Embed Size (px)
Citation preview

The brainstem is defined as the midbrain,pons and medulla. Gliomas within thebrainstem comprise 10-20% of all
pediatric CNS tumors. In the United States, thereare approximately 150-300 annual cases (8).Brainstem gliomas can occur at any age, althoughthey generally present in childhood, with themean age of diagnosis at 7 to 9 years (14, 43,58). There is no gender predilection.
In the era before modern imaging, allbrainstem gliomas were regarded as a singlepathological entity, and the prognosis was con-sidered uniformly poor. In 1969, Matson sum-marized that “regardless of specific histology,brainstem gliomas must be classified as malig-nant tumors since their location in itself rendersthem inoperable” (45). Pool was one of the firstneurosurgeon to advocate surgery for certainbrainstem tumors. He operated upon several chil-dren and reported a survival of 10 to 25 years(33). In the early 1980s, several neurosurgeonsbegan reporting favourable surgical outcomes for
certain types of brainstem gliomas (10, 25, 27,35, 57). Classification systems were then intro-duced which attempted to identify those tumorsthat benefited from surgery. These morphologi-cal systems further evolved with the advent ofmagnetic resonance imaging (MRI), thus help-ing to predict tumor behaviour and determine thebest management algorithm for these tumors.
This article reviews the current literatureand provides treatment options for brainstemgliomas. We also present our series of brainstemtumors treated at a single institution.
IMAGING AND CLASSIFICATION
Magnetic resonance imaging has emerged as theprimary diagnostic modality for brainstem glio-mas. MRI multiplanar images assist in the es-tablishment of the tumor diagnosis, identifica-tion of tumor epicenter and prediction of its bio-logical behavior. Astrocytomas are the most com-mon intrinsic tumor of the brainstem. On histol-ogy, these tumors are fibrillary, in contrast to
CURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Jallo GI§ MD, Freed D† MS, Roonprapunt C† MD, PhD and Epstein F† MD§Division of Pediatric Neurosurgery, Johns Hopkins Hospital, Baltimore, Maryland; †Division of PediatricNeurosurgery, Institute for Neurology and Neurosurgery, Beth Israel Medical Center, New York, New York
ABSTRACT
Brainstem gliomas have historically been one of the most difficult pediatric cancers to treat.Tumors arising in the brainstem were once uniformly discounted as surgically unresectable lesions.Early neurosurgeons thought this location to be inoperable and fraught with disaster. The advent ofcomputed tomography (CT), magnetic resonance imaging (MRI) and sophisticated neurophysiologicalmonitoring techniques have significantly advanced the surgical treatment of these precarious lesions.Brainstem gliomas are now recognized as a heterogenous group of tumors. They have been broadlyclassified into several categories depending upon the classification scheme. All these classificationsystems provide a framework to predict growth patterns, surgical resectability and overall prognosisfor these heterogeneous tumors. These systems allow the surgeon to better differentiate low-gradetumors from the diffuse inoperable tumor type. The authors review the current management of brainstemtumors and their experience with brainstem gliomas over a 5 year period.
KEYWORDS: brainstem glioma • cervicomedullary • midbrain tumors • pontine glioma
Annals of Neurosurgery www.annals-neurosurgery.org
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003
1

cerebellar astrocytomas which are predominantlypilocytic. Other tumors which may arise in thebrainstem include PNET (Primitive Neuroecto-dermal Tumors), lymphomas, gangliogliomasand oligodendrogliomas (21). Lymphoma is dis-tinguished by its uniform enhancement aftergadolinium administration. Although ependymo-mas typically extend into the fourth ventricle orcerebellopontine angle, they can occasionallyresemble an intrinsic tumor of the brainstemsince they may cause brainstem compression orappear to insinuate into the brainstem. Nonneo-plastic lesions such as cavernous malformations,tuberculomas, and epidermoids have also beenreported to arise within the brainstem. Additionalimaging studies such as angiography, MRIspectroscopy or diffusion-weighted MRI se-quences may be required for the uncertain diag-nosis (23, 48). These imaging sequences havesupplanted the need for stereotactic biopsy forcertain brainstem gliomas (7).
Many classification schemes have beendevised for brainstem tumors (Table 1). The ear-liest classifications relied on computed tomog-raphy and surgical observations. More recentclassification schemes include MRI sequences.All these systems categorize the tumor byepicenter (diffuse or focal) or imaging charac-teristics. The simplest classification divides thesetumors into two groups, either focal or diffuseregardless of tumor epicenter. The more com-plex schemes subdivide these tumors by loca-tion, growth pattern (‘focality’), presence of hy-drocephalus or hemorrhage, and growth pattern.
DIFFUSE BRAINSTEM GLIOMA
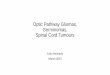
Diffuse gliomas are the most commonly encoun-tered tumor of the brainstem accounting for 58-75% of all tumors (5, 27). On T1-weighted MRIscan, they appear hypointense with indistinctmargins, reflecting the infiltrative nature of thesehigh grade lesions (Figure 1). Diffuse gliomasof the brainstem are generally greater than 2 cmin size at time of presentation. They are charac-terized by diffuse infiltration and swelling (orhypertrophy) of the brainstem. The epicenter ofthe lesion is usually the pons, however rostral orcaudal tumor extension is not unusual. Thesediffuse gliomas are distinguished from focaltumors by their indiscrete hyperintensity on T2-
weighted imaging. Gadolinium enhancement canbe variable and has no prognostic implication(30). These diffuse gliomas are typically malig-nant fibrillary astrocytomas (Grade III or IV).
FOCAL TUMORS
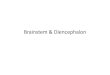
Focal tumors are defined as demarcated lesionsof the brainstem found in either the midbrain,pons or medulla. These focal tumors may be solidor cystic and they always have clear, distinctborders on MRI (Figure 2). The tumor size andcharacteristics are similar on both T1 and T2sequences because of the relative lack of infil-tration and edema. Tumor enhancement follow-ing gadolinium administration may be variable,but uniform enhancement is suggestive of a ju-venile pilocytic astrocytoma. These focal tumorsare mostly benign (Grade I or II) lesions, how-ever anaplastic gangliogliomas and PNETs havebeen reported (1).
EXOPHYTIC TUMORS
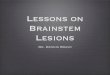
Dorsal exophytic brainstem gliomas are a groupof tumors that arise from the subependymal glialtissue (Figure 3). The bulk of the tumor resideswithin the fourth ventricle which accounts forthe relatively late onset of symptoms. MRI re-veals a well-demarcated lesion with similar T1-hypointensity and T2-hyperintensity signal char-acteristics.
On histology, these tumors are almost al-ways low-grade gliomas. They tend to growalong paths of least resistance (into the fourthventricle and into cisterns) rather than infiltratethe brainstem (36). Most of these exophytictumors will enhance with gadolinium, and canbe difficult to distinguish from ependymomas orchoroid plexus papillomas (13). In our experi-ence, exophytic tumors that grow laterally andventrally into the brainstem are higher-gradetumors as compared to those exophytic tumorsthat project dorsally into the fourth ventricle.
CERVICOMEDULLARY TUMORS
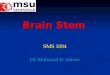
Cervicomedullary brainstem gliomas are simi-lar to intramedullary spinal cord gliomas (Fig-ure 4). The epicenter of these tumors may be ei-ther in the medulla or cervical spinal cord. OnMRI, these tumors show mixed low and inter-mediate signal intensity within the solid part of
www.annals-neurosurgery.org
2
CURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

