Embed Size (px)
Citation preview
Ultrasound in Med. & Biol. Vol. 18, No. 9, pp. 769-781, 1992 0301-5629/92 $5.00 + .00 Printed in the U.S.A. © 1992 Pergamon Press Ltd.
C H A I R 4
W O R S T - CASE ESTIMATES OF TEMPERATURE ELEVATION.
In Chapter 1 it is stated that harm from thermal causes will not occur in a diagnostic examination if the maximum in situ temperature rise does not exceed 1.5°C. Hence thermal safety can be assured if means can be found to determine and control the in situ temperature rise produced in a clinical procedure. In the absence of acceptable measurement techniques for doing this, the only feasible approach is through computations. In Chapter 2 it is pointed out that computations have been successful in specialized situations, but that difficulties are inevitable in clinical situations. Here uncertainties arise because of variations in anatomy as well as in thermal and acoustic properties of tissue.
In creating a computational model, assumptions are made about (1) the tissue, (2) the acoustic field, (3) the scanning regime and (4) the dwell time (the time during which a specific site is exposed). An exact model would precisely represent each of the above four conditions. However, an exact model is unattainable because of computational problems and inadequate knowledge of tissue properties. Instead, simplified worst-case models are used. These are intended to represent, as closely as possible, clinical situations of interest; however, they rely on conservative engineering approximations for the estimation of worst-case temperature elevations. Some caution is required in the formulation of such worst-case models, since the combinations of conservative engineering approximations can, in some instances, lead to highly improbable results that greatly overest imate the risk of heating. On the other hand, if the approximations are not conservative, safety cannot be adequately assured. Engineering approximations and a knowledge of their appropriate combination should improve in the future, leading to more accurate worst-case temperature estimates. The tissue models to be considered are as follows (see Table 4.1). (A more thorough discussion of tissue models in general is given in Chapter 3).
. Homogeneous Attenuating Medium. This model applies to many diagnostic applications. A modest perfusion rate, such as that associated with skeletal muscle, would give a reasonable worst case. A perfusion length of 1 cm, and corresponding to a perfusion rate of 1.5 kg m -3 s q (about 8 ml min ° lhg ' l ) would represent perfusion at a somewhat faster rate than in resting muscle (1).
. Fixed Attenuation Model. This model applies to examination of the embryo and the fetus in utero by a path through the abdomen (2,3). It represents worst-case
769
770 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
conditions by minimizing the attenuation of the ultrasound beam before impinging on the target tissue. The gestational age needs to be taken into account; see Chapter 3. The model also applies to intra- operative examinations and other situations in which a path through water or saline is interposed between the transducer and the interrogated tissue; here the "fixed attenuation" is zero.
. Soft-Tissue/Bone-Interface Model. This model is increasingly applicable to the examination of the fetus as the gestational age increases. It is also relevant to intracranial studies, and may also be appropriate for other situations (see Table 4.1). When bone is exposed to ultrasound, a higher temperature rise occurs (for a given set of exposure parameters) than if only soft tissue is exposed. In addition, if only a small area of a bone surface is exposed, the surface temperature of the bone quickly reaches its steady-state value, and capillary perfusion in the surrounding soft tissue may play an insignificant role in cooling the bone, as compared to cooling by conduction.
Applications for these models are suggested in Table 4.1.
Chapter 5 (Recommendations) includes a list of acoustical parameters which can be measured and which are needed in calculating temperature elevations in different situations. In the same chapter much reference is made to a derived quantity WDE C, which has been proven useful in the calculations. This quantity is here defined as the ratio, under selected conditions, of the acoustic power to ATlim, the latter being the maximum temperature rise produced under the conditions chosen. (ATIi m is the steady-state value of the temperature rise, i.e., the limiting value approached as time increases). Under linear acoustical conditions ATli m is proportional to the power W and WDE G is independent of W; then WDE G gives the power for which ATli m is equal to 1°C, and is sometimes called the "one-degree power". From its definition, it follows that ATIi m is given by;
ATli m = W / W D E G (1)
Of course, both W and WDE G m u s t be expressed in the same units of power. Numerous formulae for calculating WDE G are given in Chapter 5; these apply to different situations and are expressed in terms of the above-mentioned acoustical parameters.
ALGORITHMS FOR TEMPERATURE ESTIMATES.
