Gestational Trophoblastic Diseases
Sana Afridi Final year MBBS
08-168
Objectives
• What is gestational trophoblastic diseases?
• Classification of gestational trophoblastic diseases.
• Clinical picture, signs symptoms.• Diagnosis, treatment of is gestational
trophoblastic diseases.
Gestational Trophoblastic Diseases
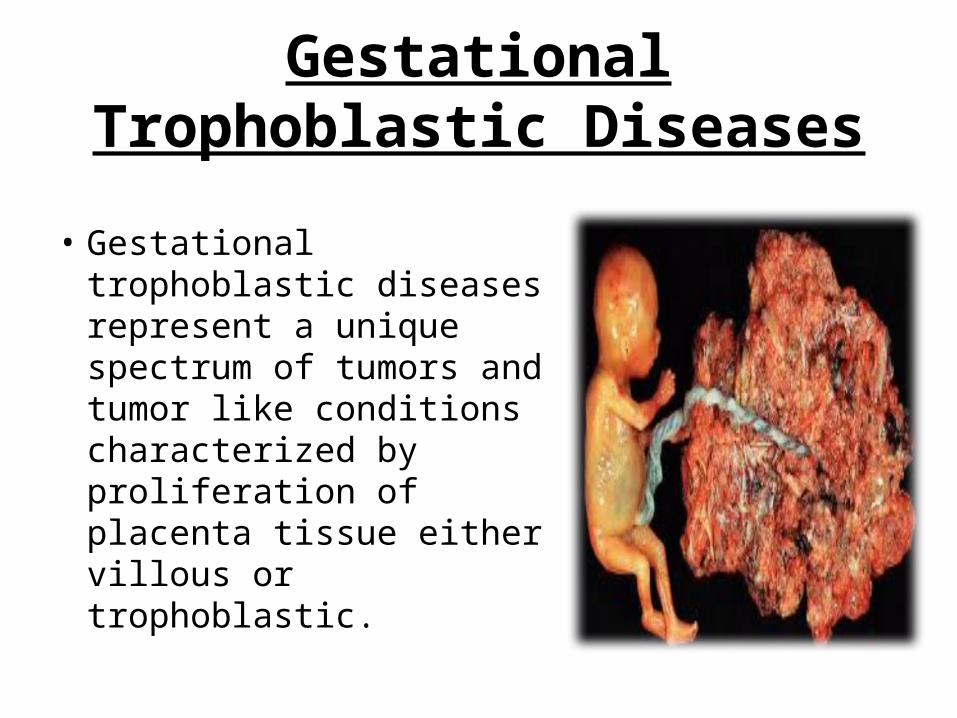
• Gestational trophoblastic diseases represent a unique spectrum of tumors and tumor like conditions characterized by proliferation of placenta tissue either villous or trophoblastic.
• the incidence of GTD varies greatly between different parts of the world.
• The reported incidence of hydatidiform mole ranges from 23 to 1299 cases per 100,000 pregnancies.
Epidemiology
Predisposing Factors:- • Age below 15 and above 40 years.• Previous History of hydatidiform mole • Previous Miscarriage• Excessive smoking• Reduced B carotene intake
PATHOLOGICAL CLASSIFICATION
1. Hydatiditorm mole. (85 %)2. Invasive mole. (12-15%)3. Gestational choriocarcinoma.(5-8%)4. Placental site Trophoblastic tumor.
Complete
Partial
Clinical Classification.
Benign ( 80%). Malignant (20%).