TABLE 1
Classification Systems for Brainstem Tumors
the tumor. MRI assists in delineating the rostraland caudal pole of these tumors, as well as iden-tifying any associated syrinx or cysts.
The majority of these tumors are benign lowgrade astrocytomas, and they demonstrate dis-tinct growth patterns (28, 36). These tumors have
CT = computed tomography; MRI = magnetic resonance imaging
3
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
raey,rohtuA metsySnoitacifissalC nodesabmetsyS
5891,nietspE
cisnirtnIesuffid
lacofyralludemocivrec
cityhpoxEelgnaenitnopolleberecotnilaretaloretnA
sitnopmuihcarbotnilaretaloretsoPelcirtnevhtruofotniroiretsoP
detanimessiDygolotycevitisoP
yhpargoleymevitisoP
TC
6891,nietspE
esuffiDlacoF
amedeon,mc2nahtsselssamdebircsmucriCyralludemocivreC
dnaIRM,TCnoitavresbOlacigruS
6891,kniortS
amoilgcityhpoxelasrod-IpuorGsromutmetsniarbcisnirtni-aIIpuorG
tnemecnahneon,esnedopyhsromutmetsniarbcisnirtni-bIIpuorG
cityhpoxe,gnicnahnetsartnoc,esnedrepyhtnemecnahnetsartnochtiwromutcitsyclacof-IIIpuorG
gnicnahnetsartnoc,esnedosicisnirtnilacof-VIpuorG
TC
1991,hcivokraB
noitacoLalludem,snop,niarbdiM
ytilacoFlacofroesuffiD
htworgromutfotnetxednanoitceriDtnemegralnemetsniarbfoeergeD
htworgcityhpoxEsisorcenroegahrromeH
sulahpecordyhfoecnedivE
IRM
6991,thgirblAlacoF
alludeM,)amoilgenitnopcityhpoxelasrod(snoP,niarbdiMesuffiD
IRM
6991,niebhcsiF
niarbdiMlatcet,lacof,esuffiD
snoPlacof,esuffiD
alludeMcityhpoxelasrod,lacof,esuffiD
IRM
9991,xuohC
niytisnetniwol,TCnoesnedopyh,esuffid,romutcisnirtni-IepyTtnemecnahnetnacifingisonhtiw,segamidethgiew-1T
citsycrodilosebyamhcihw,romutlacofdnacisnirtni-IIepyTyllaretalroyllasrodrehtie,romutcityhpoxe-IIIepyT
romutyralludemocivrec-VIepyT
IRMdnaTC

FIGURE 1: Diffuse pontine glioma. (A) Sagittal T1-weighted MRI scan with gadoliniumdemonstrates an enlarged pons with minimal enhancement. (B) Axial T2-weightedsequence demonstrates the hyperintense signal within the enlarged pons.
A.
B.
4
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

A. B.
C.
FIGURE 2: Focal tumor. (A) Sagittal T1-weighted MRI with gadolinium demonstrates aheterogeneously enhancing tumor within the medulla. (B) Coronal image demonstratesthe location within the medulla. (C) Axial T2-weighted MRI demonstrates the intrinsicmedullary location.
5
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

FIGURE 3: Dorsalexophytic glioma.T1-weighted sagittalMRI of an exophytictumor within thefourth ventricle.
almost no infiltrative capacity and as a conse-quence their growth is limited rostrally by thedecussating white matter tracts of the corticos-pinal tract and medial lemniscus which act as abarrier for further rostral growth. Tumors whicharise within the medulla are confined by thedecussating fibers and expand within the me-dulla, pushing the motor tracts and nuclei pe-ripherally. Only high grade tumors with an infil-trative capacity grow rostrally into the brainstem.As a result, these low grade tumors may appearexophytic and displace the medulla rostrally,while the upper cervical cord appears expanded.
DIAGNOSIS AND MANAGEMENT
The clinical history and presentation are impor-tant in the establishment of the tumor histologyand overall prognosis. A careful history is ob-tained from both the child and parents. This isimportant since, often subtle changes may gounreported if both individuals are not inter-viewed. For example, old pictures may be nec-essary to date the onset of cranial neuropathies.Declining school performance, especially relatedto visual disturbances or symptoms of hydro-cephalus, may be the only presenting signs. Adetailed history should include previous upper
respiratory tract infections, pneumonia, orchanges in voice (3). The time to diagnosis (orlength of prodrome) is an indication of the tumorhistology.
Malignant lesions invariably have a rap-idly progressive course. Children with diffusebrainstem gliomas will often present acutely withmultiple cranial nerve signs, ataxia, long tractsigns, and cerebellar signs. Diffuse gliomas areunfortunately the most common brainstem le-sion, and regrettably, this tumor portends theworst prognosis among the brainstem gliomas.Most children die within 18 months from diag-nosis, similar to the clinical course for glioblas-toma multiforme (6, 43). There is no role forradical surgery or biopsy since stereotactic bi-opsy does not change the management strategy(7). A biopsy should be reserved for indetermi-nate lesions on MRI accompanied with an unu-sual presentation or when mandated by a studyprotocol. Diffuse brainstem tumors, which areassociated with neurofibromatosis need furtherinvestigation, because they tend to have a morefavorable prognosis. These NF-1 brainstemtumors typically have an indolent course, remi-niscent of their astrocytic counterparts in thehypothalamic/optic chiasm region (46, 51). Care-
6
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

