressure to damage. This will enable the fuller picture to be understood and learning to be identified around the root causes of pressure damage & the strategy that may need to be developed to
[18/04/2012 11:33:46 Sarah Southall] Call for Action Meeting 1 May Implementation of Safety Thermometer March 12 SHA Ambition 1/Safety Thermometer Progress & all other work will be monitored routinely as a standing agenda item from May 12 → [18/04/2012 11:29:44 Sarah Southall] Call for Action Session dueto be held 1 May ‐ Provider &
Safety Thermometer : Monitoring results via CQR at Monthly Intervals April 12 → CQR/Quality Team enforcement of performance notice if SHA Ambition is unlikely to be achieved ‐ judgement to be made Summer 2012 Locality Quality Lead will raise as part of feedback from Quality Visit to the Acute Trust (5‐3‐12) : Investigation Actions Visit Action to be determined via GPs at Scrutiny Group & via email copy of this assessment (today)
Scrutiny Group (April) 01/10/2012 13/04/2012
Sarah Southall Sarah Southall Sarah Southall
95 01/04/2011 Step Down ‐ Nursing Homes
The PCT commissions nurse care and/or continuing healthcare across a range of homes in Wolverhampton and some out of area. Step Down Beds are spot purchased via RWHT on behalf of the PCT ‐ quality monitoring in this area is not currently robust.
* The local authority are lead commissioners for care homes * Care Homes are required to register with CQC * PCT Commissioned care is purchased via 'spot purchase' letter, no form of contract currently in place with the Acute Trust * Acute Trust undertake a step down process on behalf of the commissioner to facilitate discharge for patients medically fit to leave acute hospital ward(s) * Minimal assurance in place for PCT commissioning/quality due to lack of robust contractual arrangements * Continuing Care Placements are routinely reviewed to ensure effectiveness/value for money not quality
High Sarah Southall
29/08/2012
High
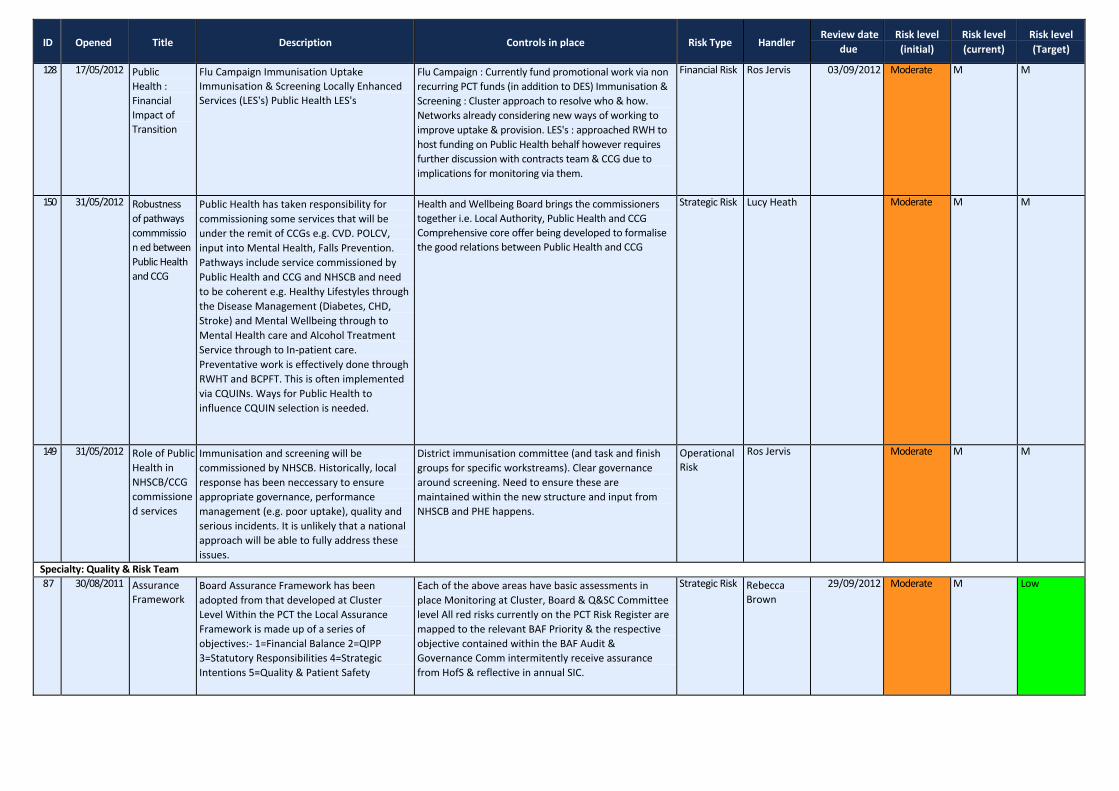
Open Risks @ Specialty June 2012
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
Specialty: Commissioning 137 21/05/2012 Any
Qualitifed Provider
cost pressure (what is the probelm/issue?) What is happening to mitigate this? Financial Risk Tim Jones 28/05/2012 Moderate
134 18/05/2012 CCG Authorisation & Ongoing Statutory Compliance
CCG Authorisation Ongoing Compliance with Statutory Duties CSS Offer/Support Services Public Engagement Equality & Diversity
National Process with appropriate guidance to enable preparatory work to be undertaken. Delegated responsibility for operational preparation identified (AS). Project Plan will considered on a weekly basis via Senior Management Team. Known responsibility for Public Engagement & Patient Experience plus Equality & Diversity ‐ service provision not clear, discussions with CSS required. Negotiation between CCG & CSS to ensure suitable offer is made and appropriate to CCG needs.
Strategic Risk Andrea Smith 01/08/2012 Moderate
81 24/11/2011 Concerns pertaining to the Wolverhampt on and Dudley Breast Screening Programme
The PCT was formally written to by the Regional Director of Breast Screening Quality Assurance regarding specific concerns pertaining to the Breast Screening Programme:‐ 1. Process mapping of the pathway 2. The provision of PACS software 3. The infrastructure of the programme
`The Commissioning and Public Health Teams liaised with RWHT in regards to the concerns and were informed that:‐ 1. The detailed process mapping will be undertaken by a member of staff at RWHT and completed by the 09 December 2011. 2. The software was installed on the 25 November 2011. 3. The Trust has advertised the post twice and although an appointment was made, the applicant subsequently withdrew. The post has been advertised for a third time and the Trust is in discussion with the programme in regards to alternative arrangements that would be implemented, should the recruitment process not identify an appropriate applicant. In addition to the above, the PCT was informed that clinical leads at RWHT are fully aware of the aforementioned issues and associated actions, and have provided assurance that the programme is operating safely. The PCT will continue to collaborate with the programme in regards to the QA Action Plan.
Operational Risk
Neeraj Malhotra
16/12/2011 High Moderate Low
146 02/04/2012 Continuing Health Care
Financial implications/burden for PCT Operational ‐ provider delivery of opertaional service
CHC Team (PCT employed) Function mapped to CSS/LA ‐ not yet confirmed Funding panels in place to assess packages of care & commissioning of these. System of risk management with CHC Team to review care provisions/££. Contract management of service provision (RWH)
Financial Risk Richard Young
29/06/2012 Moderate Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
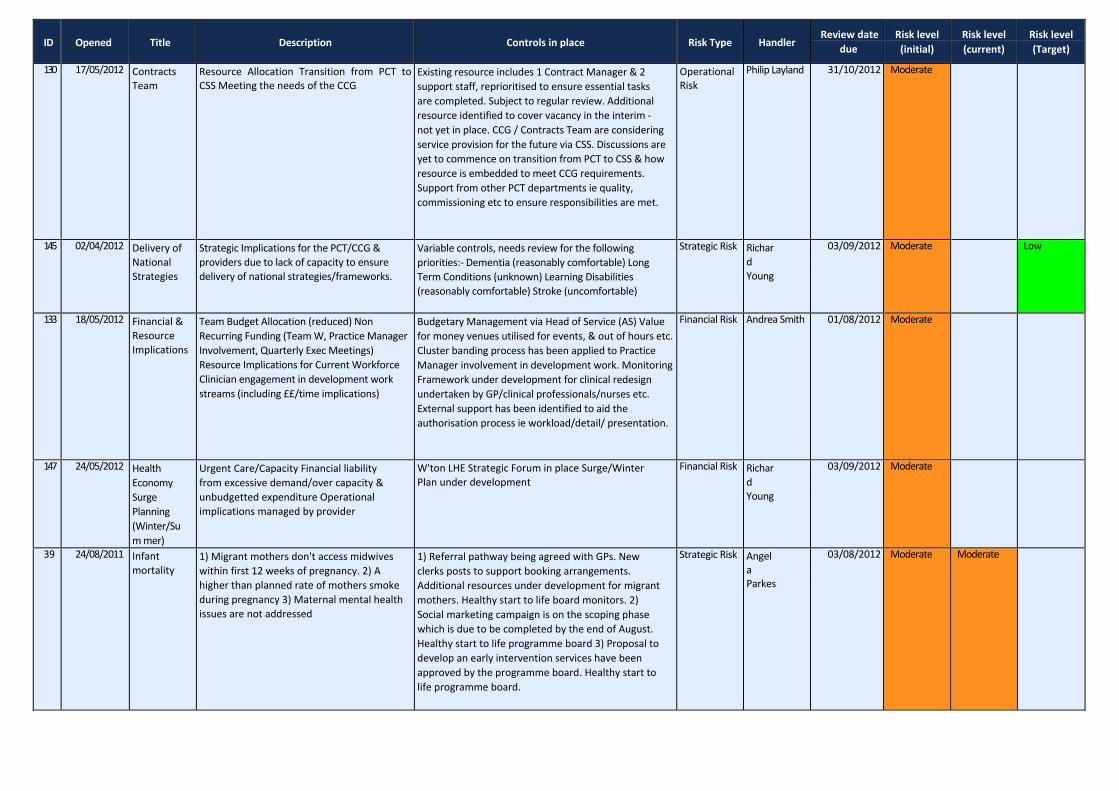
130 17/05/2012 Contracts Team
Resource Allocation Transition from PCT to CSS Meeting the needs of the CCG
Existing resource includes 1 Contract Manager & 2 support staff, reprioritised to ensure essential tasks are completed. Subject to regular review. Additional resource identified to cover vacancy in the interim ‐ not yet in place. CCG / Contracts Team are considering service provision for the future via CSS. Discussions are yet to commence on transition from PCT to CSS & how resource is embedded to meet CCG requirements. Support from other PCT departments ie quality, commissioning etc to ensure responsibilities are met.
Operational Risk
Philip Layland 31/10/2012 Moderate
145 02/04/2012 Delivery of National Strategies
Strategic Implications for the PCT/CCG & providers due to lack of capacity to ensure delivery of national strategies/frameworks.
Variable controls, needs review for the following priorities:‐ Dementia (reasonably comfortable) Long Term Conditions (unknown) Learning Disabilities (reasonably comfortable) Stroke (uncomfortable)
Strategic Risk Richard Young
03/09/2012 Moderate Low
133 18/05/2012 Financial & Resource Implications
Team Budget Allocation (reduced) Non Recurring Funding (Team W, Practice Manager Involvement, Quarterly Exec Meetings) Resource Implications for Current Workforce Clinician engagement in development work streams (including ££/time implications)
Budgetary Management via Head of Service (AS) Value for money venues utilised for events, & out of hours etc. Cluster banding process has been applied to Practice Manager involvement in development work. Monitoring Framework under development for clinical redesign undertaken by GP/clinical professionals/nurses etc. External support has been identified to aid the authorisation process ie workload/detail/ presentation.
Financial Risk Andrea Smith 01/08/2012 Moderate
147 24/05/2012 Health Economy Surge Planning (Winter/Sum mer)
Urgent Care/Capacity Financial liability from excessive demand/over capacity & unbudgetted expenditure Operational implications managed by provider
W'ton LHE Strategic Forum in place Surge/Winter Plan under development
Financial Risk Richard Young
03/09/2012 Moderate
39 24/08/2011 Infant mortality
1) Migrant mothers don't access midwives within first 12 weeks of pregnancy. 2) A higher than planned rate of mothers smoke during pregnancy 3) Maternal mental health issues are not addressed
1) Referral pathway being agreed with GPs. New clerks posts to support booking arrangements. Additional resources under development for migrant mothers. Healthy start to life board monitors. 2) Social marketing campaign is on the scoping phase which is due to be completed by the end of August. Healthy start to life programme board 3) Proposal to develop an early intervention services have been approved by the programme board. Healthy start to life programme board.
Strategic Risk Angela Parkes
03/08/2012 Moderate Moderate
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
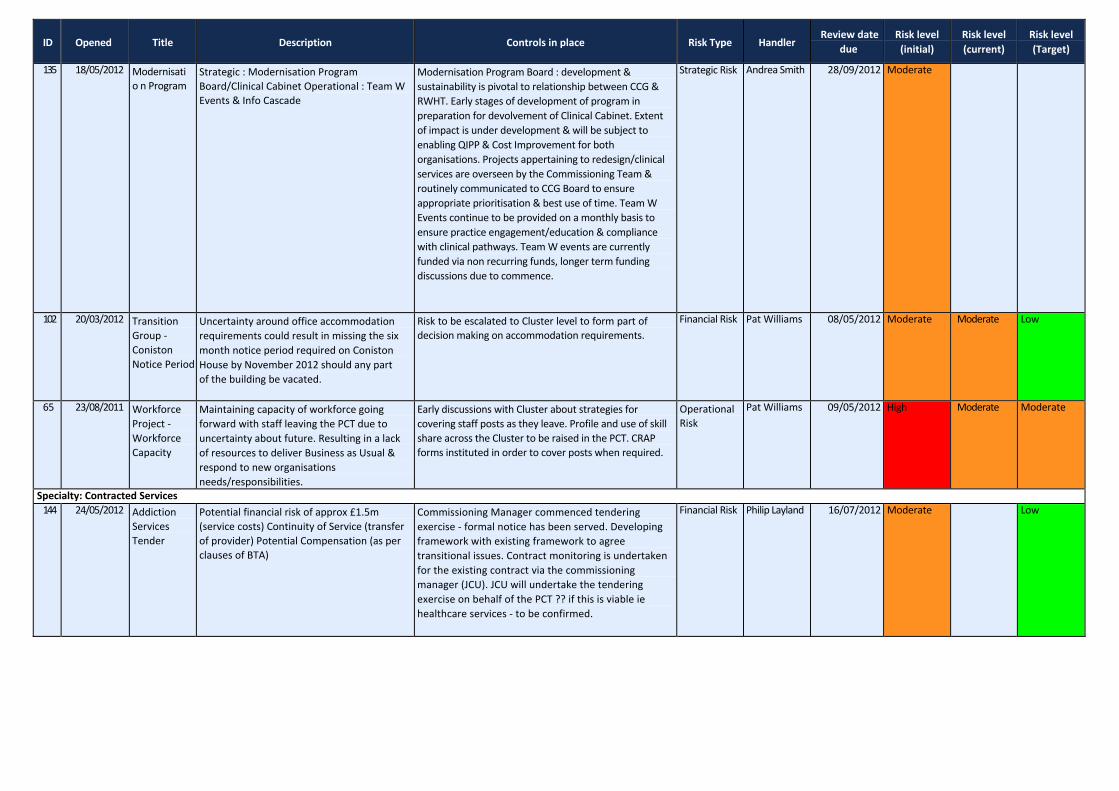
135 18/05/2012 Modernisatio n Program
Strategic : Modernisation Program Board/Clinical Cabinet Operational : Team W Events & Info Cascade
Modernisation Program Board : development & sustainability is pivotal to relationship between CCG & RWHT. Early stages of development of program in preparation for devolvement of Clinical Cabinet. Extent of impact is under development & will be subject to enabling QIPP & Cost Improvement for both organisations. Projects appertaining to redesign/clinical services are overseen by the Commissioning Team & routinely communicated to CCG Board to ensure appropriate prioritisation & best use of time. Team W Events continue to be provided on a monthly basis to ensure practice engagement/education & compliance with clinical pathways. Team W events are currently funded via non recurring funds, longer term funding discussions due to commence.