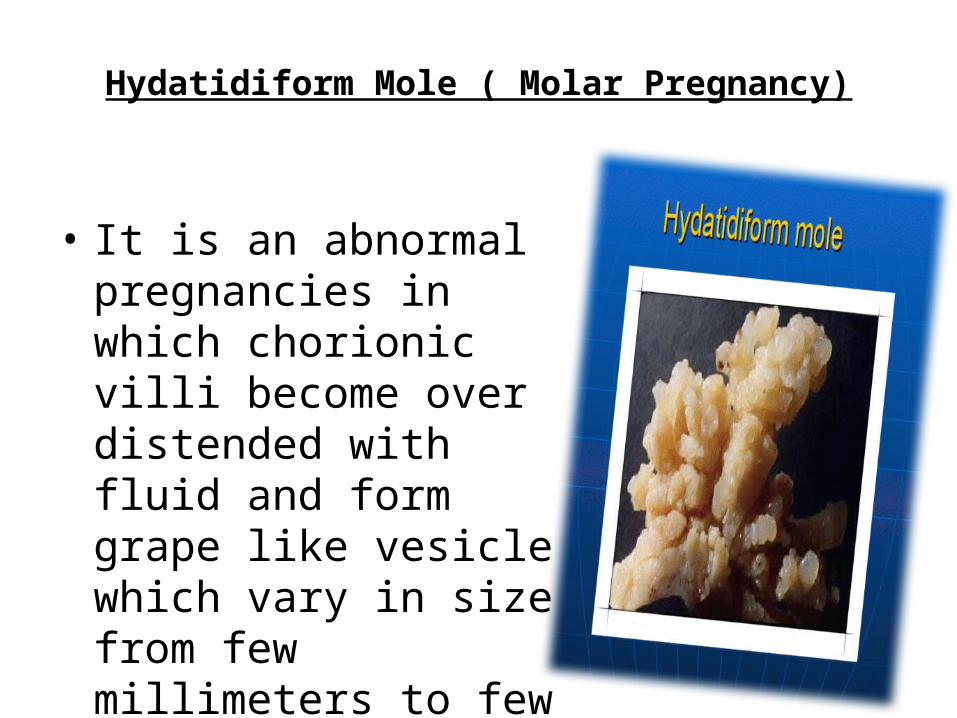
Hydatidiform Mole ( Molar Pregnancy)
• It is an abnormal pregnancies in which chorionic villi become over distended with fluid and form grape like vesicle which vary in size from few millimeters to few centimeters.
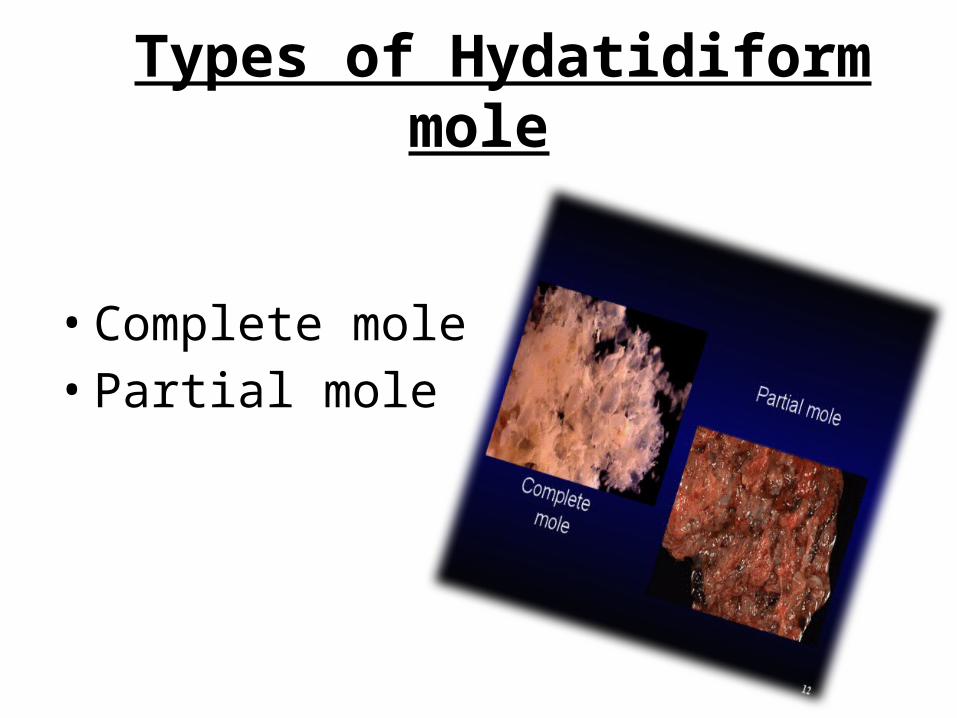
Types of Hydatidiform mole
• Complete mole• Partial mole
Complete Mole
• An abnormal pregnancy which consists of placental tissue only and there is no embryo in it.
Pronounced trophoblastic hyperplasia having both cytotrophoblastic and synctial elements.
