ANTIPSYCHOTIC INDUCED CARDIOVASCULAR AND METABOLIC SIDE EFFECTS
CURRENT UNDERSTANDING
Dr. Pawan Sharma
1
• INTRODUCTION• HISTORICAL PERSPECTIVE• EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
2
• INTRODUCTION• HISTORICAL PERSPECTIVE• EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
3
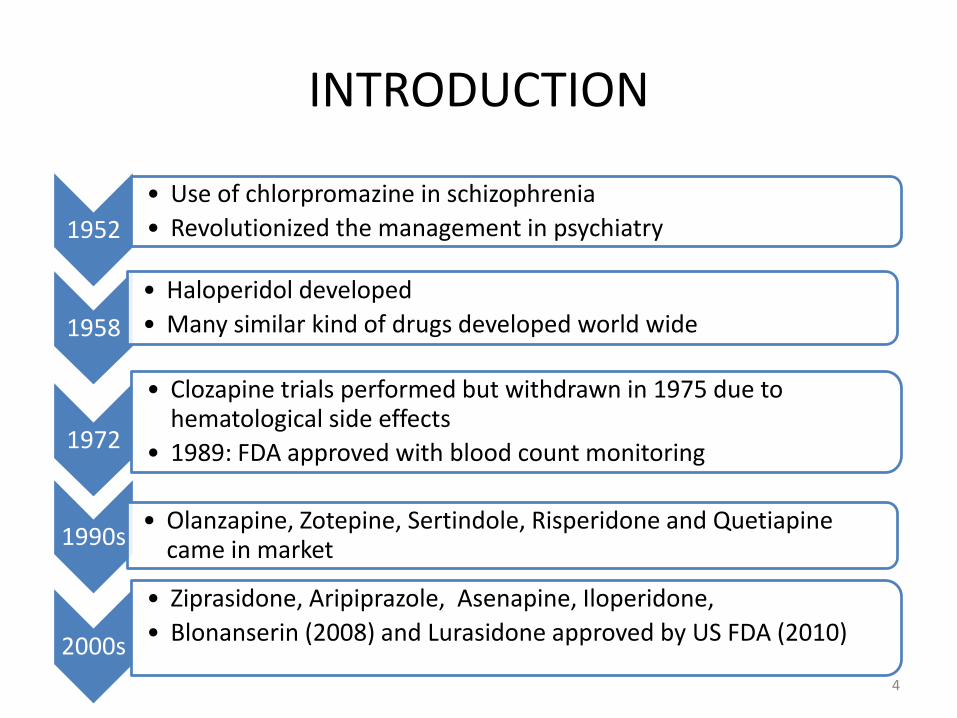
INTRODUCTION
1952
• Use of chlorpromazine in schizophrenia
• Revolutionized the management in psychiatry
1958
• Haloperidol developed
• Many similar kind of drugs developed world wide
1972
• Clozapine trials performed but withdrawn in 1975 due to hematological side effects
• 1989: FDA approved with blood count monitoring
1990s• Olanzapine, Zotepine, Sertindole, Risperidone and Quetiapine
came in market
2000s
• Ziprasidone, Aripiprazole, Asenapine, Iloperidone,
• Blonanserin (2008) and Lurasidone approved by US FDA (2010)
4
Neurotherapeutics (2009) 6, 78-85
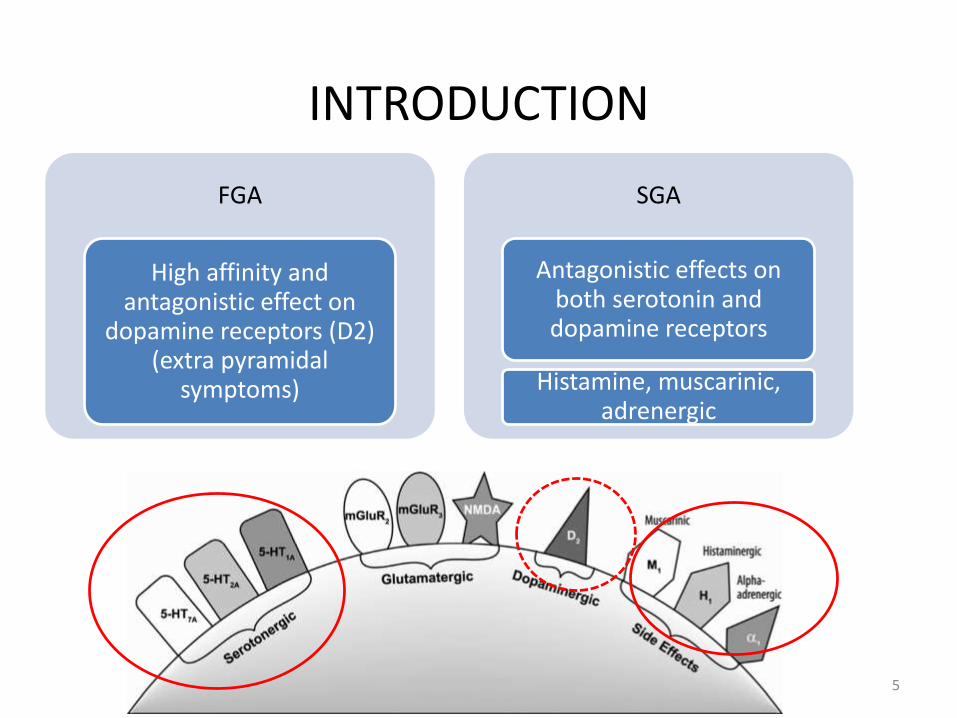
INTRODUCTION
FGA
High affinity and antagonistic effect on
dopamine receptors (D2) (extra pyramidal
symptoms)
SGA
Antagonistic effects on both serotonin and dopamine receptors
Histamine, muscarinic, adrenergic
5
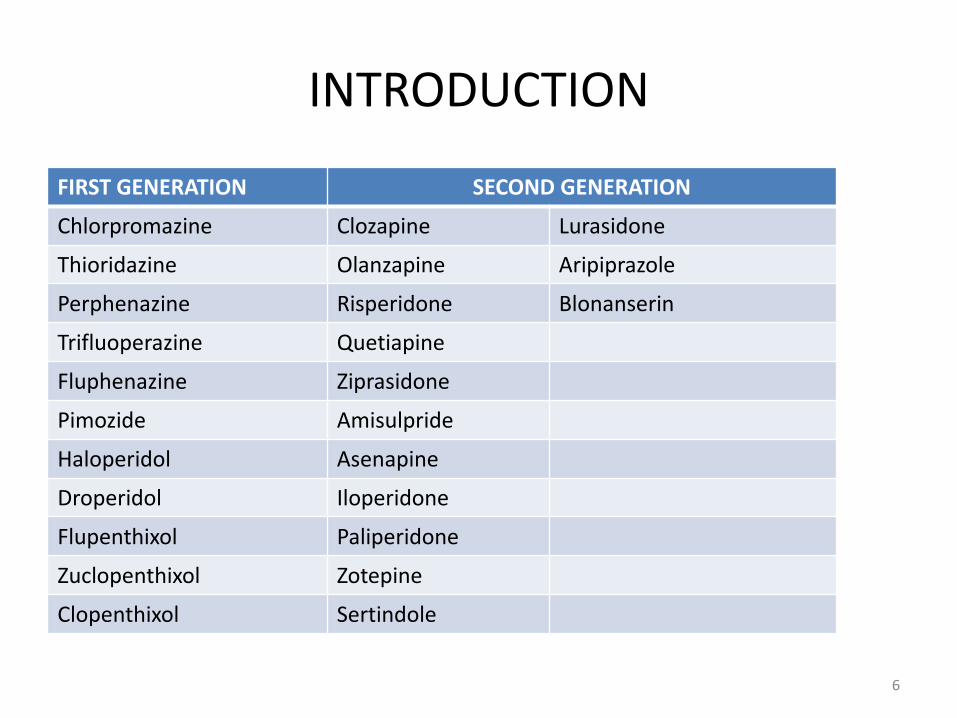
INTRODUCTION
FIRST GENERATION SECOND GENERATION
Chlorpromazine Clozapine Lurasidone
Thioridazine Olanzapine Aripiprazole
Perphenazine Risperidone Blonanserin
Trifluoperazine Quetiapine
Fluphenazine Ziprasidone
Pimozide Amisulpride
Haloperidol Asenapine
Droperidol Iloperidone
Flupenthixol Paliperidone
Zuclopenthixol Zotepine
Clopenthixol Sertindole
6
HISTORICAL PERSPECTIVE-METABOLIC AND CARDIOVASCULAR SIDE EFFECTS
• The metabolic and cardio vascular side effects of conventional antipsychotics had been recognized just after few years of introduction
• Studies show Phenothiazine derivatives to be associated with cardio vascular and metabolic side effects
– Impaired glucose tolerance and diabetes
Arneson, 1964
7
HISTORICAL PERSPECTIVE-METABOLIC SIDE EFFECTS
• The glucose tolerance studied in groups of patients during long-term treatment (more than three months) showed aberrations in glucose tolerance test
– 40% patients Chlorpromazine
– 35% patients Perphenazine
– 15% patients Clopenthixol
Amdisen A, 1964
• A prospective study of schizophrenic patients on injectable depot neuroleptic drugs as maintenance therapy showed a clinically significant weight gain in 55% of patients
Johnson, 1979
8
HISTORICAL PERSPECTIVE-METABOLIC SIDE EFFECTS
• It is common for the patients receiving Phenothiazine to gain 10-15 pounds of weight in the course of 1-2 year of treatment
• Many patients discontinue the medication due to this side effect
Jerrold, 1987
• In a meta-analysis , over a period of 10 weeks treatment
– Conventional agents, mean weight change ranged from a reduction of 0.39 kg with Molindone to an increase of 3.19 kg with Thioridazine
– Newer antipsychotic agents, mean increases were as follows: clozapine-4.45 kg olanzapine- 4.15 kg; Sertindole- 2.92 kg; risperidone-2.10 kg; and Ziprasidone- 0.04 kg.
Allison et al, 1999
9
HISTORICAL PERSPECTIVE-METABOLIC SIDE EFFECTS
• In 2003 FDA required all manufacturers of atypical antipsychotics to include a warning about the risk of hyperglycemia and diabetes
• The end of the conventional antipsychotic era and the beginning of the atypical antipsychotic era of 1990s coincided with the onset of an epidemic of type II diabetes
Stahl et al, 2009
10
HISTORICAL PERSPECTIVE-CARDIOVASCULAR SIDE EFFECTS
• The first report of sudden arrhythmic death—Thioridazine, 1963
• Isolated case reports of increased blood pressure and sudden cardiac death reported with use of haloperidol
Gerle B, 1964
• As early as 1968, American Heart Association had advised routine ECG and Chest X-ray 6 monthly for the patients on Phenothiazines
• Major and possibly fatal arrhythmias can occur in young adults without antecedent heart disease who are receiving therapeutic dosages of Thioridazine
Libscomb PA, 1980
11
HISTORICAL PERSPECTIVE-CARDIOVASCULAR SIDE EFFECTS
• In 1991, Mehtonen et al. examined all medico legal autopsies in Finland over a 3-year period (N= 24158).
– 49 sudden unexpected deaths among apparently healthy adults taking psychotropic medication.