FIGURE 4: Cervicomedullary glioma. (A) Sagittal T1-weighted MRI scan demonstratesthe extent of a typical cervicomedullary tumor. (B) Sagittal T2-weighted MRI confirmsthe extent of tumor
ful clinical examination for the stigmata of neu-rofibromatosis and family history should help inthe identification of these lesions. Magnetic reso-nance spectroscopy has also been shown to beuseful in distinguishing diffuse lesions in NF-1patients (19). Radiation and/or chemotherapy arethe current mainstay of treatment for diffusebrainstem gliomas (9).
In contrast, focal tumors are generally low-grade gliomas, and have a longer prodrome(months to years) before diagnosis when com-pared to the shorter period (weeks to months)for diffuse gliomas. The location of the focaltumor along the brainstem axis influences theclinical presentation. In general, upper brainstemtumors tend to present with hydrocephalus, ocu-lomotor dysfunction and/or cerebellar findings,whereas lower brainstem tumors present withlower cranial nerve deficits and long tract find-ings.
Midbrain gliomas of the tectum behave asvery low-grade lesions (16). Focal tumors of thetectum (tectal gliomas) begin to cause signifi-
cant neurological symptoms when they enlargeand compress the aqueduct of Sylvius therebyproducing obstructive hydrocephalus. Tegmen-tal tumors can present with hydrocephalus andoculomotor paresis with or without associatedlong-tract findings. Focal pontine gliomas gen-erally have a poorer prognosis while focal tumorsof the medulla are intermediate. Pontine lesionscause facial paresis, hearing loss or long-tractfindings. Concern should be raised when a childpresents with a localized focal non-enhancingtumor with rapid progression in symptoms.Atypical tumors which present at a very youngage and with leptomeningeal dissemination mayrepresent primitive neuroectodermal tumor(PNET) (63). An excision biopsy should be con-sidered in this situation since treatment protocolsfor PNETs differ from those for brainstem glio-mas.
Tumors of the medulla present with lowercranial nerve deficits, which manifest as changesin voice, swallowing difficulty or pneumoniadue to micro-aspirations. Although these focal
7
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

lesions are not infiltrative, they can carry a highsurgical morbidity (4). Preoperative medullarydysfunction warns of postoperative complica-tions specifically in patients demonstrating fre-quent preoperative upper respiratory tract infec-tions, preoperative pneumonia or alteration invoice (3).
Dorsally exophytic tumors may be re-garded as a type of focal tumor. There is usuallya protracted yet progressive clinical course withsymptoms due to either direct compression ofthe underlying brainstem or to raised intracra-nial pressure from obstruction of CSF pathways.Young children may present with failure to thrivedue to intractable vomiting. Older children mayexhibit headache and ataxia. Papilledema andtorticollis are common presenting signs, result-ing from increased intracranial pressure andchronic tonsillar herniation. The majority ofdorsally exophytic tumors can be managed suc-cessfully with subtotal resection, and if neces-sary, CSF diversion (Table 2) (49).
Cervicomedullary brainstem gliomas arealso associated with an indolent course. The pres-entation of these tumors is dependent on theepicenter of the lesion. Two presenting syn-dromes, a medullary and cervical cord syndrome,have been described. Medullary dysfunction maymanifest as failure to thrive due to nausea, vom-iting, or dysphagia, upper respiratory tract infec-tion, dysarthria, and sleep apnea. The cervicalcord dysfunction will manifest as chronic neckpain and progressive cervical myelopathy withweakness and spasticity. Good long-term out-comes have been achieved with radical resec-tion (Table 3) (12, 26, 53, 61).
OUR SERIES OF BRAINSTEM TUMORS
We retrospectively reviewed our tumor databasefrom 1996 to 2001 for brainstem tumors treatedat our center. We treated 135 children withbrainstem tumors. There were 85 benign (tectal,focal, dorsal exophytic, and/or cervicomedullarytumors) and 50 malignant tumors. The malig-nant tumors included 41 diffuse pontine gliomasand 9 tumors which had an equivocal diagnosison imaging studies. These 9 patients underwentsuboccipital craniotomies for radical removal ofthe tumor. The histology of these children is listedin Table 4. The overall mean survival for this
group of children with diffuse tumors was 12.1months. This is comparable to previous reportsconcerning diffuse gliomas treated with variousradiotherapy and chemotherapy protocols.
The benign tumors were distributedthroughout the brainstem, but the majority oftumors were located in the medulla (Table 5).There were 20 children with tectal gliomas whowere treated with endoscopic third ventriculos-tomy. The remaining patients underwent surgeryfor radical removal of their tumor. The predomi-nant histology in this group was low-grade as-trocytoma or ganglioglioma which accounted for54%. A malignant, anaplastic astrocytoma orglioblastoma, histology was found in only 12%of cases.
SURGICAL TREATMENT
Careful patient selection is one of the underly-ing principles behind successful brainstem tumorsurgery. The categorization of brainstem tumorshas helped to predict growth patterns and iden-tify surgically treatable lesions. Surgery for dif-fuse brainstem gliomas is generally not indicated.This section will address open surgical treatmentof focal, dorsally exophytic and cervicomedullarytumors. Certain focal lesions, particularly tectalgliomas, have an indolent natural history, anddo not generally require open surgical manage-ment. Tectal gliomas are managed by treatmentof symptomatic obstructive hydrocephalus us-ing endoscopic third ventriculostomy or shunt-ing. The advantages of endoscopic third ventricu-lostomy include avoidance of an implant deviceand potential for a minimally invasive biopsy ofthe tumor mass.
General considerations
We have favored early surgery as a firstline intervention, particularly before significantprogression of symptoms and before other treat-ments such as radiotherapy or chemotherapy areadministered. The goal of surgery is to decreasethe tumor burden without incurring significantneurological complications; this goal can oftenbe accomplished without gross total resection,however there is significant risk of morbidity.
Intraoperative neurophysiological map-ping and monitoring is recommended for allbrainstem cases (24, 47). While MRI may pro-
8
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

