Embed Size (px)
Citation preview
www.ias2011.org
The role of HIV stigma and discrimination on the health and HIV-
protective behaviors of people living with HIV in Rio de Janeiro, Brazil
Deanna Kerrigan, PhD, MPH Department of Health, Behavior, and Society
Johns Hopkins Bloomberg School of Public Health
www.ias2011.org
Stigma, Discrimination, HIV-Behaviors and
Outcomes• Stigma and Discrimination are recognized as
barriers to protective HIV-related behaviors and health outcomes e.g. access to HIV counseling & testing, HIV treatment, HIV medication adherence and overall well-being and quality of life of PLHIV
• Recently greater attention has been paid to the “layered” nature of stigma including the ways in which multiple forms of social stigmas and inequalities underlie and are associated with HIV stigma, discrimination & human rights violations
www.ias2011.org
Stigma as a Socio-Structural Process
• Stigma and discrimination related to HIV is understood here as a social process which produces and reproduces social divisions, hierarchies and unequal social structures:– Sexual Orientation– Gender– Race/Ethnicity– Class
www.ias2011.org
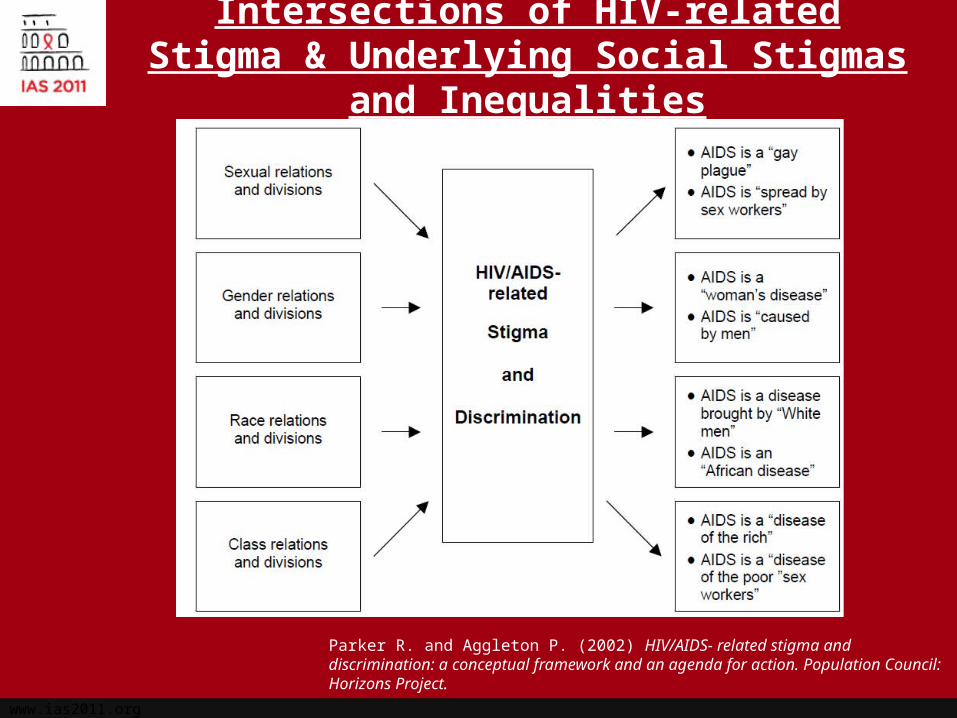
Intersections of HIV-related Stigma & Underlying Social Stigmas and Inequalities
Parker R. and Aggleton P. (2002) HIV/AIDS- related stigma and discrimination: a conceptual framework and an agenda for action. Population Council: Horizons Project.
