ABNORMAL GROWTH AND DEVELOPMENT 143
ABNORMAL GROWTH AND DEVELOPMENT RESULTING FROMDISEASE, TRAUMA AND DEFORMITY
R. SHEPHERD, DIP.PHTY.
VERTICAL APPROACH
DEVELOPMENT OF MANIPULATION
from the others; we see how dependent eacharea of skill is on the other areas of skill.For example, we see that manual prehensioncan only begin to develop some sophisticationonce the child's balance in sitting has pro..gressed to the stage when his hands are freedfrom the need to support.
The relevance of development to treatmentis misinterpreted by those therapists who con..sider only the vertical view. We hear the term'neurodevelopmental sequence' used frequently and the term itself can infer a purelychronological and therefore vertical sequence.Unfortunately it sometimes suggests that itis the chronological sequence of rolling, sit..ting, crawling, standing, which is importantto keep in mind in the planning and executionof treatment, rather than the relationship be..tween the various areas of skill.
This view has, in my opinion, only limitedusefulness in the treatment of children, or forthat matter, adults. It tells us only that anormal child progresses from a primitiveleHex bundle to motoric maturity in a certain relatively ordered sequence. It infers that
Aust.l.Physiother., XXI, 4, December, 1975
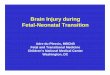
Figure 1
Hands closed. Grasp reflex +ve.Hands often open. Grasp reflexdisappearing.
Holds rattle if placed in hands.Pulls at dress.Tries to grasp objects. Plays with rattle.Bidextrou8 grasp. Plays with toes.
Holds bottle. Palmar grasp of cube.
4 weeks8 weeks
12 weeks
16 weeks
20 weeks
24 weeks
There are two concepts which interest meparticularly in the field of paediatric physiotherapy. One is the prevention of abnormalities of growth and development; the other isthe enrichment of development.
Physiotherapy of infants and childrenshould always involve both these concepts. InIny opinion, every physiotherapist workingwith children should ask herself these questions when she is assessing an infant or child,and when she is planning and carrying out hertreatment:I. Every part of this child is in the process
of growth and development. Will mytreatment today enable growth and devel..opment in all areas, from anatomical topsychological, to take place as normallyas possible?
2. Can I he sure that today's treatment, although it demonstrates an immediate improvement in his condition, will have nolong~term harmful effects in respect to hisgrowth and development?
I propose to talk about the development ofthe child and the need to understand the ideaof growth and development relating to sickness and disability. I will outline areas inwhich the physiotherapist can work to pre..vent and treat developmental delay and de..fects in growth, and finish with some philosophical thoughts about our profession.
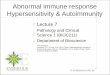
There are basically two ways of looking atdevelopment - vertically and horizontally. Ifwe look at it vertically (figure I), we see acertain sequence of events occurs in chronological order. This view gives us nothingmore than a sequence in time. However, if welook at development horizontally (figure 2),we see what skills develop together; we seethe relationship between the various areas ofdevelopment rather than each area separate

]44 THE AUSTRAIJIAN JOURNAL OF PHYSIOTHERAPY
the skills of prehension, locomotion, vocalisation, socialisation, visual and cognitive function develop in parallel to one another, andlittle attention is therefore paid to their re..lationships one to the other. It infers thatthe child develops the motor skills of rollingover at a certain stage, hut does not tell usthat his rolling over continues to becomebetter planned, more relevant and mature, ashe develops other skills. For example, a childroIls over first at six months of age. He rollsover and over in order to get under a tableby approximately twelve months, and he rollshimself over and over in a blanket by approximately five years.
There is another aspect of developmentwhich must be considered - the step..like wayin which a child develops his motor skills. Heappears to concentrate all his efforts on preparing himself for a new skill with a corresponding suspension in the development ofother skills. For example, a child learns certain manipulative and verbal skills whichdevelop fast at about the time when he hasachieved good sitting balance. When he isstanding and taking his first tentative steps,his vocalisation and manipulation develop..ment remain stationary; they may even re·gress. Once he has developed better balanceand more efficient walking, his hand function
HORIZONTAL ApPROACH
Supine Sitting Standing Hands Reaction Oro-Facial6 Months Rolls supine Sits unsup- Bounces when Grasps with Body righting Developing
to prone. ported briefly. held standing. whole hand. on body oral control.Pulls to Hands forward Reaches out. begins. Singlesitting. for support. Transfers Protective syllables.Lifts head objects hand extension Munches.spontaneously. to hand. forwards.
