Embed Size (px)
Citation preview

38 Work-Related Musculoskeletal Disorders:
Is There a Gender Differential, and if So, What Does It Mean ? L A U R A P U N N E T r * AND R O B IN H E R B E R T *
*Department of Work Environment, University of Massachusetts Lowell, Lowell, Massachusetts; *Department of Community and Preventive Medicine, Mount Sinai School of Medicine, New York, New York
I. Background
Musculoskeletal disorders (MSDs) include the many condi- tions that affect the muscles, tendons, ligaments, and joint car- tilage, as well as the anatomically associated peripheral motor and sensory nerves [1-5]. There is a strong and growing body of evidence associating a number of musculoskeletal disorders with workplace exposure to biomechanical and psychosocial factors [6,7]. Work-related musculoskeletal disorders (WMSDs) comprise a heterogeneous group of diagnoses that are often re- ferred to collectively as cumulative trauma disorder, repetitive strain i~ury, occupational cervicobrachial disorder, or overuse syndrome. Specific clinical syndromes that have been associ- ated with occupational exposure include nerve compression dis- orders (e.g., carpal tunnel syndrome), tendon inflammations and related conditions (e.g., tenosynovitis, epicondylitis, bursitis of the shoulder), disk disorders, and degenerative joint disease (Table 38.1). There are also a variety of less well-defined con- ditions such as myositis, fibromyalgia, focal dystonia, low back pain (LBP), and other regional pain syndromes. Musculoskele- tal disorders may affect any part of the body: the trunk, the upper extremities, and the lower extremities. WMSDs of the back and upper extremity appear to be more common than those affecting the lower extremity.
Some disorders, such as carpal tunnel syndrome (CTS) and lumbosacral disc herniation, have well-described clinical fea- tures, "gold standard" diagnostic tests, and relatively good con- sensus on diagnostic criteria [8,9]. However, many others, such as the specific tendonitides of the distal forearm, are not easily distinguished from one another in the clinical setting and do not have well agreed upon diagnostic criteria for use in research. Additionally, when grouped anatomically, many of these disor- ders have common epidemiologic features, particularly with re- spect to symptoms and, in working populations, the nature of the ergonomic exposure(s). For most MSDs, both onset and duration are more often chronic or subchronic than acute. Typi- cally, they tend to develop after months or years of overuse of the soft tissues, although muscle strains and tendon sprains may also occur as point-in-time injuries (meaning very soon after a sudden change in activity patterns). It has been observed that within a population occupationally exposed to particular ergon- omic stressors, several different types of clinical disorders may arise in different individuals. Thus, it has often been statistically efficient to study MSDs as a group.
Among the known or suspected nonoccupational risk factors for MSDs are age, gender, socioeconomic status, race or ethnic- ity (any of which might be confounded by occupational de-
Women and Health 474
mands), history of acute trauma, various systemic diseases (e.g., endocrine, neurologic, autoimmune, and collagen disorders), smoking, alcohol use, obesity, and recreational sports [5]. For CTS in particular, studies also have implicated factors affecting female hormone levels, such as use of oral contraceptives and surgical removal of both ovaries.
Accurate data on the incidence and prevalence of MSDs are sparse. There are no population registries of MSDs and not all people affected seek medical care, so most available data prob- ably underestimate the true magnitude of the disorders. Diffi- culties and inconsistencies in diagnosis compound this problem. However, it is clear that MSDs are widespread in many societies around the world and they account for much disability, pain, and suffering. In the United States, Canada, and Finland, for example, more people are disabled from working as a result of musculoskeletal disorders than from any other group of diseases [3,5,10,11]. It has been estimated that the direct and indirect economic burden of all musculoskeletal disease in the United States, including arthritis and repetitive trauma disorders, to- taled $149 billion in 1992 [12].
A. Work.Related Musculoskeletal Disorders
Work-related musculoskeletal disorders (WMSDs) are a sig- nificant world-wide public health problem, although official sta- tistics are difficult to compare across countries because of differences in record-keeping and case definitions. They are the single largest category of work-related illness in the United States, the Nordic countries, and Japan [3,6,13]. In the United States, workplace injuries and illnesses in the private sector, ex- cluding firms with fewer than 11 employees, are reported to the U.S. Bureau of Labor Statistics (BLS). Musculoskeletal disorders associated with "repeated trauma" in the workplace have ac- counted for over 50% of occupational illnesses since 1992, an- nually totaling over 300,000 cases [6,14]. Among the Nordic countries, reported WMSDs account for 71% of all occupational illness in Sweden but only 1% in Iceland [15]. These statistics do not include back disorders, which are defined as injuries. In 1994, about one-third of all injuries and illnesses resulting in lost work days reported to the U.S. BLS were associated with overexertion or repetitive motion, and nearly one-half affected the back [6]. Two studies of carpal tunnel syndrome suggested that about one-half of the cases occurring in the general population were work-related [16,17]. The US National Institute of Occupational Safety and Health (NIOSH) has identified musculoskeletal dis- orders of the upper extremities as a national research priority.
Copyright �9 2000 by Academic Press. All rights of reproduction in any form reserved.

C H A P T E R 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 475
Table 38.1
Common Musculoskeletal Disorders Associated with Occupational Exposure to Ergonomic Stressors
Neck and Upper Back Disorders Cervical Disc Disease: cervical disc degeneration or herniation that
may or may not be accompanied by nerve root compromise Tension-Neck Syndrome (Trapezius Spasm): localized muscle fatigue
due to static, sustained contraction with accumulation of metabolic end products in muscles combined with insufficient oxygen supply
Biomechanical risk factors: highly repetitive work, forceful exertion, static contraction
Shoulder Disorders Rotator Cuff Disorder: degeneration of any of the four tendons of the
rotator cuff, particularly the supraspinatous tendon Bicipital Tendinitis: tendinitis of the biceps tendon, particularly the
long head of the biceps Biomechanical risk factors: repetitive work, sustained shoulder pos-
tures with greater than 60 degrees of flexion or abduction
Elbow Disorders Lateral Epicondylitis ("tennis elbow"): inflammation of the insertion
of the extensor carpi radialis brevis (muscle at the lateral epicondyle) Medial Epicondylitis ("golfer's elbow"): inflammation of the insertion
of flexor muscles at the medial epicondyle Biomechanical risk factors: forceful exertion, especially in combination
with other risk factors (e.g., force and repetition, force and posture)
Hand and Wrist Disorders Carpal Tunnel Syndrome: entrapment of the median nerve within the
carpal canal of the wrist Biomechanical risk factors: repetitive work, manual force, vibration
transmitted to the hand, combination of risk factors (e.g., force and repetition, force and wrist bending)
Trigger Finger: low grade inflammation of the flexor tendon sheath that results in tendon sheath thickening and local nodular swelling, with characteristic "sticking" of the digits
DeQuervain's Disease: thickening and narrowing of the tendon sheath of the abductor pollicis longus and extensor pollicis brevis tendons in the region of the anatomic "snuff box" of the thumb
Flexor Tenosynovitis: inflammation of flexor tendons and tendon sheaths of the forearm, particularly flexor carpi ulnaris
Extensor Tenosynovitis: inflammation of the extensor tendons and ten- don sheaths of the forearm, particularly carpi radialis longus and brevis tendons
Biomechanical risk factors: repetitive work, forceful work, posture, combination of factors (e.g., force and repetition, force and posture)
Low-Back Disorders Low Back Syndrome: soft tissue injury characterized by back pain
with localized symtpoms and no neurological deficits Lumbosacral Disc Herniation Disease: lumbosacral disk degeneration
or herniation, typically with nerve root compromise and associated neurological deficits
Biomechanical risk factors: heavy physical work, awkward posture, whole-body vibration
Lower Extremity Hip Osteoarthritis: degeneration of the hip joint characterized by pain
with associated X-ray changes Biomechanical risk factors: manual material handling and other heavy
work Knee Osteoarthritis: degeneration of the knee joint characterized by
pain with associated X-ray changes Biomechanical risk factors: manual material handling, kneeling,
stairclimbing �9
Source: [6,7].
The rates of musculoskeletal disorders reported to the BLS in- creased steadily throughout the 1980s and early 1990s [ 11,14,18], and similar trends have been reported in other countries. How- ever, it is not clear to what extent this reflects a true increase in incidence, as compared with improved diagnosis, recognition of work-relatedness, or reporting. In the state of Washington, the annual incidence of paid workers' compensation claims for CTS increased significantly among women, but not men, from 1984 to 1988 [19]; it could not be determined whether this re- flected a true differential incidence or different claim-filing behavior between men and women because of social or occu-
pational factors. Many industries and occupations have rates that are as much as
three to four times higher than the overall frequencies. High-risk industries are as varied as nursing facilities, air transportation, mining, food processing, leather tanning, heavy manufactur- ing of vehicles, furniture, appliances and electrical equipment, and light manufacturing, including electronic products, textiles, shoes, apparel, and upholstery [6,14]. Upper extremity mus- culoskeletal disorders have been found to be highly prevalent in manual-intensive occupations such as clerical work, postal ser- vice work, janitorial work, industrial inspection, and packaging. Back and lower limb disorders often occur in occupations that require heavy work such as manual material handling, nonneu- tral trunk postures, or exposure to whole-body vibration, espe- cially while seated (see section I.B.). At highest risk are truck drivers, operators of cranes and other large vehicles, warehouse workers, airplane baggage handlers, various construction trades, nurses, nursing aides, and other patient-care workers [3,11,13].
In 1989, U.S. workers' compensation costs were $11.4 billion for low back and $563 million for upper extremity disorders [20,21]. However, the frequency of WMSDs is likely to be un- derestimated by as much as 60% when relying on traditional administrative data sources such as workers' compensation re- cords and OSHA logs of recordable injury and illness [22,23]. The reasons for these discrepancies probably include factors as varied as workers' access to medical care, information about work-related morbidity, perceived job security, expected suc- cess in filing compensation claims, and employer medical management and return-to-work programs. It has been esti- mated that the indirect or hidden costs of workplace injuries and MSDs can range from 2 to 3.5 times the workers' compensation costs paid by an employer [ 12,24,25].
Disability and lost work time account for a large proportion of workers' compensation costs and impact negatively on work- ers' household income and feelings of self-worth. Correlates of poor MSD outcomes have included physical demands of the job, lack of worker autonomy, job dissatisfaction, receiving workers' compensation payments, pending litigation, and psychological disturbance [26-35]. However, interpretation of these findings often is ambiguous because of interrelationships among risk factors and lack of information about the temporal sequence of events. For example, the apparent effect of compensation may be confounded by physical or psychosocial job features, educa- tion and availability of other work, disease severity, access to medical treatment, and other factors.
Because work disability is influenced by myriad psychosocial and workplace factors, it provides a limited view of the out- comes experienced by the injured worker. Furthermore, return

476 SECTION 6 - W O M E N AT WORK
Fig. 38.1 Sewing machine operator positions garment for stitching. Copyright �9 Earl Dotter.
to work is not an irreversible or unidimensional event; workers may leave and return on multiple occasions, depending on changes in job assignment and working conditions, availability and quality of medical care, information about work-related morbidity, employers' medical management, and return-to-work programs [36]. Long-term effects on job security and career advancement have been described anecdotally but have not been studied quantitatively. In addition, injured persons experience social and psychological costs, including loss of self-esteem, ability to participate in family or community activities, and to care for self and family members [37,38]. Family members as well may incur costs as they take on new tasks to compensate for the disabled individual. Data on these burdens are also ex- tremely sparse [39,40].
B. Occupational Exposures and MSD
The generic ergonomic exposures relevant to the occurrence of MSDs include both physical workload and the organization of work in general. Examples of the former are stereotyped repetition of motion patterns, rapid work pace, exertion of high and/or prolonged muscular forces, anatomically nonneutral body postures (either dynamic or static), mechanical stress concentra-
tions (direct pressure of hard surfaces or sharp edges on soft tissues), insufficient rest or recovery time during work, and con- tact with vibrating objects. Extensive laboratory evidence shows that there are multiple plausible mechanisms by which physical stressors injure the soft tissues of the musculoskeletal system [41,42]. For example, tendon strain and cell damage accumulate as a function of work pace (the frequency and duration of me- chanical loading), the level of muscular effort, and recovery time between exertions [43,44].
The epidemiologic literature linking the physical features of work to the risk of MSDs is voluminous. In one review, NIOSH concluded that there is scientific evidence of cause-and-effect relationships between repetitive motion, forceful work, and pos- tural stress for disorders of the back and upper extremities, in- cluding tendinitis and carpal tunnel syndrome [6]. The risk is particularly high when two or more of these physical job features are simultaneous and exert synergistic effects. Thus, primary prevention of MSDs in the workplace should include multifac- eted ergonomics programs that emphasize engineering controls, especially the ergonomic design of workstations, equipment, tools, and work organization to fit the physical capabilities and limitations of the human body [ 15,45].
Work organization refers to the way that production or service activities are organized, allocated, and supervised so as to deter- mine task structure, the division of labor, and skill utilization by individual workers. Work organization thus determines physical job features (e.g., work pace, repetitiveness, duration of expo- sures, and recovery time) as well as psychosocial dimensions of the work environment such as decision latitude, psychological job demands, and social support from supervisors and among coworkers. Decision latitude reflects the worker's ability to make decisions about how the work is done, to control the work process, and to decide which skills to use to accomplish the job. Increased pace of work on an assembly line, time pressure in processing or responding to information, or a more complex maintenance problem increase psychological job demands. It is often difficult to distinguish between "physical" and "psycho- social" ergonomic risk factors. High psychological work de- mands typically involve both rapid physical work pace and feelings of time pressure, and highly stereotyped finger motion patterns occur when a manual job both is monotonous and offers little decision autonomy.
High psychological job demands in combination with low decision latitude result, over time, in chronic adverse health effects such as cardiovascular disease [46]. Because psychoso- cial job characteristics influence physiological parameters such as circulatory function, sympathetic nervous symptom arousal, and muscle tension, there are several plausible mechanisms by which they may increase musculoskeletal susceptibility to me- chanical insult [47-49]. In a ten-year prospective study of work- ers in the metal industry, both social support and work content were predictive of musculoskeletal status [50]. However, most other studies on this question have been cross-sectional; because psychosocial factors may be perceived and reported differently after the development of MSDs, the reported associations are difficult to interpret with respect to etiology. Thus, there is still only limited epidemiologic evidence concerning the indepen- dent effect of occupational psychosocial factors on MSD inci- dence [51 ].

