Embed Size (px)
Citation preview

Work-Related Upper Extremity Conditions
Kurt T. Hegmann, MD, MPHProfessor and Center Director
Dr. Paul S. Richards Endowed Chair in Occupational Safety & Health
Rocky Mountain Center for Occupational & Environ. Health
University of Utah© 2011
Methodology1. Exhaustive Literature Searches (7 databases)
for Randomized Controlled Trials (RCTs):2. Articles Critiqued, Graded. Strength Assigned.3. Summary Tables Compiled4. Summary Evidence and information forwarded to
Evidence-Based Practice Panel5. Guidance (Semi)-Finalized 6. External Peer Review7. Guidance Finalized
J Occup. Env. Med 2008;282-295
Example: Grading of 1 Article

RCT Article Grading (0-11 points)1. Randomization (0, 0.5, 1.0
pts.)2. Allocation concealed (0/0.5/1)3. Baseline comparability4. Blinding of patients5. Blinding of provider
6. Blinding of assessor7. Avoid co-interventions8. Compliance Rate9. Dropout Rate10. Timing of Assessments11. Intention to Treat Analysis
Low Quality: 0-3.5 pointsModerate Quality: 4.0-7.5 points
High Quality: 8.0+ points
Strength of EvidenceA:A: Strong evidence-base: ≥Two high quality
randomized controlled trials.B:B: Moderate evidence-base: One high quality or
two or more moderate quality randomized controlled trials.
C:C: Limited evidence-base: At least one study of moderate quality.
I:I: Insufficient Evidence: Evidence insufficient orirreconcilable. (Consensus recommendations)
Evidence-based Recommendations
Strongly Recommended “A” Level EvidenceModerately Recommended “B” Level EvidenceRecommended “C” Level EvidenceInsufficient For (Consensus-based) “I” Level EvidenceInsufficient-No Recommendation(Consensus-based)
“I” Level Evidence
Insufficient Against (Consensus-based) “I” Level EvidenceRecommended Against “C” Level EvidenceModerately Recommended Against “B” Level EvidenceStrongly Recommended Against “A” Level Evidence

AcknowledgementsEvidence-based Practice Hand, Wrist, and Forearm Panel Members: J. Mark Melhorn, MD, FAAOS, FACOEM, FAADEP, FACS, FASSH, FAAHS, Chair Marian C. Arbesman, PhD, OTR/L Alfred Franzblau, MD, MS, FACOEM M. Felix Freshwater, MD Charles P. Prezzia, MD, MPH, MMM, FACOEM David M. Rempel, MD, MPH, FACOEM, FACP Arlen J. Rollins, DO, MSc, FACOEM, FACPM Richard E. Sall, MD Robert W. Watson, Jr., MD, MPH Lyn D. Weiss, MD Robert A. Werner, MD, MS, FAAPMR
Managing Editors: Production: Marianne Dreger, MA Research: Julie A. Ording, MPH Editorial Assistant: Debra M. Paddack
Research Conducted By: Kurt T. Hegmann, MD, MPH, FACOEM, FACP Matthew A. Hughes, MD, MPH Matthew S. Thiese, PhD, MSPH Ulrike Ott, MSPH Sivithee Srisukhumbowornchai, MS Deborah Gwenevere Passey Riann Bree Robbins Atim Effiong Cooper Kennedy Tessa Langley
Preliminary Results:
Lateral Epicondylalgia
8
9
Job Analysis Methods: Upper Extremity
• Strain Index (Moore & Garg 1995)
• Threshold Limit Value for Hand Activity Level (ACGIH, TLV-HAL)
• Others
• None have yet been validated. (Studies reporting “validation” are not prospective).

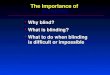
TLV and AL for HAL
0
2
4
6
8
10
2 4 6 8 10HAL (Hand Activity Level)
Nor
mal
ized
Pea
k Fo
rce 7.78 0.778TLVPF HAL= − ⋅
5.56 0.556ALPF HAL= − ⋅
1
Table 1. Rating values to assign for calculating The Strain Index.
Rating Intensity of Duration of Hand/Wrist Speed Duration/Values Exertion Exertion Efforts/Minute Posture of Work Day
1 Light <10 <4 Very Good Very Slow #1 hr.2 Somewhat Hard 10-29 4-8 Good Slow 1-23 Hard 30-49 9-14 Fair Fair 2-44 Very Hard 50-79 15-19 Bad Fast 4-85 Near Maximal ∃80 ∃20 Very Bad Very Fast ∃8
Table 1. Rating values to assign for calculating The Strain Index.
Rating Intensity of Duration of Hand/Wrist Speed Duration/Values Exertion Exertion Efforts/Minute Posture of Work Day
1 Light <10 <4 Very Good Very Slow #1 hr.2 Somewhat Hard 10-29 4-8 Good Slow 1-23 Hard 30-49 9-14 Fair Fair 2-44 Very Hard 50-79 15-19 Bad Fast 4-85 Near Maximal ∃80 ∃20 Very Bad Very Fast ∃8
Courtesy J. Steve Moore, MD, MPH, Texas A&M University
Cohort Study Overview• 1. Prospective Cohort (18 Wisconsin, Utah
companies; n=1,223). Enrolled with Consent, Questionnaires, Structured Interview, Standardized Physical Examinations, Electrodiagnostic Studies
• 2. Job Physical Exposures measured (videotapes, measures, force matching, grip strength).
• 3. Monthly follow-up for changes in symptoms, status and treatments recorded. (no treatment given)
• 4. At least quarterly monitoring of jobs for job changes and re-quantify job measures as required
• 5. Every 6-month electrodiagnostic studies for symptoms (for CTS)
12

Baseline Measures1. Consent2. Questionnaire (e.g., age, handedness, self-reported
maximum weight, sports/exercise, hobbies, tobacco, alcohol, caffeine psychosocial, etc., 266 items)
Structured Interview
483 items
Includes:• Prior Upper
Extremity symptoms, • Recent symptoms, • Hand pain
diagram
Two standardized examinations
1. Occupational medicine resident or hand therapist, Standardized examination with all maneuvers performed on all subjects as part of an inventory, 497 items
2. Boarded Occupational Medicine attending(focused on diagnostic categorization. Confirm positive findings and assess pertinent negatives)

Methods• Job Exposure Assessment Team
• Blinded to health outcomes
• Measures (e.g., force, repetition, posture)
• Ratings of perceived exertion (worker; analyst)
• Videotape• Weigh, measures• Force matching• Temperature
• Observations (e.g., impact)
Blinding Procedures
• Health outcomes team blinded to Job tasks• First examiner knew status of Pain,
Tingling/Numbness through structured interview• Second examiner also knew symptoms status• Physical Examiners blinded to NCS results• NCS performed by boarded PMR physicians,
blinded to symptoms and jobs
Case Definition: Pain in lateral epicondyle (1-10/10) + 1+ tender points on examResisted physical exam not incorporated these
analyses
“Pain” not just sore or tender, 4 kg of forceK and P required
+