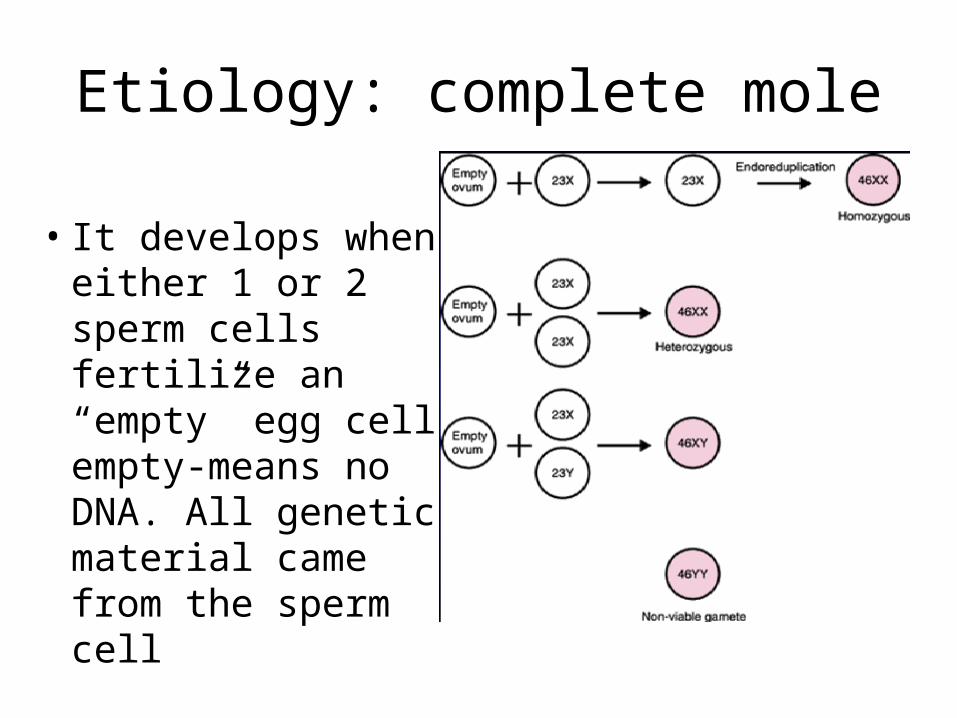
Etiology: complete mole
• It develops when either 1 or 2 sperm cells fertilize an “empty” egg cell empty-means no DNA. All genetic material came from the sperm cell

Complete MOLE
Partial mole
• In this form the embryo or fetus coexist with placenta abnormality through it tends to die at an early cystitis.
• In abnormal parts of placenta the hyperplasia only involve synctiotrophoblast.
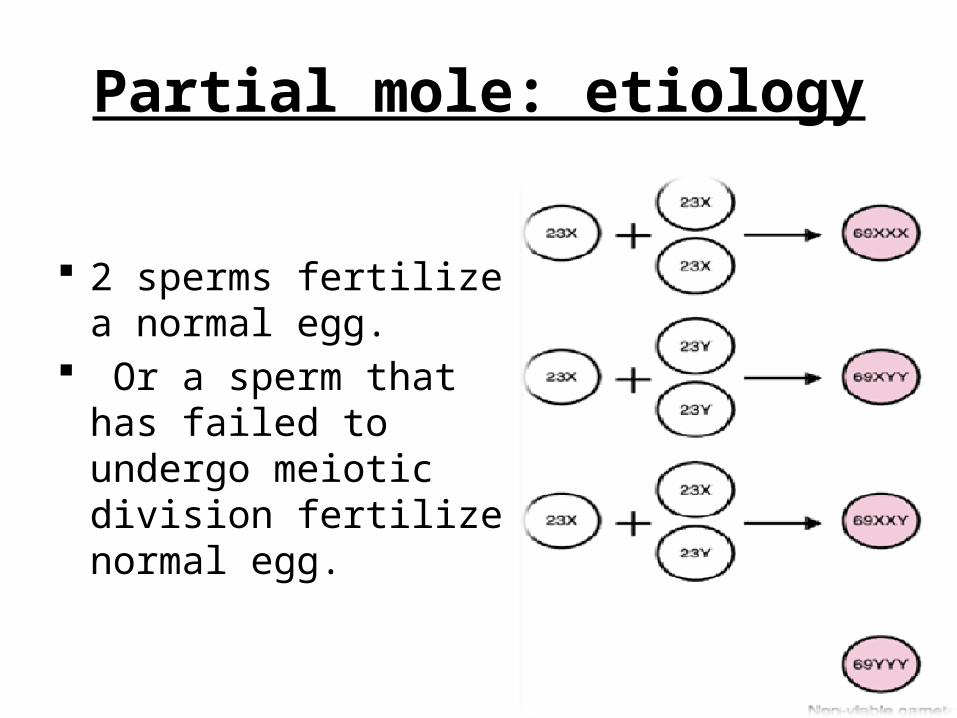
Partial mole: etiology
2 sperms fertilize a normal egg.
