Embed Size (px)
Citation preview

Tiirkish Neiirosiirgery 8: 28 - 35, 1998 Türkmen: Intercorpora/ Fixation
SPINAL INSTRUMENTATION
IntercorporalStabilization
System:Thoracolumbar
Spinal StabilizationDevice for
A NewFixation
Yeni Bir Omurga SabiHeme. Sistemi: Torakolomber SabiHeme IçinOmurga Cisimleri Arasina Yerlestirilen Tespit Cihazi
CENGIZ S. TÜRKMEN, IBRAHIM M. ZIYAL, ALPER R. KAYA, OSMAN TÜRKMENOGLU,.. ..
YUNUS AYDIN, ILGAZ DOGUSOY, KA YA OZKUS, AHMET UNAL, MUZAFFER BASAK
Sisli Etfal Hospital Department of Neurosurgery (CT, IMZ, ARK, OT, YA), Siyami Ersek Thoracic and CardiovascularSurgery Center Department of Thoracic Surgery (ID), Istanbul University Cerrahpasa Medical Faculty Department of
Anatomy (KÖ), Yildiz Technical University Department of Metallurgical Engineering (AÜ),Sisli Etfal Hospital Department of Radiology (MB), Istanbul, Turkey
Abstract: Anterior intercorporal fixation, different fromthe currently used techniques, was test ed as a newstabilization system first in human cadaver and then wasapplied to a patient. Our device is a two directional screwsystem applied with anterolateral approach to the superiorand inferior corpus end plates along the vertical axis ofcolumna vertebralis. This system which is composed oftwo screws with their fixing washers preventing rotationalmovement, and a connector was tested in human cadaversfollowing animal trials. Its advantage over the otherdevices stems from its positioning into the corpus, thecenter ofaxial compressional loads, in the same directionas the force vectoro This has been verified by means ofbiomechanical experiments and was applied the n to apatient with Ll burst fracture. it is suggested that anteriorintercorporal fixation with our device is suitable for routineclinical use due to its higher strength, simplicity andpracticality in applications as compared to the othersystems.
Özet: Günümüzde kullanilan tekniklerden farkli ve yenibir sabitleme sistem olarak, önden omurga cisimleri arasitespit önce insan kadavrasinda denendi, sonra bir olguyauygulandi. Cihazimiz, anterolateral yaklasimla üst ve altomurga cismi kikirdak tabakalanna omurga sütununundikeyekseni boyunca uygulanan iki yönlü vida sistemidir.Bu sistem, dönme hareketlerini engelleyen pullari ilebirlikte iki vida ve bir baglanti parçasindan olusmaktadirve hayvan çalismalarini takiben insan kadavralarindadenenmistir. Diger cihazlara göre yarari, omurga cismiiçindeki durumunun, eksensel basi kuvvetlerininmerkezinde ve kuvvet vektörleri ile ayni yönde olmasidir.Bu çalisma, biyomekanik deneyler neticesinde, Ll patlamakirikli bir olguya uygulanmistir. Sonuç olarak, öndenomurga cisimleri arasi tespit cihazi, yüksek direnci, kolayve pratik uygulanabilir olusu nedeni ile rutin klinikkullanim için tavsiye edilmektedir
Key Worrls: Anterior instrumentation, intercorporalfixation, stabilization, thoraco-lumbar
Anahtar Sözcükler: Omurga cisimleri arasi tespit, öndencihaz takrna, sabitlerne, torako-lomber
INTRODUCTION
The main treatment of spinal instability is toprovide fusion for the alignment of the naturalanatamical construction. The accepted view to reach
this goal and to gain early mobilization is to providespinal stabilization via spinal instrumentation. Thereexist anterior stabilization systems, posteriorstabilization systems and anterior distraction systemscurrently in use today. Although these systems have
28
Turkish Neurosurgery 8: 28 - 35, 1998
advantages and disadvantages over each other anideal system that can resist spinal multivectoralforces is not yet available (16,17).
The currently used spinal stabilization systemsdisplay failures especially due to the axial androtational direction of spinal multivectoral forces.Without the aid of a block bone graft, it is impossiblefor the posterior and anterior fixation systems toresIst the axial forces. The corpus of the vertebra Isthe region that carries most of the axial forces. Inorder to achieve the maximum effidency in resistingloads the stabilization instrument should be placedparallel to the axis of the applied forces. Regardlessof the system used, cyclic axial compressional loadslead to metal fatigue. Failures occur in the existingfixation systems as theyare subjected to loads atright angles. The technical faults during applicationof the block bone graft also cause failure. Accordingto the authors, whatwould ensure greater successin the elimination of the perpendicular forces bychanging the alignment of the device with respectto the vertebra.