Numerous publications describe mathematical models which have been developed and employed for estimating the temperature rise produced when the ultrasound beam from a diagnostic system propagates through tissue (1, 4-16)
Findings have been reported for different beam geometries and different tissue
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 771
SUGGESTED TISSUE MODEL
BEAM IN FIXED POSITION
BEAM IN 2D OR 3D SCANNING MODE
Homogeneous
Fixed attenuation
Soft-tissue/bone interface
Peripheral vascular PD, Endovaginal
Fetal vascular PD M-mode applied to fetus
Fetal PD Cardiac PD Transcranial
Obstetrics, 1st trimester General
Fetal imaging
Fetal imaging
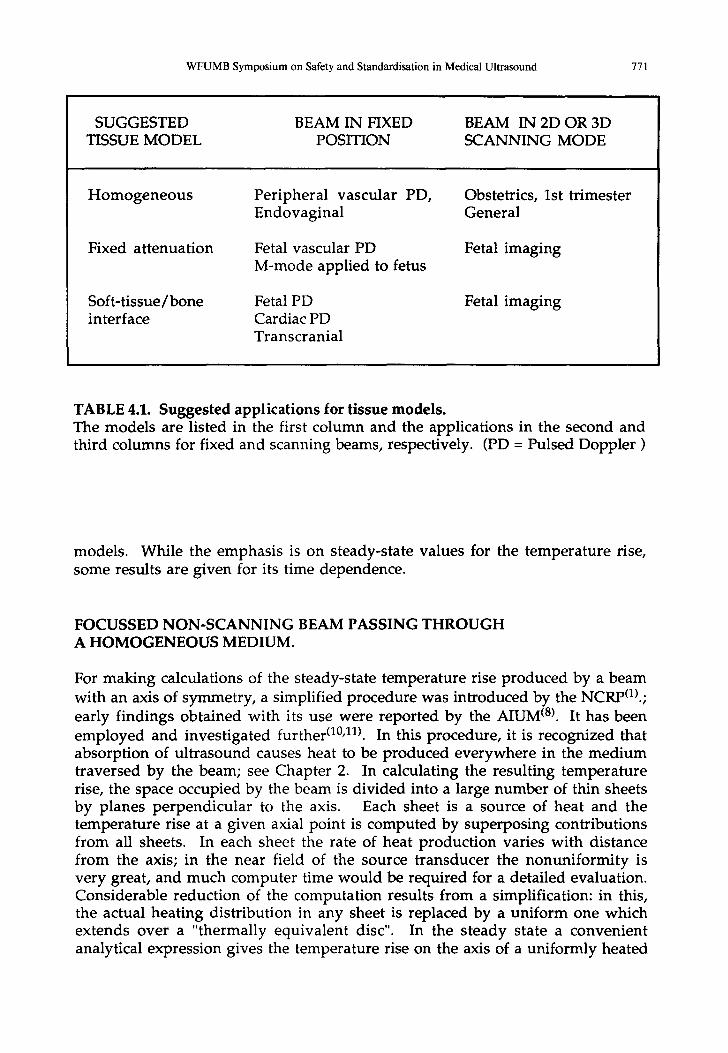
TABLE 4.1. Suggested applications for tissue models. The models are listed in the first column and the applications in the second and third columns for fixed and scanning beams, respectively. (PD = Pulsed Doppler )
models. While the emphasis is on steady-state values for the temperature rise, some results are given for its time dependence.
FOCUSSED NON-SCANNING BEAM PASSING THROUGH A HOMOGENEOUS MEDIUM.
For making calculations of the steady-state temperature rise produced by a beam with an axis of symmetry, a simplified procedure was introduced by the NCRp(1).; early findings obtained with its use were reported by the AIUM (8). It has been employed and investigated further (l°,n). In this procedure, it is recognized that absorption of ultrasound causes heat to be produced everywhere in the medium traversed by the beam; see Chapter 2. In calculating the resulting temperature rise, the space occupied by the beam is divided into a large number of thin sheets by planes perpendicular to the axis. Each sheet is a source of heat and the temperature rise at a given axial point is computed by superposing contributions from all sheets. In each sheet the rate of heat production varies with distance from the axis; in the near field of the source transducer the nonuniformity is very great, and much computer time would be required for a detailed evaluation. Considerable reduction of the computation results from a simplification: in this, the actual heating distribution in any sheet is replaced by a uniform one which extends over a "thermally equivalent disc". In the steady state a convenient analytical expression gives the temperature rise on the axis of a uniformly heated
772 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
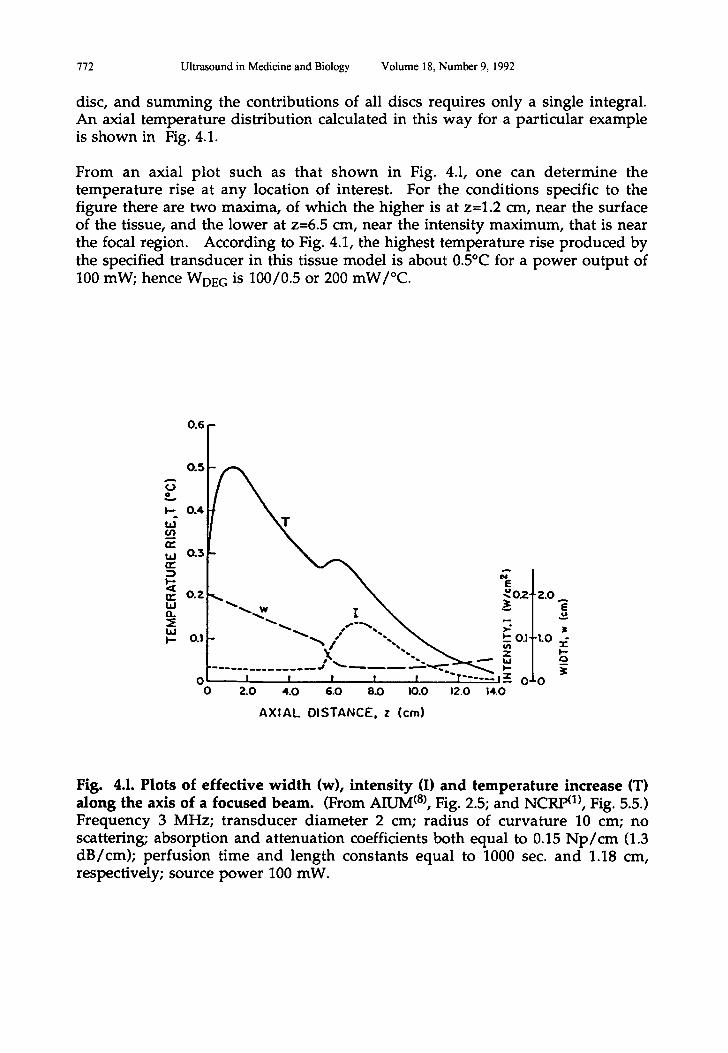
disc, and summing the contributions of all discs requires only a single integral. An axial temperature distribution calculated in this way for a particular example is shown in Fig. 4.1.