– Forty-six of these 49 deaths involved a phenothiazine, primarily
Thioridazine (28 of the 46 cases)
• 12 unexplained sudden deaths and 23 cases of syncope occurred among 1,446 patients during Sertindole premarketing trials in 1996
Glassman and Bigger, 2001
12
• INTRODUCTION• HISTORICAL PERSPECTIVE• EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
13
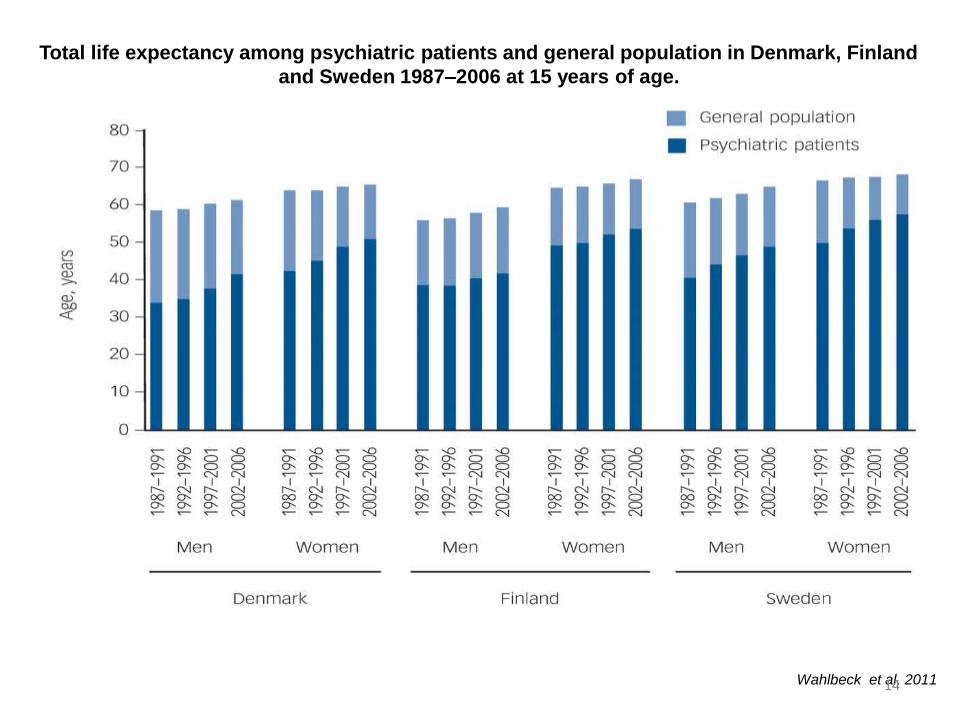
Total life expectancy among psychiatric patients and general population in Denmark, Finland
and Sweden 1987–2006 at 15 years of age.
Wahlbeck et al, 201114
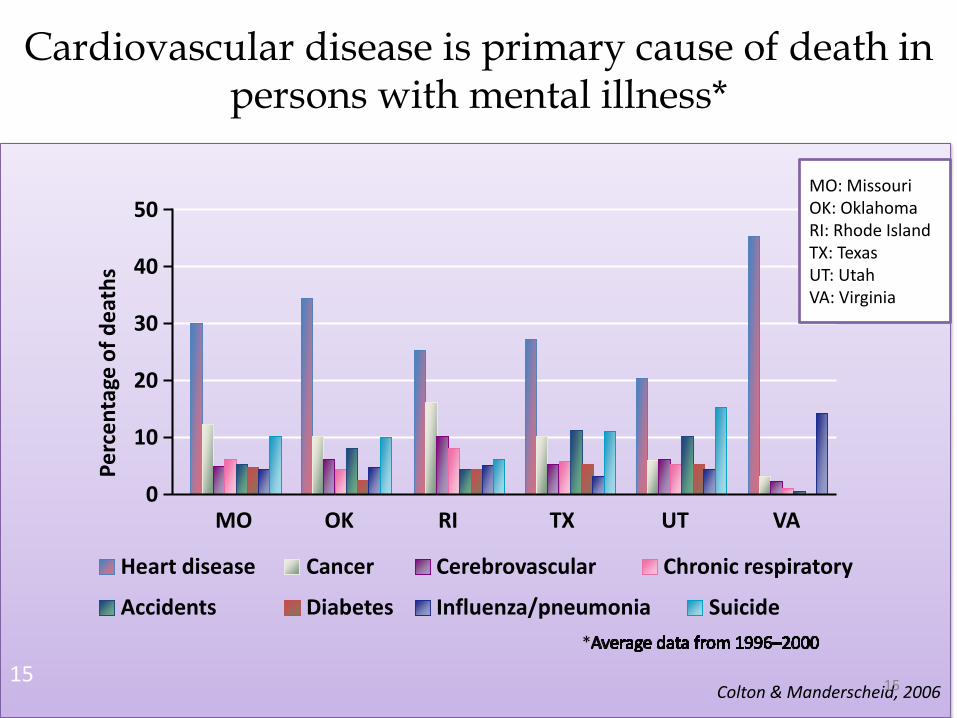
Cardiovascular disease is primary cause of death in persons with mental illness*
*
Pe
rce
nta
ge o
f d
eat
hs
50
40
20
10
0
30
Heart disease Cancer Cerebrovascular Chronic respiratory
Diabetes Influenza/pneumoniaAccidents Suicide
MO OK RI TX UT VA
Colton & Manderscheid, 200615
MO: MissouriOK: OklahomaRI: Rhode IslandTX: TexasUT: UtahVA: Virginia
15
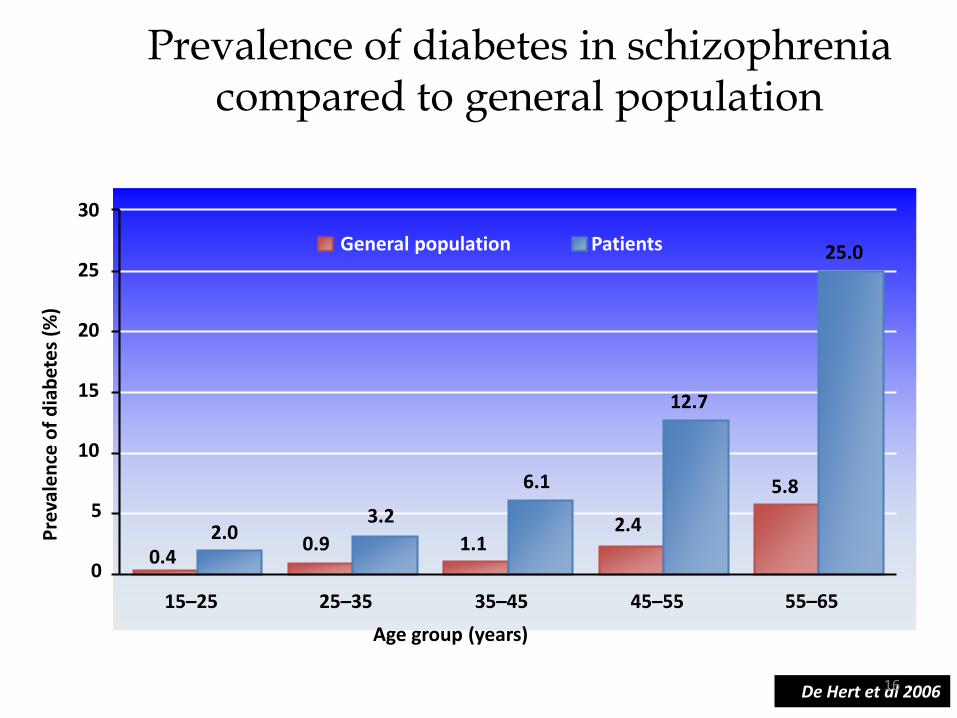
Prevalence of diabetes in schizophrenia compared to general population
8.6% diabetes; n=415
De Hert et al 2006
15
Age group (years)
General population Patients
15–25 25–35 35–45 45–55 55–65
0
5
10
20
25
30
0.42.0
0.9 1.1
6.1
25.0
5.8
Pre
vale
nce
of
dia
bet
es
(%)
3.2 2.4
12.7
1616
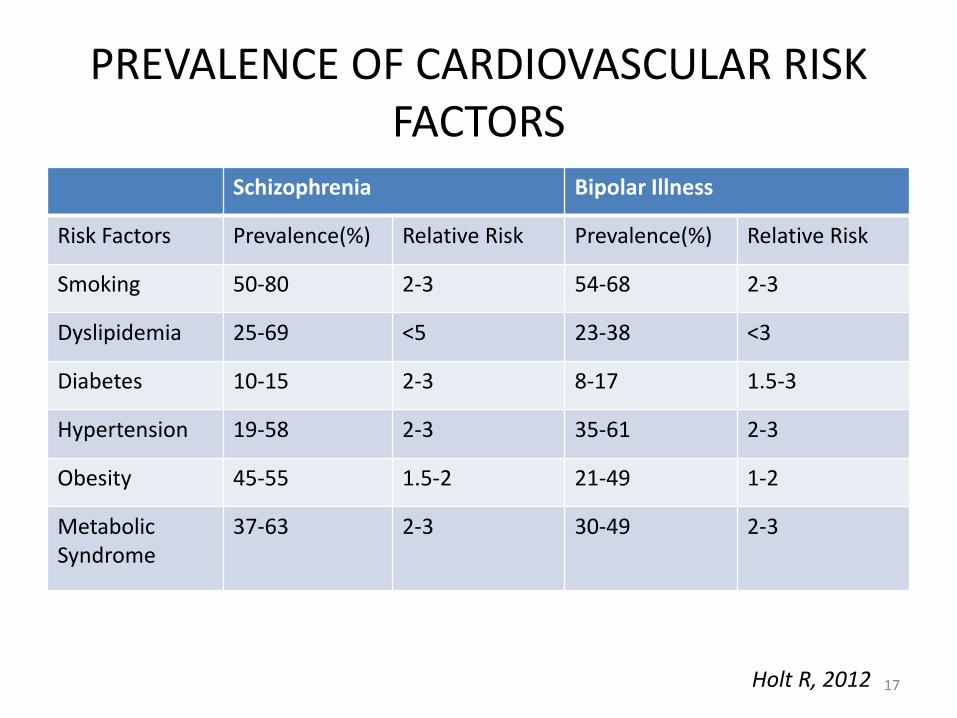
PREVALENCE OF CARDIOVASCULAR RISK FACTORS
Schizophrenia Bipolar Illness
Risk Factors Prevalence(%) Relative Risk Prevalence(%) Relative Risk
Smoking 50-80 2-3 54-68 2-3
Dyslipidemia 25-69 <5 23-38 <3
Diabetes 10-15 2-3 8-17 1.5-3
Hypertension 19-58 2-3 35-61 2-3
Obesity 45-55 1.5-2 21-49 1-2
Metabolic Syndrome
37-63 2-3 30-49 2-3
Holt R, 2012 17
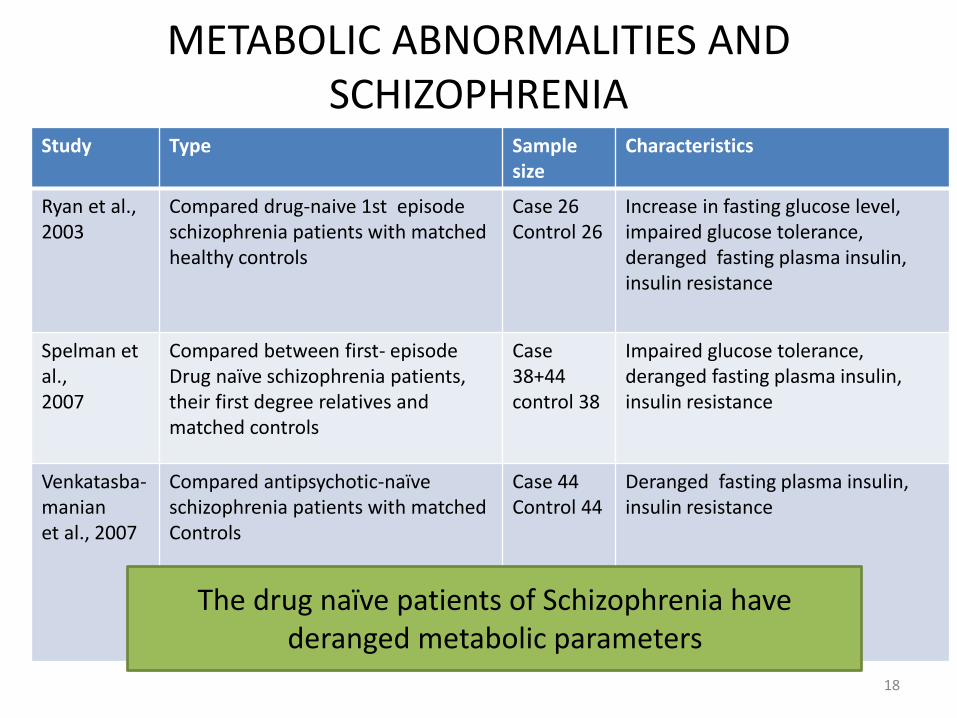
Study Type Sample size
Characteristics
Ryan et al., 2003
Compared drug-naive 1st episode schizophrenia patients with matched healthy controls
Case 26Control 26
Increase in fasting glucose level, impaired glucose tolerance, deranged fasting plasma insulin, insulin resistance
Spelman et al., 2007
Compared between first- episode Drug naïve schizophrenia patients, their first degree relatives and matched controls
Case 38+44 control 38
Impaired glucose tolerance, deranged fasting plasma insulin, insulin resistance
Venkatasba-manian et al., 2007
Compared antipsychotic-naïve schizophrenia patients with matched Controls
Case 44 Control 44
Deranged fasting plasma insulin, insulin resistance
METABOLIC ABNORMALITIES AND SCHIZOPHRENIA
The drug naïve patients of Schizophrenia have deranged metabolic parameters
18
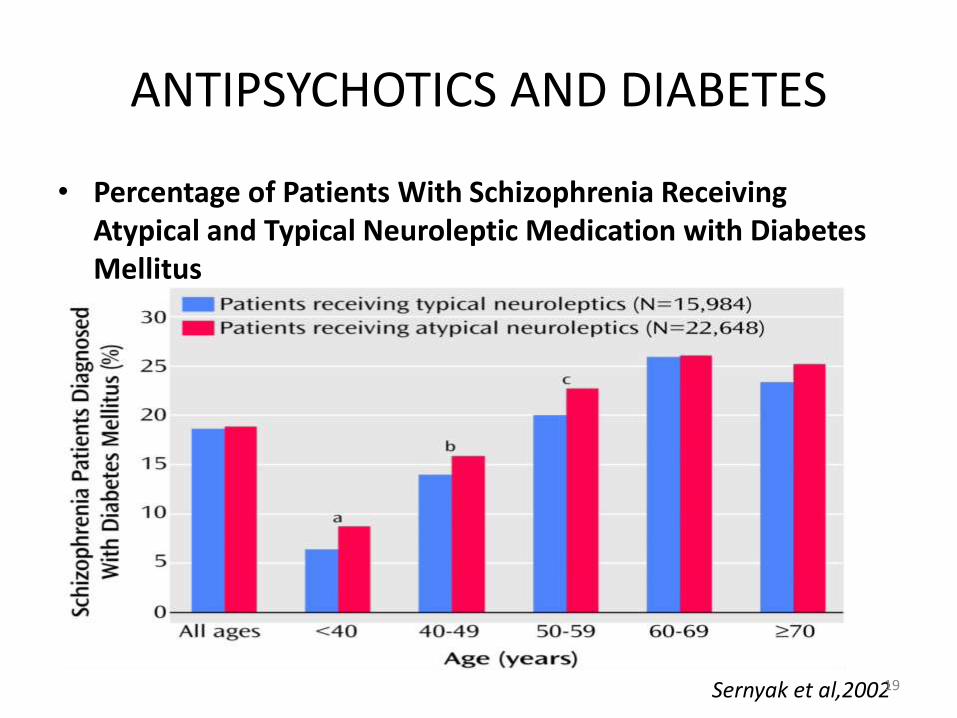
ANTIPSYCHOTICS AND DIABETES
• Percentage of Patients With Schizophrenia Receiving Atypical and Typical Neuroleptic Medication with Diabetes Mellitus
Sernyak et al,200219
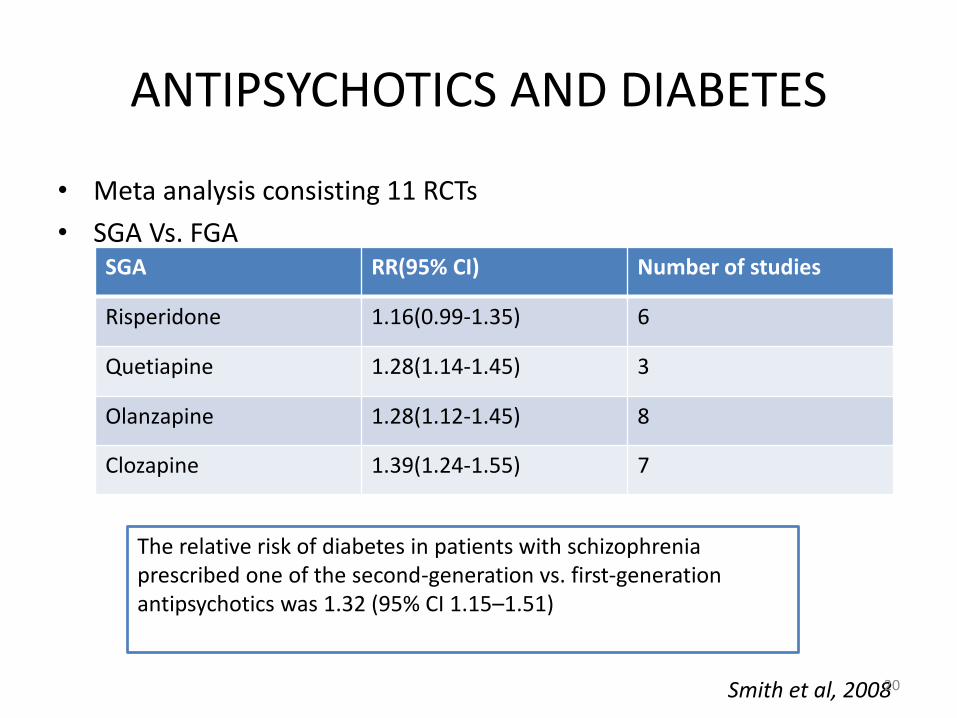
ANTIPSYCHOTICS AND DIABETES
• Meta analysis consisting 11 RCTs
• SGA Vs. FGASGA RR(95% CI) Number of studies