The main disadvantage of posterior andanterior fixation systems is that theyare exposed toforces in perpendicular direction espedally underthe axial compression loads. On the other hand thedisadvantage of the anterior distractor systems islack of fixations. Our device, developed with theprinciple of anterior intercorporal fixation, achievedhigh resistance particularly against axialcompressional loads, and allows for satisfactoryfusion.
Anterior intercorporal fixation is composed ofscrews that are applied vertically into the corpus atthe mids of the intact upper and lower corpus endplates, rota tion-preventing washers that are nailedto the same locality following the application of thescrews, and a connector. Thus, maximum strengthis obtained in the direction of the axial force vector.
MATERIALS AND METHOD
Deseription of the System:
Our device consists of two standart spongiousscrews, two rota tion- preventing washers, aconnector, and two connector- fixing screws thatconnect the spongious screws to the connector, allmade of stainless steel or titanium. Our device isdeveloped to be used in thoradc and lumbar regionsin ord er to gain stabilization following singlesegment corpectomy.!f needed, there are differentconnector sizes which can be used in case of
Türkmen: Intercorpora/ Fixation
multisegmental anterior and middle columninsuffidency. Moreover, by attaching extensionsto both spongious screws multisegmentalstabilization can also be achieved. Spongious screwsfor thorade and lumbar regions are of a standardlength of 25 mm, with a tapered shaft (maximumdiameter of 5 mm ). The extension pieces have astandard length of 10 mm. In order to ensureinterlocking in the system, the bottom section of theconnector-fixing screw which goes into the connectoris threaded.
The rota tion- preventing washer is a plaquewith 12 mm width and 22 mm length, with two 17mm nails inserted into the corpus. On this plaque,on both sides of the ho le which the spongious screwgoes through, are small holes meant for maximumfusion. The connector is of 10 mm diametercylindrical shape with 8 mm slots on both ends forthe insertion of connector- fixing pieces, and iscompletely threaded on the surface. The connectoris available in different sizes so that it can be applieddepending on the distance that arises followingcorpectomy ( the smallest 25 mm, the largest 80 mm).Af ter completing the connections, the system islocked by tightening the octagonal nuts on theconnector (Figure 1).
Biomeehanieal Tests
The ma terial used in biomechanicalexperiments was made of an austenitic stainless steel(DIN 174431,4441,X2CrNiMo 18 15 3).
a. Compression Test: A uniaxial compressiantest was carried out on the implant sample. The testwas conducted according to the ASTM E9 (12). Thespedmen was observed to tear at 2300 kp (22,5 kN).
b. Bending Test: Since the joints of the implantare exposed to bending und er actual conditions thesepoints were subjected to three points bending testsaccording to ASTM E6 and ASTM E8 (12). Maximumbending load was observed to be 220 kp (2158 N).
e. Notehed Impad Test: This test is used tomeasure the energy absorbed by the materials whensubjected to impact loads or during fracture underimpact. The tests were conducted according toASTM E23 by using a Zwick test machine (12). Themeasured impact energy was 4,6 kmp (46]).