Or a sperm that has failed to undergo meiotic division fertilize normal egg.
Clinical Features: SYMPTOMS
• Symptoms of early pregnancy:- Patients history of amenorrhea usually for 4-6 months.
.
Clinical presentation
• Vaginal Bleeding:- Patient complains of recurrent vaginal bleeding something there is history of brownish vaginal discharge. Bleeding usually starts is 3rd or 4th months of pregnancy.
• Absence of Quickening:- Fetal movements are never felt except in partial mole.
Clinical features: SIGNS
1. Size of uterus:- In most cases the size of uterus is excessively larger than expected for duration of amenorrhea.
2. Absence of uterus Contractions:- In molar pregnancy the uterus feels doughy and does not contract.
3.Bilateral ovarian enlargement:- In 25% cases bilateral ovarian enlargement palpable.
4.Absence of Foetal Part:- Foetal part not palpable and feotal heart is absent.
5.Pre eclampcia:- In 50% case signs of preeclampsia especially in first half of pregnancy.
DIAGNOSIS
• Ultrasonography: Snow storm appearance on ultrasound.
• Beta HCG level:- HCG ideal marker for diagnosis of gestational trophoblastic disease. Hcg is produced by synctiotrophoblast cell of placenta. In normal pregnancy its max amount is produced at 8-10 weeks and after it falls..
• In molar pregnancy it is produced in very large amount and its serum and urine level continue to risk beyond 12 weeks of amenorrhea.
• Pre Treatment Investigations:-
Include:-• Hb estimation diagnosis of anemia.• Blood grouping and cross matching for
transfusion.• X.ray chest To rule out primary metastasis.• T3 and T4 estimates. When thyrotoxicosis is
expected.
Treatment
• The aim of treatment is to remove trophoblastic tissue from uterus and eliminate it from other body system.
Evacuation of H Mole 1. Suction Curettage.
Method of choice for evacuation of H mole under 16 weeks of gestation
• After General Anesthetic → cervix is dilated to size of 12mm.
• Suction curette is introduced → • A negative pressure of 60-70 cm H2O is
created and suction preformed
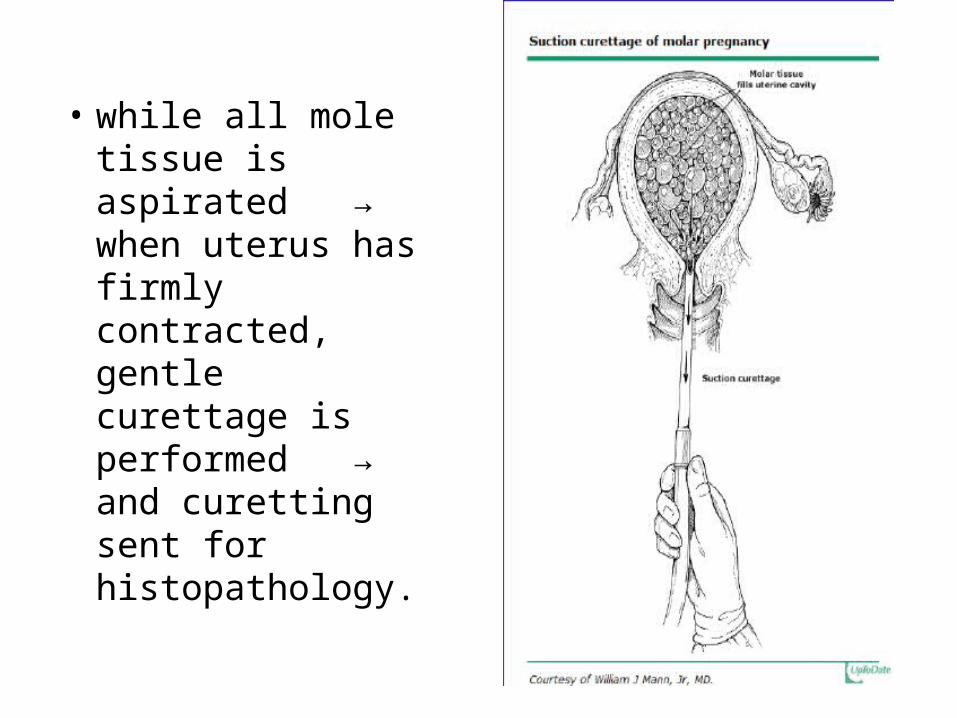
• while all mole tissue is aspirated → when uterus has firmly contracted, gentle curettage is performed → and curetting sent for histopathology.