19
Study Cohort (partial)
n = 451 Subjects, 66 (14.6%) excluded for LE at baseline
Of 385 eligible, n = 53 (13.8%) Lateral Epicondylalgia cases
Mean enrollment time: 37.8 ± 21.28 (1.9 - 71.2) months19
20
Descriptive statisticsDemographic Variables
Variable HR, p-value
Age 3.01, 0.041
Male 1.80, 0.066
Current Smoking 1.77, 0.039
High Cholesterol 1.87, 0.075
Medial Epi 3.77, 0.029
Variable HR, p-value
Felt Depressed 3.80, 0.002
Family Problems 3.34, 0.049
SI Intensity 1.012, 0.045
SI Posture 1.24, 0.161
21
Multivariate* Hazard Ratios
Variable Categories n(case)
HR (Range), p-value
Strain Index(Typical exposure)
≤ 6> 6
109 (10)276 (43)
1.0 (Reference)2.26 (1.12-4.56), 0.023
Strain Index(Peak exposure)
≤ 6> 6
105 (10)280 (43)
1.0 (Reference)2.12 (1.05-4.30), 0.036
*Adjusted for Age, Gender, Current Tobacco Use, Feeling Depressed, Prevalent Medial Epicondylalgia Diagnosis at Baseline

22
Discussion: Other Factors
• Many personal risk factors for these disorders • Risk factors may differ between disorders• Obesity is CTS risk (HR = 5.1), not for lateral epi.• Age is a risk factor for both• Gender appears weakly linked with CTS in multivariate analyses• Alcohol use, pregnancy and smoking (current or ever) showed no
association with CTS (?powering?). Smoking + for lateral epi.• Sum of DUE MSDs is a CTS risk……..Medial epi is for lateral epi.• Inflammatory arthritis (including RA) is a CTS risk (HR = 4.8)• Family history of CTS is a CTS risk (HR = 2.0)
23
Lateral Epicondylitis
24
Activity Modifications
• No quality studies on workplace “restrictions,” or similar.• No quality studies that activity modifications alter clinical course.
Widely believed some activities may materially aggravate and perpetuate symptoms of lateral epicondylalgia.
• Recommend avoiding home/work activities that substantially aggravate symptoms.
• Recommended, Insufficient Evidence (I)•

25
Job Design
• No quality studies• Force especially believed to be important where
occupational tasks materially contribute. Understanding the worksite and the employer’s willingness and the feasibility to modify the workstation may be important to maintain the employee at work and/or minimize disability time.
• Recommended, Insufficient Evidence (I)
Elbow Straps
• Highest quality studies either multiple co-interventions or used wrist-based off-loader brace, not widely used in the US.• Tendency towards reductions in pain• Limitations especially lack of blinding
• Rec. Insufficient Evidence (I)
Acetaminophen; Heat/Cold• Tylenol: No quality studies• Recommended, Insufficient Evidence (I)
• One study on cold; none on heat• No evidence of benefits.• Home applications felt to have no significant
adverse effects.• Recommended, Insufficient Evidence (I)

28
Home Exercises
• Frequency/Dose/Duration – Generally individualized and increased over time. Stretching frequently included, often progressed to strengthening.
• No quality evidence for one exercise regimen vs. another. • No quality evidence for/against a type of exercise (e.g., stretching or
strengthening; eccentric or concentric). • Frequencies range from 1-3x/day
• Studies use markedly different methods, different exercises, or do not describe the exercises used.
• Recommended, Insufficient Evidence (I)
Supervised therapy
•
• Indications – Select acute, subacute, chronic and post-operative epicondylalgia patients. Generally moderate to severe. Milder cases 2-3 appointments may benefit to start home exercise program.
• Frequency/Dose/Duration – Absence of specific information. Usually individualized frequency and approach. Often stretch, then strengthen (no quality evidence for specific approach). Total appointments 2-3 for mild, up to 12-15 for more severe. Should have progressive functional gain by 5-6 appts.
• Recommended, Evidence (C)
29
Non-Steroidal Anti-inflammatories
• Aspirin: Not evaluated. Rec. Insufficient (I)• No studies at OTC NSAID doses Rec. Insuff. (I)
• Naproxen 500mg BID, (Naproxen most studied) • Flurbiprofen 100mg QID, • Diclofenac SR 75mg BID, • Diflunisal 1gm then 500mg BID, studied.
• Acute, Subacute, Chronic: Moderately Recommended (B)• Piroxicam (Feldene), Not Recommended for primary/secondary
treatment. Evidence inferior to others.
Proton pump inhibitors for substantial gastrointestinal bleed risk (A)Misoprostol (A)Sucralfate (B)H2 blockers (C)

31
Topical Non-Steroidal Anti-inflammatories, etc.
• NSAIDs Moderately Recommended (B)• Flurbiprofen local-action transcutaneous patch (40 mg BID),(169) • DHEP lecithin 1.3% gel,(168) • Piroxicam gel (3cm, 0.5%, approximately 0.9g QID),(169) • Diclofenac sodium 2% in a pluronic lecithin liposome organo-gel (170) • Diclofenac sodium gel.(172) • One crossover trial: suggests flurbiprofen superior to piroxicam.• Piroxicam (Feldene), Not Recommended for
primary/secondary treatment. Evidence it is inferior to others
32
Narcotics
• No quality studies• Rare use in acute settings (first 2-3 days of acute
trauma.• Not Recommended (I)
Iontophoresis
• Short term efficacy of iontophoresis (current of 4.0 mA, treatment for 20-40 minutes), total of 6-10 treatments with glucocorticoid or diclofenac) for both lateral and medial epicondylitis. Six treatments for acute cases and 10 treatments for chronic cases, with functional improvement.
• Mod. Recommended (B)
33

34
Ultrasound
• Evidence somewhat conflicts.• Some for short term efficacy with ultrasound
(pulsed ratio of 1:4 and duration of 2 ms or continuous at a frequency of 0.7-1.5 MHz, an intensity of 1.0-2.0 W/cm2, for 5-10 minutes, over a 5 cm2 treatment area, 2-3 times per week based on objective results up to 5-6 weeks).
• Recommended (C)
35
Phonophoresis; Laser• Phono:• No significant differences among the various
experimental groups. • Not Recommended, (C)
• Laser: 12 high- and moderate-qualitytrials. Only 1 trial suggested some benefit, and all others either completely negative or no long term benefits.• Moderately Not Recommended, (B)
36
Extracorporeal Shock Wave Therapy
•9 high- or moderate-quality, sham-controlled (or low dose-controlled) trials.
•All 3 high-quality sham-controlled trials negative
•Two moderate-quality trials suggested efficacy, one did not.
Strongly Not Recommended (A)