Strategic Risk Andrea Smith 28/09/2012 Moderate
102 20/03/2012 Transition Group ‐ Coniston Notice Period
Uncertainty around office accommodation requirements could result in missing the six month notice period required on Coniston House by November 2012 should any part of the building be vacated.
Risk to be escalated to Cluster level to form part of decision making on accommodation requirements.
Financial Risk Pat Williams 08/05/2012 Moderate Moderate Low
65 23/08/2011 Workforce Project ‐ Workforce Capacity
Maintaining capacity of workforce going forward with staff leaving the PCT due to uncertainty about future. Resulting in a lack of resources to deliver Business as Usual & respond to new organisations needs/responsibilities.
Early discussions with Cluster about strategies for covering staff posts as they leave. Profile and use of skill share across the Cluster to be raised in the PCT. CRAP forms instituted in order to cover posts when required.
Operational Risk
Pat Williams 09/05/2012 High Moderate Moderate
Specialty: Contracted Services 144 24/05/2012 Addiction
Services Tender
Potential financial risk of approx £1.5m (service costs) Continuity of Service (transfer of provider) Potential Compensation (as per clauses of BTA)
Commissioning Manager commenced tendering exercise ‐ formal notice has been served. Developing framework with existing framework to agree transitional issues. Contract monitoring is undertaken for the existing contract via the commissioning manager (JCU). JCU will undertake the tendering exercise on behalf of the PCT ?? if this is viable ie healthcare services ‐ to be confirmed.
Financial Risk Philip Layland 16/07/2012 Moderate Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
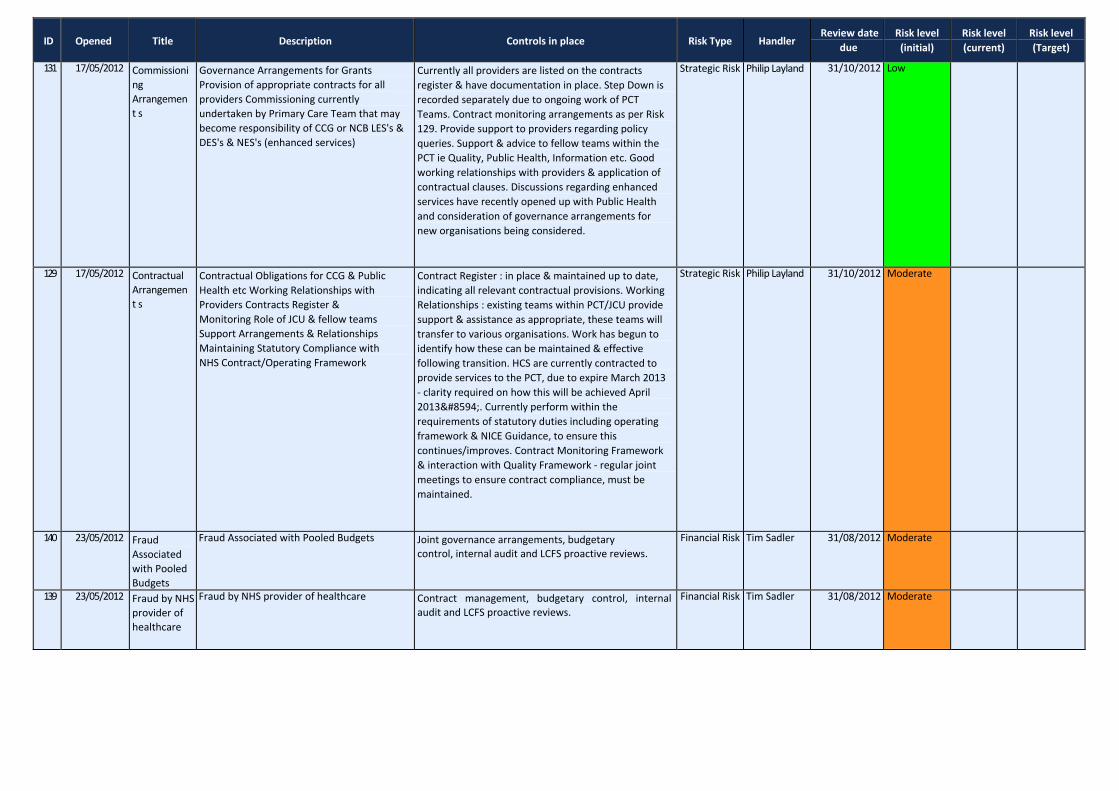
131 17/05/2012 Commissioni ng Arrangement s
Governance Arrangements for Grants Provision of appropriate contracts for all providers Commissioning currently undertaken by Primary Care Team that may become responsibility of CCG or NCB LES's & DES's & NES's (enhanced services)
Currently all providers are listed on the contracts register & have documentation in place. Step Down is recorded separately due to ongoing work of PCT Teams. Contract monitoring arrangements as per Risk 129. Provide support to providers regarding policy queries. Support & advice to fellow teams within the PCT ie Quality, Public Health, Information etc. Good working relationships with providers & application of contractual clauses. Discussions regarding enhanced services have recently opened up with Public Health and consideration of governance arrangements for new organisations being considered.
Strategic Risk Philip Layland 31/10/2012 Low
129 17/05/2012 Contractual Arrangement s
Contractual Obligations for CCG & Public Health etc Working Relationships with Providers Contracts Register & Monitoring Role of JCU & fellow teams Support Arrangements & Relationships Maintaining Statutory Compliance with NHS Contract/Operating Framework
Contract Register : in place & maintained up to date, indicating all relevant contractual provisions. Working Relationships : existing teams within PCT/JCU provide support & assistance as appropriate, these teams will transfer to various organisations. Work has begun to identify how these can be maintained & effective following transition. HCS are currently contracted to provide services to the PCT, due to expire March 2013 ‐ clarity required on how this will be achieved April 2013→. Currently perform within the requirements of statutory duties including operating framework & NICE Guidance, to ensure this continues/improves. Contract Monitoring Framework & interaction with Quality Framework ‐ regular joint meetings to ensure contract compliance, must be maintained.
Strategic Risk Philip Layland 31/10/2012 Moderate
140 23/05/2012 Fraud Associated with Pooled Budgets
Fraud Associated with Pooled Budgets Joint governance arrangements, budgetary control, internal audit and LCFS proactive reviews.
Financial Risk Tim Sadler 31/08/2012 Moderate
139 23/05/2012 Fraud by NHS provider of healthcare
Fraud by NHS provider of healthcare Contract management, budgetary control, internal audit and LCFS proactive reviews.
Financial Risk Tim Sadler 31/08/2012 Moderate
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
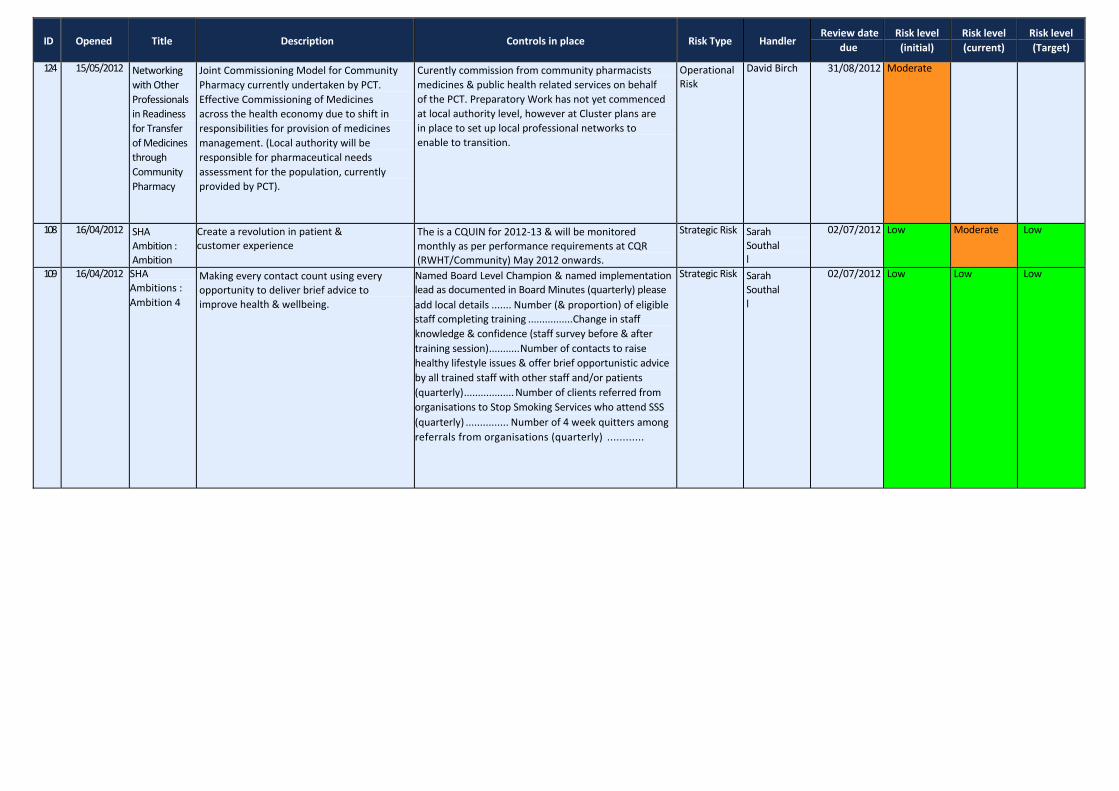
124 15/05/2012 Networking with Other Professionals in Readiness for Transfer of Medicines through Community Pharmacy
Joint Commissioning Model for Community Pharmacy currently undertaken by PCT. Effective Commissioning of Medicines across the health economy due to shift in responsibilities for provision of medicines management. (Local authority will be responsible for pharmaceutical needs assessment for the population, currently provided by PCT).
Curently commission from community pharmacists medicines & public health related services on behalf of the PCT. Preparatory Work has not yet commenced at local authority level, however at Cluster plans are in place to set up local professional networks to enable to transition.
Operational Risk
David Birch 31/08/2012 Moderate
108 16/04/2012 SHA Ambition : Ambition
Create a revolution in patient & customer experience
The is a CQUIN for 2012‐13 & will be monitored monthly as per performance requirements at CQR (RWHT/Community) May 2012 onwards.
Strategic Risk Sarah Southall
02/07/2012 Low Moderate Low
109 16/04/2012 SHA Ambitions : Ambition 4
Making every contact count using every opportunity to deliver brief advice to improve health & wellbeing.
Named Board Level Champion & named implementation lead as documented in Board Minutes (quarterly) please add local details ....... Number (& proportion) of eligible staff completing training ................Change in staff knowledge & confidence (staff survey before & after training session)...........Number of contacts to raise healthy lifestyle issues & offer brief opportunistic advice by all trained staff with other staff and/or patients (quarterly)..................Number of clients referred from organisations to Stop Smoking Services who attend SSS (quarterly) ............... Number of 4 week quitters among referrals from organisations (quarterly) ............
Strategic Risk Sarah Southall
02/07/2012 Low Low Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
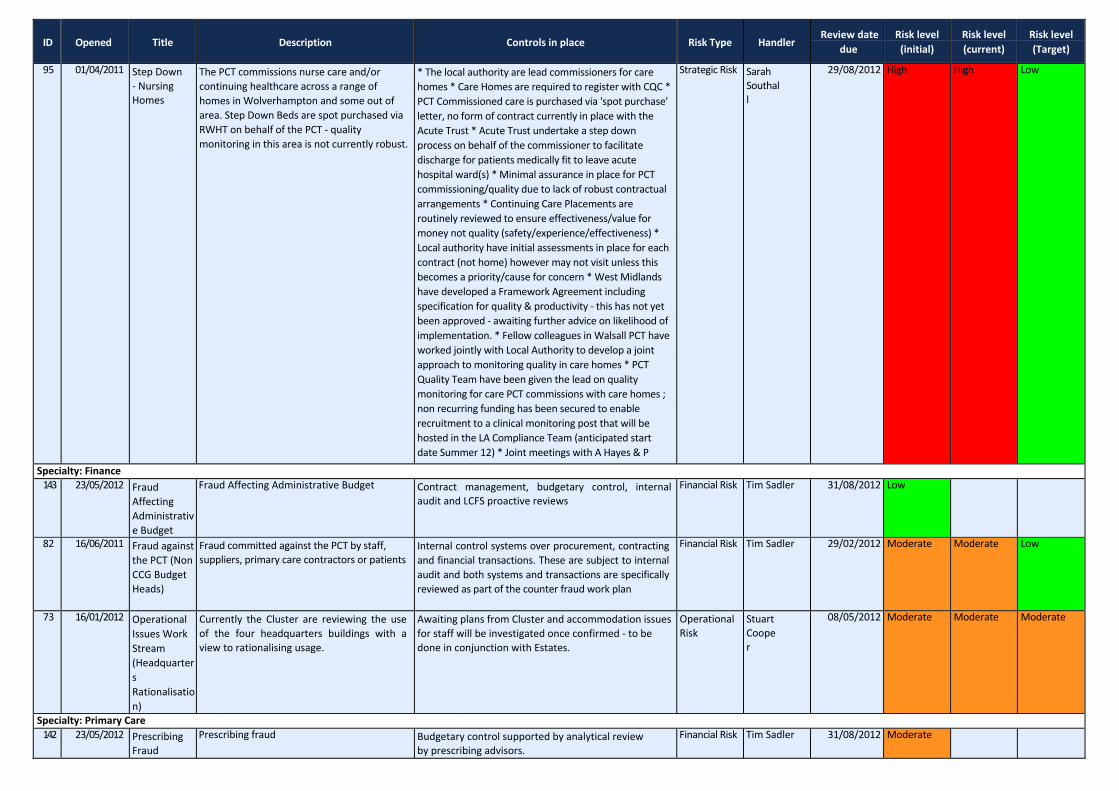
95 01/04/2011 Step Down ‐ Nursing Homes
The PCT commissions nurse care and/or continuing healthcare across a range of homes in Wolverhampton and some out of area. Step Down Beds are spot purchased via RWHT on behalf of the PCT ‐ quality monitoring in this area is not currently robust.