TABLE 2
rohtuA stneitaP ygolotsiH yregruStnavujdAyparehT
emoctuO noissergorP
3991,kcalloP 81 IIroIedarGAGL61IIIedarGamotycortsA1
amoilgoilgnaG1
latotraeN stneitap2 evila71)shtnom311,naidem(
stneitap4
4991,bitahK 21 APJ11AGL1
latotraen6latotbus6
2 evila11)shtnom62,naidem(
3
,niebhcsiF6991
01 A/N A/N A/N evila7)shtnom53,naem(
A/N
Summary of Reported Dorsal Exophytic Brainstem Tumors
rohtuA stneitaP ygolotsiH yregruStnavujdAyparehT
emoctuO noissergorP
,nietspE7891
02
IIroIedarGAGL11IIIedarGamotycortsa4
amoilgoilgnag3amomydnepe2
A/N stneitap4evila61
shtnom42,naidem(sromutedarghgihfo4/4sromutedargwolfo61/1
,nostreboR4991
71AGL01
amoilgoilgnag6amotycortsadexim1
latotbus51 2evila51
)shtnom84,naidem(sromutedargwolfo61/1
,nostreboR4991
4APJ3
amomydnepe1A/N A/N A/N stneitap6
,renieW7991
93
AGL51amomydnepe9amoilgoilgnag7
APJ3amotycortsacitsalpana3
amoilgdexim2
latotssorg21latotraen7
latotbus51laitrap5
enonevila93
)shtnom84,naem(sromutedarghgihfo4/3
sromutedargwolfo53/21
Summary of Reported Cervicomedullary Tumors
TABLE 3
Near total >90% resection, subtotal >50% but <90%, partial <50%.LGA, low grade astrocytoma; JPA, juvenile pilocytic astrocytoma
snoPamoilGenitnoPesuffiD
amotsalboilGamotycortsAcitsalpanA
TENP
14421
alludeMamomydnepEcitsalpanA
amotycortsAcitsalpanA11
TABLE 4
Malignant Tumors of the Brainstem Treated atBeth Israel Medical Center 1996-2001(Including diffuse pontine gliomas)
TABLE 5Low Grade Tumors of the Brainstem Treated at
Beth Israel Medical Center 1996-2001
9
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003
niarbdiMlatceTlacoF
0261
snoP )lacof( 7
alludeMlacoF
cityhpoxelasroD4121
yralludemocivreC 61

vide accurate localization of the tumor, it doesnot provide information regarding the functionof surrounding normal tissues. Although safeentry zones (suprafacial /infrafacial triangles,intercollicular midline incision) have been de-scribed, intrinsic tumors of the brainstem oftendistort the normal anatomy, and thus obscuringnormal landmarks (47). Neurophysiologicalmapping overcomes this limitation by identify-ing displaced structures, and thus avoidingbrainstem injury. In addition, continuous moni-toring of standard evoked potentials (motor andsensory), and cranial nerve reflex circuits can beused to give real time feedback as to the integ-rity of the brainstem during tumor resection (24).
Special microsurgical equipment, whichhave greatly enhanced the operative technique,include the operating microscope, plated bayo-nets forceps (29), Nd:YAG contact laser (38),and the Cavitron ultrasonic aspirator (CUSA)(22, 37). The current CUSA models are equippedwith smaller handsets that allow them to be safelyused in the confined limits of brainstem. Thecontact Nd:YAG laser provides precision cuttingcoupled with coagulation of adjacent tissues dueto the laser’s affinity for hemoglobin. It can beused for tumor resection with minimal injury tothe surrounding brainstem cranial nerve nuclei.Surgical approaches to the brainstem are pre-dominantly through the posterior fossa. Theprone position provides excellent exposure of theentire brainstem except for upper midbraintumors. Some surgeons prefer the sitting posi-tion (18), however the prone position reducesthe risk of venous air embolism andpneumocephalus. In addition, the prone positionprovides a surgical field that is readily accessi-ble to both the surgeon and assistant. The sur-geon’s arms are not elevated throughout the caseand there is less general fatigue. Proper position-ing, especially with regard to neck flexion andshoulder placement is important for adequatevisualization of the anticipated lesion. There aremany different skull base approaches availabledepending on the location of the tumor.
Midbrain
Although most tumors of the upper midbrain aremanaged conservatively with CSF diversion,some tumors in this area progress and require
open surgery. The dorsal midbrain can be ex-posed by the infratentorial-supracerebellar ap-proach first described by Krause and then popu-larized by Stein (56). A craniotomy is fashionedto incorporate the transverse sinus. The cerebel-lum and vermis may then be retracted caudallyto expose the dorsal aspect of the mesencephalon.This approach allows direct access to the mid-brain without intervening brain tissue (11). Thedeep venous drainage system, including the veinof Galen and internal cerebral veins, are gener-ally above the surgical field and thus easilyavoided. Lesions on the ventral medial aspect ofthe midbrain near the interpeduncular cistern arereached by a standard pterional approach. Ven-tral lateral masses of the midbrain may bereached by a subtemporal approach and usuallyinvolve splitting the tentorial incisura. It shouldbe kept in mind, however, that the subtemporalapproach has the disadvantage of potentially re-quiring prolonged retraction of the temporal lobe.
Pons
For dorsally-situated tumors of the pons or me-dulla, a midline suboccipital craniotomy is themost common approach in our practice. A crani-otomy is generally preferred over a craniectomyespecially in children (34). Replacement of thebone flap provides additional protection, and al-lows better restoration of anatomical tissueplanes, which becomes important in the unfor-tunate patients who may require multiple resec-tions (42). The telovelar approach provides ad-equate exposure to all dorsally exophytic tumors(52). Excessive traction on the cerebellar hemi-spheres and dissection on the vermis should beavoided, because of the risk of cerebellar mut-ism and pseudobulbar symptoms (50, 62). Forfocal intrinsic tumors, the resection begins afterthe floor of the fourth ventricle has been identi-fied and mapped for safe points of entry. If dis-tortion and discoloration of the floor are insuffi-cient to localize the tumor, ultrasound can be usedto determine where the tumor is closest to thefloor.
Tumors of the ventral lateral aspect of thepons extending into the cerebellopontine anglemay be reached with the lateral retrosigmoid ap-proach. The asterion, which is formed by thelambdoid and temporal squamous sutures, is a
10
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

