-
8/12/2019 Gestational Trophoblastic Disease ppt
1/43
Fetal Medicine
Gestational Trophoblastic Disease
Jeannet E. Canda, RN,MAED
NDDUCollege of Nursing
-
8/12/2019 Gestational Trophoblastic Disease ppt
2/43
Fetal Medicine
Gestational Trophoblastic Disease (GTD)is a relatively rare
event with a calculated incidence of 1/714 livebirths.
There is evidence of ethnic variation in the incidence of GTD in
theUK, with women from Asia having a higher incidence compared
withnon-Asian women (1/387 versus 1/752 live births).
This may under-represent the true incidence of the
diseasebecause of problems with reporting, particularly with regard
topartial moles.
-
8/12/2019 Gestational Trophoblastic Disease ppt
3/43
Fetal Medicine
Hydatiform mole
Invasive mole
Choriocarcinoma
Placental site trophoblastic tumor
Partial
Complete
GESTATIONAL TROPHOBLASTIC DISEASE
-
8/12/2019 Gestational Trophoblastic Disease ppt
4/43
Fetal Medicine
Epidemiology
The incidence of molar pregnancy varies in different parts of
the
world.
Women of Asian origin: 1 in 550 to 1 in 600.
Women of European origin: 1 in 1200 live births
-
8/12/2019 Gestational Trophoblastic Disease ppt
5/43
Fetal Medicine
Age is probably the most important factor in the incidence
ofdeveloping complete hydatidiform mole.
Where the incidence for women aged 25 to 29 is standardized
as 1, the risk is
6 X in women who become pregnant under 15 years
411 X in patients who become pregnant over the age of 50
Epidemiology
-
8/12/2019 Gestational Trophoblastic Disease ppt
6/43
Fetal Medicine
North America and Europe:
Partial mole 1/700
Complete mole 1/1500-2000
Asian Countries:
Partial mole 1/120
Complete mole 1/350-500
HYDATIDIFORM MOLE
Incidence
-
8/12/2019 Gestational Trophoblastic Disease ppt
7/43
Fetal Medicine
1. Maternal age > 40 years
< 15 years
2. Paternal age > 45 years
3. Previous hydatidiform mole 1st
1-2%2nd 15-28%
4. Vitamin A deficiency
HYDATIDIFORM MOLE
Risk factors
-
8/12/2019 Gestational Trophoblastic Disease ppt
8/43
Fetal Medicine
Background
Hydatidiform mole is subdivided into complete and partial
molebased on genetic and histo-pathological features.
Complete moles are diploid andro-genetic in origin no evidence
of fetal tissue.
Arise as a consequence of
1. duplication of the haploid sperm following fertilisation of
an emptyovum ( diandry)2. Some complete moles arise after dispermic
fertilisation of an
empty ovum. (dispermy)
Molar PregnancyComplete Mole
-
8/12/2019 Gestational Trophoblastic Disease ppt
9/43
Fetal Medicine
Emptyovum
Empty
ovum
46XX
46XX
or 46XY
23X or Y23X
23XComplete Mole
(46XX diploid)
Complete Mole (46XXor 46XY, diploid)
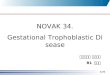
A single sperm fertilizes an
empty ovum, with duplicationof the 23X haploid set
ofchromosomes, giving rise to ahomozygous diploid complete
mole.
Two sperms with twoindependent haploid sets ofchromosomes
fertilize anempty ovum, producing a
dyspermic complete mole witheither 46XX or 46XY
karyotype.
COMPLETE MOLE
Modified from Cheung, 1995
-
8/12/2019 Gestational Trophoblastic Disease ppt
10/43
Fetal Medicine
Complete molar pregnancy
Complete hydatidiform mole forms a multivesicular mass
withdiffuse hydropic villi and a variable degree of
trophoblasticproliferation.
There is usually no evidence of a foetus. This conceptus is
diploid
and androgenetic in origin.
The incidence of a GT Tumour is approximately 1000X more
likelyfollowing a complete hydatidiform mole than after a
full-term
pregnancy.One possible explanation is that genomic imprinting
plays arole in tumourigenesis since the complete mole is
androgenetic inorigin.
-
8/12/2019 Gestational Trophoblastic Disease ppt
11/43
-
8/12/2019 Gestational Trophoblastic Disease ppt
12/43
Fetal Medicine
l d
-
8/12/2019 Gestational Trophoblastic Disease ppt
13/43
Fetal Medicine
F l M d
-
8/12/2019 Gestational Trophoblastic Disease ppt
14/43
Fetal Medicine
F l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
15/43
Fetal Medicine
Triploid in origin with usually two sets of paternal haploid
genes and
one set of maternal haploid genes.
They occur, in almost all cases, following
dispermicfertilisation of an ovum. There is usually evidence of a
fetusor fetal red blood cells.
