Embed Size (px)
DESCRIPTION
Hemoglobinbrain function malfunctioncerebral blood flowartificial blood vesicle engineeringliposome encapsulated vesiclesstorageblood brain barrierdescription of the structural change of hemoglobintraumatic brain injuryrelative permeabilitybiochemistry in medical ingeneering of artificial blood különleges előállítási technikák
Citation preview

ADVANCES IN CLINICAL PRACTICE jgh_6925 11..20
Management of ascites in cirrhosisFlorence Wong
Department of Medicine, Toronto General Hospital, University of Toronto, Toronto, Ontario, Canada
AbstractAscites is a common complication of liver cirrhosis associated with a poor prognosis. Thetreatment of ascites requires dietary sodium restriction and the judicious use of distal andloop diuretics, sequential at an earlier stage of ascites, and a combination at a later stage ofascites. The diagnosis of refractory ascites requires the demonstration of diuretic non-responsiveness, despite dietary sodium restriction, or the presence of diuretic-related com-plications. Patients with refractory ascites require second-line treatments of repeat large-volume paracentesis (LVP) or the insertion of a transjugular intrahepatic portosystemicshunt (TIPS), and assessment for liver transplantation. Careful patient selection is para-mount for TIPS to be successful as a treatment for ascites. Patients not suitable for TIPSinsertion should receive LVP. The use of albumin as a volume expander is recommended forLVP of >5–6 L to prevent the development of circulatory dysfunction, although the clinicalsignificance of post-paracentesis circulatory dysfunction is still debated. Significant mor-tality is still being observed in cirrhotic patients with ascites and relatively preserved liverand renal function, as indicated by a lower Model for End-Stage Liver Disease (MELD)score. It is proposed that patients with lower MELD scores and ascites should receiveadditional points in calculating their priority for liver transplantation. Potential new treat-ment options for ascites include the use of various vasoconstrictors, vasopressin V2 receptorantagonists, or the insertion of a peritoneo-vesical shunt, all of which could possiblyimprove the management of ascites.
Key words
ascites, diuretics, large volume paracentesis,portal hypertension, renal sodium retention,TIPS.
Accepted for publication 24 August 2011.
Correspondence
Dr Florence Wong, 9th floor, North Wing,Room 983, Toronto General Hospital, 200Elizabeth Street, Toronto, ON M5G2C4,Canada. Email: [email protected]
IntroductionThe risk for developing ascites is approximately 60% at 10 yearsafter cirrhosis diagnosis if the underlying cause of the cirrhosis isleft untreated.1 The appearance of ascites heralds the onset ofdecompensation, and the survival of these patients changes from80% at 5 years1 to 50% at 5 years2 without liver transplantation.This is because the hemodynamic changes and circulatory dys-function that accompany the progression of cirrhosis predisposethese patients to other complications (Fig. 1) associated with wors-ening prognosis (Table 1).3 In a study assessing the natural historyof patients with cirrhosis, hospitalized for the management ofascites, during a mean follow-up period of 41 � 3 months, 28% of263 patients developed dilutional hyponatremia, 11% developedrefractory ascites, and 7.6% developed hepatorenal syndrome(HRS). The occurrence of any of these complications furtherreduced survival2 (Fig. 2).
The effective treatment of ascites in cirrhosis involves correct-ing one or more of the pathophysiological processes that lead toascites formation (Fig. 3). In short, the presence of cirrhosis andportal hypertension leads to vasodilatation in the systemic andsplanchnic circulations, but vasoconstriction in the renal circula-tion. Together with alterations in renal auto-regulation, a reductionin functional liver cell mass, and the development of cirrhotic
cardiomyopathy, these processes result in a gradual increase inrenal sodium and water retention. The presence of portal hyper-tension then preferentially localizes the excess fluid in the perito-neal cavity as ascites.
The management of ascites requires a stepwise approach, begin-ning with dietary sodium restriction and diuretic therapy, followedby second-line treatments once refractory ascites sets in.
Dietary sodium restrictionThe underlying pathophysiology that leads to ascites formation incirrhosis is renal sodium retention; therefore, the mainstay oftreatment of ascites is to induce a negative sodium balance. Thiscan be achieved by reducing the dietary sodium intake, as well asincreasing the renal sodium output using a combination of diuret-ics.4 It is not uncommon for patients with ascites who are not ondiuretics to have renal sodium excretion of < 20 mmol/day. Such apatient on a no-added-salt diet containing 130–150 mmol ofsodium will retain at least 100 mmol of sodium/day, equivalent tothe accumulation of 10 L of ascitic fluid in 2 weeks (100 mmol/day ¥ 14 days � 140 mmol/L = 10 L) (Table 2). The InternationalAscites Club has recommended a sodium intake of 88 mmol/day.5
This will require the use of special, low-sodium food items, andconsultation with a dietician is usually required. Patients are more
doi:10.1111/j.1440-1746.2011.06925.x
11Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

likely to adhere to a low-sodium diet if there is family support. Inpatients who normally consume a high-salt diet, the use of sodiumrestriction alone can lead to the reduction of ascites, especially ifthe urinary sodium excretion is > 78 mmol/day.6 If a patient whoadmits to adhering to a low-sodium diet and is still gaining weightrapidly, calculating the sodium balance (see Table 2) can oftenbring the message home. Salt substitutes usually contain highpotassium contents, and can lead to hyperkalemia if patients arealso on potassium-sparing diuretics. In the majority of cirrhoticpatients with ascites, diuretics are usually required to induce anatriuresis.
Diuretic therapyDiuretics block sodium reabsorption along the various nephronsites, thereby increasing renal sodium excretion. Water excretionthen follows passively. It is customary to start diuretic therapy withan aldosterone antagonist, such as spironolactone, otherwise all
the renal sodium that is not absorbed at the loop of Henle with theuse of a loop diuretic alone will be reabsorbed at the distal tubuleunder the unopposed action of the high aldosterone levels.Spironolactone is usually administered at a start-up dose of100 mg/day, and gradually increased up to 400 mg/day. Thediuretic effect can be seen within 48 h, but the peak onset of actionis 2 weeks, due to impaired metabolism in cirrhotics and a verylong half-life of up to 5 days.5 Amiloride can be used instead ofspironolactone, starting at 5 mg/day, and gradually increased to20 mg/day. It has a shorter half-life, and therefore, a quicker onsetof action, but is less effective than spironolactone, as shown in arandomized, controlled trial.7 Potassium canrenoate, anotheraldosterone antagonist, is popular in Europe, and has been shownto reduce the 1-year cumulative occurrence of ascites in cirrhosis.8
The starting dose is usually 200 mg/day, and gradually increasedto 400 mg/day.
