BENIGN
SKIN LESIONS
ALLPPT.com _ Free PowerPoint Templates, Diagrams and Charts
facebook.com/groups/dermatologycourseonline

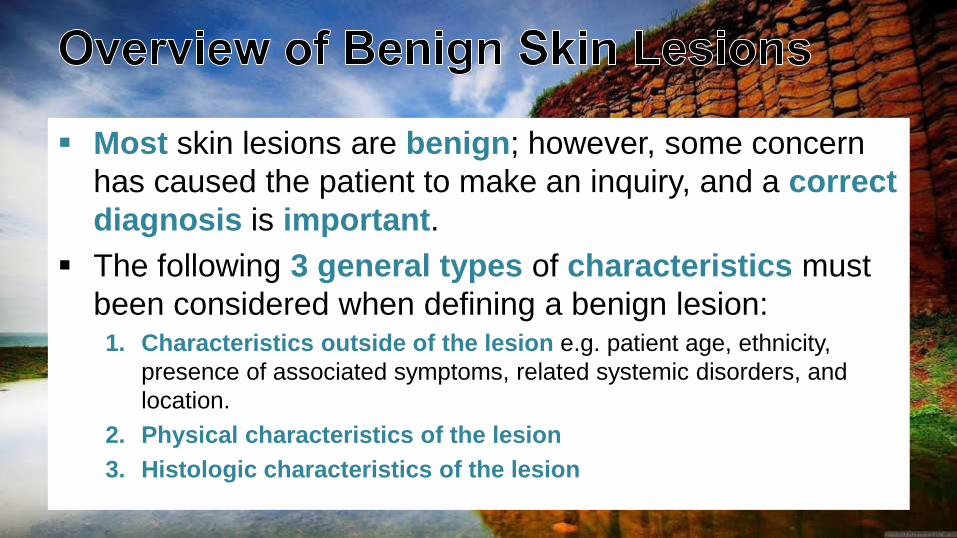
Most skin lesions are benign; however, some concern
has caused the patient to make an inquiry, and a correct
diagnosis is important.
The following 3 general types of characteristics must
been considered when defining a benign lesion:1. Characteristics outside of the lesion e.g. patient age, ethnicity,
presence of associated symptoms, related systemic disorders, and
location.
2. Physical characteristics of the lesion
3. Histologic characteristics of the lesion
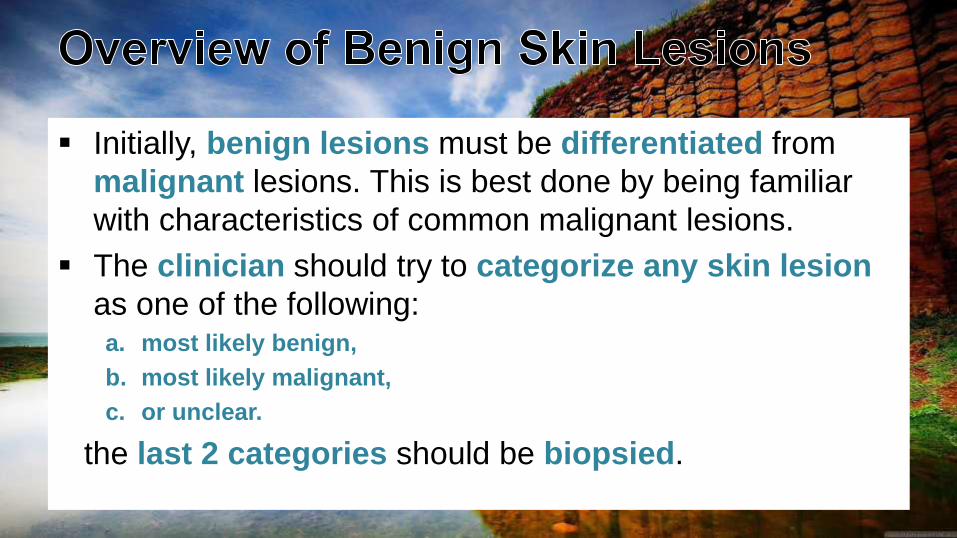
Initially, benign lesions must be differentiated from
malignant lesions. This is best done by being familiar
with characteristics of common malignant lesions.
The clinician should try to categorize any skin lesion
as one of the following: a. most likely benign,
b. most likely malignant,
c. or unclear.
the last 2 categories should be biopsied.
Benign lesions of the surface epithelium.
Cutaneous Cysts.
Benign Melanocytic Neoplasms
Neoplasms and proliferations of follicular lineage
Neoplasms and proliferations with sebaceous differentiation
Neoplasms and proliferations with apocrine differentiation
Neoplasms and proliferations with eccrine differentiation
Fibrous and Fibrohistiocytic Proliferations of the Skin and Tendons
Muscle, Adipose and Cartilage Neoplasms
Vascular Neoplasms
MULTIPLE SOLITARY LINEAR
1. Seborrheic keratosis2. DPN3. Stucco keratosis4. Disseminated superficial
actinic porokeratosis5. Porokeratosis palmaris
et plantaris disseminata6. Acrokeratosis
verruciformis of Hopf
1. Inverted follicular keratosis
2. Keratoacanthoma3. Cutaneous horn4. Clear cell acanthoma5. Warty dyskeratoma6. Lichenoid keratosis
1. Epidermal nevus2. ILVEN3. Linear porokeratosis4. Nevus comedonicus5. Mosaic form of Darier
disease
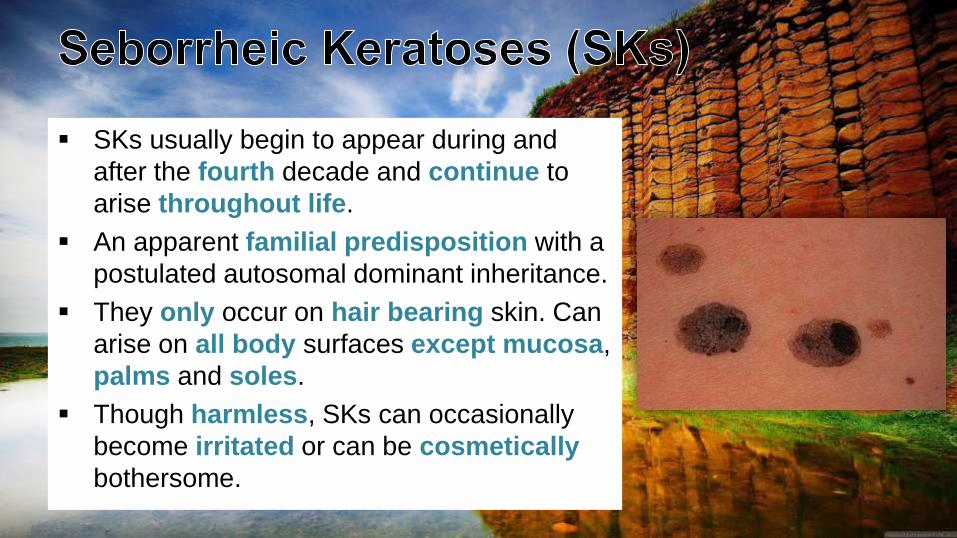
SKs usually begin to appear during and
after the fourth decade and continue to
arise throughout life.
An apparent familial predisposition with a
postulated autosomal dominant inheritance.
They only occur on hair bearing skin. Can
arise on all body surfaces except mucosa,
palms and soles.
Though harmless, SKs can occasionally
become irritated or can be cosmetically
bothersome.
The exact cause of seborrhoeic keratoses is not known may be;
1. There is a familial predisposition in those with hundreds of lesions.
2. Sun exposure (Although SKs are common in areas covered by
clothing) higher prevalence of SKs within sun-exposed areas such
as the head and neck in contrast to non-sun exposed areas in the
same subjects.
3. Very rarely, eruptive SKs may denote an underlying internal
malignancy. The syndrome is known as the sign of Leser-Trélat.
4. Neoplastic origin (somatic mutations).
5. HPV may be implicated.
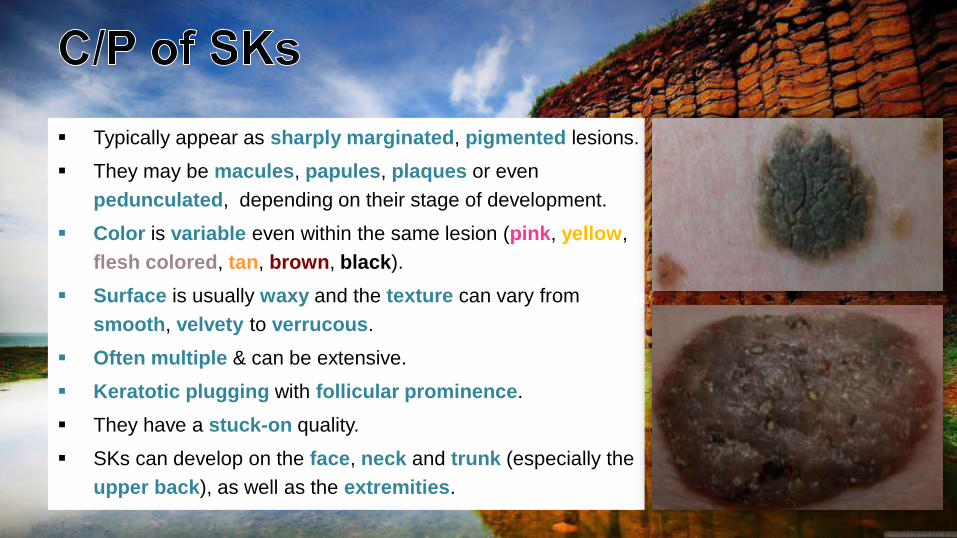
Typically appear as sharply marginated, pigmented lesions.
They may be macules, papules, plaques or even
pedunculated, depending on their stage of development.
Color is variable even within the same lesion (pink, yellow,
flesh colored, tan, brown, black).
Surface is usually waxy and the texture can vary from
smooth, velvety to verrucous.
Often multiple & can be extensive.
Keratotic plugging with follicular prominence.
They have a stuck-on quality.
SKs can develop on the face, neck and trunk (especially the
upper back), as well as the extremities.
Usually measure about 1 cm in diameter but they can
become quite large, i.e. > 5 cm in diameter.
Lesions may become inflamed due to rupture of the small
pseudocysts they contain or from trauma, or rarely from
infection with microorganisms such as Staphylococcus
aureus.
Conditions associated with an abrupt “flare” of lesions
followed by regression include pregnancy, coexisting
inflammatory dermatoses (in particular erythroderma) and
malignancy.
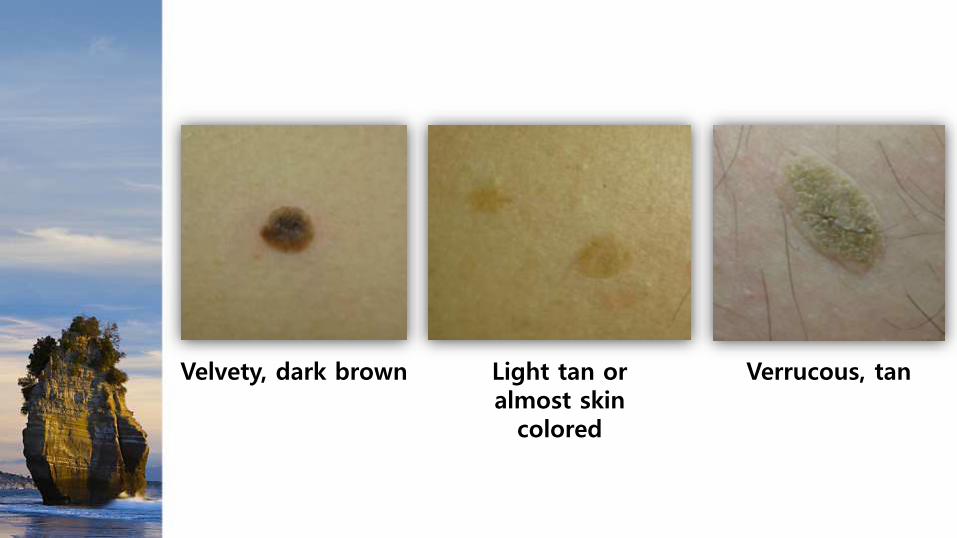
Velvety, dark brown Verrucous, tanLight tan or almost skin
colored

Multiple SKs

Multiple SKs
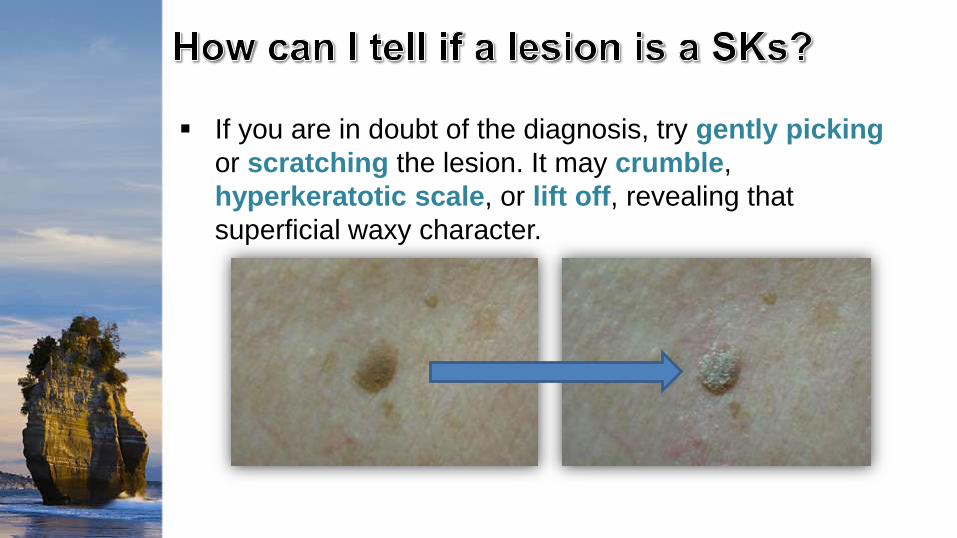
If you are in doubt of the diagnosis, try gently picking
or scratching the lesion. It may crumble,
hyperkeratotic scale, or lift off, revealing that
superficial waxy character.

This SK has been partially picked off (If picked off
or curetted, SKs will leave a pink moist base with
minimal bleeding)
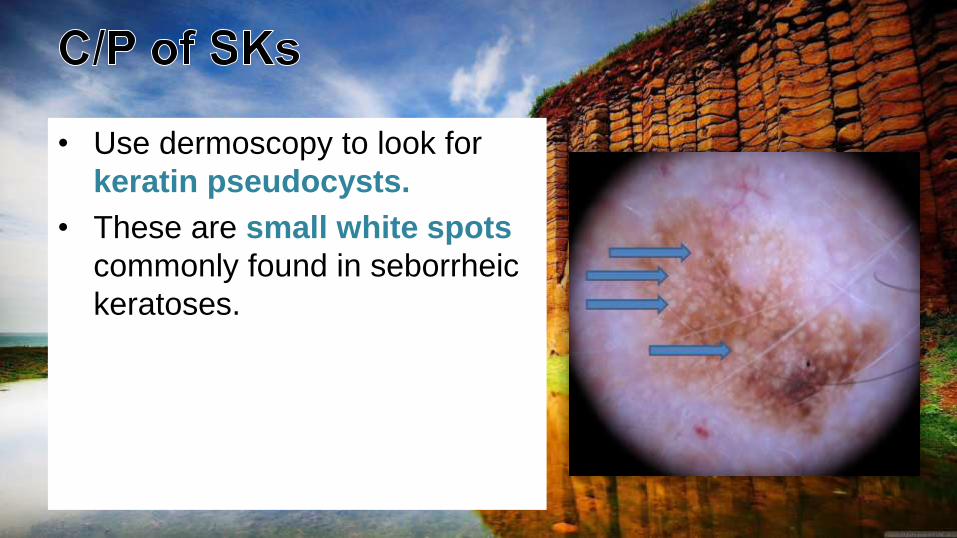
• Use dermoscopy to look for
keratin pseudocysts.
• These are small white spots
commonly found in seborrheic
keratoses.
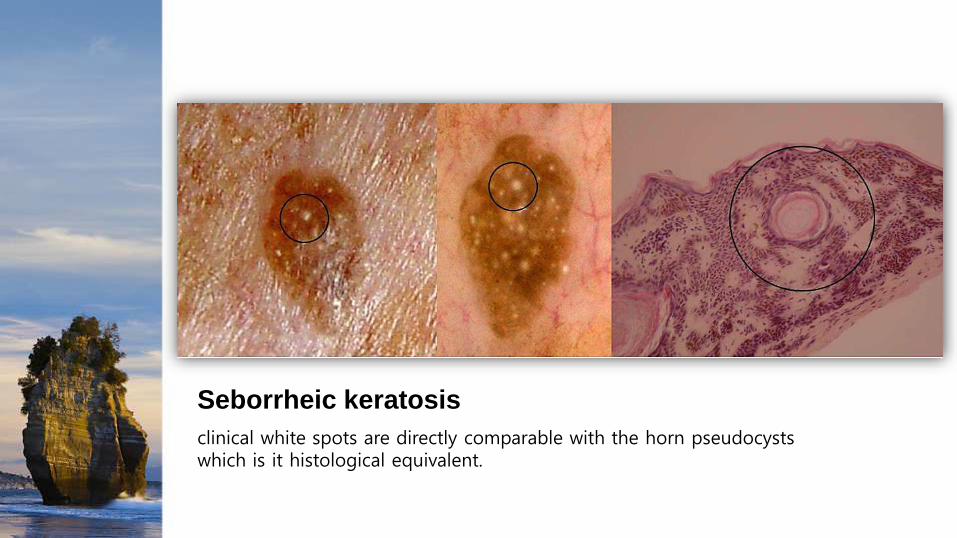
Seborrheic keratosis
clinical white spots are directly comparable with the horn pseudocysts which is it histological equivalent.

