Embed Size (px)
Citation preview

SEPTEMBER 2016 In collaboration with:
INTRODUCTION
Extensive progress has been made in the evaluation of South Africa’s new National Adherence Guidelines (AGL) for chronic diseases. After an extensive period of preparations, baseline assessment, patient file review and routine data enhancement at the selected health facilities, actual patient enrolment into the evaluation started in July 2016.
This brochure summarizes the findings from the baseline assessment in the 24 evaluation sites and
the first lessons drawn from preparing these health facilities for the evaluation.
Five AGL minimum package interventions are being evaluated under this study:
1. Fast track initiation counseling
2. Enhanced adherence counseling for unstable patients
3. Adherence clubs
4. Decentralized medication delivery
5. Early tracing of all missed appointments
The overall aims of the evaluation are to assess the
impact of these interventions on HIV patients’
treatment outcomes; estimate the costs of the
interventions; and describe the cascade of care for
TB, hypertension, and diabetes at these same
clinics. The study is a matched cluster randomized
study in 24 clinics, 12 of which will receive early
implementation of the minimum package and 12
will delay implementation and serve as control
sites. Clinics were matched on clinic characteristics:
total remaining on ART, clinic size, setting, location
and viral suppression. The two parts of the
evaluation – intervention effectiveness and process
of AGL scale-up—are detailed in two separate
protocols which have been approved by all
necessary bodies.
Teams have been hired by the academic partner
(Boston University/HE2RO) and put in place in
each of the four evaluation provinces chosen by
DOH, which are Gauteng, KwaZulu Natal, Limpopo
and North West. All evaluation activities are
specified in standard operating procedures.
The time scale of the evaluation is continuous
learning from scale-up and implementation, end-
2016 results on patient and health care workers
views (process evaluation), and effectiveness
results by late 2017.
The evaluation benefits for broad support by site-
level, district and provincial DOH staff and local
implementation partners at site and district level
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

2
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
DIVERSITY OF METHODS OF RECORDING AND STORING DATA One of the key findings has been the diversity of
methods of recording and storing data on patients
within the evaluation sites Ekurhuleni (Gauteng),
Mopani (Limpopo), Bojanala (North West) and
uThungulu (KwaZulu-Natal).
Facilities use a number of paper registers to track
vital information on patients within their clinics.
These include both standardised registers and
stationery (e.g. the PHC tick register, HIV patient
stationery, chronic patient record, TB treatment
record) and non-standard registers (e.g., for
counselling sessions, tracing, adherence club). Not
all clinics use all the standardized registers. There
is partial use of TB monitoring tools, such as the TB
register & sputum register (83% of facilities), the
notification of medical condition for TB (38%) and
the TB screening tool (38%).
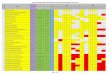
DATABASES AND REGISTERS IN USE AT EACH OF THE 24 EVALUATION SITES AS OF END DECEMBER 2015
CLINIC
EKURHULENI, GP MOPANI, LP BOJANALA, NW UTHUNGULU, KZN
Mo
tsam
ai
Ph
ola
Par
k
Kh
um
alo
Tam
aho
Ram
oko
no
pi
Zon
kizi
zwe
1
Gra
ce M
ugo
den
i
Giy
ani
Tzan
een
Mo
tup
a
Dzu
mer
i
Nko
wan
kow
a
Letl
hab
ile
Heb
ron
Wo
nd
erko
p
Maj
akan
eng
Tlh
aban
e
Baf
oke
ng
Kin
g D
iniz
ulu
Tho
koza
ni
Bu
chan
ana
Nkw
alin
i
Nse
len
i
Nta
mb
anan
a
DATABASES
TIER.Net x x x x x x x x x x x x x x x x x x x x x x x x
eHealth (Ekurhuleni District) x x x x
DHIS x x x x x x x x x
Lab-track (NHLS) x x x x
STANDARD REGISTERS
Headcount register x x x
PHC comprehensive tick register x x x x x x x x x x x x x x x x x x
HCT counselling and testing register x x x x x x x x x x x x x x x x x x
TB register x x x x x x x x x x x x x x x x x x x x
Sputum register (TB patients) x x x x x x x x x x x x x x x x x x x x
Notification of med. condition (TB) x x x x x x x x x
NHLS Specimen Shipping List Book x x x x x x
Daily clinic register (Pink register) x x x x x
Pre-ART register x x x
NON-STANDARD REGISTERS Counselling session register x x x x x x x x x x
Tracing register x x x x x x x x x x x x
Adherence club register x x x x x x
Chronic register x x x
STANDARD STATIONARY WITHIN PATIENT FILES HIV patients on treatment x x x x x x x x x x x x x x x x x x x x x x x x
Chronic patient record x x x x x x x x x
TB Treatment record x x x x x x x x x x x x x x x x x x x x x x x x
TB Screening tool x x x x x x x x x
Appointment/carrier cards x x x
All sites within the evaluation are currently using
TIER.Net (versions 1.8.3 and 1.8.4) meaning the data
are computerised and downloadable. TIER.Net will
provide the majority of the data for the evaluation
and there has been significant strengthening of these
routine data based on a diagnostic to maximise their
completeness.

