May 8, 2013
www.healthadvances.com
Health Advances, LLC BOSTON SAN FRANCISCO ZURICH
Skip Irving Partner and Managing Director
Advancing Research to Treatments: Unmet Needs In Glioblastoma
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 2
Unmet Need
Senator Ted Kennedy - 2008 Democratic National Convention in Denver, Colorado August 25, 2008. –
REUTERS
Senator Kennedy’s tragic death brought greater visibility to the tremendous need for improved brain tumor treatment options.
§ 76 years old at diagnosis
§ May 17, 2008: Seizure at his home in Hyannis, MA
§ Medflight from Cape Cod Hospital to Mass General Hospital in Boston
§ Diagnosed with Glioblastoma Multiforme
§ August 25, 2009: Died15 months after diagnosis

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 3
By annual incidence, glioblastomas are the most common type of malignant brain tumor.
Gliomas
Other Malignant
Non- Malignant
0%
25%
50%
75%
100%
Brain Tumors Gliomas
Perc
enta
ge
Other Gliomas
Oligoastrocytic Tumors
Pilocytic Astrocytomas
Anaplastic Astrocytomas
Oligodendrogliomas
Ependymal Tumors
Diffuse Astrocytomas
Glioblastomas
US Distribution of Brain and CNS Tumor Incidence By Histology
2005-2009
Unmet Need
Source: CBTRUS, American Brain Tumor Association website.
Glioblastomas Most malignant, most
aggressive and shortest survival
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 4
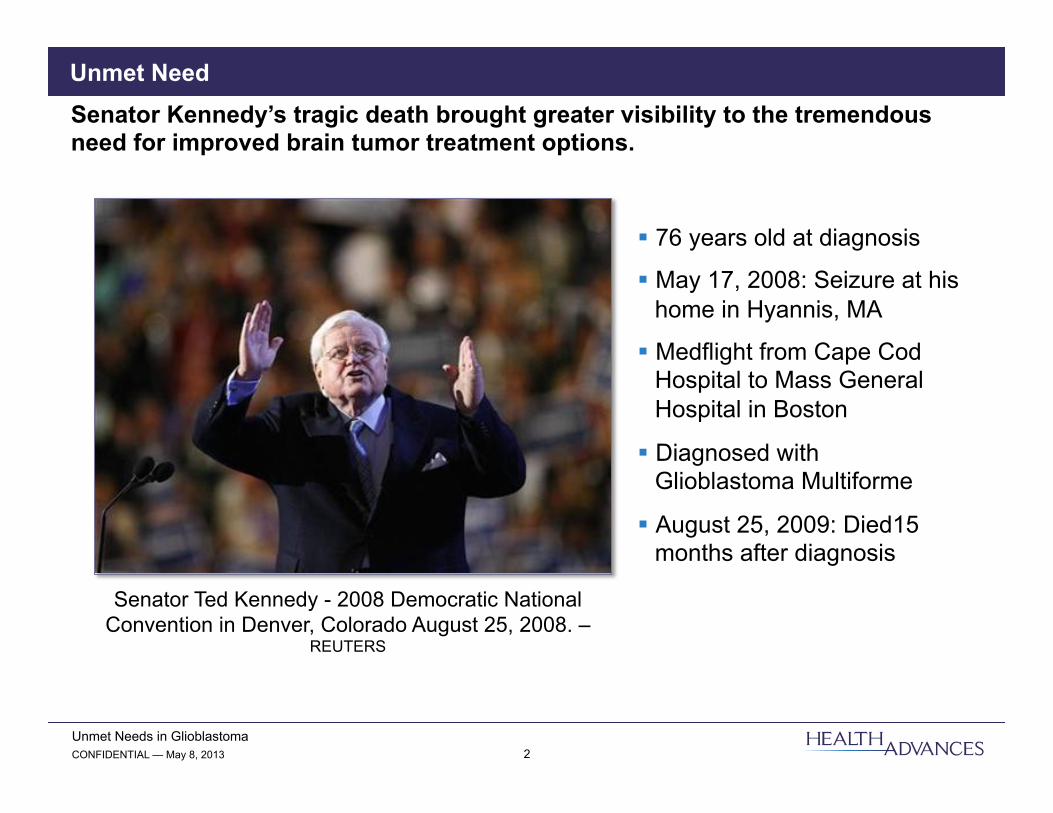
Note: Relative survival rates for primary malignant gliomas are from SEER, 1973-2004. Source: DataMonitor, CBTRUS, SG Cowen, Medscape.