* The local authority are lead commissioners for care homes * Care Homes are required to register with CQC * PCT Commissioned care is purchased via 'spot purchase' letter, no form of contract currently in place with the Acute Trust * Acute Trust undertake a step down process on behalf of the commissioner to facilitate discharge for patients medically fit to leave acute hospital ward(s) * Minimal assurance in place for PCT commissioning/quality due to lack of robust contractual arrangements * Continuing Care Placements are routinely reviewed to ensure effectiveness/value for money not quality (safety/experience/effectiveness) * Local authority have initial assessments in place for each contract (not home) however may not visit unless this becomes a priority/cause for concern * West Midlands have developed a Framework Agreement including specification for quality & productivity ‐ this has not yet been approved ‐ awaiting further advice on likelihood of implementation. * Fellow colleagues in Walsall PCT have worked jointly with Local Authority to develop a joint approach to monitoring quality in care homes * PCT Quality Team have been given the lead on quality monitoring for care PCT commissions with care homes ; non recurring funding has been secured to enable recruitment to a clinical monitoring post that will be hosted in the LA Compliance Team (anticipated start date Summer 12) * Joint meetings with A Hayes & P
Strategic Risk Sarah Southall
29/08/2012 High High Low
Specialty: Finance 143 23/05/2012 Fraud
Affecting Administrativ e Budget
Fraud Affecting Administrative Budget Contract management, budgetary control, internal audit and LCFS proactive reviews
Financial Risk Tim Sadler 31/08/2012 Low
82 16/06/2011 Fraud against the PCT (Non CCG Budget Heads)
Fraud committed against the PCT by staff, suppliers, primary care contractors or patients
Internal control systems over procurement, contracting and financial transactions. These are subject to internal audit and both systems and transactions are specifically reviewed as part of the counter fraud work plan
Financial Risk Tim Sadler 29/02/2012 Moderate Moderate Low
73 16/01/2012 Operational Issues Work Stream (Headquarter s Rationalisatio n)
Currently the Cluster are reviewing the use of the four headquarters buildings with a view to rationalising usage.
Awaiting plans from Cluster and accommodation issues for staff will be investigated once confirmed ‐ to be done in conjunction with Estates.
Operational Risk
Stuart Cooper
08/05/2012 Moderate Moderate Moderate
Specialty: Primary Care 142 23/05/2012 Prescribing
Fraud Prescribing fraud Budgetary control supported by analytical review
by prescribing advisors. Financial Risk Tim Sadler 31/08/2012 Moderate
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
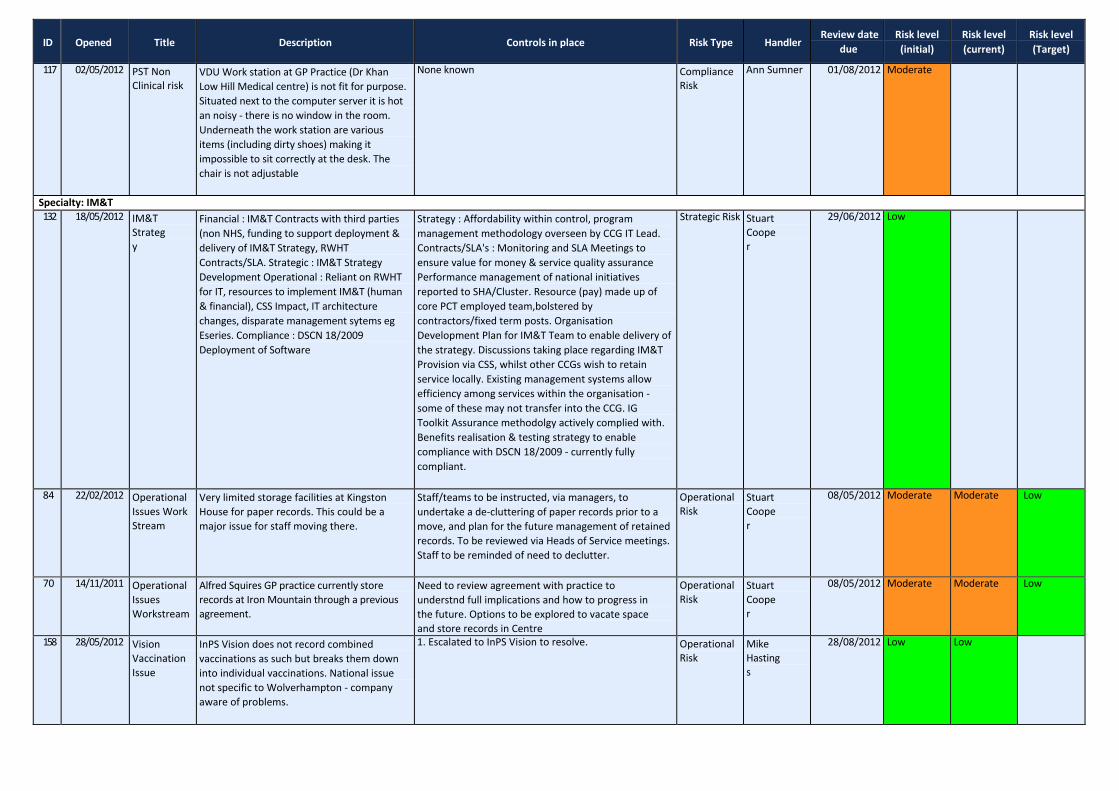
117 02/05/2012 PST Non Clinical risk
VDU Work station at GP Practice (Dr Khan Low Hill Medical centre) is not fit for purpose. Situated next to the computer server it is hot an noisy ‐ there is no window in the room. Underneath the work station are various items (including dirty shoes) making it impossible to sit correctly at the desk. The chair is not adjustable
None known Compliance Risk
Ann Sumner 01/08/2012 Moderate
Specialty: IM&T 132 18/05/2012 IM&T
Strategy
Financial : IM&T Contracts with third parties (non NHS, funding to support deployment & delivery of IM&T Strategy, RWHT Contracts/SLA. Strategic : IM&T Strategy Development Operational : Reliant on RWHT for IT, resources to implement IM&T (human & financial), CSS Impact, IT architecture changes, disparate management sytems eg Eseries. Compliance : DSCN 18/2009 Deployment of Software
Strategy : Affordability within control, program management methodology overseen by CCG IT Lead. Contracts/SLA's : Monitoring and SLA Meetings to ensure value for money & service quality assurance Performance management of national initiatives reported to SHA/Cluster. Resource (pay) made up of core PCT employed team,bolstered by contractors/fixed term posts. Organisation Development Plan for IM&T Team to enable delivery of the strategy. Discussions taking place regarding IM&T Provision via CSS, whilst other CCGs wish to retain service locally. Existing management systems allow efficiency among services within the organisation ‐ some of these may not transfer into the CCG. IG Toolkit Assurance methodolgy actively complied with. Benefits realisation & testing strategy to enable compliance with DSCN 18/2009 ‐ currently fully compliant.
Strategic Risk Stuart Cooper
29/06/2012 Low
84 22/02/2012 Operational Issues Work Stream
Very limited storage facilities at Kingston House for paper records. This could be a major issue for staff moving there.
Staff/teams to be instructed, via managers, to undertake a de‐cluttering of paper records prior to a move, and plan for the future management of retained records. To be reviewed via Heads of Service meetings. Staff to be reminded of need to declutter.
Operational Risk
Stuart Cooper
08/05/2012 Moderate Moderate Low
70 14/11/2011 Operational Issues Workstream
Alfred Squires GP practice currently store records at Iron Mountain through a previous agreement.
Need to review agreement with practice to understnd full implications and how to progress in the future. Options to be explored to vacate space and store records in Centre
Operational Risk
Stuart Cooper
08/05/2012 Moderate Moderate Low
158 28/05/2012 Vision Vaccination Issue
InPS Vision does not record combined vaccinations as such but breaks them down into individual vaccinations. National issue not specific to Wolverhampton ‐ company aware of problems.
1. Escalated to InPS Vision to resolve. Operational Risk
Mike Hastings
28/08/2012 Low Low

ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
Specialty: Independent/Private Sector 141 23/05/2012 Fraud by
Non NHS Providers of Healthcare Services
Fraud by Non NHS Providers of Healthcare Services
Contract management, budgetary control, internal audit and LCFS proactive reviews.
Financial Risk Tim Sadler 31/08/2012 Moderate
Specialty: Knowledge Hub 127 16/05/2012 Information
Service : Transition to CSS
CSS Business Intelligence Offer Convergence of Data Warehouse(s) Move to new Location (no transition plan) Mortality Reporting Public Health Access to New Data Warehouse
Business Intelligence Offer ‐ small group meeting to progress AT will become involved (weekly meetings). Business Continuity Plan for Data Warehouse being developed via AT/SC/Dr Mahindroo to minimise risk of loss/disruption to data. Public Health Access has been flagged with IT & CSS colleagues to ensure continuity/access etc. Data Consent : MH is seeking support from LMC (summer 2012) to enable Graphnet consent to be progressed. Discussions already commenced with CCG & Dr Foster to ensure continuity of availability to CCG.
Strategic Risk Alison Turner 03/09/2012 Moderate M M
126 16/05/2012 Information Team & Capacity
Retention of Staff Increasing Workload Driven by Transition Office Move Contractual Reporting & Information Analysis
Team is curerntly at full compliment, no vacancies/nor notice given. Priorities lists in place overseen by Head of Service to ensure team remain focussed ‐ regularly reviewed. Working collaboratively across BCC to identify opportunities to share/exchange/innovate information services. Regular discussions in regard to move to single site, plans shared & preparation taking place ie data warehouse etc. Team Meetings taking place (weekly) to cascade/update/review team business.
Strategic Risk Alison Turner 28/09/2012 Moderate M M
Specialty: Medicine Management (Optimisation) 125 15/05/2012 Management
of Controlled Drugs
Statutory Responsibility of the PCT placed by the government following the Shipman Enquiry including oversight of all providers across the health economy ie independent contractors, community pharmacy, Nuffield, RWH, BCP, Compton, St Judes, Sedgeley House, Ambulance Service etc Responsibility to work with local Police & Regulatory Organisations.
Quarterly Controlled Drugs Local Intelligence Network Meeting All organisations have to submit a quarterly occurrence report, exposing deficiencies & information sharing agreement in place. Use Prescribing data sources to monitor prescribing behaviour in GP Practices. Included within Excellence in Primary Care ‐ contract monitoring tools for GPs, Dentists & community Pharmacists.