If the use of a distal diuretic is not producing the desiredresponse, a loop diuretic, such as furosemide, can be added, start-ing at a dose of 40 mg/day, and gradually increased to 160 mg/day.The dose response curve of furosemide is sigmoidal. Therefore,once a maximum diuretic response is reached, further increases infurosemide dose will not increase the diuretic response. The mostsuccessful therapeutic regimen is the combination of a distal
Figure 1 Stages of ascites in cirrhosis. HRS,hepatorenal syndrome. = spontaneous bac-terial peritonitis.
Table 1 Prognosis factors in cirrhotic patients with ascites
Parameter Median survival (months)
Mean arterial pressure (mmHg)> 80 46< 80 11
Serum creatinine (mg/dL)< 1.2 251.2–1.5 11� 1.5 4
Hyponatremia (serum [Na] < 130 mmEq/L)No 27Yes 7
Urinary Na excretion (mmEq/day)� 10 46< 10 17
Plasma renin activityNormal 57Increased 6
Plasma norepinephrine (epinephrine)Normal 23Increased 13
Na, sodium. Adapted from Cardenas and Arroyo,3 with permission.
Figure 2 Survival of hospitalized patients with ascites with or withoutcomplications. (Adapted from Planas et al.,2 with permission.) , Nocomplications; , Spontaneous bacterial peritonitis; , Refractoryascites; , Dilutional hyponatremia; , Hepatorenal syndrome.
Management of ascites in cirrhosis F Wong
12 Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

diuretic, such as spironolactone, and a loop diuretic, such as furo-semide, beginning with 100 mg and 40 mg respectively, andincreased in a step-wise fashion, preferably maintaining the sameratio of dosages, in order to maintain normal potassium levels.6
There have been discussions as to whether the simultaneous orsequential use of an aldosterone antagonist and a loop diuretic ismore efficacious in the treatment of ascites. Santos et al.9 reportedthat both the sequential or combined use of diuretics was similarin terms of the diuretic response and diuretic-induced complica-tions. However, Angeli et al. demonstrated in a randomized, con-trolled trial that treatment with combined diuretics could mobilizemoderate ascites more rapidly than sequential diuretics, and was
associated with less side-effects, including renal failure.10 Theexplanation for the difference in the findings could be that thepatients in the study of Santos et al. were at a much earlier stageof ascites, with 60% of the patients enrolled at their first presen-tation of ascites, and at least 40% of them had normal supinelevels of aldosterone.9 In the study of Angeli et al.,10 at least 70%of patients had recurrent ascites that required repeat paracenteses.Most had hyperaldosteronism, and many had reduced renal func-tion. Therefore, it is reasonable to use sequential diuretics inpatients with ascites at first appearance, and they will likelyrespond with a satisfactory natriuresis with ascites reduction.However, patients with recurrent ascites will be better served with
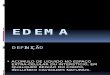
Figure 3 Pathogenesis of ascites formation.EABV, effective arterial blood volume; GFR,glomerular filtration rate; Na, sodium; RAAS,rennin–angiotensin–aldosterone system; RBF,renal blood flow; SNS, sympathetic nervoussystem.
F Wong Management of ascites in cirrhosis
13Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

combination diuretic therapy in order to reduce the time requiredto achieve a satisfactory diuretic response and to reduce the risk ofhyperkalemia.
Patients on diuretic therapy need to be monitored regularly forelectrolyte abnormalities, over-diuresis, and renal failure. As thevolume of ascites that can be resorbed into the systemic circulationis approximately 400 mL/day,11 weight loss in excess of 0.5 kg/daymeans that there is reduction of the intravascular volume, therebyplacing these patients at risk of the development of renal failurefrom over-diuresis. Patients with peripheral edema can toleratemore rapid fluid loss until the edema has resolved. Compliancewith and response to sodium restriction and diuretics can be evalu-ated regularly by 24-h urine collection for sodium excretion. Insituations where this is not feasible, a random urine sodium to apotassium ratio of > 1 predicts a > 78 mmol/day sodium excretionin 90% of patients.12 Non-compliance with a low-sodium diet isreflected by an adequate renal sodium excretion, but without anyweight loss. A low renal sodium excretion necessitates increasingthe diuretics doses as tolerated, up to the maximum recommendedlevels. When the combination of sodium restriction and diuretics isgiven to carefully-monitored patients, 90% of them can reduce oreven eliminate their ascites with significant improvement in theirquality of life.
AlbuminAlbumin is a plasma protein that is most responsible for plasmacolloid oncotic pressure. It is a negatively-charged molecule thatattracts sodium and water, and therefore, it is a very good volumeexpander.13 In addition, it has many other functions, such as ligandbinding, and antioxidant and endothelial stabilizing properties.Therefore, albumin seems the ideal solution to manage conditionswhere there is intravascular volume reduction, inflammation, orcirculatory dysfunction. Albumin has been advocated as a treat-ment for many complications of cirrhosis and ascites, such asspontaneous bacterial peritonitis14 and HRS.15 As the basic patho-physiological process that leads to the development of ascites is a
reduction of the effective arterial blood volume,16 it makes physi-ological sense to use albumin in the management of ascites,although this has been controversial.
In one randomized, controlled trial in cirrhotic patients withascites, weekly infusions of 25 g of albumin added to standarddiuretics was shown to produce a significantly better diureticresponse compared to diuretics alone, including shorter hospitalstay, lower probability of ascites reaccumulation, and a lowerlikelihood of readmission to hospital, but no effect on survival.17 Ina later study by the same investigators, the use of 25 g/weekalbumin for 1 year, and thereafter, 25 g every 2 weeks for up to120 months in patients with first-onset ascites, resulted in a sig-nificant increase in survival of 16 months and a significantly lowerprobability of ascites recurrence.18 The major drawback of chronicalbumin use is its cost. For this reason, there is currently nostandard recommendation to use albumin as an adjunct therapy todiuretics in the treatment of uncomplicated ascites.