Risperidone 1.16(0.99-1.35) 6
Quetiapine 1.28(1.14-1.45) 3
Olanzapine 1.28(1.12-1.45) 8
Clozapine 1.39(1.24-1.55) 7
The relative risk of diabetes in patients with schizophrenia prescribed one of the second-generation vs. first-generation antipsychotics was 1.32 (95% CI 1.15–1.51)
Smith et al, 200820
METABOLIC SYNDROME
• Cluster of physiological abnormalities characterized by insulin resistance leading to increased risk of DM type II and cardiovascular risk
• WHO defines:
– Diabetes or impaired fasting glycaemia or impaired glucose tolerance or insulin resistance
– Plus 2 or more of the following
• Obesity: BMI 30 or waist-to-hip ratio 0·9 (male) or 0·85 (female)
• Dyslipidaemia: triglycerides 150 mg/dl or HDL cholesterol<50 (male) or 40 (female) mg/dl
• Hypertension: blood pressure 140/90 mm Hg
• Microalbuminuria: albumin excretion> 20 g/min
21
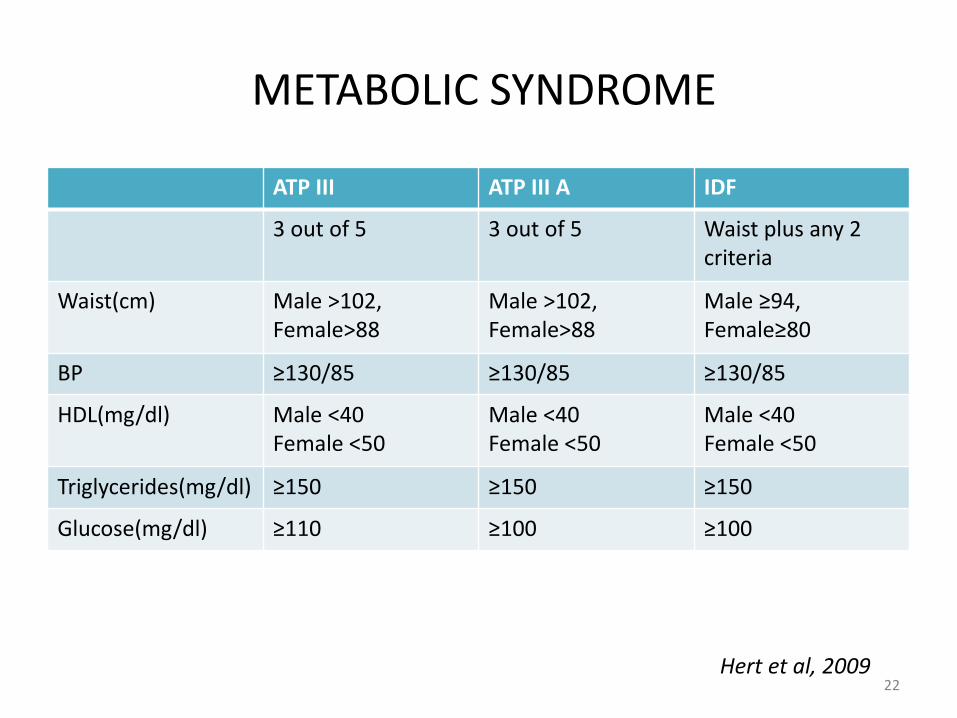
METABOLIC SYNDROME
ATP III ATP III A IDF
3 out of 5 3 out of 5 Waist plus any 2 criteria
Waist(cm) Male >102, Female>88
Male >102, Female>88
Male ≥94, Female≥80
BP ≥130/85 ≥130/85 ≥130/85
HDL(mg/dl) Male <40Female <50
Male <40Female <50
Male <40Female <50
Triglycerides(mg/dl) ≥150 ≥150 ≥150
Glucose(mg/dl) ≥110 ≥100 ≥100
Hert et al, 200922
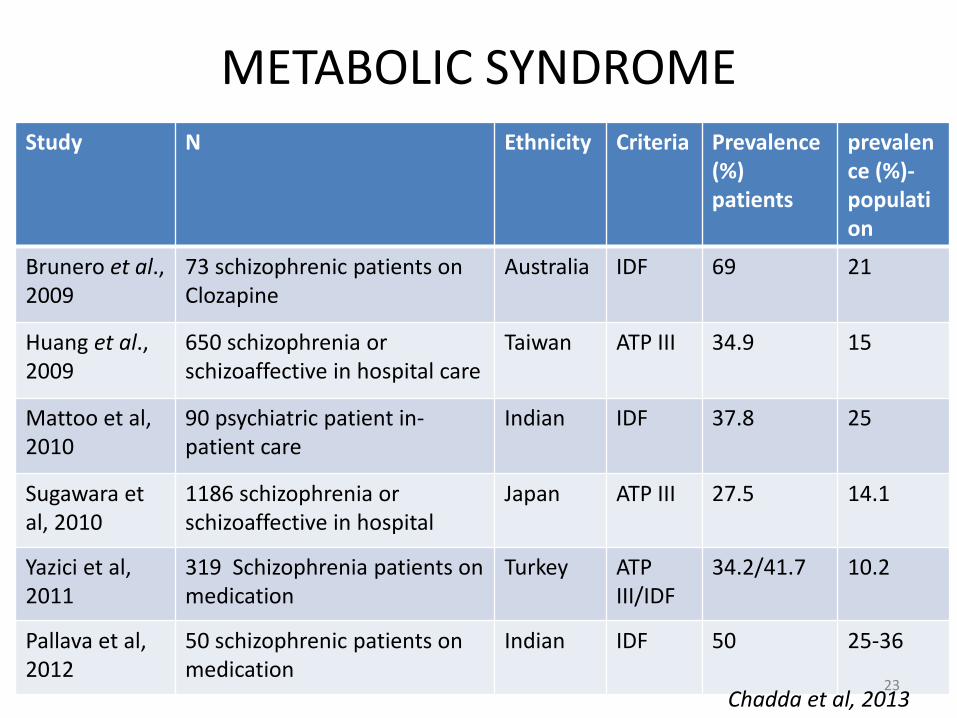
METABOLIC SYNDROMEStudy N Ethnicity Criteria Prevalence
(%) patients
prevalence (%)-population
Brunero et al., 2009
73 schizophrenic patients on Clozapine
Australia IDF 69 21
Huang et al., 2009
650 schizophrenia or schizoaffective in hospital care
Taiwan ATP III 34.9 15
Mattoo et al, 2010
90 psychiatric patient in-patient care
Indian IDF 37.8 25
Sugawara et al, 2010
1186 schizophrenia or schizoaffective in hospital
Japan ATP III 27.5 14.1
Yazici et al,2011
319 Schizophrenia patients on medication
Turkey ATP III/IDF
34.2/41.7 10.2
Pallava et al, 2012
50 schizophrenic patients on medication
Indian IDF 50 25-36
Chadda et al, 201323
METABOLIC SYNDROME
• Study exploring metabolic syndrome status in patients of CATIE (Clinical Antipsychotic Trial of Intervention Effectiveness)
• N=660
• Compared between base line and 3 months of treatment
– Olanzapine and Quetiapine: largest mean increase of waist circumference (0.7 inch) followed by Risperidone (0.4 inch) no change in Ziprasidone group
– Olanzapine group had increased fasting triglyceride (+21.5mg/dl) compared to Ziprasidone (-32.1 mg/dl)
– No significant finding in blood pressureMeyer et al, 2008
24
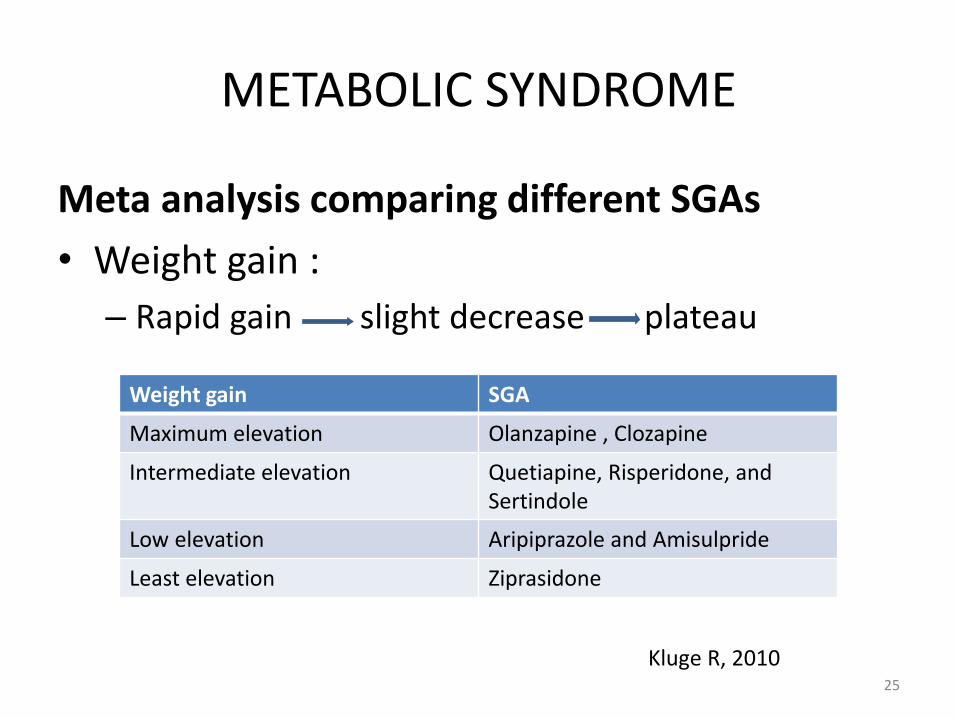
METABOLIC SYNDROME
Meta analysis comparing different SGAs
• Weight gain :
– Rapid gain slight decrease plateau
Weight gain SGA
Maximum elevation Olanzapine , Clozapine
Intermediate elevation Quetiapine, Risperidone, and Sertindole
Low elevation Aripiprazole and Amisulpride
Least elevation Ziprasidone
Kluge R, 201025
METABOLIC SYNDROME
• Olanzapine caused the most elevation in cholesterol, clearly more than Aripiprazole, Risperidone, and Ziprasidone