Strategic Risk David Birch 31/10/2012 Low M M
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
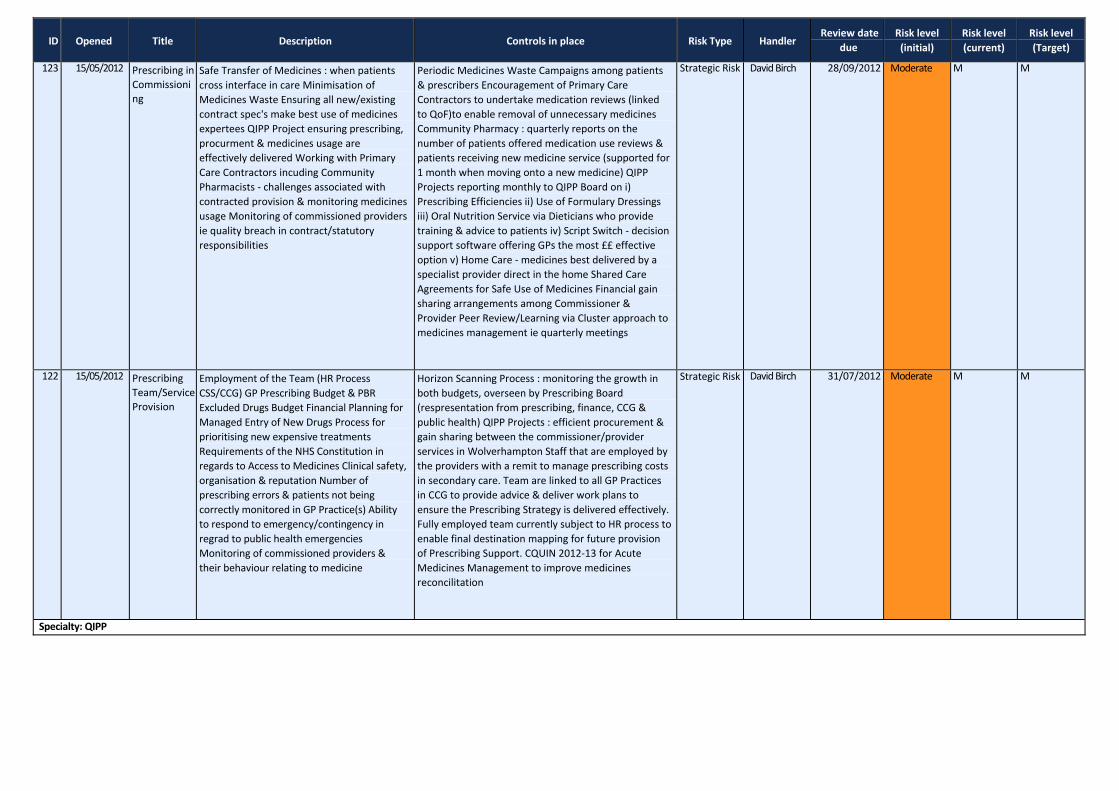
123 15/05/2012 Prescribing in Commissioni ng
Safe Transfer of Medicines : when patients cross interface in care Minimisation of Medicines Waste Ensuring all new/existing contract spec's make best use of medicines expertees QIPP Project ensuring prescribing, procurment & medicines usage are effectively delivered Working with Primary Care Contractors incuding Community Pharmacists ‐ challenges associated with contracted provision & monitoring medicines usage Monitoring of commissioned providers ie quality breach in contract/statutory responsibilities
Periodic Medicines Waste Campaigns among patients & prescribers Encouragement of Primary Care Contractors to undertake medication reviews (linked to QoF)to enable removal of unnecessary medicines Community Pharmacy : quarterly reports on the number of patients offered medication use reviews & patients receiving new medicine service (supported for 1 month when moving onto a new medicine) QIPP Projects reporting monthly to QIPP Board on i) Prescribing Efficiencies ii) Use of Formulary Dressings iii) Oral Nutrition Service via Dieticians who provide training & advice to patients iv) Script Switch ‐ decision support software offering GPs the most ££ effective option v) Home Care ‐ medicines best delivered by a specialist provider direct in the home Shared Care Agreements for Safe Use of Medicines Financial gain sharing arrangements among Commissioner & Provider Peer Review/Learning via Cluster approach to medicines management ie quarterly meetings
Strategic Risk David Birch 28/09/2012 Moderate M M
122 15/05/2012 Prescribing Team/Service Provision
Employment of the Team (HR Process CSS/CCG) GP Prescribing Budget & PBR Excluded Drugs Budget Financial Planning for Managed Entry of New Drugs Process for prioritising new expensive treatments Requirements of the NHS Constitution in regards to Access to Medicines Clinical safety, organisation & reputation Number of prescribing errors & patients not being correctly monitored in GP Practice(s) Ability to respond to emergency/contingency in regrad to public health emergencies Monitoring of commissioned providers & their behaviour relating to medicine
Horizon Scanning Process : monitoring the growth in both budgets, overseen by Prescribing Board (respresentation from prescribing, finance, CCG & public health) QIPP Projects : efficient procurement & gain sharing between the commissioner/provider services in Wolverhampton Staff that are employed by the providers with a remit to manage prescribing costs in secondary care. Team are linked to all GP Practices in CCG to provide advice & deliver work plans to ensure the Prescribing Strategy is delivered effectively. Fully employed team currently subject to HR process to enable final destination mapping for future provision of Prescribing Support. CQUIN 2012‐13 for Acute Medicines Management to improve medicines reconcilitation
Strategic Risk David Birch 31/07/2012 Moderate M M
Specialty: QIPP
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
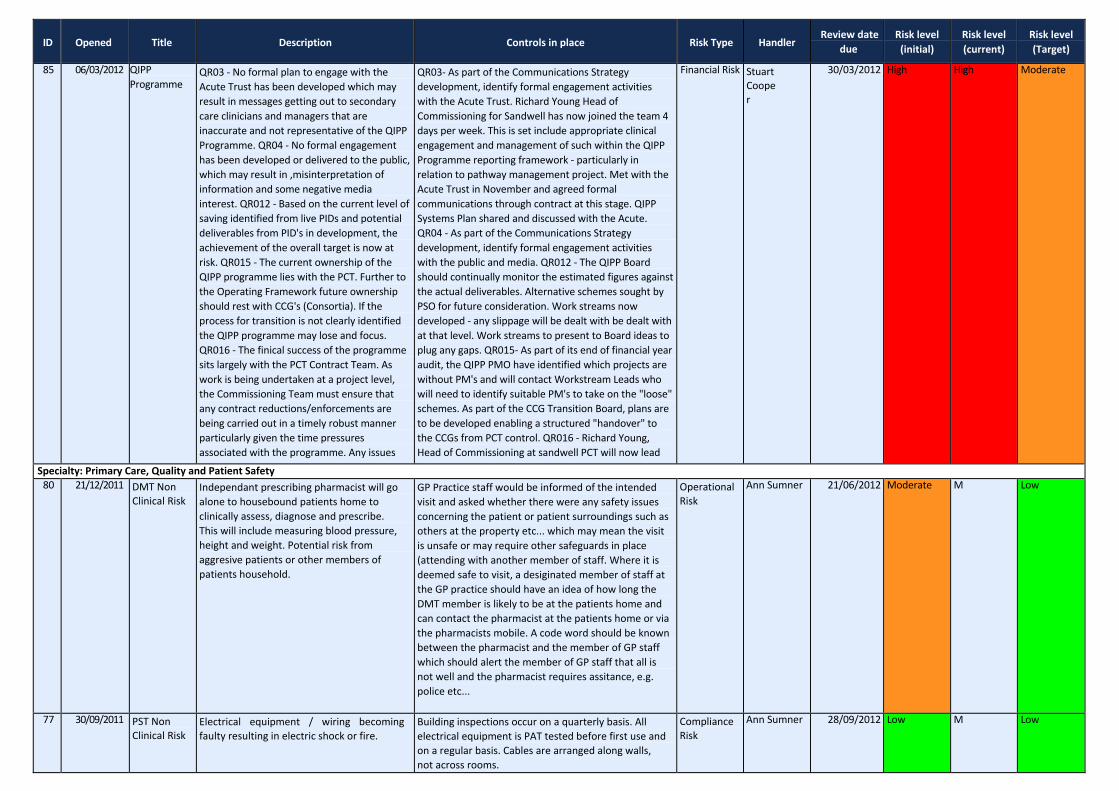
85 06/03/2012 QIPP Programme
QR03 ‐ No formal plan to engage with the Acute Trust has been developed which may result in messages getting out to secondary care clinicians and managers that are inaccurate and not representative of the QIPP Programme. QR04 ‐ No formal engagement has been developed or delivered to the public, which may result in ,misinterpretation of information and some negative media interest. QR012 ‐ Based on the current level of saving identified from live PIDs and potential deliverables from PID's in development, the achievement of the overall target is now at risk. QR015 ‐ The current ownership of the QIPP programme lies with the PCT. Further to the Operating Framework future ownership should rest with CCG's (Consortia). If the process for transition is not clearly identified the QIPP programme may lose and focus. QR016 ‐ The finical success of the programme sits largely with the PCT Contract Team. As work is being undertaken at a project level, the Commissioning Team must ensure that any contract reductions/enforcements are being carried out in a timely robust manner particularly given the time pressures associated with the programme. Any issues
QR03‐ As part of the Communications Strategy development, identify formal engagement activities with the Acute Trust. Richard Young Head of Commissioning for Sandwell has now joined the team 4 days per week. This is set include appropriate clinical engagement and management of such within the QIPP Programme reporting framework ‐ particularly in relation to pathway management project. Met with the Acute Trust in November and agreed formal communications through contract at this stage. QIPP Systems Plan shared and discussed with the Acute. QR04 ‐ As part of the Communications Strategy development, identify formal engagement activities with the public and media. QR012 ‐ The QIPP Board should continually monitor the estimated figures against the actual deliverables. Alternative schemes sought by PSO for future consideration. Work streams now developed ‐ any slippage will be dealt with be dealt with at that level. Work streams to present to Board ideas to plug any gaps. QR015‐ As part of its end of financial year audit, the QIPP PMO have identified which projects are without PM's and will contact Workstream Leads who will need to identify suitable PM's to take on the "loose" schemes. As part of the CCG Transition Board, plans are to be developed enabling a structured "handover" to the CCGs from PCT control. QR016 ‐ Richard Young, Head of Commissioning at sandwell PCT will now lead
Financial Risk Stuart Cooper
30/03/2012 High High Moderate
Specialty: Primary Care, Quality and Patient Safety 80 21/12/2011 DMT Non
Clinical Risk Independant prescribing pharmacist will go alone to housebound patients home to clinically assess, diagnose and prescribe. This will include measuring blood pressure, height and weight. Potential risk from aggresive patients or other members of patients household.
GP Practice staff would be informed of the intended visit and asked whether there were any safety issues concerning the patient or patient surroundings such as others at the property etc... which may mean the visit is unsafe or may require other safeguards in place (attending with another member of staff. Where it is deemed safe to visit, a desiginated member of staff at the GP practice should have an idea of how long the DMT member is likely to be at the patients home and can contact the pharmacist at the patients home or via the pharmacists mobile. A code word should be known between the pharmacist and the member of GP staff which should alert the member of GP staff that all is not well and the pharmacist requires assitance, e.g. police etc...
Operational Risk
Ann Sumner 21/06/2012 Moderate M Low
77 30/09/2011 PST Non Clinical Risk
Electrical equipment / wiring becoming faulty resulting in electric shock or fire.
Building inspections occur on a quarterly basis. All electrical equipment is PAT tested before first use and on a regular basis. Cables are arranged along walls, not across rooms.
Compliance Risk
Ann Sumner 28/09/2012 Low M Low

ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
78 26/07/2011 PST Non Clinical Risk
Risk of insufficient fire arrangements in place The receptionist provides Nominated Incident Officer cover for the building but no longer works here full time
Fire training mandatory requirement. Fire alarms tested weekly. Signing in register available in reception for roll call in event of fire. Risk assesment completed by Sarah Meaney 26.7.11
Compliance Risk
Ann Sumner 26/01/2012 Moderate Moderate Low
79 30/09/2011 PST Non Clinical Risk
One of the offices currently used by PST does not have any ventilation, no outside windows, no air conditioning, this can result in staff working in that room having headaches and feeling fatigue.
Door left open when room in use. Manager looking into possibility of changing rooms with the Health Visitors, who only use their room on an occasional basis.
Operational Risk
Ann Sumner 28/09/2012 Low M Low
75 09/09/2011 PST Non Clinical Risk
Printer toner may cause ill health if ingested in quantity, may cause eye irritation. Skin irritation and dermatitis may result from prolonged contact.
COSHH poster on display next to the printer which lists first aid proceedure. Disposable gloves provided
Compliance Risk
Ann Sumner 01/12/2011 Low Low Low
76 23/03/2011 PST Non Clinical Risk
Risk of eye strain, soreness to the neck or wrist , backache or headache/fatigue
Workstations and adjustable chairs available. Windows have blinds which stop glare to display screen. All staff have been instructed to familiarise themselves with the DSE policy and to complete a VDU assessment form on line and submit to the R&SM team. Staff know that they should take breaks away from the display screen, to do other tasks and that eye tests are available from occupational health
Compliance Risk
Ann Sumner 22/03/2012 Moderate Low Low
107 16/04/2012 SHA Ambitions : Ambition 2
Significantly improving quality & safety in Primary Care : To create a culture of improvement within Primary Medical Care with a particular focus on quality & patient safety.
* Baseline prescribing data is currently being produced from sept 2011 (SHA) * A short survey will establish the baseline by CCG by April 2012 * The most recent GP Survey data (Dec 2011) will form the baseline. Results will be bi‐annual
Strategic Risk David Birch 02/07/2012 Moderate Moderate Low
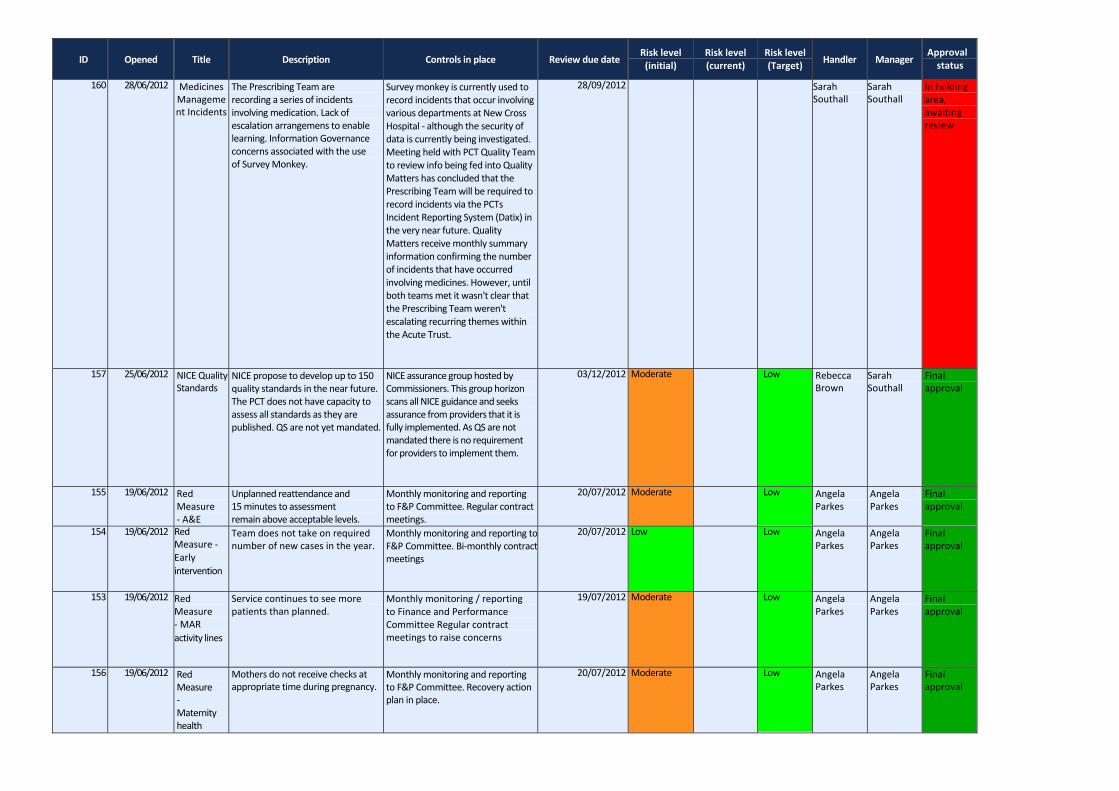
Specialty: Performance Management 155 19/06/2012 Red Measure
‐ A&E Unplanned reattendance and 15 minutes to assessment remain above acceptable levels.
Monthly monitoring and reporting to F&P Committee. Regular contract meetings.
Strategic Risk Angela Parkes
20/07/2012 Moderate M Low
154 19/06/2012 Red Measure ‐ Early intervention
Team does not take on required number of new cases in the year.
Monthly monitoring and reporting to F&P Committee.Bi‐ monthly contract meetings
Strategic Risk Angela Parkes
20/07/2012 Low M Low
153 19/06/2012 Red Measure ‐ MAR activity lines
Service continues to see more patients than planned.
Monthly monitoring / reporting to Finance and Performance Committee Regular contract meetings to raise concerns
Strategic Risk Angela Parkes
19/07/2012 Moderate M Low
156 19/06/2012 Red Measure ‐ Maternity health checks
Mothers do not receive checks at appropriate time during pregnancy.
Monthly monitoring and reporting to F&P Committee. Recovery action plan in place.