Refractory ascitesRefractory ascites is defined as ascites that cannot be easily mobi-lized (< 1.5 kg weight loss/week), despite daily doses of 400 mgspironolactone or 30 mg amiloride plus 160 mg furosemide; andthe patient must have been compliant with dietary sodium restric-tion of � 90 mmol/day for � 1 week.19 Patients who cannot tol-erate diuretics because of the development of complications aredefined as having diuretic-intractable ascites (Table 3).19 Becausethese patients are either unresponsive to or are intolerant of diuret-ics, second-line treatments, such as regular large-volume paracen-tesis (LVP) or the insertion of a transjugular intrahepaticportosystemic shunt (TIPS), are needed for the management oftheir ascites. All of these patients should also be considered forliver transplantation, unless there is a contraindication.
LVP
Several large randomized, controlled trials have shown that LVP of4–6 L is safer and more effective for the treatment of tense ascitesthan the use of high doses of diuretics.20–22 The incidence of sys-temic and hemodynamic disturbance, electrolyte abnormalities,renal impairment, and encephalopathy was lower in those treatedwith repeated LVP compared to diuretic therapy. Shorter durationof hospitalization was observed with LVP, but the rates of hospitalreadmission and survival were similar to those of diuretictherapy.20 Because LVP does not alter the pathogenetic mecha-nisms that lead to ascites formation, ascites will recur following aparacentesis.
The frequency and the volume of LVP can be determined fromthe patient’s sodium intake. For a patient who is adherent tosodium restriction of 88 mmol/day, the weekly weight gain, andtherefore ascites accumulation, should be < 4 L/week (Table 2),and this should be correspondingly less for patients whosesodium intake is less than 88 mmol/day. Therefore, a patient whois requesting a LVP of 10–12 L every week is obviously notadhering to a low-sodium diet. Counseling with a dietician isoften helpful to reduce the sodium intake in order to make LVPmore manageable for both the physician and the patient.
The next question is whether intravascular volume replacementis necessary following LVP. Reaccumulation of ascites following
Table 2 Calculating the sodium balance
ScenarioI
Urinary sodium excretion is 90 mmol/dayInsensible sodium loss is 10 mmol/dayNa intake = 88 mmol/dayNa output = 100 mmol/dayNa balance = (88–100) mmol/day = -12 mmol or-84 mmol/weekAscitic [Na] = 140 mmol/L (Same as serum [Na])Therefore fluid loss = -84 mmol / 140 mmol/L = -0.6 LWeight loss/week = 0.6 kg
ScenarioII
Urinary sodium excretion is 0 mmol/dayInsensible sodium loss is 10 mmol/dayNa intake = 88 mmol/dayNa output = 10 mmol/dayNa balance = (88–10) mmol/day = +78 mmolAscitic [Na] = 140 mmol/L (Same as serum [Na])Therefore fluid gain = +78 mmol / 140 mmol/L = 0.56 LWeight gain/day = 0.56 kg or Weight gain/week = 3.92 kg
Na, sodium.
Management of ascites in cirrhosis F Wong
14 Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

LVP can lead to a reduction in central circulatory volume, withpotential for compromising systemic hemodynamics, a conditionknown as paracentesis-induced circulatory dysfunction (PICD),defined as an increase in plasma renin activity by > 50% of thepreparacentesis level to a final value of > 4 ng/mL/h.23 This couldlead to further activation of the already activated vasoconstrictorsystems and place the patient at risk of the development of renaldysfunction. There are data to suggest that paracentesis of < 6 Lcan be safely performed without the use of volume expanders,24,25
thus the incidence of circulatory dysfunction is only 7% in para-centeses of < 6 L, and there is little, if any, clinical consequence.25
This is especially true in patients with peripheral edema, since theedema fluid can be reabsorbed to replenish the central circulation.In contrast, the use of total paracentesis was associated with thedevelopment of PICD in 37% of patients.23
There has been much debate about the use of volume expandersfollowing every paracentesis, because PICD does not occur afterevery episode of LVP,26 nor does every case of PICD lead to thedevelopment of renal impairment.27 In one study, only 40% ofpatients who experienced PICD developed significant renalimpairment, while 11% developed renal impairment, even withoutany evidence of circulatory dysfunction.23 Gines et al. not onlyadvocated the use of plasma expanders following every paracen-tesis, they also demonstrated that the use of albumin was the mosteffective of all volume expanders to reduce the incidence ofPICD.28 However, other studies have shown that synthetic plasmaexpanders are as effective as albumin in preventing hyponatremiaand renal impairment following LVP.29,30 To support the use ofalbumin, a recent double-blind, randomized pilot study showedthat the number of liver-related complications was significantlylower in patients who were infused with albumin compared with
those infused with polygeline.31 Given the fact that albumin hasnot been shown to cause any harm in cirrhosis, the InternationalAscites Club recommends that, until further results are available,the infusion of albumin of 6–8 g is to be given per liter of asciticfluid removed for LVP of > 5–6 L.19 A recent study from Torontodemonstrated that as long as the ascitic volume removed is lessthan 8 L, and the standard dose of albumin of 6–8 g/L of asciticfluid removed is given, the development of PICD is not associatedwith any renal dysfunction.32
Although cirrhotic patients might have coagulopathy andthrombocytopenia, the incidence of clinically-significant intra-abdominal bleeding during an LVP is estimated to be ª0.5%.Therefore, the routine use of fresh–frozen plasma or platelet con-centrates is not recommended. Leakage of ascitic fluid through thepuncture site is a relatively frequent complication. The Z-tracttechnique should reduce its occurrence. Ascites leakage post-LVPshould be managed by placing a purse-string suture around thepuncture site or by applying skin adhesive, and instructing thepatient to lie with the puncture site uppermost.33 The use of acolostomy bag to contain the ascites leak should be discouragedbecause of the increased risk of infection.