C H A P T E R 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 477
II. Gender and Musculoskeletal Disorders
Being female is often described as a "risk factor" for many musculoskeletal disorders because prevalences in the general population and in large groups of employees have been re- ported to be twice as high among women compared to men [10,16,17,52-64]. However, comparisons of other endpoints have shown no, or no statistically significant, gender differences [17,61,62,64-66], and occasionally, especially for low back pain (LBP), the risk has been lower for women than for men [10,62,67,68].
To the extent that there are gender differences in MSD occur- rence, their interpretation is not straightforward. Different oc- cupational exposures might be responsible because women are concentrated in jobs with certain physical features because of the failure of many work sites to accommodate female anthro- pometry, or because women either sustain increased exposure to, or have higher perceived exposure to, psychosocial job strain (see section III.A.). In light of widespread sexual divisions of labor, it is essential to distinguish between gender differences in crude prevalence or risk and differences in the effects of occu- pational exposures on MSD occurrence or outcome.
Factors that might affect the gender-specific relationships be- tween occupational exposures and MSDs include differences in performance of household work, roles in the home and recrea- tional activities, or gender differences in pain reporting and health care seeking behavior. The possible role of biological factors such as gender-related differences in strength, muscle mass, tendon and muscle composition, and hormonal fluctua- tion on soft tissue should also be considered.
The following sections attempt to summarize the literature pertinent to these related but different questions:
Do MSDs (overall, or those that can be attributed to working conditions) occur more often among women workers than among men workers?
Are women at higher risk of MSDs than men in jobs with the same or similar levels of occupational exposure to ergonomic stressors?
Do women with work-related MSDs have different outcomes (e.g., pain severity and functional loss, disability, interference with social and family life, financial losses) than men?
Are there innate biological differences that might affect the risk of WMSDs in women compared with men?
A. Occurrence of MSDs among Women Workers
The evidence shows that working conditions explain a sub- stantial proportion of MSDs among women workers. The same associations between MSDs and ergonomic stressors that have been reported in male and mixed occupational groups have also been observed in analyses exclusively of women. For ex- ample, women employed in garment manufacturing have a higher prevalence of upper extremity symptoms and long-term disability due to musculoskeletal disorders when compared to women in other occupations [69-73]; such MSDs exhibit an exposure-response relationship with length of employment but also appear to induce garment workers to leave employment [73-77].
Upper extremity muscle, tendon, and joint disorders were el- evated among women workers in packing jobs [71,78], textile manufacturing [79,80], and electronics manufacturing [81,82]. Female assembly-line manufacturing workers had higher a prev- alence of shoulder and hand pain compared to a random sample of women from the general population; both work pace and duration of employment showed exposure-response trends [83].
Women working in poultry processing were more than twice as likely to have impaired median nerve sensory latencies (age- adjusted) as women applying to work in the same facility [84], and those employed in jobs with high versus low exposure to repetitive and forceful motions had more than twice the preva- lence of upper extremity disorders, especially those affecting the hand and wrist [85]. Similar effects have been reported among female fish processing employees [86-89].
In the service sector, work-related musculoskeletal disorders have been documented extensively among health care employ- ees such as female nurses and home health aides, as well as among food preparation and laundry workers [90-95]. The prevalence of CTS in female cashiers is higher than that in other grocery store workers [96] and is associated with poor work station design [97] as well as with hours worked per week and years worked as a cashier [98]. Work-related MSDs have also been reported among women cleaners [99,100], childcare work- ers [101], and nursery school cooks [102]. Multiple studies of female clerical workers operating video display units (VDUs) have shown an elevated risk of neck/shoulder and hand/arm disorders compared with women in other occupations [103- 106]. Among VDU operators, there is an increased risk with greater postural strain [107], more hours per day at the VDU [ 108], and faster call handling by telephone operators [ 109].
In the extensive literature on musculoskeletal disorders among working people, many investigations have examined whether there is an overall gender difference in the frequency of MSDs in employed populations. In a few of these studies it is possible to compare the risk in men and women after adjustment for differences in occupational exposures. A number of these stud- ies are summarized here (Tables 38.2-38.4). This review is no- nexhaustive; the primary selection criterion was the ability to control, at least partially, for gender differences in frequency or intensity of occupational ergonomic exposures in the analysis of their data.
It appears that the gender difference is least pronounced, or even nonexistent, for back pain (Table 38.2). The only study that showed a statistically significant increase in women was a large sample of the working population in the Netherlands [59]. How- ever, another Dutch study showed a higher prevalence of back and lower limb disorders among men than among women, after stratification based on mental and physical job demands [56].
With regard to upper extremity disorders there is no obvious pattern. Some studies showed a much higher risk in women than in men, and others found no difference at all. Being female was associated with at least a doubling of MSD risk in about one- third of the analyses of the proximal (Table 38.3) and distal (Table 38.4) regions of the arm.
Some studies [86,110,111 ] found larger gender differences for distal endpoints (e.g., wrist pain, CTS) than for more proxi- mal endpoints (e.g., shoulder disorders). However, others had similar results for both regions of the upper extremity [112-116].

478 S E C T I O N 6 - W O M E N AT W O R K
Table 38.2
Whole Body, Back, and Lower Limb Musculoskeletal Disorders: Relative Risk (Prevalence Ratio or Odds Ratio) in Women
Compared to Men, with 95 % Confidence IntervaP
Gender effect Reference Population (95% CI b or p-value)
[ 112] VDU workers low back symptoms NS c (p>0.05)
[27] Aircraft manufacturing workers back disorders reported to NS (p>0.05)
employer
[59] General working population, the Netherlands
back disorders 1.6 (1.4-1.8) back disorders (chronic) 1.2 (0.9-1.6) muscle or joint disorders (not 1.6 (1.4-1.9)
specified)
[139] Poultry slaughterhouse workers (cold exposed)
upper backache 1.2 (0.9-1.4) d leg pain 1.1 (0.9-1.3) a
Poultry slaughterhouse workers (assembly line)
upper backache 1.0 (0.8-1.2) a leg pain 1.0 (0.8-1.2) d
[ 1 2 2 ] Automobile manufacturing workers cumulative trauma of lower back 1.1 (NS)
(medically treated)
[ 111 ] Workers in four manufacturing facilities
low back and upper limb pain 1.3 (p>0.05) combined
[ 1 1 6 ] Slaughterhouse workers back pain 1.2 (0.7-1.9) a
Note. Increase in women statistically significant at p~<0.05 (boldface). aAdjusted for job title or ergonomic exposure, at minimum, and for age
and other factors where possible, by stratified or multivariate analysis. bCI = confidence interval. cNS -- not stated: point estimate or confidence interval not reported. aPrevalence ratio (cross-sectional study), odds ratio (case-control
study), and/or confidence interval calculated by authors from data in the paper.
Because of possible gender differences in pain reporting (see section V.B.), one could also hypothesize that the effect in
women might be higher for symptoms than for endpoints re-
quiting physical examination or more objective confirmation. For example, in a cross-sectional study at seven manufacturing facilities, Silverstein et al. found that hand/wrist disorders were strongly associated with exposure to both high manual forces and repetition rates [117]. Women had an increased risk com- pared to men, even adjusting for job demands (Table 38.4); most of the gender difference appeared to occur in jobs requiting high
manual force but low repetition, where more male than female subjects were employed. When the outcome was restricted to carpal tunnel syndrome by symptoms and physical examination, there was no longer an effect of gender after adjusting for job demands [ 118]. Three other studies of CTS also reported no or
Table 38.3
Neck, Shoulder, and Combined Upper Extremity Musculoskeletal Disorders: Relative Risk (Prevalence Ratio or Odds Ratio) in
Women Compared to Men, with 95 % Confidence IntervaP
Reference Population and body region Gender effect
(95% CP or p-value)
[222] Workers in routinized visual display unit (VDU) work
neck symptoms 1.5 (1.0-2.2) shoulder symptoms 2.2 (1.4-3.4)
Workers in CAD or programming VDU work
neck symptoms 2.9 (1.6-5.5) shoulder symptoms 3.1 (1.6-5.8)
[ 112] VDU workers tension neck syndrome 2.0 (0.7-5.6) e
(symptoms and signs) 6.4 (1.9-21.5) r any shoulder diagnosis 7.1 (1.6-32.2)
(symptoms and signs)
[113] Workers in VDU jobs with similar gender distribution
neck disorders (symptoms) 1.9 (0.8-4.5) shoulder disorders (symptoms) 1.5 (0.5-4.8)
[223] Newspaper employees neck disorders (symptoms) 2.3 (1.5-3.5)
[86] Fish processing workers shoulder girdle pain (various 1.1 (0.7-1.7) d
diagnoses)
[ 1 2 0 ] General population, Sweden neck/shoulder disorders (recent 11.4 (4.7-28)
medical care and signs)
[58] General population, England (orthopedic clinic patients)
shoulder disorders NS c (p>0.05)
[ 1 1 4 ] Telecommunication workers neck disorders (symptoms) NS (p>0.05) shoulder disorders (symptoms) NS (p>0.05)
[ 1 3 8 ] Workers in two poultry processing facilities
neck and UE 8 disorders 1.2 (0.7-1.9) d (symptoms)
neck and UE disorders 1.1 (0.5-2.4) d (symptoms and signs)
[60] General population, Finland h chronic neck pain (age 30-64) 1.6 (1.4-1.9) d chronic neck pain (age 65+) 1.3 (1.0-1.7) d
[ 115] Textile manufacturing workers epicondylitis NS (p=0.03) shoulder conditions NS (p>0.05) neck conditions NS (p>0.05) myalgia NS (p=0.001) arthralgia NS (p>0.05)
[ 165] Public sector office workers neck/shoulder/back symptoms 1.9 (p=0.005)
[ 1 2 2 ] Automobile manufacturing workers cumulative trauma of the neck 1.1 (NS)
(medically treated) rotator cuff syndrome (medically 1.1 (NS)
treated) other UE cumulative trauma 1.0 (NS)
(medically treated)

C H A P T E R 38. W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 479
Table 38.3
(continued)
Reference Population and body region Gender effect
(95% CI b or p-value)
[ 224 ] Newspaper employees upper extremity disorders 2.2 (1.5-3.3)
(symptoms)
[ 110,168] Automobile manufacturing workers, cross-sectional
shoulder/upper arm disorders 1.6 (1.1-2.2) (symptoms)
shoulder/upper arm disorders 1.7 (1.2-2.4) (symptoms and signs)
Automobile manufacturing workers, 1-year follow-up
upper extremity disorders 1.4 (0.6-3.5) (symptoms and signs)
[ 111 ] Workers in four manufacturing facilities
trapezius pain 10.1 (p>0.05)
[ 1 1 6 ] Slaughterhouse workers neck and shoulder pain 1.3 (0.9-1.9) a
Note. Increase in women statistically significant at p ~< 0.05 (boldface). aAdjusted for job title or ergonomic exposure, at minimum, and for
age and other factors where possible, by stratified or multivariate analysis. bcI = confidence interval. cNS = not stated: point estimate or confidence interval not reported. dprevalence ratio (cross-sectional study), odds ratio (case-control
study), and/or confidence interval calculated by authors from data in the paper.
eWomen without children under age 16 at home. fWomen with children under age 16 at home. gUE = upper extremity. hAges 30-64: adjusted for physical demands in current job. Age 65+:
adjusted for physical demands in longest held previous job.
only very weak associations with gender [71,96,119]. On the other hand, the occurrence of specific hand/wrist tendinitis con- ditions in the seven manufacturing plants showed a gender ef- fect almost identical to that for all disorders [43]. In fact, several of the strongest associations with gender [112,120,121] were observed for more restrictive case definitions.
Thus, although women often are reported to have higher rates of (work-related) musculoskeletal disorders, after adjusting for occupational exposure there is no consistent pattern in the liter- ature. Possible reasons for the discrepancies among studies in- clude differences in study populations (i.e., types and extent of occupational and non-occupational exposures) and how well er- gonomic exposures were characterized. Adjustment only for plant type or department [115,116,121,122] probably results in greater nondifferential misclassification of exposure and re- sultant residual confounding of the gender comparison (see III.A.). Although some of these studies are consistent with the hypothesis that women have higher rates than men of MSDs, further research is required in studies designed to adjust ade- quately for exposure differences before general conclusions can be drawn.
Table 38.4
Wrist and Hand Musculoskeletal and Nerve Compression Disorders: Relative Risks (Prevalence Ratio or Odds Ratio) in
Women Compared to Men, with 95 % Confidence Interval a
Reference Population and body region Gender effect
(95% CP or p-value)
[43] Workers in seven manufacturing facilities
hand or wrist tendinitis (symptoms and signs)
[ 1 1 2 ] Workers in routinized visual display unit (VDU) work
any arm or hand diagnosis (symptoms and signs)
[ 113 ] Workers in VDU jobs with similar gender distribution
wrist and hand symptoms
[158 ] Automobile assembly line workers forearm/hand symptoms
[86] Fish processing workers carpal tunnel syndrome
[58] General population, England (orthopedic clinic patients)
finger disorders wrist and forearm disorders
[ 1 3 7 ] Automobile manufacturing workers forearm/hand symptomsr
[ 1 1 4 ] Telecommunication workers elbow, wrist, and hand disorders
(symptoms)
[71 ] Workers in three industrial sectors carpal tunnel syndrome
[ 115] Textile manufacturing workers carpal tunnel syndrome tendinitis ganglions
[119] Workers from four industries, at 5-year follow-up
slowed median NCV8
[165] Public sector office workers hand/arm symptoms
[ 1 2 2 ] Automobile manufacturing workers carpal tunnel syndrome
(medically treated)
[ 1 1 0 ] Automobile manufacturing workers, cross-sectional
wrist/hand disorders (symptoms) wrist/hand disorders (symptoms
and signs)
[ 1 1 7 ] Workers in six manufacturing facilities
hand/wrist disorders (symptoms and signs)
[ 118 ] Workers in seven manufacturing facilities
CTS (symptoms and signs)
[225] Industrial automotive workers CTS symptoms (also had longer
NCV latencies)
4.3 (p<0.05)
5.2 (1.2-22.8) e
1.7 (0.8-3.6)
1.6 (1.2--2.1)d
2.6 (1.3- 5.2 )d
NS c (p>0.05) 1.8 (1.1-2.9)
1.2 (1.0-1.4)
NS (p>0.05)
1.5 (0.7-3.0)
NS (p=0.02) NS (p=0.01) NS (p>0.05)
NS (p>0.05)
NS (p>0.05)
2.3 (1.6-3.3)
2.2 (1.6-3.0) 2.7 (2.0-3.7)
4.8 (p<0.05)
1.2 (0.3-4.7) d
1.3 (0.9-1.7) a
(continued)