• No differences were found in comparison between Amisulpride, Clozapine and Quetiapine
• Quetiapine showed more cholesterol increase than Risperidone and was close to that observed with olanzapine
• Similarly olanzapine and clozapine had maximum change in the glucose utilization
Kluge, R 2010
26
METABOLIC SYNDROME
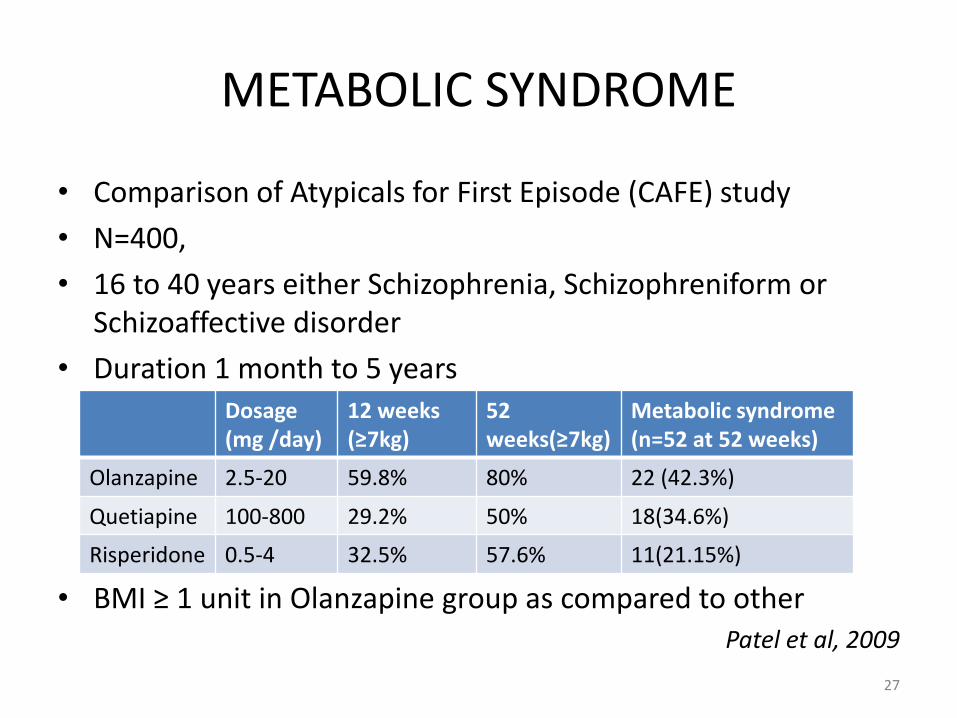
• Comparison of Atypicals for First Episode (CAFE) study
• N=400,
• 16 to 40 years either Schizophrenia, Schizophreniform or Schizoaffective disorder
• Duration 1 month to 5 years
• BMI ≥ 1 unit in Olanzapine group as compared to otherPatel et al, 2009
Dosage(mg /day)
12 weeks (≥7kg)
52weeks(≥7kg)
Metabolic syndrome (n=52 at 52 weeks)
Olanzapine 2.5-20 59.8% 80% 22 (42.3%)
Quetiapine 100-800 29.2% 50% 18(34.6%)
Risperidone 0.5-4 32.5% 57.6% 11(21.15%)
27
CARDIOVASCULAR SIDE EFFECTS
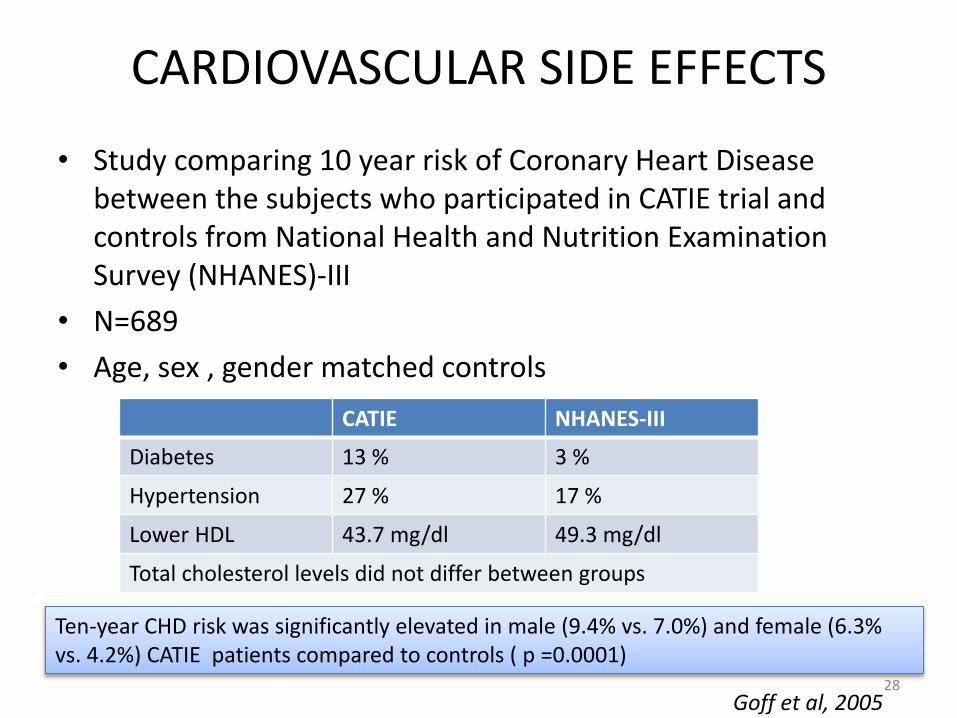
• Study comparing 10 year risk of Coronary Heart Disease between the subjects who participated in CATIE trial and controls from National Health and Nutrition Examination Survey (NHANES)-III
• N=689
• Age, sex , gender matched controls
CATIE NHANES-III
Diabetes 13 % 3 %
Hypertension 27 % 17 %
Lower HDL 43.7 mg/dl 49.3 mg/dl
Total cholesterol levels did not differ between groups
Ten-year CHD risk was significantly elevated in male (9.4% vs. 7.0%) and female (6.3% vs. 4.2%) CATIE patients compared to controls ( p =0.0001)
Goff et al, 200528
CARDIOVASCULAR SIDE EFFECTS
• Study comparing the effect of Ziprasidone, Risperidone, olanzapine, Quetiapine, Thioridazine, and Haloperidol on the QT interval
• All previous medications stopped for 7 days , Placebo for 5 days and base line ECG performed
• Randomly assigned to receive one of the six drugs
• Blood levels were obtained, and repeat ECGs were recorded at the time of maximum drug blood level
• Maximum prolongation was seen with Thioridazine group followed by Ziprasidone ,Quetiapine and Risperidone (unlike published literature)
Glassman et al, 200129
CARDIOVASCULAR SIDE EFFECTS
• Clozapine: Cardiomyopathy and Myocarditis
• Range from subclinical presentation to fulminant pulmonary edema and cardiogenic shock
• 15 cases (0.187%) of clozapine-related myocarditis out of 8000 clozapine-treated patients in Australian patients
Kilian et al, 1999
• 9 of 94 patients initiated on clozapine over 3 years appeared to have experienced a suspected myocarditis (incidence of 9.6%)
Reinders et al,2004
• Tends to appear at any time during treatment but more frequently from 4 days to 22 weeks after initiation
30
HYPERPROLACTINEMIA
• Roughly equated to the potency of an antipsychotic to block D2 receptors
• More common with FGA than SGA except Risperidone and Paliperidone
• Short-term– Include menstrual disturbances– Galactorrhea, sexual dysfunction, infertility in women – Sexual dysfunction and Gynaecomastia in men