d. Fatigue Test: This test measures the lifetime of material before failure under cyclic loading.Tests were conducted according to DIN 51228by usinga Denison Test machine. Measurement was made
29
Turkish Neurosurgery 8: 28 - 35, 1998 Türkmen: Intercorparal Fixation
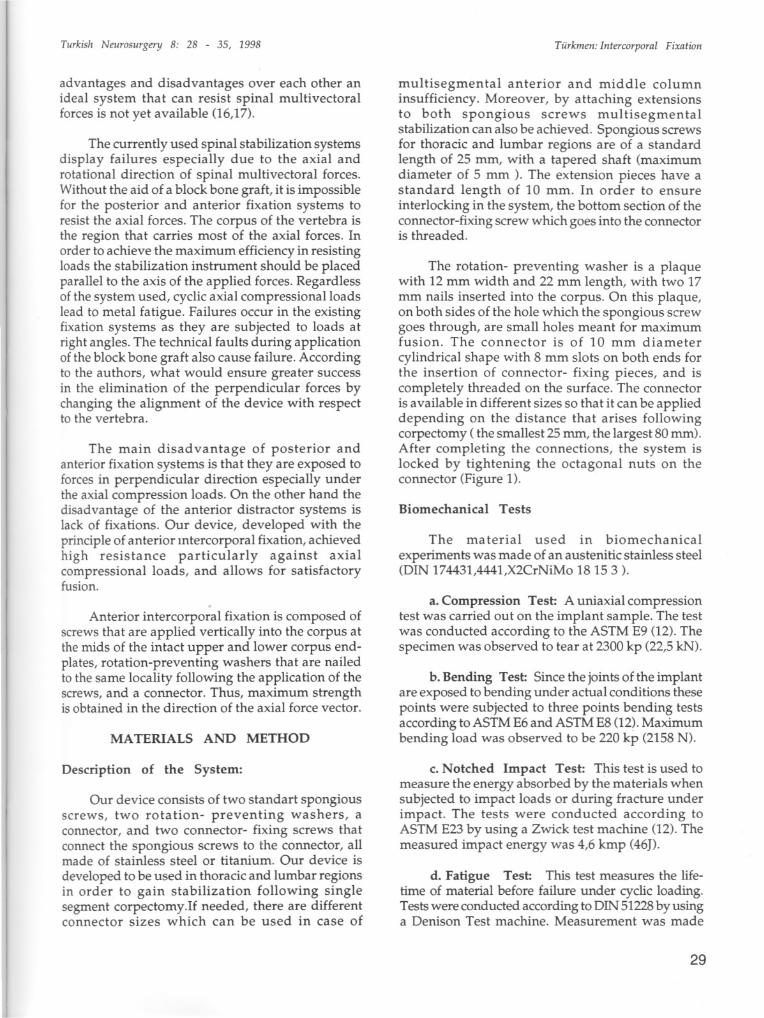
Figure1,a,b: TheAnterior Intercorporal FixationDeviceconsistsof two standard spongious screws, two rotation preventingwashers, a connector, and two connector fixing screws that connect the spongious screws to the connector.
according to four different models with followingresults:
a) 24'forward, 6'backward (Pmax=56,3kg(550N), Pmin=14,lkg(138N)failure at14.000 cycle (l4x1000)
b) 12'forward, 6' backward(Pmax=28,lkp(276N),Pmin= 14,1kp(138N)failure35,OOOcycle(35x1000)
c) 12'forward (Pmax=28,l kp(276N),Pmin=0)failure at 45.000 cycle (45x1000)
d) Lateral deflechon 9'forward, 6'backwardfailure at 56.000cycle(56x1000)
e. Torsion Test: These tests were conducted
und er uniaxial vertical loading by using 2N and 343N with a torquemeter. In these tests the device didnot exhibit failure. Instead, the failure criteria wasthe onset of tear in the sample vertebra. The resistanceagainst the torsional load increased 41 % when thetear length reached 5.11 mm. The reason for this wasthought to be jamming of the trabecules. Changingthe uniaxial load from 2N to 343N seemed to haveany apparent effect on the test results.
Tearing was observed at 3047 Nmm.Tear reached 5.11 mm at 4733 Nmm.
No biomechanical study was conducted onimplants made of titanium.
Cadaver Studyand Application
In this study, the device was applied to 11cadavers following choosing the suitable screw inanimal studies. The vertebral column was exploredusing classical anterolateral approach in humancadaver. Corpectomy was carried out in the targetvertebra. First, the lower surface of the upper corpusis drilled for the insertion of the screw by using aright-angle chisel (Figure 2.1). Then, the spongious
30
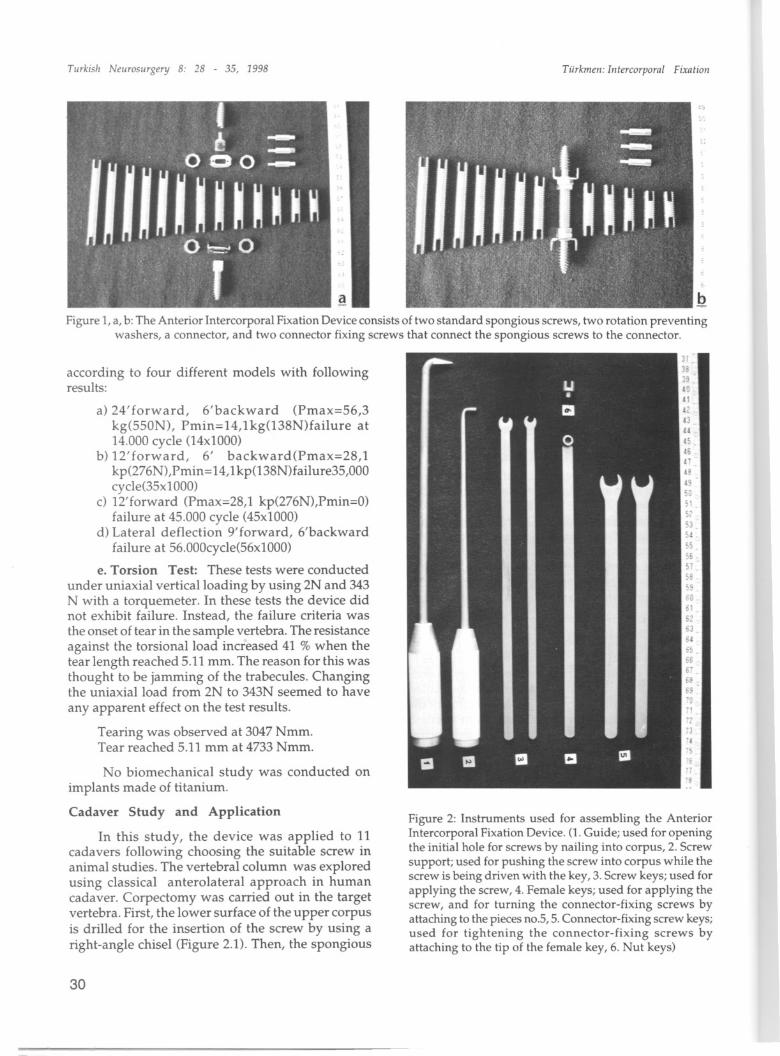
Figure 2: Instruments used for assembling the AnteriorIntercorporal FixationDevice.(l. Guide; used for openingthe initial hole for screws by nailing into corpus, 2. Screwsupport; used for pushing the screw into corpus while thescrew is being driven with the key, 3.Screw keys;used forapplying the screw, 4. Female keys; used for applying thescrew, and for turning the connector-fixing screws byattaching to thepiecesno.5,5.Connector-fixingscrew keys;used for tightening the connector-fixing screws byattaching to the tip of the female key, 6. Nut keys)