useful landmark for planning the bony removal.The junction of the transverse and sigmoid si-nuses is identified, and used as a guide for duralopening. The tumor may be debulked with spe-cial attention to the location of the tracts of cra-nial nerves 5, 7 and 8, and, if involving the me-dulla, 9 and 10.
Medulla and upper cervical spine
For intrinsic tumors of the medulla, a sub-occipital craniotomy with removal of the dorsallateral bony rim of the foramen magnum en-hances the exposure of the bulging medulla. Acervical laminotomy or laminectomy is per-formed for tumors which extend caudally intothe cervical region. The medulla is typically dis-placed superiorly as the tumor grows posteriorto the obex. The tumor is quite superficial here,almost invariably subpial in location. The pos-terior inferior cerebellar arteries, which may bedisplaced, must be preserved to avoid cerebellaror brainstem infarcts. However, superficial pialvessels may be taken if obstructing the intramed-ullary component of tumor.
Special considerations
One of the early considerations for abrainstem focal tumor is to determine a safe en-try point. Cystic focal tumors are generally easierto treat than solid lesions, because they can bemore easily entered and their walls inspected fortumor nodules without having to manipulate thesurrounding tissue. Discoloration and loss of sur-face markings may be used as rough guides inmapping the floor of the fourth ventricle whensearching for safe entry zones. The contact laseris used to perform the initial incision ormyelotomy into the brainstem. This processeliminates the superficial feeding blood vesselsand initiates tumor retraction. What often hin-ders complete resection is the lack of tumor de-marcation from the surrounding brain. The neu-rosurgeon must remember that complete resec-tion is prohibitive if there is no discernible planebetween tumor and brainstem parenchyma dueto the high probability for postoperative morbid-ity. It should also be kept in mind that a near-total resection, with a thin residual tumor mar-gin, is equally successful. It is important to mini-mize retraction of surrounding neural tissue dur-
ing the resection. The tumor is removed in apiecemeal fashion using a combination of suc-tion-aspiration and the CUSA. Tumor debulkingand dissection is achieved by working from theinside-out direction. The Nd:YAG laser is some-times helpful in removing small amounts oftumor at the margins or in tight confines. Cau-tery is to be avoided at the margins of the tumoras this will frequently result in injury to the sur-rounding functional tissue. Mapping of the wallsof the resection cavity can be performed in anattempt to define tumor margins. Tissue speci-mens are always sent early for frozen sectionanalysis. If the lesion is identified as a high-gradetumor, then the operation is generally curtailed,because there has been no proven long-term ben-efit to surgical debulking of these aggressive le-sions.
Dorsally exophytic tumors were the firsttype of brainstem gliomas to be routinely treatedwith radical surgery (30, 41, 49). Most of thedissection and removal is accomplished outsideof the brainstem since these tumors are predomi-nantly localized in the fourth ventricle. Thesetumors are approached via a standard midlinesuboccipital approach. One of the most impor-tant aspects of the case is to progressively debulkthe tumor while keeping the floor of the fourthventricle in view as it is important not to enterthe brainstem parenchyma. Cranial nerves 6 & 7are especially susceptible to injury because theirnuclei and/or tracks are close to the dorsal sur-face of the stem and the floor of the 4th ventri-cle. The area immediate around the obex andcalamus scriptorius should be avoided, becauseof possible injury to cranial nuclei for 10 & 12.When these structures are injured, patients de-velop impaired swallowing, loss of cough reflex,and dysphonia. A subtotal resection with preser-vation of neurological function is the goal of thesurgery.
Patients with cervicomedullary tumors alsobenefit from radical surgical treatment (12, 26,53, 61). A midline suboccipital craniotomy andcervical laminectomies provide the necessary ex-posures. Excessive removal of cervical laminais avoided to prevent the development of spinaldeformity. Osteoplastic laminectomy is consid-ered if a multilevel cervical laminectomy is re-quired (2). Although this technique may not al-
11
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

ways prevent deformity, there is re-ossificationof the bony segments which can avoid the cos-metic deformity frequently seen with multilevellaminectomies. The location of the tumor andany associated cysts is confirmed with the ultra-sound. A midline myelotomy is performed withthe Nd:YAG laser in order to avoid injury to theposterior columns. The myelotomy is first di-rected over any associated rostral or caudal cyst,and then extended over the solid part of thetumor. Identification of the dorsal root entryzones bilaterally is necessary to properly find themidline. This can be done visually or with map-ping of the dorsal surface to establish the mid-line between the two dorsal columns (24). Thetumor’s dorsal surface is exposed, and the tumorentered with a piecemeal removal from the centeroutwards performed. This is done using theCUSA, laser, and bipolar cautery with the sametechniques described earlier for intrinsic focalbrainstem tumors. Meticulous care in the clo-sure is important for the avoidance of a CSF leak,a complication not uncommon when operatingon these tumors.
Potential complications
Clinically, the patient’s preoperative symp-toms may be transiently or permanently wors-ened after surgery. For that reason special careneeds to be taken during the postoperative pe-riod (60).
If a significant amount of the medulla isinvolved with tumor, the patient is left intubatedfor at least 48 to 72 hours after surgery. This iscritically important for any patient with evidenceof dysfunction in lower cranial nerves. Impairedcentral respiratory function may result in carbondioxide retention and progressive hypoxia lead-ing to respiratory arrest and further neurologicalinjury which is usually permanent (4). The pa-tient is weaned from the ventilator after 24 con-secutive hours of stable respiratory drive.
Cranial nerve deficits are variable and de-pendent on the surgical approach. Surgery withinthe pons can result in transient diplopia due tointernuclear ophthalmoplegia. This complicationis often transient and improves. For persistentdiplopia, ophthalmologic treatment with specialeyeglass prisms may be necessary. Facial palsycan be devastating not only cosmetically but also
functionally with regard to corneal injury. Sev-eral plastic surgical procedures have been de-veloped to restore facial tone and protect the eyefrom corneal abrasions and keratitis (54). Dam-age to the lower cranial nerves (9-12) can resultin severe dysphagia, vocal cord paralysis, andloss of gag and cough reflexes. As a result, thesepatients are at risk for subclinical micro-aspira-tions, which may lead to recurrent and debilitat-ing pneumonia. Formal swallowing evaluationsare performed for all patients with questionablefunction before advancement of diet. Becauseof these latter risks we have learned to be ag-gressive in employing tracheostomy and feed-ing gastrostomy in the first several months aftersurgery when there is swallowing dysfunction.
ONCOLOGIC OUTCOME
Although a neuro-oncologist coordinates theadjuvant care for all patients, the neurosurgeonshould be aware of the protocols for brainstemgliomas. Radiation therapy has provided onlymarginal gains in the overall prognosis for dif-fuse high-grade tumors. Standard irradiationtreatment combined with new chemotherapyprotocols have had some mixed results (Table6) (15, 20, 31, 32, 39, 40, 59). These issues arereviewed elsewhere (9). There are new therapeu-tic options under current investigation includ-ing convection-enhanced delivery (44, 55), ra-dio-sensitizing agents, hyperbaric and intersti-tial radiotherapy.
There have been minimal improvementsin long-term survival of low grade brainstemgliomas directly attributed to adjuvant therapy.Given the significant advances in surgical man-agement of brainstem lesions and decrease insurgical morbidity, second surgery has becomea viable option (17). Indications for the secondsurgery have included: (1) delayed, recurrentgrowth in either the solid or cystic componentof the tumor resulting in new symptoms or (2)re-exploration after the initial resection washalted prematurely due to transient intraoperativeinjury confirmed by monitoring. The goal ofthese re-operations is identical to that of the firstoperation; i.e., sufficient debulking of the tumorso as to lessen symptoms without causing pro-gression in neurologic deficits.
12
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