From an axial plot such as that shown in Fig. 4.1, one can determine the temperature rise at any location of interest. For the conditions specific to the figure there are two maxima, of which the higher is at z=1.2 cm, near the surface of the tissue, and the lower at z=6.5 cm, near the intensity maximum, that is near the focal region. According to Fig. 4.1, the highest temperature rise produced by the specified transducer in this tissue model is about 0.5°C for a power output of 100 mW; hence WDE C is 100/0.5 or 200 mW/°C.
A
(..3 =,%,
I.-
r.n n,," ILl n" :3
n,"
EL
t.cJ I '-
0 .4
0.:3
r " ,.o .,. / "--~ ,.---~. \
°-lJl-,.o o.11- ~'..., / "-,._ ~ ~
~ - - . . . . . . . . . . . . . "" ~ ' " - ~ ' - ' ~ " ~ ' - - ~ '- i 0 i I I I 1 f "T . . . . . . I ~ 0 0
O 2.0 4.0 6.0 8.O I0.0 12.O 14.0
A X I A L D I S T A N C E , z ( cm)
Fig. 4.1. Plots of effective width (w), intensity (I) and temperature increase (T) along the axis of a focused beam. (From AIUM (8), Fig. 2.5; and NCRP (1), Fig. 5.5.) Frequency 3 MHz; transducer diameter 2 cm; radius of curvature 10 cm; no scattering; absorption and attenuation coefficients both equal to 0.15 N p / c m (1.3 dB/cm); perfusion time and length constants equal to 1000 sec. and 1.18 cm, respectively; source power 100 mW.
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 773
Other plots of AT vs axial distance have been made for a wide range of conditions. Thomenius (1°), as background for an AIUM/NEMA (16) standard made computations of the steady-state temperature rise as a function of z for many values of the frequency f, the transducer diameter D and the radius of curvature R, all for a chosen value of the power W. For each he determined WD~ C, the ratio of W to the maximum temperature rise ATli m. Tables of results appear in a forthcoming report of the NCRP O), and a summary of his findings has been published (1°). Other determinations of AT vs z in a homogeneous medium under different conditions have been carried out (11'12'13'15). In all of the above publications the beam is assumed to be focused and the medium perfused to a specified extent. In a related earlier study, Nyborg and Steele (6) followed a similar approach but for an unfocused beam and an unperfused medium.
A general finding from the above studies is that the shape of a AT vs z curve is very dependent on the boundary condition and on other parameters. For the plot in Fig. 4.1 the boundary condition at z=0 is as if a medium existed for z<0 with thermal and acoustical properties identical to those of the real medium (which occupies the space z>0); however, no heat is produced in the space z<0 since there is no ultrasound field there. This condition applies roughly if the transmitted beam passes through water or saline before entering absorbing tissue. Another boundary condit ion applies if the "z<0 medium" is thermally insulating; this is approximately applicable when a transducer with epoxy coating is in contact with tissue. For this thermally-insulating condition, the maximum that occurs at z=1.2 cm in Fig. 4.1 shifts to the boundary and its magnitude is twice the temperature rise that occurs at z=0 under the "Fig. 4.1" boundary condition.
For many combinations of D, R and f (under the "Fig. 4.1" boundary condition) the near-surface maximum of AT (at z=1.2 cm in Fig. 4.1) dominates over the near-focus maximum, i.e., in Fig. 4.1, the one occurring at z=6.5 cm, near the position of highest intensity. Also, it is often true that the highest value of AT does not exceed twice the value of AT at z=0. (AIUM, 1988; NCRP, 1991). However, the nature of the AT maxima is strongly dependent on the f-number R/D. When the f-number is greater than three, the maxima remain separate with the near-surface maxima dominant, as described above. However (under the "Fig. 4.1" boundary conditions), as R decreases, thus causing the f-number to decrease (for fixed D), the near-focus maximum of AT moves nearer to the surface and its magni tude increases relative to that of the near-surface maximum. The two maxima may merge to yield a single maximum whose magnitude exceeds twice the value of AT at z=0 o0,11)
Equation 3 in Chapter 5 gives a formula for WDEG, obtained as an approximate fit (i.e., a multidimensional regression plane) to the data in the Thomenius tables referred to above, while Eqs. 1 and 2 in the same chapter give approximations to them with more restricted validity. These data and equations are for a homogeneous soft-tissue medium whose acoustical and thermal properties are as stated in Chapter 5. Higher values of the perfusion rate and lower values of the absorption coefficient lead to reduced values of ATli m.