Dermoscopy of SKs showing horny pseudocysts
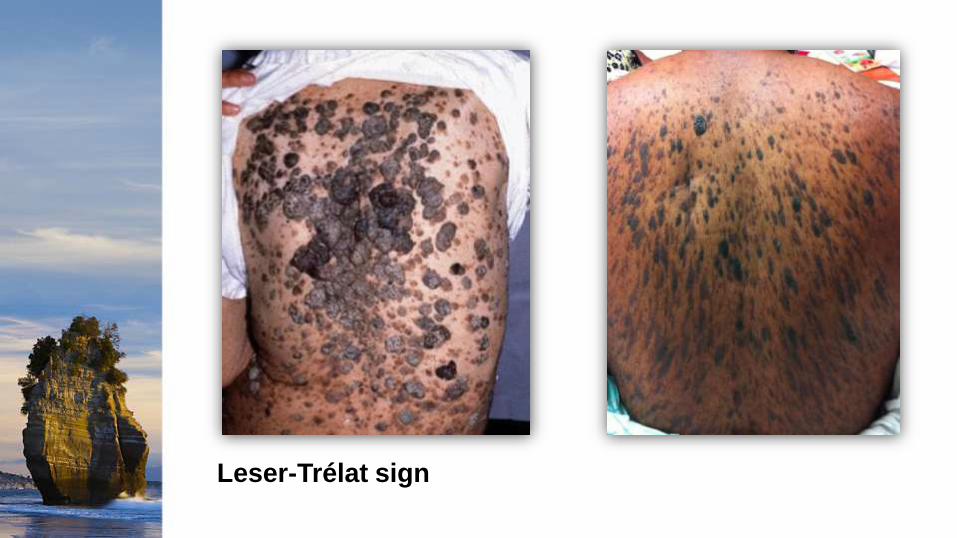
Leser-Trélat sign
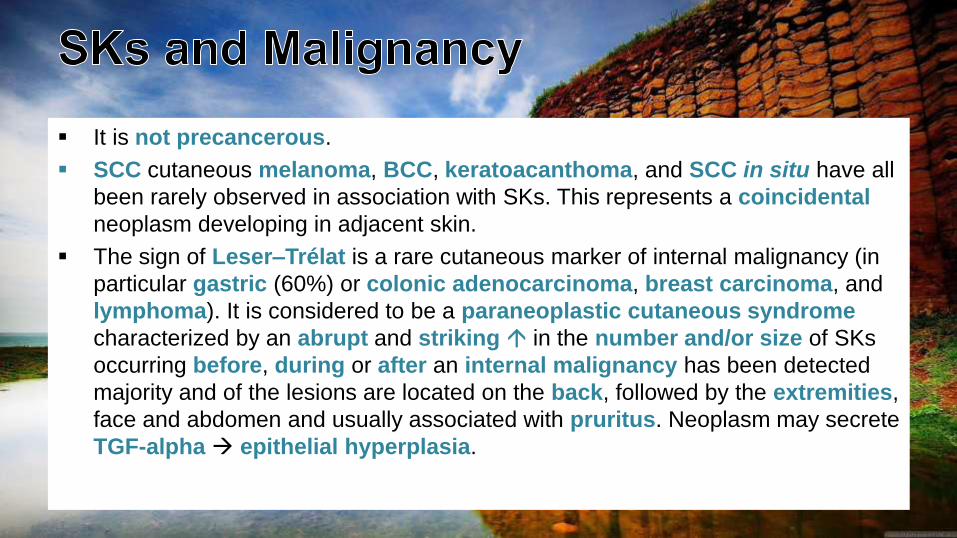
It is not precancerous.
SCC cutaneous melanoma, BCC, keratoacanthoma, and SCC in situ have all
been rarely observed in association with SKs. This represents a coincidental
neoplasm developing in adjacent skin.
The sign of Leser–Trélat is a rare cutaneous marker of internal malignancy (in
particular gastric (60%) or colonic adenocarcinoma, breast carcinoma, and
lymphoma). It is considered to be a paraneoplastic cutaneous syndrome
characterized by an abrupt and striking in the number and/or size of SKs
occurring before, during or after an internal malignancy has been detected
majority and of the lesions are located on the back, followed by the extremities,
face and abdomen and usually associated with pruritus. Neoplasm may secrete
TGF-alpha epithelial hyperplasia.

I. IRRITATED SEBORRHOEIC KERATOSIS
II. DERMATOSIS PAPULOSA NIGRA
III. STUCCO KERATOSES
IV. INVERTED FOLLICULAR KERATOSES
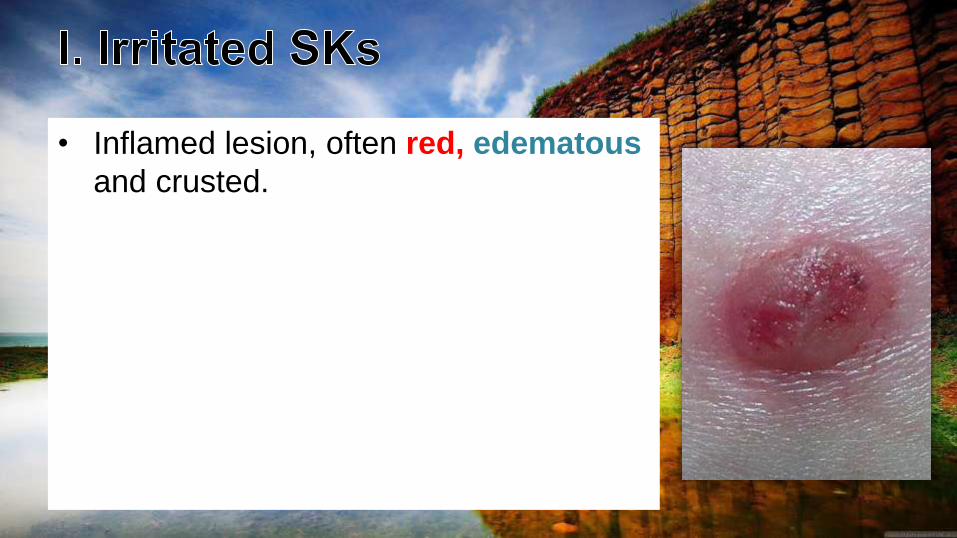
• Inflamed lesion, often red, edematous
and crusted.

Irritated SKs
erythematous, edematous and crusty
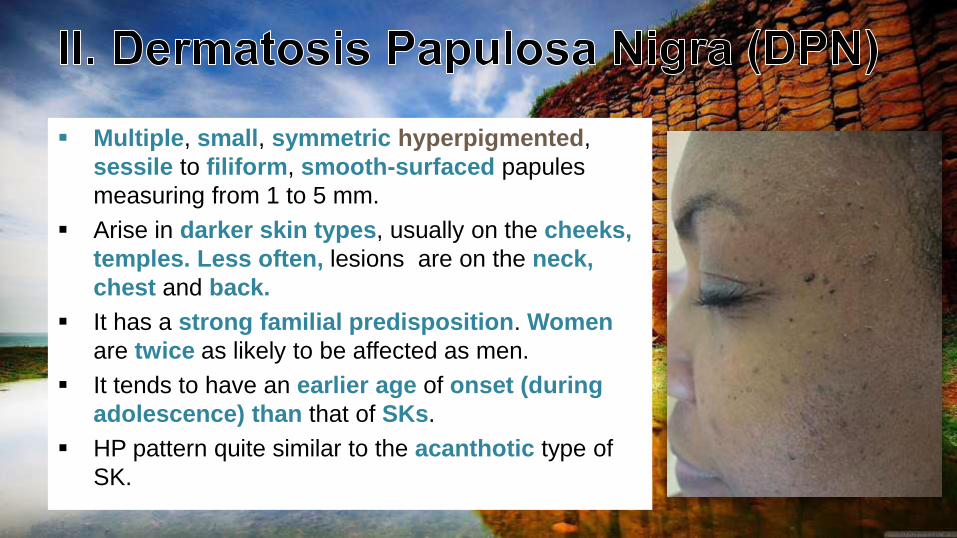
Multiple, small, symmetric hyperpigmented,
sessile to filiform, smooth-surfaced papules
measuring from 1 to 5 mm.
Arise in darker skin types, usually on the cheeks,
temples. Less often, lesions are on the neck,
chest and back.
It has a strong familial predisposition. Women
are twice as likely to be affected as men.
It tends to have an earlier age of onset (during
adolescence) than that of SKs.
HP pattern quite similar to the acanthotic type of
SK.
DPN
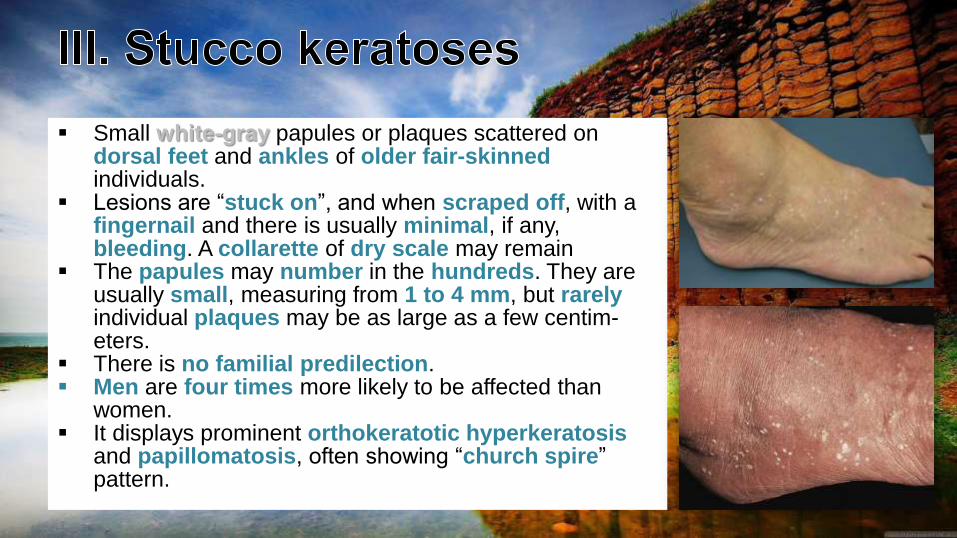
Small white-gray papules or plaques scattered on dorsal feet and ankles of older fair-skinnedindividuals.
Lesions are “stuck on”, and when scraped off, with a fingernail and there is usually minimal, if any, bleeding. A collarette of dry scale may remain
The papules may number in the hundreds. They are usually small, measuring from 1 to 4 mm, but rarelyindividual plaques may be as large as a few centim-eters.
There is no familial predilection. Men are four times more likely to be affected than
women. It displays prominent orthokeratotic hyperkeratosis
and papillomatosis, often showing “church spire” pattern.
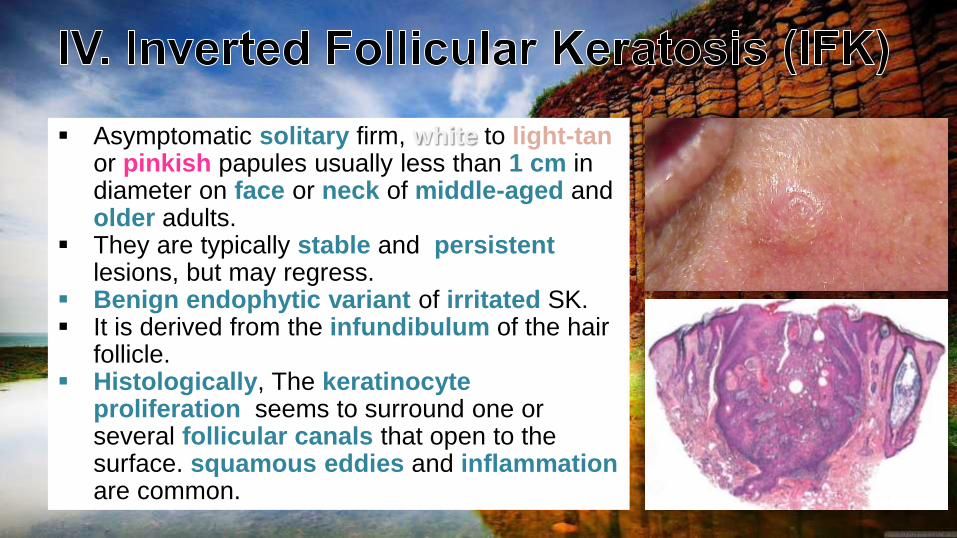
Asymptomatic solitary firm, white to light-tanor pinkish papules usually less than 1 cm in diameter on face or neck of middle-aged and older adults.
They are typically stable and persistentlesions, but may regress.
Benign endophytic variant of irritated SK. It is derived from the infundibulum of the hair
follicle. Histologically, The keratinocyte
proliferation seems to surround one or several follicular canals that open to the surface. squamous eddies and inflammationare common.
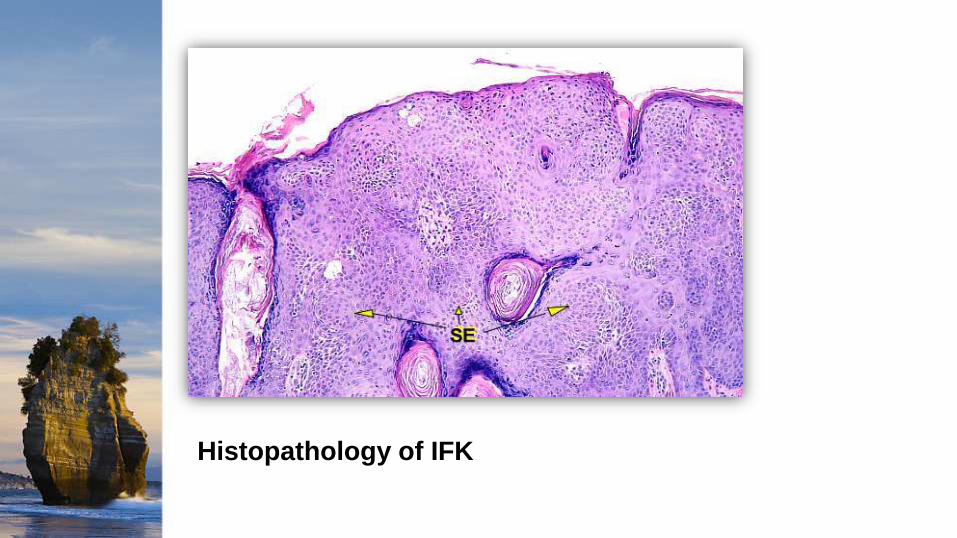
Histopathology of IFK
There are at least six histologic types of SK but different histologic features are often present in the same lesion:
1. Acanthotic: the most common.
2. Hyperkeratotic: more prominent hyperkeratosis and papillomatosis.
3. Reticulated: delicate strands of epithelium that extend from the epidermis in an interlacing pattern.
4. Irritated: perivascular, diffuse or lichenoid lymphoid infiltrate. Squamous eddies are common findings.
5. Clonal: well defined nests of loosely packed uniform cells in the epithelium.
6. Melanoacanthoma: shows dendritic melanocytes packed with melanin which is absent in keratinocytes.
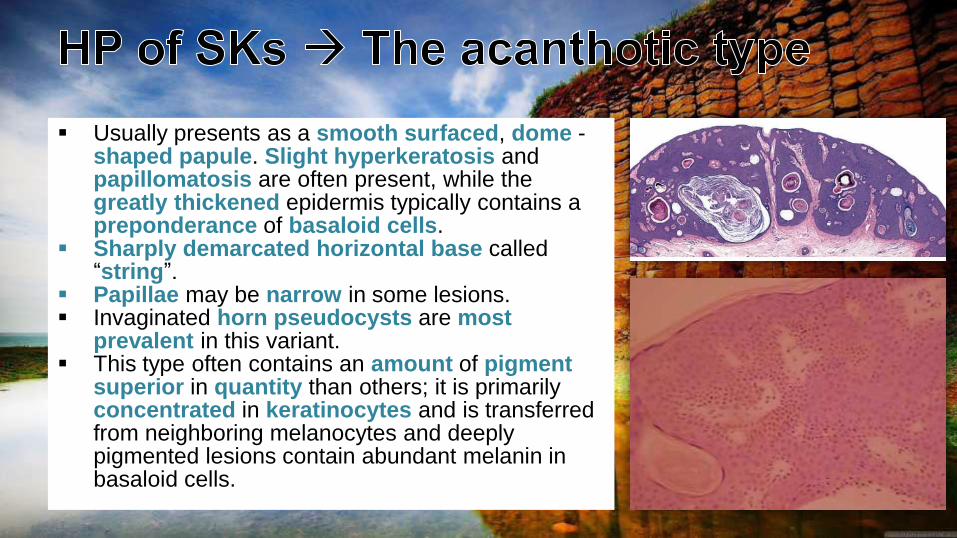
Usually presents as a smooth surfaced, dome -shaped papule. Slight hyperkeratosis and papillomatosis are often present, while the greatly thickened epidermis typically contains a preponderance of basaloid cells.
Sharply demarcated horizontal base called “string”.
Papillae may be narrow in some lesions. Invaginated horn pseudocysts are most
prevalent in this variant. This type often contains an amount of pigment
superior in quantity than others; it is primarily concentrated in keratinocytes and is transferred from neighboring melanocytes and deeply pigmented lesions contain abundant melanin in basaloid cells.
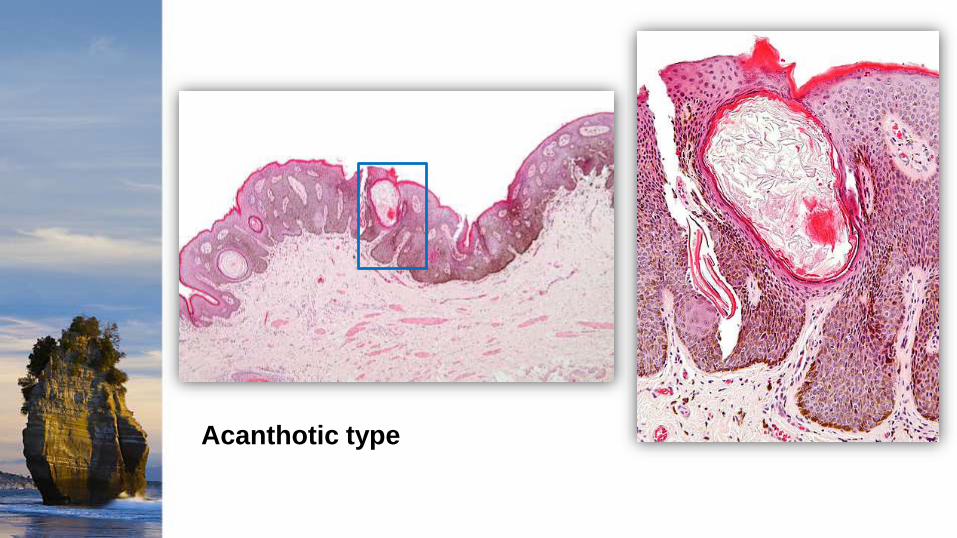
Acanthotic type
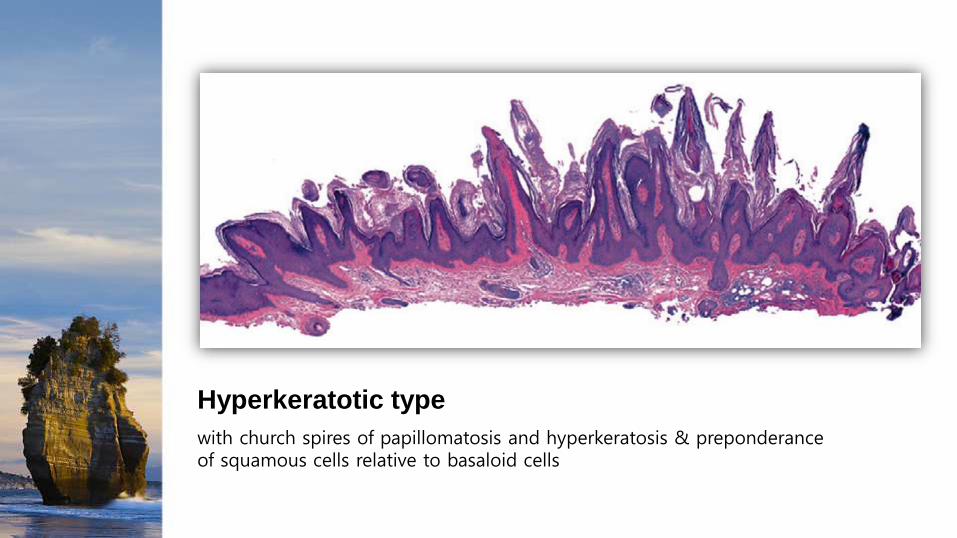
Hyperkeratotic type
with church spires of papillomatosis and hyperkeratosis & preponderance of squamous cells relative to basaloid cells
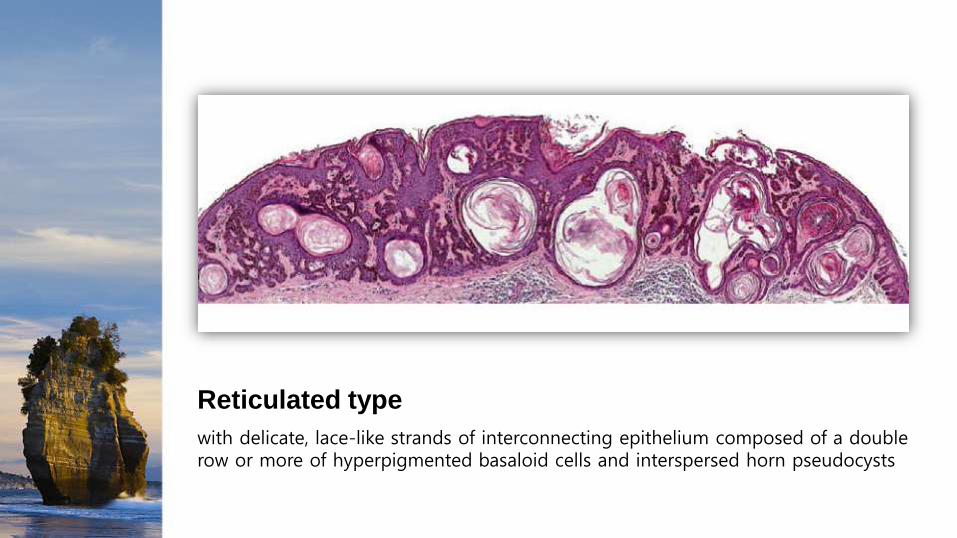
Reticulated type
with delicate, lace-like strands of interconnecting epithelium composed of a double row or more of hyperpigmented basaloid cells and interspersed horn pseudocysts

