Dr.Mohammad Shekhani; CABM/FRCP
Reference:
Jim Fielder, RRT-NPS
Overlake Hospital Medical Center
Plus:
Dr.Mohammad Shekhani; CABM/FRCP
Reference:
Jim Fielder, RRT-NPS
Overlake Hospital Medical Center
Plus:
Prepared by:Prepared by:

Procedural Sedation
Procedural Sedation
The new Conscious SedationThe new Conscious Sedation

Procedural Sedation
Procedural Sedation A clinical technique that creates a decreased
level of awareness for a patient yet maintains protective airway reflexes and adequate spontaneous ventilation.
The goals of procedural sedation are to provide analgesia, amnesia, and anxiolysis(reduce anxiety) during a potentially painful or frightening procedure.
A clinical technique that creates a decreased level of awareness for a patient yet maintains protective airway reflexes and adequate spontaneous ventilation.
The goals of procedural sedation are to provide analgesia, amnesia, and anxiolysis(reduce anxiety) during a potentially painful or frightening procedure.

The Procedures
The Procedures Cardioversion
Thoracentesis Thoracotomy/chest tube placement Central catheter placement Transesophageal Echocardography Orthopedic/fracture reductions Dislocation reductions Endoscopy ERCP
Cardioversion Thoracentesis Thoracotomy/chest tube placement Central catheter placement Transesophageal Echocardography Orthopedic/fracture reductions Dislocation reductions Endoscopy ERCP

The Procedures continued:
The Procedures continued:
Percutaneous Tracheotomy Major dental procedures Laceration repair in both pediatrics and adults Bone marrow aspiration Burn or wound debridement Cardiac catheterization Interventional radiology procedures Circumcision And the list goes on. . . .
Percutaneous Tracheotomy Major dental procedures Laceration repair in both pediatrics and adults Bone marrow aspiration Burn or wound debridement Cardiac catheterization Interventional radiology procedures Circumcision And the list goes on. . . .

Procedural Sedation
Procedural Sedation And everyday patients are put at
risk: Oversedation At risk patients:
OSA Undiagnosed cardiac issues Hypersensitivity to sedation drugs Etc, etc.
And everyday patients are put at risk: Oversedation At risk patients:
OSA Undiagnosed cardiac issues Hypersensitivity to sedation drugs Etc, etc.

Procedural Sedation
Procedural Sedation These patients and their safety are in our
hands We must screen We must monitor We must have procedures in place to protect We must be prudent in our sedation and zealous
in our monitoring!
These patients and their safety are in our hands We must screen We must monitor We must have procedures in place to protect We must be prudent in our sedation and zealous
in our monitoring!

Our Path Today. . . Our Path Today. . . POX was the monitor in the past.
Capnography is “Gold Standard” for monitoring in Procedural Sedation
POX was the monitor in the past.
Capnography is “Gold Standard” for monitoring in Procedural Sedation

Procedural Sedation
Procedural Sedation Oximetery appeared in the 1980’s
It quickly became the 5th Vital Sign
Oximetery appeared in the 1980’s
It quickly became the 5th Vital Sign

OximetryOximetry Gained popularity
By 1987, the standard of care for the administration of a general anesthetic in the US included pulse oximetry
Gained popularity
By 1987, the standard of care for the administration of a general anesthetic in the US included pulse oximetry

OximetryOximetry It has been observed to be the
great cover-up “number” It has been observed to be the
great cover-up “number”

Capnography Emerges
Capnography Emerges
Abnormal ETCO2 findings were observed with many acute respiratory events. A majority of patients with acute respiratory events had ETCO2 abnormalities that occurred before oxygen desaturation or observed hypoventilation.
Acad Emer Med, 2006 May Burton JH, Harrah JD, Germann CA, Dillion
DC. Department of Emergency Medicine, Maine Medical Center, Portland, ME, US
Abnormal ETCO2 findings were observed with many acute respiratory events. A majority of patients with acute respiratory events had ETCO2 abnormalities that occurred before oxygen desaturation or observed hypoventilation.
Acad Emer Med, 2006 May Burton JH, Harrah JD, Germann CA, Dillion
DC. Department of Emergency Medicine, Maine Medical Center, Portland, ME, US