www.ias2011.org
Specific Aims
– To examine the relationship between HIV stigma and discrimination and protective health behaviors and outcomes among a diverse sample of PLHIV attending public clinics in Rio de Janeiro, Brazil• Reported health, care adherence, HIV medication adherence,
consistent condom use, and reported STIs since diagnosis
– To assess how other forms of underlying social stigmas intersect with HIV stigma and discrimination among a diverse sample of PLHIV attending public clinics in Rio de Janeiro, Brazil• Gender, sexual orientation, income, race/ethnicity, sex work,
drug use, incarceration
www.ias2011.org
Brazilian Context
Brazil is leader in rights-based HIV prevention, treatment & care:
First lower to middle income country to establish universal access to treatment
Battle against stigma and discrimination central to national response to HIV in Brazil
Relatively limited research on HIV stigma and discrimination among PLHIV in Brazil
www.ias2011.org
Study Setting, Population & Sampling Strategy
• Government-run public health clinics providing treatment and care to PLHIV in Rio de Janeiro
• Clinics (6/22) selected to ensure social and geographic diversity within greater Rio area
• Sample of 900 PLHIV– Specific targets to capture demographic
characteristics and diversity of clinics– Gender, sexual orientation, and % on ARVs
www.ias2011.org
Methods
• Structured survey to assess psychosocial and structural factors associated with HIV behaviors and health outcomes among participating PLHIV– Approximately 1 hour, private setting at clinic
• STI screening: Syphilis, Gonorrhea, Chlamydia– FTA-ABS syphilis & PCR analysis for GC
• Medical Record Extraction: CD4 count, viral load, opportunistic infections, hospitalizations
www.ias2011.org
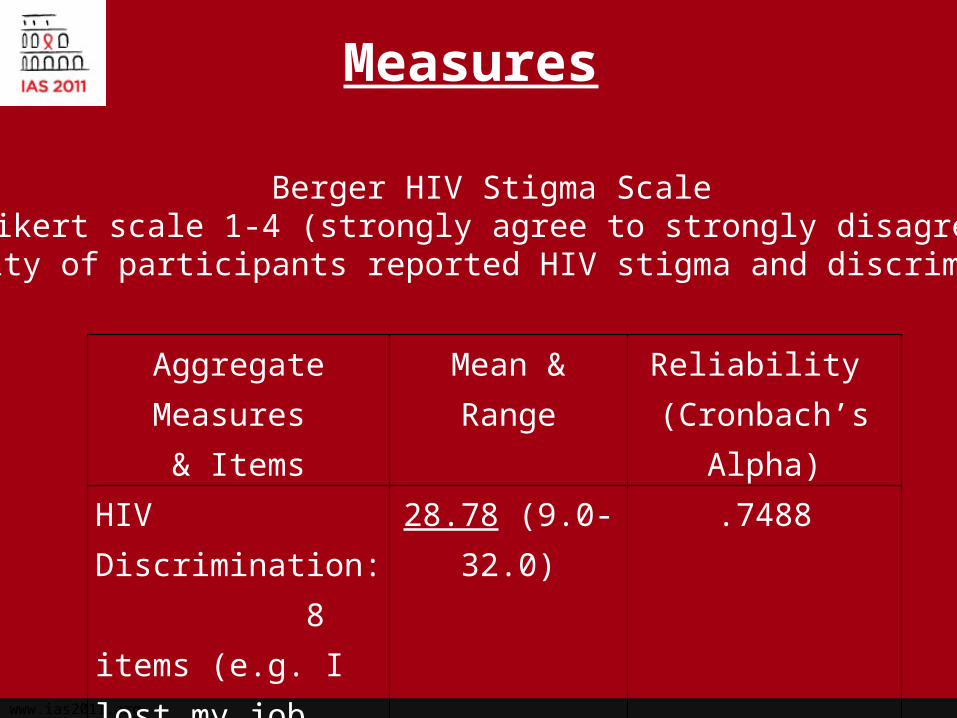
Measures
Aggregate Measures & Items
Mean & Range Reliability (Cronbach’s Alpha)
HIV Discrimination: 8 items (e.g. I lost my job because of HIV)
28.78 (9.0-32.0) .7488
HIV Stigma: 8 items (e.g. I feel guilty because of HIV)
25.46 (8.0-32.0) .7545
Berger HIV Stigma ScaleLikert scale 1-4 (strongly agree to strongly disagree)
Minority of participants reported HIV stigma and discrimination
www.ias2011.org
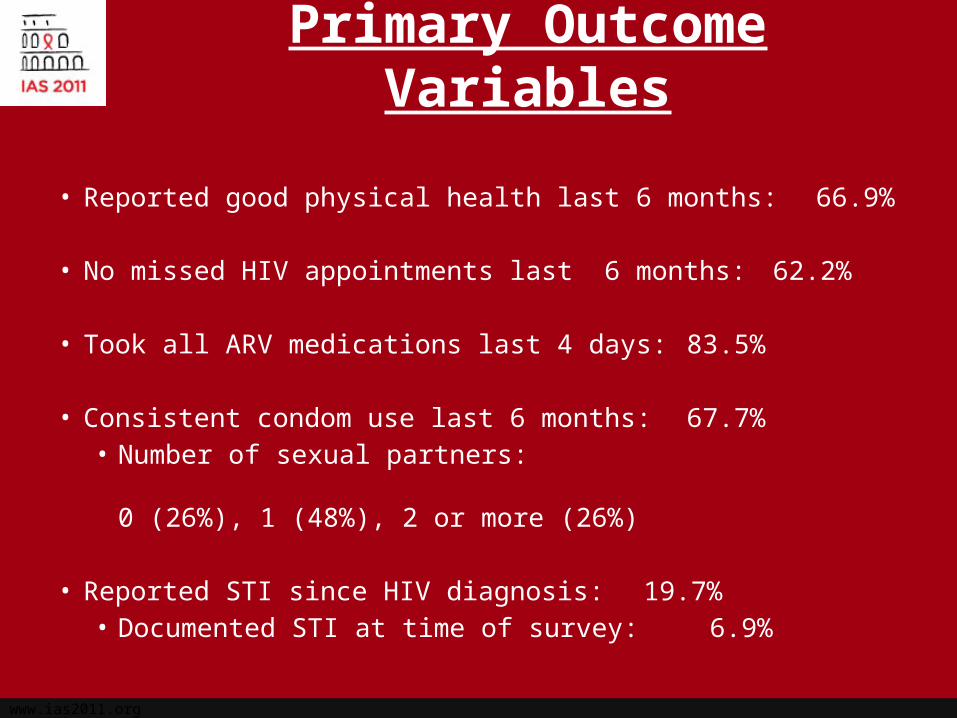
Primary Outcome Variables
• Reported good physical health last 6 months: 66.9%