Turkish Neurosiirgery" 8: 28 - 35, 1998
screw is inserted into this hole by using a right anglescrew supporter aided with a special type of key(Figure 2.2, 2.3). The same procedure is followed onthe inferior corpus (Figure 3A). Following theinsertion of screws into the superior and inferiorvertebral bodies, the end plates are excised. Thus,an appropriate surfaee for the bone graft fusionaround the system is obtained. The conneetor-fixingpieces are applied to both spongious screws(Figure 2.4, 2.5). The rotation-preventing washers arenailed on to the corpuses af ter attaching to theconnector-fixing pieces (Figure 3B). Then theconneetor is inserted into the gap and the system islocked by tightening the pentagonal nu ts on bothsides (Figure 2.6, 3C). The graft is taken from costaand placed around the system to provide fusion(Figure 3D). Figure 4 demonstrates the applicationof the device to human cadaver. The rest of cavity isfilled with bone chips. if a multisegmental fixationis desired the extension pieees can be appIiedbetween the spongious screw and the conneetorfixing screw.
Case Report:
A 38- year-old woman was admitted to ourclinic after a fall from height. She had paraparesis
Türkmen: l/itereorpora/ Fixatio/l
and bilateral leg fractures. Spinal x-ray (Figure 5)and computed tomography revealed that she had 10% compression fracture on Th 12 (Figure 6) and typeBburst fraeture on Ll vertebral body (Figure 7). Withanterolateral approach, thoracotomy was performed.After decompression with Ll corpeetomy our devicewas applied (Figure 8)
Early postoperative anteroposterior (Figure 9)and lateral (Figure 10) plain x-rays demonstratedthe succesful application of the device. it was notneeded to use extension pieces. The patient was setwith thoracolumbar orthose after removing thethorax tube on postoperative second day. She wastransported to the rehabiIitation center on thepostoperative tenth day. The movements were notrestricted during the rehabilitation program withorthose. Four and half month later fusion was provedwith radiological evalution and the thoraeolumbarorthose was removed. Six months later the patientwas invited to control. She could walk without
support. it was also demonstrated with spinal x-rayand computed tomography seanning that fusion wascontinued on the level where our device was applied(Figures 11,12,13).