480 S E C T I O N 6 - - W O M E N AT W O R K
Table 38.4 (continued)
Reference Population and body region Gender effect
(95% CP or p-value)
[ 17] General population employed during past year, U.S.
self-reported CTS 1.9 (1.6-2.4) self-reported medical history of 2.2 (1.5-3.3)
CTS
[ 1 1 6 ] Slaughterhouse workers arm and hand pain 1.0 (0.7-1.4) d
Note. Increase in women statistically significant at p~<0.05 (boldface). aAdjusted for job title or ergonomic exposure, at minimum, and for age
and other factors where possible, by stratified or multivariate analysis. bcI = confidence interval. cNS = not stated: point estimate or confidence interval not reported. dprevalence ratio (cross-sectional study), odds ratio (case-control
study), and/or confidence interval calculated by authors from data in the paper.
eWomen with children under age 16 at home (only). fAdjusted for repetitive hand movements > 4 hours daily. Adjust-
ment for precision movements or repetitive finger movements, either > 45 minutes or > 4 hours per day, gave similar results, as did adjust- ment for manual handling activities.
gNCV = nerve conduction velocity.
B. Outcomes of Musculoskeletal Disorders among Women Workers
Women are usually reported as experiencing more work dis- ability and losing more days from work due to CTS and other MSDs than men [30,52,62,123-127]. However, other studies have found no gender differences in clinical or occupational outcomes of MSDs [ 10,26,54]. A large study of U.S. automobile manufacturing workers found that being female was associated with a larger excess of upper extremity disability than back disorder disability, after adjusting for production department [ 121 ]. In Norway, absenteeism from work for more than 14 days in 1994 because of neck and shoulder MSD was more frequent among women than among men, but the gender difference was greatest among people over 45 years of age and in the lowest income group [128]. After adjustment for these two variables, men had a higher cumulative incidence of long-term absentee- ism and little difference in mean duration. On the other hand, English men had more short-term MSD absenteeism (~<7 days) than women after adjustment for age and socioeconomic status, but there was no gender difference in longer absences [ 124].
The predictors of MSD disability and other outcomes have rarely been examined separately by gender. One study found that return to work after CTS treatment was markedly lower for women than for men, even taking into account prior symptom severity and functional impairment [ 127]. Another study showed that a multifaceted rehabilitation program for chronic back pain benefitted only the female participants [129]. Women workers differ from their male counterparts in several important respects that might influence outcomes. First, as noted earlier, women's jobs are more repetitive and offer less decision autonomy than men's jobs; thus, women may be at greater risk than men for
Fig. 38.2 Laundry worker stocks poorly designed hospital bed linen storage racks, forcing her to lift heavy bedding above shoulder height. Chicago, Illinois (1993). Copyright �9 Earl Dotter.
work-associated musculoskeletal disability because of difficulty with job performance or reinjury [130]. Second, women gener- ally have more responsibility for household work and care of family members, so the family burden may have more influence on return-to-work decisions by women than by men; further, the cost of lost household services greatly outweighs wage losses for women [131 ]. Physicians' perceptions of the work demands in men's and women's jobs may also differentially affect medi- cal treatment or the success of a compensation claim and thus the financial option to stay out of work [37,132].
III. Interpretation of Gender Differences: Occupational Physical Stressors
A. Exposure Differences
Because of workplace sex segregation, both formal and infor- mal, women and men typically experience qualitatively and quantitatively different working conditions. In many epidemio- logic studies of WMSDs, comparisons of the risk for women and for men may be confounded by differences in occupational exposures. In particular, job title or occupation has often been

CHAPTER 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 481
used to categorize ergonomic exposure. Use of such imprecise measures of exposure may create the appearance that gender is an independent risk factor for development of WMSDs when in fact occupational exposures may not have been adequately ac- counted for.
In a sample of the general population in Sweden, followed from 1970 to 1993, men had a higher index of physical work load overall than did women [133]. The difference was most pronounced among younger men during the period from 1970 to 1980 [134]. Physical work demands decreased over the 24 years among men, especially the younger subjects, whereas a small increase in physical demands was observed in younger women in the early 1980s. Similarly, in a large cross-sectional sample of the Finnish population, men aged 30 to 64 years were more likely to be in jobs with high exposure to physical stress at work, and women were more likely to be in jobs with inter- mediate exposure [60]. The same pattern was found among sub- jects aged 65 or more with respect to physical work load in the previous job of longest duration.
Such summary exposure indices may be insensitive to differ- ences in types of exposures and often place more emphasis on whole-body exertions and energy expenditure than on localized, repetitive stresses to the upper extremities. In the industrial sec- tor, including food processing, women are overrepresented in packing and assembly or other "light" jobs that require rapid, precise, repetitive hand motions [86,111,117,135-139]. Similar gender differences in ergonomic exposures have been reported in the service sector, including cleaning [99], grocery store work [96], and operation of VDUs [ 140].
Even within the same occupation, physical exposures may differ by gender. For example, women and men working in the same factories, with the same job titles, did not always perform tasks with the same physical requirements or work organization [ 141,142]. Women performed more repetitive work on average, whereas men were less likely to sit for prolonged periods. Men were significantly more likely than women to work irregular and unpredictable hours and more than 40 hours per week.
As a group, women also hold jobs with less control over the work process, less latitude for making autonomous decisions, and fewer opportunities for job modification [46,50,143-145]. These gender differences in decision autonomy and monotony have even been observed within female-dominated jobs [143].
Jobs requiting high static loading of the neck and shoulder, with repetitive use of small muscle groups, involve a high risk of upper extremity disorders such as carpal tunnel syndrome and hand-wrist tendinitis. During dynamic low-load manual work, both the speed of motion and high precision demands substantially increase measured muscle forces relative to their capacity [146,147]. Ironically, the physical demands of these female-intensive jobs are often perceived to be less strenuous than the jobs typically performed by men because they do not require high-force whole body exertions such as lifting and car- rying very heavy objects [99,141,142]. In contrast, in the health care sector many women hold jobs such as nurse or nursing assistant, with high patient lifting demands and high rates of low back injury.
Women may sustain greater exposure to biomechanical stres- sors even when performing the same tasks as men because many workplaces have been designed on the basis of anthropometric
data for men and are ergonomically inappropriate for women. Men and women, on average, differ in many aspects of physical body size and functional capacity, such as stature, body segment lengths, flexibility, and muscle strength [148]. These differences lead to a poorer fit, on average, of tools, equipment, work- stations, gloves, and other personal protective equipment for women workers, with resulting increases in biomechanical dis- advantage and postural strain [149-153]. As a result, gender differences in work technique or posture for performing the same tasks have been observed [43,154,155].
A strong association has been found between gender segre- gation at the occupational level and absence from work because of MSDs in both genders [156,157]. In the few gender-integrated occupations (40-60% men), both women and men had the low- est rates of sickness absence. Absenteeism for MSDs was higher when there was gender segregation in either direction and very high, especially for women, in the group of extremely male- dominated occupations (>90% men). Whether sex segregation per se is a risk factor (possibly as a source of psychosocial strain) or if it is confounded by (or acts as a proxy for) differ- ences in physical working conditions has not been clarified.
B. Interaction between Exposure and Gender
Only a small number of MSD studies have compared the effects of similar job features on men and women to examine whether gender modifies the effect of ergonomic exposure on MSD risk. Among those reviewed here, the findings are markedly inconsistent. Some investigations found stronger associations for MSDs and physical stressors among women [122,158], whereas others reported no or few differences between men and women in the associations between MSDs and ergonomic exposures [86,117, 122,138] or that women are at higher risk from some exposures and men from others [57,159]. It is difficult to find any pattern among these results, even when examining specific exposure-endpoint relationships. For example, a group of French authors reported that carrying heavy loads was a risk factor for joint pain with restricted movement only in men [57], whereas heavy lifting was a risk factor for LBP only among women in an English study [ 160]. In the U.S. general population, osteoar- thritis of the knee was associated with occupational demands for knee bending and manual material handling in men only; few women had jobs with similar physical demands [ 161 ]. However, two other studies showed a stronger association with occupational physical activity among women than among men [162,163].
In a few studies, risk ratios for the effect of exposure on MSDs have been higher among women than among men, al- though the findings varied by specific exposures and specific MSD endpoints [137,160]. Three prospective studies showed that MSD symptoms in women were more responsive to changes in occupational exposures. Two Nordic groups reported that women, but not men, experienced increased frequency of distal upper extremity symptoms following increased repetitiveness of manual motion patterns [89,164]. Among U.S. public sector office workers, neck, shoulder, and back symptoms were twice as likely to improve among female compared with male em- ployees after office relocation [ 165].
Eight different studies have shown more MSDs among women than among men in the lowest stratum of ergonomic exposure,

482 S E C T I O N 6 - W O M E N A T W O R K
70%
60%
50%
40%
30%
20%
10%
0%
e 4
ak,= , 0 . 4
7-12 13-18 19-25
Exposure Score
e4 e~
12Men
13Women
40%
30%
20%
10%
0% , e ~ , ~ , . . . .
I:-nl Women . .
0 - 6 7-12 13-18 19-25
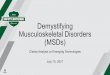
Exposure Score Fig. 38.3 Frequency of upper extremity musculoskeletal disorders on examination, by baseline exposure, among 1198 workers in automotive engine and stamping operations. (a) Baseline prevalence; (b) one-year cumulative incidence (data from references [ 110,167,168]).
with the difference decreasing in the higher exposure groups so that the effect of ergonomic stressors on MSD risk was greater among men [17,60,86,158,166,167]. For example, among au- tomobile manufacturing employees, there was substantial effect modification of physical exposure by gender, in which women had a higher baseline risk than men in the lower exposure groups but about the same risk in the highest exposure group (Fig. 38.3a) [ 167]. However, at the one-year follow-up, the risk of new upper extremity disorders, adjusted for physical exposure level, varied much less between men and women (Fig. 38.3b) [ 168]. Possible explanations include that a healthy worker selec- tion effect (HWE) might be operating predominantly among women employed in the most physically demanding jobs, or that gender differences in symptom reporting are modified by the intensity of ergonomic exposures.
Other findings are consistent with the possibility that women workers are disproportionately affected by HWE selection pro- cesses. Among automobile assembly line workers, women, but not men, with higher seniority had higher pressure pain thresh- olds in the forearm and hand [ 158]. Similarly, the proportion of female, but not male, package sorters decreased with increasing seniority [ 151 ]. Because the physical demands of the job were disproportionate to women's body size and strength, the authors hypothesized that selection out of the workplace had been more pronounced among women over time because of excessively heavy work. On the other hand, in two other studies, the effect of MSDs on the selection process appeared to be stronger in men than in women [160,169]. HWE patterns are obviously
influenced by opportunities to move into less demanding jobs, which may vary not only by gender but also by region and economic circumstances such as unemployment rates.
IV. Interpretation of Gender Differences: Occupational Psychosocial Exposures
As with physical ergonomic exposures, the effects of psycho- social job conditions on MSDs have rarely been examined in men and women separately. Leino and H~inninen [50] found that low work control at baseline predicted 10-year musculoskeletal morbidity of the neck/shoulder in white-collar women and of the low back in blue-collar women, whereas it had no predictive value among men. Monotonous work content was associated with signs of MSDs of the low back and lower limbs among blue-collar workers of both genders, and low social support at work was likewise a risk factor both for men and for women. All analyses were adjusted for a rough measure of physical workload that emphasized whole body effort rather than repeti- tive manual work, so intrastratum confounding by physical job demands could not be ruled out.
In two Swedish cross-sectional studies, multiple interactions between gender, psychological load, decision latitude, and so- cial support were found. In one, musculoskeletal symptoms were generally elevated when high job demands were combined either with low job control or with low social support [ 170]. The prevalence ratios for psychosocial job features and neck symp- toms were slightly higher among women than among men, whereas the effects on shoulder and back symptoms were stronger for men. In the other study, high decision latitude was also associated with an increased risk of neck and shoulder symptoms among women only [ 171 ]. In an examination of pos- sible mechanisms of effect, psychological work demands were associated with physiological indicators of strain (self-reported muscle strain and cortisone levels); muscle tension was, in turn, associated with symptoms from the back, neck, and shoulders. There was also an unexpectedly high prevalence of MSD symp- toms in the highest socioeconomic class among working women, which contradicted the traditional (albeit male-based) model that high decision latitude alleviates psychosocial stress. The authors noted that well-educated women in jobs with high de- cision latitude were found to perceive high stress related to re- sponsibility at work, but this was confounded by responsibilities for the family. In addition, a Canadian study similarly found that women were more substantially affected by high job de- mand and more adversely affected by high job routinization than men [ 144]. These authors also hypothesized that women's greater vulnerability to job demands could be a function of de- mand at home (see section V.A.).
There are other types of psychosocial strain in the workplace that may be more common or more important for women than for men. These include responsibility for the well-being of oth- ers (health care, childcare, teaching); responsibility to multiple supervisors (clerical work); unpredictable, "flexible" schedul- ing that interferes with family responsibilities, especially caring for children; lack of social support, especially in traditionally male-dominated occupations such as construction and heavy manufacturing [152]; and sex discrimination and overt sexual