Gagging lessBangs. Pats. Equilibrium frequent and
!eactions +ve lessIn prone. exaggerated.Takes foodfrom spoonwith lips.
Figure 2
This chronological sequence is just the heginning of the information we need in orderto understand rolling, if we are to treat thechild who cannot, for some reason, roll overnormally. What we really need to know iswhy the normal child takes so long to developthe more mature rolling skill; what other skillshe needed to develop in order to be able toroll himself in that blanket. To find the answerwill involve looking horizontally at normaldevelopment, seeing what other skills relateto the development of rolling. We will see,broadly speaking, that he developed this skillas he developed his ability to motor plan in avariety of activities.
The vertical sequential view is a narrow one.The horizontal view, more useful in terms ofassessment and treament, is a broader one.
Aust.J.Physiother., XXI, 4, December, 1975
and speech begin to develop more rapidlyagain. So we look at development horizontallyin order to see how the acquisition of skillin one area will affect the development of skillin another, and we will use this knowledge tohelp children develop the motor skills they arelacking.
One of the most important phenomena inthe development of motor skills is the wayin which a normal child prepares himself,very directly and with great attention to detail,for the acquisition of each new skill. Anunderstanding of the elements of this pre..paration will form the background to theplanning of any treatment programme,whether for adults or children, because itwill give the details which must necessarilyhe accomplished if a particular motor skill

ABNORMAL GROWTH AND DEVELOPMENT 145
is to be learned or relearned. For example,rolling is not specifically a preparation forwalking, although the child learns to roll overlong before he walks, and of course his abilityto walk owes something to all the skills hehas learned beforehand. More important interms of the analysis of motor skills is thefact that he prepares himself for walkingnluch more specifically. Once he has learnt topull himself to standing, he begins to practisethe specific skills needed for walking. He be..gins to develop balance in standing by reaching out for toys, and this involves some transference of weight. He concentrates particularly on lateral balance, and cruises sidewaysaround the furniture. He is still trying toachieve a perfect symmetry between flexionand extension, and will be seen to sit abruptly,indicating too much flexion, or over-balancebackwards or stand on tiptoe, indicating toomuch extension. When he first stands aloneand starts to walk forwards you can see howmuch hetter his lateral halance is than hisantero..posterior balance. He stands and walksat this stage with his feet apart; his first attempts to transfer weight forwards on to onefoot result in small steps which progress himforwards only a little. He does not walk efficientl1y until he has practised all the variouselements of this skill, singly and together, inpreparation: until all these elements have become integrated. This process will take severalyears.
Another phenomenon in the developmentof motor skills is the appearance of sensitiveperiods (McGraw, 1946, Connolly, 1972, 11lir:gworth, 1970), when the child demonstratesa readiness for and a considerable drive towards one particular activity. These periodsare probably related to the development ofhis central nervous system, and must followon from the child's own preparatory activities.Physiotherapists treating children do not always understand the importance of these sensitive periods, and consequently miss oppor..tunities for successful treatment. For example,it is not uncommon for a myelomeningocelechild to be seen by the therapist for a briefperiod when he is an infant, and then notagain until he is eighteen months old, whenshe begins to teach him to walk. A normalchild who has been preparing himself for
walking for several months, demonstrates aconsiderable drive to walk between twelve andeighteen months. This is the so-called sensitive period for walking, but his parents wouldsay he is 'ready' to walk. There is a tendencywith the disabled child to leave attempts atwalking until he is 'ready' for it, withoutrealising that he will never achieve this stateof readiness if he is not helped to preparefor it.
The myelomeningocele child would develophis ability to walk much more naturally if thetherapist saw him throughout that importantfirst twelve months, in order to help him withthose parts of the preparation which he isunable to initiate himself; making sure, forexample, that he develops head control andextension against gravity to prepare himselffor an anti-gravity position, making sure hestands from an early age as would a normalchild, getting him used to being at a certainheight above the ground, helping him todevelop his central nervous system hy receivjng and integrating sensory information of alvide and appropriate variety. She will helphim to develop his curiosity so that he winwant to move around. She will ensure that hewill feel natural on his feet when the timecomes for him to begin walking. It is a lackof this kind of preparation which results inmany spina bifida children being so long inlearning to walk, and the older the child isbefore he stands the more likely it is that he,\Till develop a fear of falling, a timidity aboutwalking, and a preference for what is to himthe more natural position of sitting.