Reticulated type
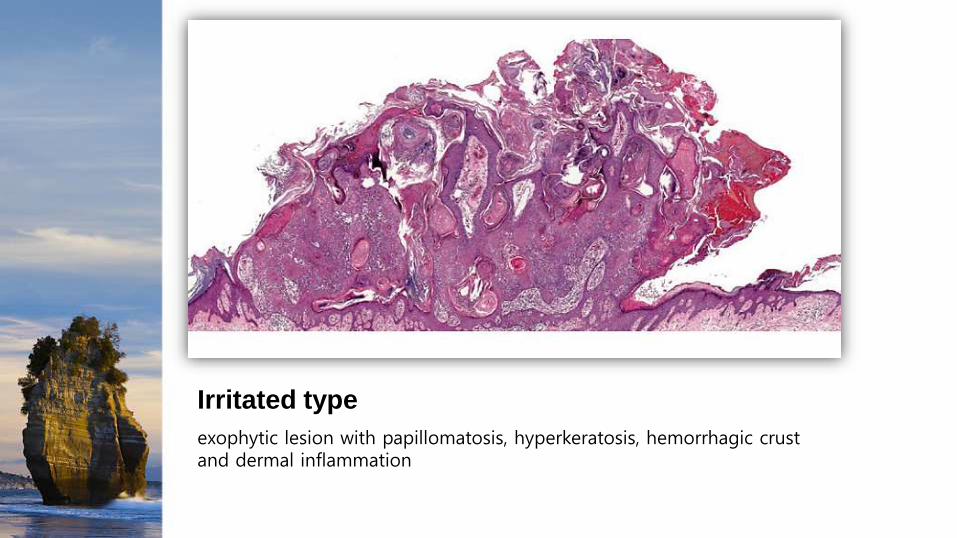
Irritated type
exophytic lesion with papillomatosis, hyperkeratosis, hemorrhagic crust and dermal inflammation
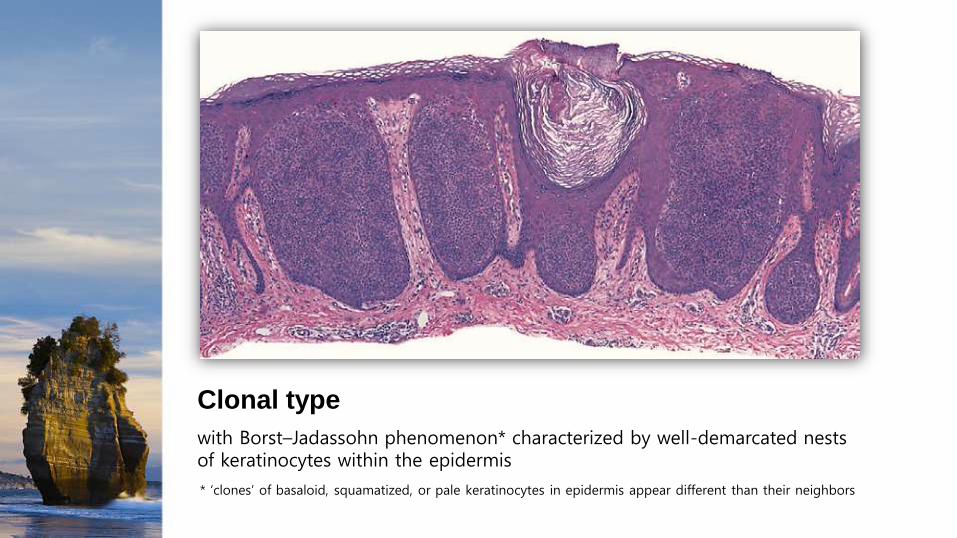
Clonal type
with Borst–Jadassohn phenomenon* characterized by well-demarcated nests of keratinocytes within the epidermis
* ‘clones’ of basaloid, squamatized, or pale keratinocytes in epidermis appear different than their neighbors
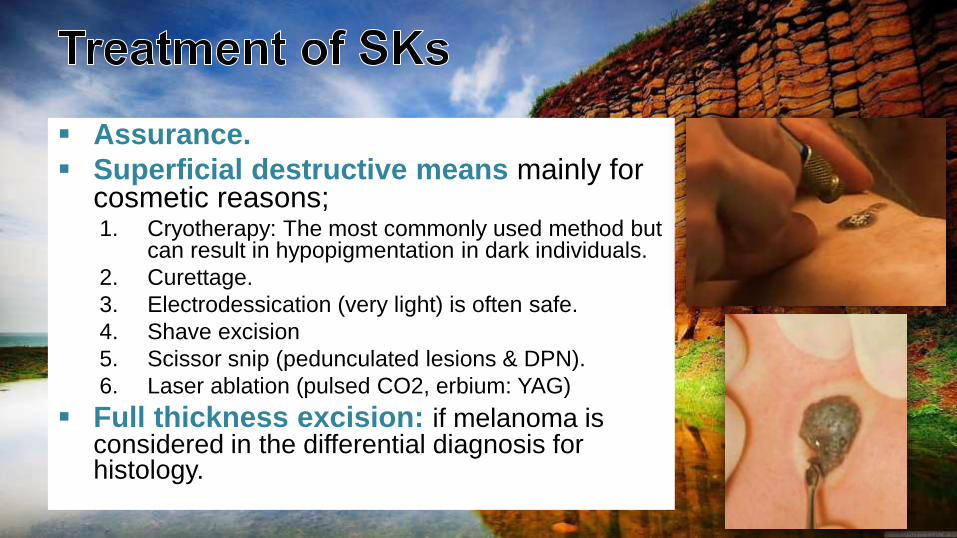
Assurance.
Superficial destructive means mainly for cosmetic reasons;1. Cryotherapy: The most commonly used method but
can result in hypopigmentation in dark individuals.
2. Curettage.
3. Electrodessication (very light) is often safe.
4. Shave excision
5. Scissor snip (pedunculated lesions & DPN).
6. Laser ablation (pulsed CO2, erbium: YAG)
Full thickness excision: if melanoma is considered in the differential diagnosis for histology.

They are due to an hamartoma of the epidermis present at birth (50%) or develop during childhood (mostly in the first year of life) and persist indefinitely.
The abnormality arises from a defect in the ectoderm (outer layer of the embryo that gives rise to epidermis and neural tissue).
Most commonly, hyperpigmented papillomatous papulesand plaques appear in a linear array along Blaschko’s lines.
The incidence of epidermal nevus is estimated to be 1 in 1000 infants.
Sporadic rarely inherited.
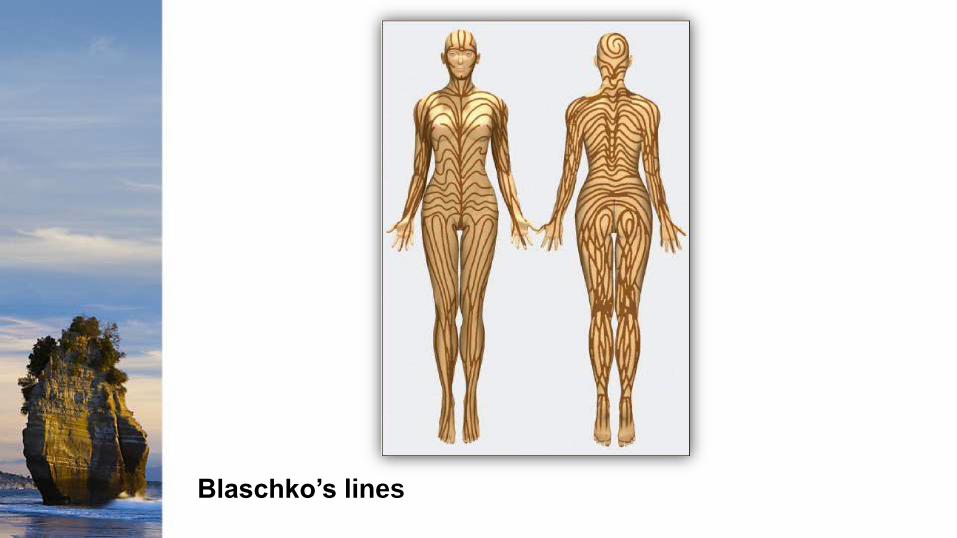
Blaschko’s lines