C H A P T E R 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 483
harassment. These sources of strain typically are not measured by standardized instruments, such as the Job Content Question- naire [ 172], and thus may represent sources of unmeasured con- founding or effect modification in epidemiologic studies. The possible contribution of racial or ethnic discrimination as a source of stress has not been examined.
Women workers in traditionally male-dominated jobs often feel that they need to work harder or take more risks than their male colleagues take in order to prove themselves to their su- pervisors and coworkers [152]. On this issue the psychosocial aspects of the work environment, especially a lack of social support, have potential consequences for the physical exposures if overcompensation leads to workers injuring themselves, for example, by trying to lift loads that are too heavy.
V. Interpretation of Gender Differences: Extrinsic Factors
A. Double Exposure: Work and Home
Household responsibilities result in greater overall exposure to physically demanding activities and psychosocial strain, as well as a reduction in opportunities for recovery after the work- ing day. The extra responsibilities of household chores and childcare have traditionally been borne more heavily by women, and there are significant gender differences in time spent on domestic work. For example, among French workers with chil- dren, women spent more time than men on domestic chores (21.8 hours per week compared with 4.9 for men), and women without children also performed significantly more housework than men (17.3 hours per week compared to only 5.3 for men) [141].
A Swedish study investigated gender differences among 12,777 workers in the distribution of home responsibilities and psychosocial work environment characteristics, as well as re- sources to deal with these potential stressors [ 173]. Exposure to nonoccupational stress was assessed through measurements of household work, number and age of children, and childcare re- sources. The study found that after adjusting for work and home characteristics, gender was no longer associated with psycho- somatic strain. The authors noted that there were major differ- ences in the life experiences of Swedish women and men that went far beyond their occupational exposures, and that these daily life circumstances might account for some of the observed disparity in the prevalence of musculoskeletal disease.
There are other data that lend support to the hypothesis that housework may at least partially explain the discrepancy in musculoskeletal disorders between male and female workers. Bergqvist et al. found that, among VDU users, women with young children at home had higher prevalences of MSDs than men or other women, after adjusting for work-related and other demographic factors [112]. In a large group of female sewing machine operators, having children was associated with about double the risk of chronic shoulder pain; the authors suggested that the reason might be the physical load of lifting and carrying small children [69]. Interestingly, in a prospective study, extra domestic work and few social contacts were predictors of LBP among men only, although unsatisfactory leisure time was a risk factor both in men and in women [159]. There has been little
study of the magnitude or variability of ergonomic stressors during home activities [ 174] or their effects on MSD risk.
B. Pain Reporting and Seeking Medical Care
Another possible explanation for the apparent higher rates of MSDs in women may be a greater willingness to report symp- toms on interview, to report problems to workplace supervisors, or to seek medical care for conditions of the same pain severity. As already noted, the literature is inconclusive as to whether women are more often absent from work for MSDs, after ad- justing for age, socioeconomic status, and job demands. Some investigators have explicitly suggested that women are prone to overreporting symptoms and malingering [ 175]. However, there have been few published comparisons of the validity of MSD symptoms reported by male and female workers. In a large sample of the U.S. general population, women reported more MSD symptoms than men but did not have more findings on physical examination [54]. In contrast, a Dutch study reported that gender differences in seeking medical care and use of med- ications were roughly similar to the differences in musculoskel- etal symptom prevalence [59]. Bergqvist et al. [ 112] found that, as a group, men were actually more likely than women to report upper extremity and neck symptoms without physical exami- nation findings in the same body region [176]. Among CTS patients, correlations between subjective assessment of hand weakness and measured grip strength were comparable between men and women [177].
Health care-seeking behavior often varies between men and women, although study findings disagree as to whether or not women and men with MSD symptoms seek care at different rates [38,66,178-180]. In a group of patients with temproman- dibular pain, women were overrepresented but had similar rat- ings of chronic and experimental pain as men; the authors suggested that women might be more responsive to symptoms and more willing to admit health problems [181 ]. On the other hand, women often have surgery for degenerative joint disease at a later stage than men, despite significant pain and functional impairment, in part because of their caregiving roles in the fam- ily [ 182].
Several authors have examined pressure pain thresholds (PPT), which can be interpreted either as a measure of pain tolerance or of prior damage to the muscle tissue. PPT values are gener- ally higher in men than women [ 183-185]. One study showed that pain thresholds in the neck and shoulder region were asso- ciated with the psychosocial work environment; the interpreta- tion of the findings may involve plasma cortisol or endorphin levels or may be partially mediated by sleep disturbance [ 185].
Bystr6m et al. reported that PPTs of the fight hand and fore- arm were lower among auto assembly line workers with forearm or hand symptoms in the previous 7 days [ 158]. Men had about 50-60% higher thresholds than women, both overall and among asymptomatic workers. The difference in PPT between men with and without symptoms was much smaller than the corre- sponding difference in women, suggesting either that reported symptoms were more misclassified among men (men denied symptoms more often?) or that PPT did not reflect the same pain phenomenon in the two genders. In addition, the effect of

484 S E C T I O N 6 - - W O M E N AT WORK
assembly line work on physical examination findings of de Quervain's tendinitis was greater in men, but the reverse was true for clinical diagnosis (which also required symptoms), sug- gesting that men might have more preclinical conditions or be less likely to acknowledge symptoms than women.
Among 184 active workers with abnormal sensory nerve con- duction studies, women were almost three times more likely than men to acknowledge symptoms consistent with CTS; sub- jects in more repetitive jobs were also more likely to report symptoms [ 186].
These results present a mixed picture. Some suggest that women are more likely to report symptoms or seek medical care for MSDs, whereas others disagree. However, the question is difficult to evaluate, because there is no objective gold standard for musculoskeletal pain. Clinical examination methods do not necessarily measure the same domains. Pain is inherently sub- jective, yet it is a legitimate entity for study and prevention. Furthermore, pain is the experience motivating the behaviors that result in MSD costs, such as seeking medical care, work absenteeism, and filing claims for compensation. If men deny pain and delay seeking medical attention, their disorders may progress further and be less amenable to medical treatment and workplace intervention. Whether pain perceptions and pain- related behavior actually vary between men and women, and in what ways, deserves further and careful study.
VI. Interpretation of Gender Differences: Physiological Factors
Physiological factors affect work performance and can pos- sibly interact with ergonomic exposures to increase the likelihood of developing musculoskeletal disorders. Physiological factors with gender-related differences that may predispose a person to the development of WMSDs include muscle strength and mus- cle fiber type distribution, anthropometric measures, hormonal differences, and biological changes associated with pregnancy.
A. Muscle Strength and Physiology
Gender-related biological differences may result in differen- tial vulnerability of women to physical workplace factors. Prominent among these differences is muscle strength and dis- tribution. Women's total body strength is, on average, about two-thirds that of men's; however, the ratio in static strength (ability to move a stationary weight) ranges from 35 to 85%, depending on the tasks and muscles involved [148]. Women's average strength is relatively lower in the upper extremities [187] and closer to men's for leg exertions, dynamic lifting, pushing, and pulling activities, and manual handling of smaller containers. The difference is also smaller when men and women have similar industrial experience or athletic training [ 188]. De- spite the average differences, there is also substantial overlap in the strength distribution between men and women, as much as 50% or more for certain muscle groups, especially because many muscle strength values are not normally distributed. In all, the factors of gender, age, weight, and height only explain about one-third of the variability in human strength data.
With respect to musculoskeletal disorders, the health im- plications of the average strength differential are not clear.
Kilbom reported a relationship between decreased neck dis- orders and isometric strength in women with heavy, varied jobs, but not in women in so-called light repetition jobs [ 189]. How- ever, in another study there was no evidence that low muscle strength predicted upper extremity MSDs [82]. In a group of Swedish students followed from age 16 to age 34, physical ca- pacity in adolescents was found in both genders to influence the development of neck, shoulder, and low back symptoms in adulthood [190]. Several measures of flexibility and grip strength were associated with decreased risk of neck, shoulder, and low back problems in adulthood, although bench press strength predicted an increased risk of LBP. Other studies have been similarly inconclusive as to whether or not muscle strength is protective against LBP [67,191,192], and at least one other study has shown high muscle force capacity to be a risk fac- tor [193]. It should be noted that although stronger muscles are capable of generating higher internal forces, they do not imply greater strength in other soft tissues, such as nerves and spinal discs.
Another possible explanation for the low predictive value of muscle force capacity, especially in low-effort work, relates to the physiologic process of muscle fiber recruitment during con- tractions. The near-continuous firing of low-threshold motor units during static work has been proposed as a mechanism for the selective injury of individual muscle fibers, even when the muscle as a whole is not fatigued [194,195]. Women, on aver- age, have a higher relative volume of slow-twitch (aerobic) to fast-twitch (anaerobic) muscle fibers than men [ 196]. It has been hypothesized, although not confirmed, that individuals with more slow-twitch fibers may be less likely to alternate among muscle motor units during low-force contractions [147,197]. This theory deserves further investigation as a possible expla- nation of gender differences in the occurrence of neck/shoulder disorders in jobs with high static muscle loading.
Strength testing has been proposed as a gender-neutral hiring criterion that might protect both men and women from WMSDs [193]. Because there is a large overlap between population dis- tributions of the static strength of men and women, selection of individuals able to lift a given weight will not exclude all pro- spective female employees from heavy jobs. However, evidence is inconclusive concerning the effectiveness of static strength testing to predict an individual's likelihood of injury. Using such criteria might unnecessarily exclude persons who would not suf- fer injury and include those who would.
Furthermore, Stevenson et al. have argued that there is a gen- der bias inherent in standard strength testing procedures be- cause motion patterns observed in the workplace are typically used to determine the relevant testing maneuvers, but women often use different strategies to perform physically demanding tasks [155,198]. In addition, the gender difference in static strength is greatly diminished after correction for body weight and fat composition, an appropriate procedure if women select work strategies to optimize their biomechanical and physiolog- ical advantage in ways related to these physical characteristics [ 149,188]. Furthermore, strength tests do not measure other im- portant physiological capacities such as dynamic (aerobic) en- durance or range of motion, all of which differ little between the genders or even favor women [196,198-200], and which also may be relevant to injury occurrence or susceptibility.

CHAPTER 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 485
B. Tendons, Ligaments, and Connective Tissue
Tendons in women appear to have different responses to re- petitive motion exposures than those in men. In particular, one study demonstrated that flexor digitorum profundus tendons from women were significantly stiffer than those from males when tension was applied [44]. Additionally, tissue creep (time- dependent elongation) was less pronounced in female than in male tendons.
It is possible that gender differences between the regulation of cell activity in women compared with men may contribute to differences in development of WMSDs. Overall, the literature indicates that tendon and ligament cells from female subjects are influenced by sex hormones as well as by pregnancy-related factors. Ligaments have receptors for sex hormones and are re- sponsive to hormones and changes in hormone levels [201]. Both human and rabbit tendon tissues have been found to con- tain receptors for sex hormones and studies have revealed that cell activity in these tissues is influenced by pregnancy. Studies of sex hormone receptors in connective tissue indicate that hor- monal influences that fluctuate during the menstrual cycle or during pregnancy may contribute to differences in regulation of ligaments and tendons and subsequent development of muscu- loskeletal disorders [202].
Sex hormones may also play a role in the degradation of cartilage through regulation of the inflammatory response [203]. Overuse injuries to tendons are thought to result primarily from fatigue of tissues followed by an inflammatory response [204]. There is a growing body of evidence to suggest that neurogenic inflammation may play a role in the induction of peritendinitis as well as the response to tendinitis [44]. Such responses can be generated by exposure to the neurotransmitters Substance P and calcitonin. Conceivably, gender-based differences in induction and elaboration of inflammatory responses might result in dif- ferential susceptibility through these neurogenic mechanisms.
C. Endocrine Factors
The role of female hormones in development of MSDs is very poorly understood. Although tendons and ligaments have recep- tors for female sex hormones, the implications of these findings are not known. The literature is inconsistent as to the relevance of endocrine influences, such as oral contraceptive use or bilat- eral oophorectomy, on the occurrence of carpal tunnel syndrome among employed persons [55,72,86,96,118,135,205]. LBP has been associated with menstruation, oral contraceptive use, in- duced abortion, number of live births, menopausal symptoms, and lower age at menopause, although the evidence is very sparse and the mechanisms of these associations are largely un- known [206-208]. One study has suggested a possible hor- monal role in biochemical changes related to joint cartilage degeneration [ 163]. Data are lacking as to whether or not these indicators of hormonal status are important modifiers of the effect of ergonomic exposures at work on MSDs.
D. Pregnancy
A number of physical changes occur during pregnancy that may at least transiently place women at increased risk for mus-
culoskeletal disorders. These include increases in body weight and changes in body weight distribution as well as an insuffici- ency of abdominal muscles. Additionally, pregnant women have altered connective tissue function, including increased peripheral joint laxity, possibly due to release of relaxin or other hormones.
Pregnancy-associated anthropometric changes may increase susceptibility of women to physical ergonomic stresses. Paul and Frings-Dresen described work postures in pregnant com- pared with nonpregnant women [209]. Pregnancy resulted not only in greater body weight and changed body mass distribu- tion, but also in a difference in the fit between body and work- place dimensions. For example, pregnant women sat further from work surfaces compared to nonpregnant women. Their hips were typically positioned further backwards, with in- creased compensatory trunk flexion, arm anteflexion, and exten- sion. Workplace layouts in which the work surface height was self-selected resulted in marked diminution of postural strain, highlighting the importance of workplace accommodation.
Although upper extremity strength is not substantially af- fected by pregnancy [210], whole-body lifting capacity is al- tered in later pregnancy as the center of gravity moves and as increased body size prevents objects from being lifted close to the body. In addition, the ligaments and muscles of the back and abdomen are stretched, making lifting potentially more hazard- ous. There is evidence of increased risk of low back injury for pregnant women performing specific tasks such as heavy lifting, standing, and frequent climbing of stairs [211], although LBP in pregnancy has not been associated with measures of physical fitness or strength [212,213]. There has also been little effort to distinguish LBP associated with pregnancy from an increase in risk of work-related low back pain during pregnancy.
Lastly, carpal tunnel syndrome associated with pregnancy is a well-described phenomenon [214-216], although the cause has not been completely elucidated. However, it has been hy- pothesized that fluid retention in pregnancy may be sufficient to lead to nerve compression at the wrist and subsequent carpal tunnel syndrome. Generally, carpal tunnel syndrome cases remit spontaneously after delivery, lending further support to the suggestion that biological changes during pregnancy are respon- sible. However, the effect of ergonomic exposures in the work- place on carpal tunnel syndrome during pregnancy has not been adequately investigated. It is not known if pregnant women working in jobs associated independently with increased risk of CTS are at greater risk of developing CTS than pregnant women who do not sustain such exposures. Additionally, the possible role of postpartum occupational exposures in preventing the usual postpartum spontaneous recovery has not been investi- gated. Thus, although pregnancy only accounts for a small por- tion of women's work lives, the relationship between the potential increased risk of MSD development in pregnancy and subsequent inability to heal due to sustained biomechanical in- sult in the workplace, even after pregnancy has ended, is trou- blesome, particularly in nations such as the United States that do not provide for prolonged maternity leave from work.
VII. Conclusions and Research Needs
Musculoskeletal disorders occur in relation to ergonomic ex- posures both in men and in women. There is substantial clinical,