Capnography Emerges
Capnography Emerges
The results of this controlled effectiveness trial support routine use of microstream capnography to detect alveolar hypoventilation& reduce hypoxemia during procedural sedation in children. In addition, capnography allowed early detection of arterial oxygen desaturation because of alveolar hypoventilation in the presence of supplemental oxygen. The current standard of care for monitoring all patients receiving sedation relies overtly on pulse oximetry, which does not measure ventilation.
Pediatrics, 2006 Jun Lightdale JR, Goldman DA, Feldman HA, Newburg AR,
Dinardo JA, Fox VL. Children's Hospital Boston, Boston, Massachusetts, USA
The results of this controlled effectiveness trial support routine use of microstream capnography to detect alveolar hypoventilation& reduce hypoxemia during procedural sedation in children. In addition, capnography allowed early detection of arterial oxygen desaturation because of alveolar hypoventilation in the presence of supplemental oxygen. The current standard of care for monitoring all patients receiving sedation relies overtly on pulse oximetry, which does not measure ventilation.
Pediatrics, 2006 Jun Lightdale JR, Goldman DA, Feldman HA, Newburg AR,
Dinardo JA, Fox VL. Children's Hospital Boston, Boston, Massachusetts, USA

Capnography Emerges
Capnography Emerges
When propofol is administered for ED deep sedation to facilitate pediatric orthopedic reduction, continuous capnography detects most airway and respiratory events leading to intervention before clinical examination or pulse oximetry.
Ann Emerg Med 2007 Jan Anderson JL, Junkins E, Pribble C, Guenther. Division of
Pediatric Emergency Medicine, University of Utah, Salt Lake City, UT, USA
When propofol is administered for ED deep sedation to facilitate pediatric orthopedic reduction, continuous capnography detects most airway and respiratory events leading to intervention before clinical examination or pulse oximetry.
Ann Emerg Med 2007 Jan Anderson JL, Junkins E, Pribble C, Guenther. Division of
Pediatric Emergency Medicine, University of Utah, Salt Lake City, UT, USA

Capnography Emerges
Capnography Emerges
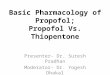
In the 1990’s Anesthesia came onboard and identified Capnography as a standard
Numerous articles, studies show Capnography catches what Oximetry can hide
In the 1990’s Anesthesia came onboard and identified Capnography as a standard
Numerous articles, studies show Capnography catches what Oximetry can hide
Capnography Tracing
Oximetery Tracing

Capnography Emerges
Capnography Emerges Other Professional Societies have come alongside Anesthesia
and have adopted Capnography and made it a new standard of care/monitoring Gastroenterology Emergency Medicine Orthopedics Critical Care Pediatrics
Other Professional Societies have come alongside Anesthesia and have adopted Capnography and made it a new standard of care/monitoring Gastroenterology Emergency Medicine Orthopedics Critical Care Pediatrics

Oridion Microstream The Oridion Microstream uses a disposable
technology that allows consistent results from both a cannula/clamshell or cannula/biteblock devices.
Oridion Microstream The Oridion Microstream uses a disposable
technology that allows consistent results from both a cannula/clamshell or cannula/biteblock devices.


EDP/GDP:EDP/GDP: The use of propofol by endoscopists & trained registered nurses for
endoscopy has been supported by a large body of evidence indicating its safety. Propofol, like all sedative agents,has inherent risks when it is misused. Relatively modest training allows responsible/appropriately cautious
individuals to titrate propofol as competently/ safely as they can administer opioids, benzodiazepines& other agents.
The benefits to patients of EDP are obvious& the cost savings of EDP compared with MAC are enormous.
The growth of EDP is inhibited by a lack of cooperation from the anesthesia community.
The evidence produced by endoscopists dedicated to the safe/ cost-effective administration of moderate sedation for endoscopy is
growing&evidence is a powerful harbinger of change.
The use of propofol by endoscopists & trained registered nurses for endoscopy has been supported by a large body of
evidence indicating its safety. Propofol, like all sedative agents,has inherent risks when it is misused. Relatively modest training allows responsible/appropriately cautious
individuals to titrate propofol as competently/ safely as they can administer opioids, benzodiazepines& other agents.
The benefits to patients of EDP are obvious& the cost savings of EDP compared with MAC are enormous.
The growth of EDP is inhibited by a lack of cooperation from the anesthesia community.
The evidence produced by endoscopists dedicated to the safe/ cost-effective administration of moderate sedation for endoscopy is
growing&evidence is a powerful harbinger of change.