Originate from pluripotent cells in the basal layerof the embryonic epidermis.
Mosaicism (skin cells that have the active abnormal gene spread out to form the epidermal naevus, whereas the remaining skin cells form the other areas of apparently normal skin) for activating mutations in the gene that encodesfibroblast growth factor receptor 3 (FGFR3) was demonstrated in “common” epidermal nevi.
While these lesions are classically referred to as “epidermal” nevi, the hamartomatous processalso involves at least some portion of the dermis, especially the papillary dermis.
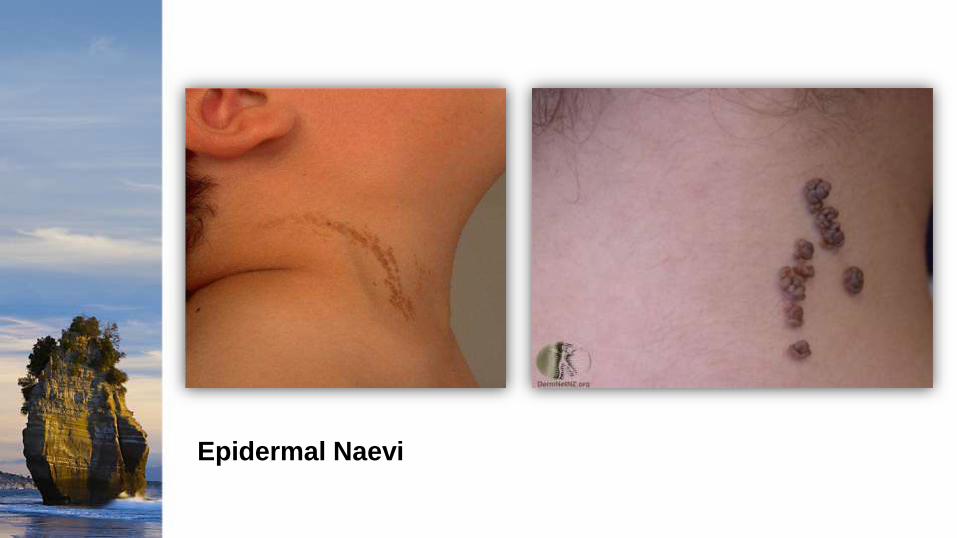
Epidermal Naevi
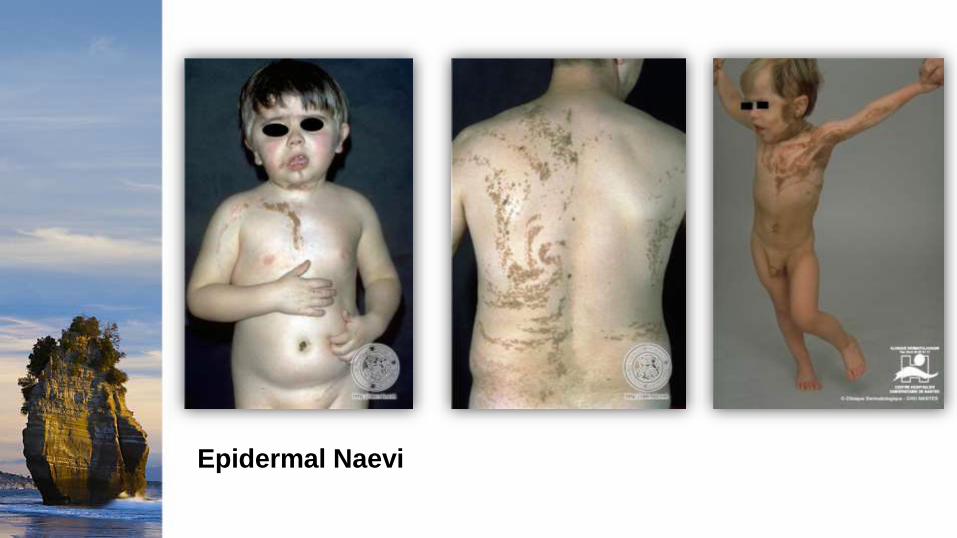
Epidermal Naevi
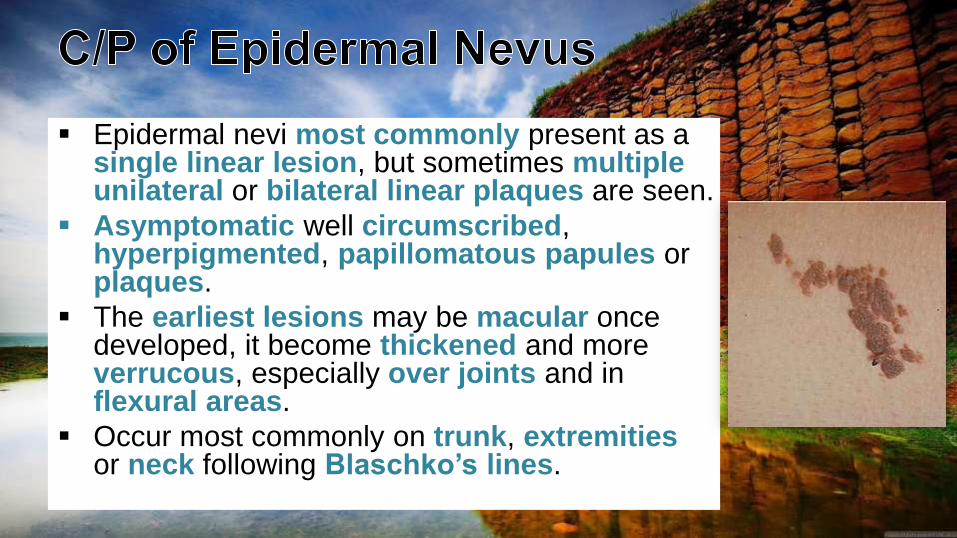
Epidermal nevi most commonly present as a single linear lesion, but sometimes multipleunilateral or bilateral linear plaques are seen.
Asymptomatic well circumscribed, hyperpigmented, papillomatous papules or plaques.
The earliest lesions may be macular once developed, it become thickened and more verrucous, especially over joints and in flexural areas.
Occur most commonly on trunk, extremitiesor neck following Blaschko’s lines.
TYPES OF EPIDERMAL NAEVI:
1. Localized Linear Epidermal Naevus (Nevus
Verrucosus)
2. Naevus Unius Lateris
3. Systematised Epidermal Naevus (Ichthyosis Hystrix)
4. ILVEN
5. Epidermolytic Epidermal Naevus
6. Acantholytic Epidermal Naevus
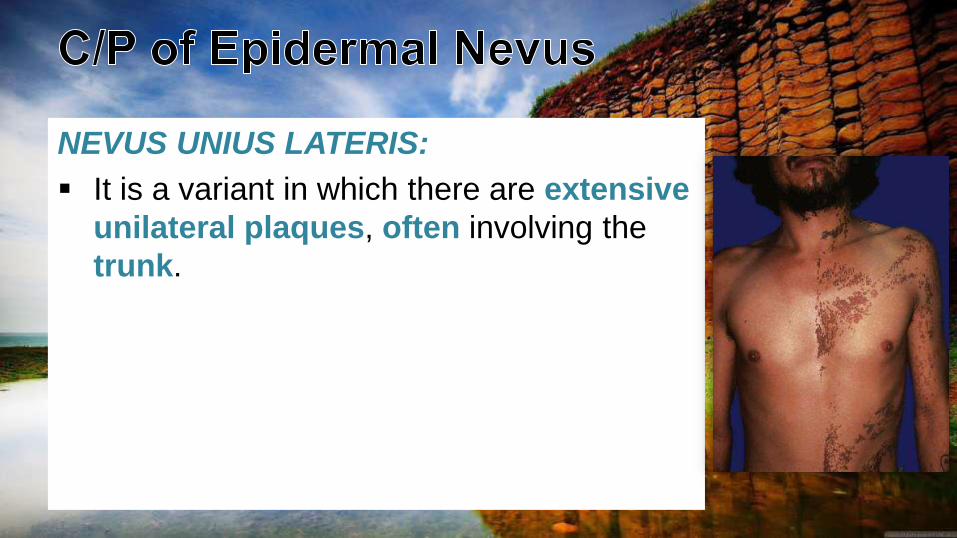
NEVUS UNIUS LATERIS:
It is a variant in which there are extensive
unilateral plaques, often involving the
trunk.
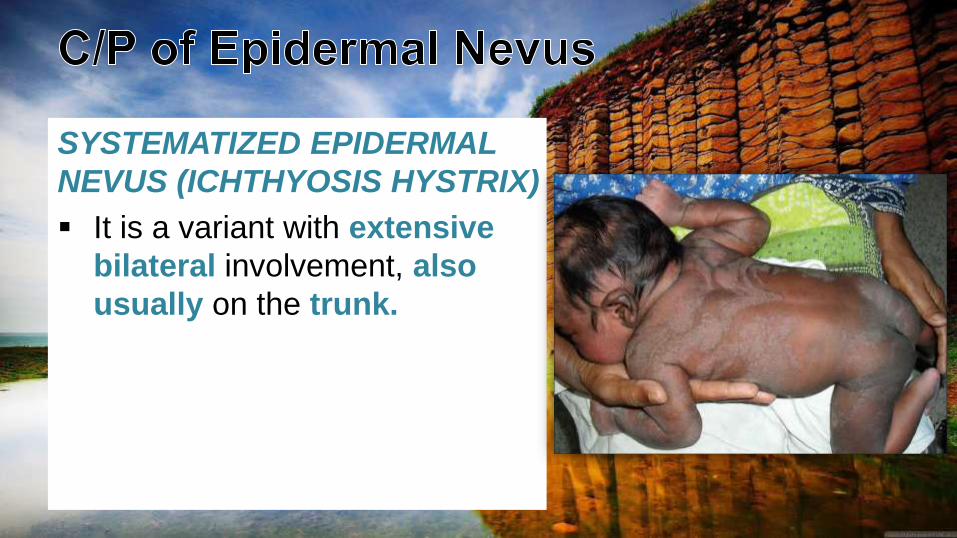
SYSTEMATIZED EPIDERMAL
NEVUS (ICHTHYOSIS HYSTRIX)
It is a variant with extensive
bilateral involvement, also
usually on the trunk.
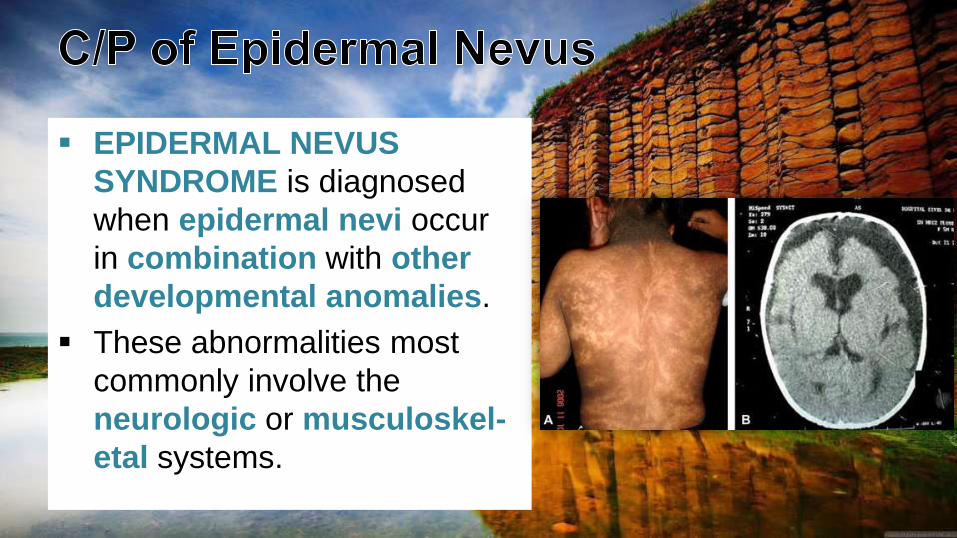
EPIDERMAL NEVUS
SYNDROME is diagnosed
when epidermal nevi occur
in combination with other
developmental anomalies.
These abnormalities most
commonly involve the
neurologic or musculoskel-
etal systems.
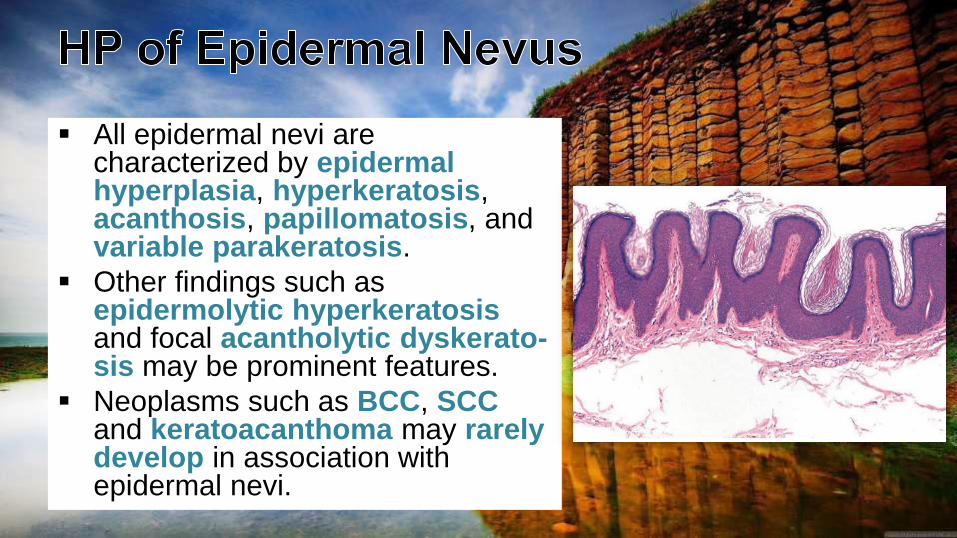
All epidermal nevi are characterized by epidermalhyperplasia, hyperkeratosis, acanthosis, papillomatosis, and variable parakeratosis.
Other findings such as epidermolytic hyperkeratosisand focal acantholytic dyskerato-sis may be prominent features.
Neoplasms such as BCC, SCCand keratoacanthoma may rarelydevelop in association with epidermal nevi.
Infants and children with epidermal nevi, particularly multiple or extensive lesions, require a thorough evaluation for systemic abnormalities.
MEDICAL:1. Topical therapies such as corticosteroids, retinoic acid, tars, anthralin, 5-fluorouracil
and podophyllin have all been used, but they are of limited benefit.
2. Oral therapy with systemic retinoids for long term has been reported to be effective at decreasing the thickness of systematized epidermal nevi, although it does not result in resolution.
SURGICAL: 1. Superficial destructive means (e.g. by cryotherapy, shave excision or curettage)
recurrence is common as only the epidermis is removed. Laser ablation may also be undertaken, but, to be effective, it must induce scarring and fibrosis of at least the papillary dermis. Therefore, this treatment is often not cosmetically acceptable to patients and test sites are recommended.
2. Full thickness surgical excision is curative but can be complicated by hypertrophic scars or keloid formation.

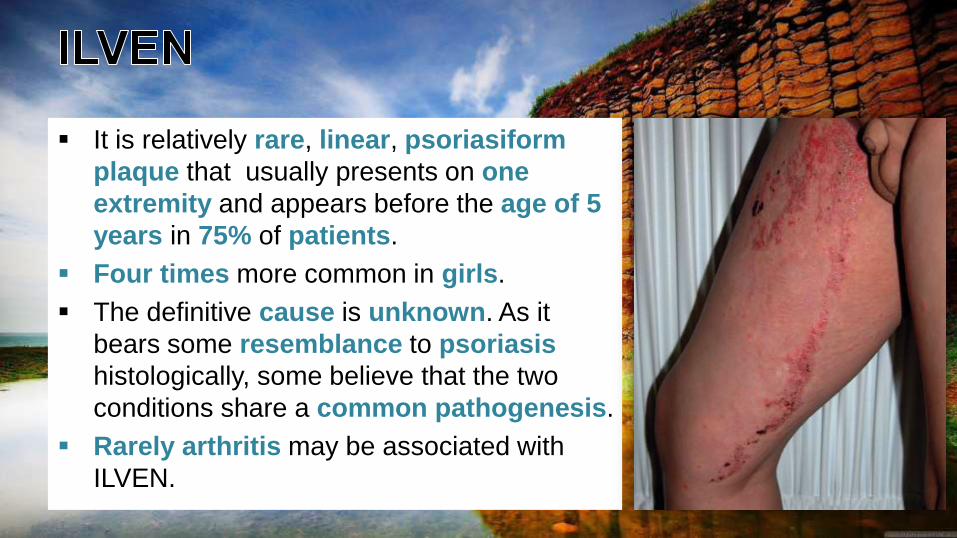
It is relatively rare, linear, psoriasiform
plaque that usually presents on one
extremity and appears before the age of 5
years in 75% of patients.
Four times more common in girls.
The definitive cause is unknown. As it
bears some resemblance to psoriasis
histologically, some believe that the two
conditions share a common pathogenesis.
Rarely arthritis may be associated with
ILVEN.