• Long term:– Estrogen deficiency in women – Testosterone deficiency in men resulting in decreased
bone mineral density Bostwick et al, 2009
31
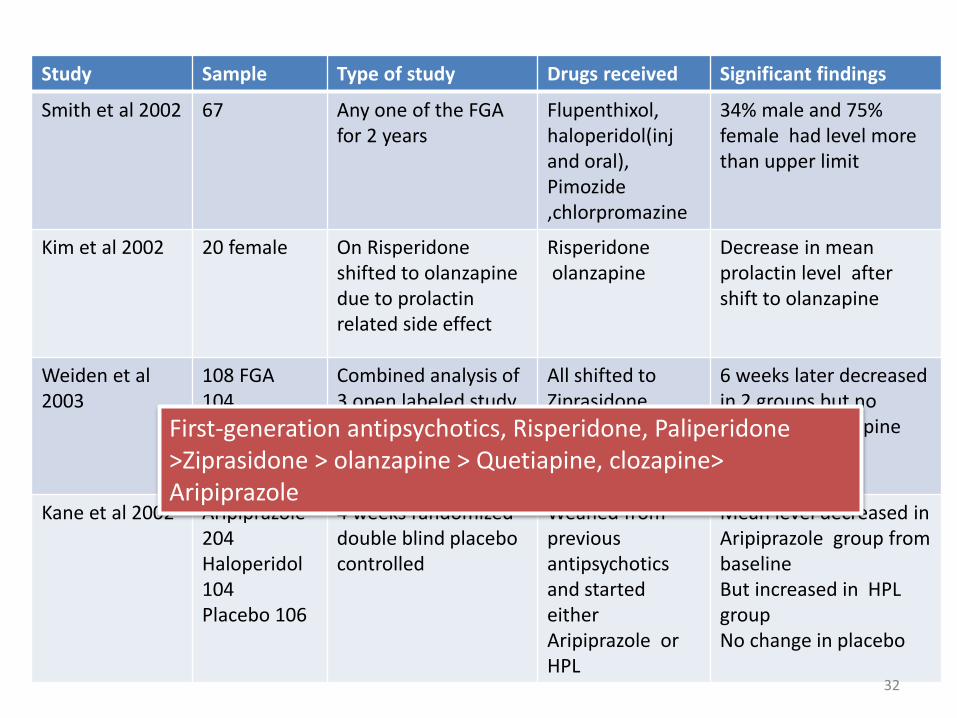
Study Sample Type of study Drugs received Significant findings
Smith et al 2002 67 Any one of the FGAfor 2 years
Flupenthixol, haloperidol(injand oral), Pimozide,chlorpromazine
34% male and 75% female had level more than upper limit
Kim et al 2002 20 female On Risperidone shifted to olanzapine due to prolactin related side effect
Risperidoneolanzapine
Decrease in mean prolactin level after shift to olanzapine
Weiden et al 2003
108 FGA104 olanzapineRisperidone58
Combined analysis of3 open labeled study
All shifted to Ziprasidone
6 weeks later decreased in 2 groups but no change in olanzapine group
Kane et al 2002 Aripiprazole -204Haloperidol 104Placebo 106
4 weeks randomized double blind placebocontrolled
Weaned from previousantipsychotics and started either Aripiprazole or HPL
Mean level decreased in Aripiprazole group from baseline But increased in HPL groupNo change in placebo
First-generation antipsychotics, Risperidone, Paliperidone >Ziprasidone > olanzapine > Quetiapine, clozapine> Aripiprazole
32
To summarize
• There is definite risk of antipsychotics for
– Weight gain
– Diabetes
– CHD
– Metabolic Syndrome
– QTc prolongation and Sudden cardiac death
– Hyperprolactinemia
• The relative risk of metabolic abnormalities is more with second generation antipsychotics as compared to first generation
33
• INTRODUCTION• HISTORICAL PERSPECTIVE • EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
34
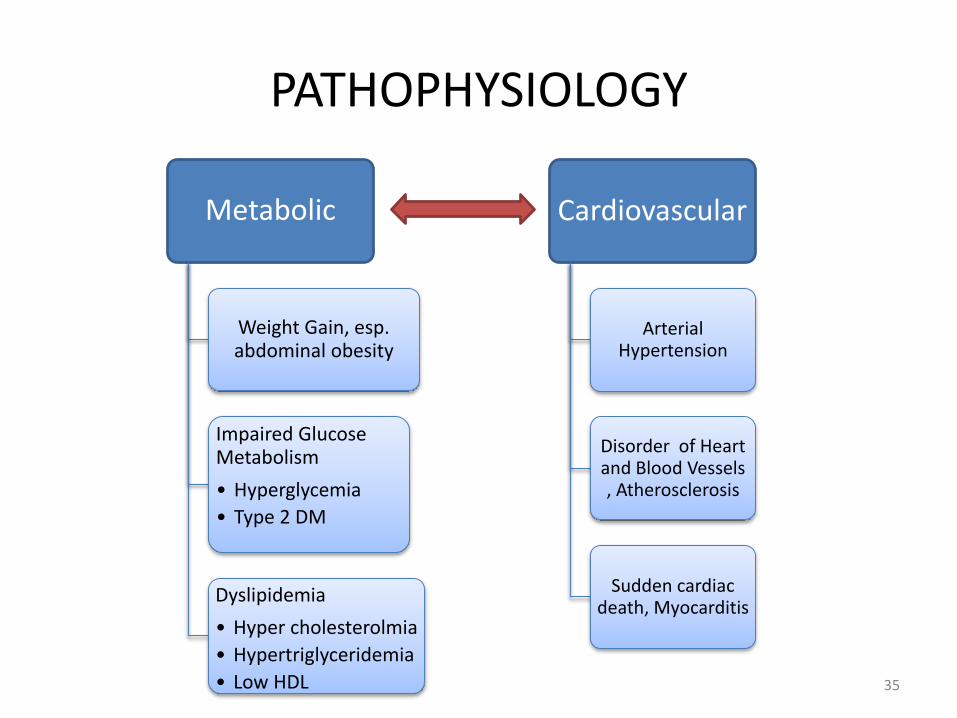
PATHOPHYSIOLOGY
Metabolic
Weight Gain, esp. abdominal obesity
Impaired Glucose Metabolism
• Hyperglycemia
• Type 2 DM
Dyslipidemia
• Hyper cholesterolmia
• Hypertriglyceridemia
• Low HDL
Cardiovascular
Arterial Hypertension
Disorder of Heart and Blood Vessels , Atherosclerosis
Sudden cardiac death, Myocarditis
35
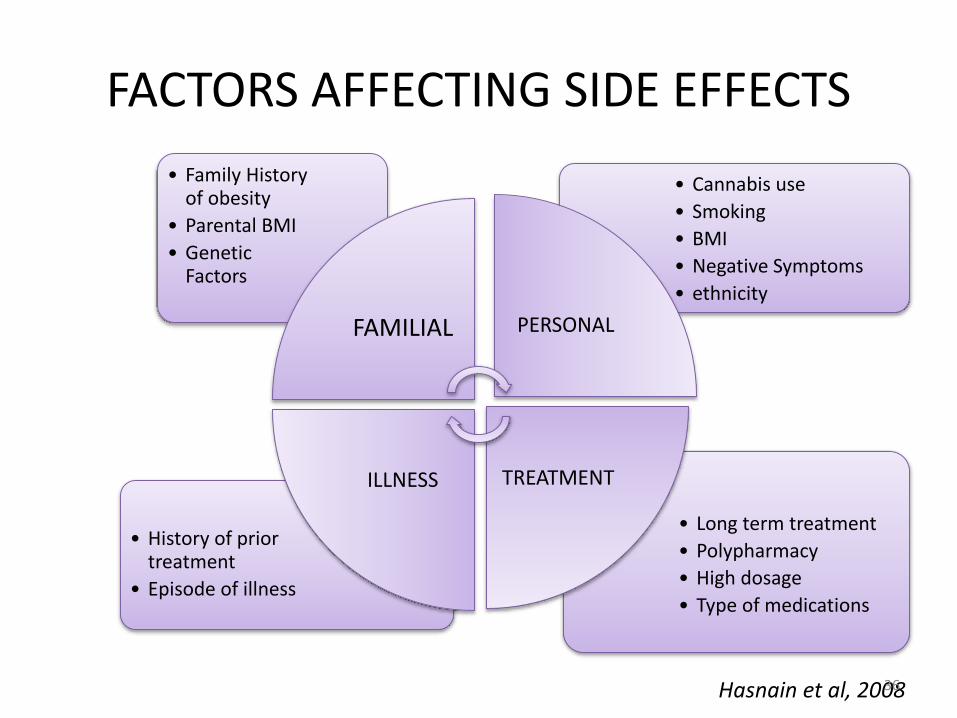
FACTORS AFFECTING SIDE EFFECTS
• Long term treatment
• Polypharmacy
• High dosage
• Type of medications
• History of prior treatment
• Episode of illness
• Cannabis use
• Smoking
• BMI
• Negative Symptoms
• ethnicity
• Family History of obesity
• Parental BMI
• Genetic Factors
FAMILIAL PERSONAL
TREATMENTILLNESS
Hasnain et al, 200836
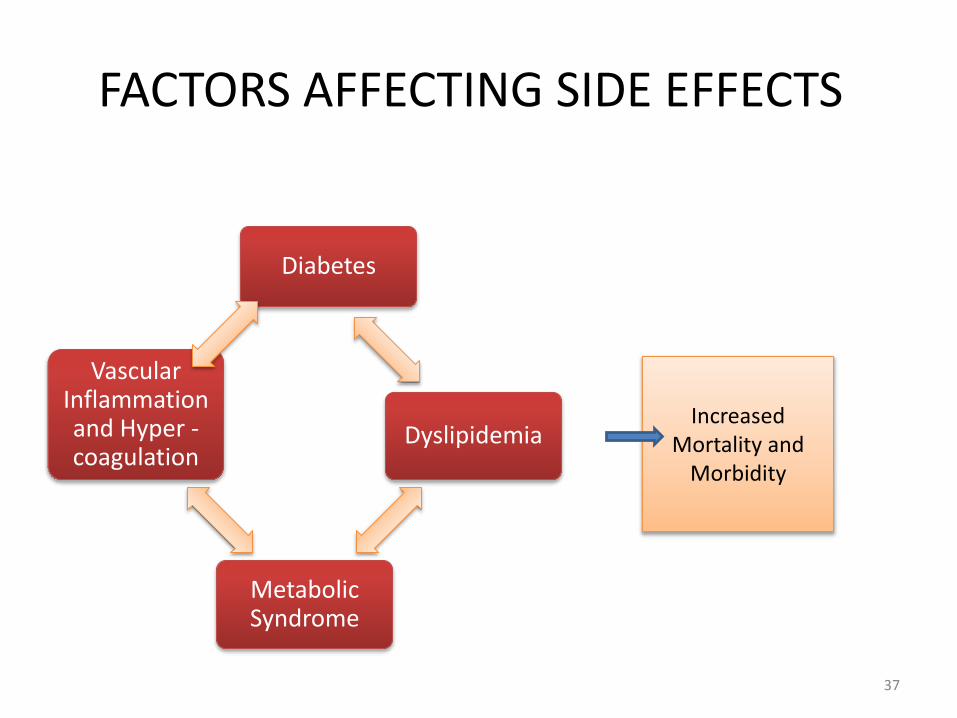
FACTORS AFFECTING SIDE EFFECTS
Diabetes
Dyslipidemia
Metabolic Syndrome
Vascular Inflammation and Hyper -coagulation
Increased Mortality and
Morbidity
37
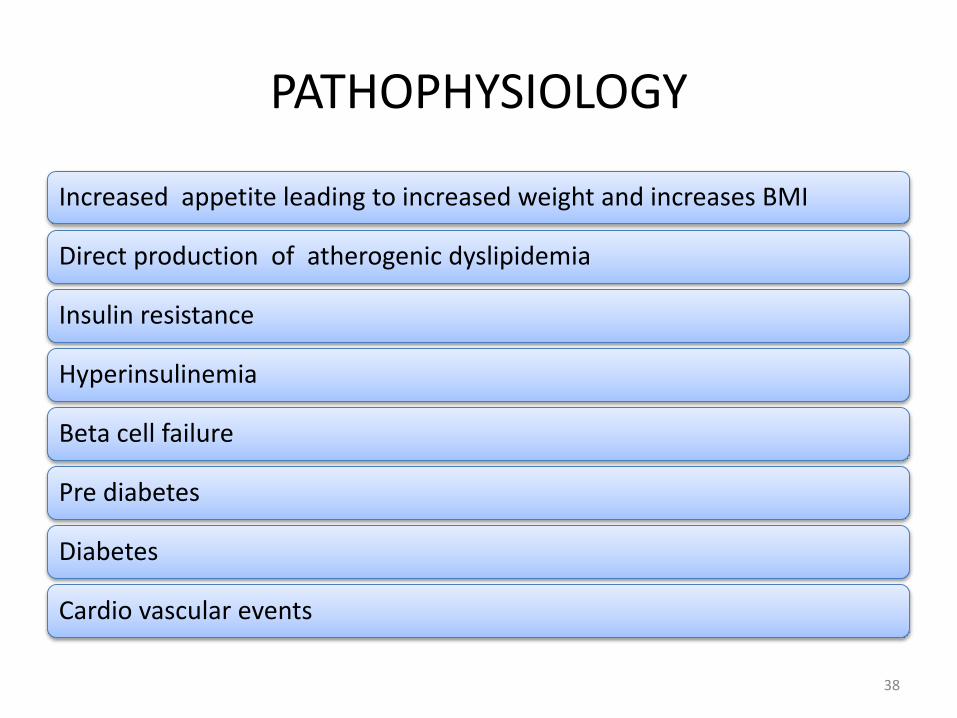
PATHOPHYSIOLOGY
Increased appetite leading to increased weight and increases BMI
Direct production of atherogenic dyslipidemia
Insulin resistance
Hyperinsulinemia
Beta cell failure
Pre diabetes
Diabetes
Cardio vascular events
38
PATHOPHYSIOLOGY• Blockade of H1 receptors and activation of hypothalamic AMP