3
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
THE IDEAL DATA FLOW IN A PHC CLINIC Given the number of registers, stationary and
clinical databases, it is essential for the evaluation
to understand how the data are generated and
registers are completed. The ideal flow of data is
illustrated below, and the routine data
strengthening activities are working towards this
ideal. Where a register or stationery is not used at a
clinic, alternative methods of recording may be put
in place (e.g., clinic or provider grown tools) or data
gaps may arise.
DATA FLOW PROCESS IN A PUBLIC SECTOR FACILITY

4
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
QUALITY OF COMPLETION OF REGISTERS Not all clinics use all the standardised registers and for
those that do, they are kept in various degrees of
completeness. Each of the listed registers contributes
data to the evaluation, if well completed.
QUALITY OF COMPLETION AND RELEVANCE FOR EVALUATION
STANDARD REGISTERS
PHC comprehensive tick register Varied level of completion. The major gap has been incomplete folder numbers for each patient. For the evaluation, this is a useful means to identify patients who were screened, diagnosed and treated for hypertension and diabetes.
HCT counselling and testing register Reasonable completion overall, but very limited on baseline CD4. For the evaluation this is a tool to understand linkages between HIV testing and ART.
TB register High level of completion in clinics using it.
Sputum register (TB patients) High in clinics using it. Headcount register High level of completion.
Daily clinic (pink) register Inconsistent recording of folder number, which is problematic.
Pre-ART register Extremely low completion. Not useful to evaluation due to limited completeness.
NON-STANDARD REGISTERS Counselling session register Varied use, AGL SOPs might lead to better use of a standard registers.
Tracing register Varied – inconsistent approaches and formats across facilities. Valuable to the evaluation to understand tracing success, if completed well.
Adherence club register Varied use, AGL SOPs might lead to standard and supported register.
Chronic register Varied and being phased out. It is a useful means to quickly identify patients who were screened, diagnoses and treated for hypertension and diabetes.
STANDARD STATIONARY WITHIN PATIENT FILES HIV patients on treatment High. There are concerning data gaps in terms of Viral Load recording, as well as completion of the
Social Assistance areas that may affect understanding of adherence.
Chronic patient record Varied completion. Unfortunately, this form is not widely available. TB Treatment record High completion. It provides information to understand the TB treatment experience.
TB Screening tool When completed the quality is high, but it is frequently not completed.
Appointment/carrier cards Inconsistent use (these are kept by the patient)
NATIONAL ID NUMBERS One key piece of data that is
incompletely captured is the national ID
number. Across the evaluation sites,
42% of active patients on TIER.Net had
their RSA ID recorded (January 2016). Of
all Tier.Net records (105,307), 23% were
active and with RSA ID.
North West and Gauteng had the lowest
completion rate of active patients with
North West facilities recording below
25%. This may be due to differing
numbers of patients with national IDs at
the sites (as non-South Africans would
not have an ID) but this limits the number
of patients for whom mortality can be
cross referenced with the national death
index.