����������� �
������������� ���
����������������������
� �� �����������������������
������ ����������������������
�����������
���� �����������
��
�� ������
������ ��������
�����!����� ��������!���
� ������ ��������������������
����������"#$���!�������
���������������������%�&������'($)*
'�
FIGURE 5. Surgical management algorithm for brainstem tumors in childrenNF-1 = neurofibromatosis 1
yparehtomehC yparehtoidaR stneitaP emoctuO
elozadinosiM,UDH,UNCC,UF-5 yG55 82skeew44TSM
PPOC yG65 7shtnom4tanoissergorP
enosinderP,UNCC,RCV yG06-05TR53
omehC+TR93smrahtobshtnom9TSM
edimafsoforT,61-PV yG45 81syad971SFP
61-PV,nitalpobraC yG2.07 9skeew44tadeid9/8
TABLE 6
Chemotherapy and Radiotherapy Protocols for the Treatment of Diffuse Pontine Gliomas
MST, mean survival time; PFS, progression-free survival
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003
13

CONCLUSION
Brainstem gliomas are a heterogenous group oftumors, which may be diffuse, focal, dorsallyexophytic, or cervicomedullary. These classifi-cation schemes help in predicting growth pat-
terns and identifying surgically treatable lesions.Almost all diffuse tumors are malignant and non-resectable. The majority of other tumors are fo-cal low-grade astrocytomas that are amenable tosurgical cure and long-term survival.
14
REFERENCES
1. Abbott R: Tumors of the medulla. Neurosurg ClinN Am 4:519-527, 1993.
2. Abbott R, Feldstein N, Wisoff JH, Epstein FJ:Osteoplastic laminotomy in children. PediatrNeurosurg 18:153-156, 1992.
3. Abbott R, Shiminski-Maher T, Epstein FJ: Intrinsictumors of the medulla: predicting outcome aftersurgery. Pediatr Neurosurg 25:41-44, 1996.
4. Abbott R, Shiminski-Maher T, Wisoff JH, EpsteinFJ: Intrinsic tumors of the medulla: surgicalcomplications. Pediatr Neurosurg 17:239-244,1991.
5. Albright AL: Brain stem gliomas, in Youmans J4th (ed) Neurological Surgery. Philadelphia,W.B. Saunders Co., 1996, pp 2603-2611.
6. Albright AL, Guthkelch AN, Packer RJ, Price RA,Rourke LB: Prognostic factors in pediatric brain-stem gliomas. J Neurosurg 65:751-755, 1986.
7. Albright AL, Packer RJ, Zimmerman R, Rorke LB,Boyett J, Hammond GD: Magnetic resonancescans should replace biopsies for the diagnosisof diffuse brain stem gliomas: a report from theChildren’s Cancer Group. Neurosurgery33:1026-1030, 1993.
8. Allen J: Brain stem glioma. Neurology andNeurosurgery: Update Series 4:2-7, 1983.
9. Allen JC, Siffert J: Contemporary chemotherapyissues for children with brainstem gliomas.Pediatr Neurosurg 24:98-102, 1996.
10. Alvisi C, Cerisoli M, Maccheroni ME: Long-termresults of surgically treated brainstem gliomas.Acta Neurochir 76:12-17, 1985.
11. Ammirati M, Bernardo A, Musumeci A, BricoloA: Comparison of different infratentorial-supracerebellar approaches to the posterior andmiddle incisural space: a cadaveric study. JNeurosurg 97:922-928, 2002.
12. Behnke J, Christen HJ, Bruck W, Markakis E:Intra-axial endophytic tumors in the pons and/or medulla oblongata. I. Symptoms,
neuroradiological findings, and histopathologyin 30 children. Childs Nerv Syst 13:122-134,1997.
13. Beltramello A, Lombardo MC, Masotto B, BricoloA: Imaging of brain stem tumors. OperativeTechniques in Neurosurgery 3:87-105, 2000.
14. Berger MS, Edwards MS, LaMasters D, Davis RL,Wilson CB: Pediatric brain stem tumors:radiographic, pathological, and clinicalcorrelations. Neurosurgery 12:298-302, 1983.
15. Blaney S, Berg SL, Pratt C, Weitman S, SullivanJ, Luchtman-Jones L, Bernstein M: A phase Istudy of irinotecan in pediatric patients: apediatric oncology group study. Clin CancerRes 7:32-37, 2001.
16. Bowers DC, Georgiades C, Aronson LJ, CarsonBS, Weingart JD, Wharam MD, Melhem ER,Burger PC, Cohen KJ: Tectal gliomas: naturalhistory of an indolent lesion in pediatric patients.Pediatr Neurosurg 32:24-29, 2000.
17. Bowers DC, Krause TP, Aronson LJ, Barzi A,Burger PC, Carson BS, Weingart JD, WharamMD, Melhem ER, Cohen KJ: Second surgeryfor recurrent pilocytic astrocytoma in children.Pediatr Neurosurg 34:229-234, 2001.
18. Bricolo A: Surgical managment of intrinsic brainstem gliomas. Operative Techniques inNeurosurgery 3:137-154, 2000.
19. Broniscer A, Gajjar A, Bhargava R, Langston JW,Heideman R, Jones D, Kun LE, Taylor J: Brainstem involvement in children withneurofibromatosis type 1: role of magneticresonance imaging and spectroscopy in thedistinction from diffuse pontine glioma.Neurosurgery 40:331-338, 1997.
20. Broniscer A, Leite CC, Lanchote VL, MachadoTM, Cristofani LM: Radiation therapy and high-dose tamoxifen in the treatment of patients withdiffuse brainstem gliomas: results of a Braziliancooperative study. Brainstem GliomaCooperative Group. J Clin Oncol 18:1246-1253,2000.
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