774 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
Calculations of AT by the NCRP approach require more computation for finite values of the thermal exposure time than for steady-state ("infinite time") conditions. Determinations that have been made for a limited range of conditions show that the steady-state value ATli m can be considerably greater than the value of AT reached after, say, 3 minutes. A simplified model for estimating the spatial maximum of AT for finite time has been proposed O7). Formulae applicable to auto-scanned beams, developed for the AIUM/NEMA standard O6), are given in Equations 6 and 7 in Chapter 5.
FIXED-ATTENUATION MODEL FOR FLUID LAYER PATH PRECEDING SOFT TISSUE.
This model is introduced to account for the situations (i) where a focussed beam passes through a fluid medium in which the attenuation is negligible and (ii), in obstetrical applications, where the beam passes through a relatively thin layer of tissue with fixed acoustical properties, before entering and passing through a non-attenuating fluid layer and focussing on a soft tissue of interest that is being e x a m i n e d (2,3). This model applies, for example, (i) to ophthalmological diagnosis, (ii) to the employment of the full bladder technique, and (iii) to transcutaneous diagnosis of the uterus during pregnancy where there is a significant amniotic-fluid path between the transducer and the fetus.
Application to Exposure of the Embryo (First Trimester).
In the AIUM (8) and NCRP °) documents, "worst-case" tissue models for obstetrics are described, based on experimental determinations discussed in the report of the WFUMB second Safety Symposium O8). In these models the ultrasound beam is considered to be focused on the fetus, the beam width at the focus being "d". Estimates of WDE G for this model can, as for the homogeneous tissue model, be made either experimentally, or theoretically. In a theoretical approach it is recommended in N C R P (1) that an in situ value of WDE G for fetal exposure in the first trimester be calculated by a variation of the method used for Fig 4.1. By this method the beam as it enters the uterus is considered to be the same as if it originated at the entry point; the "effective source", unfocused, is of diameter d, and the source power is reduced from that of the original source by the attenuation along the prior path. Calculations of temperature rise are then made according to the same procedure used in Fig. 4.1, considering the same homogeneous model for the tissue. Again one may obtain the needed information from a full axial plot analogous to Fig. 4.1. Alternatively, the in situ value of WDE C can be obtained from published tables or formulae O,16). For the corresponding source output power, the in situ value would be corrected for the attenuation recommended in Chapter 3.
Application to Exposure of the Fetus (Second and Third Trimesters).
The soft-tissue model discussed in the previous section is considered applicable to examinations during pregnancy when the bony structures of the fetus have
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 775
not yet ossified. This applies also to the embryonic stage of development of the fetus. In the second and third trimester the worst-case calculation is based on the assumption that the ultrasound beam is focussed on bone, as described in the next section.
MODELS FOR ULTRASONIC HEATING OF BONE.
Among the various tissues of the body, bone is reported to experience the highest temperature rise when exposed to ultrasound. The mechanism for the heat product ion is not well understood, however. Although it is known that the a t tenuat ion coefficients for bone are very high, the relative impor tance of scat tering and absorpt ion has not been de te rmined for ei ther cortical or trabecular bone. Neither has the effect of angle-of-incidence on heat generation been adequately studied. Experimental investigations are reviewed (1) in which bone is exposed to ultrasound and the resulting temperature rise measured. The tempera ture rise at the surface of mature bone upon which u l t rasound is incident can approximate what it would be if half of all the energy incident on a bone surface were absorbed in a thin layer near the surface (1A9). In human fetal bone (femur) the temperature rise produced for a given incident intensity was found to increase with gestational age(I,2°); this increase was, in part, because of changes in properties of the bone material and, in part, because of increase in diameter of the femur.
One of the algorithms recommended in NCRP (1) is based on heating of mouse skull bone by an ul trasound beam focused on it. According to this the in situ value of WDE C, in milliwatts, is given by;
W D E G = 4 d 6 (2)
where d 6 is the 6 dB focal diameter of the beam in millimeters, and the beam is assumed cylindrically symmetrical. To obtain the corresponding value of WDEG in terms of the source output power, correction must be made for at tenuation along the prior path, as discussed in Chapter 3.
OTHER CONSIDERATIONS.
The algorithms in Eqs. 1 and 2 are based on solutions of the Bioheat Transfer Equation and on the assumption that linear acoustics holds. It is shown in Appendix C of the NCRP document (1) that the heating is considerably increased under some conditions as a result of nonlinear propagation, especially when part of the path is through a fluid whose attenuation coefficient is small. Chapter 6 takes up this topic.