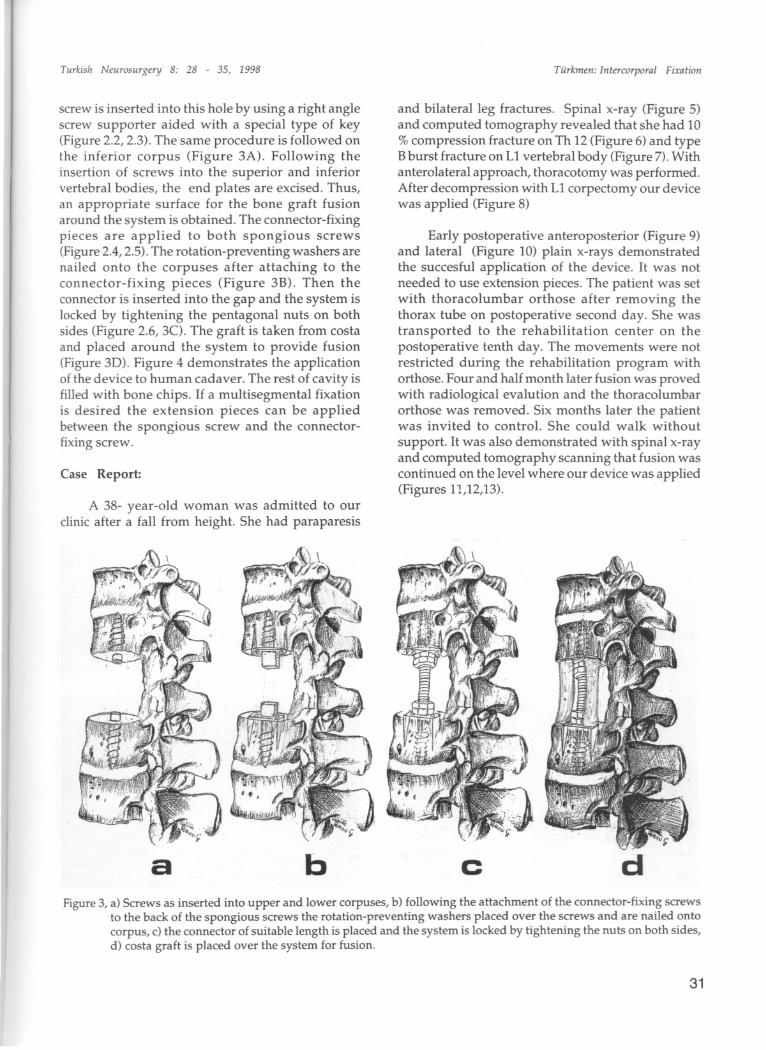
b c dFigure3,a) Screws as inserted into upper and lower corpuses, b) following the attachment of the connector-fixing screws
to the back of the spongious screws the rotation-preventing washers placed over the screws and are nailed ontocorpus, c) the connecter of suitable length is placed and the system is lockedby tightening the nuts on both sides,d) casta graft is placed over the system for fusion.
31
Turkish Neurosurgery 8: 28 - 35, 1998
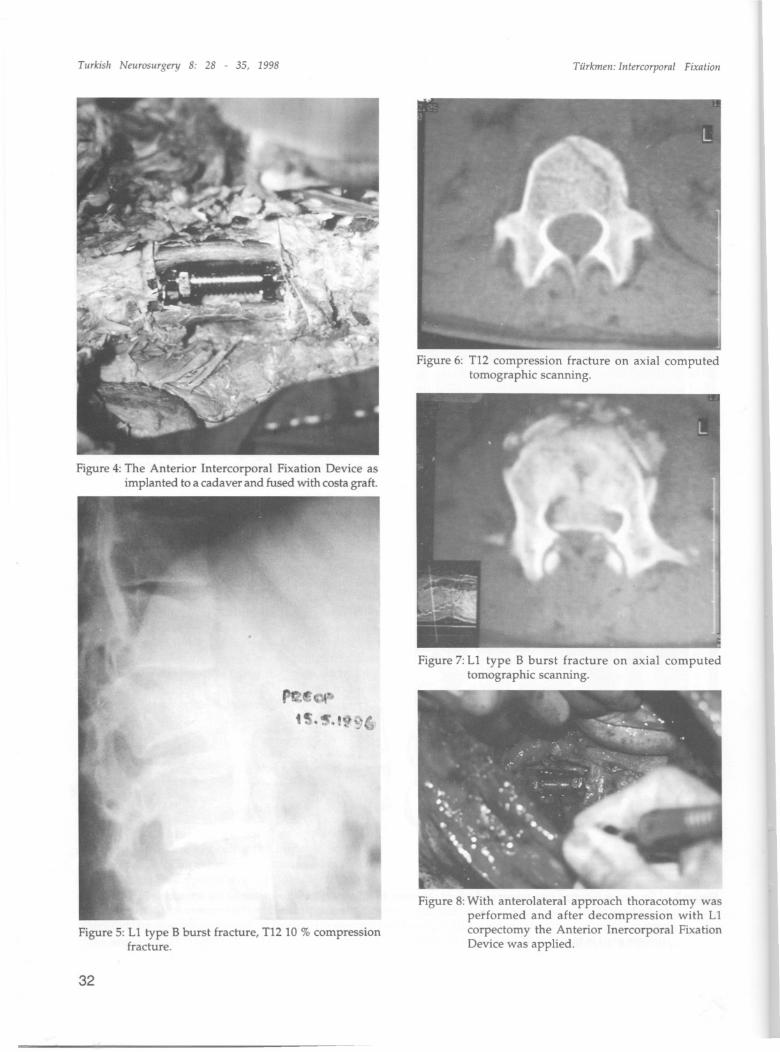
Figure 4: The Anterior Intercorporal Fixation Device asimplanted to a cadaver and fused with costa graft.