21. Choux M, Lena G, Do L: Brainstem tumors, inChoux M, Di Rocco C, Hockley A (eds):Pediatric Neurosurgery. New York: ChurchillLivingstone, 2000, pp 471-491.
22. Constantini S, Epstein F: Ultrasonic dissection inneurosurgery, in Wilkins RH, Rengachary SS(eds): Neurosurgery, ed 2, New York: McGraw-Hill, 1996, Vol 1, pp 607-608.
23. Dechambre S, Duprez T, Lecouvet F, RaftopoulosC, Gosnard G: Diffusion-weighted MRIpostoperative assessment of an epidermoidtumour in the cerebellopontine angle.Neuroradiology 41:829-831, 1999.
24. Deletis V, Sala F, Morota N: Intraoperativeneurophysiological monitoring and mappingduring brain stem surgery: a modern approach.Operative Techniques in Neurosurgery 3:109-113, 2000.
25. Epstein F, McCleary EL: Intrinsic brain-stemtumors of childhood: surgical indications. JNeurosurg 64:11-15, 1986.
26. Epstein F, Wisoff J: Intra-axial tumors of thecervicomedullary junction. J Neurosurg67:483-487, 1987.
27. Epstein F, Wisoff JH: Intrinsic brainstem tumorsin childhood: surgical indications. J Neurooncol6:309-317, 1988.
28. Epstein FJ, Farmer JP: Brain-stem glioma growthpatterns. J Neurosurg 78:408-412., 1993.
29. Epstein FJ, Ozek M: The plated bayonet: a newinstrument to facilitate surgery for intra-axialneoplasms of the spinal cord and brain stem.Technical note. J Neurosurg 78:505-507, 1993.
30. Fischbein NJ, Prados MD, Wara W, Russo C,Edwards MS, Barkovich AJ: Radiologicclassification of brain stem tumors: correlationof magnetic resonance imaging appearance withclinical outcome. Pediatr Neurosurg 24:9-23,1996.
31. Freeman CR, Bourgouin PM, Sanford RA, CohenME, Friedman HS, Kun LE: Long term survivorsof childhood brain stem gliomas treated withhyperfractionated radiotherapy. Clinicalcharacteristics and treatment related toxicities.The Pediatric Oncology Group. Cancer 77:555-562, 1996.
32. Freeman CR, Kepner J, Kun LE, Sanford RA,Kadota R, Mandell L, Friedman H: A detrimental
effect of a combined chemotherapy-radiotherapyapproach in children with diffuse intrinsic brainstem gliomas? Int J Radiat Oncol Biol Phys47:561-564, 2000.
33. Gilday DL, Ash J: Accuracy of brain scanning inpediatric craniocerebral neoplasms. Radiology117:93-97, 1975.
34. Gnanalingham KK, Lafuente J, Thompson D,Harkness W, Hayward R: Surgical proceduresfor posterior fossa tumors in children: doescraniotomy lead to fewer complications thancraniectomy? J Neurosurg 97:821-826, 2002.
35. Hoffman HJ, Becker L, Craven MA: A clinicallyand pathologically distinct group of benign brainstem gliomas. Neurosurgery 7:243-248, 1980.
36. Jallo G, Kothbauer K, Epstein F: Surgicalmanagment of cervicomedullary and dorsallyexophytic brain stem tumors. OperativeTechniques in Neurosurgery 3:131-136, 2000.
37. Jallo GI: CUSA EXcel ultrasonic aspirationsystem. Neurosurgery 48:695-697, 2001.
38. Jallo GI, Kothbauer KF, Epstein FJ: Contact lasermicrosurgery. Childs Nerv Syst 18:333-336,2002.
39. Kaplan AM, Albright AL, Zimmerman RA, RorkeLB, Li H, Boyett JM, Finlay JL, Wara WM,Packer RJ: Brainstem gliomas in children. AChildren’s Cancer Group review of 119 cases.Pediatr Neurosurg 24:185-192, 1996.
40. Kedar A, Maria BL, Graham-Pole J, Ringdahl DM,Quisling RG, Mickle JP, Mendenhall NP, MarcusRB, Jr., Gross S: High-dose chemotherapy withmarrow reinfusion and hyperfractionatedirradiation for children with high-risk braintumors. Med Pediatr Oncol 23:428-436, 1994.
41. Khatib ZA, Heideman RL, Kovnar EH, LangstonJA, Sanford RA, Douglas EC, Ochs J, JenkinsJJ, Fairclough DL, Greenwald C, et al.:Predominance of pilocytic histology in dorsallyexophytic brain stem tumors. PediatrNeurosurg 20:2-10, 1994.
42. Kurpad SN, Cohen AR: Posterior fossacraniotomy: an alternative to craniectomy.Pediatr Neurosurg 31:54-57, 1999.
43. Littman P, Jarrett P, Bilaniuk LT, Rorke LB,Zimmerman RA, Bruce DA, Carabell SC, SchutL: Pediatric brain stem gliomas. Cancer45:2787-2792, 1980.
15
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