TIPS
A TIPS functions like a side-to-side portocaval shunt, and is veryeffective in reducing portal pressure. As sinusoidal portal hyper-tension is one of the pathogenetic mechanisms of ascites forma-tion in cirrhosis, it stands to reason that a successful TIPSinsertion should be able to eliminate ascites. In addition, the suc-cessful insertion of TIPS returns a significant volume from thesplanchnic circulation to the systemic circulation, thereby reduc-ing the extent of underfilling of the effective arterial bloodvolume.34 Even in the absence of diuretics, increased sodiumexcretion begins after the first month following TIPS insertion.Thereafter, it increases further to culminate in a renal sodiumexcretion of approximately 100 mmol/day at 12 months.35
Patients will need to stay on a low-sodium diet in the post-TIPSperiod, or must take diuretics in order to facilitate ascites clear-ance. Within 6 months, complete resolution of ascites occurs inapproximately two-thirds of patients, and a partial response inthe other one-third. Further resolution can occur up to 12 monthspost-TIPS, with ultimately approximately 80% of patients com-pletely clearing their ascites.
Recent results have shown that the presence of diastolic dys-function, part of the cirrhotic cardiomyopathy syndrome,36 is asso-ciated with poor ascites clearance after TIPS.37 Successful TIPSplacement with elimination of ascites improves renal functionand35 nutritional status, and causes positive nitrogen balance,38 allleading to improved quality of life.
Five randomized, controlled trials have compared LVP versusTIPS as a treatment for ascites.39–43 All have showed that TIPS ismuch more effective than LVP in terms of the control of ascites,but at the expense of more episodes of hepatic encephalopathy.44
Other TIPS-related complications include those related to theprocedure itself, and those related the presence of a shunt(Table 4).45,46 The recent advent of polytetrafluoroethylene(PTFE)-covered stents has significantly reduced the incidence ofTIPS stenosis; this was seen in up to 70% of cases with bare stents
Table 3 Diagnostic criteria for refractory ascites
1. Treatment duration: Patients must be on intensive diuretictherapy (spironolactone 400 mg/day and furosemide 160 mg/day)for at least 1 week and on a salt-restricted diet of less than90 mmol/day or 5.2 g of salt/day.
2. Lack of response: Mean weight loss of < 0.8 kg over 4 days andurinary sodium output less than the sodium intake.
3. Early ascites recurrence: Reappearance of grade 2 or 3 ascites†
within 4 weeks of initial mobilization.4. Diuretic-induced complications
a. Diuretic-induced hepatic encephalopathy: development ofencephalopathy in the absence of any other precipitating factor.
b. Diuretic-induced renal impairment: increase of serum creatinineby > 100% to a value > 2 mg/dL in patients with ascitesresponding to treatment.
c. Diuretic-induced hyponatremia: decrease of serum sodium by> 10 mmol/L to a serum sodium of < 125 mmol/L.
d. Diuretic induced hypo- or hyperkalemia: change in serumpotassium to < 3 mmol/L or > 6 mmol/L, despite appropriatemeasures.
†Grading of ascites; Grade 1 = mild ascites only detectable by ultrasoundexamination; Grade 2 = moderate ascites that is manifest by moderatesymmetrical distension of the abdomen; Grade 3 = large or grossascites with marked abdominal distension.Adapted from Salerno et al.19
F Wong Management of ascites in cirrhosis
15Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

in the first year after TIPS insertion,47 but with PTFE-coveredstents, hepatic encephalopathy occurs in approximately 50% ofpatients in the first 2 years.48 This can easily be controlled withmedical therapy, although occasionally, reducing the diameter ofthe stent is required for the management of the hepatic encephal-opathy. The covered stents have the advantage of avoiding bileleakage into the stent lumen due to decreased abluminal porosity,and also a smoother internal lining, thereby permitting a moreuniform endothelial growth.47,49,50
Until recently, TIPS has not been shown to provide a survivalbenefit in patients who receive it for the management of ascites.44
However, a recent meta-analysis using individual patient data fromthe four larger TIPS versus LVP randomized, controlled trialsshowed that TIPS does provide a survival advantage in thecarefully-selected patients (Fig. 4).51 Therefore, patient selection iscrucial to maximize the benefits of TIPS. In general, patients whoare elderly, with a history of recurrent hepatic encephalopathy, orthose with known cardiac dysfunction or pulmonary hypertension,as well as those with renal failure should be carefully assessedbefore being accepted for TIPS. In addition, TIPS insertionrequires a patent portal vein for TIPS insertion to be technicallyfeasible, and there should no structural abnormalities, such asmultiple hepatic cysts. Finally, patients should be free of infectionsprior to TIPS insertion. If the presence of infection at another sitecolonizes the TIPS, which is not removable once inserted, thepatient will become intermittently bacteremic, making it difficultto eradicate the infection.
The absolute and relative contraindications for TIPS insertionare shown in Table 5. Currently, a randomized, controlled trial isbeing conducted to assess the effect of TIPS versus LVP on thesurvival of patients at an earlier stage of the natural history ofascites, especially those with better liver function. If improvedsurvival can be confirmed in certain subgroups of patients usingTIPS, then the selection of patients for TIPS placement will haveto take into consideration the patient’s age, severity of liver dys-function, and extent of circulatory dysfunction.
Liver transplantationAll patients with refractory ascites should be assessed for livertransplantation, the only procedure which corrects both theimpaired liver function and portal hypertension. Splanchnic andsystemic hemodynamic abnormalities, which are pivotal in thepathogenesis of ascites formation, slowly return to normal afterliver transplantation. Therefore, liver transplantation is the idealtreatment for advanced cirrhosis and ascites. However, with theintroduction of the Model for End-Stage Liver Disease (MELD)score for the allocation of donor organs for liver transplantation,52
the presence of ascites no longer has any weighting in prioritizingpatients for liver transplantation. It follows that patients withrefractory ascites and low MELD scores, such as abstinent alco-holics or patients with inactive viral hepatitis, can remain on theliver transplant waiting list for an extended period of time withoutever receiving a donor organ.
Various investigators have confirmed that mortality for patientson the liver transplant waiting list remains high (> 20% at180 days), despite a lower MELD score of < 21, if the patient alsohas moderate ascites and hyponatremia.53–55 The more severe theascites, the higher the waiting-list mortality.55 In fact, low-serumsodium and the presence of moderate ascites have been shown tobe independent predictors of early pretransplant mortality inpatients with a MELD score of < 21.53 As well, the Child–Pughscore, which includes ascites, seems to be a better index of prog-nosis than the MELD score in patients who have a MELD score of> 14.4.56 Efforts are now being made to modify the criteria for theallocation of donor organs, such as assigning points for persistentascites and low-serum sodium in calculating the final score fororgan allocation. This would improve the likelihood of patientswith ascites receiving liver transplantation in a timely fashion.