ILVEN
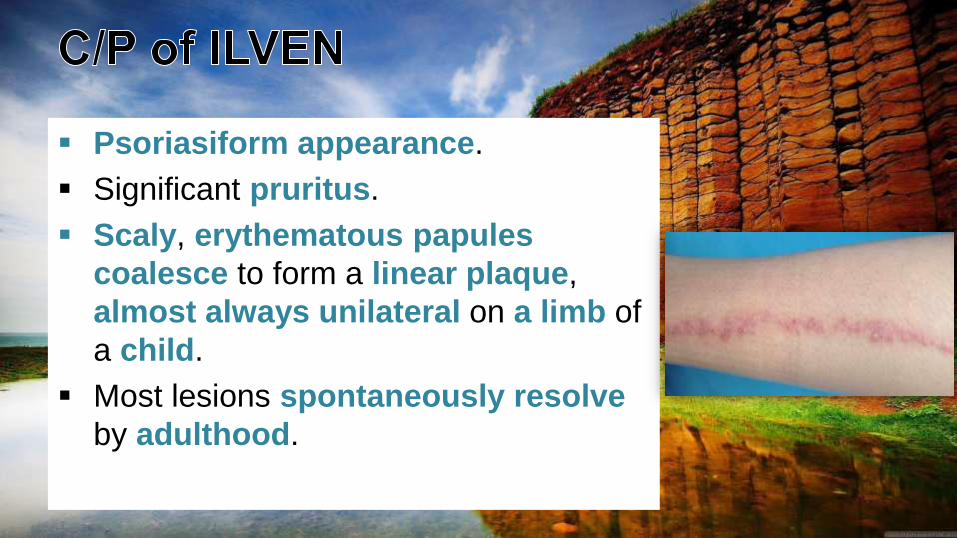
Psoriasiform appearance.
Significant pruritus.
Scaly, erythematous papules
coalesce to form a linear plaque,
almost always unilateral on a limb of
a child.
Most lesions spontaneously resolve
by adulthood.
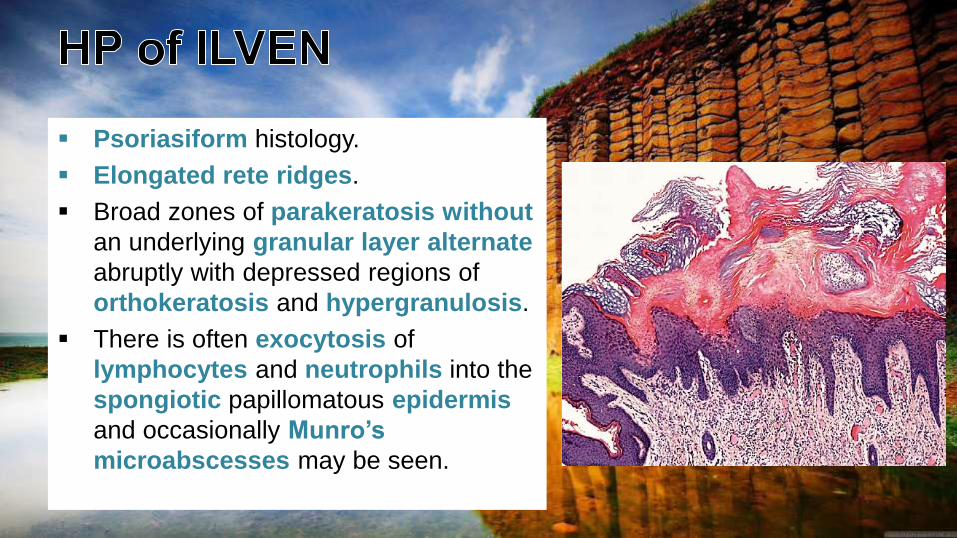
Psoriasiform histology.
Elongated rete ridges.
Broad zones of parakeratosis without
an underlying granular layer alternate
abruptly with depressed regions of
orthokeratosis and hypergranulosis.
There is often exocytosis of
lymphocytes and neutrophils into the
spongiotic papillomatous epidermis
and occasionally Munro’s
microabscesses may be seen.

ILVEN is difficult to treat. Treatments that are successful in psoriasis
are only partially effective for ILVEN.
MEDICAL:
1. Combination therapy with topical tretinoin and 5-fluorouracil creams
has been employed with beneficial results, but long-term success can
only be achieved with maintenance therapy.
2. Calcipotriol may be partially effective.
SURGICAL:
1. Pulsed dye laser has been used successfully in some cases.
2. Surgical excision is effective but results in scarring.

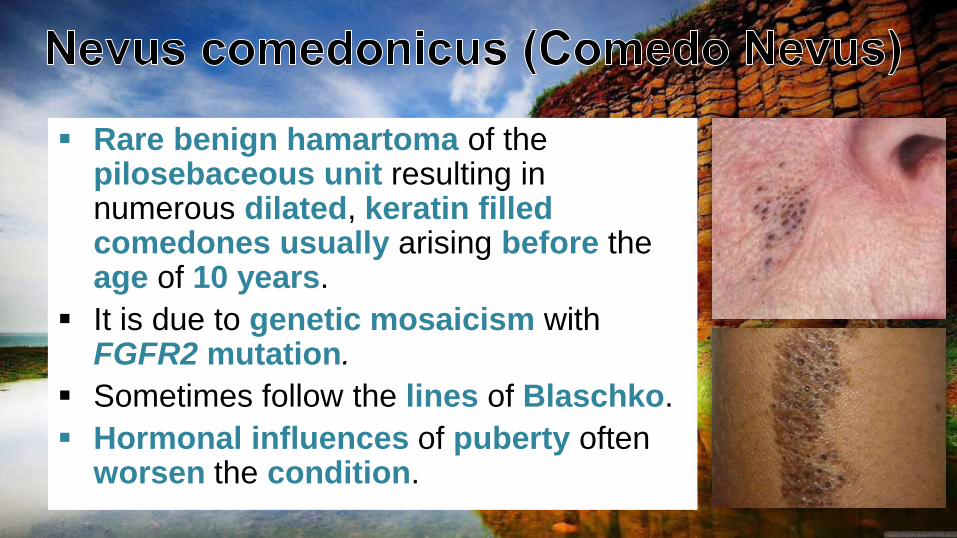
Rare benign hamartoma of the pilosebaceous unit resulting in numerous dilated, keratin filledcomedones usually arising before the age of 10 years.
It is due to genetic mosaicism withFGFR2 mutation.
Sometimes follow the lines of Blaschko.
Hormonal influences of puberty often worsen the condition.

Nevus Comedonicus

Usually a single circumscribed
area or linear streak composed of
clusters of dilated follicular ostia
with central keratinous plugs
contain firm, darkly pigmented,
cornified material.
Their size is variable and they can
range from a few centimeters in
diameter to extensive lesions
affecting half of the body.
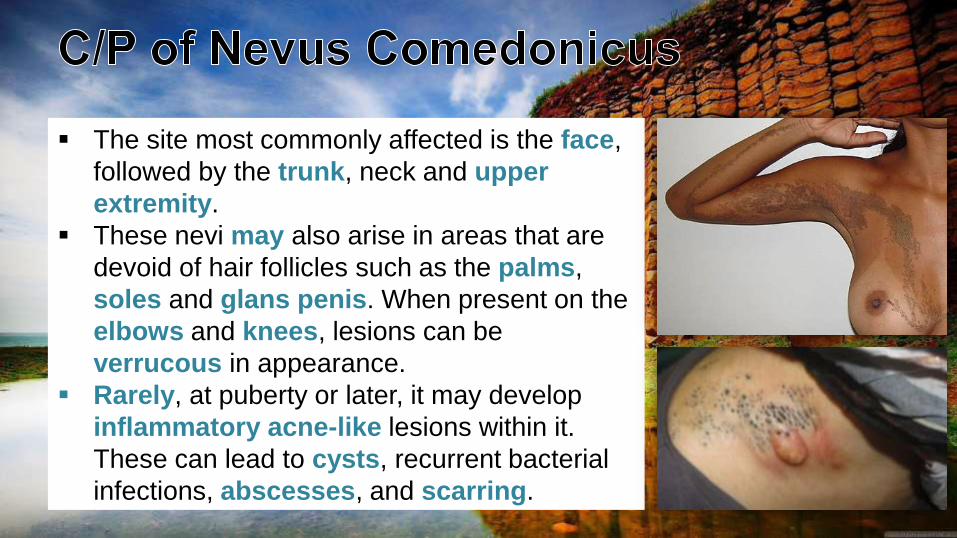
The site most commonly affected is the face,
followed by the trunk, neck and upper
extremity.
These nevi may also arise in areas that are
devoid of hair follicles such as the palms,
soles and glans penis. When present on the
elbows and knees, lesions can be
verrucous in appearance.
Rarely, at puberty or later, it may develop
inflammatory acne-like lesions within it.
These can lead to cysts, recurrent bacterial
infections, abscesses, and scarring.
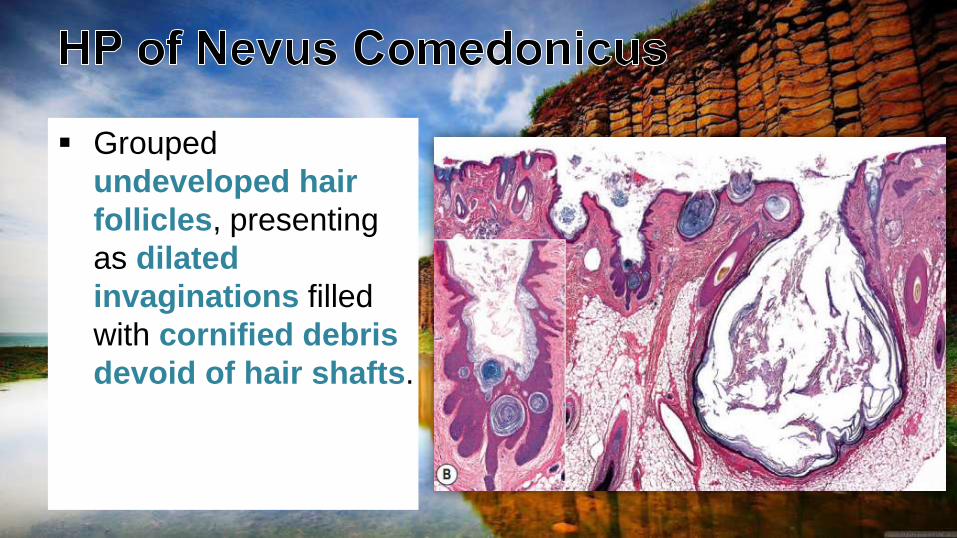
Grouped
undeveloped hair
follicles, presenting
as dilated
invaginations filled
with cornified debris
devoid of hair shafts.
MEDICAL:
1. Keratolytic agents e.g. salicylic acid, tretinoin and ammonium lactate
may be helpful, but they are not curative.
2. Isotretinoin is not usually recommended owing to the long term
treatment required, but it may be beneficial in preventing cyst formation.
3. Antibiotics may be necessary to treat secondary infections.
SURGICAL:
1. Manual comedo extraction, laser, dermabrasion may be done but it
is not curative.
2. Excision of localized lesions, although it is often difficult to excise
larger lesions.

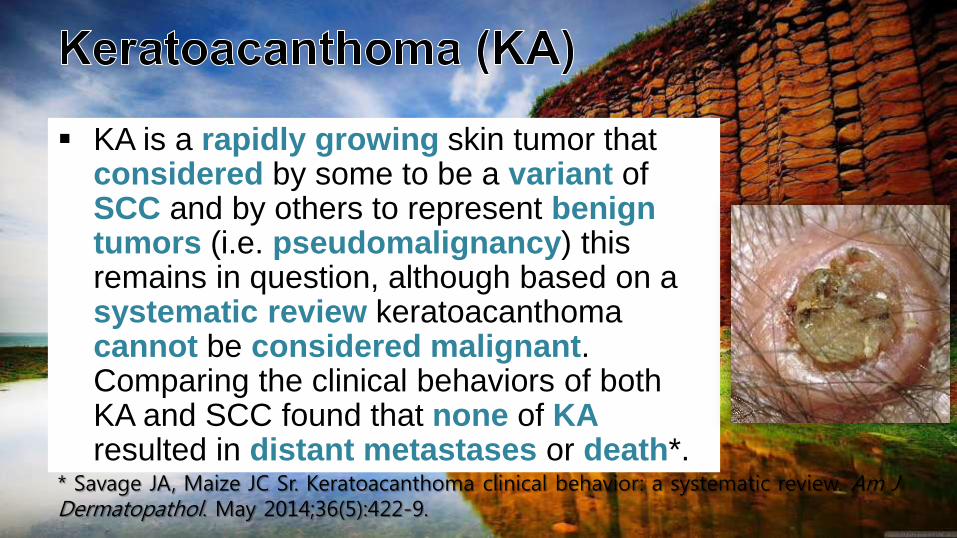
KA is a rapidly growing skin tumor that considered by some to be a variant of SCC and by others to represent benigntumors (i.e. pseudomalignancy) this remains in question, although based on a systematic review keratoacanthoma cannot be considered malignant. Comparing the clinical behaviors of both KA and SCC found that none of KAresulted in distant metastases or death*.
* Savage JA, Maize JC Sr. Keratoacanthoma clinical behavior: a systematic review. Am J Dermatopathol. May 2014;36(5):422-9.
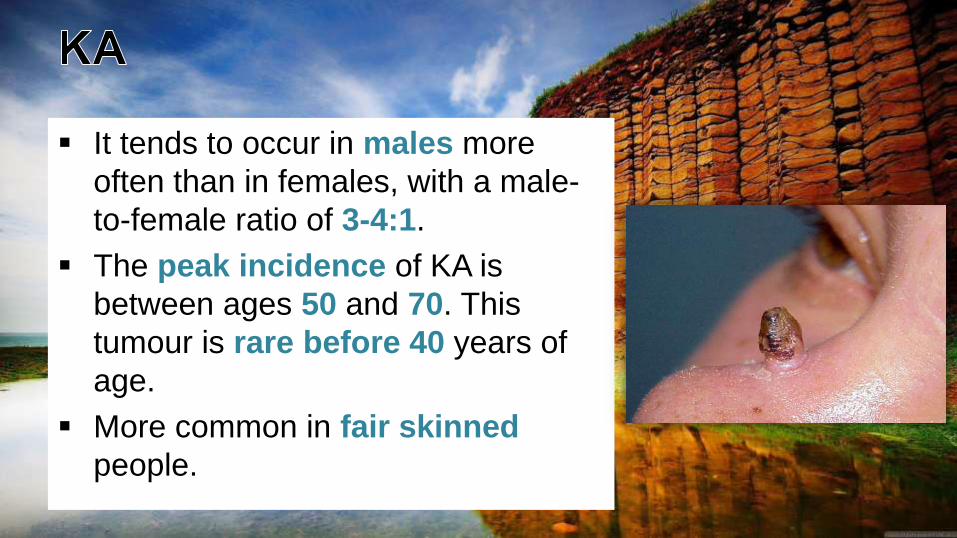
It tends to occur in males more
often than in females, with a male-
to-female ratio of 3-4:1.
The peak incidence of KA is
between ages 50 and 70. This
tumour is rare before 40 years of
age.
More common in fair skinned
people.
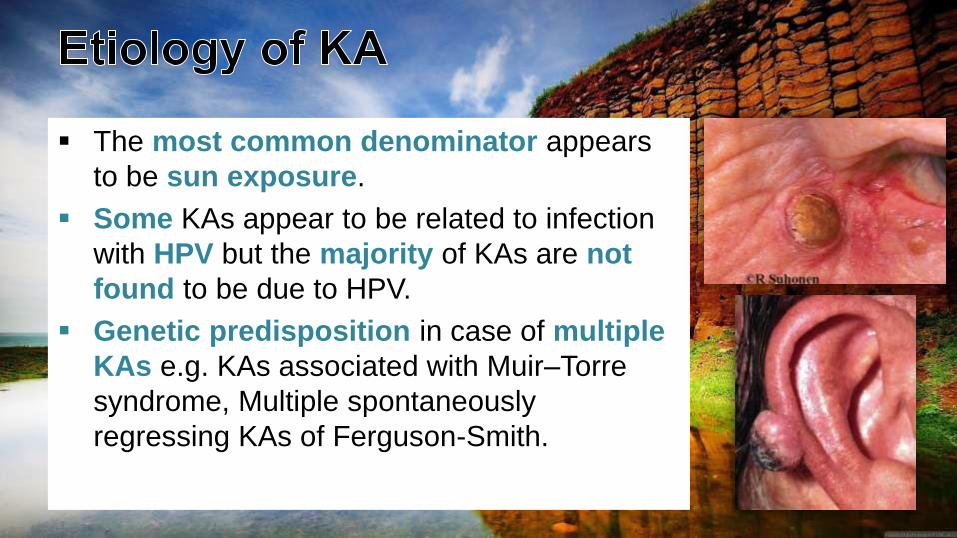
The most common denominator appears
to be sun exposure.
Some KAs appear to be related to infection
with HPV but the majority of KAs are not
found to be due to HPV.
Genetic predisposition in case of multiple
KAs e.g. KAs associated with Muir–Torre
syndrome, Multiple spontaneously
regressing KAs of Ferguson-Smith.