37
Acupuncture• Chronic Epi. ONLY• Indications – Mod-severe. Fail NSAIDs (oral and/or topical),
exercise, elbow straps. Most should have failed injections. Overall benefits modest and may be transitory.
• Frequency/Dose/Duration – Various regimens, e.g., 2-3 treatments/wk for 8-10 treatments. Needling depths 1.25-2.5cm for ~20 min. Should benefit after 4-5 appts. otherwise change technique or discontinue. Trials showing most benefit were 10-12 treatments over 4-6 weeks. No comparative trials for different regimens. No benefit ‘real’ vs. sham.
• Recommended, Insuff. Evidence (I)
Injections: Glucocorticosteroids
• Trials techniques targeted most tender pt (n=3) or tendon origin (n=1).
• Medications used• Methylprednisolone 20mg;(151, 152)
• Triamcinolone acetonide 10mg,(12, 13, 202, 265, 269) 20mg;(265) • Triamcinolone acetate;(266)
• Hydrocortisone 25mg;(265)
• Betamethasone 6mg;(194)
• Triamcinolone 0.2mg.(179)
• One comp. trial: Triamcinolone 10mg superior to hydrocortisone 25mg.
• One trial: peppering technique superior to injection alone or anesthetic with peppering technique (Dogramaci 09).
• Appear inferior to platelet-rich plasma or autologous blood (Peerbooms 2010; Gosens 2011; Kazemi 10; Ozturan 10).
38
Injections: Glucocorticosteroids
• Natural history: improve or resolve
• Strong evidence of short term benefit. But, strong evidence of recurrence• ?Alter long term prognosis?• ?Worse results long-term for some?
• ? Use to tide people over the most severe pain?
Mod. Recommended (B)• Bupivicaine superior to Lidocaine
for adjuvant with corticosteroid (at 2 wks).
Recommended (C)
39
Smidt N, et al. Lancet. 2002; 359:657-662.

40
Botulinum• 4 high-quality trials of botulinum injections vs. placebo.• 3 suggest short to intermediate term benefits(271, 272, Espandar
10), one does not(270), and one suggests glucocorticosteroid injections superior (Lin 10). No longer term quality studies available.
• Invasive and reports of fatalities. Muscle weakness common (Placzek 07; Wong 05; Espandar 10; Lin 10), thus major adverse effects requiring considerable evidence of longer term efficacy to warrant. Thus, these are not recommended.
• Not Recommended, Insufficient Evidence (I)
41
Platelet-Rich Plasma Injections
• Chronic only. (No rec. acute or subacute).• One high-quality trial suggests superiority of PRP injx.
at 2 years (Gosens 11).
• Indications − At least 6 months, failed NSAID(s), straps, stretching and strengthening exercises, and at least one glucocorticosteroids injection (278)
• Dose/Frequency – Injection ~3mL platelet-rich plasma buffered with NS plus 8.4% sodium bicarbonate plus bupivacaine 0.5% with epinephrine (1:200,000), with peppering technique.
Recommended (C)
Autologous Blood Injx• Chronic only. (No rec. acute or subacute).• One trial suggested AB injections superior to
glucocorticoid (Kazemi 10), and one suggested inferiority of AB to glucocorticoid at 4 weeks, but not at 1 yr when AB was superior (Ozturan 2010).
• Indications − At least 6 months, failed NSAID(s), straps, stretching and strengthening exercises, and at least one glucocorticosteroids injection.(Kazemi 10; Creaney 11; Ozturan 10)
• Dose/Frequency – 2mL of autologous blood from a peripheral vein, then injected into most tender location(s).(278) One trial used US guidance, but no comparative trial to suggest superior results (Creasney 11).
• Recommended, Evidence (C)42

PERIARTICULAR VISCOSUPPLEMENTATION (HYALURONATE
and GLYCOSAMINOGLYCAN) INJECTIONS
• One trial of glycosaminoglycan injections found conflicting results of efficacy between 2 participating centers that are not well explained. (Akermark 95)
• One trial suggested substantial efficacy of sodium hyaluronate vs. placebo. (Petrella 10)
No Recommendation, Insufficient Evidence (I)43
44
No Recommendations• Magnets, Pulsed magnetic fields• Massage, Friction Massage• Manipulation• Mobilization• Pulsed magnetic fields• Diathermy• TENS
Electrical Stimulation• Biofeedback• Prolotherapy
45
Surgery: Lateral Epicondylitis
One trial suggests percutaneous release superior to open release with earlier return to work and patient satisfaction.(285)
One trial of tenotomy vs. shockwave therapy found no differences, though may be underpowered as some trends favor surgery.(238)
• Indications: Fail 3-6 months of non-operative treatment, surgery may be considered with debridement of inflammatory or scar tissue. Preliminary evidence that less invasive procedures have fewer complications.
• Recommended, Insufficient Evidence (I)

Lateral Epicondylitis – Case 1
• 42 y/o RHD male• CC: Presents with lateral R elbow pain after acutely pulling with force on a part that did not release 3 days ago.
• Symptoms: Pain at R lateral epicondyle with no radiation. No tingling. No past similar history. Not improving.
• PMH: Negative
Lateral Epicondylitis – Case 1
• Job history: Installs plastic trim parts in automotive assembly plant. Tasks involve positioning, seating, flexing parts, then securing by engaging clips or driving fasteners with low torque air guns.
• PE: Full R elbow ROM. Tender localized to the lateral epicondyle, not distally. Pain is reproduced with resisted wrist and middle finger extension.
Lateral Epicondylitis – Case 1
• Clinical course: Instructed in anatomy and protective body mechanics. Advised to avoid lifting with the forearm pronated (palm down). Given elbow strap. At return visit in 1 week, the symptoms were fully resolved.

Lateral Epicondylitis – Case 2
• 50 y/o RHD female • CC: Presents with 3‐4 month history of gradual onset lateral right elbow pain without trauma or incident.
• Symptoms: Pain at R lateral epicondyle radiating to mid‐dorsal forearm. No tingling. No L arm pain. No past similar history. Notes pain using a rubber mallet.
• PMH: DM; HTN
Lateral Epicondylitis – Case 2
• Job history: Positions and installs interior plastic auto parts that secure with clips. Same job for several years. Started using a rubber mallet to seat a part 1‐2 months before onset of symptoms.
• PE: Full R elbow ROM. Tender localized to the lateral epicondyle, not distally. Pain is reproduced with resisted wrist and middle finger extension.
Lateral Epicondylitis – Case 2
• Clinical course: Instructed in anatomy and protective body mechanics. Given elbow strap. Restricted from use of mallet and given alternative job. Given ice and massage treatments. No change in symptoms until injection of 10 mg of triamcinolone acetonide and anesthetic 2 months after presenting, then dramatic improvement in pain for 1 month, with residual weakness.