Potential new treatments for ascitesMany investigators have been exploring other treatments forrefractory ascites, because not all cases of refractory ascites aresuitable for TIPS insertion, nor can every patient who receives aTIPS eliminate their ascites, and liver transplant is not available forall patients with advanced liver disease. The following is asummary of potentially-available agents.
Vasoconstrictors
Various vasoconstrictors have been assessed to determine whetherimproved splanchnic and systemic hemodynamics could lead toimproved renal hemodynamics and increased renal sodium excre-tion, thereby reducing the ascites.
Midodrine is an alpha adrenergic receptor agonist that isapproved for the treatment of postural hypotension. It is alsopopular in North America for the treatment of HRS. Its alphaagonist action results in an increase in mean arterial pressure incirrhosis.57 In two small studies totaling 56 patients, the use ofmidodrine, either as a single oral dose,58 or given three times perday orally for 7 days,59 significantly improved renal hemodynam-ics, together with a significant increase in renal sodium excretion.In one of the studies,59 there was a significant correlation betweenthe increase in systemic vascular resistance and an increase inglomerular filtration rate and enhanced renal sodium excretion.
Table 4 Complications related to transjugular intrahepatic portosys-temic shunts (TIP)
Procedure related HemoperitoneumLaceration of capsuleLaceration of vesselsArteriovenous fistulaHemobiliaArrhythmia
Prosthesis related Migration of stentKinkingHemolytic anemiaInfection of stent (endotipsitis)
TIPS dysfunction ThrombosisStenosis
Hepatic encephalopathy New onsetWorsening
Progressive liver failure Child–Pugh score � 12Hepatocellular carcinomaCardiovascular Arrhythmia
Cardiac failure
Management of ascites in cirrhosis F Wong
16 Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

However, in patients who have normal systemic hemodynamics,the use of midodrine has not been shown to improve renal sodiumexcretion.60 With longer-term administration of midodrine (for1 month in 8 patients with cirrhosis and refractory ascites),together with weekly albumin infusion and long-acting, slow-release octreotide, there was a significant reduction in plasmarenin and aldosterone concentrations, but only a trend towards areduction in the volume of ascites removed by paracentesis,without any effects on renal function.61
Terlipressin is a vasopressin analog that acts on the V1 receptorin the splanchnic vasculature to cause splanchnic vasoconstriction,thereby decreasing splanchnic inflow and lowering the portal pres-sure. The improvement in systemic hemodynamics has been suc-cessfully used in the treatment of HRS in cirrhosis. The role ofterlipressin in the management of ascites has also been assessed inseveral studies. A single dose of 2 mg terlipressin given intrave-nously was effective in improving renal blood flow, the glomerularfiltration rate, and renal sodium excretion in cirrhotics withoutrenal dysfunction with (n = 8) or without (n = 11) ascites.62 Theimprovement in renal function correlated with decreased plasmanorepinephrine and renin levels, and increased atrial natriureticpeptide concentrations. These results were confirmed in anotherstudy, which included 12 patients with cirrhosis and ascites, butwithout azotemia or hyponatremia.63 Systemic hemodynamicsimproved, associated with increases in creatinine clearance, diure-sis and natriuresis.63
The positive results in these preliminary studies suggest thatvasoconstrictors should be explored further as potential treatmentsfor ascites. However, until the results of randomized, controlledtrials are available, these agents cannot be regarded as standard ofcare in the management of refractory ascites.
Vasopressin V2 receptor antagonists
Vasopressin V2 receptor antagonists, or “vaptans”, are agents thatcompete with vasopressin for attachment onto the V2 receptors atthe renal collecting duct to inhibit water reabsorption at that site,thereby inducing an aquaresis and reduced serum water content.The vaptans were first developed for the management ofhyponatremia in patients with edematous states.64–66 It wasobserved in some of the above studies that the vaptans were alsoable to reduce the extent of ascites in cirrhotic patients.66 It isfeasible that by maintaining serum sodium, the use of vaptans hadpermitted diuretics to be continued, thereby improving the controlof ascites.
In a recent publication that reports on three large randomized,controlled trials involving 1200 patients with cirrhosis and ascites,the use of satavaptan either alone or in combination with diureticswas not shown to be clinically beneficial in the management ofascites. Further, in one of the three studies, it was associated withan increased mortality.67 Short-term studies involving othervaptans, such as M000268 or tolvaptan,69 have shown efficacy ofthese two vaptans in improving ascites. However, the study withM0002 only involved 15 patients for a total administration courseof 2 weeks, while that using tolvaptan included 18 patients for atotal of nine study days. Therefore, while the results are encour-aging, it is not clear whether longer-term studies involving a largercohort of patients with either M0002 or tolvaptan will confirmtheir efficacy in reducing ascites in cirrhosis. Currently there is norecommendation to use vaptans in the management of ascites.
ALFApump system
The ALFApump system (Sequana Medical AG, Zurich, Switzer-land) is the latest investigational tool that is being developed forthe management of ascites. It is a subcutaneously-implanted,
Figure 4 Survival of different subgroups ofpatients following transjugular intrahepaticportosystemic shunt insertion. (Adapted fromSalerno et al.,51 with permission.)
Table 5 Contraindications for transjugular intrahepatic portosystemicshunt insertion for the management of refractory ascites
Absolute Relative
• Uncontrolled encephalopathy • > 70 years of age• Congestive heart failure • Any infection, including dental
sepsis• Severe pulmonary
hypertension• Non-compliance with sodium
restriction• Child–Pugh score � 12 • Hepatoma (especially if central)• Multiple hepatic cysts • Portal vein thrombosis• Unrelieved biliary obstruction
F Wong Management of ascites in cirrhosis
17Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

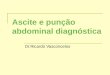
battery-powered peritoneo-vesical shunt that pumps excess peri-toneal fluid into the bladder where the patient can eliminate itthrough normal urination (Fig. 5). To date, 40 patients havereceived the device in a phase-3 clinical trial, which successfullyremoved 90% of the ascites (Dr Noel Johnson, pers. comm., 2011).With meticulous attention to aseptic techniques and the use ofprophylactic antibiotics, the rate of infection has been no higherthan what is expected in the cirrhotic population, despite the pres-ence of the foreign body. With the device recently being approvedin Europe, it is expected that this will significantly transform themanagement of ascites in the future, ultimately reducing thenumber of patients who require LVP as the mainstay of treatmentfor their ascites.