486 S E C T I O N 6 - - W O M E N AT W O R K
biomechanical, and epidemiologic evidence supporting the rela- tionship between MSDs and ergonomic factors in the workplace, including high repetition, high manual forces, and vibration [6]. For example, the relative risk of CTS among individuals highly exposed to repetitive hand motion, forceful exertions, wrist bending, and segmental vibration has been estimated to range from 2 to 7 [55,118,217,218], implying an etiologic (i.e., pre- ventive) fraction ranging from 50 to 87% in worker populations with high prevalences of ergonomic exposures [219].
Thus, there is adequate scientific knowledge regarding spe- cific occupational ergonomic stressors to prevent a large propor- tion of MSDs among working people. Preventive measures should not and need not be discriminatory with respect to gender. The best approach to eliminating musculoskeletal injuries from the workplace is the implementation of engineer- ing controls, such as changes in equipment and workstation and job design, in the context of a comprehensive ergonomic program with participation from all levels of the enterprise [15,220,221].
More research is needed to elucidate whether MSD risk varies between women and men in jobs with the same occupational exposures, and whether work-related MSDs have the same out- comes in women and in men. Women often report MSDs more frequently than men; however, this difference appears to be less marked for low back disorders and when men and women are compared within homogenous job groups. Exposure-response relationships have been examined by gender in only a few studies, and the results have not been consistent. However, some studies suggest that men may have higher risk than women with increasing exposure to physical stressors, although women have a higher background risk. This may mean that other factors have a greater effect on women in low-exposure jobs and are less important when there is high physical loading, or because women with higher occupational exposures (physi- cal and/or psychosocial) are more likely than men to leave em- ployment or change jobs due to work-related MSDs. In contrast, the sparse literature suggests that women may both experience different levels of job strain and have increased vulnerability to similar levels of job strain compared with men, possibly be- cause of the added demands of household responsibilities. All of these explanations remain tentative at present and require further study.
Despite the widespread belief that MSDs disproportionately affect women, the outcomes of these conditions have been ex- amined primarily among men. In order to tailor rational inter- ventions for primary or secondary prevention of disability, further study of the prognostic factors among women is an im- portant research priority.
Analysis of gender as a "risk factor" for MSDs, or adjusting for gender differences, does not elucidate these issues. Future epidemiologic studies of MSDs should include subjects of both genders to avoid unnecessary constraints on the available ex- posure contrasts. The associations of musculoskeletal disorders with gender and occupational ergonomic exposures should be assessed separately in order to determine whether women are at increased risk when exposed to the same ergonomic stressors as men. Gender-stratified presentation of data is valuable because it permits examination, rather than smoothing over, of differ- ences in the exposure-response relationships.
Acknowledgments
Rachel Kidman, for her assistance in compiling and managing the literature search; Karen Messing, for her insightful reading and synthe- sis of the literature; Ulf Bergqvist, Jeff Katz, ,~sa Kilbom, Letitita Davis and Helen Wellman for discussions with LP about these issues.
References
1. Gerr, F., Letz, R., and Landrigan, P. J. (1991). Upper-extremity musculoskeletal disorders of occupational origin. Ann. Rev. Public
Health 12, 543-566. 2. Hagberg, M. (1994). Neck and shoulder disorders. In "Textbook
of Occupational and Environmental Medicine" (L. Rosenstock and M. R. Cullen, eds.), pp. 356-364. Saunders, Philadelphia.
3. Pope, M. H., Andersson, G. B. J., Frymoyer, J. W., and Chaffin, D. B., eds. (1991). "Occupational Low Back Pain: Assessment, Treatment and Prevention," Mosby, St. Louis, MO.
4. Rempel, D. M., Harrison, R. J., and Barnhart, S. (1992). Work- related cumulative trauma disorders of the upper extremity. JAMA,
J. Am. Med. Assoc. 267, 838-842. 5. RiihimLki, H. (1995). Back and limb disorders. In "Epidemiology
of Work Related Diseases" (C. McDonald, ed.), pp. 207-238. BMJ Publishing Group, London.
6. Bernard, B. P., ed. (1997). "Musculoskeletal Disorders and Work- place Factors: A Critical Review of Epidemiologic Evidence for Work-related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back." U.S. Department of Health and Hu- man Services, National Institute for Occupational Safety and Health, Cincinnati, OH.
7. Maetzel, A., Makel~i, M., Hawker, G., and Bombardier, C. (1997). Osteoarthritis of the hip and knee and mechanical occupational exposure--a systematic overview of the evidence. J. Rheum. 24, 1599-1607.
8. Agency for Health Care Policy and Research (1994). "Clini- cal Practice Guideline: Acute Low Back Problems in Adults." U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research, Rockville, MD.
9. Rempel, D., Evanoff, B., Amadio, P. C. et al. (1998). Consensus criteria for the classification of carpal tunnel syndrome in epide- miologic studies. Am. J. Public Health 88, 1447-1451.
10. Badley, E. M., and Ibafiez, D. (1994). Socioeconomic risk factors and musculoskeletal disability. J. Rheum. 21, 515-522.
11. Rempel, D. M., and Punnett, L. (1997). Epidemiology of wrist and hand disorders. In "Musculoskeletal Disorders in the Workplace: Principles and Practice" (M. Nordin, G. B. Andersson, and M. H. Pope, eds.), pp. 421-430. Mosby, Philadelphia.
12. Yelin, E., Callahan, L. E, and National Arthritis Data Work Group (1995). The economic cost and social and psychological impact of musculoskeletal conditions. Arthritis Rheum. 38, 1351-1367.
13. SjCgaard, G., Sejersted, O. M., Winkel, J., Smolander, J., Jcrgensen, K. and Westgaard, R. H. (1993). Exposure assess- ment and mechanisms of pathogenesis in work-related musculo- skeletal disorders: Significant aspects in the documentation of risk factors. In "Work and Health: Scientific Basis of Progress in the Working Environment" (O. Svane and C. Johansen, eds.), pp. 75-87. European Commission, Directorate-General V, Em- ployment, Industrial Relations and Social Affairs, Copenhagen, Denmark.
14. Bureau of Labor Statistics (1996). "Occupational Injuries and Ill- nesses: Counts, Rates, and Characteristics, 1993." U. S. Depart- ment of Labor, Bureau of Labor Statistics, Washington, DC.
15. Westgaard, R. H., and Winkel, J. (1997). Ergonomic intervention research for improved musculoskeletal health: A critical review. Int. J. Ind. Ergonomics 20, 463-500.

C H A P T E R 38. W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 487
16. Cummings, K., Maizlish, N., Rudolph, L., Dervin, K., and Ervin, A. (1989). Occupational disease surveillance: Carpal tunnel syn- drome. Morbid. Mortal. Wkly. Rep. 38, 485-489.
17. Tanaka, S., Wild, D. K., Seligman, P. J., Halperin, W. E., Behrens, V. J., and Putz-Anderson, V. (1995). Prevalence and work- relatedness of self-reported carpal tunnel syndrome among U.S. workers: Analysis of the Occupational Health Supplement data of 1988 National Health Interview Survey. Am. J. Ind. Med. 27, 451-470.
18. Brogmus, G. E., Sorock, G. S., and Webster, B. S. (1996). Recent trends in work-related cumulative trauma disorders of the upper extremities in the United States: An evaluation of possible rea- sons. J. Occup. Environ. Med. 38, 401.
19. Franklin, G. M., Haug, J., Heyer, N., Checkoway, H., and Peck, N. (1991). Occupational carpal tunnel syndrome in Washington State, 1984-1988. Am. J. Public Health 81, 741-746.
20. Webster, B. S., and Snook, S. H. (1994). The cost of compensable upper extremity cumulative trauma disorders. J. Occup. Med. 36, 713-717.
21. Webster, B. S., and Snook, S. H. (1994). The cost of 1989 work- ers' compensation low back pain claims. Spine 19, 1111-1116.
22. Fine, L. J., Silverstein, B. A., Armstrong, T. J., Anderson, C. A., and Sugano, D. S. (1986). Detection of cumulative trauma disor- ders of upper extremities in the workplace. J. Occup. Med. 28, 674-678.
23. Nelson, N. A., Park, R. M., Silverstein, M. A., and Mirer, F. E. (1992). Cumulative trauma disorders of the hand and wrist in the auto industry.Am. J. Public Health 82, 1550-1552.
24. Leigh, J. P., Markowitz, S. B., Fahs, M., Shin, C., and Landrigan, P. J. (1997). Occupational injury and illness in the United States: Estimates of costs, morbidity and mortality. Arch. Intern. Med. 157, 1557-1568.
25. Oxenburgh, M. S. (1991). "Increasing Productivity and Profit through Health and Safety." Commerce Clearing House, Chicago.
26. Adams, M. L., Franklin, G. M., and Barnhart, S. (1994). Outcome of carpal tunnel surgery in Washington State workers' compensa- tion. Am. J. Ind. Med. 25, 527-536.
27. Bigos, S. J., Battir, M. C., Spengler, D. M., Fisher, L. D., Fordyce, W. E., Hansson, T. H., Nachemson, A. L., and Wortley, M. D. (1991). A prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine 16, 1-6.
28. Burdorf, A., Naaktgeboren, B., and Post, W. (1998). Prognostic factors for musculoskeletal sickness absence and return to work among welders and metal workers. Occup. Environ. Med. 55, 490-495.
29. Cotton, P. (1991). Symptoms may return after carpal tunnel sur- gery. JAMA, J. Am. Med. Assoc. 265, 1922-1925.
30. Ekberg, K., and Wildhagen, I. (1996). Long-term sickness absence due to musculoskeletal disorders: The necessary intervention of work conditions. Scand. J. Rehabil. Med. 28, 39-47.
31. Frymoyer, J. W. (1992). Predicting disability from low back pain. Clin. Orthop. Relat. Res. 279, 101-109.
32. Kulick, M. I., Gordillo, G., Javidi, T., Kilgore, E. S., and Newmeyer, W. L. (1986). Longterm analysis of patients having surgical treat- ment for carpal tunnel syndrome. J. Hand Surg. l lA, 59-66.
33. Leavitt, E (1992). The physical exertion factor in compensable work injuries: A hidden flaw in previous research. Spine 17, 307-310.
34. Nathan, P. A., Meadows, K. D., and Keniston, R. C. (1993). Re- habilitation of carpal tunnel surgery patients using a short surgical incision and an early program of physical therapy. J. Hand Surg. 18A, 1044-1050.
35. Walsh, N. E., and Dumitru, D. (1988). The influence of compen- sation on recovery from low back pain. Occup. Med.: State of the Art Revs. 3, 109-121.
36. Baldwin, M. L., Johnson, W. G., and Butler, R. J. (1996). The error of using return to work to measure the outcomes of health care. Am. J. Ind. Med. 29, 632-641.
37. Reid, J., Ewan, C., and Lowy, E. (1991). Pilgrimage of pain: The illness experiences of women with repetition strain injury and the search for credibility. Soc. Sci. Med. 32, 601-612. �9
38. Verbrugge, L. M., and Ascione, E J. (1987). Exploring the ice- berg: Common symptoms and how people care for them. Med.
Care 25, 539-569. 39. Pransky, G., and Himmelstein, J. (1996). Outcomes research: Im-
plications for occupational health. Am. J. Ind. Med. 29, 573-583. 40. Strunin, L. (1997). The human costs of occupational injuries. In
"National Occupational Injury Research Symposium". NIOSH, Morgantown, WV.
41. Armstrong, T. J., Buckle, P., Fine, L. J. et al. (1993). A conceptual model for work-related neck and upper-limb musculoskeletal dis- orders. Scand. J. Work Environ. Health 19, 73-84.
42. Gordon, S. L., Fine, L. J. and Blair, S., eds. (1995). "Repetitive Motion Disorders of the Upper Extremity." American Academy of Orthopedic Surgeons, Rosemont, IL.
43. Armstrong, T. J., Fine, L. J., Goldstein, S. A., and Silverstein, B. A. (1987). Ergonomics considerations in hand and wrist tendi- nitis. J. Hand Surg. 12A (2, Pt. 2), 830-837.
44. Goldstein, S. A., Armstrong, T. J., Chaffin, D. B. et al. (1987). Analysis of cumulative strain in tendons and tendon sheaths. J. Biomech. 20, 1-6.
45. Hagberg, M., Silverstein, B., Wells, R., Smith, R., Carayon, P., Hendrick, H., Perusse, M., Kuorinka, I., and Forcier, L., eds. (1995). "Work-related Musculoskeletal Disorders (WMSD): A Handbook for Prevention." Taylor & Francis, London.
46. Karasek, R. A., and Theorell, T. (1990). "Healthy Work. Stress, Productivity and the Reconstruction of Working Life." Basic Books, New York.
47. Schwartz, J. E., Picketing, T. G., and Landsbergis, E A. (1996). Work-related stress and blood pressure: Current theoretical mod- els and considerations from a behavioral medicine perspective. J. Occup. Health Psychol. 1, 287-310.
48. Wa~rsted, M., Bjrrklund, R. A., and Westgaard, R. H. (1991). Shoulder muscle tension induced by two VDU-based tasks of dif- ferent complexity. Ergonomics 34, 137-150.
49. Westgaard, R. H., and BjiSrklund, R. (1987). Generation of muscle tension additional to postural muscle load. Ergonomics 30, 911-923.
50. Leino, E I., and H~inninen, V. (1995). Psychosocial factors at work in relation to back and limb disorders. Scand. J. Work Environ.
Health 21, 134-142. 51. Bongers, E M., de Winter, C. R., Kompier, M. A. J., and Hilde-
brandt, V. H. (1993). Psychosocial factors at work and musculo- skeletal disease. Scand. J. Work Environ. Health 19, 297-312.
52. Blanc, E D., Faucett, J., Kennedy, J. J., Cisternas, M., and Yelin, E. (1996). Self-reported carpal tunnel syndrome: Predictors of work disability from the National Health Interview Survey Occu- pational Health Supplement. Am. J. Ind. Med. 30, 362-368.
53. Chrubasik, S., Junck, H., Zappe, H. A., and Stutzke, O. (1998). A survey on pain complaints and health care utilization in a German population sample. Eur. J. Anaesthesiol. 15, 397-408.
54. Cunningham, L. S., and Kelsey, J. L. (1984). Epidemiology of musculoskeletal impairments and associated disability. Am. J.
Public Health 74, 574-579. 55. de Krom, M. C. T. E M., Kester, A. D. M., Knipschild, E G., and
Spaans, E (1990). Risk factors for carpal tunnel syndrome. Am. J.
Epidemiol. 132, 1102-1110. 56. de Zwart, B. C. H., Broersen, J. P. J., Frings-Dresen, M. H. W.,
and van Dijk, E J. H. (1997). Musculoskeletal complaints in the Netherlands in relation to age, gender and physically demanding work. Int. Arch. Occup. Environ. Health 70, 352-360.