• No missed HIV appointments last 6 months: 62.2%
• Took all ARV medications last 4 days: 83.5%
• Consistent condom use last 6 months: 67.7%• Number of sexual partners:
0 (26%), 1 (48%), 2 or more (26%)
• Reported STI since HIV diagnosis: 19.7%• Documented STI at time of survey: 6.9%
www.ias2011.org
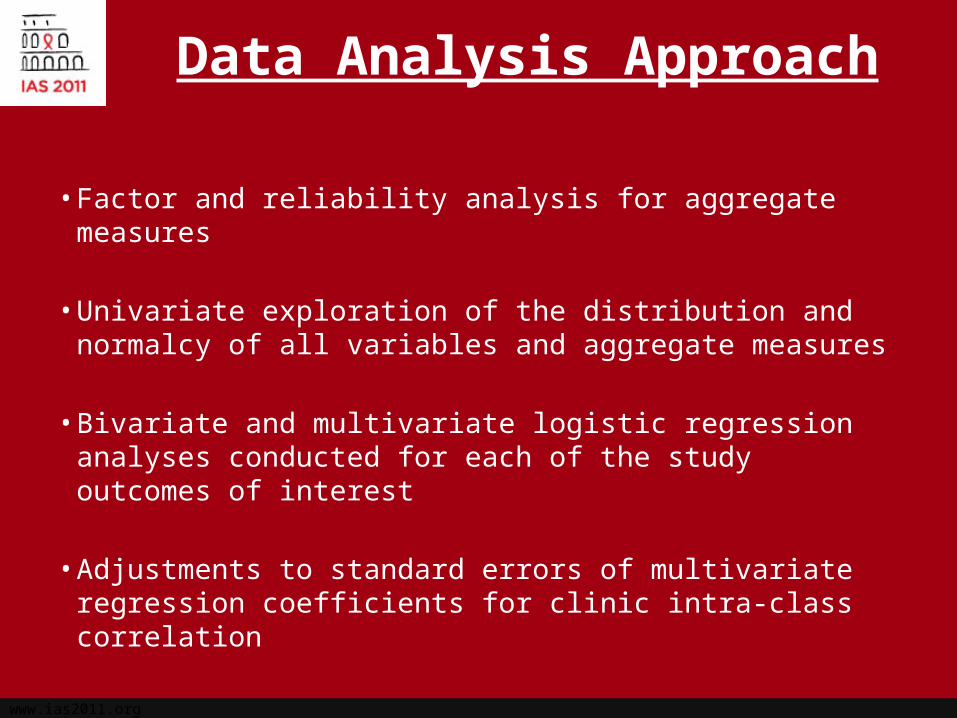
Data Analysis Approach
• Factor and reliability analysis for aggregate measures
• Univariate exploration of the distribution and normalcy of all variables and aggregate measures
• Bivariate and multivariate logistic regression analyses conducted for each of the study outcomes of interest
• Adjustments to standard errors of multivariate regression coefficients for clinic intra-class correlation
www.ias2011.org
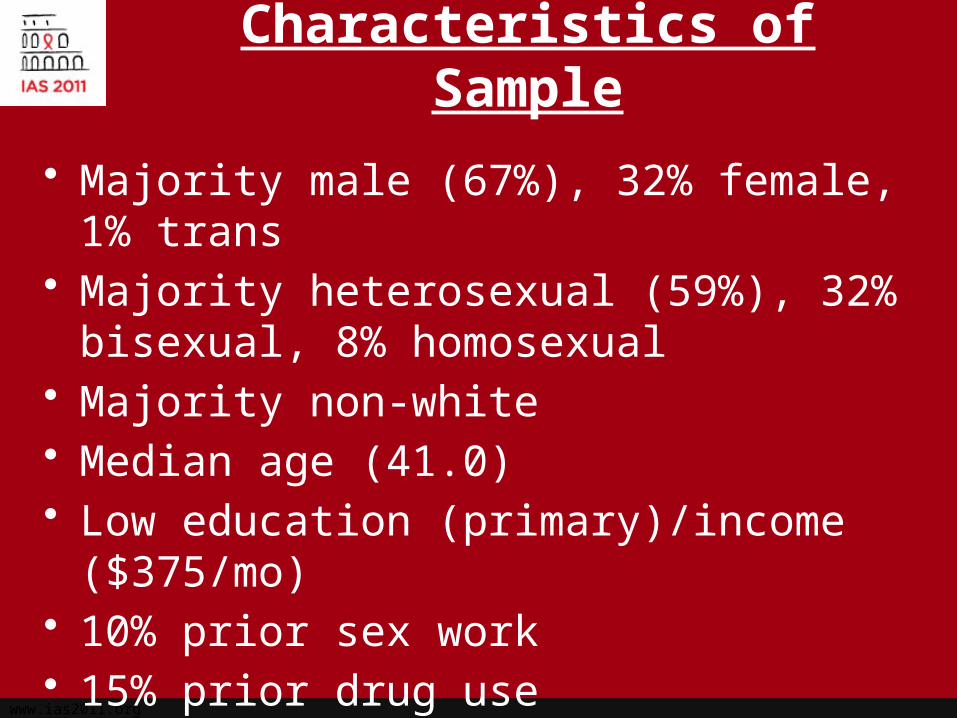
Characteristics of Sample
• Majority male (67%), 32% female, 1% trans• Majority heterosexual (59%), 32% bisexual,
8% homosexual• Majority non-white• Median age (41.0)• Low education (primary)/income ($375/mo)• 10% prior sex work• 15% prior drug use• 75% of sample on ARVs
www.ias2011.org
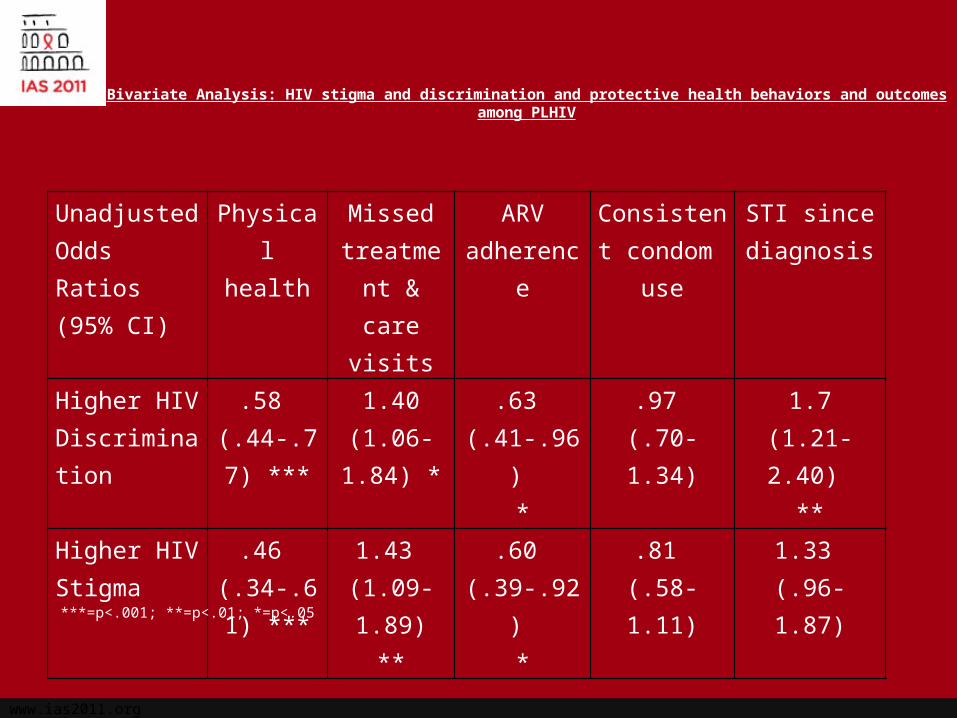
Bivariate Analysis: HIV stigma and discrimination and protective health behaviors and outcomes among PLHIV