Strategic Risk Angela Parkes
20/07/2012 Moderate M Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
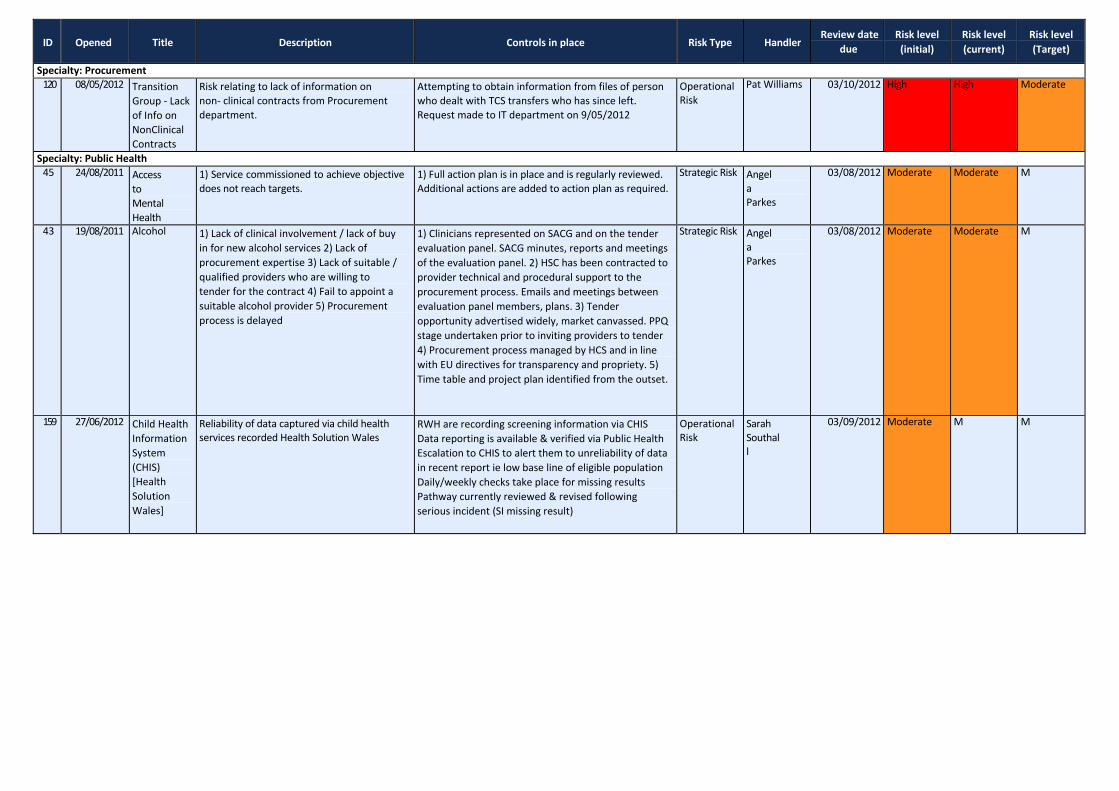
Specialty: Procurement 120 08/05/2012 Transition
Group ‐ Lack of Info on NonClinical Contracts
Risk relating to lack of information on non‐ clinical contracts from Procurement department.
Attempting to obtain information from files of person who dealt with TCS transfers who has since left. Request made to IT department on 9/05/2012
Operational Risk
Pat Williams 03/10/2012 High High Moderate
Specialty: Public Health 45 24/08/2011 Access
to Mental Health
1) Service commissioned to achieve objective does not reach targets.
1) Full action plan is in place and is regularly reviewed. Additional actions are added to action plan as required.
Strategic Risk Angela Parkes
03/08/2012 Moderate Moderate M
43 19/08/2011 Alcohol 1) Lack of clinical involvement / lack of buy in for new alcohol services 2) Lack of procurement expertise 3) Lack of suitable / qualified providers who are willing to tender for the contract 4) Fail to appoint a suitable alcohol provider 5) Procurement process is delayed
1) Clinicians represented on SACG and on the tender evaluation panel. SACG minutes, reports and meetings of the evaluation panel. 2) HSC has been contracted to provider technical and procedural support to the procurement process. Emails and meetings between evaluation panel members, plans. 3) Tender opportunity advertised widely, market canvassed. PPQ stage undertaken prior to inviting providers to tender 4) Procurement process managed by HCS and in line with EU directives for transparency and propriety. 5) Time table and project plan identified from the outset.
Strategic Risk Angela Parkes
03/08/2012 Moderate Moderate M
159 27/06/2012 Child Health Information System (CHIS) [Health Solution Wales]
Reliability of data captured via child health services recorded Health Solution Wales
RWH are recording screening information via CHIS Data reporting is available & verified via Public Health Escalation to CHIS to alert them to unreliability of data in recent report ie low base line of eligible population Daily/weekly checks take place for missing results Pathway currently reviewed & revised following serious incident (SI missing result)
Operational Risk
Sarah Southall
03/09/2012 Moderate M M
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
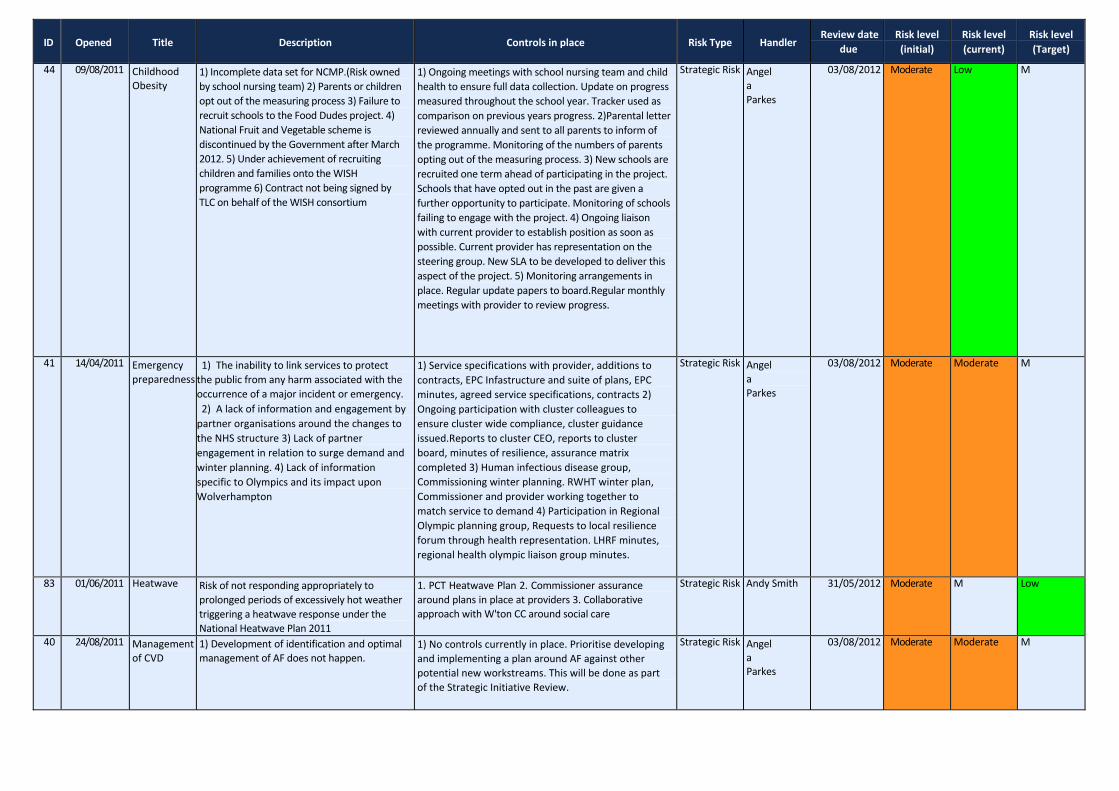
44 09/08/2011 Childhood Obesity
1) Incomplete data set for NCMP.(Risk owned by school nursing team) 2) Parents or children opt out of the measuring process 3) Failure to recruit schools to the Food Dudes project. 4) National Fruit and Vegetable scheme is discontinued by the Government after March 2012. 5) Under achievement of recruiting children and families onto the WISH programme 6) Contract not being signed by TLC on behalf of the WISH consortium
1) Ongoing meetings with school nursing team and child health to ensure full data collection. Update on progress measured throughout the school year. Tracker used as comparison on previous years progress. 2)Parental letter reviewed annually and sent to all parents to inform of the programme. Monitoring of the numbers of parents opting out of the measuring process. 3) New schools are recruited one term ahead of participating in the project. Schools that have opted out in the past are given a further opportunity to participate. Monitoring of schools failing to engage with the project. 4) Ongoing liaison with current provider to establish position as soon as possible. Current provider has representation on the steering group. New SLA to be developed to deliver this aspect of the project. 5) Monitoring arrangements in place. Regular update papers to board.Regular monthly meetings with provider to review progress.
Strategic Risk Angela Parkes
03/08/2012 Moderate Low M
41 14/04/2011 Emergency preparedness
1) The inability to link services to protect the public from any harm associated with the occurrence of a major incident or emergency. 2) A lack of information and engagement by partner organisations around the changes to the NHS structure 3) Lack of partner engagement in relation to surge demand and winter planning. 4) Lack of information specific to Olympics and its impact upon Wolverhampton
1) Service specifications with provider, additions to contracts, EPC Infastructure and suite of plans, EPC minutes, agreed service specifications, contracts 2) Ongoing participation with cluster colleagues to ensure cluster wide compliance, cluster guidance issued.Reports to cluster CEO, reports to cluster board, minutes of resilience, assurance matrix completed 3) Human infectious disease group, Commissioning winter planning. RWHT winter plan, Commissioner and provider working together to match service to demand 4) Participation in Regional Olympic planning group, Requests to local resilience forum through health representation. LHRF minutes, regional health olympic liaison group minutes.
Strategic Risk Angela Parkes
03/08/2012 Moderate Moderate M
83 01/06/2011 Heatwave Risk of not responding appropriately to prolonged periods of excessively hot weather triggering a heatwave response under the National Heatwave Plan 2011
1. PCT Heatwave Plan 2. Commissioner assurance around plans in place at providers 3. Collaborative approach with W'ton CC around social care
Strategic Risk Andy Smith 31/05/2012 Moderate M Low
40 24/08/2011 Management of CVD
1) Development of identification and optimal management of AF does not happen.
1) No controls currently in place. Prioritise developing and implementing a plan around AF against other potential new workstreams. This will be done as part of the Strategic Initiative Review.
Strategic Risk Angela Parkes
03/08/2012 Moderate Moderate M
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
128 17/05/2012 Public Health : Financial Impact of Transition
Flu Campaign Immunisation Uptake Immunisation & Screening Locally Enhanced Services (LES's) Public Health LES's
Flu Campaign : Currently fund promotional work via non recurring PCT funds (in addition to DES) Immunisation & Screening : Cluster approach to resolve who & how. Networks already considering new ways of working to improve uptake & provision. LES's : approached RWH to host funding on Public Health behalf however requires further discussion with contracts team & CCG due to implications for monitoring via them.
Financial Risk Ros Jervis 03/09/2012 Moderate M M
150 31/05/2012 Robustness of pathways commmission ed between Public Health and CCG
Public Health has taken responsibility for commissioning some services that will be under the remit of CCGs e.g. CVD. POLCV, input into Mental Health, Falls Prevention. Pathways include service commissioned by Public Health and CCG and NHSCB and need to be coherent e.g. Healthy Lifestyles through the Disease Management (Diabetes, CHD, Stroke) and Mental Wellbeing through to Mental Health care and Alcohol Treatment Service through to In‐patient care. Preventative work is effectively done through RWHT and BCPFT. This is often implemented via CQUINs. Ways for Public Health to influence CQUIN selection is needed.
Health and Wellbeing Board brings the commissioners together i.e. Local Authority, Public Health and CCG Comprehensive core offer being developed to formalise the good relations between Public Health and CCG
Strategic Risk Lucy Heath Moderate M M
149 31/05/2012 Role of Public Health in NHSCB/CCG commissione d services
Immunisation and screening will be commissioned by NHSCB. Historically, local response has been neccessary to ensure appropriate governance, performance management (e.g. poor uptake), quality and serious incidents. It is unlikely that a national approach will be able to fully address these issues.
District immunisation committee (and task and finish groups for specific workstreams). Clear governance around screening. Need to ensure these are maintained within the new structure and input from NHSCB and PHE happens.
Operational Risk
Ros Jervis Moderate M M
Specialty: Quality & Risk Team 87 30/08/2011 Assurance
Framework Board Assurance Framework has been adopted from that developed at Cluster Level Within the PCT the Local Assurance Framework is made up of a series of objectives:‐ 1=Financial Balance 2=QIPP 3=Statutory Responsibilities 4=Strategic Intentions 5=Quality & Patient Safety
Each of the above areas have basic assessments in place Monitoring at Cluster, Board & Q&SC Committee level All red risks currently on the PCT Risk Register are mapped to the relevant BAF Priority & the respective objective contained within the BAF Audit & Governance Comm intermitently receive assurance from HofS & reflective in annual SIC.
Strategic Risk Rebecca Brown
29/09/2012 Moderate M Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
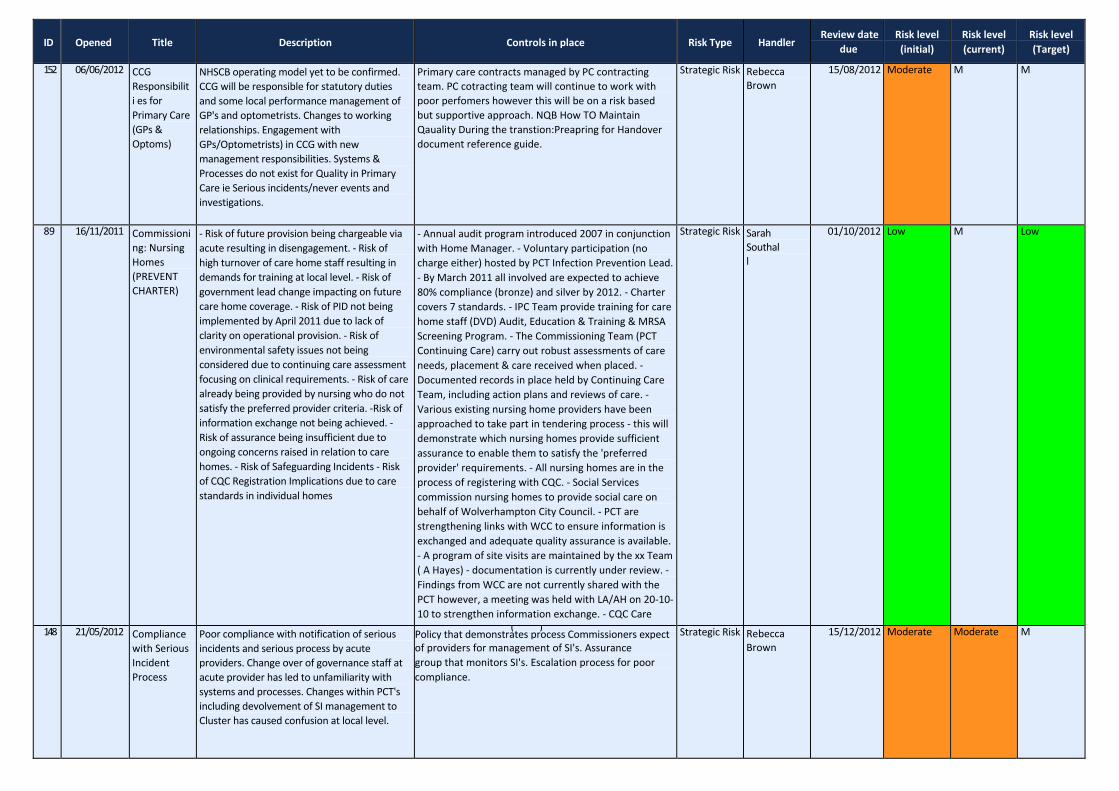
152 06/06/2012 CCG Responsibiliti es for Primary Care (GPs & Optoms)
NHSCB operating model yet to be confirmed. CCG will be responsible for statutory duties and some local performance management of GP's and optometrists. Changes to working relationships. Engagement with GPs/Optometrists) in CCG with new management responsibilities. Systems & Processes do not exist for Quality in Primary Care ie Serious incidents/never events and investigations.