5
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
DIVERSITY OF ADHERENCE SUPPORT MODELS One important insight from the baseline assessment
has been in the diversity of models for adherence
support. By end 2015, nearly all evaluation sites were
implementing the fast track initiation counseling
model, the tracing of patients who miss appointments
and adherence counselling for ART patients with an
unsuppressed viral load. However, there was high
diversity in the ways these models were being
implemented:
Enhanced adherence counselling were led by
professional nurses, lay counsellors or
community-based organisations. Some were
using the MSF Adherence Plan.
Tracing interventions varied greatly with some
sites tracing using phone calls only after varying
durations of time after a missed appointment,
and others implementing tracking using
community based outreach teams that also visit
homes.
The two interventions that were not being
implemented on a wide scale were adherence
clubs and decentralised medication delivery. For
the 12 sites using some form of adherence clubs
or decentralised drug delivery schemes, nearly
all were in KZN and following SOPs developed by
MSF. Some adherence clubs were multi-disease
clubs.
Decentralized medication delivery was only used
in KZN (1–13 pick-up sites).
Overall, adherence interventions were frequently
implemented in a way that differed from the AGL,
nevertheless, they were being implemented in some
form.
CLINICS IMPLEMENTING SOME FORM OF THE GUIDELINES PROPOSED IN THE ADHERENCE GUIDELINES
Overall, facilities in uThungulu/KZN provided the
highest number of these 6 key adherence services
with an average of 4.7 of the 6 services provided per
facility. Bojanala/NW facilities provided on average
2.2 of the 6 services, and Ekurhuleni/GP and
Mopani/LP facilities on average 1.7 and 1.8 of the 6
services, respectively.
CLINIC (C=control site)
Fast track initiation
counselling
Counselling for unsuppressed
VL
Decentralised medication
delivery Adherence clubs Tracing of lost
patients Fast lane
appointments
GA
UTE
NG
Motsamai X
Phola Park X X X X Khumalo X X X X
Tamaho (C) X X X
Ramokonopi (C) X X Zonkezizwe 1 (C) X X X
LIM
PO
PO
Grace Mugodeni X X X X
Giyani Tzaneen X X
Motupa (C) X
Dzumeri (C) X X Nkowankowa (C) X X
NO
RTH
WES
T
Lethabile X X X Hebron X X
Tlhabane X X
Wonderkop (C) X X X Majakaneng (C) X X
Bafokeng (C) X
KW
AZU
LU N
ATA
L King Dinizulu X X X X X Thokozani X X X X
Buchanana X X X X
Nkwalini (C) X X X X X Nseleni (C) X X X X X
Ntambanana (C) X X X X X

6
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
STATISTICS ON RE-ENTRY INTO CARE The evaluation sites were
also described in terms of
their retention in care
statistics of ART patients,
using TIER.Net data (as of 5
January, 2016). The number
of active ART patients over
the past 2 years (2014-
2015) was 78,569. A total
of 26,904 (34%) had a gap
of more than 90 days
between visits.
The diversity in retention
rates was considerable. In
all sites except three, the
main reason listed for a
patient being out of care is
being lost to follow up, at 50% or greater. Deaths
comprised no more than 10% of all patients out of
care, though in most sites this was collected through
passive reporting and may underestimate total
mortality. In some sites transfer was a major reason
for being out of care, being listed as high as 75% in
some sites in North West. In most other provinces,
transfers accounted for only 10-25% of patients out of
care.
VIRAL LOAD SUPPRESSION The baseline assessment also analysed viral load data
from each site for 2015.
The proportion of patients with a viral load
measure in the last 12 months varied greatly,
from 71% in Limpopo to 90% in Gauteng with
even greater variation at the clinic level
(range:40–99%).
The rate of suppression among those
with a viral load result also varied by
province with a low in North West of
67% to a high of 86% in KwaZulu Natal.
The assessment also found that time to
ART initiation was challenging to calculate,
mainly because pre-ART data was not
historically completed for all patients and
calculating the time between eligibility for
ART and date of initiation can be difficult.
Prior to starting data enhancement no
facility had more than 50% of records with
pre-ART dates and many facilities had little or no
information. Completion of pre-ART data was
subsequently addressed as part of data enhancement
and by the implementing partners to ensure that time
to initiation of treatment can be accurately and
correctly calculated for all HIV patients.
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
Gauteng KwaZulu Natal Limpopo North West
Viral load tests data by province (TIER.Net 2015 data)
Total active VL Taken last 12 mos VL Result VL Suppressed