Propofol adminstration principles:Propofol adminstration principles:
1. Propofol, has a time to peak effect of 90 seconds.
It also has a rapid offset of action, extended with cumulative dosing.
We must continually observe/ measure the patient’s level of sedation/ventilatory effort, airway patency/ level of sedation.
1. Propofol, has a time to peak effect of 90 seconds.
It also has a rapid offset of action, extended with cumulative dosing.
We must continually observe/ measure the patient’s level of sedation/ventilatory effort, airway patency/ level of sedation.

Propofol adminstration principles:Propofol adminstration principles: 2.Titration: EDP is usually done by giving boluses, in the same
fashion that other agents for endoscopist-delivered sedation are given.
The size of the bolus is chosen based on the patient’s size, age& comorbidities& whether the patient has received adjunctive opioids and/or benzodiazepines& their respective doses.
EDP is very different from that commonly used by anesthesiologists using propofol to induce GA
2.Titration: EDP is usually done by giving boluses, in the same fashion that other agents for endoscopist-delivered sedation are given.
The size of the bolus is chosen based on the patient’s size, age& comorbidities& whether the patient has received adjunctive opioids and/or benzodiazepines& their respective doses.
EDP is very different from that commonly used by anesthesiologists using propofol to induce GA

Propofol adminstration principles:Propofol adminstration principles: An initial bolus of 20-40 mg is followed by repeated boluses of 10-
20 mg, typically never given at an interval closer than 20 seconds apart.
Pretreatment with low doses of benzodiazepines& opioids (eg, midazolam 1 mg/ fentanyl 50 mg) will reduce the size of boluses, frequency of administration,& total dose of propofol required by more than half.
An initial bolus of 20-40 mg is followed by repeated boluses of 10-20 mg, typically never given at an interval closer than 20 seconds apart.
Pretreatment with low doses of benzodiazepines& opioids (eg, midazolam 1 mg/ fentanyl 50 mg) will reduce the size of boluses, frequency of administration,& total dose of propofol required by more than half.

Propofol adminstration principles:Propofol adminstration principles: The principles of titration include the recognition that there is a
3- to–5-fold variability between individuals in their pharmacologic response to sedative agents, including propofol.
During titration , the need for& size of additional boluses is determined by observation of the patient’s level of sedation & ventilatory effort.
The frequency of administration of propofol is greater than tradi- tional agents because the duration of action is shorter.
The principles of titration include the recognition that there is a 3- to–5-fold variability between individuals in their pharmacologic response to sedative agents, including propofol.
During titration , the need for& size of additional boluses is determined by observation of the patient’s level of sedation & ventilatory effort.
The frequency of administration of propofol is greater than tradi- tional agents because the duration of action is shorter.

Propofol adminstration principles:Propofol adminstration principles: Most EDP has been performed without capnography, but it
provides additional information about ventilation&it is not a substitute for continuous monitoring of ventilation & airway patency.
Bispectral monitoring typically lags too far behind the sedation level to be useful in the titration process for short procedures, such as endoscopy.
Continuous monitoring of ventilation by clinical means as well as monitoring of pulse oximetry, blood pressure, heart rate& cardiac rhythm are required
Most EDP has been performed without capnography, but it provides additional information about ventilation&it is not a substitute for continuous monitoring of ventilation & airway patency.
Bispectral monitoring typically lags too far behind the sedation level to be useful in the titration process for short procedures, such as endoscopy.
Continuous monitoring of ventilation by clinical means as well as monitoring of pulse oximetry, blood pressure, heart rate& cardiac rhythm are required






Thank You
Thank You
Recommended