As has been written elsewhere (Shepherd,1974), 'The child is not a miniature adult.The period of development into a fully integrated human being which begins in the embryo does not cease until growth, mental andemotional, as well as physical, is complete~
In the physical sense development does notmerely mean that the various parts of thechild grow larger, but also that these partschange, adapting to some extent, according tothe demands of the environment.' When wetreat children, do we understand the differencebetween the child and the adult well enoughto be sure our treatment is effective in thelong as well as the short term?
Aust.J.Physiother., XXI, 4, December, 1975

146 THE AUSTRALIAN JOURNAL OF PHYSIOTHERAPY
In the short term, deformity, disease andtrauma have similar effects upon children asupon adults, but in the long term an impor.tant difference emerges. This difference liesin the effects of deformity, disease and traumaon the growth and development of the child.These secondary effects, which may not be..come evident until after some time, may befar more disabling than the original disability.There are certain obvious examples of this,although it is a field which has been insufficiently explored so far. The shortenedlimh of the child who has had paraplegiasince birth; the abnormal development of thethoracic cage and lungs in a child who hashad respiratory disability since birth; theabnormal sensorimotor development of achild who has been unable to experience thenormal life of an infant and young child;these are examples of the long.-term effectsof disability on growth and development.
If we consider these growth changes whichare occurring, and if we consider that bones,joints, soft tissues and organs develop andgrow according to the stresses put upon them,we can see that if the stresses put upon themare abnormal, the growth and development ofthese structures themselves will be abnormal.Let us look at some examples:
The Foot. The normal foot undergoes con..siderable developmental change during thefirst few years of life. Nat all of the honesare ossified at birth; indeed the final boneto ossify does so only in the child's thirdyear" These bones develop their shape andother attributes as they grow, and their growthis influenced by the stresses put upon them"
The baby with severe talipes equinovarusis born with a foot the structures of which arealready deformed. Our aim is that growthshould not further add to the deformity, andfor this reason, treatment to gain a moremobile foot is begun as early as possible.Mobilisation of talipes equinovarus shouldonly be attempted by therapists who have adetailed knowledge of the normal anatomyand, more important, the pathological anatomy of the foot, as well as an awareness ofthe plasticity of the infant foot and the po..tentially deforming effects of growth" It isnot sufficient to mohilise the infant's foot until
Aust.l.Physiother., XXI~ 4, Decemher, 1975
it is cosmetically presentable and functioningsufficiently well for his needs at the moment.We must also be sure that the foot is mobileat the appropriate joints, that the positiongained is normal, that stress is not beingplaced abnormally on these growing and shaping structures. The effects of this may notreveal themselves until much later. The ten..dency for many corrected club feet to relapseis, says Sharrard (1971), due to treatmentwhich did not gain correction, nor normalfoot mobility, nor a normal relationship he..tween the structures of the foot, but only apseudo-correction. In these cases the calcan·eum remains too plantarflexed for normalmovement to occur, and the dorsiflexionoccurs instead at the joints of the midfoot.The foot cannot be said to have relapsed asthe deformity has never been corrected. Thereare other problems arising from inexperttreatment of club feet, and these also will notbecome obvious until the child is older. SharI ard (op. cit.) comments that forcible manipulation to correct equinus may result in further deformity of the talus, and may evendamage the tibial and fibular epiphyses.
The Respiratory System. The lungs are notfully developed at birth; not just incompletelygrown in terms of size, but incompletely developed in terms of complexity. Up to theage of eight years, lung growth proceeds withan increase in the number of hronchiolar di..visions, alveoli, alveolar diameters and sur·face area for gas exchange. The number ofalveoli and airways increases len times frominfancy to adulthood. There are twentymillion alveoli present at birth and three hundred million in adult life (Avery, 1968,!(endig, 1967).
In the newborn infant the airways have agreater relative diameter and the anatomicaldead space is correspondingly larger than thatof the adult. The development of the airwaysand alveoli is dependent to some extent uponthe demands made upon them. The presenceof disease or the retention of secretions maytherefore result in abnormal development.
Physiotherapists treating all infants, including those who are premature, need to be con..stantly aware of the damage which can he

ABNORMAL GROWTH AND DEVELOPMENT 147
done to immature airways if secretions arenot swiftly removed, and of the risk of traumadue to inexpert or over..enthusiastic aspira..tion techniques. They need to realise the risksinvolved in relatively small changes in temperature and oxygen concentrations, and theeffects of these on premature habies whenthey are treating these infants nursed in in..cuhators.