Lateral Epicondylitis – Case 2
• Clinical course (cont’d): Underwent formal course of OT following injection, with focus on strengthening. Discharged symptom free 1 month following injection. Reported recurrence 2 weeks later, but did not return to clinic for a month. Underwent another course of OT, including iontophoresis and ultrasound. No effect from OT.
Lateral Epicondylitis – Case 2
• Clinical course (cont’d): Underwent surgery via personal physician 10 months after presenting. Case accepted by workers’compensation, but authorization for surgery was denied under utilization review. Returned to work 4 months post‐op with no restrictions. One month later, complained of lateral elbow pain.
Carpal Tunnel Syndrome

Carpal Tunnel Prevalence
• Symptoms of tingling, numbness (+/- pain) in the median nerve distribution of the hand are common in general population (14.4%)
• Based on clinical exam and electrophysiologic testing, only about 2.7% of these have CTS
Atroshi, I. JAMA 1999;282(2):153-8.
55
Carpal Tunnel Diagnosis
Presumptive Diagnosis should have:• *Tingling or numbness in median nerve
distribution (two or more digits)• *Symptoms that are provoked either
nocturnally or with sustained grasp
Note – CTS does not necessarily produce hand or wrist pain. Pain often indicates a different diagnosis. Only pain is not CTS.
Katz JN. J Hand Surg 199056
Value of Phalen’s for Screening
NCV Status (L & R hands combined)Abnormal Normal
Phalen’s Pos
Neg
• Sensitivity = 29.3% Prevalence = 16.4%• Specificity = 86.3%• PPV = 30.2%• NPV = 85.7%
49 113
118 709

Value of Tinel’s for ScreeningNCV Status (L & R hands combined)
Abnormal NormalTinels Pos
Neg
• Sensitivity = 18.6% Prevalence = 14.7%• Specificity = 86.1%• PPV = 21.4%• NPV = 83.9%
Hegmann & Garg
31 114
136 708
Electrodiagnostic Testing • EDS for initial evaluation of CTS patients is Not
Recommended (Evidence I)• Not necessary as they do not change initial management of condition
• EDS is Recommended for Diagnosis and Pre-operative Assessment (Evidence C)• For patients without clear diagnosis (e.g., negative response to injection) or prior to surgical release
59
Ultrasound is NOT Recommended (I)
MRI is NOT Recommended (I)
Diagnostic Testing

Cohort Study Overview• 1. Prospective Cohort (18 Wisconsin, Utah
companies; n=1,223). Enrolled with Consent, Questionnaires, Structured Interview, Standardized Physical Examinations, Electrodiagnostic Studies
• 2. Job Physical Exposures measured (videotapes, measures, force matching, grip strength).
• 3. Monthly follow-up for changes in symptoms, status and treatments recorded. (no treatment given)
• 4. At least quarterly monitoring of jobs for job changes and re-quantify job measures as required
• 5. Every 6-month electrodiagnostic studies for symptoms (for CTS)
61
NCS Criteria• Boarded- PMR physician • Normals:• -Transcarpal delta <0.5 msec
-Motor latency <4.4 msec-Sensory latency <3.7 msec
Measured all, regardless of symptoms.
Methods cont. Case definition for CTS
Abnormal NerveConduction Velocity
Numbness/tinglingin any 2+ median
served digit(s)
+
Median Nerve - Yellow

Overall ResultsRight
1-month prevalence of T/N 36.2%Median Nerve Distribution T/N 30.5%Abnormal NCV (All) 29.5%Mildly abnormal NCV 18.6%Moderate/severe NCV 10.9%Positive Tinel’s Findings 14.5%Positive Phalen’s Findings 18.1%
65
This prelim report: Study Cohort
n = 451 eligible Subjects, n = 36 CTS cases
Mean enrollment time: 37.8 ± 21.28 (1.9 - 71.2) months65
66
Demographic VariablesVariable HR, p-value
Age 8.4, 0.037
Female 2.2, 0.057
BMI 4.0, < 0.001Family Hx
of CTS 2.0, 0.059
Inflamm. Arthritis 4.1, 0.002
Osteoarth. 2.1, 0.097
DeQuerv 3.8, 0.012
Variable HR, p-value
Trigger Dgt 2.5, 0.022
Lat. Epi 2.5, 0.016
Med. Epi 3.8, 0.012
Felt Depressed
7.5, 0.010
Job Dissat. 7.2, 0.016

67
Univariate Hazard RatiosMedical History
Variable Categories n(case) HR (Range), p-value
Sum of DUE MSDs ( p = 0.003)
012≥ 3
329 (17)78 (11)26 (5)18 (3)
---3.1 (1.45-6.60), 0.0044.0 (1.47-10.78), 0.0075.0 (1.45-17.06), 0.011
68
Univariate Hazard RatiosJob Physical Exposure Metrics
Variable Categories n(case) HR (Range), p-value
TLV for HAL(WRPE, Typical exposure)
(p = 0.373)
< 0.56≥ 0.56 to ≤ 0.78
> 0.78
93 (7)107 (5)251 (24)
---0.7 (0.13-1.52), 0.4551.2 (0.51-2.73), 0.656
69
Multivariate Hazard RatiosStrain Index
Variable Categories n(case) HR (Range), p-value
Strain Index(Typical exposure)
(p = 0.011)
≤ 6> 6 to ≤ 12> 12 to ≤ 18> 18 to ≤ 24
> 24
126 (7)122 (8)90 (10)20 (4)93 (7)
---2.3 (0.75-6.95), 0.1444.3 (1.50-12.45), 0.00710.0 (2.59-38.71), 0.0012.5 (0.81-7.81), 0.112

Work Limitations
• Indications – Select patients with combined forceful and repeated, stereotypical use of the hands or use of high amplitude vibrating tools. Of note, these types of jobs involve a minority of patients with CTS
• Indications for Discontinuation – Resolution, lack of improvement, or desire of the patient to remove limitations.
• Recommended, Insufficient Evidence (I)
Exercises for CTS patients
No recommendation for or against use of exercises (e.g., tendon-gliding) for treating CTS.
• No Recommendation, Insuff. Evidence (I)
Exercise is recommended for rehabilitation of post-operative CTS patients with significant deficits.
• Recommended, Insufficient Evidence (I)
Wrist SplintsNocturnal wrist splinting for acute,
subacute, or chronic CTS. (Stevinson 03)
Frequency – Splints while sleeping. No recommendation regarding daytime use (Walker 00; Manente 01; Werner 05; Premoselli 06; Gerritsen
02). (one study with improved electrodiagnostics, not symptoms and may alter posture and force). All splint trials with benefits. No head-to-head trials.
Discontinuation – Re-adjust splint if no response in couple weeks. If no improvement, splints should be discontinued and diagnosis revisited.
• Mod. Recommended, (B)