Relative Survival Rates for Primary Malignant Gliomas
Unmet Need
Glioblastomas progress rapidly without therapy.
0%
20%
40%
60%
80%
100%
120%
0 12 24 36 60 96 120
Rel
ativ
e Su
rviv
al R
ates
Months After Diagnosis
Mixed Glioma
Oligodendroglioma
Anaplastic Astrocytoma
Glioblastoma
Ependymoma
Astrocytoma, NOS
Clinical history is less than three months in majority of patients; Prognosis worse for
elderly patients

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 5
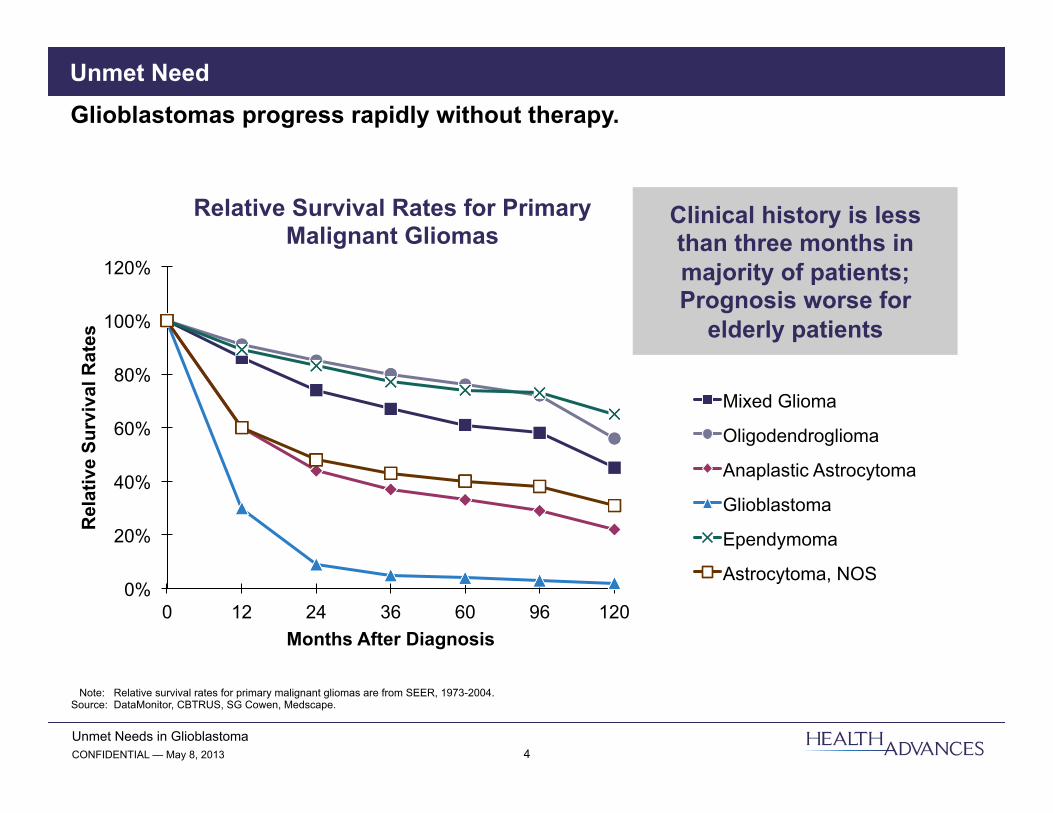
The best current standard of care extends overall survival to about 14 to 16 months.