These are all very sobering thoughts. Weall hope that we have never allowed suchsecondary disabilities to occur, hut unfor..tunately, because of our slackness in record..ing data and in checking up on long..termresults of our treatments, we are probablyrarely confronted with the results of our in..eptitude.
The Central Nervous System, The centralnervous system is immature at birth. It isinteresting that the ascending (sensory) fibresof the spinal cord are relatively well myelinated while the descending motor tracts andthe white matter of the cerebral and cere·bellar hemispheres are not. The cerebellumitself is immature for the first two years oflife. Although the maturation of the nervoussystem is little understood, there does appeara direct relationship between the developmentof myelination within the nervous system andthe development of neural function, and astimulus to myelination may come from activity within the various systems (Dekahan,]970). It appears that tracts may become myelinated at the same time as they become func ..tional. 'Use of a neural synapse increases theease by which the fundamental connection ismade; disuse of a synapse reduces the probability that the connection will be made'(Eccles, 1961).
The relationship between sensorimotor development and the developing nervous systemis a relatively unexplored field in human experimentation, yet there have been several experiments on animals which show that devel..oping structures need to be used in order tonlaintain their potential effectiveness. Eccles(1973) describing what he called 'the elegant experiments' of Wiesel and Hubel, writes'It is some days after hirth before kittensopen their eyes; nevertheless, at birth the Ie..tina is connected with detailed topography to
the visual cortex in the adult pattern ..•Here we have an excellent illustration of theestablishment of precise patterned connectionsfrom eye to brain prior to usage . • . Butif this beautifully grown structure is not usedfor some weeks after the time the kitten normally opens its eyes, it becomes disorganised,the destruction being permanent. Use by patterned vision is essential for stabilising thisfragile organisation of retino..cortical connectives ...' There have heen many other experiments on animals which describe diminished function following on from lack of useof part of the central nervous system.
In a way many of us are only now reallydiscovering the sensory system and realisingthat the most important physical methodsavailable to us involve controlled sensoryinput. The most important element in learningmotor skills seems to be the presence andthe quality of sensory feedback. The develop..ment of sensorimotor skills depends upon thebrain receiving the appropriate sensory feed ..back and integrating this information.
The normaJ infant as he is handled andstimulated by his parents gets sensory feedback which enables him to perfect motorskills. There is a constant monitoring of signals received, a checking and correcting untilthe appropriate motor response is achieved.
Sensory feedback must he particularly essential for a developing immature brain. AsAyres (1973) says, 'Gravity, sounds, sights,tactile stimuli, and those arising from themuscles and related structures impose them..selves upon the child, making demands uponhim that help deterlnine the nature of growthof the nervous system.'
The relationship between motor development and the development of perceptual, cog..nitive, visual, verbal and social skills has beendescribed by Held (1965), Denner and Cashdan (1967), Cashdan (1969), and Piaget inmany publications. A considerable impetusappears to he given to the development ofother skills by the development of movement.
Therefore, where disability interferes withnormal sensorimotor development, it will benecessary to stimulate it by treatment whichtakes into account the way in which a normal
Aust.!.Physiother., XXI, 4, December, 1975

148 THE AUSTRALIAN JOURNAL OF PHYSIOTHERAPY
child learns. In treating a child by sensorystimulation and facilitation of movement, weare attempting to feed into his central ner..vallS system stimuli which he otherwisewould not experience. We are putting thechild into a situation in which he is enabledto learn.
Let us look at some examples:1. A baby aged fouf months demonstrated
strong labyrinthine activity in supine, withextension of his whole body and retractionof his shoulders. He cried a lot, was diffi..cult to feed, and his eyes maintained a pronounced convergent strabismus. He wasput in a hammock in which his head andtrunk were relatively flexed and his shoulders protracted. Within twenty-four hourshe could bring his hands to the midline,reach out towards a toy; he had lost hisstrabismus and was able to look aroundand apparently fix and focus his eyes.He no longer cried as before. Of course,no claim can be made that suppression ofthis abnormal activity would be permanent, but such a treatment device enabledhim to begin to learn with his hands andeyes, and begin to appreciate and respondto social overtures from his family, something he had previously been quite unableto do.