ConclusionThe medical management of ascites, including dietary sodiumrestriction and diuretic therapy, has not changed significantly forseveral decades. The development of TIPS two decades ago as atreatment for refractory ascites was regarded as the “new kid onthe block”, but the emergence of many TIPS-associated compli-cations quickly dampened the enthusiasm of clinicians caring forpatients with refractory ascites, until the randomized, controlledtrials and subsequent meta-analyses further refined the patientselection criteria for TIPS insertion. Currently, patients who arenot suitable for TIPS insertion depend on regular LVP to controltheir ascites, while they await their turn for liver transplantation.With the recognition that the presence of ascites in patients withlow MELD scores can negatively impact their prognosis, effortsare now being made to reassign points for the presence of ascitesin calculating the priority for liver transplantation, so that patientswith low MELD scores and ascites are not being disadvantaged.
Improved understanding of the pathophysiology of ascites for-mation provides possible novel options for the future, such asvasoconstrictor therapy that aims at correcting the abnormal physi-ology of cirrhosis. Technological advances mean that even in thosepatients whose only option is repeat LVP, it is possible in the futureto have a device implanted so as to discharge the ascites throughthe urinary system. Preliminary data have suggested that survivalmight be improved with these newer treatments. The future willneed to include randomized, controlled trials to evaluate and
confirm the results of these recent studies to ultimately providebetter treatments for ascites in patients with cirrhosis.
References1 D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and
prognostic indicators of survival in cirrhosis: a systematic review of118 studies. J. Hepatol. 2006; 44: 217–31.
2 Planas R, Montoliu S, Balleste B et al. Natural history of patientshospitalized for management of cirrhotic ascites. Clin. Gastroenterol.Hepatol. 2006; 4: 1385–94.
3 Cardenas A, Arroyo V. Management of ascites and hydrothorax.Best Pract. Res. Clin. Gastroenterol. 2007; 21: 55–75.
4 Leung W, Wong F. Medical management of ascites. Expert Opin.Pharmacother. 2011; 12: 1269–83.
5 Moore KP, Wong F, Gines P et al. The management ofascites—report on the consensus conference of the InternationalAscites Club. Hepatology 2003; 38: 258–66.
6 Runyon BA, AASLD Practice Guidelines Committee. Managementof adult patients with ascites due to cirrhosis: an update. Hepatology2009; 49: 2087–107.
7 Angeli P, Della Pria M, De Bei E et al. Randomized clinical studyof the efficacy of amiloride and potassium canrenoate innonazotemic cirrhotic patients with ascites. Hepatology 1994; 19:72–9.
8 Bolondi L, Piscaglia A, Gatta A et al., DOC (Decrease Of Complica-tions in cirrhosis) Study Group. Effect of potassium canrenoate, ananti-aldosterone agent, on incidence of ascites and variceal progres-sion in cirrhosis. Clin. Gastroenterol. Hepatol. 2006; 4: 1395–402.
9 Santos J, Planas R, Pardo A et al. Spironolactone alone or incombination with furosemide in the treatment of moderate ascites innonazotemic cirrhosis. A randomized comparative study of efficacyand safety. J. Hepatol. 2003; 39: 187–92.
10 Angeli P, Fasolato S, Mazza E et al. Combined versus sequentialdiuretic treatment of ascites in non-azotaemic patients with cirrhosis:results of an open randomised clinical trial. Gut 2010; 59: 98–104.
11 Shear L, Ching S, Gabuzda GJ. Compartmentalization of ascites andedema in patients with hepatic cirrhosis. N. Engl. J. Med. 1970; 282:1391–6.
12 Pinto-Marques P, Vieira A. Urinary sodium/potassium ratio onrandom sample as a useful tool to assess diuretic-induced natriuresison chronic liver disease-associated ascites. Am. J. Gastroenterol.2007; 102: 212–13.
13 Wong F. Drug insight: the role of albumin in the management ofchronic liver disease. Nat. Clin. Pract. Gastroenterol. Hepatol. 2007;4: 43–51.
14 Fernández J, Monteagudo J, Bargallo X et al. A Randomizedunblinded pilot study comparing albumin versus hydroethyl starch inspontaneous bacterial peritonitis. Hepatology 2005; 42: 627–34.
15 Guevara M, Arroyo V. Hepatorenal syndrome. Expert Opin.Pharmacother. 2011; 12: 1405–17.
16 Cárdenas A, Arroyo V. Mechanisms of water and sodium retentionin cirrhosis and the pathogenesis of ascites. Best Pract. Res. Clin.Endocrinol. Metab. 2003; 17: 607–22.
17 Gentilini P, Casini-Raggi V, Di Fiore G et al. Albumin improves theresponse to diuretics in patients with cirrhosis and ascites: results ofa randomized, controlled trial. J. Hepatol. 1999; 30: 639–45.
18 Romanelli RG, La Villa G, Barletta G et al. Long-term albumininfusion improves survival in patients with cirrhosis and ascites: anunblinded randomized trial. World J. Gastroenterol. 2006; 12:1403–7.
19 Salerno F, Guevara M, Bernardi M et al. Refractory ascites,pathogenesis, definition, and therapy of a severe complication incirrhotic patients. Liver Int. 2010; 30: 937–47.
Figure 5 Schematic picture of a peritoneo-vesical shunt in situ.
Management of ascites in cirrhosis F Wong
18 Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

20 Gines P, Arroyo V, Quintero E et al. Comparison of paracentesisand diuretics in the treatment of cirrhosis with tense ascites: resultsof a randomized study. Gastroenterology 1987; 93: 234–41.
21 Salerno F, Badalamenti S, Incerti P et al. Repeated paracentesis andi.v. albumin infusion to treat “tense” ascites in ascitic patients: a safealternative therapy. J. Hepatol. 1987; 5: 102–8.
22 Pinto PC, Amerian J, Reynolds TB. Large volume paracentesis innon-edematous patients with tense ascites: its effect on intravascularvolume. Hepatology 1988; 8: 207–10.
