Embed Size (px)
Citation preview

Women and Heart DiseaseWomen and Heart Diseaseby Debra Kellyby Debra Kelly
History Anatomy Physiology Risk Factors Symptoms Treatments HRT Prevention
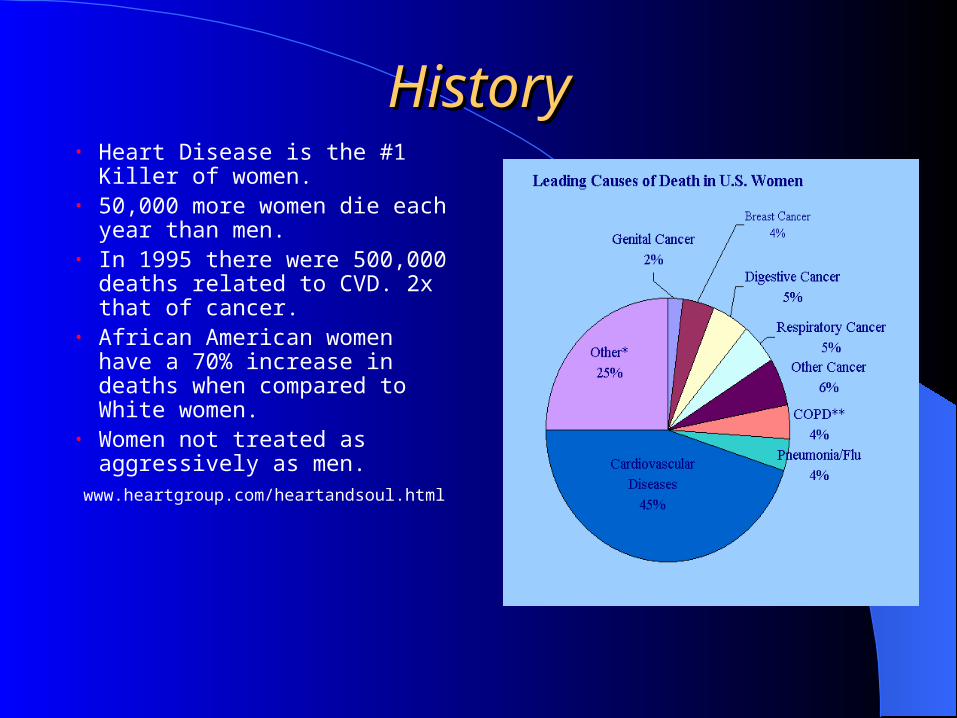
HistoryHistory• Heart Disease is the #1 Killer of
women.• 50,000 more women die each
year than men.• In 1995 there were 500,000
deaths related to CVD. 2x that of cancer.
• African American women have a 70% increase in deaths when compared to White women.
• Women not treated as aggressively as men.
www.heartgroup.com/heartandsoul.html

Anatomy of CirculationAnatomy of Circulation Right Coronary Artery
Supplies the right ventricle and right atria.
Right Posterior Descending Artery
Supplies the posterior portion of heart(AV node, IV Septum and posterior papillary muscle).
Left Coronary Artery Branches into the anterior descending and
circumflex ,they supply Left Ventricle,anterior papillary muscle and anterior IV septum and left atria.
Women's arteries are 0.5 to 1.0 mm smaller in diameter than those of men.
www.heartpoint.com/coronarteries.html

Physiology of ThrombusPhysiology of Thrombus
Hyperlipedemia contributes to plaque formation.
Arteries most effected are proximal left anterior descending, proximal right coronary artery and the distal right coronary artery
Injury theory, plaque rupture and thrombosis formation cause blockage.
www.yoursurgery.com/proceduredetails.cfm

Risk FactorsRisk Factors
Risk Factors That Risk Factors That Can be Treated Or
Cannot Be Changed Changed
Heredity Smoking Diabetes
Gender /Race High Blood Pressure Obesity
Increasing Age Sedentary Life Hyperlipidemia

Unchangeable Risk FactorsUnchangeable Risk Factors
Heredity: The risk increases 2 to 3 fold in patients with a family history of MI and rose with the number of relatives with a history of MI.
Gender: Mortality rate higher in women. 50,000 die annually.
1st heart attacks often fatal. Within 1 year of MI 42% of women die/24% of men. 6 years after 1st MI 33% of women will suffer 2nd MI as opposed to 21% of men. Fewer studies are done with women .
Race: African American Women have an increased mortality rate as opposed to white women, they are more likely to be overweight and also have diabetes and hypertension, independent risk factors.