Primary care contracts managed by PC contracting team. PC cotracting team will continue to work with poor perfomers however this will be on a risk based but supportive approach. NQB How TO Maintain Qauality During the transtion:Preapring for Handover document reference guide.
Strategic Risk Rebecca Brown
15/08/2012 Moderate M M
89 16/11/2011 Commissioni ng: Nursing Homes (PREVENT CHARTER)
‐ Risk of future provision being chargeable via acute resulting in disengagement. ‐ Risk of high turnover of care home staff resulting in demands for training at local level. ‐ Risk of government lead change impacting on future care home coverage. ‐ Risk of PID not being implemented by April 2011 due to lack of clarity on operational provision. ‐ Risk of environmental safety issues not being considered due to continuing care assessment focusing on clinical requirements. ‐ Risk of care already being provided by nursing who do not satisfy the preferred provider criteria. ‐Risk of information exchange not being achieved. ‐ Risk of assurance being insufficient due to ongoing concerns raised in relation to care homes. ‐ Risk of Safeguarding Incidents ‐ Risk of CQC Registration Implications due to care standards in individual homes
‐ Annual audit program introduced 2007 in conjunction with Home Manager. ‐ Voluntary participation (no charge either) hosted by PCT Infection Prevention Lead. ‐ By March 2011 all involved are expected to achieve 80% compliance (bronze) and silver by 2012. ‐ Charter covers 7 standards. ‐ IPC Team provide training for care home staff (DVD) Audit, Education & Training & MRSA Screening Program. ‐ The Commissioning Team (PCT Continuing Care) carry out robust assessments of care needs, placement & care received when placed. ‐ Documented records in place held by Continuing Care Team, including action plans and reviews of care. ‐ Various existing nursing home providers have been approached to take part in tendering process ‐ this will demonstrate which nursing homes provide sufficient assurance to enable them to satisfy the 'preferred provider' requirements. ‐ All nursing homes are in the process of registering with CQC. ‐ Social Services commission nursing homes to provide social care on behalf of Wolverhampton City Council. ‐ PCT are strengthening links with WCC to ensure information is exchanged and adequate quality assurance is available. ‐ A program of site visits are maintained by the xx Team ( A Hayes) ‐ documentation is currently under review. ‐ Findings from WCC are not currently shared with the PCT however, a meeting was held with LA/AH on 20‐10‐ 10 to strengthen information exchange. ‐ CQC Care
Strategic Risk Sarah Southall
01/10/2012 Low M Low
148 21/05/2012 Compliance with Serious Incident Process
Poor compliance with notification of serious incidents and serious process by acute providers. Change over of governance staff at acute provider has led to unfamiliarity with systems and processes. Changes within PCT's including devolvement of SI management to Cluster has caused confusion at local level.
( )Policy that demonstrates process Commissioners expect of providers for management of SI's. Assurance group that monitors SI's. Escalation process for poor compliance.
Strategic Risk Rebecca Brown
15/12/2012 Moderate Moderate M
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
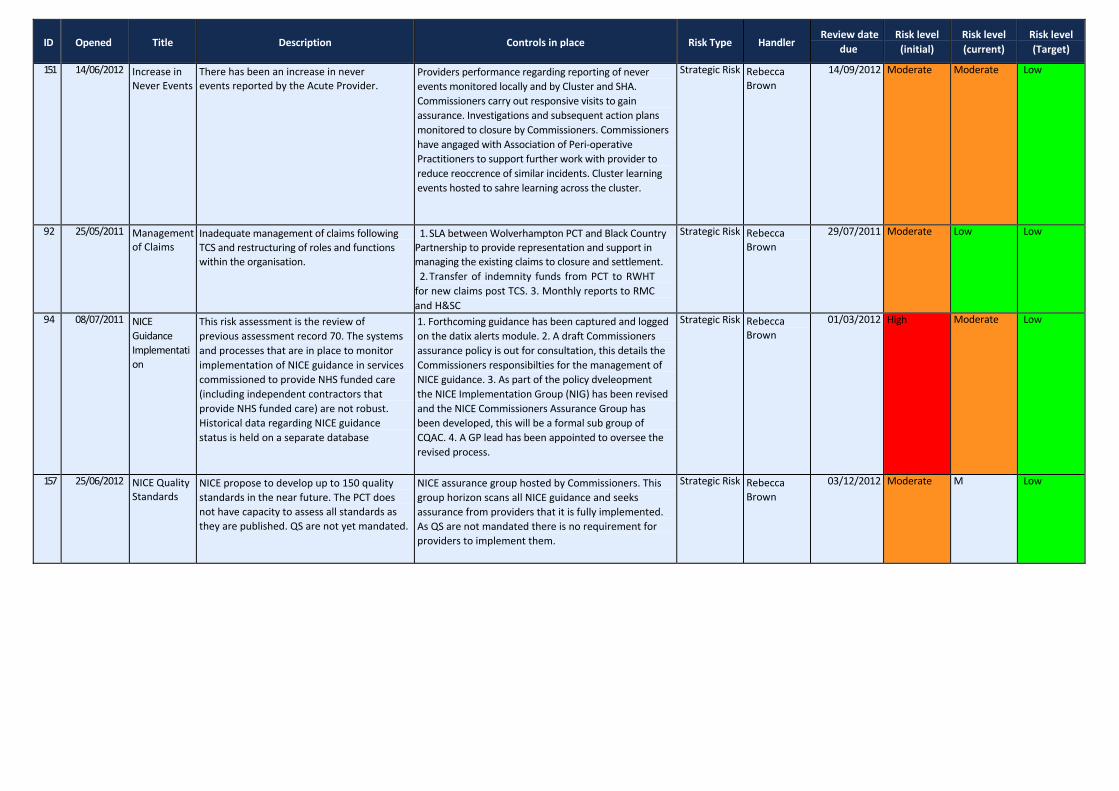
151 14/06/2012 Increase in Never Events
There has been an increase in never events reported by the Acute Provider.
Providers performance regarding reporting of never events monitored locally and by Cluster and SHA. Commissioners carry out responsive visits to gain assurance. Investigations and subsequent action plans monitored to closure by Commissioners. Commissioners have angaged with Association of Peri‐operative Practitioners to support further work with provider to reduce reoccrence of similar incidents. Cluster learning events hosted to sahre learning across the cluster.
Strategic Risk Rebecca Brown
14/09/2012 Moderate Moderate Low
92 25/05/2011 Management of Claims
Inadequate management of claims following TCS and restructuring of roles and functions within the organisation.
1. SLA between Wolverhampton PCT and Black Country Partnership to provide representation and support in managing the existing claims to closure and settlement. 2. Transfer of indemnity funds from PCT to RWHT for new claims post TCS. 3. Monthly reports to RMC and H&SC
Strategic Risk Rebecca Brown
29/07/2011 Moderate Low Low
94 08/07/2011 NICE Guidance Implementati on
This risk assessment is the review of previous assessment record 70. The systems and processes that are in place to monitor implementation of NICE guidance in services commissioned to provide NHS funded care (including independent contractors that provide NHS funded care) are not robust. Historical data regarding NICE guidance status is held on a separate database
1. Forthcoming guidance has been captured and logged on the datix alerts module. 2. A draft Commissioners assurance policy is out for consultation, this details the Commissioners responsibilties for the management of NICE guidance. 3. As part of the policy dveleopment the NICE Implementation Group (NIG) has been revised and the NICE Commissioners Assurance Group has been developed, this will be a formal sub group of CQAC. 4. A GP lead has been appointed to oversee the revised process.
Strategic Risk Rebecca Brown
01/03/2012 High Moderate Low
157 25/06/2012 NICE Quality Standards
NICE propose to develop up to 150 quality standards in the near future. The PCT does not have capacity to assess all standards as they are published. QS are not yet mandated.
NICE assurance group hosted by Commissioners. This group horizon scans all NICE guidance and seeks assurance from providers that it is fully implemented. As QS are not mandated there is no requirement for providers to implement them.
Strategic Risk Rebecca Brown
03/12/2012 Moderate M Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
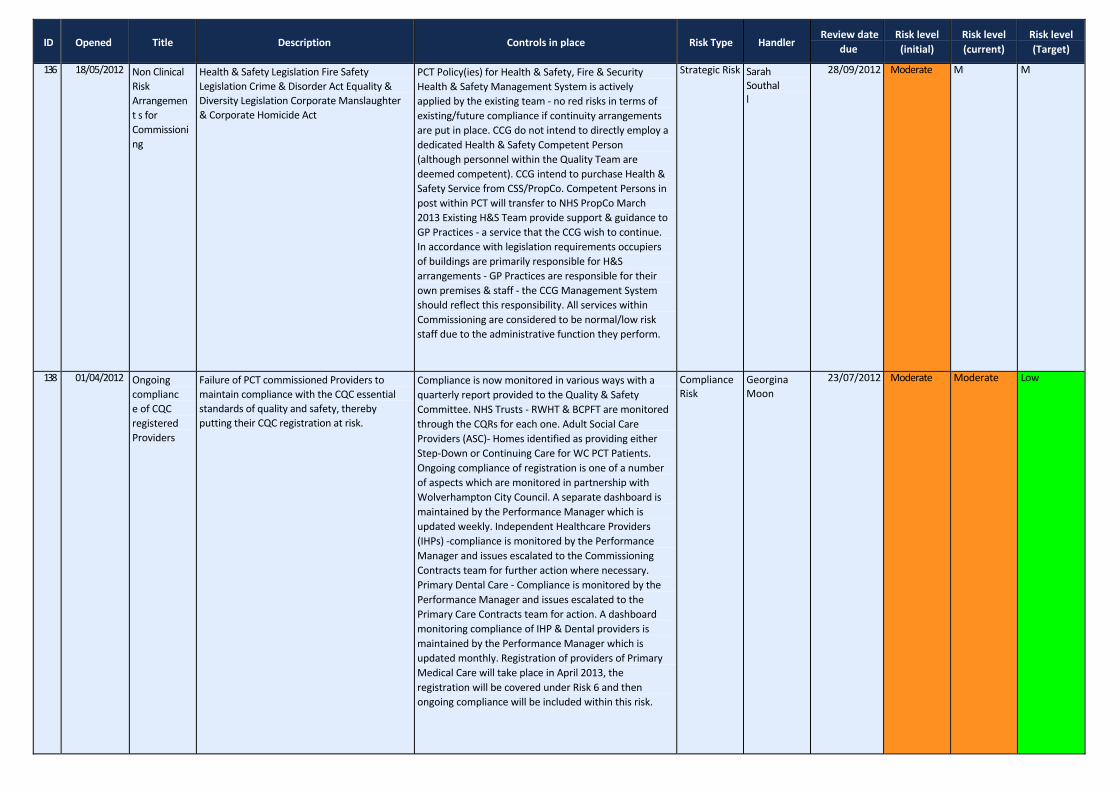
136 18/05/2012 Non Clinical Risk Arrangement s for Commissioni ng
Health & Safety Legislation Fire Safety Legislation Crime & Disorder Act Equality & Diversity Legislation Corporate Manslaughter & Corporate Homicide Act
PCT Policy(ies) for Health & Safety, Fire & Security Health & Safety Management System is actively applied by the existing team ‐ no red risks in terms of existing/future compliance if continuity arrangements are put in place. CCG do not intend to directly employ a dedicated Health & Safety Competent Person (although personnel within the Quality Team are deemed competent). CCG intend to purchase Health & Safety Service from CSS/PropCo. Competent Persons in post within PCT will transfer to NHS PropCo March 2013 Existing H&S Team provide support & guidance to GP Practices ‐ a service that the CCG wish to continue. In accordance with legislation requirements occupiers of buildings are primarily responsible for H&S arrangements ‐ GP Practices are responsible for their own premises & staff ‐ the CCG Management System should reflect this responsibility. All services within Commissioning are considered to be normal/low risk staff due to the administrative function they perform.
Strategic Risk Sarah Southall
28/09/2012 Moderate M M
138 01/04/2012 Ongoing compliance of CQC registered Providers
Failure of PCT commissioned Providers to maintain compliance with the CQC essential standards of quality and safety, thereby putting their CQC registration at risk.
Compliance is now monitored in various ways with a quarterly report provided to the Quality & Safety Committee. NHS Trusts ‐ RWHT & BCPFT are monitored through the CQRs for each one. Adult Social Care Providers (ASC)‐ Homes identified as providing either Step‐Down or Continuing Care for WC PCT Patients. Ongoing compliance of registration is one of a number of aspects which are monitored in partnership with Wolverhampton City Council. A separate dashboard is maintained by the Performance Manager which is updated weekly. Independent Healthcare Providers (IHPs) ‐compliance is monitored by the Performance Manager and issues escalated to the Commissioning Contracts team for further action where necessary. Primary Dental Care ‐ Compliance is monitored by the Performance Manager and issues escalated to the Primary Care Contracts team for action. A dashboard monitoring compliance of IHP & Dental providers is maintained by the Performance Manager which is updated monthly. Registration of providers of Primary Medical Care will take place in April 2013, the registration will be covered under Risk 6 and then ongoing compliance will be included within this risk.