Also, the algori thms in Eqs. 1 and 2 do not take into account the addit ional temperature rise which occurs because of self-heating within the transducer. This topic is taken up in Chapter 7.
776 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
APPLICATIONS OF WORST-CASE MODELS TO THE ESTIMATION OF TEMPERATURE ELEVATIONS PRODUCED BY DIAGNOSTIC EQUIPMENT.
Examples of est imates of temperature elevation in the fetus dur ing transabdominal pulsed Doppler examination have been given in a recent s tudy (21). In this study, manufacturers provided measured characteristics of ultrasonic fields for pulsed Doppler devices with spatial-peak time,average in tens i t ies , ISPTA, greater than 500 mW/cm 2. A total of 236 console/transducer/ operating-mode/intended-use combinations were analyzed. The calculations were based on appropriate combinations of the fixed-attenuation models for transabdominal examinations, first-trimester soft-tissue heating models, and the second and third trimester bone-heating models described above. These results are referred to below as "NCRP" results since they are based on the algorithms and calculations presented in the 1991 NCRP report (1). The method of calculation and estimates of uncertainties are given by Bly, et al. (21).
In addition, with the same database described above, results have been calculated for this report using the bone heating model adopted by the AIUM/NEMA Output Display Standard Committee (ODSC). In the ODSC model, WDEC was approximated by Eq. 2, but there was assumed to be a homogeneous soft-tissue path between the transducer and the bone. The attenuation coefficient of the tissue path was 0.3 dB cm-lMHz "1. Results calculated with this model are identified below as "ODSC". The temperature elevations are called ATli m for the NCRP calculations and TI (Thermal Index) for the ODSC calculations.
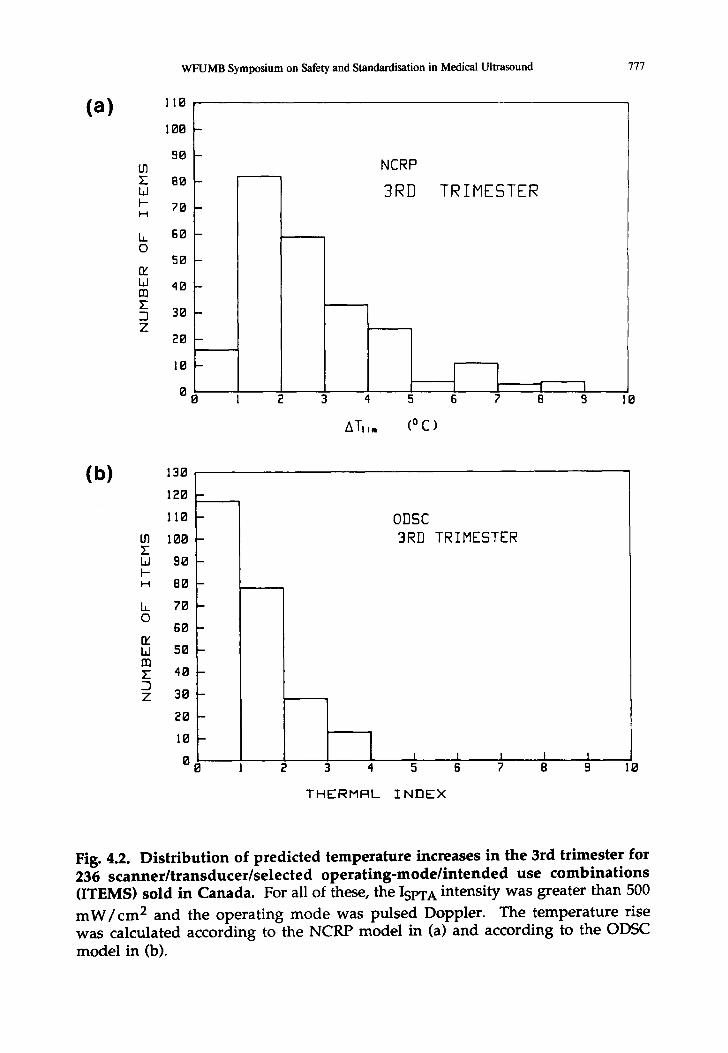
Safety considerations differed, depending on which model was used for the calculations. In the first trimester, the largest of the 236 calculated ATIi m values was 1.6°C, with the vast majority of ATl i m values being less than 1°C. Therefore (see Chapter 1), a thermal hazard could be ruled out for these devices in first- trimester examinations. For bone heating in the third-trimester fetus, the distribution of temperature elevations is shown in Figure 4.2. As shown in Figure 4.2(a), a significant number of items yields ATIi m values greater than the rise of 4°C which (see Chapter 1) is considered hazardous for dwell times of 15 minutes or more. As shown in Figure 4.2(b), a relatively small number of items yielded TI values approaching 4. These results indicated that, for a large number of cases, the calculated temperature elevations using the NCRP model provided assurances of safety. However, for some of the cases of fetal bone heating which were examined, the calculated temperature elevations and conclusions about the thermal hazard depended significantly on both the model and the transducer performance characteristics.