2. The mentally retarded baby is unahle toinitiate his own development, and the poorresponse his parents receive from himmakes them less stimulating than theywould be to a normal child. They areless inventive with the games they playand vocalise less to him if he does notvocalise back. He receives therefore relatively few sensations of movement and thisis one of the reasons why certain simpleactivities tend to become perseverant. Theearliest signs of mental retardation areoften motor, demonstrated by low tone,feeding problems, decreased spontaneousactivity, perseverant activities such as headrolling and hand regard, poor head control, poor antigravity control, poor balanceand protective responses. The baby's de..velopment tends to become arrested atcertain stages. He may learn to sit hut
Aust.J.Physiother., XXI,. 4, December, 1975
may not progress any further. Let us takethe example of a child aged ten months,with Down's Syndrome, who cannot yet sitalone because he has not developed balance reactions or protective support on hishands. He lies on his back for a largepart of the day indulging in persistenthand regard and head rolling. In pronehe is relatively helpless as he is unableto sit himself up. It was at this stage thathe was sent to a physiotherapist. Unfortunately he was used to this limited behaviour; it had become well learned andfor a while he resisted any change. If hehad been treated from an early age hisdevelopment would not have come to a haltat this stage.
There are mentally retarded babies whocannot bear to touch objects, who keeptheir hands fisted and pull away fromproffered toys. This aversive response,which may be related to what Ayres (op.cit.) calls 'tactile defensiveness', can beovercome by a programme of organisedtactile stimulation which enables the childto accept different sensations in the palmof his hand and which allows him to be..gin some manual exploration of his en..vironment, which he otherwise would havelacked.
3. There is a relatively new field emergingfor physiotherapists who are skilled indevelopmental assessment and treatment,and this is in the management of childrenwith learned disabilities who have associated sensorimotor problems. The mostcommon ahnonnalities are perceptual,with poor balance and manipulation, andlow tone commonly associated. There mayalso he an element of pronounced hyperactivity in some of these children. AsAyres says, 'The learning disabled child'snervous system has not developed in anormal manner, so he is unable to organise an appropriate response to the demands of the environment.' With morespecific and thorough testing proceduresthan we have at the moment, we shouldbe ahle to locate and treat these childrenbefore their non-achievement in schoolbecomes a serious problem.

ABNORMAL GROWTH AND DEVELOPMENT 149
4. Anotller new field for physiotherapists isin the management of feeding difficultiesin infants. The normal infant, from birthuntil he is a few months old and is beginning to lose his primitive sucklingreflex, will demonstrate an immatureswallow due to incoordination of themuscles of swallowing. He will thereforetend to gag and choke at times, and whenhe is first presented with semisolids he,viII tend to push them out of his mouthwith a thrusting tongue. As his centralnervous system matures so his ability tocope with food and saliva will improve.
There seem to me to be three main reasonswhy assessment and treatment of oral dysfunction in disabled babies should begin early.There is considered (Mueller, 1974) to be acorrelation between the normal devel'opment oforal function in feeding and the developmentof speech.. Secondly, the relationship betweenthe baby and his mother can become severelystrained if there are difficult feeding sessions.Thirdly, the baby who is too difficult to feedis treated in hospital with a gastric tube, andalthough this transports the food into thestomach, it does not have any remedial effectupon the problem itself.
Just as the physiotherapist is trained toobserve movement and function of the restof the body, so she should be able to assessoral function in an infant. Feeding problemsare sometimes the first signs that a baby isnot developing normally, and there is an important and as yet unrecognized avenue ofwork for physiotherapists in assessing andimproving the oral function of infants in babyhealth centres, paediatric hospitals and community care centres.
I would stress that there should be an increasing emphasis placed on physiotherapyfor infants at risk of developmental delayand for those young babies who are alreadydemonstrating such delay, whether it be adelay in oral function or in more generalisedsensorimotor activity. The babies who cometo mind particularly are the mentally retarded, those with spina bifida cystica andthe cerebral palsied, although there are manyothers who should also be considered. It isthe two former groups which are particularly
neglected. There is considerable emphasisnow, in most parts of this country, on theearly treatment of cerebral palsied infants.Unfortunately, in the case of cerebral palsy,too much emphasis has been placed on thechanging of tone and the facilitation of morenormal movements, discussion of whichtends to become confused. We should, instead,be talking about the ways in which we tryto prevent the generalised developmental delaywhich must result from the inabifity of thebaby to receive sensation from and respondto his environment. In other words, we shoulduse our skills with the objective of stimulating the baby's developing central nervoussystem. Whatever else we believe we are ableto do, this remains our principal aim, andit should he our aim with all children whosedisability will result in developmental delay.