7
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
CHRONIC DISEASE SCREENING AND CO-MORBIDITIES As part of the process of assessing the quality of data
being collected and putting in place a plan to
enhance routine data collection, a patient file review
was done at each site:
1. Verifying information captured in patient files
against what was recorded on electronic and
paper records and exploring how files were
linked - to establish data gaps and areas that
needed attention as part of the data
enhancement process.
2. Identifying TB, hypertension and diabetes
mellitus patients, and assessing whether newly
screened, diagnosed or treated patients could
be identified through existing registers for the
evaluation (and if not how to identify these
patient files).
The file review included patients from the chronic
and acute streams of the evaluation sites. A
convenience sample of 30-80 acute and chronic
patient files was reviewed. There were no estimates
done for Limpopo due to lack of file creation for non-
HIV chronic patients.
Out of 826 files reviewed, 76% (n=626) were
chronic patients, including 44% (n=360) HIV
patients, 2% (n=16) with a current diagnosis of
TB, 30% (n=249) prevalent hypertension
patients, and 8% (n= 66) prevalent diabetes
patients.
Of the files reviewed, 391 (47%) of clinic
patients were screened for TB, 338 (41%) were
screened for hypertension, and 89 (11%) were
screened for diabetes at their last visit.
Relative prevalence and comorbidities of this
convenience sample of clinic files:
Of the 360 HIV patients, 13% (n=47) had one
comorbidity (diabetes, hypertension, or TB),
and 1% (n=4) had two comorbidities.
Of the 246 HIV negative patients, three-
quarters (73%, n=172) had a hypertension
diagnosis, and nearly a quarter (22%, n=51)
were comorbid with hypertension and diabetes.
CHRONIC DISEASE PREVALENCE AND COMORBIDITIES FOR A CONVENIENCE SAMPLE OF CLINIC FILES NW, GP, KZN)

8
EVALUATION of the NATIONAL ADHERENCE GUIDELINES for CHRONIC DISEASE SEPTEMBER 2016
These results are somewhat comparable to results
for HIV positive patients in a study in Western
Cape, North West, Northern Cape and Limpopo
looking at all clinical encounters at selected
primary health care clinics i , but co-morbidity
being less frequent than in another South African
study which reported 30% of patients with two or
more comorbidities although patients tended to
be older. ii Taken together, this suggests our
estimates for comorbidity may be underestimated.
CONCLUSION AND OUTLOOK The process of engaging with the evaluation sites
has led to a number of key insights:
We have learned how the data flows work at
the participating health facilities in order for
data to go from patient interactions (point of
care) to a completed database (in electronic
form and downloadable).
Through site assessments and patient file
reviews at each evaluation site, we have
understood the quality and completion of
routine data and identified data gaps
We have determined the adherence
interventions/approaches in use prior to the
introduction of the AGL at the intervention sites
We have worked closely with the sites to
ensure good routine data collection
procedures through the enactment of data
improvement plans, in order to have the
outcome data required for the evaluation.
During evaluation site visits, we identified
challenges to implementing the AGL interventions:
These are relating to human resources (e.g.
staff shortages, not enough data staff),
equipment (broken SMS printers, lack of scales
and blood pressure cuffs), data systems (not
enough TIER computers, no space for filing) and
infrastructure (drug shortages).
There is a joint effort by DOH, local
implementation partners and the evaluation
team to resolve these challenges as they arise.
Data collection for the impact evaluation started
June 2016, and this part of the evaluation requires
no patient contact and relies fully on routinely
collected data at the evaluation sites. In includes HIV
patients, as well as TB, hypertension and diabetes
patients. The quality and completeness of the
routine data will be continuously monitored at each
facility throughout the period of the study.
Data collection for the process evaluation is ongoing
and will include surveys among HIV patients
receiving AGL services and health care staff providing
them.
Following the process of AGL introduction and scale-up of standardised AGL interventions in the
12 intervention sites has already provided valuable early learning for the national AGL scale-up.
For additional information, please contact: Mokgadi Phokojoe, Director Care and Support, National Department of Health ([email protected])
Nicole Fraser-Hurt, World Bank Group ([email protected])
i Lalkhen & Mash, 2015. Multimorbidity in non-communicable diseases in South African primary healthcare SAMJ 105; 134-138 ii Negin J, et al. Prevalence of HIV and chronic comorbidities among older adults AIDS 2012; 26 Suppl 1:S55–S63





















![· R[PbXUXRPS^b bTVd] [Pb _aX]RX_P[Tb \P]XUTbcPRX^]Tb R[X]XRPb$ R^\^ caPbc^a]^b ST _^cT]RXP$ _TaeTabX^]Tb bTgdP[Tb$ ]Tda^bXb ST P]VdbcXP$ ]Tda^bXb ^QbTbXePb$](https://img.pdfslide.net/doc/110x75/5c66928909d3f2d0218c80c9/-rpbxuxrpsb-btvd-pb-axrxptb-pxutbcprxtb-rxxrpb-r-capbcab.jpg)