Therapeutic Options
* Data for bevacizumab represents newly-diagnosed glioblastoma and is from a phase II clinical trial with no placebo control. Source: UpToDate; Gil-Salu, J., Neurocirugia, 2004; Walker, M., J. Neurosurgery, 1978; Westphal, M., Neuro-Oncology, 2003; Stupp, R., NEJM, 2005; Athanassiou, H., JCO, 2005;
Stewart, L., Lancet, 2002; Lai, A., JCO, 2011.
Median Overall Survival Time of Glioblastoma Patients by Therapy
0
6
12
18
24
Surgery Only
+ Radiotherapy (RT)
+ RT + Carmustine
+ RT + Carmustine
Implant
+ RT + Temozolomide
+ RT + Temozolomide + Bevacizumab*
Mon
ths
Treatment Regimen
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 6
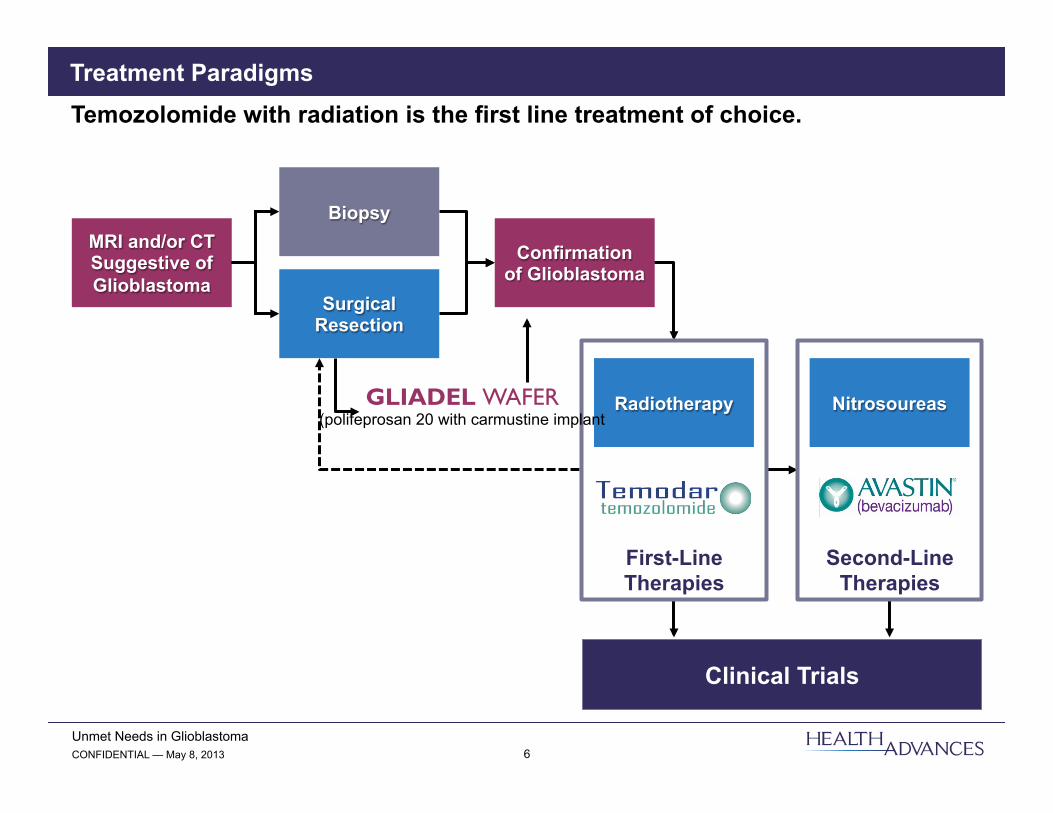
Surgical Resection
Treatment Paradigms Temozolomide with radiation is the first line treatment of choice.