kinase leads to increased appetite
• 5HT2C receptor is involved in the feeding behavior
• Peripheral factors unrelated to appetite, such as increased cellular lipogenesis because of enhanced activity of fatty acid synthase and stearoyl-CoA desaturase
• Hypothetical role of receptor X: adipose tissue, liver and skeletal muscle – and possibly the brain – which would lead to insulin resistance
• Hypothetical role of M3 muscarinic cholinergic receptors: more propensity for developing Diabetic ketoacidosis
Stahl et al, 2009
39
PATHOPHYSIOLOGY
• Genome wide association studies (GWAS) to search for genetic variation affecting the susceptibility to metabolic side effects
• Schizophrenia patients from CATIE trial
• Different SNPs and intragenic markers were found to be significant in the change of metabolic parameters
• SNP in MEIS2 gene mediated the effects of Risperidone on waist circumference
Adkins et al, 2011
40
PATHOPHYSIOLOGY
• To study the susceptibility of antipsychotic induced metabolic changes, 76 mice were treated with haloperidol, olanzapine or clozapine for 7 days
• Functional analysis was conducted on the putative targets of altered microRNA
• Metabolic pathways were enriched in olanzapine and clozapine treatments, possibly associated with their weight gain side effects
• Suggests a role for microRNA in the mechanism of action and the metabolic side effects of the atypical antipsychotic drugs
Santarelli et al, 2013
41
• INTRODUCTION• HISTORCAL PERSPECTIVE• EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
42
MANAGEMENT FOR WEIGHT GAIN AND METABOLIC ABNORMALITIES
The 2010 PORT guidelines:
• Early behavioral intervention
• Pharmacotherapy
switching from one agent to another
addition of another medication before the initiation of antipsychotic treatment
addition of another medication during the antipsychotic treatment
Buchanan et al. 2010
43
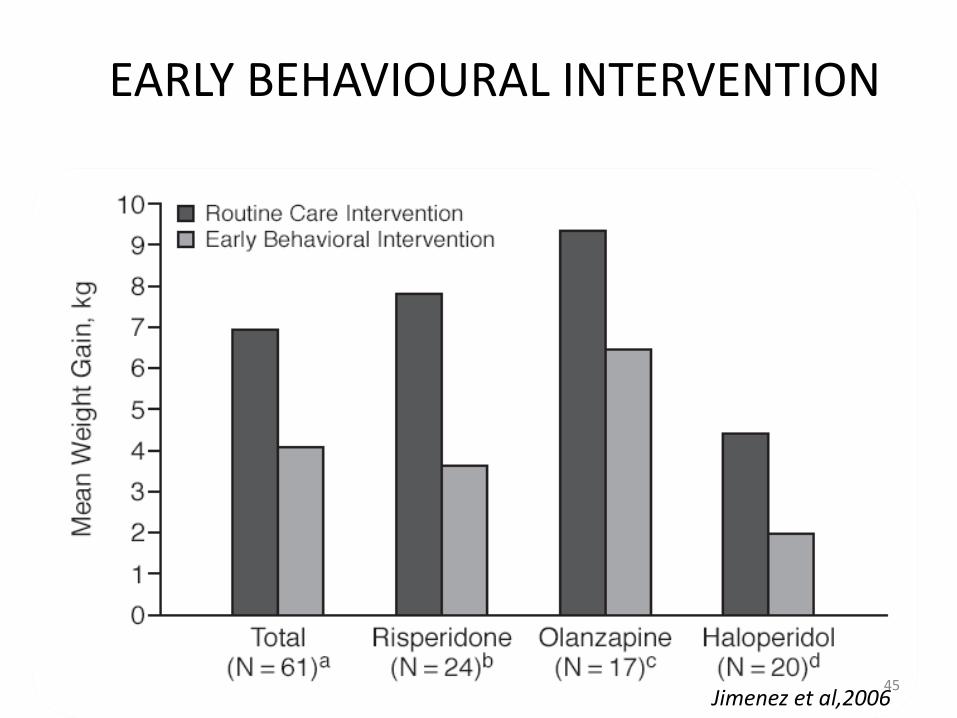
EARLY BEHAVIOURAL INTERVENTION
• 61 treatment naive psychotic patients
• Randomly assigned to Olanzapine, Risperidone or Haloperidol
• Further randomized to either early behavioral intervention (EBI) or routine care intervention (RCI)
• EBI: 8 flexible intervention modules that incorporated behavioural interventions, nutrition, and exercise) (10-14 sessions over 3 M)
• RCI: patients were informed about potential weight gain and advised to increase their exercise and limit food intake
Jimenez et al,2006
44
EARLY BEHAVIOURAL INTERVENTION
J Clin Psychiatry. 2006 Aug;67(8):1253-60 Jimenez et al,200645
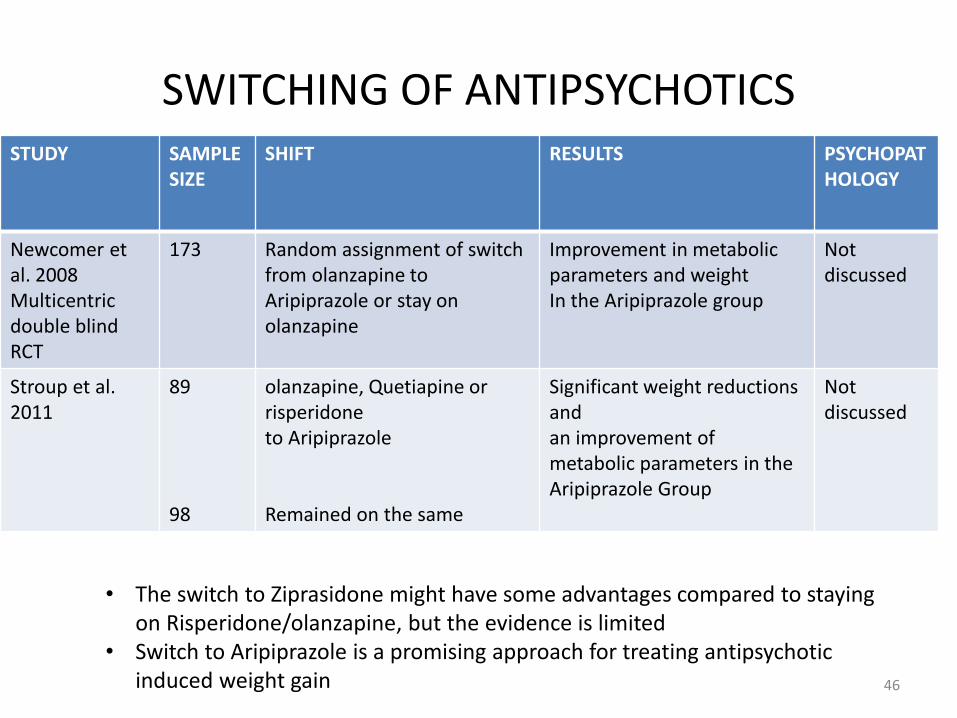
SWITCHING OF ANTIPSYCHOTICSSTUDY SAMPLE
SIZE SHIFT RESULTS PSYCHOPAT
HOLOGY
Newcomer et al. 2008Multicentric double blind RCT
173 Random assignment of switch from olanzapine to Aripiprazole or stay on olanzapine
Improvement in metabolic parameters and weight In the Aripiprazole group