488 S E C T I O N 6 - - W O M E N AT W O R K
57. Derriennic, E, Iwatsubo, Y., Monfort, C., and Cassou, B. (1993). Evolution of osteoarticular disorders as a function of past heavy physical work factors: Longitudinal analysis of 627 retired sub- jects living in the Paris area. Br. J. Ind. Med. 50, 851-860.
58. English, C. J., Maclaren, W. M., Court-Brown, C., Hughes, S. P. F., Porter, R. W., Wallace, W. A., Graves, R. J., Pethick, A. J., and Soutar, C. A. (1995). Relations between upper limb soft tissue disorders and repetitive movements at work. Am. J. Ind. Med. 27, 75-90.
59. Houtman, I. L. D., Bongers, P. M., Smulders, P. G. W., and Kompier, M. A. J. (1994). Psychosocial stressors at work and musculoskeletal problems. Scand. J. Work Environ. Health 20, 139-145.
60. MLkel~i, M., Heli6vaara, M., Sievers, K., Impivaara, O., Knekt, P., and Aromaa, A. (1991). Prevalence, determinants, and conse- quences of chronic neck pain in Finland. Am. J. Epidemiol. 134, 1356-1367.
61. Petersson, C. J. (1983). Degeneration of the gleno-humeral joint. Acta Orthop. Scand. 54, 277-283.
62. Praemer, A., Furner, S., and Rice, D. P. (1992). "Musculoskeletal Conditions in the United States." Academy of Orthopaedic Sur- geons, Park Ridge, IL.
63. Stevens, J. C., Sun, S., Beard, C. M., O'Fallon, W. M., and Kur- land, L. T. (1988). Carpal tunnel syndrome in Rochester, Minne- sota, 1961 to 1980. Neurology 38, 134-138.
64. Viikari-Juntura, E., Vuori, J., Silverstein, B. A., Kalimo, R., Kuosma, E., and Videman, T. (1991). A life-long prospective study on the role of psychosocial factors in neck-shoulder and low-back pain. Spine 16, 1056-1061.
65. Burchfiel, C. M., Boice, J. A., Stafford, B. A., and Bond, G. G. (1992). Prevalence of back pain and joint problems in a manufac- turing company. J. Occup. Med. 34, 129-134.
66. Carey, T., Evans, A., Hadler, N., Lieberman, G., Kalsbeek, W., Jackman, A., Fryer, J., and McNutt, R. (1996). Acute severe low back pain: A population-based study of prevalence and care- seeking. Spine 21, 339-344.
67. Kujala, U. M., Taimela, S., Viljanen, T., Jutila, H., Viitasalo, J. T., Videman, T., and Batti6, M. C. (1996). Physical loading and per- formance as predictors of back pain in healthy adults: A 5-year prospective study. Eur. J. Appl. Physiol. 73, 452-458.
68. Manninen, P., Riihimaki, H., and Heli6vaara, M. (1996). Has mus- culoskeletal pain become less prevalent? Scand. J. Rheumatol. 25, 37-41.
69. Andersen, J. H., and Gaardboe, O. (1993). Prevalence of persistent neck and upper limb pain in a historical cohort of sewing machine workers. Am. J. Ind. Med. 24, 677-687.
70. Brisson, C., Vinet, A., and Vezina, M. (1989). Disability among female garment workers: A comparison with a national sample. Scand. J. Work Environ. Health 15, 323-328.
71. Leclerc, A., Franchi, P., Cristofari, M. E, Delemotte, B., Mereau, P., Teyssier-Cotte, C., Touranchet, A., and Study Group on Repet- itive Work (1998). Carpal tunnel syndrome and work organisation in repetitive work: A cross sectional study in France. Occup. En- viron. Med. 55, 180-187.
72. Punnett, L., Robins, J. M., Wegman, D. H., and Keyserling, W. M. (1985). Soft tissue disorders in the upper limbs of female garment workers. Scand. J. Work Environ. Health 11, 417-425.
73. Schibye, B., Skov, T., Ekner, D., Christiansen, J. U., and Sjcgaard, G. (1995). Musculoskeletal symptoms among sewing machine op- erators. Scand. J. Work Environ. Health 21, 427-434.
74. Andersen, J. H., and Gaardboe, O. (1993). Musculoskeletal dis- orders of the neck and upper limb pain among sewing machine operators: A clinical investigation. Am. J. Ind. Med. 24, 689-700.
75. Blhder, S., Barck-Holst, U., Danielsson, S., Ferhm, E., Kalpamaa, M., Leijon, M., Lindh, M., and Markhede, G. (1991). Neck and
shoulder complaints among sewing-machine operators: A study concerning frequency, symptomatology and dysfunction. Appl. Ergonomics 22, 251-257.
76. Brisson, C., Vinet, A., Vezina, M., and Gingras, S. (1989). Effect of duration of employment in piecework on severe disability among female garment workers. Scand. J. Work Environ. Health 15, 329-334.
77. Punnett, L. (1996). Adjusting for the healthy worker selection effect in cross-sectional studies. Int. J. Epidemiol. 25,1068-1075; 26, 914.
78. Luopaj~irvi, T., Kuorinka, I., Virolainen, M., and Holmberg, M. (1979). Prevalence of tenosynovitis and other injuries of the upper extremities in repetitive work. Scand. J. Work Environ. Health 5(Suppl. 3), 48-55.
79. Hadler, N. M., Gillings, D. B., Imbus, H. R., Levitin, P. M., Makuc, D., Utsinger, P. D., Yount, W. J., Slusser, D., and Moskov- itz, N. (1978). Hand structure and function in an industrial setting. Influence of three patterns of stereotyped repetitive usage. Arthri- tis Rheum. 21, 210-220.
80. Koskela, R.-S., Klockars, M., and J~_rvinen, E. (1990). Mortality and disability among cotton mill workers. Br. J. Ind. Med. 47, 384-391.
81. Kilbom, A., Persson, J., and Jonsson, B. G. (1986). Disorders of the cervicobrachial region among female workers in the electron- ics industry. Int. J. Ind. Ergonomics 1, 37-47.
82. Jonsson, B. G., Persson, J., and Kilbom, .~. (1988). Disorders of the cervicobrachial region among female workers in the electronics industry: A two-year follow up. Int. J. Ind. Ergonomics 3, 1-12.
83. Ohlsson, K., Attewell, R., and Skerfving, S. (1989). Self-reported symptoms in the neck and upper limbs of female assembly work- ers: Impact of length of employment, work pace, and selection. Scand. J. Work Environ. Health 15, 75-80.
84. Schottland, J. R., Kirschberg, G. J., Fillingim, R., Davis, V. P., and Hogg, E (1991). Median nerve latencies in poultry processing workers: An approach to resolving the role of industrial "cumu- lative trauma" in the development of carpal tunnel syndrome. J. Occup. Med. 33, 627-631.
85. Hales, T. R., and Fine, L. J. (1989). "Health Hazard Evaluation Report: Cargill Poultry Division, Buena Vista GA." National In- stitute for Occupational Safety and Health, Cincinnati, OH.
86. Chiang, H.-C., Ko, Y.-C., Chen, S.-S., Yu, H.-S., Wu, T. N., and Chang, P.-Y. (1993). Prevalence of shoulder and upper-limb dis- orders among workers in the fish-processing industry. Scand. J. Work Environ. Health 19, 126-131.
87. Messing, K., and Reveret, J. P. (1983). Are women in female jobs for their health? A study of working conditions and health effects in the fish-processing industry in Quebec. Int. J. Health Serv. 13, 635-647.
88. Ohlsson, K., Hansson, G., Balogh, I., StrOmberg, U., Phlsson, B., Nordander, C. et al. (1994). Disorders of the neck and upper limbs in women in the fish processing industry. Occup. Environ. Med. 51, 826-832.
89. Olafsd6ttir, H., and Rafnsson, V. (1995). New technique increases the prevalence of musculoskeletal symptoms from upper limbs among women in fish fillet plants. "2nd International Scientific Conference on Prevention of Work-Related Musculoskeletal Dis- orders (PREMUS 95)." Montr6al, Qu6bec.
90. Ahlberg-Hult6n, G. K., Theorell, T., and Sigala, E (1995). Social support, job strain and musculoskeletal pain among female health care personnel. Scand. J. Work Environ. Health 21, 435-439.
91. Engkvist, I.-L., Hagberg, M., Lind6n, A., and Malker, B. (1992). Over-exertion back accidents among nurses' aides in Sweden. Saf Sci 15, 97-108.
92. Estryn Behar, M., Kaminski, M., Peigne, E., Maillard, M. E, Pelletier, A., Berthier, C. et al. (1990). Strenuous working condi-