MRI and/or CT Suggestive of Glioblastoma
Biopsy
Confirmation of Glioblastoma
Clinical Trials
Second-Line Therapies
Nitrosoureas
First-Line Therapies
Radiotherapy GLIADEL WAFER (polifeprosan 20 with carmustine implant
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 7
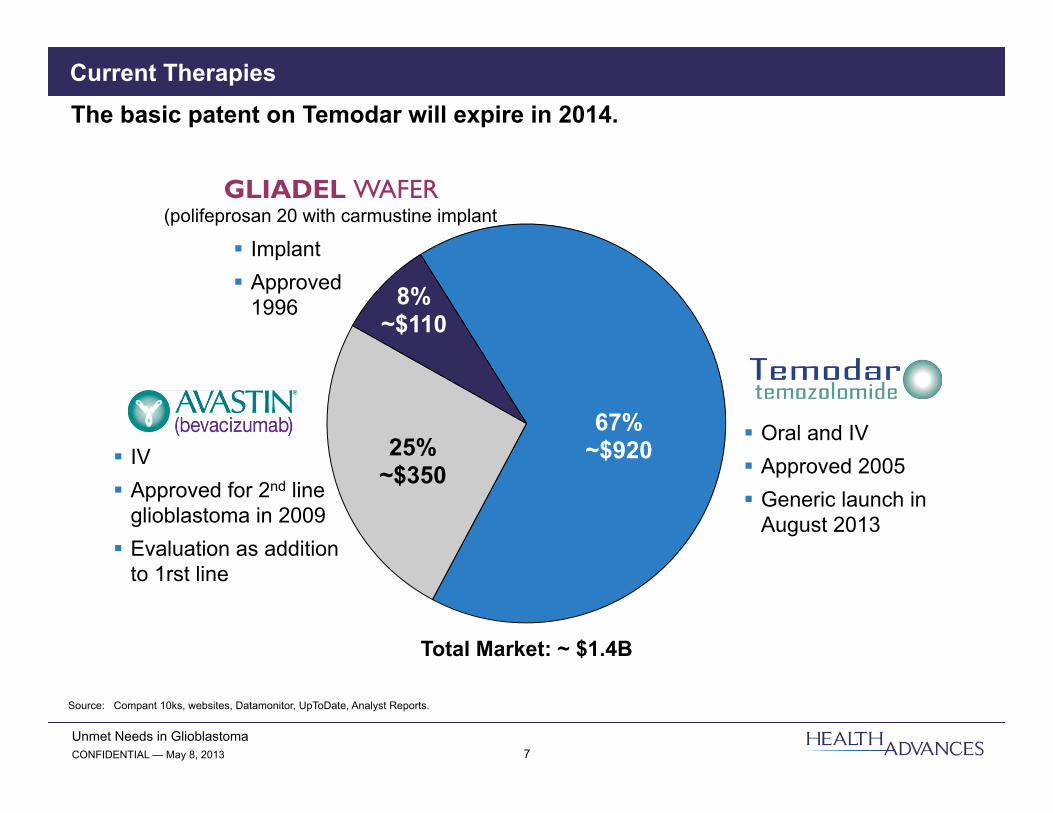
Current Therapies The basic patent on Temodar will expire in 2014.
Source: Compant 10ks, websites, Datamonitor, UpToDate, Analyst Reports.