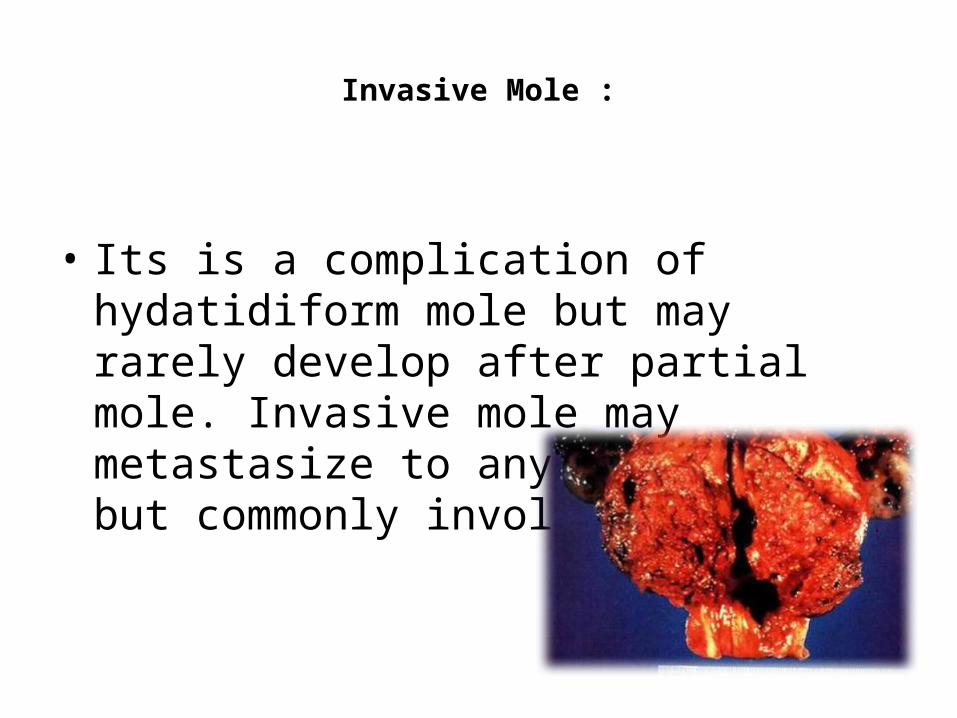
Invasive Mole :
• Its is a complication of hydatidiform mole but may rarely develop after partial mole. Invasive mole may metastasize to any part of body but commonly involves lungs.