For any treatment designed to stimulate ababy's development, the physiotherapist, aswell as being skilled in assessment and treat..menl, must also understand sufficient abouteducational processes to be able to teach thebaby's parents how to carryon with treatment at home. The major part of treatment,ill the case of babies with disabilities resulting in developmental delay, consists of correcthandling during play, bathing, feeding andsimilar activities. This prevents the need forlengthy periods spent in performing difficulttechniques of treatment, which may result inconsiderable anxiety for the parents..
Parents will not learn how to treat theirchild at home by watching the therapist demonstrate, any more than a physiotherapyundergraduate will learn by watching histutor demonstrate. In my experience, parents,once they understand the reasons behind suchan approach, appreciate being able to treatthe baby in front of the therapist, who corrects their handling and is able to reassurethem about the effectiveness of what they aredoing.
All physiotherapy in paediatrics should bedevelopmental. There should he no sub-branchcalled 'developmental', suggesting that thereare areas of child care which do not requirean understanding of developmental processes.If the physiotherapist does not understandgrowth and development she can neither
Aust.].Physiother., XXI, 4, December, 1975

150 THE AUSTRALIAN JOURNAL OF PHYSIOTHERAPY
understand the child nor can she understandwhat she is trying to accomplish. Her aimswill be short..term - to enable him to walkor to clear his chest. Jnst as thephysiotherapist prepares the adult for hisreturn to work and family, so she should prepare the infant and child for normal growthand development.
I hope we will soon establish in this coun..try long~term postMgraduate training in paedi~
atrics to enable our profession to take itsplace in the emerging areas of paediatrics,which will demand many more people, withmuch more expertise, than are availablenow. OUf years of equating specialisation withexperience are past. Physiotherapy requiresproperly trained specialists. At the moment,poor treatment by an individual therapistmay lead to the belief that physiotherapy it..self is ineffective.
I hope also that we will see paediatriccentres established, where infants and child..ren, who do not need hospital care, will re~
ceive treatment in a more natural atmosphere,and where their parents will be shown howto enable their child to achieve his developlllental potential. We must expand our services into baby health centres and schools,and learn to work with clinic sisters andschool teachers. The possibilities of physioM
therapy in paediatrics are not yet being real..ised, and our care remains hospital.based andsickness..orientated. Let us reappraise ourrole in the paediatric health field and workto,vards a more total care of the child.
Aust.J.Physiother., XXI, 4, December, 1975
REFERENCES
AVERY, M. E. (1968), The Lung and its Disordersin the Newborn Infant. Saunders, Philadelphia.
AYRES, A. J. (1973), Sensory Integration and Learn·ing Disorders. Western Psychological Services, LosAngeles.
CASHDAN, A. (1969), "The role of movement inlanguage learning." Clinics in DevelopmentalMedicine 33. Heinemann, London.
CONNOLLY, K. (1972), "Learning and the concept ofcritical periods in infancy." Develop. Med. ChildNeurol. 14.
DEKABAN, A. (1970), Neurology of Early Child~
hood. Williams and Wilkins, Baltimore.DENNER, B. and CASHDAN, A. (1967), "Sensory
processing and the recognition of forms in nur~
sery school children." Hr. /. Psychology 58, 101.ECCLES, J. C. (1961), "The effects of use and disuse
on synaptic function." In Delafresnaye, J. F. (Ed.),Brain Mechanisms and LeJrning. Blackwell,Oxford.
ECCLES, J. C. (1973), The Understanding oj theBrain. McGraw, New York.
HELD, R. (1965), "Plasticity in sensory~motor systems." Scientific American 213 (5), 84.
ILLINGWORTH, R. S. (1970), The Development 0/the Infant and Young Child. Livingstone, Edin~
burgh.KENDIG, E. L. (1967), Disorders of the Respiratory
Tl act in Children. Saunders, Philadelphia.MCGRAW, M. B. (1946), The Neuromuscular Matur
ation of the Human Infant. Hafner, New York.MUELLER, H. (1974), in Finnie, N., Handling the
Young Cerebral Palsied Child at Home. Heine~
mann, London.SHARRARD, W.. J. W. (1971), Paediatric Orthopae~
dies and Fractures. Blackwell, Oxford.SHEPHERD, R. B. (1974), Physiotherapy in Paedia
trics. Heinemann, London.
Recommended