KA
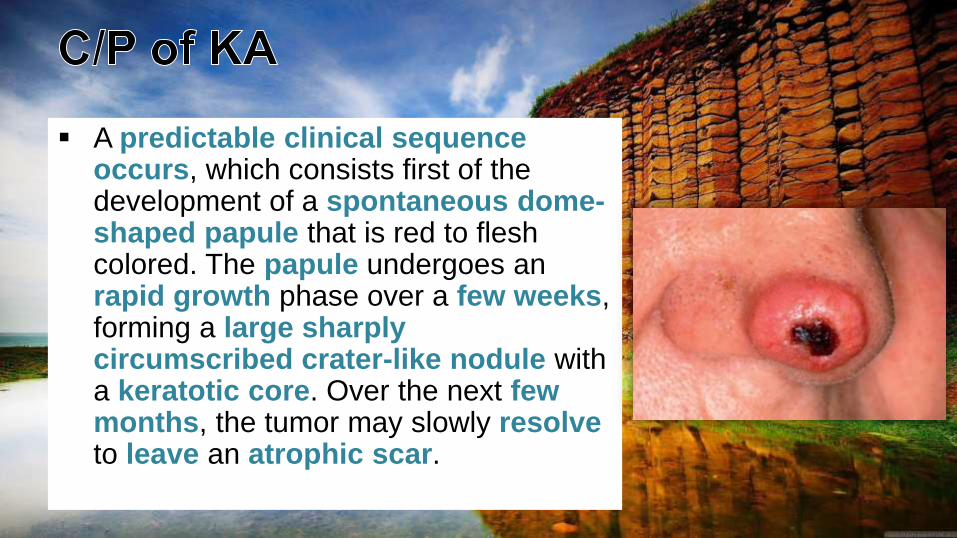
A predictable clinical sequenceoccurs, which consists first of the development of a spontaneous dome-shaped papule that is red to flesh colored. The papule undergoes an rapid growth phase over a few weeks, forming a large sharplycircumscribed crater-like nodule with a keratotic core. Over the next fewmonths, the tumor may slowly resolveto leave an atrophic scar.
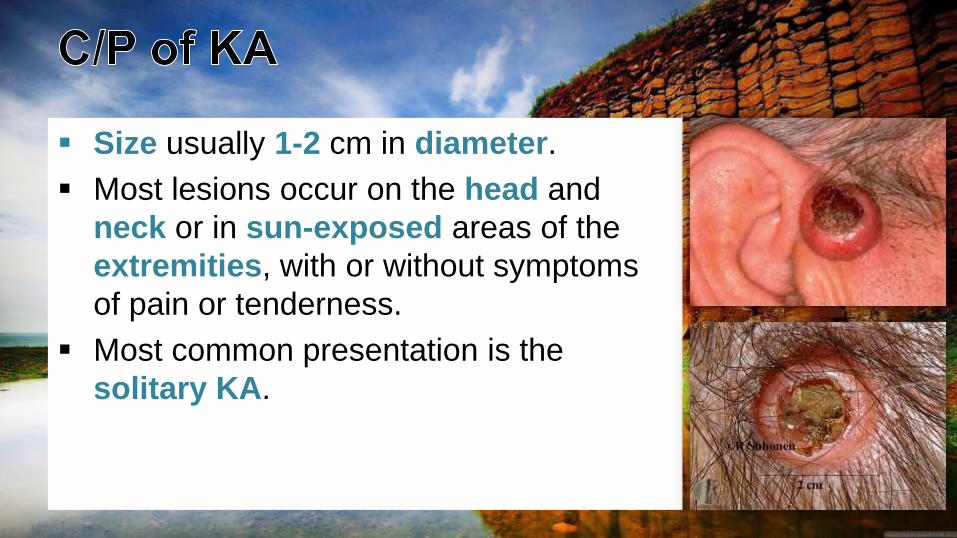
Size usually 1-2 cm in diameter.
Most lesions occur on the head and
neck or in sun-exposed areas of the
extremities, with or without symptoms
of pain or tenderness.
Most common presentation is the
solitary KA.
Three growth phases are described:
1. Proliferative phase: a solitary papule appears suddenly and then rapidly grows to its maximum size over 2 to 4 weeks.
2. Mature phase: the lesion is stable in size and appearance for weeks to months; it may appear crateriform if the core has been partially removed.
3. Resolving phase: the base becomes indurated, the central core is expelled, and the base resorbs, leaving a atrophic scar. This phase may last several months.

Keratoacanthoma centrifugum marginatum
Progressive peripheral expansion and central involution with residual atrophy
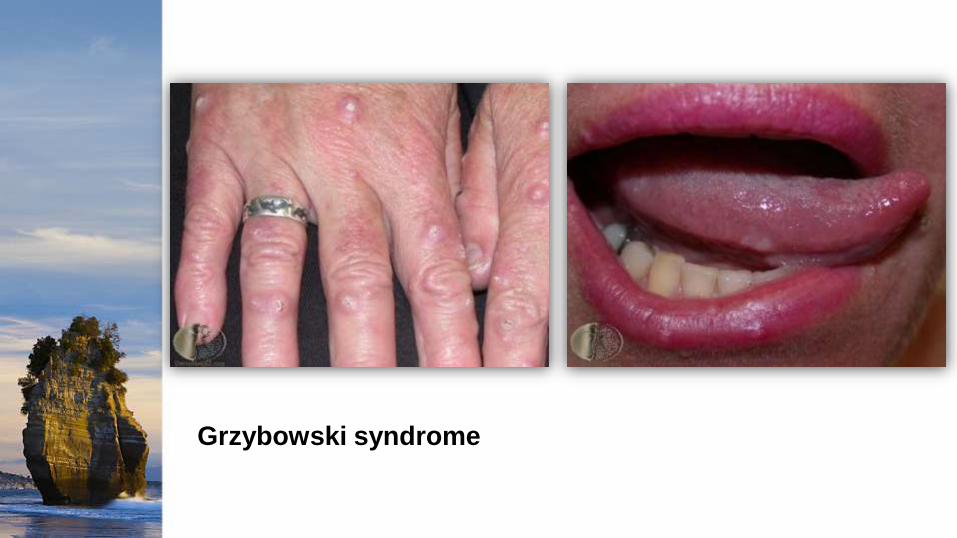
Grzybowski syndrome

Multiple spontaneously regressing KAs of Ferguson-Smith
The patient had approximately 40 firm, 1- to 2-cm, dome-shaped, red-to-flesh colored, hyperkeratotic nodules on the lateral upper arm and extensor forearms.
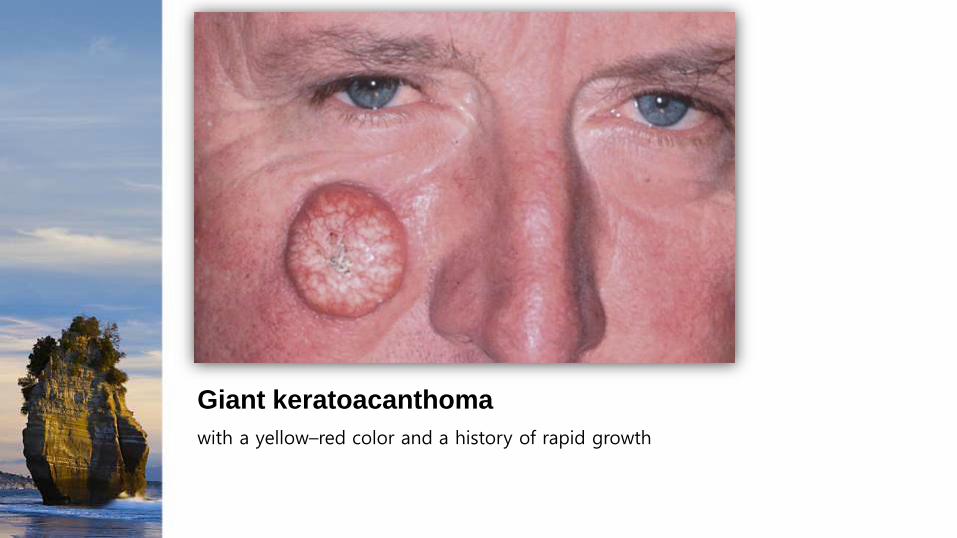
Giant keratoacanthoma
with a yellow–red color and a history of rapid growth
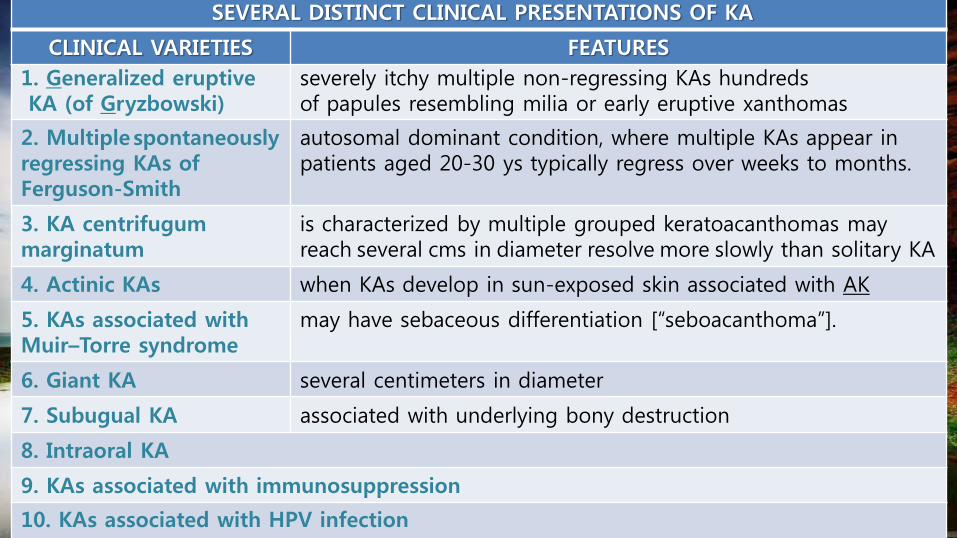
SEVERAL DISTINCT CLINICAL PRESENTATIONS OF KA
CLINICAL VARIETIES FEATURES
1. Generalized eruptiveKA (of Gryzbowski)
severely itchy multiple non-regressing KAs hundreds of papules resembling milia or early eruptive xanthomas
2. Multiplespontaneously regressing KAs of Ferguson-Smith
autosomal dominant condition, where multiple KAs appear in patients aged 20-30 ys typically regress over weeks to months.
3. KA centrifugummarginatum
is characterized by multiple grouped keratoacanthomas may reach several cms in diameter resolve more slowly than solitary KA
4. Actinic KAs when KAs develop in sun-exposed skin associated with AK
5. KAs associated with Muir–Torre syndrome
may have sebaceous differentiation [“seboacanthoma”].
6. Giant KA several centimeters in diameter
7. Subugual KA associated with underlying bony destruction
8. Intraoral KA
9. KAs associated with immunosuppression
10. KAs associated with HPV infection
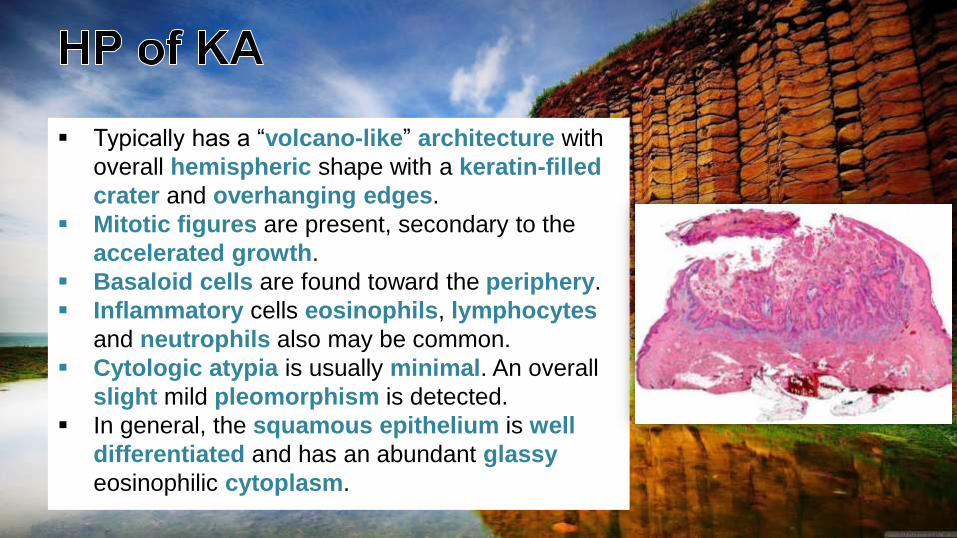
Typically has a “volcano-like” architecture with
overall hemispheric shape with a keratin-filled
crater and overhanging edges.
Mitotic figures are present, secondary to the
accelerated growth.
Basaloid cells are found toward the periphery.
Inflammatory cells eosinophils, lymphocytes
and neutrophils also may be common.
Cytologic atypia is usually minimal. An overall
slight mild pleomorphism is detected.
In general, the squamous epithelium is well
differentiated and has an abundant glassy
eosinophilic cytoplasm.
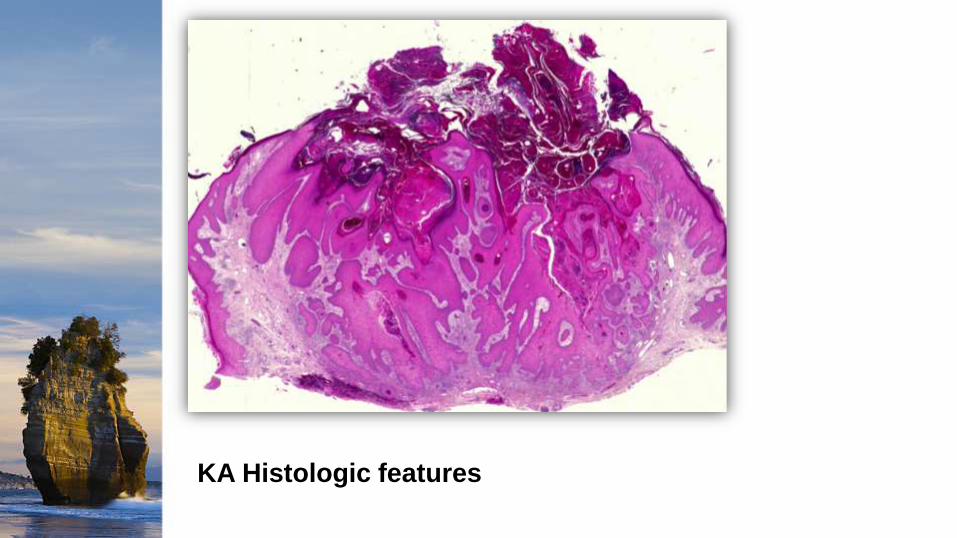
KA Histologic features
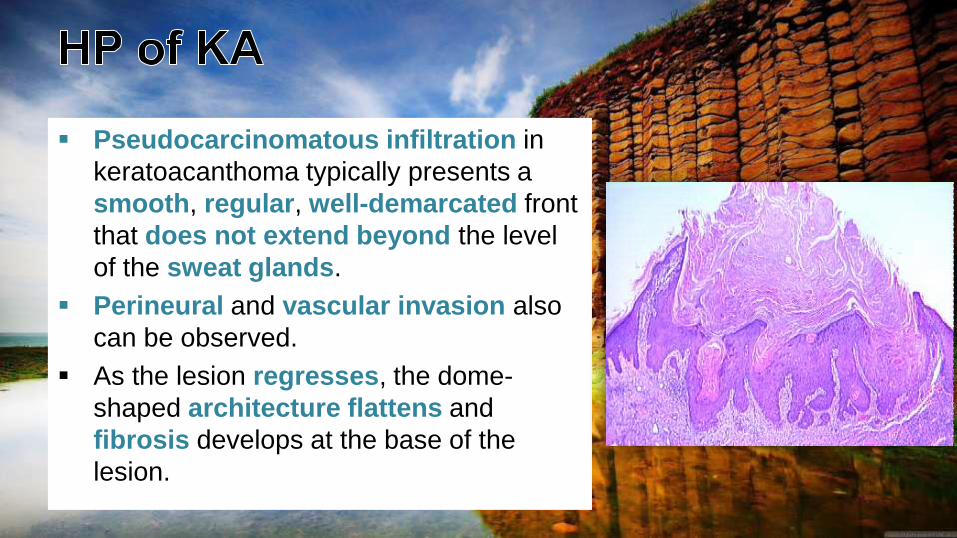
Pseudocarcinomatous infiltration in
keratoacanthoma typically presents a
smooth, regular, well-demarcated front
that does not extend beyond the level
of the sweat glands.
Perineural and vascular invasion also
can be observed.
As the lesion regresses, the dome-
shaped architecture flattens and
fibrosis develops at the base of the
lesion.
Immunohistochemical staining can help differentiate
KA from other epidermal carcinomas.
Filaggrin is ubiquitous in KA but uncommon in
carcinoma.
While the lesion is generally self-limited it should be treated for several reasons;1. To obtain pathology: KA can be difficult to distinguish from invasive SCC. 2. To be rid of an unsightly, tender or worrisome lesion3. To minimize the scar, due to potential cosmetic compromise with the healing of
the lesion. Treatment requires destruction of the lesion. Options include:
1. Surgical Excision (the treatment of choice)2. Cryotherapy3. Curettage and Electrodesiccation4. Laser5. Radiotherapy
Treatment of Multiple KAs:1. Acitretin2. Isotretinoin3. 5-Fluorouracil 4. Methotrexate5. Cyclophosphamide
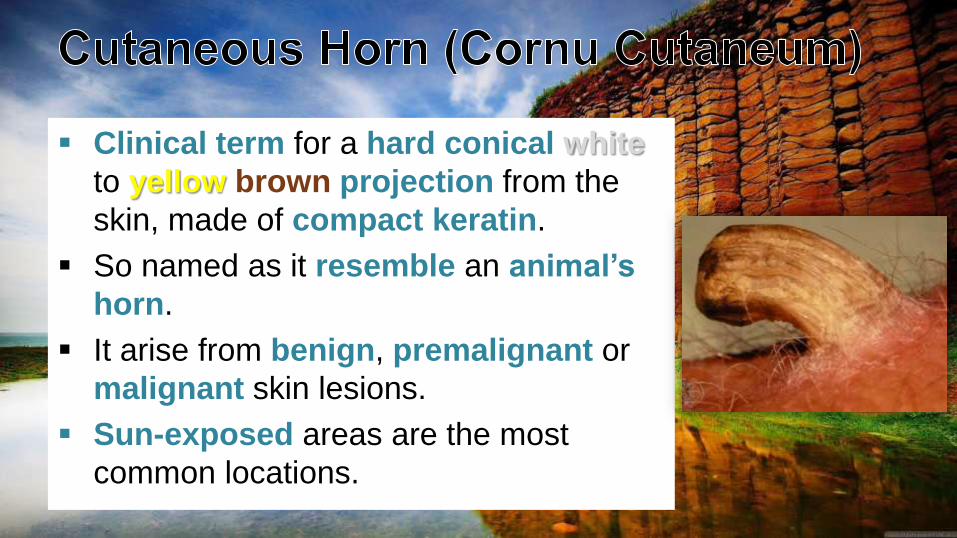
Clinical term for a hard conical white
to yellow brown projection from the
skin, made of compact keratin.
So named as it resemble an animal’s
horn.
It arise from benign, premalignant or
malignant skin lesions.
Sun-exposed areas are the most
common locations.
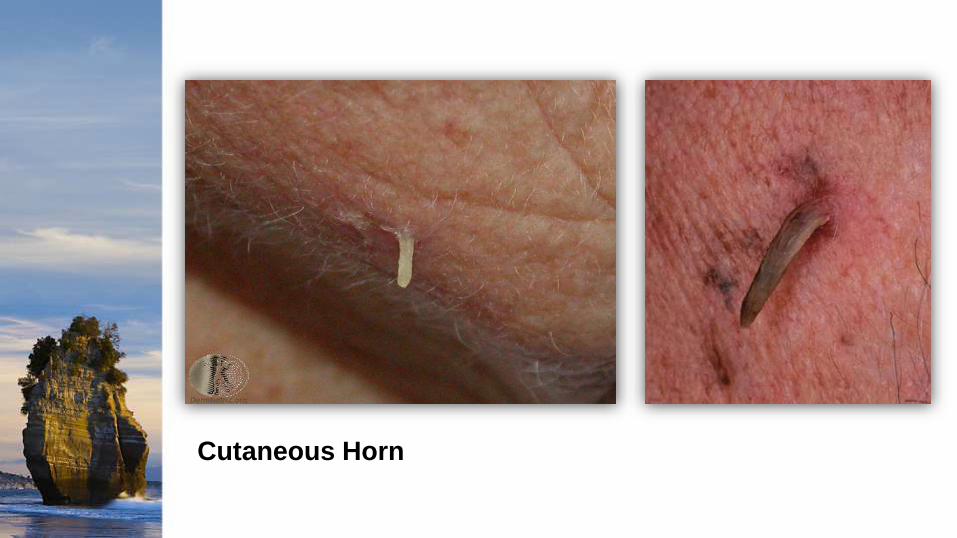
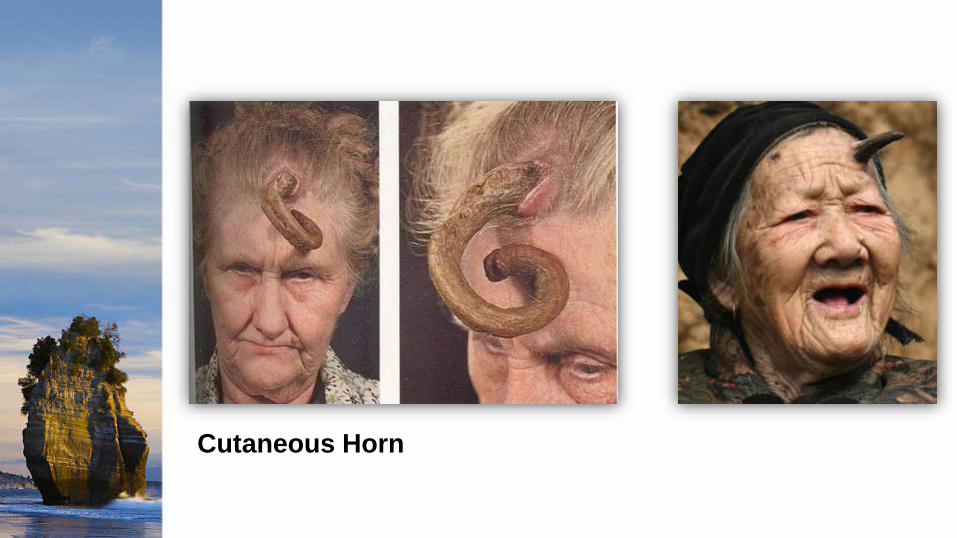
Cutaneous Horn
Cutaneous Horn