Compliance Risk
Georgina Moon
23/07/2012 Moderate Moderate Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
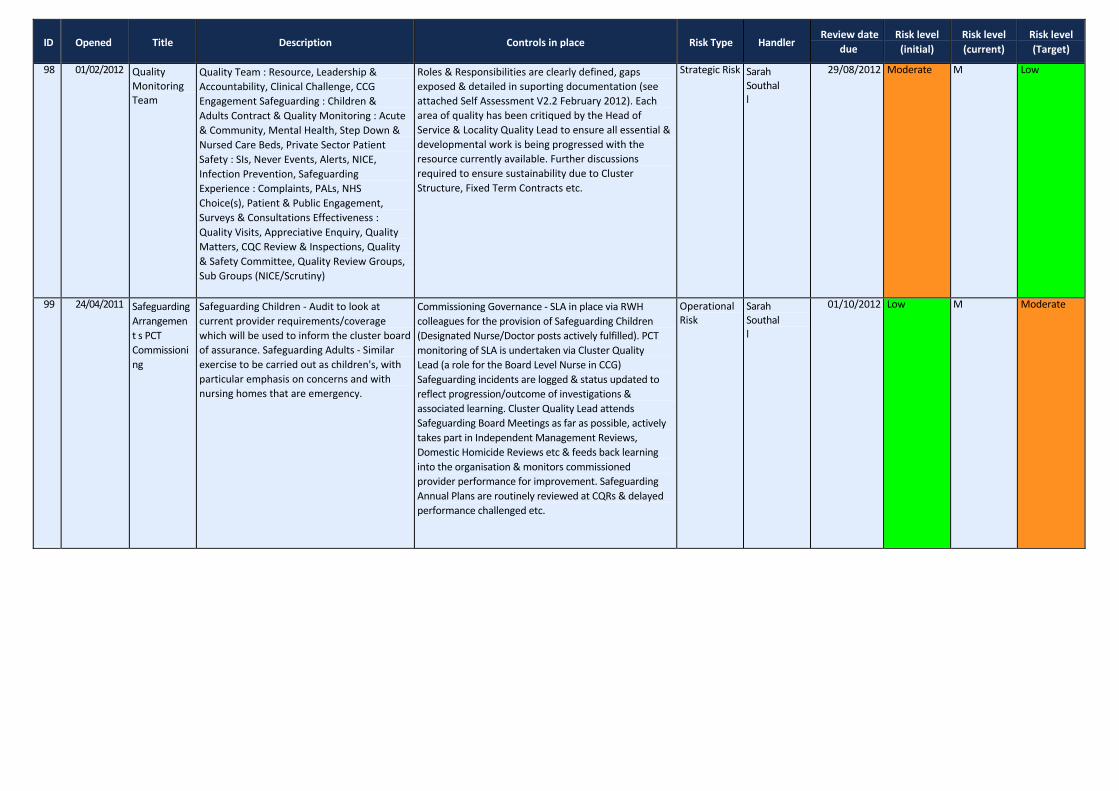
98 01/02/2012 Quality Monitoring Team
Quality Team : Resource, Leadership & Accountability, Clinical Challenge, CCG Engagement Safeguarding : Children & Adults Contract & Quality Monitoring : Acute & Community, Mental Health, Step Down & Nursed Care Beds, Private Sector Patient Safety : SIs, Never Events, Alerts, NICE, Infection Prevention, Safeguarding Experience : Complaints, PALs, NHS Choice(s), Patient & Public Engagement, Surveys & Consultations Effectiveness : Quality Visits, Appreciative Enquiry, Quality Matters, CQC Review & Inspections, Quality & Safety Committee, Quality Review Groups, Sub Groups (NICE/Scrutiny)
Roles & Responsibilities are clearly defined, gaps exposed & detailed in suporting documentation (see attached Self Assessment V2.2 February 2012). Each area of quality has been critiqued by the Head of Service & Locality Quality Lead to ensure all essential & developmental work is being progressed with the resource currently available. Further discussions required to ensure sustainability due to Cluster Structure, Fixed Term Contracts etc.
Strategic Risk Sarah Southall
29/08/2012 Moderate M Low
99 24/04/2011 Safeguarding Arrangement s PCT Commissioni ng
Safeguarding Children ‐ Audit to look at current provider requirements/coverage which will be used to inform the cluster board of assurance. Safeguarding Adults ‐ Similar exercise to be carried out as children's, with particular emphasis on concerns and with nursing homes that are emergency.
Commissioning Governance ‐ SLA in place via RWH colleagues for the provision of Safeguarding Children (Designated Nurse/Doctor posts actively fulfilled). PCT monitoring of SLA is undertaken via Cluster Quality Lead (a role for the Board Level Nurse in CCG) Safeguarding incidents are logged & status updated to reflect progression/outcome of investigations & associated learning. Cluster Quality Lead attends Safeguarding Board Meetings as far as possible, actively takes part in Independent Management Reviews, Domestic Homicide Reviews etc & feeds back learning into the organisation & monitors commissioned provider performance for improvement. Safeguarding Annual Plans are routinely reviewed at CQRs & delayed performance challenged etc.
Operational Risk
Sarah Southall
01/10/2012 Low M Moderate
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
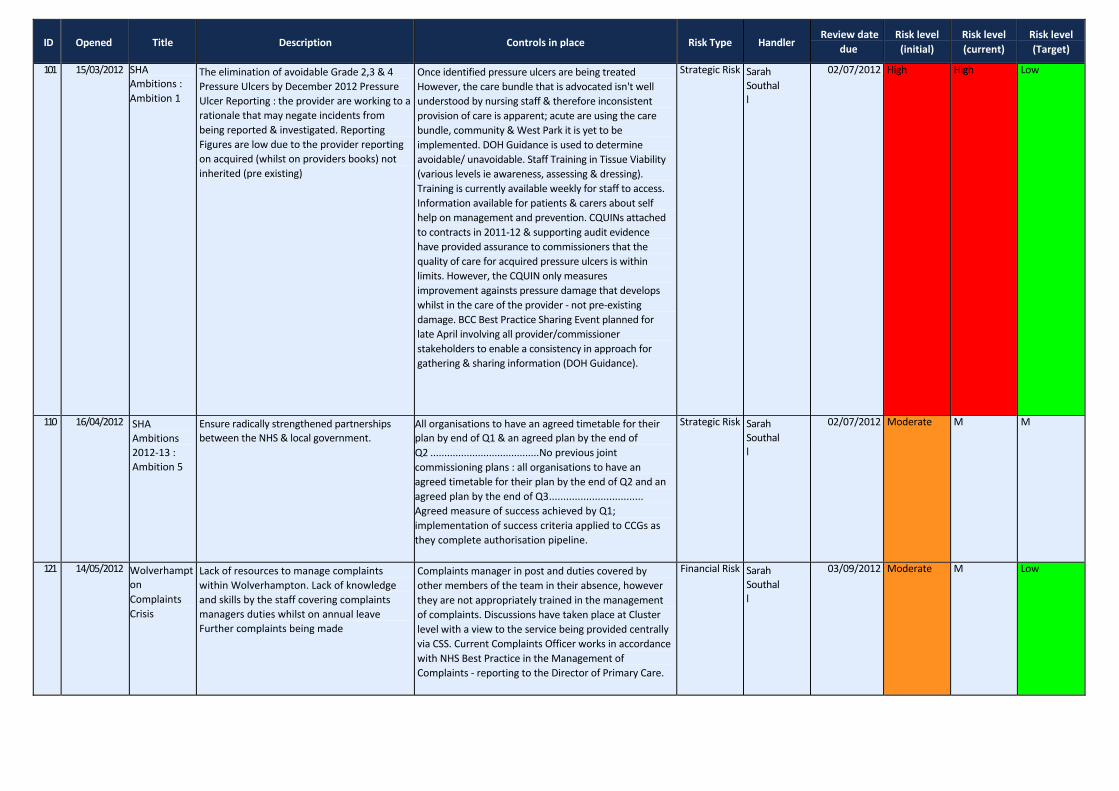
101 15/03/2012 SHA Ambitions : Ambition 1
The elimination of avoidable Grade 2,3 & 4 Pressure Ulcers by December 2012 Pressure Ulcer Reporting : the provider are working to a rationale that may negate incidents from being reported & investigated. Reporting Figures are low due to the provider reporting on acquired (whilst on providers books) not inherited (pre existing)
Once identified pressure ulcers are being treated However, the care bundle that is advocated isn't well understood by nursing staff & therefore inconsistent provision of care is apparent; acute are using the care bundle, community & West Park it is yet to be implemented. DOH Guidance is used to determine avoidable/ unavoidable. Staff Training in Tissue Viability (various levels ie awareness, assessing & dressing). Training is currently available weekly for staff to access. Information available for patients & carers about self help on management and prevention. CQUINs attached to contracts in 2011‐12 & supporting audit evidence have provided assurance to commissioners that the quality of care for acquired pressure ulcers is within limits. However, the CQUIN only measures improvement againsts pressure damage that develops whilst in the care of the provider ‐ not pre‐existing damage. BCC Best Practice Sharing Event planned for late April involving all provider/commissioner stakeholders to enable a consistency in approach for gathering & sharing information (DOH Guidance).
Strategic Risk Sarah Southall
02/07/2012 High High Low
110 16/04/2012 SHA Ambitions 2012‐13 : Ambition 5
Ensure radically strengthened partnerships between the NHS & local government.
All organisations to have an agreed timetable for their plan by end of Q1 & an agreed plan by the end of Q2 .......................................No previous joint commissioning plans : all organisations to have an agreed timetable for their plan by the end of Q2 and an agreed plan by the end of Q3................................. Agreed measure of success achieved by Q1; implementation of success criteria applied to CCGs as they complete authorisation pipeline.
Strategic Risk Sarah Southall
02/07/2012 Moderate M M
121 14/05/2012 Wolverhampt on Complaints Crisis
Lack of resources to manage complaints within Wolverhampton. Lack of knowledge and skills by the staff covering complaints managers duties whilst on annual leave Further complaints being made
Complaints manager in post and duties covered by other members of the team in their absence, however they are not appropriately trained in the management of complaints. Discussions have taken place at Cluster level with a view to the service being provided centrally via CSS. Current Complaints Officer works in accordance with NHS Best Practice in the Management of Complaints ‐ reporting to the Director of Primary Care.
Financial Risk Sarah Southall
03/09/2012 Moderate M Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
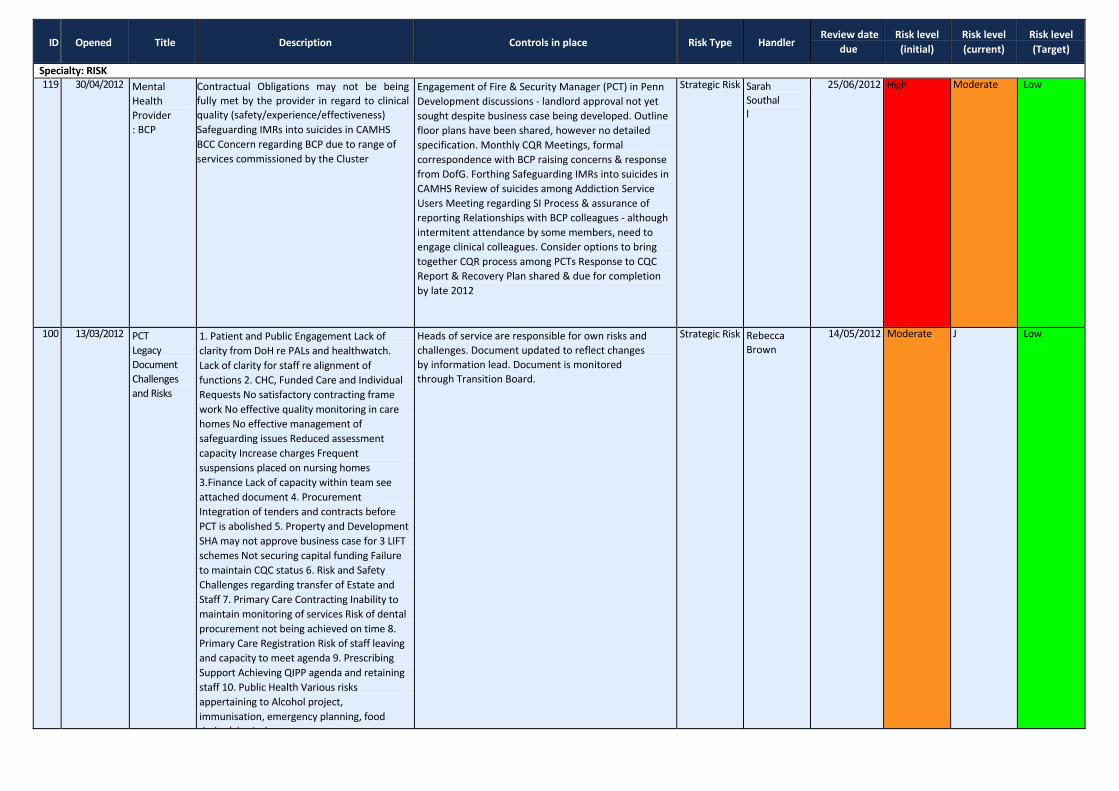
Specialty: RISK 119 30/04/2012 Mental
Health Provider : BCP
Contractual Obligations may not be being fully met by the provider in regard to clinical quality (safety/experience/effectiveness) Safeguarding IMRs into suicides in CAMHS BCC Concern regarding BCP due to range of services commissioned by the Cluster
Engagement of Fire & Security Manager (PCT) in Penn Development discussions ‐ landlord approval not yet sought despite business case being developed. Outline floor plans have been shared, however no detailed specification. Monthly CQR Meetings, formal correspondence with BCP raising concerns & response from DofG. Forthing Safeguarding IMRs into suicides in CAMHS Review of suicides among Addiction Service Users Meeting regarding SI Process & assurance of reporting Relationships with BCP colleagues ‐ although intermitent attendance by some members, need to engage clinical colleagues. Consider options to bring together CQR process among PCTs Response to CQC Report & Recovery Plan shared & due for completion by late 2012
Strategic Risk Sarah Southall
25/06/2012 High Moderate Low
100 13/03/2012 PCT Legacy Document Challenges and Risks
1. Patient and Public Engagement Lack of clarity from DoH re PALs and healthwatch. Lack of clarity for staff re alignment of functions 2. CHC, Funded Care and Individual Requests No satisfactory contracting frame work No effective quality monitoring in care homes No effective management of safeguarding issues Reduced assessment capacity Increase charges Frequent suspensions placed on nursing homes 3.Finance Lack of capacity within team see attached document 4. Procurement Integration of tenders and contracts before PCT is abolished 5. Property and Development SHA may not approve business case for 3 LIFT schemes Not securing capital funding Failure to maintain CQC status 6. Risk and Safety Challenges regarding transfer of Estate and Staff 7. Primary Care Contracting Inability to maintain monitoring of services Risk of dental procurement not being achieved on time 8. Primary Care Registration Risk of staff leaving and capacity to meet agenda 9. Prescribing Support Achieving QIPP agenda and retaining staff 10. Public Health Various risks appertaining to Alcohol project, immunisation, emergency planning, food d d / h i l
Heads of service are responsible for own risks and challenges. Document updated to reflect changes by information lead. Document is monitored through Transition Board.