For a small number of the devices in the database described above, the calculated ATli m and TI values may be significantly underestimated due to limitations in the data reported by the manufacturers. A discussion of this subject is given (21) for the ATli m calculations. In order to compensate for this deficit in the results provided above and further assess the potential for fetal heating, calculations were performed for several transducers with defined frequencies and focusing
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 777
(a)
tO E 1,1 H H
b_ 0
rr L~ m Z -I Z
110
100
90
80
70
60
50
40
30
20
10
0
D
B
m
I
B
B
D
0
NCRP
3RD TRIMESTER
l i i 3 4 5 6 7 8 9
ATI ,. (0 C )
(b) 130
120
110
to 100 E Ld 90 H H 80
b_ 70 O
60 rr L~ 50
E 40 D Z 30
20
10
0 0 2 3 4 5
THERMRL INDEX
0DSC
3RD TRIMESTER
6 ? 8 9 10
Fig. 4.2. D i s t r i b u t i o n of p r ed i c t ed t e m p e r a t u r e increases in the 3rd t r imes te r for 2 3 6 s c a n n e r / t r a n s d u c e r / s e l e c t e d o p e r a t i n g - m o d e / i n t e n d e d use c o m b i n a t i o n s (ITEMS) so ld in Canada . For all of these, the ISPTA intensi ty was greater than 5 0 0
m W / c m 2 a n d the ope ra t i ng m o d e was pu l sed Doppler . The t e m p e r a t u r e rise was ca lcu la ted acco rd ing to the N C R P m o d e l in (a) and accord ing to the ODSC m o d e l in (b).
778 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
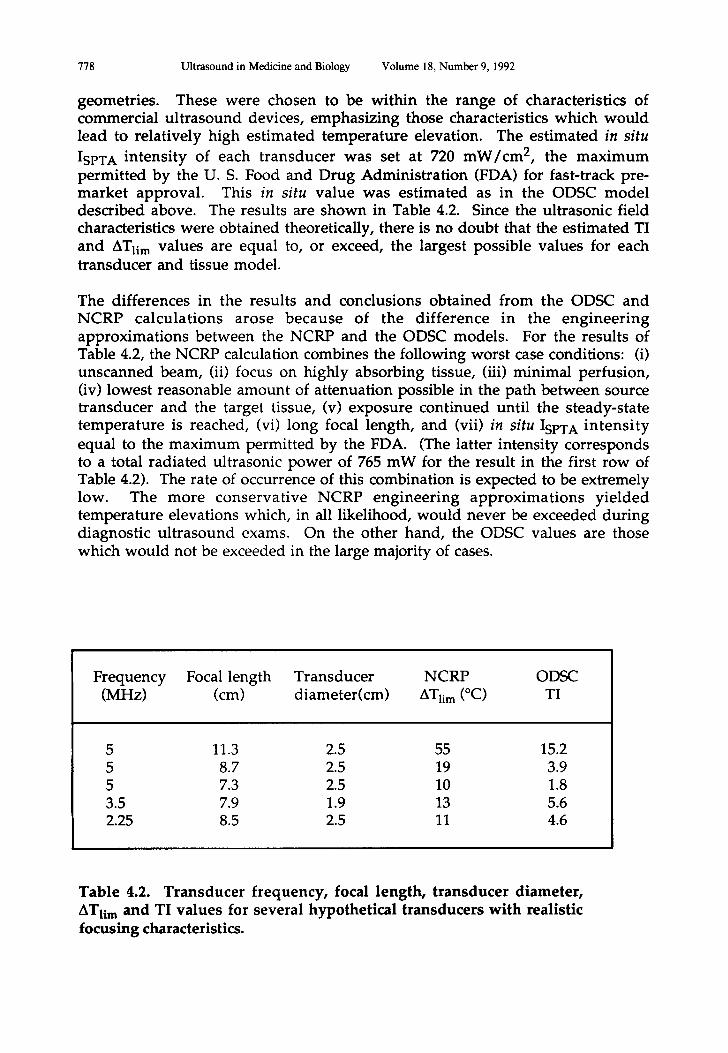
geometries. These were chosen to be within the range of characteristics of commercial ultrasound devices, emphasizing those characteristics which would lead to relatively high estimated temperature elevation. The estimated in situ
ISPTA intensity of each transducer was set at 720 mW/cm 2, the maximum permitted by the U. S. Food and Drug Administration (FDA) for fast-track pre- market approval. This in situ value was estimated as in the ODSC model described above. The results are shown in Table 4.2. Since the ultrasonic field characteristics were obtained theoretically, there is no doubt that the estimated TI and ATli m values are equal to, or exceed, the largest possible values for each transducer and tissue model.
The differences in the results and conclusions obtained from the ODSC and NCRP calculations arose because of the difference in the engineering approximations between the NCRP and the ODSC models. For the results of Table 4.2, the NCRP calculation combines the following worst case conditions: (i) unscanned beam, (ii) focus on highly absorbing tissue, (iii) minimal perfusion, (iv) lowest reasonable amount of attenuation possible in the path between source transducer and the target tissue, (v) exposure continued until the steady-state temperature is reached, (vi) long focal length, and (vii) in situ ISPTA intensi ty equal to the maximum permitted by the FDA. (The latter intensity corresponds to a total radiated ultrasonic power of 765 mW for the result in the first row of Table 4.2). The rate of occurrence of this combination is expected to be extremely low. The more conservative NCRP engineering approximations yielded temperature elevations which, in all likelihood, would never be exceeded during diagnostic ultrasound exams. On the other hand, the ODSC values are those which would not be exceeded in the large majority of cases.