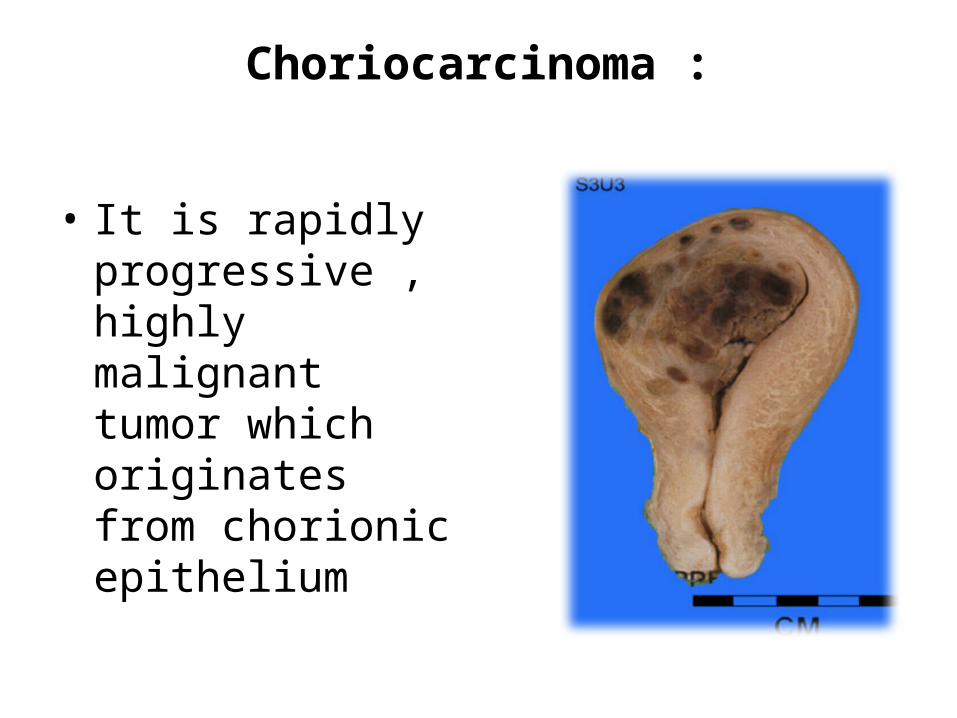
Choriocarcinoma :
• It is rapidly progressive , highly malignant tumor which originates from chorionic epithelium
Clinical features :
• Vaginal bleeding: intermittent vaginal bleeding• Vaginal discharge: brownish vaginal discharge• Other: weakness• Cough• Neurological symptoms• Abdominal or vaginal mass• Amenorrhea `
Investigations:
• Raised hCG levels• Biopsy• X-ray Chest• Ultrasonography• C.T scan
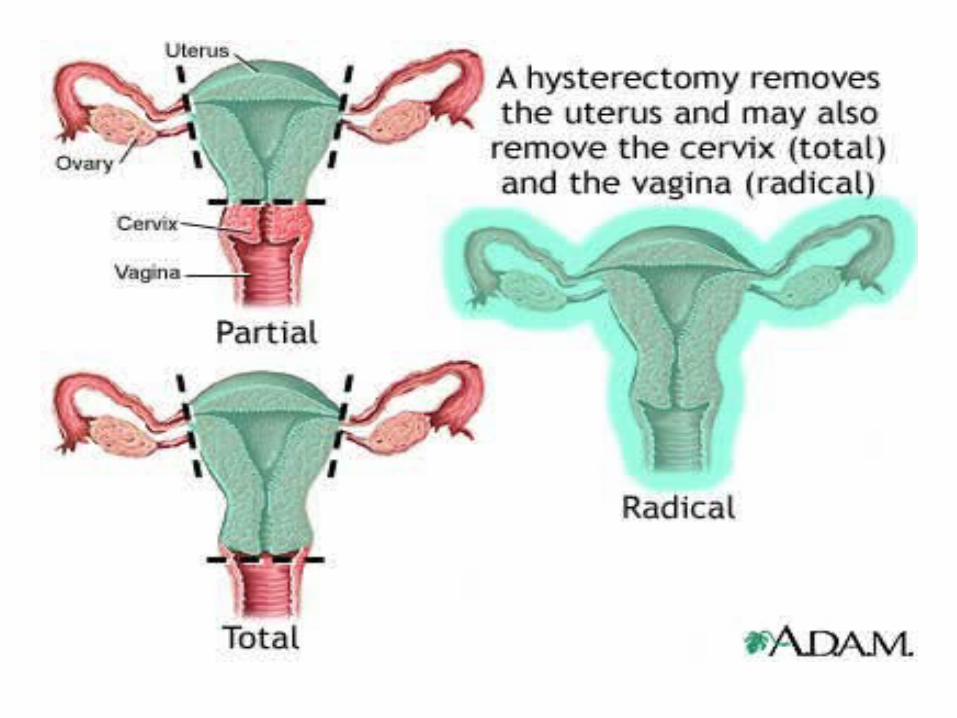
Treatment
• Chemotherapy• Surgery: Hysterectomy.
THANKS
Recommended