Unadjusted Odds Ratios (95% CI)
Physical health
Missed treatment
& care visits
ARV adherence
Consistent condom use
STI since diagnosis
Higher HIV Discrimination
.58 (.44-.77)
***
1.40(1.06-1.84)
*
.63 (.41-.96)
*
.97 (.70-1.34)
1.7(1.21-2.40)
**
Higher HIV Stigma
.46 (.34-.61)
***
1.43 (1.09-1.89)
**
.60 (.39-.92)
*
.81 (.58-1.11)
1.33 (.96-1.87)
***=p<.001; **=p<.01; *=p<.05
www.ias2011.org
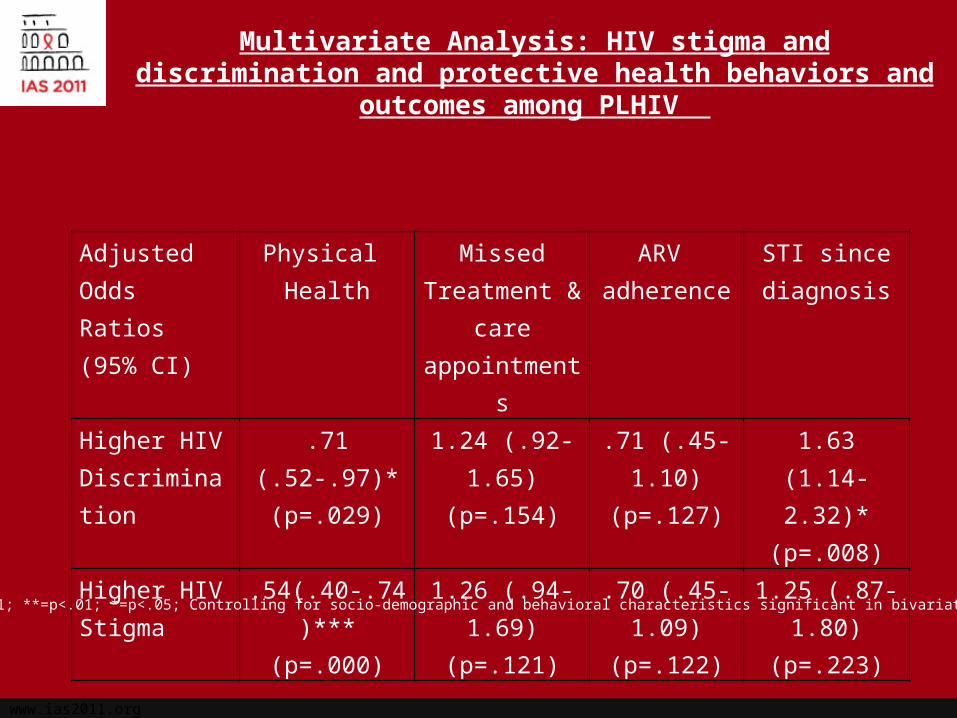
Multivariate Analysis: HIV stigma and discrimination and protective health behaviors and outcomes among PLHIV
Adjusted Odds Ratios (95% CI)
Physical Health
MissedTreatment &
care appointments
ARV adherence
STI since diagnosis
Higher HIV Discrimination
.71 (.52-.97)*(p=.029)
1.24 (.92-1.65)(p=.154)
.71 (.45-1.10)(p=.127)
1.63 (1.14-2.32)*
(p=.008)Higher HIV Stigma
.54(.40-.74)***(p=.000)
1.26 (.94-1.69)(p=.121)
.70 (.45-1.09)(p=.122)
1.25 (.87-1.80)(p=.223)
***=p<.001; **=p<.01; *=p<.05; Controlling for socio-demographic and behavioral characteristics significant in bivariate analysis
www.ias2011.org
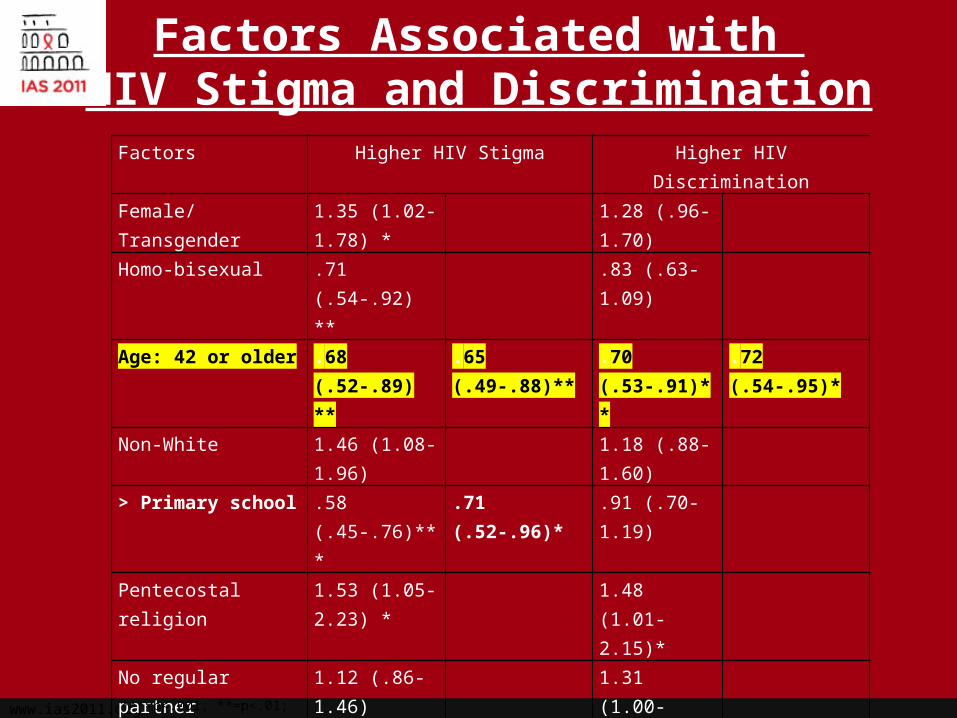
Factors Associated with HIV Stigma and Discrimination