Figure 5: Ll type B burst fracture, T12 10 % compressionfracture.
32
Türkmeii: Illtercorpora/ Fixatioii
Figure 6: T12 compression fraeture on axial computedtomographic scanning.
Figure 7: Ll type B burst fracture on axial computedtomographic scanning.
Figure 8: With anterolateral approach thoracotomy wasperformed and after decompression with Llcorpeetomy the Anterior Inercorporal FixationDevice was applied.
Turkish Neurosurgery' 8: 28 - 35, 1998
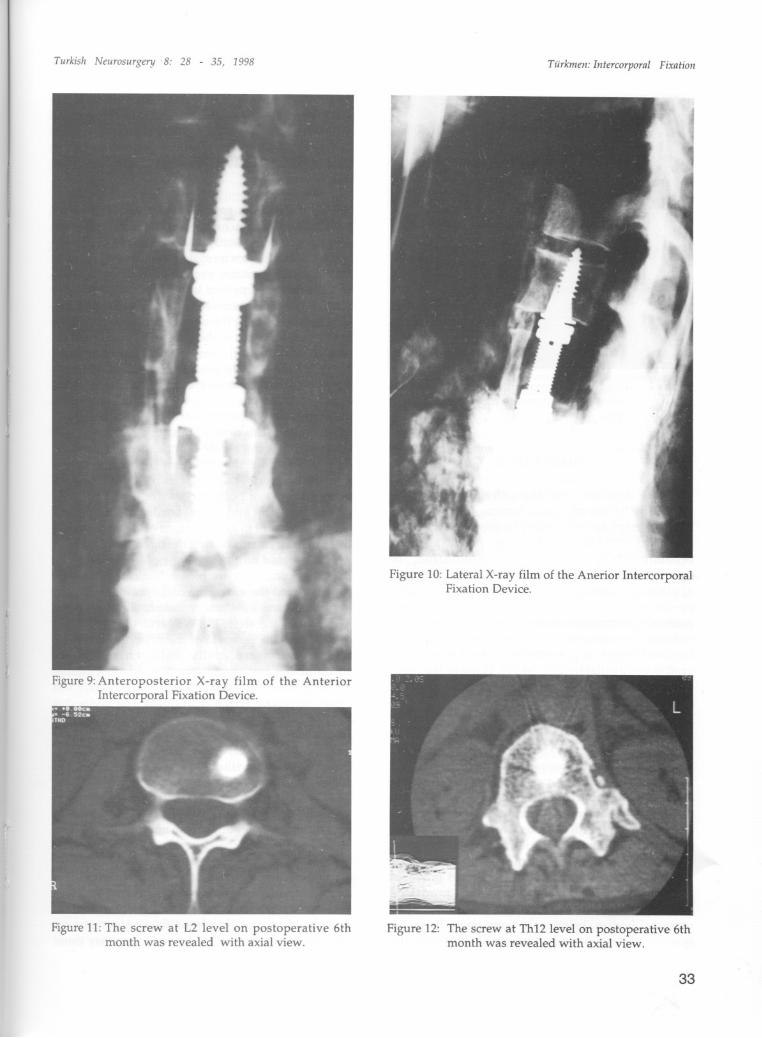
Figure 9: Anteroposterior X-ray film of the AnteriorIntercorporal Fixation Device.