NSAIDsNSAIDs and acetaminophen
NOT recommended as primary treatment for subacute or chronic CTS. (Chang 98)
• Not Recommended, (C)
NSAIDs & Acetaminophen for post-operative CTS-related pain. (NSAIDs > Acetaminophen)
Mod. Recommended, (B) ○ placebo Δ NSAID-SR ● diuretic ■ steroid
Chang 1998
Oral GlucocorticoidsGlucocorticosteroids for chronic CTS
if decline injection. (Injection superior). (Wong 01)
Indication – Unresponsive to splinting. Injx rather than oral. Oral relatively contraindicated among diabetics.
Frequency/Dose – Dose and duration unclear! Trials used: 1) Prednisolone acetate 25mg/d x 10d;
2) Prednisolone 20mg/d for 2 weeks, then 10mg/d for 2 weeks;
3) Prednisone 20mg/d x 1wk, then 10/d x 1 wk;
4) Prednisolone 20mg/d for 2 weeks.
= oral group; Δ = injection group
Wong 2001
Oral Glucocorticoids
Some evidence 2 weeks as effective as 4 weeks.
One course (10 to 14 days) recommended, rather than repeated courses.
Prescriptions of low rather than high doses are recommended.
Moderately Recommended, Evidence (B)(Note: injections recommended as superior to oral forms)

Glucocorticosteroid Injections
Indications – CTS unresponsive to wrist splinting, generally >3 weeks. EDX not believed necessary prior to injections.
Dose – Unclear. o Methylprednisolone acetate (12,15,20,40,60mg),
o Betamethasone (6.0,6.4mg),
o Triamcinolone hexacetonide (20mg),
o Hydrocortisone (25, 100mg).
Glucocorticosteroid Injections
Higher doses (e.g., methylprednisolone 20mg vs. 40mg vs. 60mg) (Dammers 06, O’Gradaigh 00) result in minimal, slightly longer durations of benefit and non-significant improvements in outcomes.
Generally, methylprednisolone 20mg or equivalent as initial dose. Some increase dose in proportion to perceived symptom severity, but no quality evidence. Whether to use depot prep. unclear. Most include >1mL anesthetic (e.g., 1% lidocaine) allowing rapid assessment after injection.
Frequency/Duration – One injection scheduled. Results carefully documented. Even short-term believed prognostic.
No evidence series of injections effective. One study with series of 2 injections Not superior to 1.
No evidence limits to No. of injections for episode/lifetime.
Indications for Discontinuation – Second injection, typically moderately higher dose, may be indicated if partial relief, or if first injection thought to not be intracarpal.

If no partial response to injection(s), no recommendation for more injection(s).
Failures to partially respond, particularly if median nerve successfully anesthetized, are a priori suspected to Not have CTS. Thorough search for alternate diagnosis.
Patients responding, but redevelop symptoms believed to be ideal surgical candidates.
• Strongly Recommended, Evidence (A)
Glucocorticosteroid Injx.
Carpal tunnel injections recommended for treatment of acute CTS without fractures.
Acute CTS with fractures should be referred for potential emergent surgical release
•
Recommended, Insufficient Evidence (I)
Lidocaine Patches
Lidocaine patches are recommended for treatment of select CTS cases with pain.
• Indications – Moderate to severe CTS with pain as central complaint and after more efficacious treatments, such as splinting and glucocorticosteroid injection(s).
• Frequency/Duration – Usually 3/day. Caution regarding widespread use of topical anesthetics.
Recommended, Insufficient Evidence (I)

UltrasoundUltrasound for acute, subacute, or chronic
CTS.• Indications – CTS sufficiently symptomatic to
warrant treatment. Generally give splints and/or a glucocorticosteroid injection prior to considering ultrasound as appear more effective.
• Frequency – Regimen in highest quality study:Daily 15-minute sessions, 5/week x 2 weeks,
then 2/week for 5 more weeks; 1MHz with intensity 1.0W/cm2, pulsed mode duty cycle of 1:4 and transducer area of 5cm2. (Ebenbichler 98)
Another successful regimen consisted of 15-minute sessions, 5/week for 3 weeks. (Bakhtiary 04)
• Recommended, Evidence (C)
Iontophoresis, Phonophoresis
No recommendation for or against for treatment of acute, subacute, or chronic CTS. (1 weak, small negative ionto with dexamethasone study)
•
• No Recommendation, Insufficient Evidence (I)
OthersDiuretics Moderately Not Rec’d, (B)Low Level Laser Not Recommended, (C)Pyridoxine (vB6) Not Recommended, (C)Magnets Not Recommended, (C)Opioids Not Recommended, (I)Massage Not Recommended, (I)Acupuncture No Recommendation, (I)Manipulation No Recommendation, (I)Biofeedback No Recommendation, (I)

Carpal Tunnel ReleaseSurgical release Strongly
Recommended (A) for non-operative treatment failure with subacute or chronic CTS. (Dumontier 95; Agee 92; Trumble 02; Saw 03; Brown 93; Erdman 94; Sennwald 95; Ferdinand 02; Jacobsen 96; MacDermid 03; Atroshi 06, 09; Wong 03)
Also Recommended (I) for emergent or urgent indications (e.g., acute compression due to fracture, compartment syndrome with symptoms of nerve impairment).
•Gerritsen, JAMA 2002
Carpal Tunnel Release• Most should have had ≥ 1 steroid injection with
at least partial or complete relief then return of symptoms. If no steroid injection with at least partial benefit, should have electrodiagnostic study (EDS) consistent with CTS .
• Mild CTS with normal EDS exists, but clinical impression of moderate or severe CTS with normal EDS is very rare, generally mistaken diagnosis.
• Positive EDS in asymptomatic patients very common, is not CTS, suggests need to carefully select patients for EDS and properly interpret results.
• Strongly Recommended, Evidence (A)
Surgical Technique
• Open vs. Endoscopic – both are Recommended (A)
• Knifelight – Recommended (C)• Many adjunctive procedures reviewed, mostly Not Recommended.
87