Frequency Focal length Transducer NCRP ODSC (MHz) (cm) diameter(cm) ATIi m (°C) TI
5 11.3 2.5 55 15.2 5 8.7 2.5 19 3.9 5 7.3 2.5 10 1.8 3.5 7.9 1.9 13 5.6 2.25 8.5 2.5 11 4.6
Table 4.2. Transducer frequency, focal length, transducer diameter, ATli m and TI values for several hypothetical transducers with realistic focusing characteristics.
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 779
CONCLUSIONS.
Methods have become available for estimating the temperature rise produced by ultrasound in diagnostic applications. These are useful in showing the influence of various factors and for giving estimates of the maximum temperature rise. Even a formula of limited accuracy can be useful, for ruling out the possibility of thermal hazard, if (i) it is known that the actual temperature rise cannot exceed the calculated one, and (ii) the latter does not exceed the damage threshold for the tissue being examined. For example, the recommendations in Chapter 1 establish such thresholds for fetal exposures.
If the temperature rise calculated from a relatively simple algorithm of limited accuracy exceeds the damage threshold a more accurate algorithm should also be used, if available, to improve the confidence in the result. If the best available estimate of the temperature rise exceeds the damage threshold, the dwell time should be limited, using as guidance such data as those in Fig. 1.1.
.
.
.
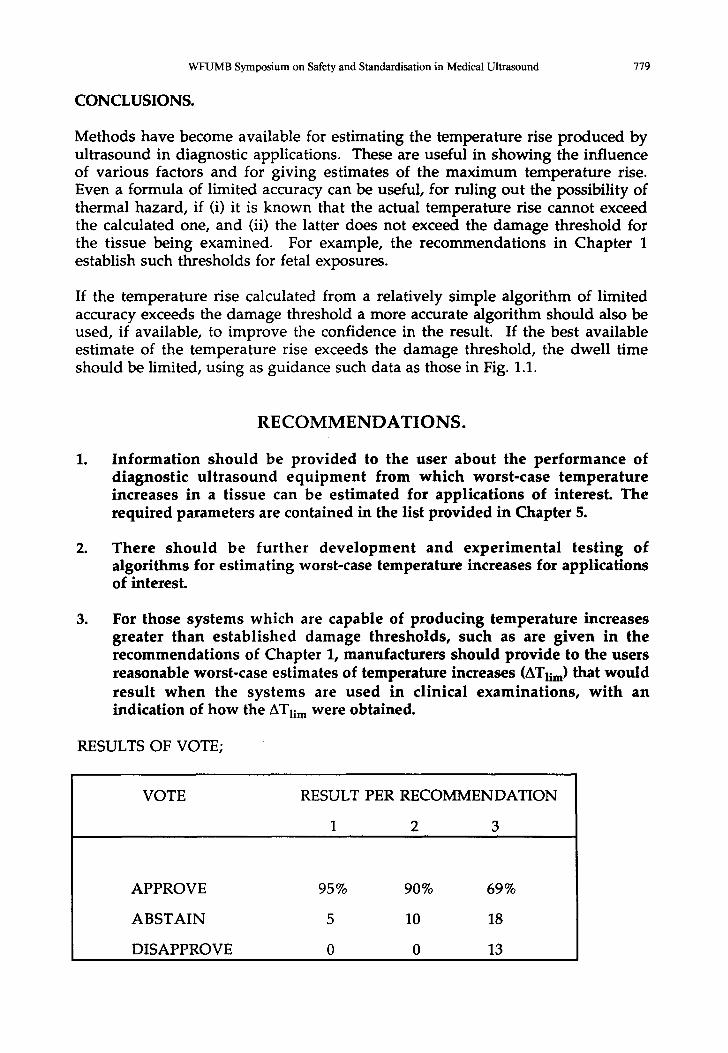
R E C O M M E N D A T I O N S .
Information should be provided to the user about the performance of diagnostic ultrasound equipment from which worst-case temperature increases in a tissue can be estimated for applications of interest. The required parameters are contained in the list provided in Chapter 5.
There should be further development and experimental test ing of algorithms for estimating worst-case temperature increases for applications of interest.
For those systems which are capable of producing temperature increases greater than established damage thresholds, such as are given in the recommendations of Chapter 1, manufacturers should provide to the users reasonable worst-case estimates of temperature increases (ATIi m) that would result when the systems are used in clinical examinations, with an indication of how the ATIi m w e r e obtained.
RESULTS OF VOTE;
VOTE RESULT PER RECOMMENDATION
1 2 3
APPROVE 95 % 90 % 69 %
ABSTAIN 5 10 18
DISAPPROVE 0 0 13
780 Ultrasound in Medicine and Biology Volume 18, Number 9, 1992
R E F E R E N C E S .