Figure 11: The screw at L2 level on postoperative 6thmonth was revealed with axial view.
Türkmen: bitercorporal Fixation
Figure 10: Lateral X-ray film of the Anerior IntercorporalFixation Device.
Figure 12: The screw at Th12 level on postoperative 6thmonth was revealed with axial view.
33

Turkish NeuroSllrgery 8: 28 - 35, 1998
Figure 13: The fusion provided with costa graft onpostoperative 6th rnonth was proven with axia!view.
DISCUSSION
The importance of the anterior and middlecolumn in the case of, thoracolumbar, burst fractureshas been emphasized in many biomechanical studies(4, 9, 10, 11). In these cases, many authorsrecommend posterior instrumentation intranspedicular way to provide stability following theapplication of anterior block graft either in the sameoperation or in a second session (7). Anterior andposterior instrumentation systems used today areespecially insufficient against axial compression andtorsional forees, if powerful tricortical block bonegraft is not available (2,3, 16,19). None of the manmade systems is as strong as the natural structure(16,17). Positioning of the existing anterior andposterior instrumentation system s in aperpendicular fashion with respect to the verticalforce axis of the vertebral column leads to a relative
increase in the load exerted onto the implant, andthus, causes failure. Our device which is based onanterior intercorporeal fixation is placed parallel tothe anatomical force axis. Therefore, while it doesnot di ffer from the other system s in terms of resistingflexion and extension motions it is, as shown inbiomechanical studies, more advantageousespecially against axial compession and torsionalforces (16). Rezaian's, Pinto and modifiedHarrington systems which are placed betweenvertebral bodies, being only temporary distractorsystems, do not provide fixation (1, 5). While the
34
Türkmen: Intereorporal Fixation
fusion region in Rezaian's and Pinto systems arequite small, the fusion region in the system reportedhere is larger, and therefore, more satisfactory. Sinceour system provides fixation, we can use it inosteoporotic patients and multipI segment involvedcases.
Our device is easy to apply. In the cadaverstudy, application of the screws following thecorpectomy took only ten minutes, while theapplication of the entire system required 35 minutesin total. There was not problem during applicationof the device to a patient with Ll burst. Only a fewsimple equipments are used during application. Theonly crucial point is the alignment of the connectorand the other pieces in the same direction. Insertionof the screws should be done carefully withouthurry. if the screws are misaligned placing theconnector will be troublesome, and spongiousstructure of corpus will not allow for insertion ofthe screws once more by redrilling. Although smalldiversions in the direction of the screws can be
tolerated, opening a new channel is quite difficult.In this example the problem of localizing themidpoint of verteb ra e is solved by, caleulating themeasurements of posterior border of the corpus corpus midpoint and lateral border of the corpus corpus midpoint in axial sections of CT, than we usethese measurements during the operation.Since ourdevice is based on the principle of ' Fixation alongthe Ana tomical Axis ' the biomechanical results were
superior, and therefore, the costa graft is sufficientfor a quick and satisfactory fusion, eliminating theneed for bloek graft (8, 17). We performed with costagraft. When the removal of the system is required,the screws were easily unfastened withoutencountering any complication. In all other studieson sheep, cow and human cadavers the implant waseasily remove d without undoing the connectorscrews. Another advantage of this system over theother anterior stabilization systems is that removingonly the pathological vertebra body is sufficient forthe application without the need to expose theadjacent vertebra bodies.
Moreover, since the application is quite easyand the area is far enough from neural element s andimportant vascular structures, it is also thought thatthe risk of complication during application mayconsiderably be reduced (6, 13,14,15,18). Since in theanterior and middle colon insufficiencies the forcevector ofaxial and rotational forces are in verticaldirection, horizontally placed fixation systems aresubjected to momental forces and these may cause

Turkish Neurasurgery "8: 28 - 35, 1998
their failure. For a long time many instruments havebeen tried in the intercorporal space; Rezaians andPinto systems are still used. Lack of fixation is themajor disadvantage of these systems. By solving thisproblem our system has an advantage over others.
In conclusian, Anterior Intercorporal FixationDevice achieves resistance especially against theaxial compressional and rotational forees, andprovides short segment stabilization. Exposition ofonly the pathologic vertebrae corpus is adequate.Application of the system is quite safe, because thisarea is away from neural and important vascularstructures. In addition to all with its practicability itneeds to be improved to find widespread use.