67% ~$920 25%
~$350
8% ~$110
§ Oral and IV § Approved 2005 § Generic launch in
August 2013
§ IV § Approved for 2nd line
glioblastoma in 2009 § Evaluation as addition
to 1rst line
§ Implant § Approved
1996
GLIADEL WAFER (polifeprosan 20 with carmustine implant
Total Market: ~ $1.4B
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 8
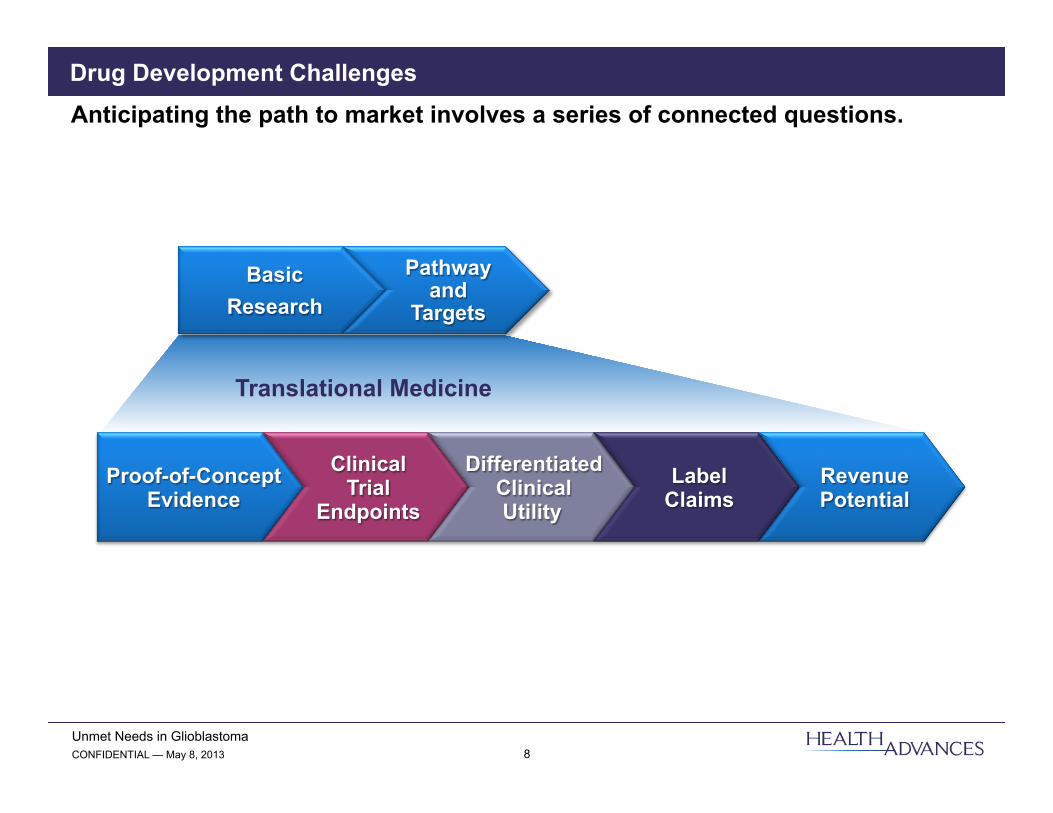
Drug Development Challenges Anticipating the path to market involves a series of connected questions.
Proof-of-Concept Evidence
Clinical Trial
Endpoints
Differentiated Clinical Utility
Label Claims
Revenue Potential
Basic Research
Pathway and
Targets
Translational Medicine

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 9
Dramatic unmet needs will drive interest in any new therapy.
Opportunities
Development Challenges
Challenges
Blood-Brain Barrier § Formulation and delivery?
Tumor Heterogeneity § Breadth of use?
Lack of Screening Tools § Risk factors? § DX prior to malignancy?
Low Incidence/Rapid Progression § Market potential? § Trial recruitment?
High Unmet Need § Incremental improvement § Risk tolerant § Rapid market uptake
Small Population, Orphan Drug Potential
Survival Drives Prevalence § Increased population § Extended duration of therapy
Pricing Flexibility § Extreme mortality § Low generic impact
Combination Therapy § Multiple mechanisms
Centers of Excellence § Focused call points § Specialty market strategy
Paucity of Biomarkers § Assessing prognosis? § Patient segmentation? § Differential treatment?
And

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 10
Development Challenges Better understanding of specific patients sub-segments can be valuable for clinical development and precision in selecting treatment options.
Frequency 25% 75% 45% 55% 50% 50%
Overall Survival 23 months1 15 months 22 months2 13 months2 15 months2 9 months2
Negative for
EGFRvIII
Positive for
EGFRvIII
EGFRvIII
Unmethyl-ated
MGMT
Methylated MGMT
MGMT Gene
Over 65 Under 65
Age
1 Data based on general patient populations treated with rindopepimut immunotherapy and temozolomide and lacking a placebo control. 2 Data based on patient populations receiving radiotherapy and temozolomide.
Source: Babu, R., Core Evidence, 2012; Hegi, M., NEJM, 2005; Oszvald, A., Journal of Neurosurgery, 2012.
Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 11
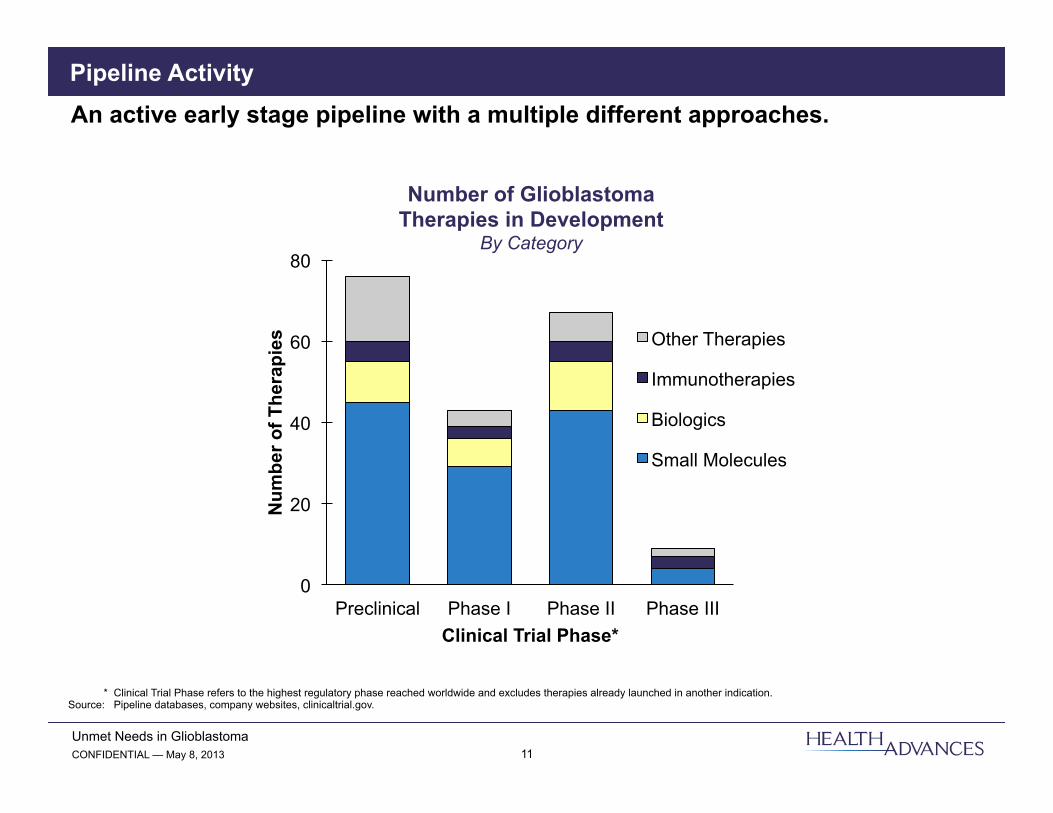
Pipeline Activity An active early stage pipeline with a multiple different approaches.
Number of Glioblastoma Therapies in Development
By Category
0
20
40
60
80
Preclinical Phase I Phase II Phase III
Num
ber o
f The
rapi
es
Clinical Trial Phase*
Other Therapies
Immunotherapies
Biologics
Small Molecules
* Clinical Trial Phase refers to the highest regulatory phase reached worldwide and excludes therapies already launched in another indication. Source: Pipeline databases, company websites, clinicaltrial.gov.

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 12
Today’s Presentations § Small molecule glycolysis inhibitor § Drug-resistant cellular therapy
§ Therapeutic vaccine § Bi-specific antibody
Pipeline Activity Presentations today reflect the diversity of therapeutic approaches being investigated.
Small Molecule
Chemotherapy
Monoclonal Antibodies
Other Approaches
§ Gene therapy § Lytic viruses § Nucleic acid
therapies § Nanoparticles § Stem cell therapy
Immunotherapies § Active immunization § Adoptive therapies
New Options for Glioblastoma
Patients

Unmet Needs in Glioblastoma CONFIDENTIAL — May 8, 2013 13
Skip Irving Partner
Health Advances LLC 9 Riverside Road
Weston, MA 02493
781-647-3435 www.healthadvances.com
Recommended