44. Lonser RR, Walbridge S, Garmestani K, ButmanJA, Walters HA, Vortmeyer AO, Morrison PF,Brechbiel MW, Oldfield EH: Successful and safeperfusion of the primate brainstem: in vivomagnetic resonance imaging of macromoleculardistribution during infusion. J Neurosurg97:905-913, 2002.
45. Matson DD: Tumors of the posterior fossa. In:Neurosurgery of Infancy and Childhood. 2nd(ed) Springfield, IL, Thomas, 1969, pp 469-477.
46. Milstein JM, Geyer JR, Berger MS, Bleyer WA:Favorable prognosis for brainstem gliomas inneurofibromatosis. J Neurooncol 7:367-371,1989.
47. Morota N, Deletis V, Epstein FJ, Kofler M, AbbottR, Lee M, Ruskin K: Brain stem mapping:neurophysiological localization of motor nucleion the floor of the fourth ventricle.Neurosurgery 37:922-930, 1995.
48. Murakami N, Matsushima T, Kuba H, Ikezaki K,Morioka T, Mihara F, Inamura T, Fukui M:Combining steady-state constructive interferenceand diffusion-weighted magnetic resonanceimaging in the surgical treatment of epidermoidtumors. Neurosurg Rev 22:159-162, 1999.
49. Pollack IF, Hoffman HJ, Humphreys RP, BeckerL: The long-term outcome after surgicaltreatment of dorsally exophytic brain-stemgliomas. J Neurosurg 78:859-863, 1993.
50. Pollack IF, Polinko P, Albright AL, Towbin R, FitzC: Mutism and pseudobulbar symptoms afterresection of posterior fossa tumors in children:incidence and pathophysiology. Neurosurgery37:885-893, 1995.
51. Raffel C, McComb JG, Bodner S, Gilles FE:Benign brain stem lesions in pediatric patientswith neurofibromatosis: case reports.Neurosurgery 25:959-964, 1989.
52. Rhoton AL: Cerebellum and Fourth Ventricle.Neurosurgery(Supplement) 47:S7-S27, 2000.
53. Robertson PL, Allen JC, Abbott IR, Miller DC,Fidel J, Epstein FJ: Cervicomedullary tumors inchildren: a distinct subset of brainstem gliomas.Neurology 44:1798-1803, 1994.
54. Rose E: Aesthetic Facial Restoration. New York:Lippincott-Raven Publishers, 1998.
55. Sandberg DI, Edgar MA, Souweidane MM:Convection-enhanced delivery into the ratbrainstem. J Neurosurg 96:885-891, 2002.
56. Stein B: The infratentorial supracerebellarapproach to pineal lesions. J Neurosurg:197-202, 1971.
57. Stroink AR, Hoffman HJ, Hendrick EB,Humphreys RP, Davidson G: Transependymalbenign dorsally exophytic brain stem gliomas inchildhood: diagnosis and treatmentrecommendations. Neurosurgery 20:439-444,1987.
58. Walker DA, Punt JA, Sokal M: Clinicalmanagement of brain stem glioma. Arch DisChild 80:558-564, 1999.
59. Walter AW, Gajjar A, Ochs JS, Langston JW,Sanford RA, Kun LE, Heideman R: Carboplatinand etoposide with hyperfractionatedradiotherapy in children with newly diagnoseddiffuse pontine gliomas: a phase I/II study. MedPediatr Oncol 30:28-33, 1998.
60. Wang G, Zhang J, Sun M, Wang C: Surgicalmanagement of brainstem mass lesions:respiratory insufficiency occurrence andrecovery. Neurosurgery Quarterly 11:302-313,2001.
61. Weiner HL, Freed D, Woo HH, Rezai AR, Kim R,Epstein FJ: Intra-axial tumors of thecervicomedullary junction: surgical results andlong-term outcome. Pediatr Neurosurg 27:12-18, 1997.
62. Wisoff JH, Epstein FJ: Pseudobulbar palsy afterposterior fossa operation in children.Neurosurgery 15:707-709, 1984.
63. Zagzag D, Miller DC, Knopp E, Farmer JP, LeeM, Biria S, Pellicer A, Epstein FJ, Allen JC:Primitive neuroectodermal tumors of thebrainstem: investigation of seven cases.Pediatrics 106:1045-1053, 2000.
Correspondence:Jallo GI, Division of Pediatric Neurosurgery, The JohnsHopkins Hospital, Harvey 811, 600 North Wolfe Street,Baltomore, MD 21287. Tel.: 410-955 7851; Fax.: 410-955 7862;
Submitted: 20 December 2002Accepted: 26 May 2003Published: 21 August 2003
16
www.annals-neurosurgery.orgCURRENT MANAGEMENT OF BRAINSTEM GLIOMAS
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003

COMMENTS
The authors have provided a useful review articleon the current approaches to brainstem gliomas.Based on a five year review of their experiencewith these lesions they have proposed a surgicalalgorithm of management. This distinguishesbetween inoperable tumours and those amenableto surgery. The article provides helpful guidelinesto differentiate these tumours based on theclinical history and radiological findings. Therelated literature review is comprehensive, up-to-date and correlates with the text.
Bruce MathewHull Royal InfirmaryHull, UK
I read this article with deep interest. There is nonew knowledge however, this is an excellentreview and retains enough information for thepractioners to appreciate.
Diffusely involved tumors in the brainstem arebiologically malignant and not amenable tosurgical resection. The surgery has no role in thetreatment except for CSF diversion surgery for
associated obstructive hydrocephalus. Radiationand chemotherapy are the current mainstay oftreatment, however the results of these adjunctivetreatment are disappointing, and do not improvethe long term prognosis. Surgery can be of help when the tumor is focal,exophytic or preferably localized in thecervicomedullary junctional area. Although itseems to be that there are some benefits fromsurgery, yet it poses some concern due to anunacceptable postoperative morbidity and or therisk of the long term neurological deficits. The statistics show that regardless of differentmodes of treatment more than 80% of the patientswill succumb within 2 years of diagnosis.
Authors illustrated their wide experiences in 135cases of brain stem tumors. The perioperativeconsideration and surgical techniques areelegantly described. The authors are to becongratulated for this excellent review article.
Yoon S HahnUniversity of Illionois at ChicagoChicago, US
Annals of Neurosurgery, 2003; 3(1): 1-17© Annals of Neurosurgery & Jallo GI et al. 2003
CURRENT MANAGEMENT OF BRAINSTEM GLIOMAS www.annals-neurosurgery.org
17