23 Ruiz-del-Arbol L, Monescillo A, Jimenez W, Garcia-Plaza A,Arroyo V, Rodes J. Paracentesis-induced circulatory dysfunction:mechanism and the effect on hepatic hemodynamics in cirrhosis.Gastroenterology 1997; 113: 579–86.
24 Peltekian K, Wong F, Liu P, Allidina Y, Sherman M, Blendis LM.The effect of large volume paracentesis on total central bloodvolume, systemic and renal hemodynamics and renal sodiumhandling in cirrhosis. Am. J. Gastroenterol. 1997; 92: 394–9.
25 Sola-Vera J, Minana J, Ricart E et al. Randomized trial comparingalbumin and saline in the prevention of paracentesis-inducedcirculatory dysfunction in cirrhotic patients with ascites. Hepatology2003; 37: 1147–53.
26 Gines P, Tito L, Arroyo V et al. Randomized comparative study oftherapeutic paracentesis with and without intravenous albumin incirrhosis. Gastroenterology 1988; 94: 1493–502.
27 Moreau R, Asselah T, Condat B et al. Comparison of the effect ofterlipressin and albumin on arterial blood volume in patients withcirrhosis and tense ascites treated by paracentesis: a randomised pilotstudy. Gut 2002; 50: 90–4.
28 Gines A, Fernandez-Esparrach G, Monescillo A et al. Randomizedtrial comparing albumin, dextran 70, and polygeline in cirrhoticpatients with ascites treated by paracentesis. Gastroenterology 1996;111: 1002–10.
29 Panos MZ, Moore K, Vlavianos P et al. Single, total paracentesis fortense ascites: sequential hemodynamic changes and right atrial size.Hepatology 1990; 11: 662–7.
30 Salerno F, Badalamenti S, Lorenzano E, Moser P, Incerti P.Randomized comparative study of hemaccel vs. albumin infusionafter total paracentesis in cirrhotic patients with refractory ascites.Hepatology 1991; 13: 707–13.
31 Moreau R, Valla DC, Durand-Zaleski I et al. Comparison ofoutcome in patients with cirrhosis and ascites following treatmentwith albumin or a synthetic colloid: a randomized controlled pilottrial. Liver Int. 2006; 26: 46–54.
32 James PD, Oosterveld L, Wong F. Circulatory dysfunction after largevolume paracentesis in patients with cirrhosis and ascites. (Abstract).Hepatology 2009; 50 (Suppl. 4): 476A.
33 Thomsen TW, Shaffer RW, White B, Setnik GS. Videos in clinicalmedicine: paracentesis. N. Engl. J. Med. 2006; 355: e21.
34 Wong F, Sniderman K, Liu P, Blendis LM. The mechanism of theinitial natriuresis after transjugular intrahepatic portosystemic shunt.Gastroenterology 1997; 112: 899–907.
35 Wong W, Liu P, Blendis LM, Wong F. Renal sodium handlingduring long-term follow-up and the effect of sodium loading incirrhotic patients treated with TIPS for refractory ascites. Am. J.Med. 1999; 106: 315–22.
36 Wong F. Cirrhotic cardiomyopathy. Hepatol. Int. 2009; 3: 294–304.37 Rabie RN, Cazzaniga M, Salerno F, Wong F. The use of E/A ratio as
a predictor of outcome in cirrhotic patients treated with transjugularintrahepatic portosystemic shunt. Am. J. Gastroenterol. 2009; 104:2458–66.
38 Allard JP, Chau J, Sandokji K, Blendis LM, Wong F. Effects ofascites resolution after successful TIPS on nutrition in cirrhoticpatients with refractory ascites. Am. J. Gastroenterol. 2001; 96:2442–7.
39 Lebrec D, Giuily N, Hadenque A et al. Transjugular intrahepaticportosystemic shunt: comparison with paracentesis in patients withcirrhosis and refractory ascites: a randomized trial. J. Hepatol. 1996;25: 135–44.
40 Rossle M, Ochs A, Gulberg V et al. A comparison of paracentesisand transjugular intrahepatic portosystemic shunting in patients withascites. N. Engl. J. Med. 2000; 342: 1701–7.
41 Sanyal A, Gennings C, Reddy KR et al., and the North AmericanStudy for Treatment of Refractory Ascites. A randomized controlledstudy of TIPS versus large volume paracentesis in the treatment ofrefractory ascites. Gastroenterology 2003; 124: 634–43.
42 Gines P, Uriz J, Calahorra B et al. Transjugular intrahepaticportosystemic shunt versus repeated paracentesis plus intravenousalbumin for refractory ascites in cirrhosis. A multicenter randomizedcomparative study. Gastroenterology 2002; 123: 1839–47.
43 Salerno F, Merli M, Riggio O et al. Randomized controlled study ofTIPS vs. paracentesis with albumin in cirrhosis with refractoryascites. Hepatology 2004; 40: 629–35.
44 D’Amico G, Luca A, Morabito A, Miraglia R, D’Amico M.Uncovered transjugular intrahepatic portosystemic shunt forrefractory ascites: a meta-analysis. Gastroenterology 2005; 129:1282–93.
45 Colombato L. The role of transjugular intrahepatic portosystemicshunt (TIPS) in the management of portal hypertension. J. Clin.Gastroenterol. 2007; 41 (Suppl. 3): S344–51.
46 Sanyal AJ, Freedman AM, Luketic VA et al. The natural history ofportal hypertension after transjugular intrahepatic portosystemicshunts. Gastroenterology 1997; 112: 889–98.
47 Barrio J, Ripoll C, Banares R et al. Comparison of transjugularintrahepatic portosystemic shunt dysfunction in PTFE-coveredstent-grafts versus bare stents. Eur. J. Radiol. 2005; 55: 120–4.
48 Riggio O, Angeloni S, Salvatori FM et al. Incidence, natural history,and risk factors of hepatic encephalopathy after transjugularintrahepatic portosystemic shunt with polytetrafluoroethylene-covered stent grafts. Am. J. Gastroenterol. 2008; 103:2738–46.
49 Angermayr B, Cejna M, Koenig F et al., Vienna TIPS Study Group.Survival in patients undergoing transjugular intrahepaticportosystemic shunt: ePTFE-covered stent grafts versus bare stents.Hepatology 2003; 38: 1043–50.