Cutaneous Horn
Cutaneous horns are more common in older patients,
with the peak incidence in those between 60 and 70.
Men are affected more frequently than women and
there is a higher risk of the lesion being malignant in
men.
They are more common in people with fairer skins (skin
phototype I and II).
SYMPTOMS:
Cutaneous horns are usually asymptomatic, however
as they are protuberant, they can be injured causing
pain and inflammation.
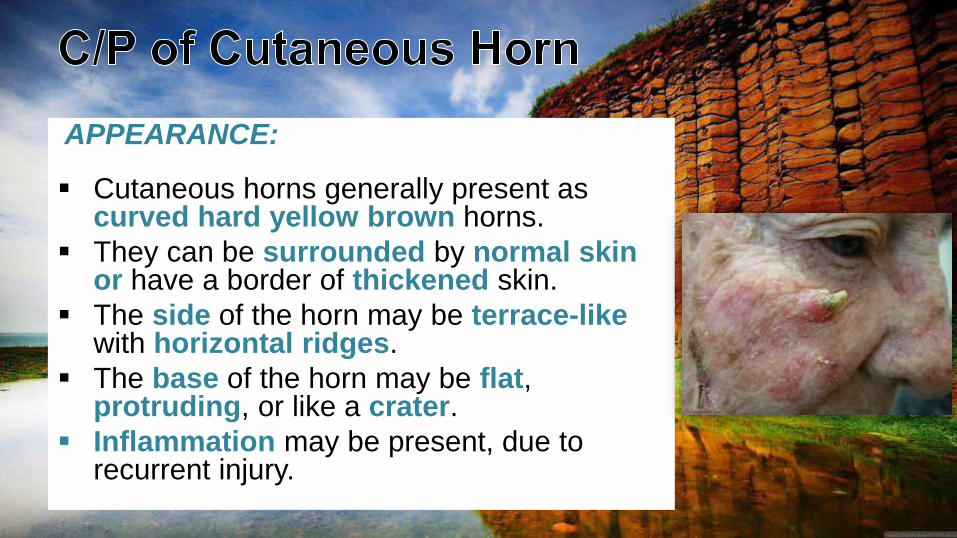
APPEARANCE:
Cutaneous horns generally present as curved hard yellow brown horns.
They can be surrounded by normal skinor have a border of thickened skin.
The side of the horn may be terrace-likewith horizontal ridges.
The base of the horn may be flat, protruding, or like a crater.
Inflammation may be present, due to recurrent injury.
SIZE:
Typically, the horn is taller than twice the width at the base.
It may vary from a few millimeters to several centimetres in size.
LOCATION:
Cutaneous horns are usually single, but can be multiple.
They can occur anywhere on the body, but are morecommon on sun-exposed areas especially the head and ears, dorsum of hands and forearms.
They may also occur on the chest, neck, shoulder and penis.
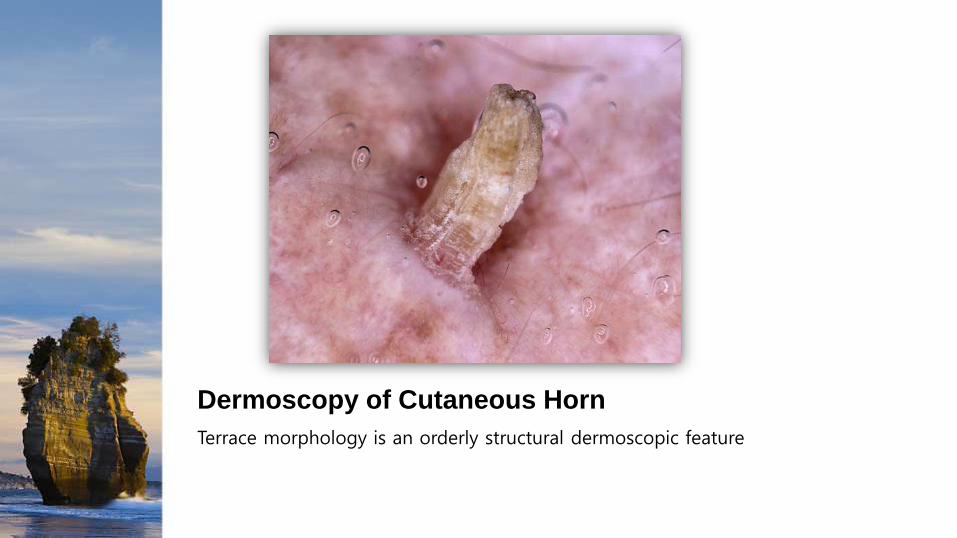
Dermoscopy of Cutaneous Horn
Terrace morphology is an orderly structural dermoscopic feature
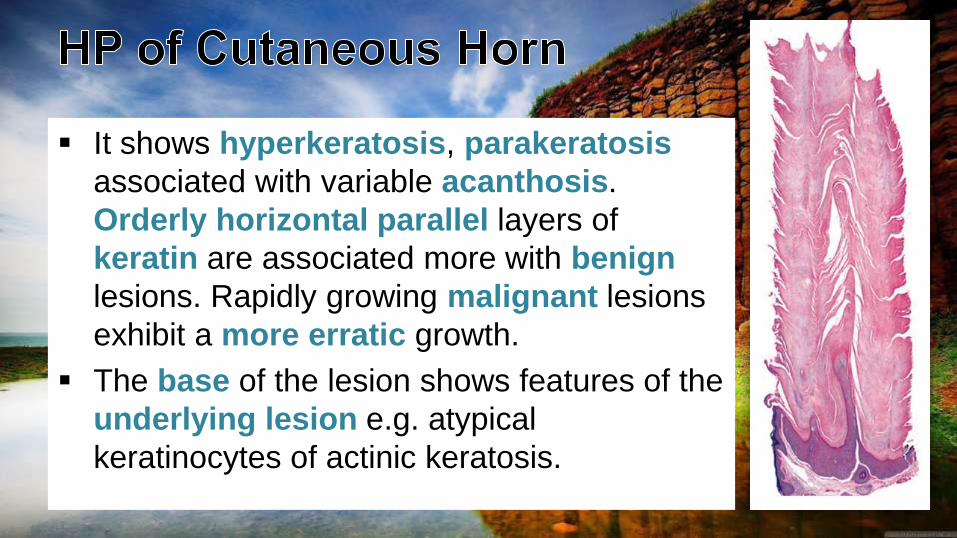
It shows hyperkeratosis, parakeratosis
associated with variable acanthosis.
Orderly horizontal parallel layers of
keratin are associated more with benign
lesions. Rapidly growing malignant lesions
exhibit a more erratic growth.
The base of the lesion shows features of the
underlying lesion e.g. atypical
keratinocytes of actinic keratosis.
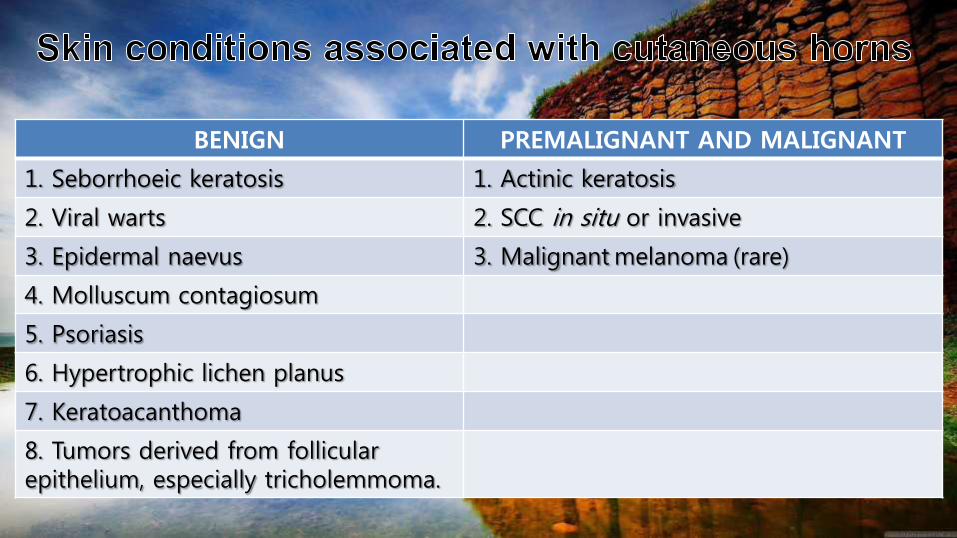
BENIGN PREMALIGNANT AND MALIGNANT
1. Seborrhoeic keratosis 1. Actinic keratosis
2. Viral warts 2. SCC in situ or invasive
3. Epidermal naevus 3. Malignant melanoma (rare)
4. Molluscum contagiosum
5. Psoriasis
6. Hypertrophic lichen planus
7. Keratoacanthoma
8. Tumors derived from follicular epithelium, especially tricholemmoma.
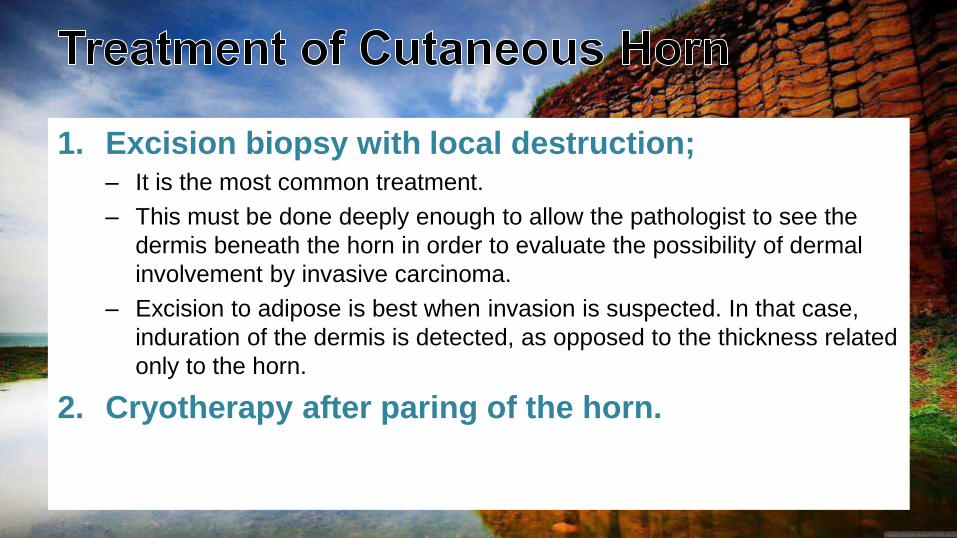
1. Excision biopsy with local destruction; – It is the most common treatment.
– This must be done deeply enough to allow the pathologist to see the
dermis beneath the horn in order to evaluate the possibility of dermal
involvement by invasive carcinoma.
– Excision to adipose is best when invasion is suspected. In that case,
induration of the dermis is detected, as opposed to the thickness related
only to the horn.
2. Cryotherapy after paring of the horn.
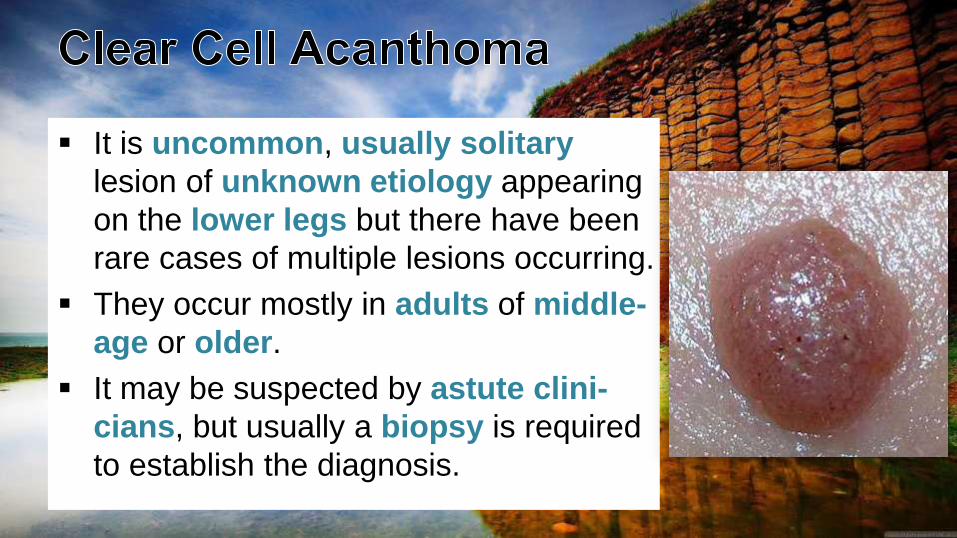
It is uncommon, usually solitary
lesion of unknown etiology appearing
on the lower legs but there have been
rare cases of multiple lesions occurring.
They occur mostly in adults of middle-
age or older.
It may be suspected by astute clini-
cians, but usually a biopsy is required
to establish the diagnosis.
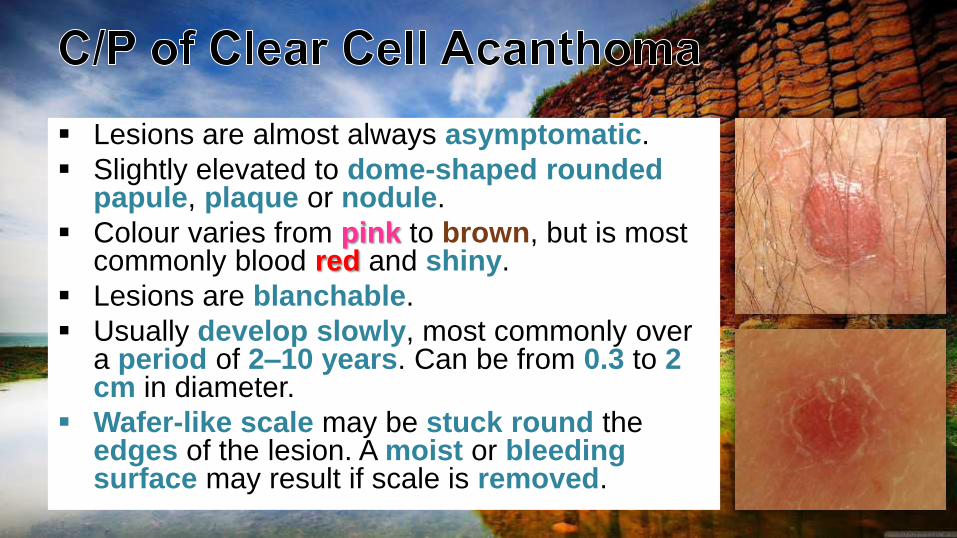
Lesions are almost always asymptomatic.