Adjunctive procedures/approaches
Epineurotomy – Strongly Not Recommended (A)Internal Neurolysis – Strongly Not Recommended (A)Flexor retinacular lengthening – Not Recommended (B)Ulnar bursal preservation – Not Recommended (B)Superficial nerve sparing incision – Not Recommended (B)Flexor tenosynovectomy – Not Recommended (C)Ulnar incisional approach – Not Recommended (C)Biopsy of abnormal tenosynovium – Recommended (I)
88
Case 1Carpal Tunnel Syndrome
• 27 y/o RHD male• CC: Bilateral hand stiffness, swelling for 2‐3 mornings, better through the day; thumbs ache, burn
• Symptoms: States he “shakes” his hands to relieve numbness; limited nocturnal waking due to numbness; no neck pain
• PMH: Insulin using diabetic for 17 years
Case 1 – CTS
• Job history: Hired October ’07; recent jobs: 10 months metal finishing auto bodies (hand and machine grinding, sanding); at symptom onset, was 2 weeks rotating among 5 jobs, all using pneumatic guns to secure bumpers to ̴55 Newton‐meters torque; at time of visit: 4 weeks using a hoist, doing subassembly, using a nut runner (symptoms much improved)

Case 1 – CTS
• PE: No thenar atrophy; abductor pollicis brevis strength normal; positive Phalen’s and Tinel’s bilaterally; Right hand radiographs normal
Case 1 – CTS NCSPeak Latency Peak Amplitude
R median sens. 4.2 msec 23 μVR ulnar sens. 3.3 msec 29 μVR median motor 4.4 msec 9.1 mVR ulnar motor 2.9 msec 9.6 mVL median sens. 3.9 msec 31 μVL ulnar sens. 3.2 msec 27 μVL median motor 4.1 msec 12.9 mVL ulnar motor 3.3 msec 9.4 mV
Case 1 – CTSEMG Results
• Bilateral positive waves and fibrillation potentials (1+/1+) in the abductor pollicis brevis muscles, and increased insertional activity on the left

Case 1 – CTS
• Interpretation of NCS/EMG studies: Moderate to severe bilateral CTS with some axon loss most compatible with acute CTS. No evidence for diabetic neuropathy, cervical radiculopathy, or ulnar neuropathy.
• Clinical course: Treated with rigid wrist splints with instructions to use them during sleep. 1 month later, reports gradual improvement using splints, on different job, and 1 week off
Case 1 – CTS
• Subsequently found to have traveled by snowmobile over 100 miles during winter holiday break in December/January. He initially presented 3rd week of January. Workers’ compensation claim denied.
Case 2Carpal Tunnel Syndrome
• 55 y/o RHD female • CC: Acute onset of R hand/wrist pain after twisting her wrist throwing heavy trash bag; no direct trauma
• Symptoms: Radial wrist and hand pain; numbness in digits I‐III; Wakes up and “shakes” her hand to get the feeling back

Case 2CTS
• PMH: Denies previous similar problems; thyroid replacement since the 1980s; monitored q 3 months; No history of DM, RA
• Job history: 22 years school custodian• PE: Tender at FCR tendon insertion; No atrophy– What if her BMI was 33.2 kg/m2?
• NCS/EMG 3 weeks after presentation:
Case 2 – CTS NCS/EMG
Peak Latency Peak Amplitude
R median sens. 6.90 msec 5.1 μV
R median motor 6.95 msec 6.2 mV
L median sens. 4.70 msec 12.1 μV
L median motor 4.00 msec 8.9 mV
Case 2 – CTS
• Interpretation of nerve conduction studies and electromyography: Severe right and moderate left carpal tunnel syndrome
• Clinical course: Responded moderately well to nocturnal splinting; no response to physical therapy; Remains significantly symptomatic; working with restrictions
• Old medical records reveal NCS/EMG positive for CTS 2 years ago

Flexor Tendinoses and Trigger Digit
Flexor Tendinoses and Trigger Digit
Generally non-inflammatory with hypertrophy of A-1 pulley, narrowing of canal and resulting symptoms of pain and snapping of digit particularly with extension. (Moore 00; Saldana 01; Mulpruek 98; Ryzewicz 06; Troell 1921; Hauck 1910; Flörcken 1912; Finkelstein 1930)
• Spectrum from localized pain to triggering to locking. (Moore 00) Most common abnormality is A1 pulley thickening. Less common are abnormalities of metacarpal-phalangeal joint, carpal tunnel, and other pulley anomalies. (Moore 00)
Flexor Tendinoses and Trigger Digit
“As the epidemiological evidence is weak, the etiological fraction for occupational tasks is unknown. (Trezies 98) Thus, work-relatedness is somewhat unclear. (Melhorn 08) The available biomechanical evidence suggests pinch force may be a risk factor (Vogel 89; Ploetz 38; Hadji-Zavar 59; Compere 33; Hume 90; Hauck 23; Sperling 51; Zelle 36; Lapidus 52; Fahey 54; Lipscomb 59; Lenggenhager 69; Sairanan 57; Rayan 90; Moore
00; Sperling 51; Gorsche 98).”• Many cases reportedly idiopathic• Associated with diabetes mellitus, rheumatoid arthritis, CTS,
Dupuytren’s disease, osteoarthrosis, amyloidosis, hypothyroidism, heredity, and partial tendon laceration. (Fujiwara 05; Sperling 51; Rhoades 84; Buch-Jaeger 92;
Gottlieb 91; Yosipovich 90) May be connective tissue disorders. (Trezies 98; Saldana 01)
• Diabetes mellitus has worse prognosis for glucocorticosteroid injection. (Baumgarten 07; Nimigan 06)
102

No special tests typically performed. (Saldana 01; Moore 00)
X-rays usually unhelpful. Threshold for testing for diabetes mellitus, hypothyroidism, arthritic disorders should be low particularly to prevent other morbidity. (Moore 00; Saldana 01)
Initial care not well defined. “As quality evidence for efficacy of other interventions
is lacking and success of injections is strong, arguably, the initial management should be glucocorticosteroid injection.” (Nimigan 06)
Splints for select cases (i.e., declining injection). Splints used prior to advent of injection. Recommend patient education that injx much more effective.
• Recommended, Insufficient Evidence (I)
Exercise not generally indicated acutely and most do not require exercise program. For residual deficits, particularly post-operatively, exercise may be needed.
Trigger Digit: Injections
• Indications – Triggering digit or symptoms of pain over A-1 pulley consistent with stenosing tenosynovitis. Injection at first appointment may be best initial intervention. (Nimigan 06)
• Dose − Optimal dose unknown. Quality studies with:
• Betamethasone 6mg, (Baumgarten 07; Murphy 95)
• Depot prep. of methylprednisolone 20mg (Lambert 92);
• Triamcinolone “1mL” (Peters-Veluthamaningal 08)
• Most combined with anesthetic.