C H A P T E R 38. W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 489
tions and musculo-skeletal disorders among female hospital work- ers. Int. Arch. Occup. Environ. Health 62, 47-57.
93. Jensen, R. C. (1990). Back injuries among nursing personnel re- lated to exposure. Appl. Occup. Environ. Hyg. 5, 38-45.
94. Ono, Y., Lagerstrrm, M., Hagberg, M., Lindrn, A., and Malker, B. (1995). Reports of work related musculoskeletal injury among home care service workers compared with nursery school workers and the general population of employed women in Sweden. Oc- cup. Environ. Med. 52, 686-693.
95. Punnett, L. (1987). Upper extremity musculoskeletal disorders in hospital workers. J. Hand Surg. 12A(2. Pt. 2), 858-862.
96. Osorio, A. M., Ames, R. G., Jones, J., Castorina, J., Rempel, D., Estrin, W. et al. (1994). Carpal tunnel syndrome among grocery store workers. Am. J. Ind. Med. 25, 229-245.
97. Vrzina, N., Geoffrion, L., Chatigny, C., and Messing, K. (1994). A manual materials handling job: Symptoms and working condi- tions among supermarket cashiers. Chron. Dis. Can. 15, 17-22.
98. Morgenstern, H., Kelsh, M., Kraus, J., and Margolis, W. (1991). A cross-sectional study of hand/wrist symptoms in female grocery checkers. Am. J. Ind. Med. 20, 209-218.
99. Messing, K., Chatigny, C., and Courville, J. (1998). 'Light' and 'heavy' work in the housekeeping service of a hospital. Appl. Ergonomics 29, 451-459.
100. Pierre-Jerome, C., Bekkelund, S. I., Mellgren, S. I., and Torbergsen, T. (1996). Quantitative magnetic resonance imaging and the elec- trophysiology of the carpal tunnel region in floor cleaners. Scand. J. Work Environ. Health 22, 119-123.
101. Stock, S. R. (1995). A study of musculoskeletal symptoms in day- care workers. In "Invisible: Issues in Women's Occupational Health/Invisible: La sant6 des travailleuses" (K. Messing, B. Neis, and L. Dumais, eds.), pp. 62-74. Gynergy Books, Charlottetown, Quebec Canada.
102. Ono, Y., Nakamura, R., Shimaoka, M., Hiruta, S., Hattori, Y., Ichihara, G., Kamijima, M., and Takeuchi, Y. (1998). Epicondyli- tis among cooks in nursery schools. Occ. Environ. Med. 55, 172-179.
103. Camerino, D., Lavano, P., Ferrario, M., Ferretti, G., and Molteni, G. (1995). Musculoskeletal disorders, working posture, psycho- social environment in female VDU operators and conventional office workers. In "Work with Display Units 94. Selected Papers of the Fourth International Scientific Conference on Work with Display Units, Milan, Italy, 2-5 October, 1994" (A. Grieco, G. Molteni, B. Piccoli, and E. Occhipinti, eds.), pp. 67-72. Elsevier, Amsterdam.
104. Marcus, M., and Gerr, E (1996). Upper extremity musculoskeletal symptoms among female office workers: Associations with video display terminal use and occupational psychosocial stressors. Am. J. Ind. Med. 29, 161-170.
105. Murata, K., Araki, S., Okajima, E, and Saito, Y. (1996). Subclini- cal impairment in the median nerve across the carpal tunnel among female VDT operators. Int. Arch. Occup. Environ. Health 68, 75-79.
106. Stellman, J., Klitzman, S., Gordon, G. C., and Snow, B. R. (1987). Work environment and the well-being of clerical and VDT work- ers. J. Occup. Behav. 8, 95-114.
107. Sauter, S. L., Schleiffer, L. M., and Knutson, S. J. (1991). Work posture, workstation design, and musculoskeletal discomfort in a VDT data entry task. Hum. Factors 33, 151-167.
108. Oxenburgh, M. S. (1987). Musculoskeletal injuries occurring in word processor operators. In "Readings in RSI: The Ergonomic Approach to Repetition Strain Injuries" (M. Stevenson, ed.), pp. 91-95. New South Wales University Press, Kensington, NSW, Australia.
109. Ferreira, J. M., Conceicao, G. M., and Saldiva, P. H. (1997). Work organization is significantly associated with upper extremities
musculoskeletal disorders among employees engaged in interac- tive computer-telephone tasks of an international bank subsidiary in Sao Paulo, Brazil. Am. J. Ind. Med. 31, 468-473.
110. Punnett, L. (1998). Ergonomic stressors and upper extremity disorders in vehicle manufacturing: Cross-sectional exposure- response trends. Occup. Environ. Med. 55, 414-420.
111. Schierhout, G. H., Myers, J. E., and Bridger, R. S. (1993). Mus- culoskeletal pain and workplace ergonomic stressors in manufac- turing industry in South Africa. Int. J. Ind. Ergonomics 12, 3-11.
112. Bergqvist, U., Wolgast, E., Nilsson, B., and Voss, M. (1995). Mus- culoskeletal disorders among visual display terminal workers; in- dividual, ergonomic and work organizational factors. Ergonomics 38, 763-776.
113. Bernard, B. P., Sauter, S., Fine, L. J., Petersen, M., and Hales, T. (1994). Job task and psychosocial risk factors for work-related musculoskeletal disorders among newspaper employees. Scand. J. Work Environ. Health 20, 417-426.
114. Hales, T. R., Sauter, S. L., Peterson, M. R., Putz-Anderson, V., Fine, L. J., Ochs, T. T., Schleifer, L. R., and Bernard, B. P. (1992). "Health Hazard Evaluation Report: U.S. West Communications, Phoenix AZ, Minneapolis/St Paul MN, Denver CO." National Institute for Occupational Safety and Health, Cincinnati, OH.
115. McCormack, R. R., Inman, R. D., Wells, A., Berntsen, C., and Imbus, H. R. (1990). Prevalence of tendinitis and related disorders of the upper extremity in a manufacturing workforce. J. Rheum. 17, 958-964.
116. Viikari-Juntura, E. (1983). Neck and upper limb disorders among slaughterhouse workers. Scand. J. Work Environ. Health 9, 283-290.
117. Silverstein, B. A., Fine, L. J., and Armstrong, T. J. (1986). Hand wrist cumulative trauma disorders in industry. Br. J. Ind. Med. 43, 779-784.
118. Silverstein, B. A., Fine, L. J., and Armstrong, T. J. (1987). Occu- pational factors and carpal tunnel syndrome. Am. J. Ind. Med. 11, 343-358.
119. Nathan, P. A., Keniston, R. C., Myers, L. D., and Meadows, K. D. (1992). Longitudinal study of median nerve sensory conduction in industry: Relationship to age, gender, hand dominance, occupational hand use, and clinical diagnosis. J. Hand Surg. 17A, 850-857.
120. Ekberg, K., Bjrrkqvist, B., Maim, P. et al. (1994). Case-control study of risk factors for disease in the neck and shoulder area. Occup. Environ. Med. 51, 262-266.
121. Park, R. M., Krebs, J. M. and Mirer, E E. (1996). Occupational disease surveillance using disability insurance at an automotive stamping and assembly complex. J. Occup. Environ. Med. 38, 1111-23.
122. Park, R. M., Nelson, N. A., Silverstein, M. A., and Mirer, E E. (1992). Use of medical insurance claims for surveillance of occu- pational disease: An analysis of cumulative trauma in the auto industry. J. Occup. Med. 34, 731-737.
123. Cheadle, A., Franklin, G., Wolfhagen, C., Savarino, J., Liu, E Y., Salley, C., and Weaver, M. (1994). Factors influencing the dura- tion of work-related disability: A population-based study of Wash- ington State workers' compensation. Am. J. Public Health 84.
124. Feeney, A., North, E, Head, J., Canner, R., and Marmot, M. (1998). Socioeconomic and sex differentials in reason for sickness absence from the Whitehall II study. Occup. Environ. Med. 55, 91-98.
125. Feuerstein, M., Berkowitz, S. M., and Peck, C. A. (1997). Musculoskeletal-related disability in U.S. army personnel: Preva- lence, gender, and military occupational specialties. J. Occup. Environ. Med. 39, 68-78.
126. Hashemi, L., Webster, B. S., Clancy, E. A., and Courtney, T. K. (1998). Length of disability and cost of work-related musculo- skeletal disorders of the upper extremity. J. Occup. Environ. Med. 40, 261-269.

490 S E C T I O N 6 - - W O M E N AT W O R K
127. Katz, J. N., Keller, R. B., Fossel, A. H., Punnett, L., Bessette, L., Simmons, B. P., and Mooney, N. (1997). Predictors of return to work following carpal tunnel release. Am. J. Ind. Med. 31, 85-91.
128. Brage, S., Nyg~d, J. F., and Tellnes, G. (1998). The gender gap in musculoskeletal-related long term sickness absence in Norway. Scand. J. Soc. Med. 26, 34-43.
129. Jensen, I. B., Nygren, A., and Lundin, A. (1994). Cognitive- behavioural treatment for workers with chronic spinal pain: a matched and controlled cohort study in Sweden. Occup. Environ. Med. 51, 145-151.
130. Yelin, E., Nevitt, M., and Epstein, W. (1980). Toward an epidemi- ology of work disability. Epidemiol. Work Disabil. 58, 386-415.
131. Levenstein, C. (1999). Economic losses from repetitive strain in- juries. In "Occupational Medicine: State of the Art Reviews" (M. Cherniack, ed.), pp. 149-161. Hanley & Belfus, Philadelphia.
132. Dembe, A. E. (1997). The history of carpal tunnel syndrome. New Solutions 7, 15-22.
133. Torg6n, M., and Kilbom, A. (1997). The REBUS study: Physical work load between 18 and 58 years of age--does it change? In "Proceedings of the 13th Triennial Congress of the International Ergonomics Association," pp. 544-546. Finnish Institute of Oc- cupational Health, Tampere, Finland.
134. Torg6n, M., Fredriksson, K., B ildt Thorbj6rnsson, C., Alfredsson, L., Ving~d, E., and Kilbom, ~,. (1998). Age in relation to physical and psychosocial exposures, physical capacity and health in 484 Swedish middle-aged men and women: The REBUS study. In "Second International ICOH Conference on Aging and Workw Work Ability of Elderly Workers: A Challenge for Occupational Health," p. 17. The Danish Working Environment Fund, Elsinore, Denmark.
135. Barnhart, S., Demers, P. A., Miller, M., Longstreth, W. T. J., and Rosenstock, L. (1991). Carpal tunnel syndrome among ski manu- facturing workers. Scand. J. Work Environ. Health 17, 46-52.
136. Courville, J., Dumais, L., and V6zina, N. (1994). Conditions de travail de femmes et d'hommes sur une cha~ne de d6coupe de volaille et d6veloppement d'atteintes musculo-squelettiques (Work- ing conditions and development of musculoskeletal disorders among women and men on a poultry cutting line). Trav. Santg 10, S17-$23.
137. Fransson Hall, C., Bystr6m, S., and Kilbom, A. (1995). Self- reported physical exposure and musculoskeletal symptoms of the forearm-hand among automobile assembly line workers. J. Occup. Environ. Med. 37, 1136-1144.
138. Kiken, S., Stringer, W., Fine, L., Sinks, T., and Tanaka, S. (1990). "Health Hazard Evaluation Report: Perdue Farms, Inc., Lewiston NC, Roberson NC." National Institute for Occupational Safety and Health, Cincinnati, OH.
139. Mergler, D., Brabant, C., V6zina, N., and Messing, K. (1987). The weaker sex? Men in women's working conditions report similar health symptoms. J. Occup. Med. 29, 417-421.
140. Evans, J. (1987). Women, men, VDU work and health: a question- naire survey of British VDU operators. Work Stress 1, 271-283.
141. Messing, K., Dumais, L., Courville, J., Seifert, A. M., and Boucher, M. (1994). Evaluation of exposure data from men and women with the same job title. J. Occup. Med. 36, 913-917.
142. Messing, K., Tissot, E, Saurel-Cubizolles, M., Kaminski, M., and Bourgine, M. (1998). Sex as a variable can be a surrogate for some working conditions. J. Occup. Environ. Med. 40, 250-260.
143. Hall, E. M. (1990). "Women's Work: An Inquiry into the Health Effects of Invisible and Visible Labor." Ph.D. thesis, Division of Behavioral Sciences and Health Education, Health Policy and Management Department, John Hopkins University School of Hy- giene and Public Health, Baltimore, Maryland; and Karolinska Institute, Stockholm.
144. Roxburg, S. (1996). Gender differences in work and well-being: Effects of exposure and vulnerability. J. Health Soc. Behav. 37, 265-277.
145. Zetterberg, C., Forsberg, A., Hansson, E., Johansson, H., Nielsen, P., Danielsson, B., Inge, G., and Olsson, B.-M. (1997). Neck and upper extremity problems in car assembly workers: A comparison of subjective complaints, work satisfaction, physical examination and gender. Int. J. Ind. Ergonomics 19, 277-289.
146. Martin, B. J., Armstrong, T. J., Foulke, J. A., Natarajan, S., Klinenberg, E., Serina, E., and Rempel, D. (1996). Keyboard re- action force and finger flexor electromyograms during computer keyboard work. Hum. Factors 38, 654-664.
147. Sjcgaard, G., and Scgaard, K. (1998). Muscle injury in repetitive motion disorders. Clin. Orthop. Relat. Res. 351, 21-31.
148. Chaffin, D. B., and Andersson, G. B. J. (1991). "Occupational Biomechanics." Wiley, New York.
149. Chatigny, C., Seifert, A. M., and Messing, K. (1995). Repetitive strain in nonrepetitive work: A case study. Int. J. Occup. Saf
Ergonomics 1, 42-51. 150. Courville, J., V6zina, N., and Messing, K. (1991). Comparison of
the work activity of two mechanics: A woman and a man. Int. J.
Ind. Ergonomics 7, 163-174. 151. Courville, J., V6zina, N., and Messing, K. (1992). Analyse des
facteurs pouvant entra~ner l'exclusion des femmes du tri des colis postaux (Ergonomic factors which may exclude women from package sorting jobs). Trav. Hum. 55, 119-134.
152. Goldenhar, L. M., and Sweeney, M. H. (1996). Tradeswomen's perspectives on occupational health and safety: A qualitative in- vestigation. Am. J. Ind. Med. 29, 516-520.
153. Green, R. A., and Briggs, C. A. (1989). Anthropometric dimen- sions and overuse injury among Australian keyboard operators. J. Occup. Med. 31, 747-750.
154. Messing, K., Courville, J., Boucher, M., Dumais, L., and Seifert, A. M. (1994). Can safety risks of blue-collar jobs be compared by gender? Saf. Sci. 18, 95-112.
155. Stevenson, J. M., Greenhorn, D. R., Bryant, J. T., Deakin, J. M., and Smith, J. T. (1996). Gender differences in performance of a selection test using the incremental lifting machine. Appl. Ergon-
omics 27, 45-52. 156. Alexanderson, K., Leijon, M.,/~kerlind, I., Rydh, H., and Bjurulf,
P. (1994). Epidemiology of sickness absence in a Swedish county in 1985, 1986 and 1987. Scand. J. Soc. Med. 22, 27-34.
157. Leijon, M., Hensing, G., and Alexanderson, K. (1999). Sickness absence due to musculoskeletal disorders in different occupational groups--the role of gender segregation. Eur. J. Public Health (to be published).
158. Bystr6m, S., Fransson Hall, C., Welander, T., and Kilbom, A. (1995). Clinical disorders and pressure-pain threshold of the fore- arm and hand among automobile assembly line workers. J. Hand
Surg. (Br. Eur. Vol.) 20B, 782-90. 159. Bildt ThorbjOrnsson, C. O., Alfredsson, L., Fredriksson, K., KiSster,
M., Mich61sen, H., Vinggtrd, E., Torg6n, M., and Kilbom, A. (1998). Psychosocial and physical risk factors associated with low back pain: A 24 year follow up among women and men in a broad range of occupations. Occup. Environ. Med. 55, 84-90.
160. Macfarlane, G. J., Thomas, E., Papageorgiou, A. C., Croft, P. R., Jayson, M. I. V., and Silman, A. J. (1997). Employment and phys- ical work activities as predictors of future low back pain. Spine
22, 1143-1149. 161. Felson, D. T., Hannan, M. T., Naimark, A., Berkeley, J., Gordon,
G., Wilson, P. W. E, and Anderson, J. (1991). Occupational phys- ical demands, knee bending, and knee osteoarthritis: Results from the Framingham Study. J. Rheum. 18, 1587-1592.
162. Anderson, J. J., and Felson, D. (1988). Factors associated with OA of the knee in the first HANES. Am. J. Epidemiol. 128, 179-189.