Lega/ Nate: This system is patented (TR 96 / 466- June 4, 1996). Patent Cooperation Treaty /TR 97/00007. Approved by the international bureau (WIPÜ)in Austria.
Correspondence: Cengiz S. Türkmen, MDKaldirim Cad. Orme SitesiBlok l,Daire 4 Talimhane mevkiiÇengelköy, istanbul,TurkeyPhone: (216) 308 8368Fax: (212) 233 9573E-mail: [email protected]
REFERENCES
1. Arbit E, Galicich JH: Vertebral body reconstructionwith a modified Harrington rod distraction systemfor stabilization of the spine affected with metastaticdisease. J Neurosurg 83:617-620, 1995
2. Closkey RF, Parson R, Lee CK, Blacksin MF,Zimmerman MC: Mechanics of interbody spinal fusion- Analysis of critica i bone graft area. Spine 18:10111015,1993
3. Crisco JJ, Panjabi MM, Oda T, Grob D, DvorakJ: Bonegraft translation of four upper cervical spine fixationtechniques in a cadaveric modeL. J Orthop Res 9:835846, 1991
4. Edward WT, Hayes Wc, Posner I, White AA, MannRW: Variation of lumbar spine stiffness with load. JBiomech Eng 109:35, 1987
5. Errico JT, Waugh T, Bauer RO: Spinal Trauma 10:285288, 1991
Türkmen: [ntercarparal Fixatian
6. Esses SI, Sachs BL,Dreyzin V:Complications associatedwith the techniques of pedide screw fixation: A selectedsurvey of ABS members. Spine 18:2231-2239, 1993
7. Farcy JP, Weidenbaum M, Mchelsen CB:A comparatiyebiomechanical study of spinal fixation using CotrellDubousset instrumentation. Spine 12:877, 1983
8. Goel VK, Pope MH: Biomechanics of fusion andstabilization. Spine 20:85-89,1995
9. Haher TR, Felmy WT, Welin D: The lAR as a functionof the three columns of the sp ine. Abstract Presentedat the Annual meeting of the ScoIiosis Research Society,Amsterdam, the Netherlands Sept. 17, 1989
10. Haher TR, Felmly WT, Baruch H, Devlin V, Welin D,O'Brien M, Ahmad J, Valenza J, Parrish S: Thecontribution of the three columns of the spine torotational stability. A biomechanical modeL. Spine14:663,1989
11. Haher TR, Tozzi JM, Lospinuso MF, Devlin V, O'BrienM, Tetant R, Ahmad J, Valenza J, Parrish S: Thecontribution of the three columns of the spine to spinalstability. Biomechanical modeL. Paraplegia 27:432, 1989
12. John RN, Joseph RO, Sunniva KR, Deborah AD,Heather JF, Diane MJ, William HC, Robert LS, KathleenM: ASM Handbook, Voulme 8 Mechanical Testing,ASM International The Materials Information Society,1994
13. Kumano K, Hirabayashi S, Pgawa Y, Aota Y: Pedidescrew and bone mineral density. Spine 19:1157-1161,1994
14. Matsuzaki H, Tokuhashi Y, Wakabayashi K, KitamuraS: Penetration of a screw into the thorade aorta in
anterior spinal instrumentation. A case report. Spine18:2327-2331,1993
15. Mc Afee PC, Weinland DJ, Calow JJ: Suryiyorshipanalysis of pedicle spinal instrumentation. Spine16:442-447,1991
16. Shono Y, Mc Afee PC, Cunningham BW: Experimentalstudy of thoracolumbar burst fractures: A radiographicand biomechanical analysis of anterior and posteriorinstrumentation systems. Spine 19:1711-1722, 1994
17. Steffe AD, BrantiganJW: The variable screw placementspinal fixation system: Report of a prospective studyof 250 patients enrolled in Food and DrugAdministration Clinical Trial. Spine 18:1160-1172, 1993
18. Wittenberg RH, Shea MS, Swartz DE, Lee KS, WhiteAA III, Hayes WC: Importance of bone mineral densityin instrumented spine fusion. Spine 16:647-652, 1991
19. Wittenberg RH, Moeller J, Shea M, White AA III, HayesWC: Compressiye strength of autologous andallogenous bone grafts for thoracolumbar and cervicalspine fusion. Spine 15:1073-1078, 1990
35