In some cases failure of meiosis I or II in the ovum leads
to
Triploidy with 46 maternally derived chromosomes and
23paternal
Partial Molar Pregnancy
F t l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
16/43
Fetal Medicine
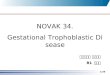
23X 23X
Dyspermy23X/23Y or23X/23X
23Y
Partial Mole (69XXY,or 69XXX, or 69XYY
triploid)
PARTIAL MOLE
23X
23X
23Y
69XXY
Fertilization of a normal 23X haploid ovum by two sperms,
producing atriploid partial mole with either 69XXY, 69XXX or 69XYY
karyotype
Modified from Cheung, 1995
F t l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
17/43
Fetal Medicine
Fetal or embryonic tissue absent present
Hydatiform swelling of chorionic villi extensive focal
Trophoblastic hyperplasia extensive focal
Scalloping of chorionic villi absent present
Trophoblastic stromal inclusions absent present
Karyotype 46XX (90%); Triploid (69 XXY)
46XY (10%)
Complete mole Partial mole
Cohn DE, Herzog TJ. Curr Opin Oncol 2000 Sep; 12(5):492-6
FEATURES OF PARTIAL AND COMPLETE MOLE
F t l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
18/43
Fetal Medicine
F t l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
19/43
Fetal Medicine
Persistent GTD
The term persistent "gestational trophoblastic disease" is
widelyused to describe the situation where a woman has had
ahydatidiform mole and still has persistently raised human
chorionicgonadotrophin (hCG) estimations
Since in the majority of cases the disease either
remitsspontaneously or can be successfully treated without
furtherpathological sampling, it is difficult to say exactlyin
whatproportion of patients their hydatiform mole modulates to
choriocarcinoma.This event probably happens in 3% to 5% of
patients who have hada complete hydatidiform mole
F t l M di i
-
8/12/2019 Gestational Trophoblastic Disease ppt
20/43
Fetal Medicine
Gestational Trophoblastic Disease
Persistent GTD may develop
1. After a molar pregnancy,
2. After a non-molar pregnancy3. After a live birth (~ 1/50
000)
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
21/43
Fetal Medicine
Gestational Trophoblastic Tumours
Overview
GTT are unique in cancer biology in that they follow
1. either a normal or abnormal pregnancy,
2. the tumours contain paternal genes and are therefore
anallograft in the maternal host.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
22/43
Fetal Medicine
Invasive Hydatidiform Mole
Invasive hydatidiform mole (complete or partial) is common
since
molar trophoblast invades the myometrium in most cases.
Pathologically invasive hydatidiform mole can be diagnosed
only
when sufficient myometrium is made available to the
pathologist
either on curettings or by hysterectomy
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
23/43
Fetal Medicine
Invasive Hydatidiform Mole
An invasive mole retains hydropic villi, which penetrate
theuterine wall.
Can cause uterine rupture and can be life threatening.
Hydropic villi may embolize to distant organs, but this
tumordoes not have metastatic potential.
Cure is possible by hysterectomy or chemotherapy.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
24/43
Fetal Medicine
Choriocarcinoma
It is an unusual tumour in that it stimulates virtually no
stromal
reaction and is therefore essentially a mixture of haemorrhage
and
necrosis with tumour cells scattered within the mass.
Tumour cells can be scanty and present problems of
pathologicalinterpretation if the possibility of choriocarcinoma
has not been
raised.
The pathology of choriocarcinoma is reflected in its
clinicalbehaviour with widespread intravascular dissemination to
lungs,
brain and other sites.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
25/43
Fetal Medicine
Choriocarcinoma
Is a very aggressive malignant tumor and arises either from
gestational chorionic epithelium or less frequently, from
totipotential cells within gonads or elsewhere.
Incidence is 1/ 30,000 pregnancies in US.
More common in Asian and African countries.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
26/43
Fetal Medicine
Choriocarcinoma
Most cases are discovered by the appearance of a bloody,
brownishdischarge, accompanied by a rising titer of HCG,
particularly thebeta subunit.
Usually appear as very hemorrhagic, necrotic masses within
theuterus.
Widespread dissemination via blood, lung (50%), vagina
(30-40%),
brain, liver and kidney.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
27/43
Fetal Medicine
Placental site trophoblastic tumours
Placental site trophoblastic tumours are now recognised as
aseparate entity.
1. rare and2. are composed mainly of cytotrophoblastic cells
3. tend to be locally invasive4. less widely metastatic than
choriocarcinoma
The optimal management of patients with placental
sitetrophoblastic tumours is unclear.
This is because(i) the tumours are rare and(ii) their biological
behaviour does appear to be variable.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
28/43
Fetal Medicine
Where the disease is localised to the uterus, hysterectomy is
thetreatment of choice.
A small number of patients treated with intensive
chemotherapyinitially have achieved complete remission but the
chemosensitivityof placental site trophoblastic tumours appears to
be quite variable
Placental site trophoblastic tumours
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
29/43
Fetal Medicine
Clinical presentation
The most common presentation of a patient with a GTD is1.
vaginal bleeding towards the end of the first trimester of
pregnancy.2. nausea and vomiting and3. uterus larger for dates
than for a normal pregnancy.