Strategic Risk Rebecca Brown
14/05/2012 Moderate J Low
ID Opened Title Description Controls in place Risk Type Handler Review date
due Risk level (initial)
Risk level (current)
Risk level (Target)
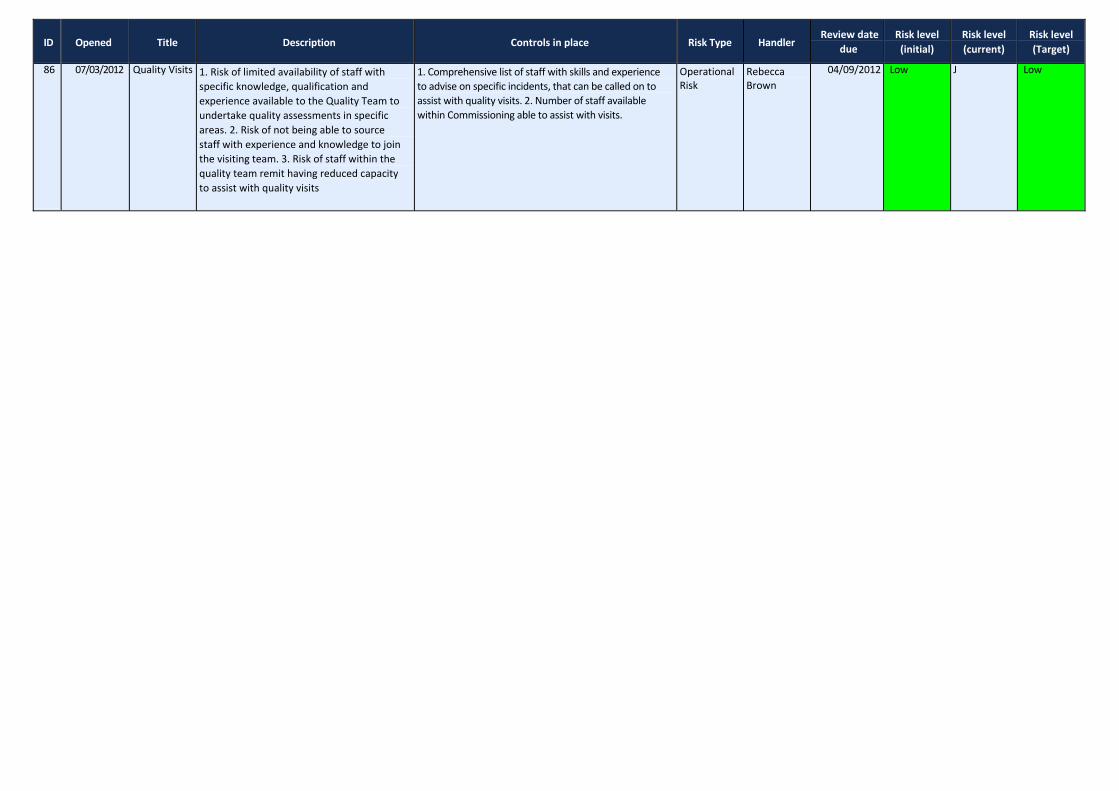
86 07/03/2012 Quality Visits 1. Risk of limited availability of staff with specific knowledge, qualification and experience available to the Quality Team to undertake quality assessments in specific areas. 2. Risk of not being able to source staff with experience and knowledge to join the visiting team. 3. Risk of staff within the quality team remit having reduced capacity to assist with quality visits
1. Comprehensive list of staff with skills and experience to advise on specific incidents, that can be called on to assist with quality visits. 2. Number of staff available within Commissioning able to assist with visits.
Operational Risk
Rebecca Brown
04/09/2012 Low J Low
colleagues ‐ althoughintermitent attendance by some members, need to engage clinical colleagues. Consider options to bring together CQR process among PCTs Response to CQC Report & Recovery Plan shared & due for completion by
Red to Amber June 2012
Title Description Harm Controls in place Handler Review dateDate Review Completed Risk Review
Risk level (current)
Next Review Date
Risk level (Target)
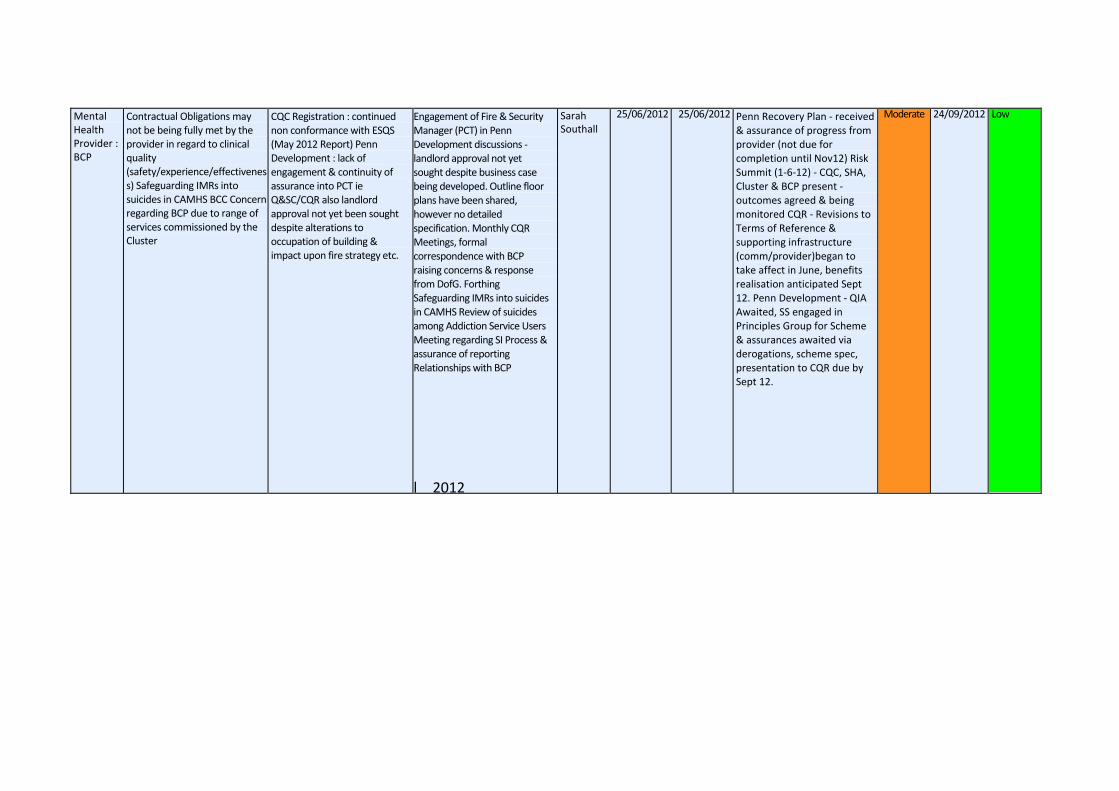
Mental Health Provider : BCP
Contractual Obligations may not be being fully met by the provider in regard to clinical quality (safety/experience/effectivenes s) Safeguarding IMRs into suicides in CAMHS BCC Concern regarding BCP due to range of services commissioned by the Cluster
CQC Registration : continued non conformance with ESQS (May 2012 Report) Penn Development : lack of engagement & continuity of assurance into PCT ie Q&SC/CQR also landlord approval not yet been sought despite alterations to occupation of building & impact upon fire strategy etc.
Engagement of Fire & Security Manager (PCT) in Penn Development discussions ‐ landlord approval not yet sought despite business case being developed. Outline floor plans have been shared, however no detailed specification. Monthly CQR Meetings, formal correspondence with BCP raising concerns & response from DofG. Forthing Safeguarding IMRs into suicides in CAMHS Review of suicides among Addiction Service Users Meeting regarding SI Process & assurance of reporting Relationships with BCP
l 2012
Sarah Southall
25/06/2012 25/06/2012 Penn Recovery Plan ‐ received & assurance of progress from provider (not due for completion until Nov12) Risk Summit (1‐6‐12) ‐ CQC, SHA, Cluster & BCP present ‐ outcomes agreed & being monitored CQR ‐ Revisions to Terms of Reference & supporting infrastructure (comm/provider)began to take affect in June, benefits realisation anticipated Sept 12. Penn Development ‐ QIA Awaited, SS engaged in Principles Group for Scheme & assurances awaited via derogations, scheme spec, presentation to CQR due by Sept 12.
Moderate 24/09/2012 Low
New Risks Added to Register June 2012
ID Opened Title Description Controls in place Review due date Risk level (initial)
Risk level (current)
Risk level (Target) Handler Manager
Approval status
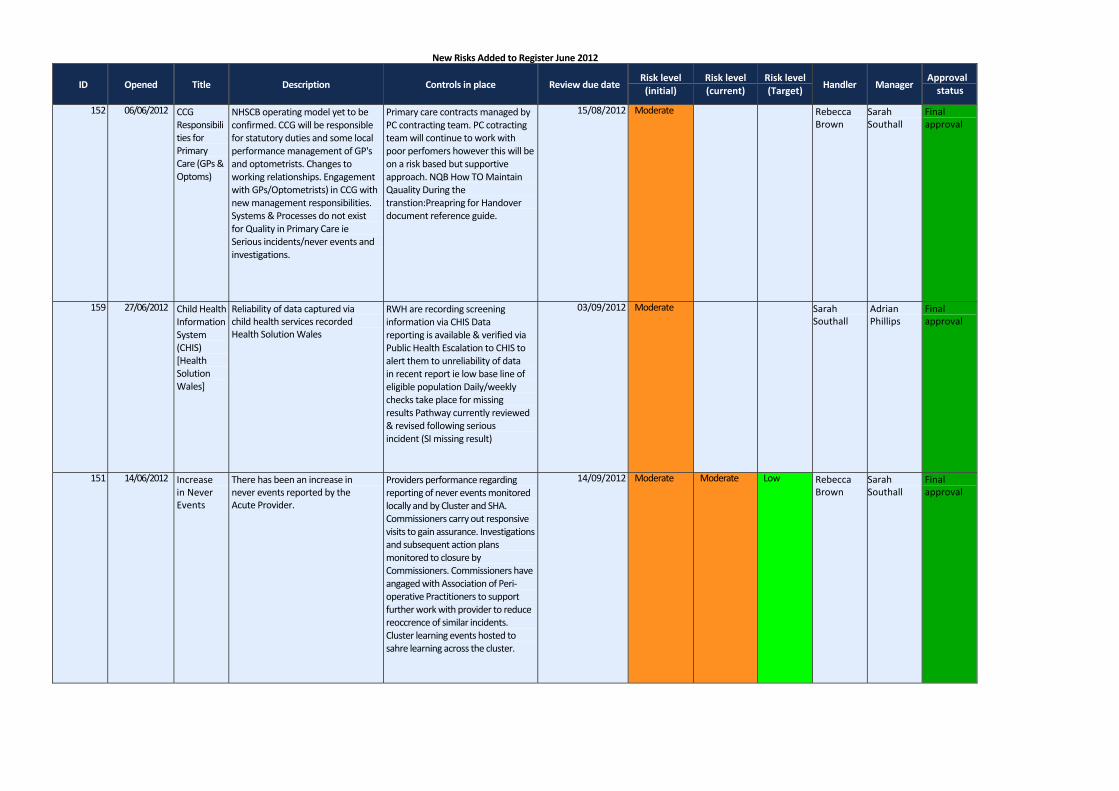
152 06/06/2012 CCG Responsibili ties for Primary Care (GPs & Optoms)
NHSCB operating model yet to be confirmed. CCG will be responsible for statutory duties and some local performance management of GP's and optometrists. Changes to working relationships. Engagement with GPs/Optometrists) in CCG with new management responsibilities. Systems & Processes do not exist for Quality in Primary Care ie Serious incidents/never events and investigations.
Primary care contracts managed by PC contracting team. PC cotracting team will continue to work with poor perfomers however this will be on a risk based but supportive approach. NQB How TO Maintain Qauality During the transtion:Preapring for Handover document reference guide.
15/08/2012 Moderate Rebecca Brown
Sarah Southall
Final approval
159 27/06/2012 Child Health Information System (CHIS) [Health Solution Wales]
Reliability of data captured via child health services recorded Health Solution Wales
RWH are recording screening information via CHIS Data reporting is available & verified via Public Health Escalation to CHIS to alert them to unreliability of data in recent report ie low base line of eligible population Daily/weekly checks take place for missing results Pathway currently reviewed & revised following serious incident (SI missing result)
03/09/2012 Moderate Sarah Southall
Adrian Phillips
Final approval
151 14/06/2012 Increase in Never Events
There has been an increase in never events reported by the Acute Provider.
Providers performance regarding reporting of never events monitored locally and by Cluster and SHA. Commissioners carry out responsive visits to gain assurance. Investigations and subsequent action plans monitored to closure by Commissioners. Commissioners have angaged with Association of Peri‐operative Practitioners to support further work with provider to reduce reoccrence of similar incidents. Cluster learning events hosted to sahre learning across the cluster.
14/09/2012 Moderate Moderate Low Rebecca Brown
Sarah Southall
Final approval
ID Opened Title Description Controls in place Review due date Risk level (initial)
Risk level (current)
Risk level (Target) Handler Manager
Approval status
160 28/06/2012 Medicines Manageme nt Incidents
The Prescribing Team are recording a series of incidents involving medication. Lack of escalation arrangemens to enable learning. Information Governance concerns associated with the use of Survey Monkey.
Survey monkey is currently used to record incidents that occur involving various departments at New Cross Hospital ‐ although the security of data is currently being investigated. Meeting held with PCT Quality Team to review info being fed into Quality Matters has concluded that the Prescribing Team will be required to record incidents via the PCTs Incident Reporting System (Datix) in the very near future. Quality Matters receive monthly summary information confirming the number of incidents that have occurred involving medicines. However, until both teams met it wasn't clear that the Prescribing Team weren't escalating recurring themes within the Acute Trust.
28/09/2012 Sarah Southall
Sarah Southall
In holding area, awaiting review
157 25/06/2012 NICE Quality Standards
NICE propose to develop up to 150 quality standards in the near future. The PCT does not have capacity to assess all standards as they are published. QS are not yet mandated.
NICE assurance group hosted by Commissioners. This group horizon scans all NICE guidance and seeks assurance from providers that it is fully implemented. As QS are not mandated there is no requirement for providers to implement them.
03/12/2012 Moderate Low Rebecca Brown
Sarah Southall
Final approval
155 19/06/2012 Red Measure ‐ A&E
Unplanned reattendance and 15 minutes to assessment remain above acceptable levels.
Monthly monitoring and reporting to F&P Committee. Regular contract meetings.
20/07/2012 Moderate Low Angela Parkes
Angela Parkes
Final approval
154 19/06/2012 Red Measure ‐ Early intervention
Team does not take on required number of new cases in the year.
Monthly monitoring and reporting to F&P Committee. Bi‐monthly contract meetings
20/07/2012 Low Low Angela Parkes
Angela Parkes
Final approval
153 19/06/2012 Red Measure ‐ MAR activity lines
Service continues to see more patients than planned.
Monthly monitoring / reporting to Finance and Performance Committee Regular contract meetings to raise concerns
19/07/2012 Moderate Low Angela Parkes
Angela Parkes
Final approval
156 19/06/2012 Red Measure ‐ Maternity health
Mothers do not receive checks at appropriate time during pregnancy.
Monthly monitoring and reporting to F&P Committee. Recovery action plan in place.
20/07/2012 Moderate Low Angela Parkes
Angela Parkes
Final approval
ID Opened Title Description Controls in place Review due date Risk level (initial)
Risk level (current)
Risk level (Target) Handler Manager
Approval status
161 28/06/2012 Safeguardin g Children
Named GP role has not been fulfilled for approx 6 months.
* Advert due to go out WC 2 July to enable recruitment to the role of Named GP * NAmed GP is likely to be in post by September 2012 (sessional rate) * Other safeguarding roles ie Board Nurse, Designated Nurse & Designated Doctor are in place and providing assurance to the PCT Q&SC * PCT Q&SC have been alerted to the role not being occupied & action being taken to resolve
28/09/2012 Sarah Southall
Sarah Southall
In holding area, awaiting review





