Treatable Risk FactorsTreatable Risk Factors
Smoking: Decreases estrogen and increases lipids. As few as 4 cigarettes/day can have twice the risk of CAD than non-smokers
High Blood Pressure: Approximately 50% of women have HTN by age 45 and 79% of African American Women respectively. > than 140/90 is determined as HTN.
Sedentary Life: Moderate exercise program can decrease BP and increase HDL and decrease VLDL levels.

Treatable Risk FactorsTreatable Risk Factors
Diabetes: Type II diabetes increases 3 to 7 fold the risk of CAD as opposed to men which is 2 to 3 fold. It also contributes to HTN and hyperlipidemia. More prevalent in African American Women. Increases risk of recurrent MI and heart failure.
Obesity: Maintenance of ideal body weight decreases risk of MI 35%-60%. Increased weight causes increases in lipids, blood pressure and diabetes.
Hyperlipidemia: postmenopausal HDL levels decline and LDL levels rise.

SymptomsSymptoms
Common Symptoms• Chest Pain, heaviness,tightness• Pain in arms• Shortness of Breath
Uncommon Symptoms• Nausea, vomiting, heartburn• Fainting, confusion, sweating• Jaw pain, neck pain, back pain• Fatigue, palpations

Acute Myocardial Infarction Acute Myocardial Infarction TreatmentsTreatments
• Angioplasty• Thrombolytics• ASA• Beta-Blockers• ACE Inhibitors• Gp IIb/IIIa Inhibitors• CABG
It’s What’s inside that
counts

AngioplastyAngioplasty
• PTCA: 1st line of treatment if within 1 hour of infarct.
• Stents: currently have a 30% restenosis rate caused from the injury cascade to the vessel wall.
• Sirolimus-Eluting Stents: new stent just out March 2003. Coated with a immunosupressive drug which prevents cell proliferation in the G1 phase . In recent studies it has shown to decrease the in-stent stenosis by 25%.
• Results: 30 days after stenting women’s death rate or MI was 3.1% as compared to men at 1.8%. The 1 year outcomes were similar for men and women, 5.8% and 6.0% respectively. Women were older had more diabetes, hypertension and hypercholesterolemia.

Pre and Post StentingPre and Post Stenting
www.areo.ufl.edu/~uhk/ANGIOPLASTY.jpg

MedicationsMedications
Thrombolytics: Within in 1 hour of symptoms can reduce mortality by 3.5%. There has been a 17% reduction in the 30 day mortality form 1975-1995.
ASA: The increased use has been the greatest contributor to decreased mortality. In 1975 only 5% usage, 1995 75% usage.
Beta-blockers: Reduces sudden death and reinfarction rate.
ACE Inhibitors: Reduces morbity and mortality in MI survivors and
women with LV dysfunction. GIIb/IIIa Inhibitors: Aggrastat, Integrilin and plavix these are
platelet aggragates which improve outcomes equally in women and men with stent placement.

Coronary Artery Bypass Coronary Artery Bypass GraftingGrafting
• 32% of all surgeries are female.• Higher complications early.
Per/post op period.• More risk factors at time of surgery (HTN, PVD, CHF and Diabetes)• Older at time of surgery• Smaller body size and artery size
difficult anastomoses.• Less relief from Angina symptoms.• Less use of Internal Mammary
Artery, which has better outcomes.• 5 years out no difference in death
rate of both sexes.www.sas.upenn.edu/~lsnyder2/Facts.html

Hormone Replacement Hormone Replacement TherapyTherapy
THE GOOD THE BAD and THE UGLY
Prevents Increases Alarming • Osteoporosis Invasive breast ca less use of proven• < colon cancer risk of stroke CAD prevention• Hot flashes risk of PE therapies.• Mood swings risk of CAD such as ASA, • Beneficial in the 1st year of HERS ACE inhibitors
Presence of study showed a 22% Beta-blockers &
Vascular injury increase in CVD lipid lowering Rx
In CABG

Prevention is the KeyPrevention is the Key
Healthy Diet Weight Loss Exercise Smoking Cessation Monitor Blood Pressure Monitor Lipids Diabetes Control

ConclusionsConclusions
• Increase usage of CV drugs known for heart disease• Increase knowledge of heart disease by women and their
doctors• Early diagnosis of heart disease symptoms• Monitoring for Diabetes, weight management• Monitoring for HTN and lipid profile• Increase usage of Cardiac Rehab programs• Inclusion of Women in more cardiac studies
“Knowledge, coupled with action, is POWER” (2)

Works CitedWorks Cited 1. Aflalo-Caldercon, B. (2002) HRT, Women and Heart Disease: What We Need to
Know about Prevention. Heart Bytes. Retrieved Feb. 18, 2003 from MedScape
http://www.medscape.com
2. Facts About Women and Cardiovascular Disease. (1998) American Heart Association, Inc.
3. Grady, D. “et.al.” (July 3, 2002) Cardiovascular Disease Outcomes During 6.8 Years of Hormone Therapy. Jama. (Vol. 288 No. 1).
4. Heindenreich, P.A., McClellan, M. (Feb. 2001) “Trends in Treatment and Outcomes for Acute Myocardial Infarction: 1975-1995.” The American
Heart Journal of Medicine. (Vol. 110 (3) pp 165-174.
5. Herrington, D.M. (Jan 7-14, 2003) Hormone Replacement Therapy and Heart Disease: Replacing Dogma with Data. Circulation Vol. 107 (1) p. 2-4.