Since the quantity of hCG produced by a normal pregnancy can
varyover quite a wide range, the initial hCG estimation is not
helpful in
differentiating between a pregnancy and a hydatidiform mole.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
30/43
Fetal Medicine
COMPLETE HYDATIFORM MOLE
CLINICAL FEATURES
Vaginal bleeding (anemia) 97%
Excessive uterine size 50%
Theco-lutein ovarian cysts 50%
Preeclampsia 27%
Hyperemesis 25%
Hyperthyroidism 7%
Trophoblastic embolization 2%(respiratory distress)
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
31/43
Fetal Medicine
The increasing performance of ultrasound examination,
either routinely in the first trimester or for management of
early pregnancy complications, allows evacuation of
mostpregnancies affected by hydatiform mole prior to
development of the classic sonographic and pathological
features.
ULTRASOUND FINDINGS
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
32/43
Fetal Medicine
Multiple hypoechoic areas extensive focal
Increased echogenicity extensive focalEnlarged uterine volume
present absent
Theca-lutein cysts present absent
> gestational sac - present
< Uterine artery PI present -
Complete mole Partial mole
ULTRASOUND FINDINGS
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
33/43
Fetal Medicine
Diagnosis of Gestational Trophoblastic Disease
Increasing use of ultrasound in early pregnancy has led to
the
earlier diagnosis of molar pregnancy.
The majority of histologically proven complete moles however
are
associated with an ultrasound diagnosis of delayed miscarriage
oranembryonic pregnancy
The ultrasound features of a complete mole are reliable but
the
ultrasound diagnosis of a partial molar pregnancy is more
complex.RCOG, February 2004
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
34/43
Fetal Medicine
Management of GTD
Suction curettage is the method of choice of evacuation for
complete molar pregnancies.
Because of the lack of fetal parts a suction catheter, up to
a
maximum of 12 mm, is usually sufficient to evacuate all
completemolar pregnancies
Medical termination of complete molar pregnancies, including
cervical preparation prior to suction evacuation, should be
avoidedwhere possible because of the potential to embolise and
disseminate trophoblastic tissue through the venous system
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
35/43
Fetal Medicine
In partial molar pregnancies where the size of the fetal
partsdeters the use of suction curettage, medical termination can
beused.
These women may be at an increased risk of requiring
treatmentfor persistent trophoblastic neoplasia, although the
proportion ofwomen with partial molar pregnancies needing
chemotherapy is low(0.5%)
Management of GTD
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
36/43
Fetal Medicine
Gestational Tropholastic Neoplasia-Requirement for diagnosis
1. 4 or more values of hCG plateau over ay least 3 weeks
2. A rise of hCG of 10% or greater for > 3 values over at
least 2weeks
3. Presence of Choriocarcinoma
4. Persistence of hCG 6 months after mole evacuation
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
37/43
F
Women scoring >7 (high risk) receive combination
chemotherapy.
IV Etoposide, Methotrexate, Actinomycin D for 2 daysfollowed by
Cyclophosphamide and Vincristine (Oncovin) (EMA-CO)
one week later.
The course is then repeated after six days.Charing Cross
Hospital, London
Treatment of persistent GTD
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
38/43
Future pregnancy
Women should be advised not to conceive until their hCG
levels
have been normal for six months.
Women who undergo chemotherapy are advised not to conceive
for
one year after completion of treatment
Risk of a further molar pregnancy is low (~ 2%)
>98% of women who become pregnant following a molar
pregnancy
will not have a further mole or be at increased risk of
obstetric
complications.
If a further molar pregnancy does occur, in 6880% of cases it
will
be of the same histological type
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
39/43
Follow-up and Fertility after Chemotherapy
Approximately 90% of patients who want to become pregnant
following chemotherapy have succeeded and there is no evidence
of
increase in foetal abnormalities.
Occasionally a G.T.T. can occur or recur after a subsequent
normalpregnancy
This emphasises the importance of reconfirming that hCG
levels
return to normal after any subsequent pregnancy in a woman
who
has had a trophoblastic disease event
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
40/43
Contraception and hormone replacementtherapy
The COC-pill, if taken while hCG levels are raised, may increase
theneed for treatment.
However, it can be used safely after the hCG levels have
returnedto normal.
Other forms of hormonal contraception do not appear to be
linkedto an increased need for treatment.
The small potential risk of using emergency
hormonalcontraception, in women with raised hCG levels, is
outweighed by
the potential risk of pregnancy to the woman.
Hormone replacement therapy may be used safely once hCG
levelshave returned to normal.
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
41/43
Survival
The overall survival in the Charing Cross series, with a
maximum
follow-up of 15 years is ~ 94%
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
42/43
The successful outcome in patients with GTT depends on
severalfactors:-
(i)Need for a national registration scheme of patients at risk
ofdeveloping a GTT(ii)The ability to monitor the disease and its
response totreatment with serial hCG estimations.(iii)The intrinsic
biological property of GTT in being inherentlyvery sensitive to a
range of chemotherapeutic agents.
Survival
Fetal Medicine
-
8/12/2019 Gestational Trophoblastic Disease ppt
43/43
Thank you