Factors Higher HIV Stigma Higher HIV Discrimination
Female/Transgender 1.35 (1.02-1.78) *
1.28 (.96-1.70)
Homo-bisexual .71 (.54-.92) ** .83 (.63-1.09)
Age: 42 or older .68 (.52-.89) ** .65 (.49-.88)** .70 (.53-.91)** .72 (.54-.95)*
Non-White 1.46 (1.08-1.96) 1.18 (.88-1.60)
> Primary school .58 (.45-.76)*** .71 (.52-.96)* .91 (.70-1.19)
Pentecostal religion 1.53 (1.05-2.23) *
1.48 (1.01-2.15)*
No regular partner 1.12 (.86-1.46) 1.31 (1.00-1.71)*
One or > child(ren) 1.63 (1.25-2.12) ***
1.65 (1.14-2.39)**
1.10 (.85-1.44)
Income: > 600 R .60 (.45-.78) *** .74 (.55-.99)* .61 (.47.80)*** .62 (.46-.82)**
No prior sex work .52 (.33-.83) ** .56 (.35-.90)* .60 (.38-.93)*
No prior drug use .69 (.47-1.01) .62 (.43-.92)* .63 (.42-.95)*Not on ARVs .95 (.71-1.28) 1.38 (1.03-
1.86)*1.56 (1.14-2.14)**
***=p<.001; **=p<.01; *=p<.05;
www.ias2011.org
Discussion
• HIV stigma and discrimination are relatively low among PLHIV attending public clinics in Rio de Janeiro, Brazil
• Significant associations documented in multivariate analyses between HIV-related stigma and discrimination and reported physical health as well as HIV-related discrimination and reported STIs since diagnosis
• HIV stigma and discrimination are associated with underlying social stigmas and inequalities e.g. poverty, sex work, drug use and are greater among younger people
• Being on ARVs is protective against HIV discrimination
www.ias2011.org
Conclusions
Findings from this study indicate the importance of addressing multiple, overlapping social stigmas among PLHIV to improve their health and well-being and reduce ongoing HIV transmission
Brazil has led the way in combating HIV stigma and discrimination, however, challenges still exist particularly among marginalized population groups
Socio-structural interventions focused addressing the multiple dimensions of stigma and discrimination experienced by PLHIV particularly those from marginalized groups are needed Evaluations of multi-level interventions to promote linkages to care,
protective HIV-related behaviors and reduce HIV/STI transmission
www.ias2011.org
Acknowledgements
Co-investigators: Francisco Bastos, MD, Monica Malta, PhD,Neilane Bertoni, MPH, Oswaldo Cruz Foundation, The Rio Collaborative Group
Thanks to study participants, clinic personnel, the study team and to the Ford Foundation





