Trigger Digit: Injections
• No quality comparisons of doses. Need for topical anesthetic untested. Subcutaneous injection over A-1 pulley as efficacious as attempted intrasheath injection. (Taras 98)
• Frequency/Duration – Single injection and results evaluated to document improvement.
• Indications for Discontinuation – If partial response, consider repeating at modestly higher dose.
• Strongly Recommended, Evidence (A)
Trigger Digit: Surgery
• Open release or percutaneous release.• Indications – Triggering digit or symptoms of stenosing
tenosynovitis unresponsive to 1+ injection, or inadequate response. Those without any response should be evaluated for alternate conditions. Adjunctive surgical treatment with glucocorticosteroid injection could be considered, (Maneerit 03) although evidence is one moderate-quality study.
• Moderately Recommended, Evidence (B)
Trigger Digit– Case 1
• 40 y/o RHD male• CC: L little finger started to lock 2 months prior to presentation in October ’09
• Symptoms and history: Pain on palmar aspect of finger with triggering, occasional locking in flexion. No trauma. No tingling. No previous similar problems.
• PMH: DM for 13 years, on insulin pump.

Trigger Digit– Case 1
• Job history: 15 years in auto assembly plant. Symptoms began after 3 ½ months in current job. Rotates on 5 jobs: installs and secures seat belts using air guns to 35 N‐m of torque; positions mats and secures by pushing on pins using pinch grip; manipulates wire harnesses and secures them using pinch grip to seat clips. Work involves no direct pressure on MCP areas of palm but is hand intensive.
Trigger Digit– Case 1
• PE: Tenderness at the A‐1 pulley of the LLF. Triggering, but no locking on exam.
• Clinical course: Symptoms did not change during 2 weeks off for vacation/layoff nor after 3 weeks during the winter shutdown. Tried a fingerless glove with a padded palm without change. LLF locked in flexion. Underwent surgical release with full resolution of symptoms.
Trigger Digit– Case 1
• Further history: He did well for 3 months after resolution of his LLF symptoms, then reported with RMF triggering doing the same job. This was treated surgically 2 months after presentation and he returned to work. He continues to work in the same job without further problem.

Trigger Digit– Case 2
• 56 y/o RHD female• Symptoms: Fingers of L hand lock up x 2 months; insidious onset; no trauma
• PMH: Bilateral CTR 3 y ago with simultaneous multiple TF release on right hand; Symptom‐free since surgery. No RA, DM, thyroid disease.
Trigger Digit– Case 2
• Job history: 20 years airline call center; takes calls using a headset; variable, but often nearly continuous use of keyboard; No other hand‐intensive activities
• PE: Heberden’s nodes; tender at palmar II‐IV MCP joints; LMF triggers
Trigger Digit– Case 2
• Clinical course: No change in symptoms with splinting. Three week relief of symptoms after steroid injection at the A‐1 pulley; then symptoms recurred. Required subsequent surgical release with resolution of symptoms.

Thank You!!
Lateral Epi. Appendix
116
117
Descriptive statisticsDemographic Variables
Variable Categories n(case) HR (Range), p-value
Age(p=0.044)
Continuous (per year change) 385(53) 1.024 (1.001-1.048),
0.044
Age(p=0.043)
18-2425-3435-4445-5455+
55 (4)76 (6)97 (12)104 (24)53 (7)
1.0 (Reference)1.00 (0.28-3.53), 0.9951.54 (0.50-4.78), 0.4523.01 (1.04-8.69), 0.0411.66 (0.49-5.67), 0.419
Gender FemaleMale
240 (40)145 (13)
1.0 (Reference)1.80 (0.96-3.37), 0.066
Current Smoking
NoYes
251 (30)134 (23)
1.0 (Reference)1.77 (1.03-3.06), 0.039

118
Univariate Hazard RatiosMedical History
Variable Categories n(case)
HR (Range), p-value
High Cholesterol NoYes
338 (43)47 (10)
1.0 (Reference)1.87 (0.94-3.73), 0.075
Kidney Failure NoYes
384 (52)1 (1)
1.0 (Reference)13.74 (1.86-101.42),
0.010
No Association Demonstrated: Diabetes, Gout, Hypertension, Inflammatory Arthritis, Osteoarthrosis, Thyroid
119
Univariate Hazard RatiosMedical History
Variable Categories n(case) HR (Range), p-value
Medial Epicondylitis
NoYes
338 (42)47 (11)
1.0 (Reference)3.77 (1.14-11.81),
0.029
Non-Specific Pain
NoYes
355 (45)30 (8)
1.0 (Reference)2.35 (1.21-4.57), 0.012
No Association Demonstrated: deQuervain’s, Hand/wrist tendinitides, aggregate disorders, trigger digit
120
Univariate Hazard Ratiospsychosocial factors
Variable Categories n(case)
HR (Range), p-value
Felt Depressed
NeverSeldomOften
Always
98 (8)217 (30)65 (15)5 (0)
1.0 (Reference)1.91(0.88-4.17), 0.1043.80 (1.60-8.99), 0.002
*
Family Problems
NeverSeldomOften
Always
85 (8)219 (33)64 (8)17 (4)
1.0 (Reference)1.72(0.79-3.73), 0.1691.29 (0.48-3.44), 0.6113.34 (1.01-11.1), 0.049
* Not enough observations to create a stable Hazard Ratio Estimate
No Association Demonstrated: Physically exhausted, mentally exhausted, general health, employer cares, get along with coworkers, job satisfaction , recommend job to others, supervisor appreciates, take job again

121
Univariate Hazard Ratiosindividual Job Physical Exposure variables
Variable Categories n(case)
HR (Range), p-value
SI Intensity of Exertion
(Typical exposure)
Continuous (per unit change) 385 (53) 1.012 (1.000-1.023),
0.045
SI Intensity of Exertion
(Peak exposure)
Continuous (per unit change) 385 (53) 1.015 (1.003-1.03),
0.017
SI Posture(Peak exposure)
Continuous (per unit change) 385 (53) 1.24 (0.92-1.68), 0.161
Not Demonstrated (p>0.20): SI Efforts/min, Hours/day, % Duration, Speed of Work
122
Multivariate* Hazard Ratios
Variable Categories n(case)
HR (Range), p-value
Strain Index(Typical exposure)
≤ 6> 6
109 (10)276 (43)
1.0 (Reference)2.26 (1.12-4.56), 0.023
Strain Index(Peak exposure)
≤ 6> 6
105 (10)280 (43)
1.0 (Reference)2.12 (1.05-4.30), 0.036
*Adjusted for Age, Gender, Current Tobacco Use, Feeling Depressed, Prevalent Medial Epicondylalgia Diagnosis at Baseline
CTS Appendix
123