Not discussed
Stroup et al. 2011
89
98
olanzapine, Quetiapine or risperidoneto Aripiprazole
Remained on the same
Significant weight reductions andan improvement of metabolic parameters in the Aripiprazole Group
Not discussed
• The switch to Ziprasidone might have some advantages compared to staying on Risperidone/olanzapine, but the evidence is limited
• Switch to Aripiprazole is a promising approach for treating antipsychotic induced weight gain 46
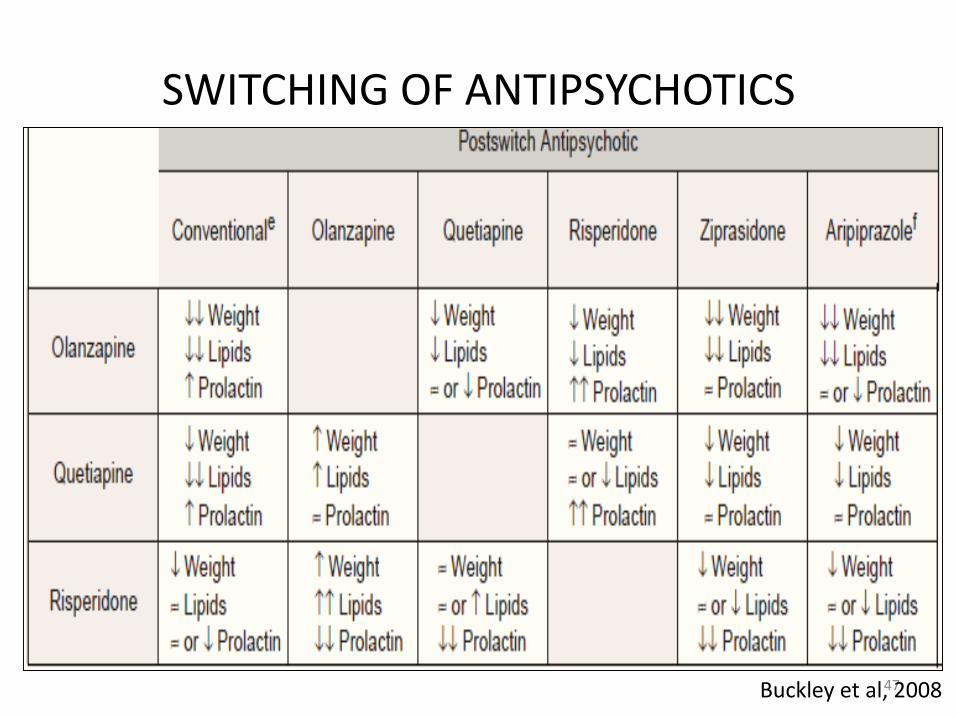
SWITCHING OF ANTIPSYCHOTICS
47Buckley et al, 2008
ADDITION OF ANOTHER MEDICATION
• Amantadine:
– Case reports
– Risk of flaring psychosis
• H2 receptor antagonist
– Nizatidine :
Double-blind RCT. Patients on olanzapine (5 – 20 mg/day) significantly less weight gain after 4 weeks add-on treatment with doses of 300 mg bd
Result not significant after 24 weeks Cavazzoni et al. 2003
48
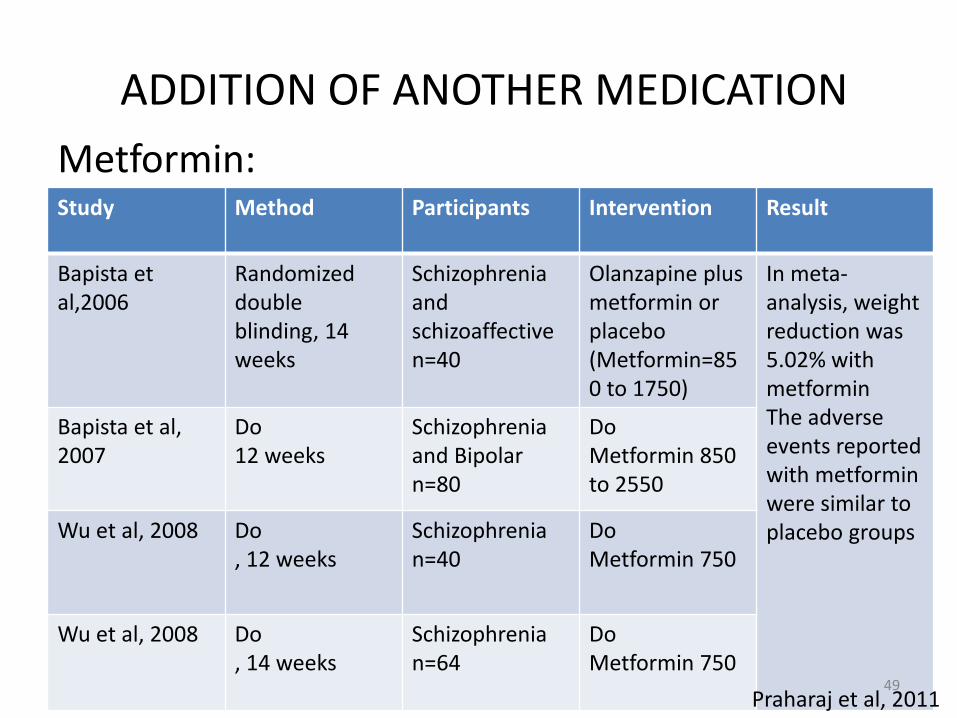
ADDITION OF ANOTHER MEDICATION
Metformin:Study Method Participants Intervention Result
Bapista et al,2006
Randomized double blinding, 14 weeks
Schizophreniaand schizoaffective n=40
Olanzapine plus metformin or placebo(Metformin=850 to 1750)
In meta-analysis, weight reduction was 5.02% with metforminThe adverse events reportedwith metformin were similar to placebo groups
Bapista et al, 2007
Do 12 weeks
Schizophrenia and Bipolar n=80
DoMetformin 850 to 2550
Wu et al, 2008 Do, 12 weeks
Schizophrenia n=40
DoMetformin 750
Wu et al, 2008 Do, 14 weeks
Schizophrenian=64
Do Metformin 750
Praharaj et al, 201149
ADDITION OF ANOTHER MEDICATION
Topiramate:• N=72 randomized to receive Olanzapine+placebo or
Olanzapine+Topiramate(100mg/day)
• Results: In the topiramate group there was found to be reduction of mean weight of 1.27±2.28 kg , decrease in glucose cholesterol and triglyceride level
Narula et al. 2010
• Topiramate with clozapine : no weight loss in a double-blind, placebo-controlled RCT in which weight gain was not the primary outcome parameter
Muscatello et al. 2011
• Some case reports but no controlled trials
– Modafinil
– Orlistat
– Rosaglitazone
50
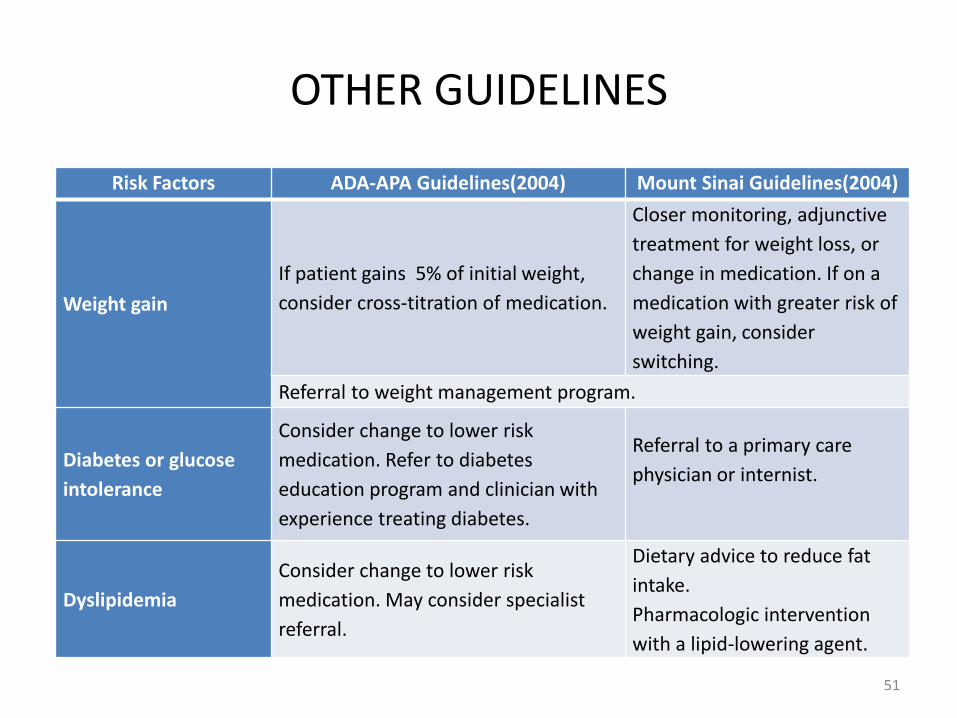
OTHER GUIDELINES
Risk Factors ADA-APA Guidelines(2004) Mount Sinai Guidelines(2004)
Weight gain
If patient gains 5% of initial weight,
consider cross-titration of medication.
Closer monitoring, adjunctive
treatment for weight loss, or
change in medication. If on a
medication with greater risk of
weight gain, consider
switching.
Referral to weight management program.
Diabetes or glucose
intolerance
Consider change to lower risk
medication. Refer to diabetes
education program and clinician with
experience treating diabetes.
Referral to a primary care
physician or internist.
Dyslipidemia
Consider change to lower risk
medication. May consider specialist
referral.
Dietary advice to reduce fat
intake.
Pharmacologic intervention
with a lipid-lowering agent.