Works Cited (Cont’d)Works Cited (Cont’d) 6. Hippisley-Cox, J. “et.al.” (Apr 2001) “Sex Inequalities in ischaemic Heart Disease
in General Practice: Cross Sectional Survey.” British Medical Journal (Vol 322(7290) pp 832-834.
7. King, K.B., Mosca, L. (Mar 22, 2000) Prevention of Heart Disease in Women:Recommendation for Management of Risk Factors. Progress in Cardiovascular Nursing.
8. Lee, I-Min. “et.al.” (Mar 21, 2001). Physical Activity and Coronary Heart Disease in Women: is “No Pain, No gain” passé? JAMA (Vol 285 (11) pp. 1447-1454)
9. Mehilli, J. “et.al.” (Oct. 11, 2000) Differences in Prognostic Factors and Outcomes Between Women and Men Undergoing Coronary Artery Stenting. JAMA (Vol 284 No. 14)
10. Miller, A., Oparil, S. (2003, Jan 21) Secondary Prevention of Coronary Heart Disease in Women: A call to Action, Annal of Interval Medicine, Vol 138(2).

Works Cited (Cont’d)Works Cited (Cont’d) 11. Mosca, L. “et. al” ( 1999 ) Guide to Prevention Cardiology for Women, AHA Inc.
&American College of Cardiology.
12. Mosca, L., Manson, J., Sutherland, S. (1997) Cardiovascular Disease in Women. American Heart Association.
13. Mosca, L. The Importance of Identifying and Reducing Cardiovascular Risk Factors in Women. Retrieved March 9, 2003 from Medscape online.
http://www.medscape.com/viewarticle/448971_2
14. Myer, J. (Jan 14, 2003) Exercise and Cardiovascular Health. Circulation. (Vol 107(1) pp e2-e5)
15. Nabel, E.G. (Aug 24, 2000) Coronary Heart Disease in Women- An Ounce of Prevention. New England Journal of Medicine. (Vol 343 (8) pp 572-574.
16. Popma, J.J., Klein, K., Medicio, R. (2003) Sirolimus- Eluting Stents. Cath Lab Digest. March 2003 (Vol 11 No. 3)

Works Cited (Cont’d)Works Cited (Cont’d) 17. Price, S.A., Wilson, L.M. (2003) Pathophysiology, Clinical Concepts of Disease
Processes. Mosby, St. Louis, Missouri, 6th Ed.
18. Rosenthal, S.M. (2000). 50 Ways Women can Prevent Heart Disease. Los Angeles, Lowell House.
19. Ruchisa, G. “et.al.” (Dec 25, 2002) Benefit of an Early Invasive Management Strategy in Women with Acute Coronary Syndromes. JAMA. Vol 288-24 pp 3124-3129.
20. Shlipak, M.G., “et.al.” (2002) Estrogen and Progesterone, Lipoprotein(a), and the Risk of Recurrent Coronary Heart Disease Events after
Menopause. JAMA, Vol 284(14) pp1845-1852.
21. Vaccarino, V. “et.al.” (July 7, 1999) Sex-Based differences in Early Morality after Myocardial Infarction. The New England Journal of Medicine. (Vol
341, No. 4)

Works Cited (Cont’d)Works Cited (Cont’d) 22. Walsh, B, Moriaty, P. Preventing CVD in Women:A work in Progress. Retrieved
Feb 18, 2003 from medscape online. Http://www.medscape.com/viewaricle/442233_2.
23. Wenger, N.K. Menopause Hormone Therapy & Risk for CVD: Current Status. Retrieved from Med Scape March 9, 2003. Http://www.medscape.com/viewaricle/448971_3
24. Weger, N.K. The Importance of Identifying and Reducing Cardiovascular Risk Factors in Women. Retrieved from Medscape March 9, 2003. Http://www.medscape.com/viewaricle/448971_1.
25. Wilansky, S., Willerson, J. (2002) Heart Disease in Women. Churchill Livingstone 1st Ed. USA.
26. Yoder, M. Pharm D, BCPS. (2003) Advances in Adjunctive Pharmacotherapy for Patients Undergoing PCI. Cath Lab Digest. March 2003 (Vol 11) #3.