124
Descriptive statisticsDemographic Variables
Variable Categories n(case)
Mean ± S.D.or % (cases%)
Age Continuous 451 (36)41.5±11.67
Range 18.7 -68.1
Gender FemaleMale
293 (29)158 (7)
65.0% (80.6%)35.0% (19.4%)
BMI
Underweight (<18.5)Normal (18.5 - 24.9)Overwt (25.0 - 29.9)
Obese (≥ 30.0)
4 (0)175 (11)143 (9)129 (16)
0.9% (0.0%)38.8% (30.6%)31.7% (25.0%)28.6% (44.4%)
125
Descriptive statisticsDemographic Variables
Variable Categories n(case) HR (Range), p-value
Age(p = 0.006)
≤ 29> 29 - ≤ 41
> 41
82 (1)126 (7)243 (28)
---4.1 (0.50-33.19), 0.1888.4 (1.14-61.40), 0.037
Gender FemaleMale
293 (29)158 (7)
2.2 (0.98-5.09), 0.057---
BMI ≤ 33> 33
383 (22)68 (14)
---4.0 (2.05-7.81), < 0.001
Family Hx of CTS
NoYes
366 (25)85 (11)
---2.0 (0.98-4.03), 0.059
126
Univariate Hazard RatiosMedical History
Variable Categories n(case)
HR (Range), p-value
Inflammatory Arthritis
NoYes
428 (30)23 (6)
---4.1 (1.71-9.90), 0.002
Osteoarthritis NoYes
411 (30)40 (6)
---2.1 (0.87-5.05), 0.097

127
Univariate Hazard RatiosMedical History
Variable Categories n(case) HR (Range), p-value
deQuervain’s NoYes
431 (32)20 (4)
---3.8 (1.35-10.85), 0.012
Lateral Epicondylalgia
NoYes
387 (26)64 (10)
---2.5 (1.19-5.11), 0.016
Medial Epicondylalgia
NoYes
433 (32)18 (4)
---3.8 (1.34-10.75), 0.012
Trigger Finger NoYes
398 (28)53 (8)
---2.5 (1.14-5.51), 0.022
Sum of DUE MSDs ( p = 0.003)
012≥ 3
329 (17)78 (11)26 (5)18 (3)
---3.1 (1.45-6.60), 0.0044.0 (1.47-10.78), 0.0075.0 (1.45-17.06), 0.011
128
Univariate Hazard Ratiospsychosocial factors
Variable Categories n(case)
HR (Range), p-value
Felt Depressed(p = 0.005)
NeverSeldomOften
Always
109 (2)258 (24)79 (8)5 (2)
---5.3 (1.26-22.51), 0.0237.5 (1.63-34.00), 0.010
n/a*
Job Satisfaction(p = 0.080)
Very SatisfiedSatisfied
Neither NorDissatisfied
Very DIssatisfied
90 (3)235 (23)107 (7)17 (3)2 (0)
---3.1 (0.94-10.43), 0.0632.1 (0.54-8.07), 0.2877.2 (1.45-35.79), 0.016
n/a*
* Often and always, dissatisfied and very dissatisfied combined due to low sample size
129
Univariate Hazard RatiosRatings of Perceived Exertion (RPE)
Variable Categories n(case) HR (Range), p-value
Peak Worker’s RPE
(Typical exposure)
≤ 5> 5
386 (26)65 (10)
---2.4 (1.14-4.92), 0.020
Peak Worker’s RPE
(Peak exposure)
≤ 5> 5
383 (26)68 (10)
---2.3 (1.10-4.73), 0.027

130
Univariate Hazard Ratiosindividual Job Physical Exposure variables
Variable Categories n(case) HR (Range), p-value
Efforts per Minute(Peak exposure)
(p = 0.028)
≤ 14> 14 to ≤ 25
> 25
83 (4)144 (9)224 (23)
---1.1 (0.33-3.83), 0.8552.7 (0.94-7.80), 0.065
131
Univariate Hazard RatiosJob Physical Exposure
Variable Categories n(case) HR (Range), p-value
Strain Index
≤ 6> 6 to ≤ 12> 12 to ≤ 18> 18 to ≤ 24
> 24
126 (7)122 (8)90 (10)20 (4)93 (7)
---1.5 (0.53-4.37), 0.4423.2 (1.19-8.70), 0.0225.2 (1.47-18.60), 0.0102.0 (0.66-5.87), 0.226
132
Univariate Hazard RatiosJob Physical Exposure Metrics
Variable Categories n(case) HR (Range), p-value
TLV for HAL(WRPE, Typical exposure)
(p = 0.373)
< 0.56≥ 0.56 to ≤ 0.78
> 0.78
93 (7)107 (5)251 (24)
---0.7 (0.13-1.52), 0.4551.2 (0.51-2.73), 0.656
TLV for HAL(WRPE, Peak exposure)
(p = 0.128)
< 0.56≥ 0.56 to ≤ 0.78
> 0.78
84 (7)104 (4)263 (25)
---0.4 (0.13-1.52), 0.1961.2 (0.51-2.73), 0.701

133
Multivariate Hazard RatiosStrain Index
Variable Categories n(case)
HR (Range), p-value
Strain Index(Typical exposure)
(p = 0.011)
≤ 6> 6 to ≤ 12> 12 to ≤ 18> 18 to ≤ 24
> 24
126 (7)122 (8)90 (10)20 (4)93 (7)
---2.3 (0.75-6.95), 0.1444.3 (1.50-12.45), 0.00710.0 (2.59-38.71), 0.0012.5 (0.81-7.81), 0.112
Age(p = 0.146)
≤ 29> 29 - ≤ 41
> 41
82 (1)126 (7)243 (28)
---1.5 (0.16-12.87), 0.7373.3 (0.43-25.67), 0.251
BMI ≤ 33> 33
383 (22)68 (14)
---5.0 (2.50-10.31), < 0.001
Sum of Other DUE MSDs
(p = 0.146)
01-2≥ 3
329 (17)104 (16)18 (3)
---2.6 (1.27-5.35), 0.0095.1 (1.40-18.26), 0.013
Inflammatory Arth. NoYes
428 (30)23 (6)
---4.8 (1.81-12.72), 0.002
134
Multivariate Hazard RatiosStrain Index 5‐category Typical Exposure
Variable Categories n(case) HR (Range), p-value
Strain Index(Typical exposure)
(p = 0.011)
≤ 6> 6 to ≤ 12> 12 to ≤ 18> 18 to ≤ 24
> 24
126 (7)122 (8)90 (10)20 (4)93 (7)
---2.3 (0.75-6.95), 0.1444.3 (1.50-12.45), 0.00710.0 (2.59-38.71), 0.0012.5 (0.81-7.81), 0.112
Family Hx CTS NoYes
366 (25)85 (11)
---2.0 (0.93-4.29), 0.076
Gardening NoYes
209 (7)242 (29)
---3.5 (1.45-8.33), 0.005
Felt Depressed(p = 0.049)
NeverSeldom
Often/Always
109 (2)258 (24)84 (10)
---5.8 (1.34-25.22), 0.0196.5 (1.41-30.14), 0.016