51
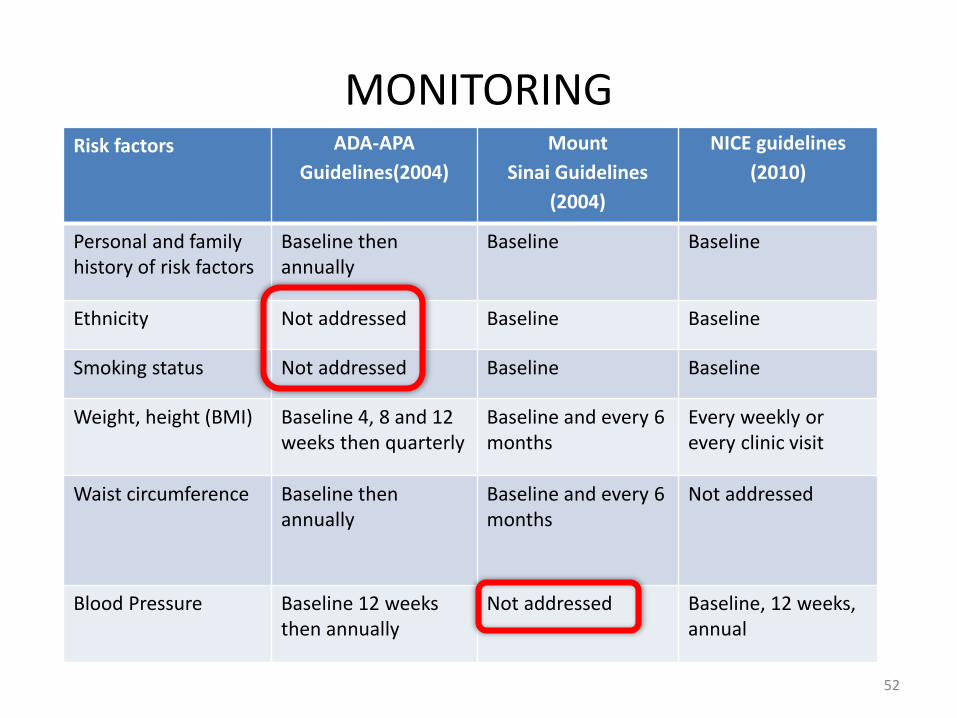
MONITORINGRisk factors ADA-APA
Guidelines(2004)
Mount
Sinai Guidelines
(2004)
NICE guidelines
(2010)
Personal and family history of risk factors
Baseline then annually
Baseline Baseline
Ethnicity Not addressed Baseline Baseline
Smoking status Not addressed Baseline Baseline
Weight, height (BMI) Baseline 4, 8 and 12 weeks then quarterly
Baseline and every 6 months
Every weekly or every clinic visit
Waist circumference Baseline then annually
Baseline and every 6 months
Not addressed
Blood Pressure Baseline 12 weeks then annually
Not addressed Baseline, 12 weeks, annual
52
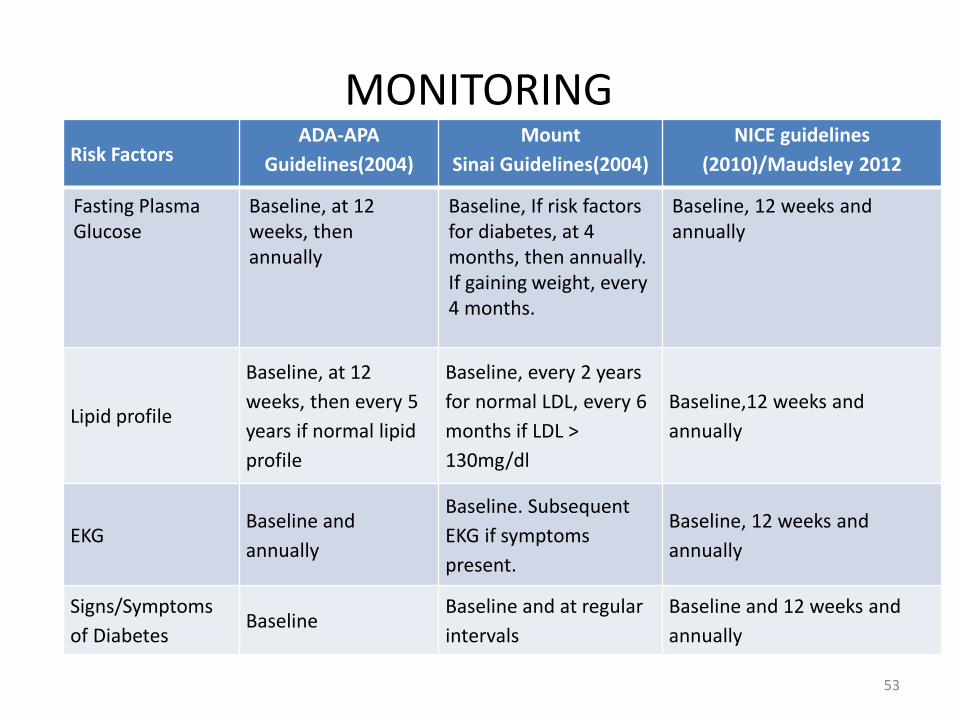
MONITORINGRisk Factors
ADA-APA
Guidelines(2004)
Mount
Sinai Guidelines(2004)
NICE guidelines
(2010)/Maudsley 2012
Fasting Plasma Glucose
Baseline, at 12 weeks, then annually
Baseline, If risk factors for diabetes, at 4 months, then annually. If gaining weight, every 4 months.
Baseline, 12 weeks and annually
Lipid profile
Baseline, at 12
weeks, then every 5
years if normal lipid
profile
Baseline, every 2 years
for normal LDL, every 6
months if LDL >
130mg/dl
Baseline,12 weeks and
annually
EKGBaseline and
annually
Baseline. Subsequent
EKG if symptoms
present.
Baseline, 12 weeks and
annually
Signs/Symptoms
of DiabetesBaseline
Baseline and at regular
intervals
Baseline and 12 weeks and
annually
53
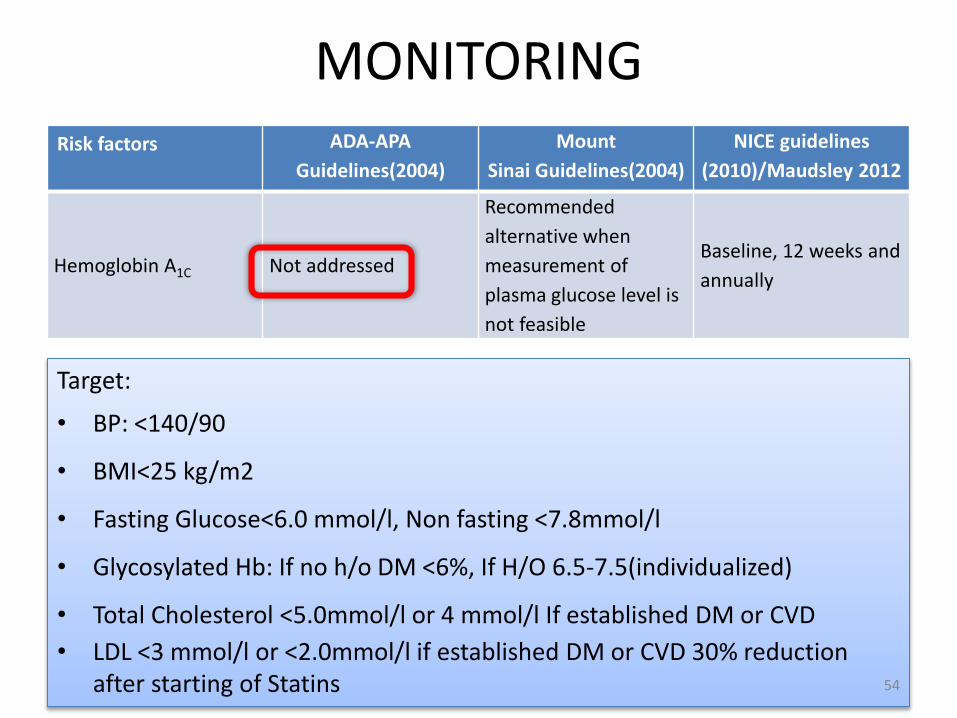
MONITORINGRisk factors ADA-APA
Guidelines(2004)
Mount
Sinai Guidelines(2004)
NICE guidelines
(2010)/Maudsley 2012
Hemoglobin A1C Not addressed
Recommended
alternative when
measurement of
plasma glucose level is
not feasible
Baseline, 12 weeks and
annually
Target:
• BP: <140/90
• BMI<25 kg/m2
• Fasting Glucose<6.0 mmol/l, Non fasting <7.8mmol/l
• Glycosylated Hb: If no h/o DM <6%, If H/O 6.5-7.5(individualized)
• Total Cholesterol <5.0mmol/l or 4 mmol/l If established DM or CVD
• LDL <3 mmol/l or <2.0mmol/l if established DM or CVD 30% reduction after starting of Statins 54

HYPERPROLACTINEMIA
Guidelines :
– Use lowest effective dosage
– Use of prolactin sparing antipsychotics
– Add another antipsychotic that normalizes prolactin like Aripiprazole
– Obtain a baseline prolactin level if any symptoms of raised prolactin present
– If still the symptoms explained by raised prolactin use of Bromocriptine or Cabergoline (risk of increasing psychotic symptoms )
Bostwick et al, 2009
55
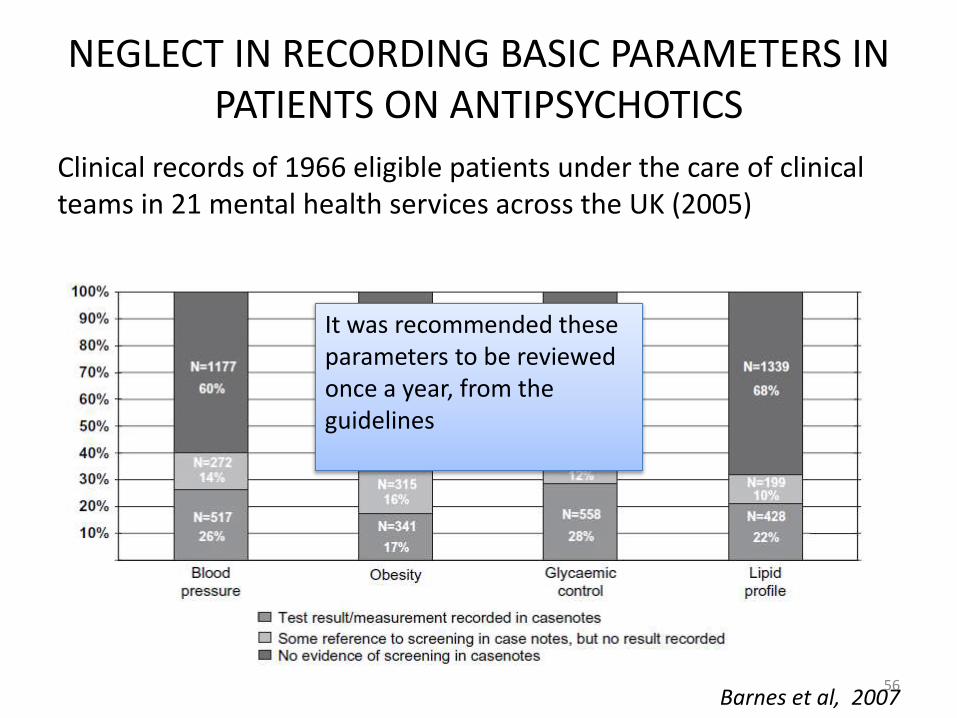
NEGLECT IN RECORDING BASIC PARAMETERS IN PATIENTS ON ANTIPSYCHOTICS
Clinical records of 1966 eligible patients under the care of clinical teams in 21 mental health services across the UK (2005)
Barnes et al, 2007
It was recommended these parameters to be reviewed once a year, from the guidelines
56
NEGLECT IN RECORDING BASIC PARAMETERS IN PATIENTS ON ANTIPSYCHOTICS
• Although blood pressure and obesity are relatively simple and easy to measure, the screening rates over the year for these variables were no better than those for tests requiring blood samples
• Increased rate of screening were seen for
– Patients on clozapine
– Advancing age
– Comorbid diagnosis of diabetes, dyslipidemia or hypertension
Barnes et al, 2007
57
• INTRODUCTION• HISTORCAL PERSPECTIVE• EPIDEMIOLOGY • PATHOPHYSIOLOGY• MANAGEMENT
PREVENTION PHARMACOTHERAPY MONITORING
• CONCLUSIONS • FUTURE DIRECTIONS
58
CONCLUSION• The metabolic and cardiovascular side effects of antipsychotics were
identified around a decade after its use started
• The potential of antipsychotic drugs to induce or trigger metabolic and cardiovascular dysregulation is firmly established but individual agents differ markedly in their propensities
• Despite the ease of measurement of the parameters for monitoring the side effects they largely remain unmonitored
• Regular monitoring and life style intervention a must for the patients receiving antipsychotics with high propensity of metabolic and cardiovascular side effects
• If still the side effects occur, multidisciplinary approach and addition of another medication can be done 59
FUTURE DIRECTIONS
• The search of antipsychotic free of all the metabolic and cardiovascular side effects is warranted
• Further research on the molecular mechanism of side effects could give better idea for newer drug development
• Regarding the switching of antipsychotics the larger studies taking the symptomatology into account would provide better insight
• Another area of research could be the genetic studies so that a earlier prediction could be made for the susceptibility to develop side effects
60

THANK YOU
61
Recommended