Slightly elevated to dome-shaped roundedpapule, plaque or nodule.
Colour varies from pink to brown, but is most commonly blood red and shiny.
Lesions are blanchable.
Usually develop slowly, most commonly over a period of 2–10 years. Can be from 0.3 to 2 cm in diameter.
Wafer-like scale may be stuck round the edges of the lesion. A moist or bleedingsurface may result if scale is removed.
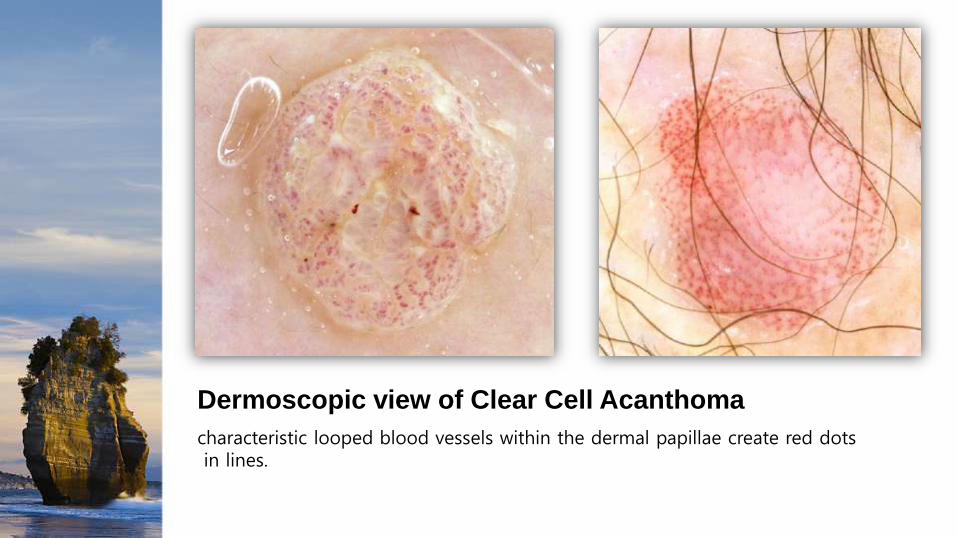
Dermoscopic view of Clear Cell Acanthoma
characteristic looped blood vessels within the dermal papillae create red dotsin lines.
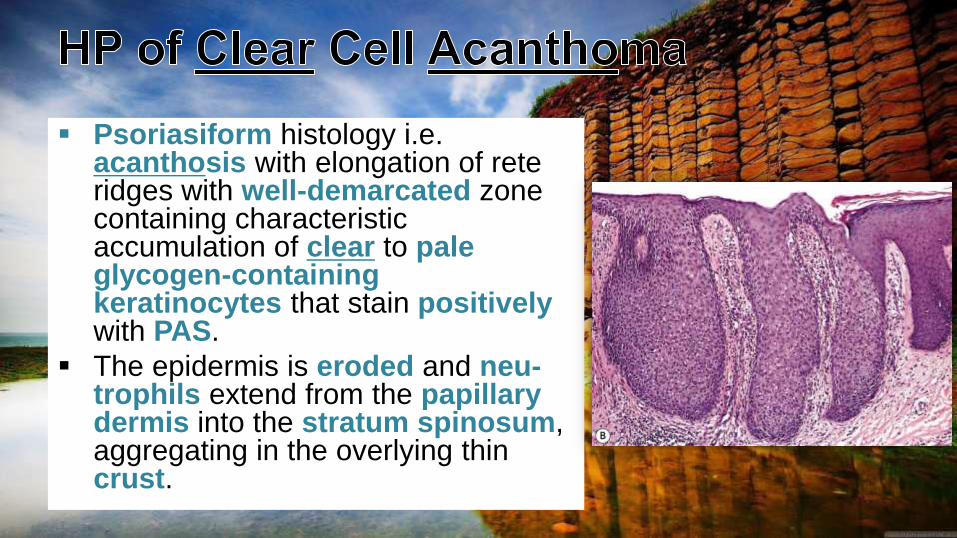
Psoriasiform histology i.e. acanthosis with elongation of rete ridges with well-demarcated zone containing characteristic accumulation of clear to paleglycogen-containingkeratinocytes that stain positivelywith PAS.
The epidermis is eroded and neu-trophils extend from the papillarydermis into the stratum spinosum, aggregating in the overlying thin crust.
They may persist for years and years without changing
or causing any complications.
Simple destruction or excision is adequate for removal.
Shave excision or curettage combined with
electrofulguration is a common form of treatment.
Most lesions do not recur.
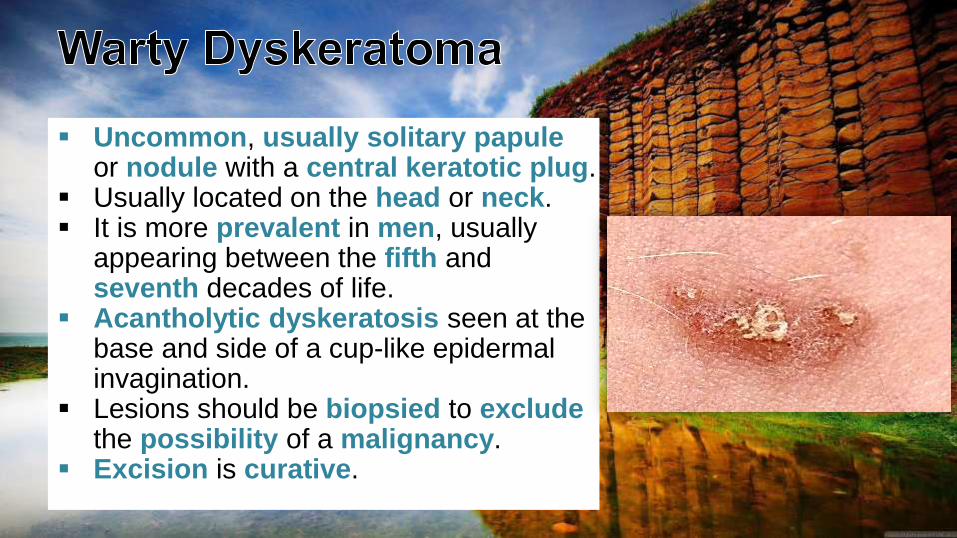
Uncommon, usually solitary papuleor nodule with a central keratotic plug.
Usually located on the head or neck. It is more prevalent in men, usually
appearing between the fifth and seventh decades of life.
Acantholytic dyskeratosis seen at the base and side of a cup-like epidermal invagination.
Lesions should be biopsied to excludethe possibility of a malignancy.
Excision is curative.
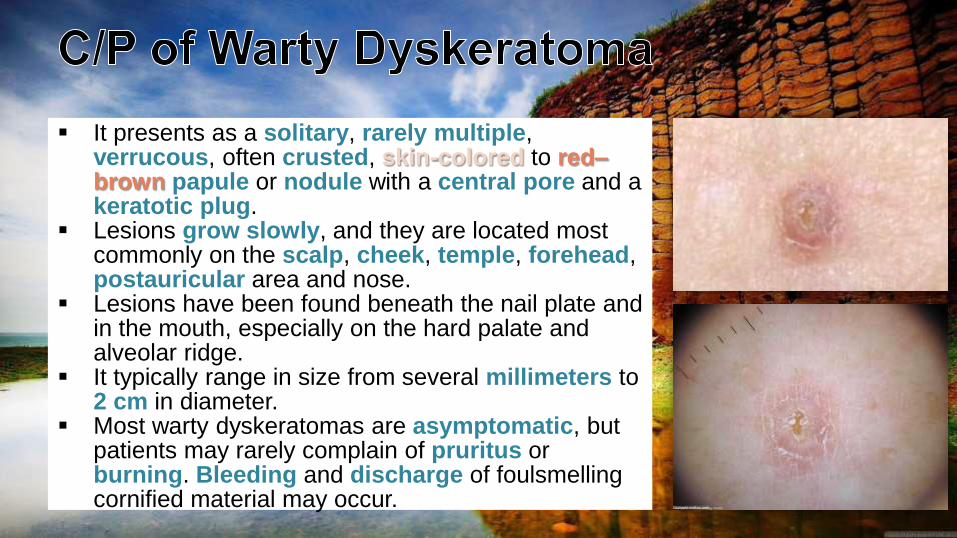
It presents as a solitary, rarely multiple, verrucous, often crusted, skin-colored to red–brown papule or nodule with a central pore and a keratotic plug.
Lesions grow slowly, and they are located most commonly on the scalp, cheek, temple, forehead, postauricular area and nose.
Lesions have been found beneath the nail plate and in the mouth, especially on the hard palate and alveolar ridge.
It typically range in size from several millimeters to 2 cm in diameter.
Most warty dyskeratomas are asymptomatic, but patients may rarely complain of pruritus or burning. Bleeding and discharge of foulsmellingcornified material may occur.
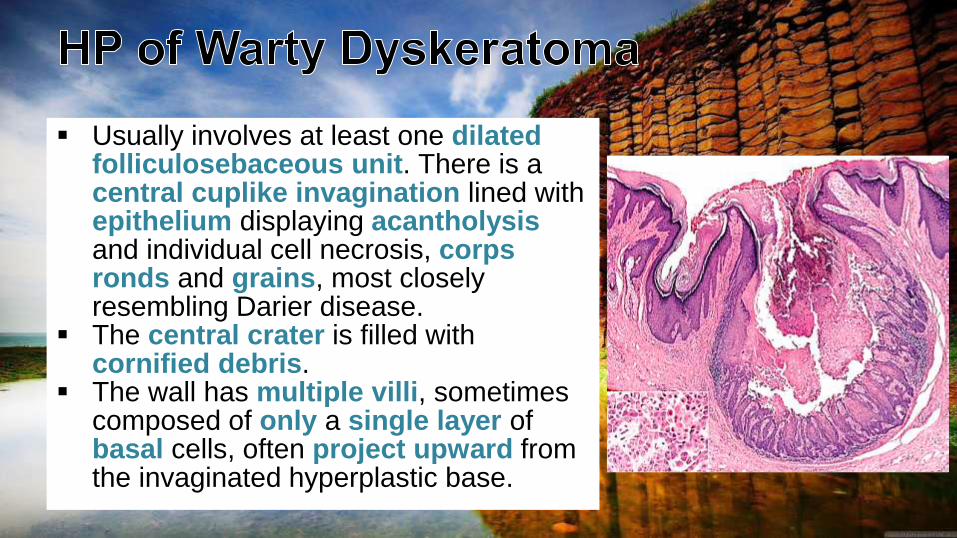
Usually involves at least one dilatedfolliculosebaceous unit. There is a central cuplike invagination lined with epithelium displaying acantholysisand individual cell necrosis, corpsronds and grains, most closely resembling Darier disease.
The central crater is filled with cornified debris.
The wall has multiple villi, sometimes composed of only a single layer of basal cells, often project upward from the invaginated hyperplastic base.
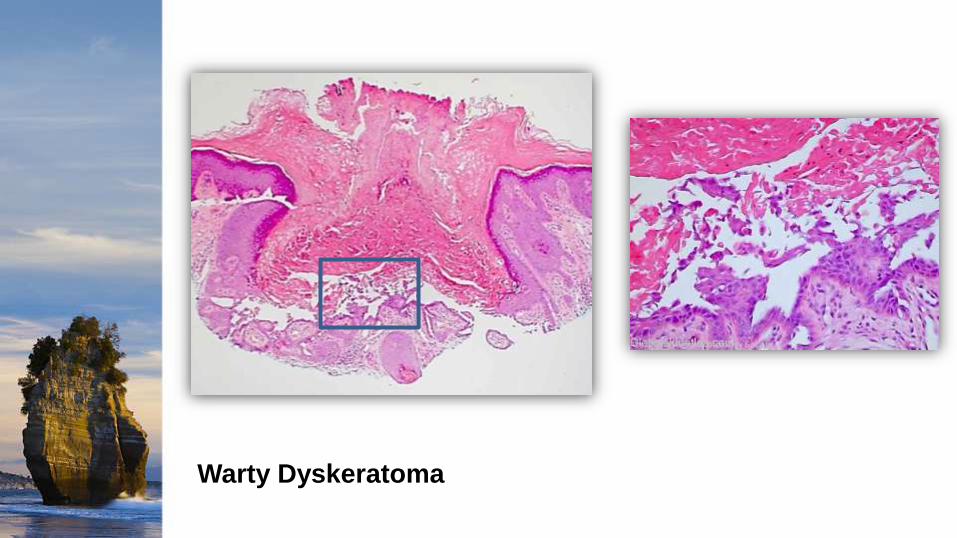
Warty Dyskeratoma
Bolognia 3rd ed.
dermnetnz.org
http://emedicine.medscape.com
http://www.globalskinatlas.com
AAD; Benign Skin Lesions (Presentation)
Skin Tumors by Seyed Morteza Mahmoodi
(Presentation)

Recommended