1. NCRP (1992) Exposure Criteria for Diagnostic Medical Ultrasound: 1. Criteria Based on Thermal Mechanisms. Report No. 113, NCRP Publications, Bethesda MD 20814, USA. (Some of the material developed for this report was made available to other organisations prior to its publication, and is included in references 8 and 18.) Carson, P. L., Rubin, J.M. and Chiang, E.H. (1989). Constant soft-tissue- distance model in pregnancy. Proc. 2nd World Federation Ultrasound Medicine Biology Symposium on Safety & Standardization in Medical Ultrasound. (Eds. G. Kossoff and W.L. Nyborg) Ultrasound Med. Biol. 15; Suppl. 1, pp. 27-29. Carson, P. L., Rubin, J.M. and Chiang, E.H. (1989) Fetal depth and ultrasound path lengths through overlying tissues. Ultrasound Med. Biol. 15, 629-639. Filipczynski, L. (1978) Temperature effect in soft tissue - estimated and measured. Proc. 2nd Congress Federation of Acoustical Societies Europe, Vol.II, FASE78, (Eds. Filipczynski, L. and Zienuik) Polish Academy of Sciences, Warsaw, pp. 23-26. NCRP (1983) Calculation of temperature elevation in a beam of ul t rasound. Appendix A, in; "Biological Effects of Ultrasound: Mechanisms and Clinical Implications", Report No.74 of the National Council of Radiation Protection and Measurements (NCRP Publications, Bethesda MD 20814, USA). Nyborg, W.L. and Steele, R.B. (1983) Temperature elevation in a beam of ultrasound. Ultrasound Med. Biol. 9; 611-620. Nyborg, W.L. (1987) Interaction mechanisms: heating, in; Ultrasound (Eds. M.H. Repacholi, M.Grandolfo, and A.Rindi,) Plenum Publishing Corporation, pp. 73-84. AIUM (1988) Bioeffects considerations for the safety of diagnostic ultrasound. Report of the AIUM Bioeffects Committee. J. Ultrasound Med. 7; S1-$38. Bacon, D.R. and Carstensen, E.L. (1990) Increased heating by diagnostic ultrasound due to nonlinear propagation. J. Acoust. Soc. America, 88; 26- 34.
10. Thomenius, K.E. (1990) Thermal dosimetry models for diagnostic ultrasound, in; Proc. IEEE Ultrasonics Symposium, pp.1399-1408.
11. Dore, G.R. (1990) Evaluation of a model for the prediction of temperature rise in tissue due to the absorption of ultrasound. NPL Report RSA(EXT)13, National Physical Laboratory, Teddington, Middlesex, TW11 OLW, UK.
12. Wu, J. and Du, G. (1990) Temperature elevation generated by a focused Gaussian beam of ultrasound. Ultrasound Med. Biol. 16; 489-498.
13. Wu, J. and Du, G. (1990) Temperature elevation in tissues generated by finite amplitude tonebursts of ultrasound. J. Acoust. Soc. America. 88, 1562-1577.
.
.
.
.
.
7.
.
.
WFUMB Symposium on Safety and Standardisation in Medical Ultrasound 781
14. Wu, J. and Du, G. (1990) Temperature elevation generated by a focused Gaussian ultrasonic beam at a tissue-bone interface. J. Acoust. Soc. America. 87; 2748-2755.
15. Wu, J. and Du, G. (1990d) Calculations of temperature elevation in tissues generated by finite amplitude tonebursts of ultrasound, in; "Frontiers of Nonlinear Acoustics", Proc. 12th International Symposium on Nonlinear Acoustics, (Eds. M.F.Hamilton, and D.T.Blackstock) Elsevier Applied Science, London, pp. 451-456.
16. AIUM/NEMA (1991) Standard for Real-Time Display of Thermal and Mechanical Indices of Diagnostic Ultrasound Equipment. American Institute Ultrasound Medicine, Rockville, MD; National Electrical Manufacturers Association, Washington, D.C. (final stage of preparation).
17. Filipczynski, L. and Wojcik, J. (1991) Estimation of transient temperature elevation in lithotripsy and in ultrasonography. Ultrasound Med. Biol. (in press).
18. WFUMB (1989) Proc. 2nd World Federation of Ultrasound in Medicine and Biology Symposium on Safety and Standardization in Medical Ultrasound. (Eds. G. Kossoff and W.L. Nyborg) Ultrasound Med. Biol. 15; Suppl. 1.
19. Carstensen, E.L., Child, S.Z., Norton, S. and Nyborg, W.L. (1990) Ultrasonic heating of the skull. J. Acoust Soc. America. 87; 1310-1317.
20. Drewniak, J. L. Carnes, K. I . and Dunn, F. (1989) In vitro ultrasonic heating of fetal bone. J. Acoust. Soc. America. 86; 1254- 1258.
21. Bly, S.H.B., Hussey, R.G., Mabee, P. and Vlahovich, S. (1992) Computed estimates of maximum temperature elevations in fetal tissues during transabdominal pulsed-Doppler examinations. Ultrasound Med. Biol. (in press).





