C H A P T E R 3 8 . W O R K - R E L A T E D M U S C U L O S K E L E T A L D I S O R D E R S 491
163. Imeokparia, R. L., Barrett, J. P., Arrietta, M. I., Leaverton, P. E., Wilson, A. A., Hall, B. J., and Marlowe, S. M. (1994). Physical activity as a risk factor for osteoarthritis of the knee. Ann. Epide- miol. 4, 221-230.
164. Bergqvist, U. (1995). Visual display terminal work--a perspec- tive on long-term changes and discomforts. Int. J. Ind. Ergonom- ics 16, 201-209.
165. Nelson, N. A., and Silverstein, B. A. (1998). Workplace changes associated with a reduction in musculoskeletal symptoms in office workers. Hum. Factors 40, 337-350.
166. Leino, P. I., Hasan, J., and Karppi, S. L. (1988). Occupational class, physical workload, and musculoskeletal morbidity in the engineering industry. Br. J. Ind. Med. 45, 672-681.
167. Punnett, L. (1997). Upper extremity disorders among male and female automotive manufacturing workers. In "Proceedings of the 13th Triennial Congress of the International Ergonomics Associ- ation," pp. 512-514. Finnish Institute of Occupational Health, Tampere, Finland.
168. Punnett, L. (1998). Comparison of analytic methods for a follow- up study of upper extremity disorders. In "Third International Scientific Conference on Prevention of Work-Related Musculo- skeletal Disorders/International Symposium on Epidemiology in Occupational Health (PREMUS-ISEOH 98)." Finnish Institute of Occupational Health, Helsinki, Finland.
169. Ostlin, P. (1988). Negative health selection into physically light occupations. J. Epidemiol. Commun. Health 42, 152-156.
170. Johansson, J. ,~. (1995). The impact of decision latitude, psycho- logical load and social support at work on musculoskeletal symp- toms. Eur. J. Public Health 5, 169-174.
171. Theorell, T., Harms-Ringdahl, K., Ahlberg-Hultrn, G., and Westin, B. (1991). Psychosocial job factors and symptoms from the loco- motor system--A multicausal analysis. Scand. J. Rehabil. Med. 23, 165-173.
172. Karasek, R. A. (1985). Job Content Questionnaire and User's Guide, Department of Work Environment, University of Massa- chusetts Lowell, Lowell, MA.
173. Hall, E. M. (1992). Double exposure: The combined impact of the home and work environments on psychosomatic strain in Swedish women and men. Int. J. Health Serv. 22, 239-260.
174. Romito, P., and Hovelacque, E (1987). Changing approaches in women's health: New insights and new pitfalls. Int. J. Health Serv. 17, 241-258.
175. Cleland, L. (1987). "RSI:" A model of social iatrogenesis. Med. J. Aust. 147, 236-239.
176. Punnett, L., and Bergqvist, U. (1997). "Visual Display Unit Work and Upper Extremity Musculoskeletal Disorders. A Review of Epidemiological Findings." National Institute of Working Life, Solna, Sweden.
177. Katz, J. N., Punnett, L., Simmons, B. P., Fossell, A. H., Mooney, N., and Keller, R. B. (1996). Workers' compensation recipients with carpal tunnel syndrome: The validity of self-reported health measures. Am. J. Public Health 86, 52-56.
178. Harreby, M., Kjer, J., Hesselsoe, G., and Neergaard, K. (1996). Epidemiological aspects and risk factors for low back pain in 38- year-old men and women: A 25-year prospective cohort study of 640 school children. Eur. Spine J. 5, 312-318.
179. Hurwitz, E. L., and Morgenstern, H. (1997). The effects of co- morbidity and other factors on medical versus chiropractic care for back problems. Spine 22, 2254-2263.
180. Von Korff, M., Wagner, E. H., Dworkin, S. E, and Saunders, K. W. (1991). Chronic pain and use of ambulatory health care. Psycho- som. Med. 53, 61-79.
181. Bush, E M., Harkins, S. W., Harrington, W. G., and Price, D. D. (1993). Analysis of gender effects on pain perception and symp- tom presentation in temporomandibular pain. Pain 53, 73-80.
182. Karlson, E. W., Daltroy, L. H., Liang, M. H., Eaton, H. E., and Katz, J. N. (1997). Gender differences in patient preferences may underlie differential utilization of elective surgery. Am. J. Med.
102, 524-530. 183. Hogeweg, J. A., Langereis, M. J., Bernards, A. T. M., Faber, J. A.
J., and Helders, P. J. M. (1992). Algometry: Measuring pain threshold, method and characteristics of healthy subjects. Scand.
J. RehabiL Med. 24, 99-103. 184. Takala, E.-P. (1990). Pressure pain threshold on upper trapezius
and levator scapulae muscles. Scand. J. Rehabil. Med. 22, 63-68. 185. Theorell, T., Nordemar, R., Michelsrn, H., and Stockholm MUSIC
I Study Group (1993). Pain thresholds during standardized psy- chological stress in relation to perceived psychosocial work situ- ation. J. Psychosom. Res. 37, 299-305.
186. Werner, R. A., Franzblau, A., Albers, J. W., and Armstrong, T. J. (1998). Median mononeuropathy among active workers: Are there differences between symptomatic and asymptomatic workers? Am. J. Ind. Med. 33, 374-378.
187. Bohannon, R. W. (1997). Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20-79 years. Arch. Phys. Med. Rehabil. 78, 26-32.
188. Messing, K. and Stevenson, J. (1996). Women in Procrustean beds: Strength testing and the workplace. Gender, Work Organ. 3,
156-167. 189. Kilbom, ,~. (1988). Isometric strength and occupational muscle
disorders. Eur. J. Appl. Physiol. 57, 322-326. 190. Barnekow-Bergkvist, M., Hedberg, G. E., Janlert, U., and Jansson,
E. (1998). Determinants of self-reported neck-shoulder and low back symptoms in a general population. Spine 23, 235-243.
191. Biering-Scrensen, F. (1984). Physical measurements as risk indi- cators for low-back trouble over a one-year period. Spine 9,
106-118. 192. Leino, P., Aro, S., and Hasan, J. (1987). Trunk muscle function
and low back disorders: A ten-year follow-up study. J. Chron. Dis.
40, 289-296. 193. Keyserling, W. M., Herrin, G. D., and Chaffin, D. B. (1980). Iso-
metric strength testing as a means of controlling medical incidents on strenuous jobs. J. Occup. Med. 22, 332-336.
194. H~igg, G. (1991). Static work loads and occupational myalgia--a new explanation model. In "Electromyographical Kinesiology" (P. A. Anderson, D. J. Hobart, and J. V. Danoff, eds.), pp. 141-144. Elsevier, Amsterdam.
195. H~igg, G. M., and Astrrm, A. (1997). Load pattern and pressure pain threshold in the upper trapezius muscle and psychosocial factors in medical secretaries with and without shoulder/neck dis- orders. Int. Arch. Occup. Environ. Health 69, 423-432.
196. Nygaard, E., and Hede, K. (1987). Physiological profiles of the male and the female. In "Exercise: Benefits, Limits and Adapta- tions" (D. Macleod et al., eds.), pp. 289-307. Spon, London.
197. Scgaard, K., Christensen, H., Fallentin, N., Mizuno, M., Quistorff, B., and Sjcgaard, G. (1998). Motor unit activation patterns during concentric wrist flexion in humans with different muscle fibre composition. Eur. J. Appl. Physiol. 78, 411-416.
198. Stevenson, J. M. (1995). Gender-fair employment practices: De- veloping employee selection tests. In "Invisible: Issues in Women's Occupational Health/Invisible: La sant6 des travail- leuses" (K. Messing, B. Neis, and L. Dumais, eds.), pp. 306-320. Gynergy Books, Charlottetown, P.E.I., Canada.
199. ,~strand, P.-O., and Rodahl, K. (1977). "Textbook of Work Phys- iology." McGraw-Hill, New York.
200. Dvorak, J., Antinnes, J. A., Panjabi, M., Loustalot, D., and Bonomo, M. (1992). Age and gender related normal motion of the cervical spine. Spine 10, $393-$398.
201. Hart, D. A., Archambault, J. M., Kydd, A., Reno, C., Frank, C. B., and Herzog, W. (1998). Gender and neurogenic variables in ten-

492 S E C T I O N 6 - - W O M E N AT W O R K
don biology and repetitive motion disorders. Clin. Orthop. Relat. Res. 351, 44-56.
202. Pacifici, R., Rifas, L., McCracken, R., Vered, I., McMurtry, C., Avioli, L. V., and Peck, W. A. (1989). Ovarian steroid treatment blocks a postmenopausal increase in blood monocyte interleukin 1 release. Proc. Nat. Acad. Sci. U.S.A. 86, 2398-2402.
203. Da Silva, J. A. P., Larbre, J., Seed, M. P., Cutolo, M., Villaggio, B., Ascott, D. L., and Willoughby, D. A. (1994). Sex differences in inflammation induces cartilage damage in rodents: the influence of sex steroids. J. Rheum. 21, 330-337.
204. Hart, D. A., Frank, C. B., and Bray, R. C. (1995). Inflammatory processes in repetitive motion and overuse syndrome: potential role of neurogenic mechanisms in tendons and ligaments. In "Re- petitive Motion Disorders of the Upper Extremity" (S. L. Gordon, L. J. Fine, and S. Blair, eds.), pp. 247-262. American Academy of Orthopedic Surgeons, Rosemont, IL.
205. Cannon, L. J., Bernacki, E. J., and Walter, S. D. (1981). Personal and occupational factors associated with carpal tunnel syndrome. J. Occup. Med. 23, 255-258.
206. Adera, T., Deyo, R. A., and Donatelle, R. J. (1994). Premature menopause and low back pain: A population-based study. Ann. Epidemiol. 4, 416-422.
207. Svensson, H.-O., Andersson, G. B. J., Hagstad, A., and Jansson, P.-O. (1990). The relationship of low-back pain to pregnancy and gynecologic factors. Spine 15, 371-375.
208. Wreje, U., Isacsson, D., and Aberg, H. (1997). Oral contraceptives and back pain in women in a Swedish community. Int. J. Epide- miol. 26, 71-74.
209. Paul, J. A., and Frings-Dresen, M. H. W. (1994). Standing work- ing posture compared in pregnant and non-pregnant conditions. Ergonomics 37, 1563-1575.
210. Masten, W. Y., and Smith, J. L. (1988). Reaction time and strength in pregnant and nonpregnant employed women. J. Occup. Med. 30, 451-456.
211. Kelsey, J. L., Greenberg, R. A., Hardy, R. J., and Johnson, M. E (1975). Pregnancy and the syndrome of herniated lumbar inter- vertebral disc; an epidemiological study. Yale J. Biol. Med. 48, 361-368.
212. Dumas, G. A., Reid, J. G., Wolfe, L. A., Griffin, M. P., and Mc- Grath, M. J. (1995). Exercise, posture, and back pain during preg- nancy: Part 1. Exercise and posture. Clin. Biomech. 10, 98-103.
213. Fast, A., Weiss, L., Ducommun, E. J., Medina, E., and Butler, J. G. (1989). Low-back pain in pregnancy: Abdominal muscles, sit-up performance, and back pain. Spine 15, 28-30.
214. Ekman-Ordeberg, G., Salgeback, S., and Ordeberg, G. (1987). Carpal tunnel syndrome in pregnancy: a prospective study. Acta Obstet. Gynecol. Scand. 66, 233-235.
215. Wand, J. S. (1990). Carpal tunnel syndrome in pregnancy and lactation. J. Hand Surg. 15B, 93-95.
216. Voitk, A. J., Mueller, J. C., Farlinger, D. E., and Johnston, R. U. (1983). Carpal tunnel syndrome in pregnancy. Can. Med. Assoc. J. 128, 277-279.
217. Nilsson, T., Hagberg, M., Burstr6m, L., and Kihlberg, S. (1994). Impaired nerve conduction in the carpal tunnel of platers and truck assemblers exposed to hand-arm vibration. Scand. J. Work Envi- ron. Health 20, 189-99.
218. Wieslander, G., Norb~ick, D., Grthe, C.-J., and Juhlin, L. (1989). Carpal tunnel syndrome (CTS) and exposure to vibration, repeti- tive wrist movements, and heavy manual work: A case-referent study. Br. J. Ind. Med. 46, 43-47.
219. Hagberg, M., Morgenstern, H., and Kelsh, M. (1992). Impact of occupations and job tasks on the prevalence of carpal tunnel syn- drome. Scand. J. Work Environ. Health 18, 337-345.
220. Cohen, A. L., Gjessing, C. C., Fine, L. J., Bernard, B. P., and McGlothin, J. D. (1997). "Elements of Ergonomics Programs: A Primer Based on Workplace Evaluations of Musculoskeletal Dis- orders." National Institute for Occupational Safety and Health, Cincinnati, OH.
221. Grant, K., and Habes, D. (1995). Summary of studies on the ef- fectiveness of ergonomic interventions. Appl. Occup. Environ. Hyg. 10, 523-530.
222. Aronsson, G., Bergqvist, U., and Almers, S. (1992). "Arbetsor- ganisation och muskuloskeletala besvar vid bildskarmsarbete (Work organization and musculoskeletal discomforts in VDT work, in Swedish)." National Institute of Working Life, Solna Sweden.
223. Burt, S., Hornung, R., and Fine, L. J. (1990). "Health Hazard Evaluation Report: Newsday Inc., Melville, NY." National Insti- tute for Occupational Safety and Health, Cincinnati, OH.
224. Polanyi, M. E D., Cole, D. C., Beaton, D. E., et al. (1997). Upper limb work-related musculoskeletal disorders among newspaper employees: Cross-sectional survey results. Am. J. Ind. Med. 32, 620-628.
225. Stetson, D. S., Silverstein, B. A., Keyserling, W. M., Wolfe, R. A., and Albers, J. W. (1993). Median sensory distal ampli- tude and latency: Comparisons between nonexposed managerial/ professional employees and industrial workers. Am. J. Ind. Med. 24, 175-189.