50 Jung HS, Kalva SP, Greenfield AJ et al. TIPS: comparison of shuntpatency and clinical outcomes between bare stents and expandedpolytetrafluoroethylene stent grafts. J. Vasc. Interv. Radiol. 2009; 20:180–5.
51 Salerno F, Cammà C, Enea M, Rössle M, Wong F. Transjugularintrahepatic portosystemic shunt for refractory ascites, ameta-analysis of individual patient data. Gastroenterology 2007; 133:825–34.
52 Kamath PS, Wiesner RH, Malinchoc M et al. A model to predictsurvival in patients with end-stage liver disease. Hepatology 2001;33: 464–70.
53 Heuman DM, Abou-Assi SG, Habib A et al. Persistent ascites andlow serum sodium identify patients with cirrhosis and low MELDscores who are at high risk for early death. Hepatology 2004; 40:802–10.
54 Somsouk M, Guy J, Biggins SW, Vittinghoff E, Kohn MA,Inadomi JM. Ascites improves upon serum sodium plus Model forEnd-Stage Liver Disease (MELD) for predicting mortality in patientswith advanced liver disease. Aliment. Pharmacol. Ther. 2009; 30:741–8.
55 Somsouk M, Kornfield R, Vittinghoff E, Inadomi JM, Biggins SW.Moderate ascites identifies patients with low Model for End-StageLiver Disease scores awaiting liver transplantation who have a highmortality risk. Liver Transpl. 2011; 17: 129–36.
F Wong Management of ascites in cirrhosis
19Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd

56 Gotthardt D, Weiss KH, Baumgartner M et al. Limitations of theMELD score in predicting mortality or need for removal fromwaiting list in patients awaiting liver transplantation. BMCGastroenterol. 2009; 9: 72.
57 Wong F, Pantea L, Sniderman K. The use of midodrine, octreotideand transjugular intrahepatic portosystemic stent shunt in thetreatment of cirrhotic patients with ascites and renal dysfunctionincluding hepatorenal syndrome. Hepatology 2004; 40: 55–64.
58 Angeli P, Volpin R, Piovan D et al. Acute effects of the oraladministration of midodrine, an alpha-adrenergic agonist, on renalhemodynamics and renal function in cirrhotic patients with ascites.Hepatology 1998; 28: 937–43.
59 Kalambokis G, Fotopoulos A, Economou M, Pappas K, Tsianos EV.Effects of a 7-day treatment with midodrine in non-azotemiccirrhotic patients with and without ascites. J. Hepatol. 2007; 46:213–21.
60 Misra VL, Vuppalanchi R, Jones D et al. The effects of midodrineon the natriuretic response to furosemide in cirrhotics with ascites.Aliment. Pharmacol. Ther. 2010; 32: 1044–50.
61 Tandon P, Tsuyuki RT, Mitchell L et al. The effect of 1 month oftherapy with midodrine, octreotide-LAR and albumin in refractoryascites: a pilot study. Liver Int. 2009; 29: 169–74.
62 Krag A, Moller S, Henriksen JH, Holstein-Rathlou NH, Larsen FS,Bendtsen F. Terlipressin improves renal function in patients withcirrhosis and ascites without hepatorenal syndrome. Hepatology2007; 46: 1863–71.
63 Kalambokis GN, Pappas K, Baltayiannis G, Katsanou A,Tsianos EV. Effects of terlipressin on water excretion after oral
water load test in nonazotemic cirrhotic patients with ascites withouthyponatremia. Scand. J. Gastroenterol. 2010; 45: 1509–15.
64 Wong F, Blei A, Blendis LM, Robertson G, Thuluvath PJ, the NorthAmerican VPA-985 Study Group. The effects of VPA-985, avasopressin receptor antagonist, on water metabolism in patientswith hyponatremia: a multi-center randomized placebo controlledtrial. Hepatology 2003; 37: 182–91.
65 Schrier RW, Gross P, Gheorghiade M et al., SALT Investigators.Tolvaptan, a selective oral vasopressin V2-receptor antagonist, forhyponatremia. N. Engl. J. Med. 2006; 355: 2099–112.
66 Ginès P, Wong F, Watson H, Milutinovic S, Ruiz del Arbol L,Olteanu D. Effects of Satavaptan, a selective vasopressin V2
receptor antagonist, on ascites and serum sodium concentration inpatients with cirrhosis and hyponatremia. Hepatology 2008; 48:204–13.
67 Wong F, Watson H, Gerbes A, Vilstrup H, Badalamenti S,Bernardi M. Ginès P, for the Satavaptan Investigators Group.Satavaptan for the management of ascites in cirrhosis: efficacyand safety across the spectrum of ascites severity. Gut 2011 (inpress).
68 Nevens F, Moreno C, Cools M, Thielemans L, Kerstens R,Meulemans A. Effects of M0002, a novel V2 antagonist on sodiumlevels and weight gain affected by water accumulation in cirrhoticpatients with ascites. J. Hepatol. 2009; 50 (Suppl. 1): S76.
69 Okita K, Sakaida I, Okada M et al. A multicenter, open-label,dose-ranging study to exploratively evaluate the efficacy, safety, anddose–response of tolvaptan in patients with decompensated livercirrhosis. J. Gastroenterol. 2010; 45: 979–87.
Management of ascites in cirrhosis F Wong
20 Journal of Gastroenterology and Hepatology 27 (2012) 11–20
© 2011 Journal of Gastroenterology and Hepatology Foundation and Blackwell Publishing Asia Pty Ltd


![[PPT]Harry K. Wong Rosemary T. Wong - Manchester …users.manchester.edu/Student/kntritch/ProfWeb/Wong... · Web viewDirections: Using information from today’s classroom management](https://img.pdfslide.net/doc/110x75/5b445d737f8b9a53428ba011/pptharry-k-wong-rosemary-t-wong-manchester-users-web-viewdirections.jpg)










![Urinary Stone Management [Dr. Edmond Wong]](https://img.pdfslide.net/doc/110x75/55d4fd91bb61eba4528b46ca/urinary-stone-management-dr-edmond-wong.jpg)





![ASCITE-Caso Clinico-Lezione [modalità compatibilità]](https://img.pdfslide.net/doc/110x75/62e2fdc7a0373e065e20cb54/ascite-caso-clinico-lezione-modalit-compatibilit.jpg)







